Back to Journals » Drug Design, Development and Therapy » Volume 19
Optimizing Micafungin Dosing in Patients with Critically Ill Candidemia and Trends of Candida Species Causing Bloodstream Infections in a Tertiary Hospital in Thailand: A Monte Carlo Simulation Approach
Authors Watcharasuwanseree J, Chueansuwan W, Suwantarat N ![]() , Santimaleeworagun W, Juntanawiwat P, Sangchankoom A, Saelim W
, Santimaleeworagun W, Juntanawiwat P, Sangchankoom A, Saelim W ![]()
Received 11 July 2025
Accepted for publication 13 October 2025
Published 24 October 2025 Volume 2025:19 Pages 9535—9544
DOI https://doi.org/10.2147/DDDT.S549066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Jutharat Watcharasuwanseree,1,2 Worawong Chueansuwan,3 Nuntra Suwantarat,4 Wichai Santimaleeworagun,5,6 Piraporn Juntanawiwat,7 Adisak Sangchankoom,8 Weerayuth Saelim5,6
1The College of Pharmacotherapy of Thailand, Nonthaburi, Thailand; 2Department of Pharmaceutical Care, Faculty of Pharmacy, Thammasat University, Pathumthani, Thailand; 3Division of Infectious Diseases, Department of Internal Medicine, Phramongkutklao Hospital and College of Medicine, Bangkok, Thailand; 4Division of Infectious Diseases, Department of Internal Medicine, Chulabhorn International College of Medicine, Thammasat University, Pathumthani, Thailand; 5Division of Pharmaceutical Care, Faculty of Pharmacy, Silpakorn University, Nakhon Pathom, Thailand; 6Pharmaceutical Initiative for Resistant Bacteria and Infectious Diseases Working Group [PIRBIG], Faculty of Pharmacy, Silpakorn University, Nakhon Pathom, Thailand; 7Department of Clinical Pathology, Division of Microbiology, Phramongkutklao Hospital, Bangkok, Thailand; 8Division of Microbiology, Clinical Laboratory, Udonthani Hospital, Udonthani, Thailand
Correspondence: Weerayuth Saelim, Division of Pharmaceutical Care, Faculty of Pharmacy, Silpakorn University, Nakhon Pathom, 73000, Thailand, Tel +6634 255 800, Fax +6634 255 801, Email [email protected]
Purpose: This study aimed to determine the optimal micafungin dosage for treating candidemia in critically ill adult patients using Monte Carlo simulation.
Patients and Methods: Clinical Candida isolates were obtained from blood cultures collected between September 2023 and December 2024 at Phramongkutklao Hospital, Thammasat University Hospital, and Udonthani Hospital. Susceptibility testing was performed using the Sensititre® YeastOne® system, applying a broth microdilution method in 96-well plates to determine minimum inhibitory concentrations (MICs). Monte Carlo simulations were conducted to identify optimal micafungin dosing regimens, using cumulative fraction of response (CFR) and probability of target attainment (PTA) as key parameters.
Results: In total, 128 clinical Candida isolates were identified. Candida tropicalis was the most frequently isolated species (32%), followed by C. albicans (22.7%), C. parapsilosis (16.4%), C. glabrata (Nakaseomyces glabrata) (12.5%), and C. auris (Candidozyma auris) (9.4%). The micafungin MIC ranges were as follows: C. tropicalis, 0.015– 0.25 μg/mL; C. albicans, 0.008– 0.015 μg/mL; C. parapsilosis, 0.5– 2 μg/mL; C. glabrata, 0.015–> 8 μg/mL; and C. auris, 0.12– 0.25 μg/mL. Pan-echinocandin-resistant C. glabrata was also detected. A standard micafungin dose (100 mg/day) may be effective for C. tropicalis infections when MIC is ≤ 0.015 μg/mL. In patients with Sequential Organ Failure Assessment scores > 10 and alanine aminotransferase > 120 U/L, the standard micafungin dose adequate CFR for empirical therapy and PTA for documented treatment at MICs up to 0.03 μg/mL, with the target threshold set at ≥ 90%. However, in the absence of MIC data and with increasing MIC trends, a higher empirical dose (up to 400 mg/day) may be warranted.
Conclusion: Non-albicans Candida bloodstream infections are increasing, along with higher MIC trends, signaling emerging resistance. Standard dosing may be insufficient in critically ill patients. Empirical high-dose micafungin could improve treatment efficacy.
