Back to Journals » Journal of Blood Medicine » Volume 14
Optimizing Haemophilia Care in Resource-Limited Countries: Current Challenges and Future Prospects
Authors Ndoumba-Mintya A, Diallo YL, Tayou TC, Mbanya DN ![]()
Received 15 October 2022
Accepted for publication 1 February 2023
Published 20 February 2023 Volume 2023:14 Pages 141—146
DOI https://doi.org/10.2147/JBM.S291536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Annick Ndoumba-Mintya,1 Yacouba L Diallo,2 Tagny C Tayou,1 Dora N Mbanya1
1Hematology & Transfusion Service, Yaoundé University Teaching Hospital, Yaoundé, Cameroon; 2Service de Médecine - CHU Hôpital du Mali, Bamako, Mali
Correspondence: Dora N Mbanya, Centre Hospitalier et Universitaire, B.P. 8046, Yaoundé, Cameroon, Tel +237 677607037, Email [email protected]
Abstract: About 75% of persons with hemophilia live in the developing world and do not have access to routine care due to many barriers. There are a lot of challenges associated with hemophilia care in resource-limited settings, ranging from financial to organisational and government commitments. This review discusses some of these challenges and future prospects, while highlighting the important role of the World Federation of Hemophilia in hemophilia patient care. A participative approach involving all stakeholders is key to optimizing care in resource-limited settings.
Keywords: hemophilia care, people living with hemophilia, challenges, prospects
Introduction
Hemophilia is a rare bleeding disorder characterized by deficiency in clotting factors eight (VIII) for Hemophilia A and nine (IX) for Hemophilia B. Hemophilia A is predominant, and constitutes about 80–85% cases.1 According to the World Federation of Hemophilia (WFH), there are an estimated 815,100 cases of hemophilia worldwide, of which only 347,026 are diagnosed, and with 276,900 cases being severe hemophilia.2 Thus, it is generally underdiagnosed, especially in developing countries, where resources available for diagnosis and care are very restricted.
In developed countries, there is availability and accessibility of clotting factor concentrates (CFC), so much so that access to prophylaxis has been provided for over the last three decades. However, in developing countries, until recently, the only form of advanced care in persons living with hemophilia (PLWH) was the on-demand use of these CFCs when available. With other competing priorities such as malaria, malnutrition, and other infectious diseases, the tendency is not to focus much on chronic non-communicable diseases, especially in Sub-Saharan Africa. Thus, hemophilia care in these settings tends to be suboptimal. According to the World Federation of Hemophilia, 75% of persons with hemophilia live in developing countries,3 but have little access to routine care due to many challenges and barriers.
Evidence suggests that the incidence of hemophilia is constant in different populations; nevertheless, only about 2% of those requiring it actually use clotting factor concentrates for treatment in Africa.4 There is a huge disparity in capacities for prompt and accurate diagnosis and for the provision of the necessary care for survival in these settings. In Africa, only 11.4% of expected hemophilia cases are identified, with less than 0.1 IU/capita utilisation of clotting factor concentrates. This review touches on the general issues and challenges related to hemophilia care, and discusses perspectives for optimising care.
Care for People Living with Hemophilia (PLWH)
Diagnosis
Care for PLWH begins with appropriate diagnosis. There is a huge difference in hemophilia diagnosis and care between the developed world and resource-limited settings, whereas in Europe and the Americas, 81% and 54% cases, respectively, are diagnosed, only 8% are diagnosed in Africa, and 15% in South-East Asia.5 And even within Africa, there is a lot of disparity and care of PLWH. In countries including South Africa, Algeria and Egypt, more patients are diagnosed in comparison to countries of sub-Saharan Africa.5,6 Early diagnosis is the norm in developed countries.7 Clinically, a bleeding disorder is suspected in the face of recurrent hemorrhage, but it must be confirmed through laboratory screening tests.
The collaboration and support from the WFH has resulted in marked increase in the diagnosis of cases of PLWH, within their various communities. For example, in Cameroon, with an estimated prevalence of 2500 PLWH, only 225 (9%) have been diagnosed and followed up in the Hemophilia Treatment Center (HTC), a marked improvement on the 9 cases in 1972; the 65 cases in 2003; 166 cases in 2019 and 180 in 2021. Of the 225 cases, 185 (82.2%) are hemophilia A, 30 are Haemophilia B (13.3%) and the 10 others are FVII deficiencies (2 cases), and Von Willebrand Factor deficiencies (8 cases). There are 125 cases of severe hemophilia (55.5%) recorded.
