Back to Journals » Clinical Interventions in Aging » Volume 21
Optimizing Early Recovery Quality in Same-Day Discharge Total Hip Arthroplasty: A Narrative Review
Authors Guo J, Li E, Zhao C, Xiao L, Xu P, Xu X
Received 9 March 2026
Accepted for publication 20 May 2026
Published 27 May 2026 Volume 2026:21 607990
DOI https://doi.org/10.2147/CIA.S607990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Junfei Guo,1,2 Erliang Li,1,2 Chengcheng Zhao,1,2 Lin Xiao,1 Peng Xu,1,2 Xin Xu1– 3
1Department of Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shannxi, People’s Republic of China; 2Key Laboratory of Pathogenesis and Precision Treatment of Arthritis, Xi’an, Shannxi, People’s Republic of China; 3Translational Medicine Centre, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shannxi, People’s Republic of China
Correspondence: Junfei Guo, Department of Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shannxi, People’s Republic of China, Email [email protected] Xin Xu, Department of Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shannxi, People’s Republic of China, Email [email protected]
Abstract: The paradigm of total hip arthroplasty (THA) is undergoing a transformative shift from prolonged inpatient care toward same-day discharge (SDD), driven by the convergence of enhanced recovery after surgery (ERAS) protocols, advances in anesthesia and analgesia, and evolving reimbursement policies. As global demand for THA continues to escalate amid population ageing, this model offers a compelling strategy to optimize healthcare resource utilization without compromising patient safety. However, the success of SDD-THA depends on a precise understanding of early postoperative recovery quality, which is a multidimensional construct encompassing pain control, functional restoration, hemodynamic stability, and patient-reported well-being. This review synthesizes contemporary evidence on early recovery trajectories and the multifactorial determinants that govern them. We analyze critical clinical strategies, including evidence-based patient selection, perioperative ERAS protocol implementation, anesthetic and multimodal analgesic optimization, blood management and complication prevention, early rehabilitation paradigms, and the influence of healthcare policy and economic frameworks on early recovery quality. By integrating these domains, we propose a patient-centered quality improvement pathway that prioritizes the velocity of functional independence as the definitive clinical endpoint. Focusing on these core perioperative optimizations ensures a sustainable, high-value SDD-THA practice.
Keywords: total Hip arthroplasty, same-day discharge, enhanced recovery after surgery, early recovery quality, perioperative optimization
Introduction
Total hip arthroplasty (THA) remains the definitive intervention for end-stage hip joint disease, providing reliable pain relief and functional restoration.1,2 The global volume of THA procedures is projected to increase dramatically over the coming decades. Population-based forecasting studies estimate that primary THA volume in the United States will rise by 284% by 2040 relative to 2014 levels, reaching approximately 1.43 million annual procedures.3 Similar growth trajectories are evident across Organisation for Economic Co-operation and Development (OECD) nationsand specifically within the Medicare population, where long-term projections suggest a multi-fold increase by 2060.4,5 These projections are attributable to the convergent forces of population ageing, rising obesity prevalence, expanding surgical indications, and continuous improvements in implant design and surgical technique.1,6 This anticipated demand poses unprecedented challenges to healthcare capacity and fiscal sustainability.5,7
Against this backdrop, the optimization of perioperative management pathways to maximize healthcare value has become an imperative. Same-day discharge (SDD) THA, in which patients undergo surgery and are discharged home on the day of the procedure, has emerged as a transformative care model that directly addressing growing systemic pressures on healthcare.8,9 This shift is catalyzed by mature enhanced recovery after surgery (ERAS) principles, which minimize surgical stress and accelerate function. Consequently, hospital length of stay (LOS) has been shortened to its logical extreme.10,11 In the United States, the removal of THA from the Centers for Medicare and Medicaid Services (CMS) inpatient-only list, combined with the COVID-19 pandemic’s pressure on hospital resources, propelled the proportion of SDD-THA from approximately 2% in 2016 to over 54% by 2020.9,12,13
However, the transition to SDD-THA requires more than just faster discharge. It demands a new way to define and manage recovery quality. We must distinguish “early recovery quality” from conventional ERAS metrics. Traditional metrics primarily focus on safety-net endpoints like complication and readmission rates. Administrative markers like LOS focus on when a patient leaves the hospital. In contrast, early recovery quality focuses on the internal physiological trajectory. It prioritizes the velocity of functional restoration and hemodynamic stability. It also accounts for the absence of distressing symptoms, such as postoperative nausea and vomiting (PONV) or orthostatic intolerance (OI). Ultimately, it emphasizes the subjective patient experience during the critical transition to the home environment.8,14 When early recovery quality is suboptimal, the consequences cascade involving failure to meet discharge criteria, unplanned hospital admission, emergency department visits, delayed rehabilitation, and increased dependence on family and community resources, negating the putative benefits of the SDD model.8,15