Keywords: MIC distribution, ICU patient, empirical dosing, invasive candidiasis
Introduction
Candida species are common components of the normal human microbiota but can act as opportunistic pathogens, especially in immunocompromised individuals. The five most common species causing invasive infections are C. albicans (38%), C. glabrata (Nakaseomyces glabrata) (29%), C. parapsilosis (17%), C. tropicalis (10%), and C. krusei (Pichia kudriavzevii) (1%).1 A major concern with invasive Candida infections is candidemia, which carries significant morbidity and mortality, particularly in critically ill patients. In the United States, a 2020 report indicated that Candida accounted for up to 28% of central line–associated bloodstream infections in this population.1,2 In Thailand, candidemia-related mortality is notably high, ranging from 50.8% to 71.2%, exceeding rates reported in China, South Korea, and Europe.3–6
Despite its clinical significance, conventional diagnostic methods such as fungal cultures are often slow and insensitive, making timely diagnosis challenging.7 Therefore, empirical antifungal therapy is commonly used, guided by local epidemiological data, which can vary widely by region.8 The current guidelines for the treatment of Candida bloodstream infections from the Infectious Diseases Society of America (IDSA) 2016 and the global guideline for the diagnosis and management of candidiasis: an initiative of the European Confederation for Medical Mycology in cooperation with the International Society of Human and Animal Mycology and the American Society for Microbiology 20259,10 recommend echinocandins as the first-line therapy, due to the increasing resistance to fluconazole and its reduced efficacy against certain Candida species. Micafungin, an echinocandin, is commonly used, but current dosing recommendations are not adjusted for critically ill patients, potentially impacting treatment success.
Micafungin resistance in C. glabrata is an increasing concern in clinical practice. A national surveillance report from the United States, conducted between 2008 and 2014, documented a resistance rate of 4.8%.11 In Thailand, C. glabrata generally remains susceptible to micafungin; however, recent data from university hospitals indicate a gradual decline in susceptibility.3,12,13 Furthermore, C. auris has emerged as a significant fungal pathogen known for causing severe infections and exhibiting resistance to multiple antifungal agents. The Centers for Disease Control and Prevention (CDC) has highlighted the urgent threat posed by this organism. Despite global concern, reports of C. auris in Thailand are still relatively limited.10,13,14
Considering these developments, this study aimed to evaluate the in vitro activity of micafungin against various Candida species and to use these susceptibility data in Monte Carlo simulations. The goal was to determine the optimal micafungin dosing strategy based on pharmacokinetic/pharmacodynamic (PK/PD) targets in critically ill patients with candidemia.
Materials and Methods
Sample Collection
Candida isolates were obtained from the blood of hospitalized patients aged ≥20 years at Phramongkutklao Hospital, Thammasat University Hospital, and Udonthani Hospital, Thailand, between September 2023 and December 2024. Duplicate isolates from the same patient were excluded from the analysis.
Fungal Strains and Antifungal Susceptibility Testing
Species identification was conducted using matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS). Antifungal susceptibility of Candida isolates was assessed using the Sensititre YeastOne system, a broth microdilution–based method, following the manufacturer’s instructions (Thermo Fisher Scientific, Cleveland, OH, USA). Isolates were first grown on blood agar at 35°C in a non-CO₂ incubator for 24–25 h, after which the inoculum was standardized to a 0.5 McFarland turbidity. A 20-µL aliquot of the suspension was added to the broth, mixed, and further diluted with Sensititre YeastOne broth. The plates were prepared with serial twofold dilutions of antifungal agents, including micafungin, ranging from 0.008 to 8 µg/mL. Minimum inhibitory concentrations (MICs) were determined after 24 h of incubation, based on a color change from blue (no growth) to pink or purple (growth). Quality control was ensured using C. parapsilosis ATCC 22019 and C. krusei ATCC 6258, following the Clinical and Laboratory Standards Institute (CLSI) M27 guidelines.15 MICs were interpreted according to the breakpoints specified in CLSI M27M44S (3rd edition). For antifungals lacking defined breakpoints, epidemiological cutoff values (ECVs) from CLSI M57S (4th edition) were used.16,17
Monte Carlo Simulation
The present analysis utilized micafungin PK parameters obtained from a study by Zhong et al18 involving critically ill patients are summarized in Supplementary Table 1. A two-compartment model was applied to describe the PK behavior of micafungin in relation to time and concentration, with the PK/PD target being the 24-h area under the concentration–time curve to the MIC (AUC0-24/MIC). Although no specific PK/PD target has been universally established to define the safety of micafungin, its safety profile is well characterized and has been used at doses exceeding the standard recommended regimen. The model of the plasma concentration of micafungin, equations incorporating alanine aminotransferase (ALT) and the Sequential Organ Failure Assessment (SOFA) score as covariate factors were used.18 The target AUC0-24/MIC values indicating the efficacy of micafungin were >3000 for all Candida species, >5000 for Candida species excluding C. parapsilosis, and >285 for C. parapsilosis.19
Micafungin regimens were administered intravenously at a loading dose ranging from 100 to 400 mg, followed by 100–400 mg every 24 h. The highest dose used in this study was determined according to doses administered in earlier clinical trials involving patients. The PK/PD of the micafungin regimens was evaluated using a 10,000-subject Monte Carlo simulation (Oracle Crystal Ball Classroom Faculty Edition-Oracle 1-Click Crystal Ball 201, Thailand). The predicted likelihood that each dosage regimen would reach the established PK/PD index and target at each MIC was defined as the probability of target attainment (PTA). Furthermore, the cumulative fraction of response (CFR) for each regimen calculated by multiplying the proportion of Candida isolates at each MIC by the corresponding PTA. Dosage regimens were considered appropriate if the CFR and PTA were at least 90% in empirical and documented therapy, respectively.