In Mali, there are currently 220 diagnosed and registered patients in the Hemophilia Treatment Center (HTC), of which 150 are hemophilia A (68.2%); 17 are hemophilia B (7.7%), and 29 are simply suspected cases. The remaining 24 cases are constituted of Willebrand disease, and other rare bleeding disorders (10.9%). On the whole, there is significant evolution, given that only in recent years all samples from Mali were exported to foreign Centers for diagnosis. Today, both screening for hemophilia and inhibitors is carried out there. Nevertheless, the diagnosis of von Willebrand’s Disease remains challenging for most countries in resource-limited settings.
Management
Once diagnosed, clinical care and follow-up is indispensable. The WFH recommends that care in PLWH be multidisciplinary requiring hematologists, paediatricians, dentists, physiotherapists, rheumatologists, radiologists, nurse coordinators, psychologists, and more.8,9 Needless to emphasize that there must be harmony between these team members, the HTC, the patients and their families, as well as a functioning laboratory for clotting factor assays and screening for inhibitors. In addition, proper records/registry should be kept on patient management for proper follow-up. Continuous patient and family education also contributes significantly to proper care for PLWH.9
Although blood and labile blood products are still a scarce commodity, transfusion therapy has been the mainstay of treatment since the 1940s, with mainly whole blood used. Plasma was used by the 1950s and cryoprecipitate by the mid 1960s. In the late 1960s, scientists and manufacturers developed methods for separating factor VIII and factor IX from pooled human plasma. Freeze-dried (lyophilized) factor VIII or factor IX concentrates were prepared in bottles and widely used in the developed world. However, in the 1980s, human blood, plasma, and plasma-derived products were discovered to be transmitting deadly blood-borne viruses (HIV, HBV, HCV) so much so that many PLWH were infected by these agents, and most died of AIDS or end-stage liver disease.
In 1984, the successful cloning of the factor VIII gene was a major breakthrough that led to the production of recombinant human factor VIII (r FVIII). Clinical trials were ongoing by 1987 and by 1992 two pharmaceutical companies had licensed rFVIII products for use in hemophilia A. Five years later, in 1997, rFIX (BeneFIX) became available for people living with hemophilia B.
In recent years treatment options have improved to include the treatment of inhibitors to FVIII or FIX as well as prophylaxis. Nevertheless, transfusion of blood and blood components remain the mainstay of managing bleeding patients in most resource-limited settings. For example, in Mali, before 2012, the treatment of bleeding events was only with fresh frozen plasma transfusions (Yacouba Diallo, personal communication). Yet blood safety challenges remain multifactorial in these settings.10 Hence, complications related to blood transfusion remain real in these settings. The transmission of infections by transfusion (TTIs) is a pending threat because of the high prevalence of HIV, hepatitis B and C viruses, syphilis and malaria in these populations, and the lack of resources for their appropriate screening. More recent technologies for reducing the transmission of these pathogens through blood transfusion, such as pathogen reduction/inactivation techniques are costly and remain inaccessible to most of these countries.
Thus, the evolution in care for PLWH in the developing world has gone from the use of large quantities of whole blood, which in itself is a scarce commodity, to the use of fresh frozen plasma, not readily available, to that of cryoprecipitate, also not usually available. The latest WHO report on blood availability, safety and quality in the African Region,11 indicates that only a few countries of the AFRO Region are actively involved with component preparations. Only 7 countries reported using apheresis, while red cell concentrates use was reported by 73.9%; platelet concentrates by 9.5%, and cryoprecipitate by 0.6%.11
The Twinning programs organized by the WFH between experienced Hemophilia Treatment Centers and emerging ones have been very successful. This program allows for exchange of experiences between the two centers and capacity building in favor of the emerging centers and has also contributed significantly in promoting care in resource-limited settings. Currently, with the collaboration of World Federation of Hemophilia’s Humanitarian Aid Program, there is increased access to factor VIII and IX concentrates, and marked improvement in care for PLWH. Access to other novel therapies has revolutionized hemophilia care.12 For example, the use of Emicizumab, a humanized bispecific monoclonal antibody that bridges activated FIXa and FX to restore the function of missing FVIIIa, has become accessible to selected patients in some low-income countries, through the WFH Humanitarian Aid Program Several beneficiaries have had remarkable improvement in their quality of life with reduced annualized bleeding rates and decreased morbidity and mortality rates.
A review by Ghosh and Ghosh13 suggests that for care to be optimal the following should be taken into consideration: the number of persons living with hemophilia; minimum amount of concentrate required to keep a PLWH relatively free of bleeds; strategies for sustainable accessibility of clotting factors for PLWH, and ways to minimize and optimize their usage.