The imperative to understand early recovery quality also carries substantial public health and health-economic significance. Mobility impairment secondary to hip disease exerts profound long-term effects on older adults’ health trajectories, quality of life, and socioeconomic participation.16 Health-economic modeling demonstrates that even modest improvements in daily ambulatory function can yield meaningful reductions in functional limitation, total healthcare expenditure, and nursing home utilization over an 18-year horizon.16 If SDD-THA can facilitate a more rapid and predictable return to independent mobility through optimized early recovery, it holds the potential to amplify these long-term health-economic dividends. Conversely, premature discharge in the absence of adequate recovery quality may increase acute care utilization, impair long-term functional trajectories, and paradoxically inflate overall healthcare costs.8
Despite the rapid migration toward SDD-THA, current literature remains fragmented, often focusing on isolated safety metrics or administrative discharge timing. A significant knowledge gap exists regarding how to systematically integrate multifactorial determinants into a cohesive recovery trajectory. This review addresses this gap by synthesizing contemporary evidence to propose an integrated, patient-centered quality improvement framework focused on optimal recovery as the definitive endpoint (Figure 1). The ultimate objective is to inform clinical practice, guide future research, and support the sustainable, high-quality expansion of SDD-THA in the context of an ageing global population
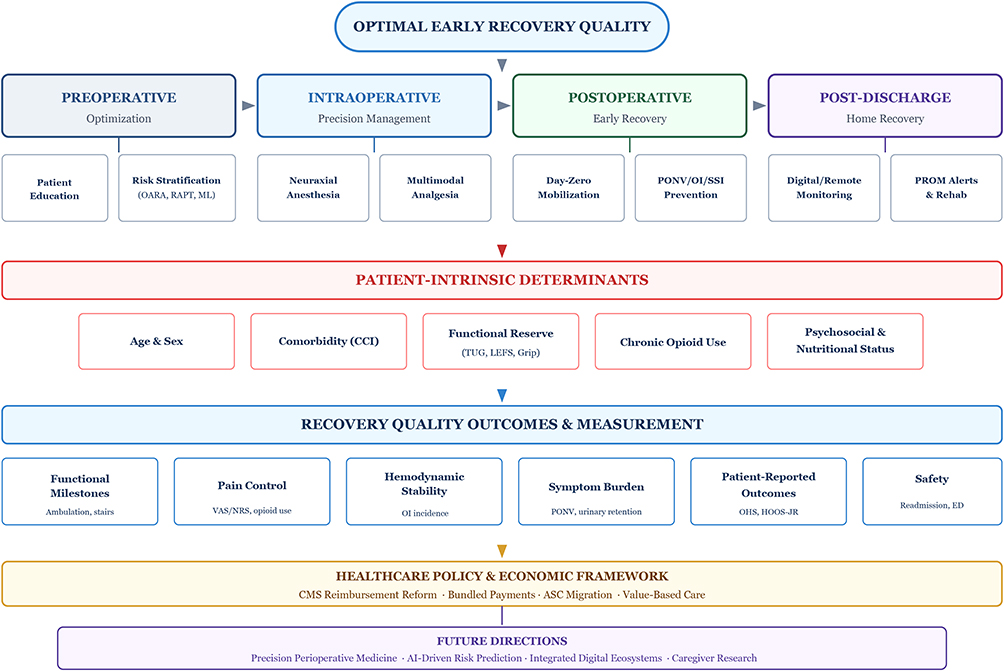 |
Figure 1 Integrated Conceptual Framework for Early Recovery Quality Optimization in SDD-THA. Abbreviations: SDD, same-day discharge; THA, total hip arthroplasty; OARA, Outpatient Arthroplasty Risk Assessment; RAPT, Risk Assessment and Prediction Tool; ML, machine learning; PONV, postoperative nausea and vomiting; OI, orthostatic intolerance; SSI, surgical site infection; PROM, patient-reported outcome measure; CCI, Charlson Comorbidity Index; TUG, Timed Up and Go; LEFS, Lower Extremity Functional Scale; OHS, Oxford Hip Score; HOOS-JR, Hip Disability and Osteoarthritis Outcome Score Joint Replacement; QoR-15, Quality of Recovery-15; CMS, Centers for Medicare and Medicaid Services; ASC, ambulatory surgery center. Notes: Arrows indicate the sequential progression of steps and the decision-making flow within the algorithm. |
Search Strategy and Selection Criteria
A comprehensive literature search was conducted across PubMed, Embase, and the Cochrane Library for English-language articles published between January 2010 and December 2025. Search terms included combinations of “total hip arthroplasty,” “same-day discharge,” “outpatient,” “enhanced recovery after surgery,” “early recovery,” and “perioperative optimization.” We prioritized high-level evidence, including systematic reviews, meta-analyses, and randomized controlled trials. Large-scale registry analyses and multicenter cohort studies were also included to provide real-world context. Case reports and non-peer-reviewed commentaries were generally excluded unless they offered unique insights into emerging technologies.
Current Landscape, Evolving Trends, and Patient Selection Strategies
Growth Trajectory and Driving Forces
The adoption of SDD-THA has accelerated markedly in recent years, with national database analyses documenting year-over-year increases in SDD rates that outpace those of same-day total knee arthroplasty (TKA).17 This growth is propelled by a confluence of clinical, economic, and policy-level drivers. The CMS removal of THA from the inpatient-only list might represents the single most influential policy catalyst, directly enabling a greater proportion of Medicare beneficiaries to undergo THA in ambulatory settings.9,18,19 Concurrently, commercial payers have increasingly favored outpatient designation to contain costs.20 The COVID-19 pandemic served as an additional accelerant, compelling healthcare systems to preserve inpatient capacity by migrating eligible elective procedures to ambulatory environments.13,21
From a clinical perspective, the safety profile of SDD-THA has been consistently validated across high-volume centers. Comparative analyses demonstrate that 90-day complication rates, readmission rates, and emergency department visit rates in SDD cohorts are equivalent to, or lower than those observed in matched inpatient cohorts, provided standardized ERAS pathways are rigorously followed.22–26 Patient satisfaction metrics further support the model, with SDD patients reporting higher satisfaction with pain management, nursing care, and discharge instruction quality.27–29
Patient Selection: A Multidimensional Decision Framework
The safety and efficacy of SDD-THA are predicated upon rigorous, evidence-based patient selection. Indiscriminate application of the SDD pathway risks increasing failure-to-launch events, which adversely impact patient experience, resource utilization, and institutional efficiency.15,30 Contemporary patient selection has evolved from simple age and comorbidity checklists into a multidimensional framework integrating medical status, functional capacity, psychosocial resources, and surgical logistics.