Results
Candida Isolates the Distribution
Over the course of the investigation, 128 clinical isolates of Candida were identified. In our study, the five most frequently isolated Candida species included C. tropicalis (32%), C. albicans (22.7%), C. parapsilosis (16.4%), C. glabrata (12.5%), and C. auris (9.4%). Other Candida species accounted for 8.1% of the isolates, including C. orthopsilosis (3.1%), C. guilliermondii (Meyerozyma guilliermondii) (1.6%), C. lusitaniae (0.8%), C. dubliniensis (0.8%), and C. krusei (0.8%).
In vitro Susceptibility of Micafungin
All C. albicans isolates exhibited 100% susceptibility to micafungin, with MIC50 and MIC90 values of 0.008 and 0.015 µg/mL, respectively. Among the non-albicans Candida species, susceptibility to micafungin remained generally high; however, an increasing trend in MIC values was observed. C. tropicalis exhibited MIC50 and MIC90 values of 0.03 and 0.06 µg/mL, respectively. For C. parapsilosis, the MIC50 and MIC90 values were 1 and 2 µg/mL, respectively; the MIC90 corresponds to the upper limit of the susceptibility breakpoint. C. glabrata exhibited MIC50 and MIC90 values of 0.015 and 0.03 µg/mL, respectively; however, an isolate with an MIC exceeding 8 µg/mL was also detected. Furthermore, C. auris exhibited relatively high MIC values, with MIC50 and MIC90 values at 0.12 and 0.25 µg/mL, respectively. Table 1 presents the MIC distribution, as well as the MIC50 and MIC90 values of micafungin for each Candida species. Additional susceptibility data for caspofungin and anidulafungin are presented in Supplementary Table 2.
 |
Table 1 MIC Distribution of Micafungin Against Candida Species Isolates |
Monte Carlo Dose Simulation
In critically ill patients with normal ALT levels (<40 U/L), micafungin therapy at a standard dose of 100 mg/day was sufficient to cover Candida isolates with MICs up to 0.015 µg/mL. For critically ill patients with ALT levels ≥40 U/L, the same regimen provided adequate coverage for isolates with MICs up to 0.03 µg/mL. Isolates with MICs as high as 0.25 µg/mL required increased micafungin doses to achieve PK/PD targets, defined as a PTA of ≥90%. PTA values for different micafungin dosing regimens against Candida species are summarized in Supplementary Table 3.
If the Candida species has been identified, critically ill patients receiving the standard micafungin dose with ALT levels <40 U/L, regardless of SOFA score, achieved the CFR target only for C. albicans. In contrast, patients with ALT ≥40 U/L, regardless of SOFA score, attained the CFR target for C. albicans and C. glabrata, but not for C. tropicalis or C. auris. Notably, in patients with SOFA scores ≥10 and ALT levels >120 U/L, the standard micafungin dose achieved the CFR target for C. albicans, C. glabrata, and C. tropicalis. However, achieving the CFR target for C. auris requires a higher dose (up to 400 mg/day). The results demonstrated that the CFR target was attained only when high-dose micafungin and elevated ALT levels were present. Simulated PK/PD target attainment differed across Candida species and depended on the micafungin dosing regimen, as presented in Table 2.