The organization of hemophilia care delivery in many African countries is at its early stages. Thus, there is still high morbidity and mortality due to hemophilia, with rampant occurrence of chronic complications and sequelae.
Challenges
Hemophilia care in resource-limited settings is plagued with various challenges that have also been reported by several authors. These include the lack of proper health care infrastructure (diagnostic laboratories and appropriate management centers), and lack of human resources trained for hemophilia care among others,6 And the challenges are similar in other countries like Nigeria.14 In most low-income settings, even establishing one HTC is a great achievement. In Cameroon for example, there is one in the capital city, and 2 satellite centers in two other cities. In 2017, their analysis of the Quality of Life (QoL) in PLWH in the HTC in Yaoundé, and despite not meeting the ideal international standards, Nzometia et al reported significant improvement in the QoL of those using the facility.15 Nevertheless, a few HTCs including that of Senegal in Dakar have both improved diagnosis, care and capacity building of care personnel.16 This HTC has evolved to become a training center on hemophilia care, and hosting several workshops and seminars.
The use of national registries for data collection (type of bleeding disorder; treatment and doses, complications etc.) and follow-up of PLWH, also contributes not only to enhance care, but serves as a good tool for advocacy. These exist in countries like Egypt.6 In other resource-limited settings, the tendency is to have a register only at the HTC. Today, the WFH has facilitated the creation of national registries in about fifty countries.
Other challenges include the fact that these settings have several competing health care priorities for the government including infectious disease, so that disorders like hemophilia get relegated to the background. Interestingly, the Senegalese government has prioritized hemophilia in its list of chronic diseases.6 Furthermore, there is lack of visibility of hemophilia patients in healthcare system including low awareness of the disorder within the medical profession, the population and the policy makers. The non-availability of clotting factor concentrates; their inadequate utilization when available, and challenges related to the development of inhibitors all hamper care for PLWH. Two studies in Cameroon reported the presence of inhibitors in PLWH on CFCs.17,18 The lack or complete absence of social security and medical insurances are all factors that further jeopardize hemophilia care in resource-limited settings.
Future Prospects
Developing a patient’s society (National Members Organisation) and a bleeding disorder registry are very important steps towards ensuring adequate treatment for PLWH in resource-limited settings, as is the case in developed countries. The World Federation of Haemophilia has been instrumental in promoting these in several countries. These patient associations collaborate with the WFH as associate members. They participate actively in sensitizing and mobilising their respective communities towards haemophilia care. The Haemophilia Association of Cameroon was created in 2003 with a handful of members. Today, they count about 216 members. In Mali, their association was created in 2012 and counts about 218 members. As part of a four-year training program supported by the Novo Nordisk Hemophilia Foundation, the Malian association contributes significantly in awareness activities, the organization of training sessions involving patients, their families, medias workers, opinion leaders, health authorities and health care providers including both modern and traditional practitioners, through all regions of Mali (Prof. Yacouba Diallo, personal communication). Furthermore, special training sessions for Laboratories technicians and biologists have been included in their activities.
Table 1 is a summary of strategies that may impact positively on haemophilia care in these settings. Government commitment should be sought, to enhance their allocation of budgets for hemophilia care. Strategies for promoting the use of safe plasma products through quality management systems and Good Manufacturing Procedures; it will avoid wastages and provide for needs. In Egypt, despite introducing hemophilia care since the late sixties, and despite heavy support from their government, they still face challenges with procurement of CFCs to be able to align with universal prophylaxis and home therapy (Mbanya et al, 2021). A good supply chain management is necessary for improved care.