Medical Comorbidity and Physiological Reserve
Lower American Society of Anesthesiologists (ASA) physical status classification consistently predicts successful SDD. Patients classified as ASA I–II demonstrate significantly higher SDD success rates compared with ASA III or higher.31–33 Specific comorbidities conferring elevated risk for prolonged LOS include congestive heart failure, chronic obstructive pulmonary disease, dependent functional status, and the presence of multiple concurrent medical conditions.18,19,34 The Charlson Comorbidity Index (CCI) provides a quantitative comorbidity burden assessment. A CCI ≥ 4 has been identified as a significant predictor of conversion from planned outpatient to inpatient status.34 Notably, isolated primary hypertension may not constitute a contraindication to same-day surgery.19 Preoperative chronic opioid use represents an underappreciated risk factor, as patients with established opioid dependence demonstrate inferior subjective and objective postoperative mobility recovery, lower step counts at three and six months, and greater self-reported ambulatory limitations.35
Age and Sex
Advancing age is an independent predictor of SDD failure, with patients over 70 years, particularly those aged 76–80 and above, exhibiting significantly elevated 30-day readmission risk.30,36,37 However, age alone should not serve as an absolute exclusion criterion. Carefully selected, highly motivated Medicare-aged patients with limited comorbidity burden can achieve outcomes comparable to younger cohorts.18,38 For patients older than 70 years, expectations regarding SDD feasibility should be appropriately calibrated, especially for female patients and those requiring preoperative assistive devices.39 Female sex has been consistently associated with higher failure-to-launch rates and greater susceptibility to postoperative OI.15,30,40,41
Functional Status and Body Composition
Preoperative functional capacity is among the most potent predictors of early recovery trajectory. The Timed Up and Go (TUG) test, with cutoffs such as < 9.7 seconds, has demonstrated significant association with shorter LOS.42 The Lower Extremity Functional Scale (LEFS) score at baseline predicts postoperative outcomes including LOS, SDD rate, independent ambulation at discharge, and home discharge probability.43 Grip strength, as a readily measurable surrogate of global muscle strength and nutritional status, independently predicts postoperative complications, unplanned readmission, discharge disposition, and functional recovery following THA.44,45 Preoperative serum albumin levels below 3.5 g/dL have been linked to low grip strength and increased complication risk, reinforcing the importance of nutritional screening.44
Psychosocial and Environmental Factors
Adequate home caregiver support and a safe domestic environment are non-negotiable prerequisites for SDD.46,47 The role of informal caregivers assumes heightened importance when patients return home within hours of a major surgical procedure. Caregiver burden following joint arthroplasty is significant and correlates with female caregiver sex, greater daily time investment, and inadequate preoperative preparation.48 A scoping review has highlighted the paucity of data regarding the impact of outpatient THA on informal caregivers, underscoring a critical evidence gap.49 Married patients demonstrate lower rates of conversion from outpatient to inpatient status.34 Psychological resilience may also influence recovery, with emerging evidence suggesting that higher resilience predicts better patient-reported physical and mental health outcomes and may attenuate early postoperative opioid consumption50 (Table 1).