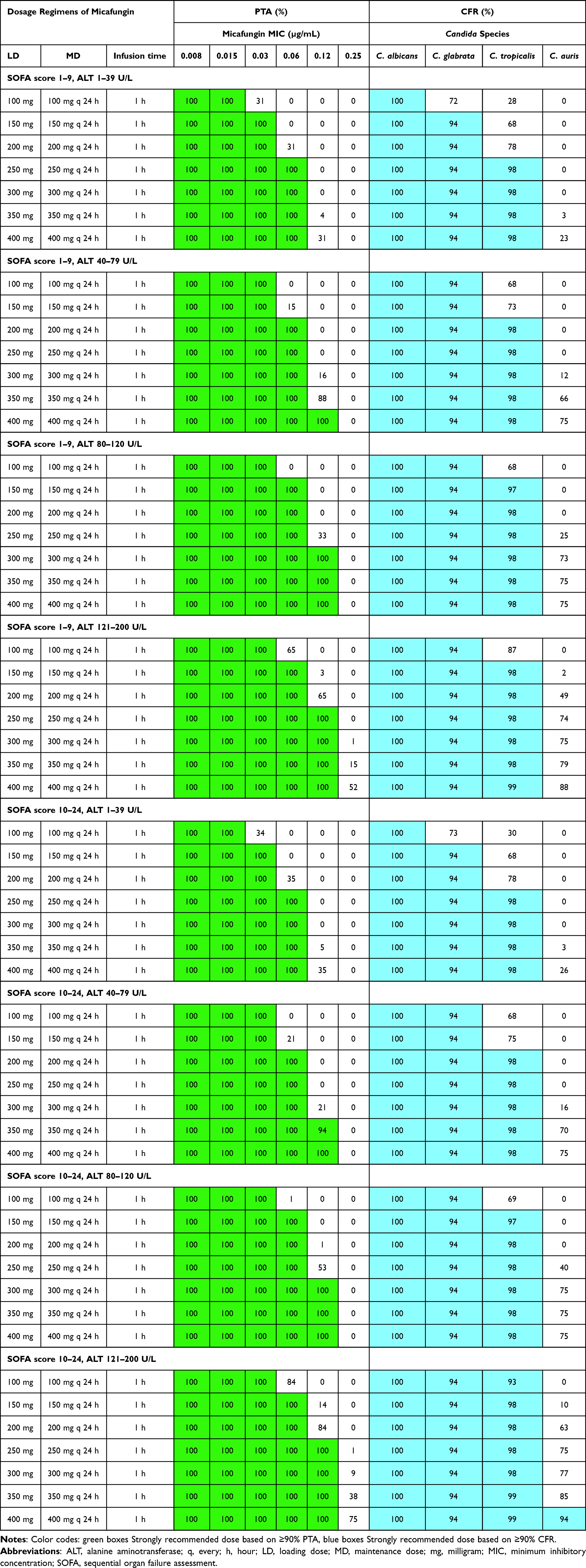 |
Table 2 PTA and CFR of Various Micafungin Dosage Regimens Was Evaluated in Critically Ill Patients at Steady State, Stratified by Sequential Organ Failure Assessment (SOFA) Score and Alanine Aminotransferase (ALT), Using a PK/PD Target of AUC0–24/MIC > 5000 Against Candida Species Not Included C. parapsilosis |
In cases involving C. parapsilosis with unknown MIC values, high-dose micafungin therapy was associated with a CFR exceeding 90% among critically ill patients presenting with elevated SOFA scores and ALT levels. In contrast, the standard-dose regimen failed to achieve the CFR target in patients with normal ALT levels. A daily dose of 400 mg was necessary to reach CFR values of 92.14% and 93.27% in patients with SOFA scores <10 and ≥10, respectively. When the MIC was known, a standard dose of micafungin was sufficient to achieve PTA when the MIC was ≤0.25 µg/mL, regardless of the SOFA score or ALT level. In patients with ALT levels ≥40 U/L, micafungin doses of at least 200 mg/day were effective in achieving PTA against C. parapsilosis isolates with MICs up to 1 µg/mL. Notably, the MICs of C. parapsilosis isolates in this study ranged from 0.5 to 2 µg/mL. Moreover, a 400-mg/day regimen achieved CFR targets even for isolates with MICs as high as 4 µg/mL. Comprehensive results for each dosing regimen against C. parapsilosis are presented in Supplementary Table 4.