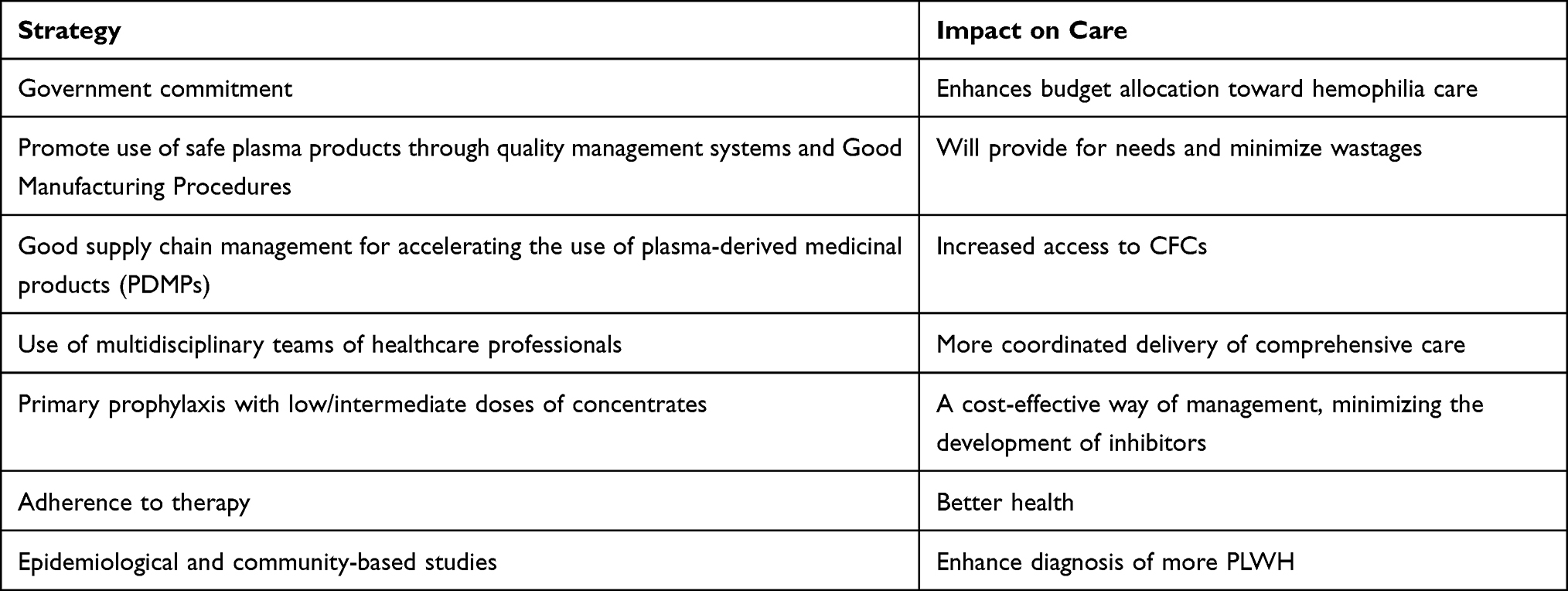 |
Table 1 Strategies for Improving Haemophilia Care in RLS |
Establishing a good supply chain management for accelerating the use of plasma-derived medicinal products (PDMPs) in resource-limited settings could increase access to CFCs. Indeed, it has been reported that 20 of 45 countries of the WHO-AFRO Region (43.5%) had included PDMPs on their national lists of Essential Medicines. These, if accessible, would be safer for use in these settings, than plasma and cryoprecipitate.
However, despite the great need for these products, there is a lot of plasma wastage in these settings. But it was equally obvious that several basic requirements are lacking for the local production of PDMPs, including insufficient plasma collections from healthy, voluntary non-remunerated, repeat, blood donors (most donors in these settings are family/replacement donors), and wastage of available plasma. The non-conformities with international guidelines and regulations for testing and issuing of plasma suitable for fractionation and the absence of well-regulated national blood services, are other issues. In a recent concept note by the World Health Organisation,19 the steps that can be taken to increase the production of quality and safe plasma from voluntary non-remunerated donors in low- and medium-income countries, useable in fractionation, were provided. This guideline is intended to provide a high-level overview and recommendations for actions that can be taken by policy-makers, national regulatory authorities, blood collection organizations, blood donors and their associations, clinicians and patients as a roadmap toward reducing wastage of plasma that could be fractionated to make the PDMPs and thus increase access to PDMPs in low- and middle-income countries.
The coordinated delivery of comprehensive care by multidisciplinary teams of healthcare professionals should be encouraged.
Primary prophylaxis with low/intermediate dose of the concentrates is a cost-effective way to manage PLWH and this also reduces inhibitor development. Strategies to encourage adherence to therapy will further enhance care in these settings. Promoting regular physiotherapy and dental care are aspects of care for PLWH to be fostered in resource-limited settings. Home therapy is another prospect to examine.
Epidemiological and community-based studies should be promoted, for improved diagnosis of PLWH, as well as the introduction of antenatal diagnostic centres.
Gene therapy is showing promising results, but there may be a number of barriers to access. The WFH has coordinated many initiatives, in partnership with private laboratories, to provide donations of Extended half-life CFC and Emicizumab to selected patients in resource-limited countries.20 However, it is very important for other stakeholders (governments, physicians, patient organisations), work together to facilitate further access to these products.