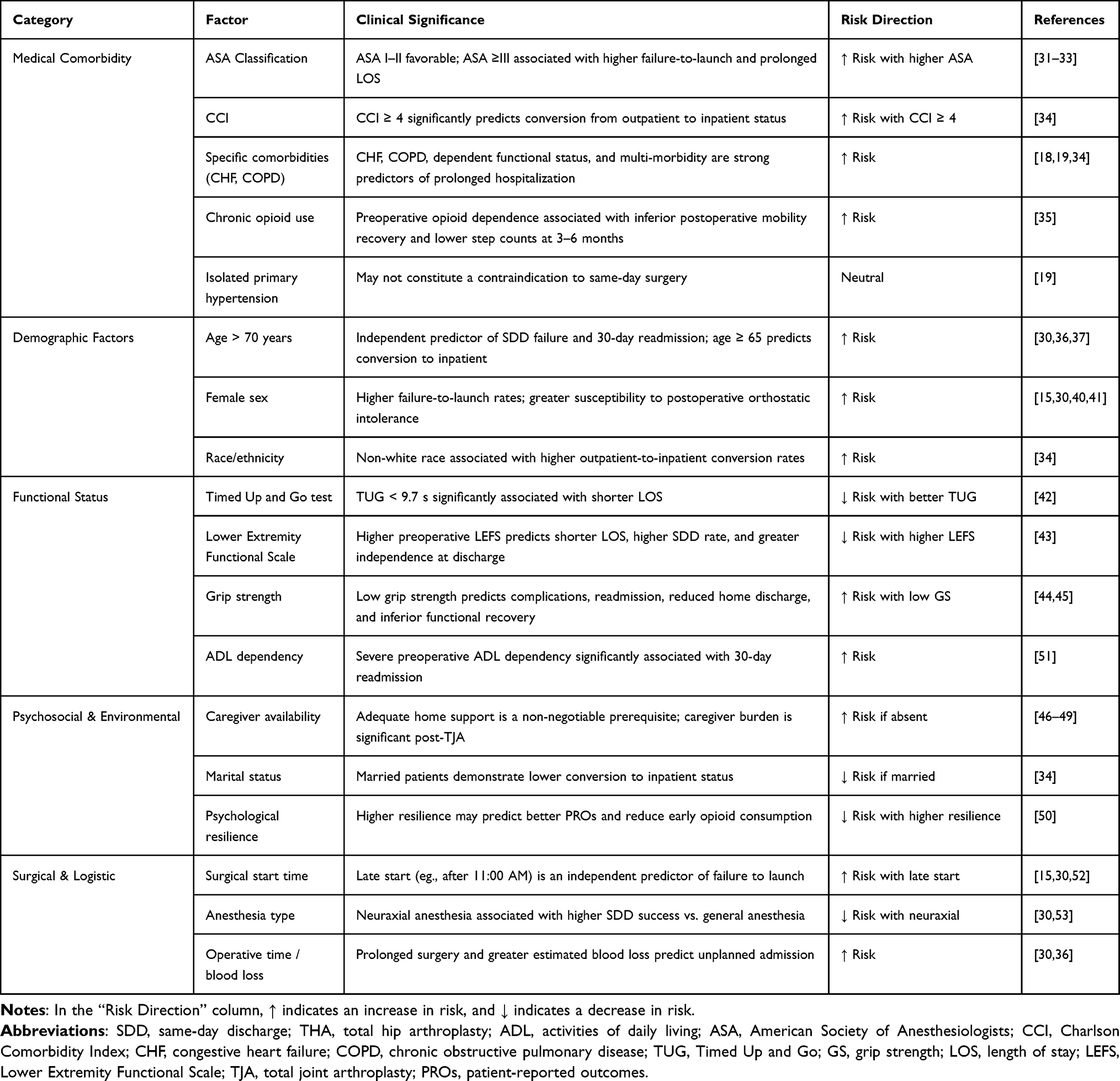 |
Table 1 Multidimensional Patient Selection Framework for SDD-THA: Risk Factors, Clinical Significance, and Supporting Evidence |
Risk Stratification Tools and Predictive Models
The development of validated risk stratification instruments has advanced the precision of patient selection. The Outpatient Arthroplasty Risk Assessment (OARA) score, which integrates age, body mass index (BMI), comorbidity burden, and medication use, was designed specifically to identify candidates suitable for SDD.32 Multicenter validation studies confirm that lower OARA scores (<80) predict higher SDD success rates with lower complication and readmission risk, outperforming ASA classification alone.32,54 The OARA has also demonstrated predictive utility in revision THA settings.55 The Risk Assessment and Prediction Tool (RAPT), which synthesizes age, sex, comorbidity, preoperative mobility, and social support, effectively discriminates between patients appropriate for outpatient versus inpatient pathways.56,57 Machine learning models integrating demographic, comorbidity, and functional variables are increasingly being applied to predict LOS and discharge status with high accuracy, providing data-driven decision support58,59 (Figure 2). Furthermore, natural language processing pipelines capable of automatically extracting and analyzing relevant clinical information from electronic health records represent a promising avenue for efficient, large-scale risk assessment.60
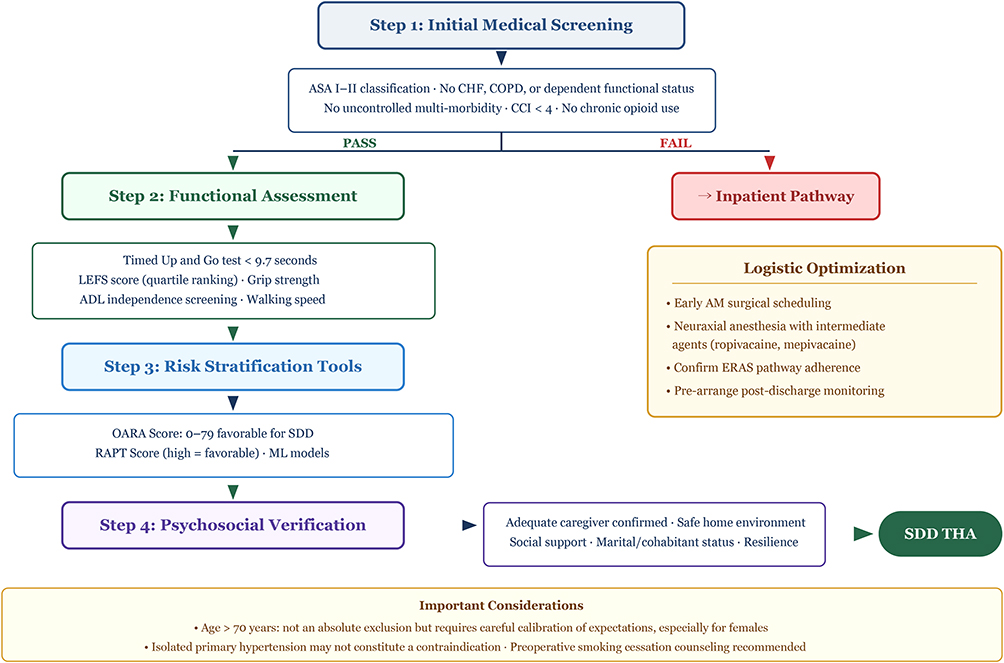 |
Figure 2 Stepwise Patient Selection and Risk Stratification Algorithm for SDD-THA. Abbreviations: SDD, same-day discharge; THA, total hip arthroplasty; ASA, American Society of Anesthesiologists; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CCI, Charlson Comorbidity Index; ERAS, enhanced recovery after surgery; LEFS, Lower Extremity Functional Scale; ADL, activities of daily living; OARA, Outpatient Arthroplasty Risk Assessment; RAPT, Risk Assessment and Prediction Tool. Notes: Arrows indicate the sequential progression of steps and the decision-making flow within the algorithm. |
Failure to Launch: Causes and Modifiable Risk Factors
Despite rigorous screening, a proportion of patients planned for SDD fail to achieve SDD. Understanding the causes of this “failure to launch” is essential for pathway refinement. The most prevalent reasons include failure to achieve physical therapy milestones (eg., independent ambulation, stair negotiation), postoperative hypotension or dizziness, PONV, inadequate pain control, and urinary retention.15,30,36,37,61 Patient preference changes after surgery also contribute to SDD failure.62 Critically, several failure-to-launch risk factors are modifiable: active smoking, excessive peak postoperative pain scores, and late surgical start times (eg., afternoon scheduling) have been consistently identified as independent predictors.15,30,52 These findings support targeted interventions including preoperative smoking cessation counseling, optimization of multimodal analgesia, expectation management, and scheduling of SDD candidates in early operative sequence.