Discussion
In this study, C. tropicalis was the most isolated species (32%), followed by C. albicans (22.7%), C. parapsilosis (16.4%), and C. glabrata (12.5%). Notably, C. auris was also detected, accounting for 9.4% of the isolates. Other Candida species accounted for 8.1% of the isolates, including C. orthopsilosis (3.1%), C. guilliermondii (1.6%), C. lusitaniae (0.8%), C. dubliniensis (0.8%), and C. krusei (0.8%). Between 2009 and 2017, the distribution of Candida species in the United States was dominated by C. albicans (48%), followed by C. glabrata (24%), C. parapsilosis (11%), and C. tropicalis (6%). The analysis of Candida isolates revealed that 57% were obtained from patients diagnosed with candidemia.20 In the Asia-Pacific region, a 2022 study conducted in China reported the distribution of Candida species across all clinical specimens. Only 6.1% of these isolates were derived from blood. The predominant species were C. albicans (49.4%), C. tropicalis (21.9%), C. parapsilosis (13.9%), and C. glabrata (11.4%). In contrast, C. auris accounted for a mere 0.2% of all clinical isolates and was absent from bloodstream infection isolates.21 In Japan, the distribution of Candida species isolated from blood between 2010 and 2019 was as follows: C. albicans, 43.6%; C. glabrata, 19.5%; C. parapsilosis, 18.8%; and C. tropicalis, 6.7%. Notably, no C. auris isolates were identified.22 Based on blood culture data from separate single-center studies conducted at different hospitals across Thailand, C. albicans (53%) was the most common Candida species from 2012 to 2013, followed by C. tropicalis (27.3%) and C. glabrata (15.2%).12 Between 2013 and 2016, C. tropicalis became predominant (36.9%), followed by C. albicans (29.2%), C. glabrata (17.7%), and C. parapsilosis (6.9%).13 During the 2016–2017 period, the predominant Candida species were C. tropicalis (49.4%), followed by C. albicans (28.8%), C. glabrata (16.7%), and C. parapsilosis (5.1%).13 In the subsequent study period (2018–2019), C. tropicalis remained the most frequently isolated species (33%), followed closely by C. albicans (29.6%).23 The distribution of Candida species in Thailand has shifted over time, with a marked increase in non-albicans Candida species. This trend is clearly reflected in our study, where non-albicans Candida species accounted for as much as 77.3% of all isolates, whereas C. albicans was identified in only 22.7%. Although our results differ from those of previous research in this area, our study collected clinical Candida isolates from blood from multiple tertiary hospital centers. This study provides a comprehensive overview of Candida species distribution in Thailand and highlights the current epidemiological landscape.
C. auris is an emerging fungal pathogen of major clinical concern due to its capacity to cause severe infections that are often resistant to multiple classes of antifungal drugs. This study presents the first report of the highest prevalence of C. auris in Thailand. Historically, C. auris was rarely detected in global surveillance, with only six cases of bloodstream infection reported across 135 medical centers in 39 countries from 2009 to 2016.24 Recent data reveal a notable epidemiological shift: by 2023, the United States reported 4514 new C. auris cases, prompting the CDC to classify it as an urgent public health threat due to multidrug resistance. In this study, micafungin MICs for C. auris isolates ranged from 0.12 to 0.25 µg/mL, with 0.5 µg/mL representing the established ECV.17 The proximity of MIC values to the ECV indicates a potential trend toward reduced susceptibility, which is significant compared to United States data showing that fewer than 2% of C. auris isolates exhibit resistance to echinocandin-class antifungals.14 These findings highlight the importance of ongoing surveillance and the need for adaptable antifungal treatment strategies, especially in areas where multidrug-resistant strains are emerging.
Therefore, this study also evaluated the susceptibility of Candida isolates to micafungin to support clinical decision-making and monitor emerging resistance trends. Notably, susceptibility testing in this study used a standardized MIC method, recognized for its accuracy and reliability in clinical practice. Micafungin was chosen as the primary antifungal due to its wider availability in resource-limited settings like Thailand, where it is listed on the National List of Essential Medicines. Conversely, caspofungin is unavailable in Thailand, and anidulafungin is rarely used because of its high cost and exclusion from the essential medicines list. Although these agents were not included in the main analysis, their MIC data are provided in Supplementary Table 2 to support reference and future investigations. Previous research conducted between 2012 and 2013 reported that micafungin had a 90% susceptibility rate against C. glabrata, with MIC values of 0.015–0.25 µg/mL.12 Further research from 2013 to 2016 demonstrated that C. albicans (MIC range: 0.008–0.015 µg/mL), C. tropicalis (MIC range: 0.015–0.06 µg/mL), and C. glabrata (MIC range: 0.008–0.015 µg/mL) all exhibited 100% susceptibility to micafungin.25 The findings revealed that C. glabrata isolates from bloodstream infections were resistant to echinocandins, which are currently recommended as the first-line therapy for candidemia, particularly in critically ill patients. In particular, one sixteenth of C. glabrata isolates exhibited resistance to micafungin (MIC range from 0.015 to >8 µg/mL). Because MIC values were progressively higher, pan-resistant strains were also detected, raising serious concerns regarding the efficacy of current antifungal treatments. Compared with other reports, the resistance rate of C. glabrata to micafungin was previously reported as 0.4%, 0.6%, 0%, and 2.8% in the Asia-Pacific region, Europe, Latin America, and North America, respectively, between 2006 and 2016.24
In this study, C. parapsilosis remained susceptible to echinocandins, though MIC values showed an upward trend compared to earlier reports. Specifically, micafungin MICs for C. parapsilosis ranged from 0.5 to 2 µg/mL, with MIC50 and MIC90 values of 1 and 2 µg/mL, respectively both higher than previously documented.12,23 Notably, some micafungin dosing regimens did not achieve the established PK/PD target. In contrast, C. albicans remained uniformly susceptible to echinocandins, with micafungin MICs ranging from 0.008 to 0.015 µg/mL, an MIC50 of 0.008 µg/mL, and an MIC90 of 0.015 µg/mL (susceptibility breakpoint: ≤0.25 µg/mL).16 All regimens of micafungin successfully met the CFR target for C. albicans.