Conclusions
The care of PLWH is plagued with many challenges and while there are also many prospects towards tackling them, concerted efforts are indispensable between all stakeholders (policy-makers, national regulatory authorities, blood collection organizations, patient associations and the international community), for these to be overcome. Unfortunately, haemophilia and other non-communicable diseases may not be considered a healthcare priority (a national health problem), in comparison to malaria, HIV/AIDS and other infectious diseases in these our settings. Awareness campaigns and advocacy becomes indispensable.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stonebraker JS, Bolton-Maggs PH, Michael Soucie J, Walker I, Brooker M. A study of variations in the reported haemophilia B prevalence around the world. Haemophilia. 2012;18:91–94. doi:10.1111/j.1365-2516.2011.02588.x
2. World Federation of Hemophilia. Nigeria includes bleeding disorders in national policy and strategic plan. Available from: https://wfh.org/nigeria-includes-bleeding-disorders-in-national-policy-and-strategic-plan/.
3. World Federation of Hemophilia. Economic benefits of basic hemophilia management and care; 2004. Available from: http://www.wfh.org.
4. World Federation of Hemophilia. Report on the Annual Global Survey 2019. Montreal: WFH; 2020.
5. World Federation of Hemophilia. Report on the Annual Global Survey 2020. Montreal: World Federation of Hemophilia; 2021.
6. Mbanya DN, Diop S, Ndoumba Mintya AN, et al. Hemophilia care in Africa: status and challenges. Transfus Clin Biol. 2021;28:158–162. doi:10.1016/j.tracli.2021.01.008
7. Haute autorite de Sante. Protocole National de Diagnostic Et de Soins (PNDS) Hemophilie. France: Haute autorite de Sante; 2019.
8. Federation Mondiale de l’Hemophilie. Lignes directrices pour la prise en charge de l’hemophilie. Montreal: Federation Mondiale de l’Hemophilie; 2012.
9. Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of hemophilia. Haemophilia. 2020;00:1–158.
10. Tagny CT, Mbanya D, Tapko JB, Lefrère JJ. Blood safety in Sub-Saharan Africa: a multi-factorial problem. Transfusion. 2008;48:1256–1261. doi:10.1111/j.1537-2995.2008.01697.x
11. World Health Organisation. African Region Status Report on Blood Availability, Safety and Quality. Brazzaville: AFRO; 2022.
12. Weyand AC, Pipe SW. New therapies for hemophilia. Blood. 2019;133:389–398. doi:10.1182/blood-2018-08-872291
13. Ghosh K, Ghosh K. Overcoming the challenges of treating hemophilia in resource-limited nations: a focus on medication access and adherence. Expert Rev Hematol. 2021;14:721–730. doi:10.1080/17474086.2021.1957826
14. Okoye HC, Korubo KI, Nwogoh B, et al. Challenges in the management of bleeding disorders in Nigeria. Niger J Clin Pract. 2018;21:468–472. doi:10.4103/njcp.njcp_319_17
15. Nzometia CY, Tagny CT, Ndoumba AM, Balogog PN, Mbanya DN. Assessing the quality of care for haemophilia at the Yaoundé reference treatment Centre of Cameroon. Blood Coagul Fibrinolysis. 2017;28:176–180. doi:10.1097/MBC.0000000000000549
16. Diop S, Haffar A, Mahlangu J, Chami I, Kitchen S, Pierce G. Improving access to hemophilia care in sub-Saharan Africa by capacity building. Blood Adv. 2019;3:1–4. doi:10.1182/bloodadvances.2019GS121537
17. Balogog PN, Tagny CT, Ndoumba A, Mbanya D. FVIII and FIX inhibitors in people living with hemophilia in Cameroon, Africa: a preliminary study. Int Jnl Lab Hem. 2014;36:566–570. doi:10.1111/ijlh.12190
18. Chendjou A, Ndoumba A, Kalla C, Tayou C, Mbanya D. FVIII inhibitors during primary prophylaxis for hemophilia A: a pilot study in Cameroon. J Blood Transfusions Dis. 2020;3:126–129.
19. World Health Organisation. Guidance on Increasing Supplies of Plasma-Derived Medicinal Products in Low- and Middle-Income Countries Through Fractionation of Domestic Plasma. Geneva: World Health Organisation; 2021.
20. Pierce GF, Adediran M, Diop S, et al. Achieving access to haemophilia care in low-income and lower-middle-income countries: expanded humanitarian aid program of the world federation of hemophilia after 5 years. Lancet Haematol. 2022;9(9):e689–e697. PMID: 36055333. doi:10.1016/S2352-3026(22)00209-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.