Perioperative ERAS Protocols: Key Elements and Implementation
The ERAS Framework: Rationale and Evidence for Protocol Adherence
The ERAS framework constitutes the clinical backbone of SDD-THA, providing a systematic, evidence-based approach to attenuating surgical stress, maintaining physiological homeostasis, and expediting functional restoration.10,63 ERAS is not a static checklist but a dynamic, individualized clinical pathway spanning the preoperative, intraoperative, and postoperative continuum. Its effectiveness derives not from any single intervention, but from the synergistic interaction of multiple concurrent modalities and the degree of institutional adherence to the protocol as an integrated whole. The landmark POWER2 prospective cohort study demonstrated a clear dose-response relationship between ERAS protocol compliance and patient outcomes that patients in the highest compliance quartile experienced significantly fewer overall and moderate-to-severe complications and shorter LOS compared with those in the lowest quartile.64 This underscores the imperative to implement ERAS as a comprehensive package rather than selectively adopting individual components10,28 (Table 2).
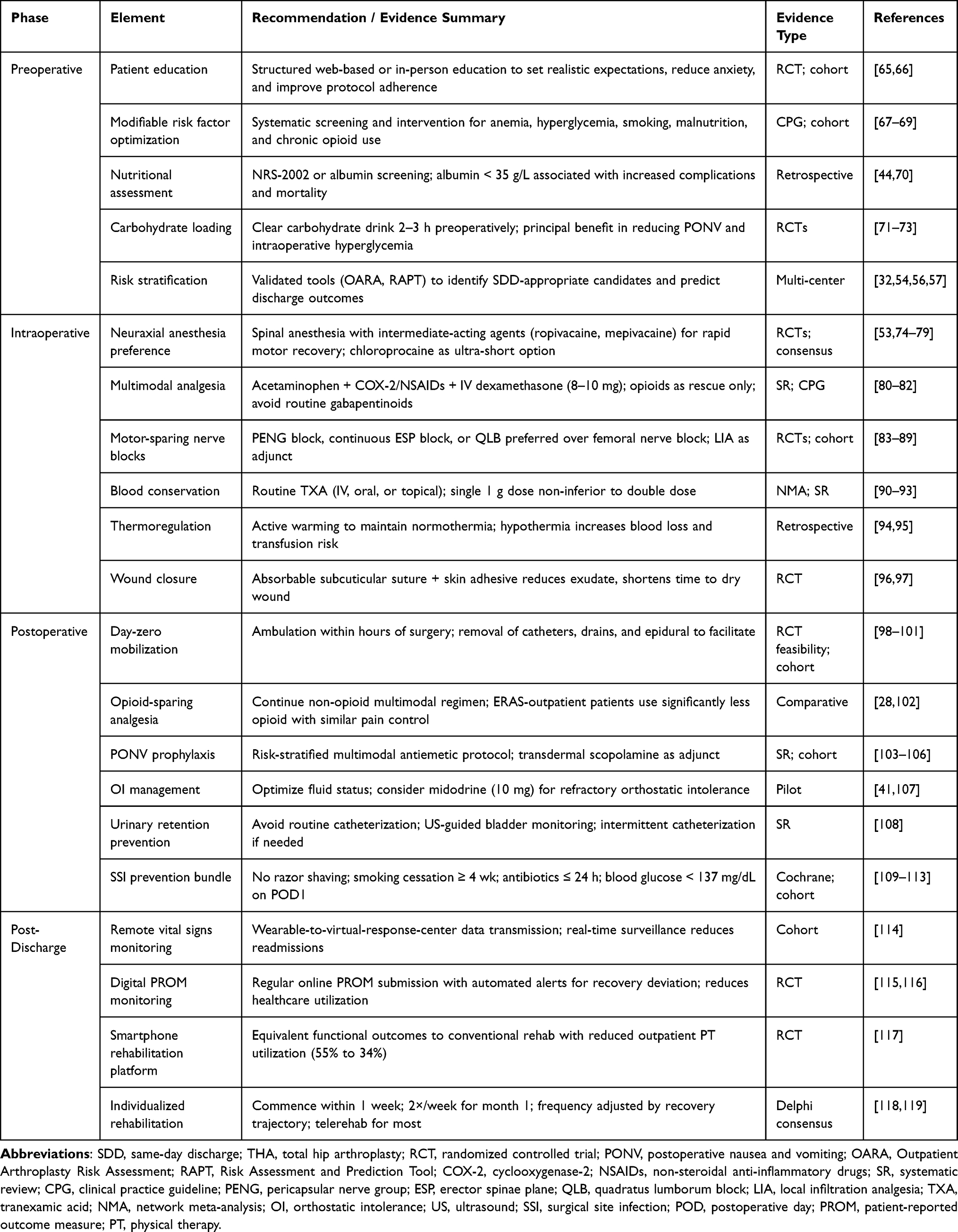 |
Table 2 Key Elements of the Integrated ERAS-SDD Protocol for THA Across the Perioperative Continuum |
Preoperative Optimization and Patient Education
The preoperative phase serves as the foundation of the ERAS pathway, centering on patient education and physiological optimization. Comprehensive preoperative education whether delivered via web-based digital platforms or in-person sessions, effectively manages expectations, alleviates anxiety, enhances adherence to rehabilitation protocols, and has been associated with shorter LOS.65,66 Clinical practice guidelines recommend systematic preoperative optimization of modifiable risk factors including anemia, hyperglycemia, and smoking.67 Diabetic patients, even within ERAS pathways, exhibit higher complication rates, prolonged LOS, and lower long-term joint-forgotten scores, highlighting the critical importance of stringent glycemic control.68 This evidence supports a paradigm shift from the traditional concept of “preoperative clearance” to proactive “preoperative optimization,” systematically screening for and intervening upon modifiable risk factors such as obesity, malnutrition, anemia, uncontrolled blood glucose, smoking, and chronic opioid use.69 Preoperative nutritional assessment should be incorporated as standard practice, as malnutrition (albumin < 35 g/L) is an independent risk factor for postoperative complications and mortality following THA.44,70
Preoperative carbohydrate loading, a traditional ERAS component, has been re-evaluated in recent evidence. Its principal benefits in non-diabetic patients may reside in attenuation of intraoperative hyperglycemia and reduction of PONV rather than direct reduction of infectious complications.71–73 For SDD patients, the mitigation of PONV and improvement of early comfort are themselves clinically meaningful objectives supporting timely discharge.
Intraoperative Management: Precision and Homeostasis
Intraoperative management within the ERAS framework encompasses anesthesia optimization, surgical technique refinement, blood conservation, and thermoregulation. Multimodal analgesia integrating local anesthetic infiltration or regional nerve block with non-opioid systemic agents constitutes the analgesic cornerstone.103,120,121 The POWER2 sub-study identified local anesthesia as an independent predictor of earlier postoperative mobilization.98 Regarding surgical technique, while ERAS consensus statements note insufficient evidence to designate any single surgical approach as superior for achieving discharge criteria,121 robot-assisted THA has attracted attention for its enhanced precision in component positioning and limb-length equalization.122 Within ERAS-managed cohorts, robot-assisted THA does not adversely affect blood loss, pain, functional recovery, or complication rates, supporting its safe integration into ERAS-outpatient pathways.123 Comparative data on surgical approach suggest that direct anterior, direct superior, and posterior approaches yield similar early recovery outcomes when performed within standardized perioperative protocols, indicating that surgeon proficiency and pathway standardization may outweigh the intrinsic advantages of any particular surgical approach.124,125 The lack of high-level RCT evidence favoring one technique over others remains a limitation in the current landscape.