Based on Monte Carlo simulations using population PK parameters from Zhong et al,18 high-dose micafungin regimens tailored to specific Candida species were essential to achieve PTA and CFR targets. The relatively high simulated doses in this study likely reflect reliance on PK/PD targets from prior literature, which do not fully account for all relevant pathogens, notably C. auris. Future research establishing species-specific PK/PD targets would enable more precise and clinically relevant dose optimization. Safety concerns are limited, as multiple real-world studies have demonstrated that high-dose micafungin is well tolerated. Repeated dosing up to 8 mg/kg/day (maximum 896 mg/day) for 1–4 weeks showed no dose-limiting toxicities in adults.26 Similarly, doses exceeding 200 mg/day (median 300 mg; IQR 275–400) for at least three consecutive days were well tolerated, with no severe hepatic or hematologic adverse events observed.27 Clinical evidence also suggests that higher-than-standard doses can shorten treatment duration and improve success rates compared with standard regimens.28 Despite this, careful monitoring for adverse reactions remains essential. The high simulated doses also highlight the potential benefit of exploring combination therapy with other antifungals for synergistic effects and underscore the importance of defining species-specific targets, which could guide more effective and personalized treatment strategies in future studies.
Our study suggests that a standard daily dose of micafungin (100 mg/day) is appropriate for Candida species, excluding C. parapsilosis, when the MIC is ≤0.015 µg/mL, regardless of SOFA score or ALT level. A minimum micafungin dose of 200 mg/day is required to achieve the PTA target at an MIC of 0.06 µg/mL in patients with SOFA scores ≥10 and ALT levels ≥40 U/L. For C. parapsilosis, the standard micafungin dose is sufficient to achieve the PTA target when the MIC is up to 0.25 µg/mL, regardless of the SOFA score or ALT level. However, in patients with ALT ≥40 U/L, target attainment can be achieved for isolates with MICs up to 0.5 µg/mL. Micafungin clearance in adult ICU patients was 30–51% higher than that in non-ICU adult patients. The AUC0-24 at steady state was 96.8 mg·h/L (72.0–132.3 mg·h/L) in ICU patients with SOFA scores ≥10 and 89.7 mg·h/L (70.7–131.7 mg·h/L) in those with SOFA scores <10. In contrast, non-ICU adult patients had a higher AUC0-24 of 125.6 mg·h/L (95.3–149.4 mg·h/L). A dose adjustment may be necessary when treating infections caused by resistant Candida strains. Although previous studies have recommended 250-mg/day micafungin for treating C. glabrata-associated infections,29 our findings demonstrated that a dose of 150 mg/day may be sufficient to achieve the CFR target in certain scenarios. However, even with simulated doses as high as 400 mg/day, effective coverage was only achievable for isolates with MICs ≤0.12 µg/mL. Notably, our study also identified isolates with MICs exceeding 8 µg/mL for which alternative antifungal agents outside the echinocandin class should be considered.
This study has several limitations that should be acknowledged. First, the dosing regimens used in our simulations were optimized to achieve established PK/PD targets; however, they have not yet been validated in real-world clinical settings. Second, this study did not collect isolates for investigating gene mutations. Finally, one limitation of this simulation study was the lack of measured PK data from the study participants. However, the population PK model of micafungin adequately describes the variability in PK parameters among critically ill patients.
Conclusion
Micafungin is one of the first-line treatment in critically ill patients with Candida bloodstream infections. Optimizing treatment outcomes requires appropriate dosing that takes local MIC values into account. C. auris should be acknowledged as an emerging and clinically significant pathogen in Thailand. Although administering doses higher than standard recommendations may enhance the likelihood of achieving PK/PD targets, particularly in cases of C. auris septicemia accompanied by high SOFA scores and elevated ALT levels, the safety of such regimens must be thoroughly assessed. Future studies evaluating clinical outcomes are necessary to determine the most effective micafungin dosing strategies for candidemia management.
Ethics Approval
Informed consent was obtained from all participants before their enrollment in the study. The study protocol was approved by the institutional ethics committee, including the Institutional Review Board of the Royal Thai Army Medical Department at Phramongkutklao College of Medicine and Phramongkutklao Hospital (approval number Q013h/66_Exp), the Research and Ethics Committee of Thammasat University Hospital (approval number 021/2566), and the Ethics Committee of Udonthani Hospital (approval number IRBRTA 1343/2566). The study was conducted in accordance with the Declaration of Helsinki, the Belmont Report, the CIOMS guidelines, and the International Conference on Harmonisation Good Clinical Practice (ICH-GCP) standards.
Acknowledgments
We thank the Microbiology Laboratory Unit of Phramongkutklao Hospital, Thammasat University Hospital, and Udonthani Hospital for providing the Candida isolates and standard antimicrobial susceptibility tests.
Funding
This research project was supported by the Kasem Pungsriwong Foundation. The funder did not participate in the study design, data collection and analysis, publication decisions, or manuscript preparation.
Disclosure
The authors declare that they have no personal relationships or financial interests that could have influenced the work presented in this publication.
References
1. Lockhart SR, Iqbal N, Cleveland AA, et al. Species identification and antifungal susceptibility testing of Candida bloodstream isolates from population-based surveillance studies in two U.S. cities from 2008 to 2011. J Clin Microbiol. 2012;50(11):3435–3442. doi:10.1128/JCM.01283-12
2. Weiner-Lastinger LM, Haass K, Gross C, et al. Pathogens attributed to central-line–associated bloodstream infections in US acute-care hospitals during the first year of the coronavirus disease 2019 (COVID-19) pandemic. Infect Control Hosp Epidemiol. 2023;44(4):651–654. doi:10.1017/ice.2022.16
3. Naranong C, Anunnatsiri S, Srigulbutr S. Epidemiology and antifungal susceptibility in patients with candidemia in a university hospital, Thailand. J Med Assoc Thai. 2020;103:1048–1056.
4. Tritipwanit K, Chindamporn A, Suankratay C. Epidemiology of candidemia at King Chulalongkorn Memorial Hospital, Thailand. J Infect Dis Antimicrob Agents. 2005;22:59–69.
5. Boonyasiri A, Jearanaisilavong J, Assanasen S. Candidemia in Siriraj Hospital: epidemiology and factors associated with mortality. J Med Assoc Thai. 2013;96 Suppl 2:S91–7.
6. Santimaleeworagun W, Saelim W, Wacharasint P, et al. Clinical outcomes by treatment type and factors associated with mortality among patients with candidemia at a Thai university hospital. Southeast Asian J Trop Med Public Health. 2020;51(5):719–728.
7. Chindamporn A, Chakrabarti A, Li R, et al. Survey of laboratory practices for diagnosis of fungal infection in seven Asian countries: an Asia Fungal Working Group (AFWG) initiative. Med Mycol. 2017;56(4):416–425. doi:10.1093/mmy/myx066
8. Perlin DS, Rautemaa-Richardson R, Alastruey-Izquierdo A. The global problem of antifungal resistance: prevalence, mechanisms, and management. Lancet Infect Dis. 2017;17(12):e383–e92. doi:10.1016/S1473-3099(17)30316-X
9. Pappas PG, Kauffman CA, Andes DR, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America. Clin Infect Dis. 2016;62(4):e1–50. doi:10.1093/cid/civ933
10. Cornely OA, Sprute R, Bassetti M, et al. Global guideline for the diagnosis and management of candidiasis: an initiative of the ECMM in cooperation with ISHAM and ASM. Lancet Infect Dis. 2025;25(5):e280–e293. doi:10.1016/S1473-3099(24)00749-7
11. Vallabhaneni S, Cleveland AA, Farley MM, et al. Epidemiology and risk factors for echinocandin nonsusceptible Candida glabrata bloodstream infections: data from a large multisite population-based candidemia surveillance program, 2008-2014. Open Forum Infect Dis. 2015;2(4):ofv163. doi:10.1093/ofid/ofv163
12. Thunyaharn S, Santimaleeworagun W, Khoprasert C, Kesakomol P, Theeraapisakkun M, Visawapoka U. Activity of triazoles and echinocandins against Candida bloodstream isolates at Phramongkutklao Hospital, Thailand. J Southeast Asian Med Res. 2021;5(2):84–90. doi:10.55374/jseamed.v5i2.96
13. Ngamchokwathana C, Chongtrakool P, Waesamaae A, Chayakulkeeree M. Risk factors and outcomes of non-albicans Candida bloodstream infection in patients with candidemia at Siriraj Hospital-Thailand’s largest national tertiary referral hospital. J Fungi. 2021;7(4):269. doi:10.3390/jof7040269
14. CDC. Candida auris [Internet]. Atlanta, GA: CDC; 2024 [updated 2024 Apr 24; cited 2025 May 29]. Available from: https://www.cdc.gov/candida-auris/index.html.
15. CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; CLSI Document M27-A4.
16. CLSI. Performance Standards for Antifungal Susceptibility Testing of Yeasts M27M44S.
17. CLSI. Epidemiological Cutoff Values for Antifungal Susceptibility Testing M57S.
18. Zhong S, Zhu X, Zhao L, et al. Optimization of micafungin dosage for Chinese patients with sepsis in the intensive care unit based on a population pharmacokinetic-pharmacodynamic analysis. Pharm Res. 2021;38(1):67–77. doi:10.1007/s11095-020-02980-z
19. Andes D, Ambrose PG, Hammel JP, et al. Use of pharmacokinetic-pharmacodynamic analyses to optimize therapy with the systemic antifungal micafungin for invasive candidiasis or candidemia. Antimicrob Agents Chemother. 2011;55(5):2113–2121. doi:10.1128/AAC.01430-10
20. Ricotta EE, Lai YL, Babiker A, et al. Invasive candidiasis species distribution and trends, United States, 2009–2017. J Infect Dis. 2021;223(7):1295–1302. doi:10.1093/infdis/jiaa502
21. Bilal H, Muhammad S, Bing H, et al. Distribution and antifungal susceptibility pattern of Candida species from mainland China: a systematic analysis. Virulence. 2022;13(1):1573–1589. doi:10.1080/21505594.2022.2123325
22. Kajihara T, Yahara K, Nagi M, et al. Distribution, trends, and antifungal susceptibility of Candida species causing candidemia in Japan, 2010-2019: a retrospective observational study based on national surveillance data. Med Mycol. 2022;60(9):myac071. doi:10.1093/mmy/myac071
23. Boonsilp S, Homkaew A, Phumisantiphong U, Nutalai D, Wongsuk T. Species distribution, antifungal susceptibility, and molecular epidemiology of Candida species causing candidemia in a tertiary care hospital in Bangkok, Thailand. J Fungi. 2021;7(7):577. doi:10.3390/jof7070577
24. Pfaller MA, Diekema DJ, Turnidge JD, Castanheira M, Jones RN. Twenty years of the SENTRY antifungal surveillance program: results for Candida species from 1997-2016. Open Forum Infect Dis. 2019;6(Suppl 1):S79–94. doi:10.1093/ofid/ofy358
25. Khumdee P, Hematulin P, Yansombat J, et al. Species characterization and antifungal susceptibility profile of yeast isolates from blood cultures of fungemic patients in Thammasat University Hospital, Thailand. J Assoc Med Sci. 2022;55(1):44–50.
26. Prentice HG, Potter M, Koblinger S. A study to determine the safety profile and maximum tolerated dose of micafungin (FK463) in patients undergoing haematopoietic stem cell transplantation. Bone Marrow Transplant. 2006;38(1):47–51. doi:10.1038/sj.bmt.1705398
27. Grant VC, Nguyen K, Rodriguez S, Zhou AY, Abdul-Mutakabbir JC, Tan KK. Characterizing safety and clinical outcomes associated with high-dose micafungin utilization in patients with proven invasive candidiasis. Trop Med Infect Dis. 2022;7(2):23. doi:10.3390/tropicalmed7020023
28. Nagamizu M, Hotta Y, Noda M, et al. Association of doses based on body constitutional parameters with the efficacy of micafungin in candidemia. J Infect Chemother. 2025;31(4):102654. doi:10.1016/j.jiac.2025.102654
29. Li X, Liu X, Mao J, Liu D, Jiao Z. Evaluation of population pharmacokinetic models of micafungin: implications for dosing regimen optimization in critically ill patients. Pharmaceutics. 2024;16(9):1145. doi:10.3390/pharmaceutics16091145
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.