Intraoperative thermoregulation is essential that hypothermia (core temperature < 36°C) independently increases intraoperative blood loss and perioperative transfusion rates.94 Active warming measures should therefore be routinely implemented.95 Wound closure technique may also influence discharge timing that absorbable subcuticular suture with skin adhesive significantly reduces wound exudate, shortens time to dry incision, and decreases LOS compared with metallic staples, offering practical advantages for SDD pathways that include “dry wound” as a discharge criterion.96,97
Postoperative Management: Analgesia, Symptom Control, and Early Mobilization
Postoperative management directly governs early recovery quality and discharge readiness. ERAS pathways emphasize non-opioid-based analgesic regimens that provide adequate pain control while minimizing opioid-related adverse effects including nausea, vomiting, ileus, sedation, which are common barriers to timely mobilization and discharge.28,120 Patients managed on ERAS-outpatient pathways demonstrate significantly lower early postoperative opioid consumption with comparable pain perception compared with traditional inpatient counterparts, achieving a superior analgesic benefit-risk ratio.28 In addition, prophylactic antiemetic administration should also be protocolized.103
Early mobilization, ideally within hours of surgery is the cornerstone postoperative objective. Mobilization within 24 hours postoperatively is associated with shorter LOS and superior functional recovery.98–100 Randomized feasibility data confirm that day-zero walking is safe and effective, significantly shortening the time to achieve functional milestones including transfer, ambulation, and stair negotiation.101 Achievement of all unnecessary physiological barriers to mobilization such as routine urinary catheterization, surgical drains, and epidural analgesia, should be avoided.98 Patients undergoing ERAS-outpatient THA demonstrate significantly earlier return to walking, stair climbing, showering, daily activities, and exercise compared with contralateral limbs managed via traditional inpatient pathways.28
Anesthesia and Multimodal Analgesia Optimization
Anesthetic Technique Selection
Anesthetic management for SDD-THA has evolved from a singular focus on intraoperative conditions to a comprehensive strategy targeting the entire perioperative recovery trajectory. The choice between neuraxial and general anesthesia remains a topic of active investigation. While the ICAROS group recommends neuraxial anesthesia based on its association with lower overall mortality and complication rates,126 the recent REGAIN multicenter RCT demonstrated no significant difference in 60-day mortality or walking independence between the two techniques.53 This highlights a critical area of uncertainty, suggesting that the benefits of spinal anesthesia may be more pronounced in specific subsets of patients rather than as a universal mandate for all SDD candidates. However, spinal anesthesia remains the preferred technique in many high-volume SDD centers in practice, due to its favorable hemodynamic profile, reduced general anesthetic exposure, and potential for earlier cognitive recovery.127
Within the domain of spinal anesthesia, the choice of local anesthetic agent profoundly influences early mobilization kinetics, which is a critical determinant of SDD feasibility. Traditional long-acting agents such as bupivacaine produce prolonged motor blockade that delays ambulation. Contemporary evidence strongly supports the use of intermediate- or short-acting agents. Ropivacaine-based spinal anesthesia enables significantly earlier lower-limb motor recovery, with studies demonstrating that warmed ropivacaine achieves grade 4 or higher motor strength within 3.5 hours postoperatively.74,75 Mepivacaine spinal anesthesia yields more predictable motor recovery compared with bupivacaine, with a double-blinded randomized trial demonstrating that 70% of mepivacaine recipients achieved independent ambulation within 3–3.5 hours versus substantially fewer bupivacaine recipients, translating to higher SDD rates.76–78 Chloroprocaine, an ultra-short-acting agent, has also demonstrated the ability to facilitate more rapid discharge without increasing complications.79 These pharmacokinetic considerations are central to optimizing the anesthetic prescription for SDD-targeted THA.
Multimodal Pharmacological Analgesia
The optimization of multimodal analgesia is paramount for SDD-THA. The 2021 PROSPECT guideline for THA recommends a foundational regimen comprising acetaminophen, COX-2-selective inhibitors or non-selective NSAIDs (administered preoperatively or intraoperatively and continued postoperatively), with opioids reserved strictly as rescue analgesics.80 Intravenous dexamethasone (8–10 mg) is recommended for its synergistic analgesic and anti-inflammatory properties.80 A systematic review and meta-analysis confirmed that perioperative systemic dexamethasone reduces LOS in total joint arthroplasty.81 Notably, the PROSPECT guideline explicitly recommends against routine gabapentinoid use, as the analgesic benefit fails to achieve the minimal clinically important difference while increasing the risk of dizziness and visual disturbance.80,82 Regarding acetaminophen delivery, preoperative oral administration provides equivalent postoperative analgesia to intravenous formulation at lower cost, aligning with the efficiency principles of SDD.128
Awareness of potential drug interactions is warranted. Dual NSAID therapy (eg., aspirin for thromboprophylaxis plus ibuprofen for analgesia) carries a small but clinically relevant risk of acute kidney injury (approximately 2.9%), although most cases are self-resolving.129 Opioid-sparing strategies, including opioid-free anesthesia protocols, have demonstrated feasibility in ambulatory THA, offering the potential for further reduction in opioid-related adverse events that impede early recovery.102
Regional Anesthesia Techniques for Hip-Targeted Analgesia
Regional anesthesia techniques constitute a critical pillar of multimodal analgesia, directly influencing early mobilization capacity. Traditional femoral nerve blockade, while providing effective analgesia, is unsuitable for SDD-targeted THA due to quadriceps motor weakness that impedes ambulation.80,83 Contemporary practice has therefore shifted toward hip-selective blocks that preserve motor function while providing targeted sensory analgesia.
The pericapsular nerve group (PENG) block has emerged as a promising technique, demonstrating superior short-term analgesia compared with femoral nerve block following hip surgery while better preserving quadriceps strength.83,84 Continuous erector spinae plane (ESP) block has been shown to significantly increase total walking distance on postoperative days one and two compared with continuous fascia iliaca block, with equivalent pain scores and opioid consumption, suggesting a kinematic advantage for early mobilization.85 The quadratus lumborum block (QLB) has demonstrated superiority over femoral nerve and fascia iliaca blocks in hip arthroscopy, with shorter post-anesthesia care unit stays,86 and anterior QLB specifically has shown promise in improving postoperative recovery quality following THA.87 The fascia iliaca block remains a valid option, with prospective randomized data confirming its efficacy in reducing postoperative opioid consumption.88 Additionally, combined lateral femoral cutaneous nerve and ilioinguinal/ iliohypogastric nerve blocks have demonstrated analgesic efficacy in direct anterior approach THA.89 Collectively, these data support the preferential use of motor-sparing, hip-targeted regional techniques in SDD-THA protocols (Table 3).
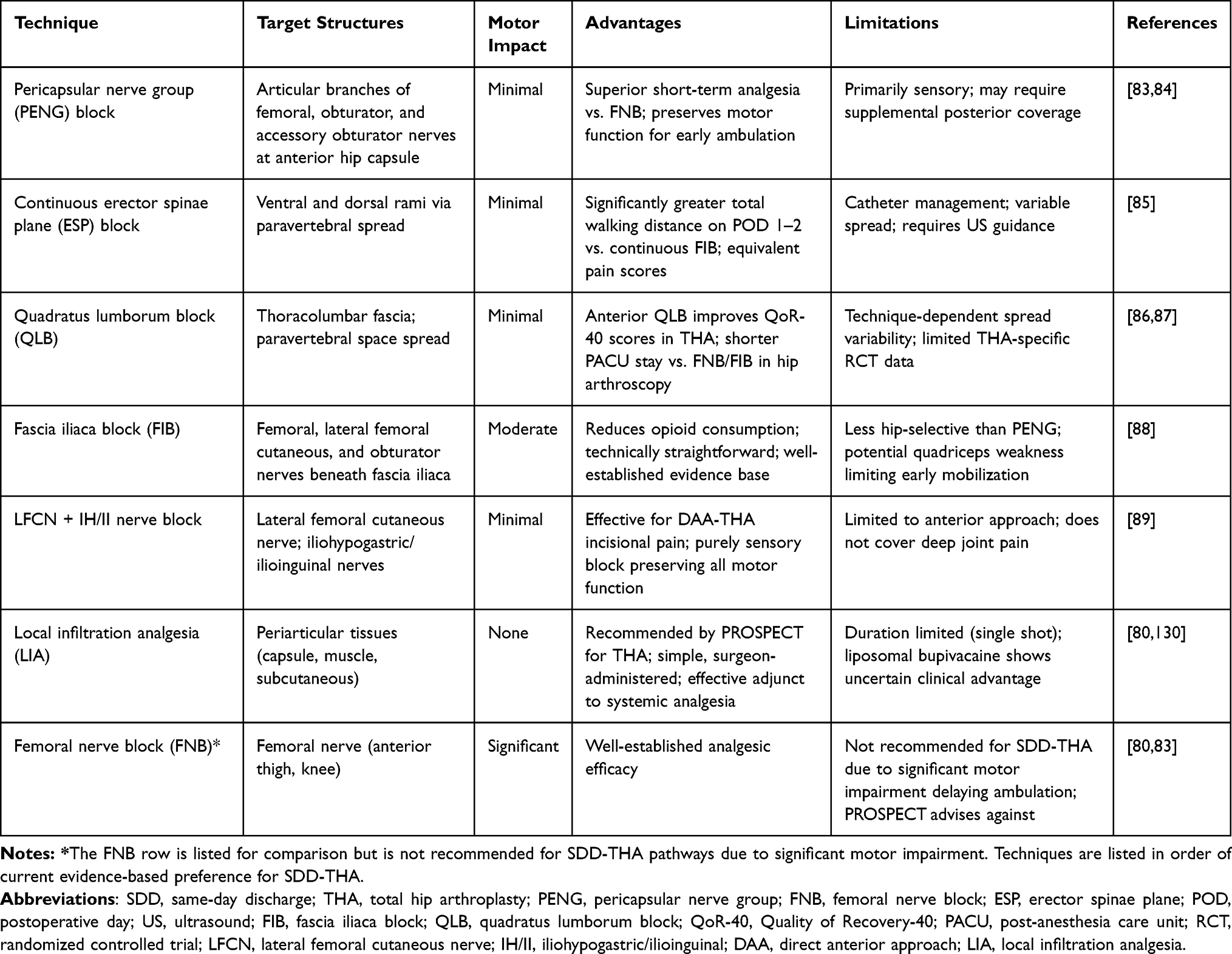 |
Table 3 Comparative Overview of Regional Anesthesia Techniques for Hip-Targeted Analgesia in SDD-THA |
Local Infiltration Analgesia and Adjuvant Agents
Local infiltration analgesia (LIA) represents an additional component of multimodal perioperative analgesia. The PROSPECT guideline recommends single-shot LIA particularly for patients with contraindications to foundational systemic analgesics or those anticipated to experience severe postoperative pain.80 Regarding the choice of local anesthetic, liposomal bupivacaine has attracted attention for its prolonged theoretical duration of action. However, a meta-analysis concluded that while it may offer statistically significant advantages in pain scores over conventional LIA, the clinical significance of this improvement is uncertain and no clear benefit in opioid reduction has been demonstrated.130 Therefore, routine use requires careful cost-effectiveness evaluation.
Among adjuvant agents, dexmedetomidine as a highly selective α2-adrenergic agonist, prolongs sensory blockade duration when used for sedation during combined spinal-epidural anesthesia compared with midazolam,131 attenuates tourniquet-induced metabolic and coagulation disturbances,132 and reduces postoperative opioid requirements. However, intravenous dexmedetomidine use in the spinal anesthesia setting warrants caution due to the potential for elevated postoperative hypotension rates.133 Transdermal scopolamine has been demonstrated to effectively reduce PONV incidence following total joint arthroplasty and may indirectly promote early functional activity through improved comfort.104
Perioperative Blood Management and Complication Prevention
Tranexamic Acid and Blood Conservation Strategies
Meticulous perioperative blood management is fundamental to ensuring hemodynamic stability, facilitating early mobilization, and achieving safe SDD. Tranexamic acid (TXA) has become the cornerstone of blood conservation in THA. Network meta-analysis and randomized controlled trials confirm that intravenous, oral, and intra-articular topical TXA administration all effectively reduce total blood loss and transfusion rates, with no significant differences in efficacy among routes.90–92 Critically, the safety profile of TXA extends to high-risk patients with histories of venous thromboembolism, myocardial infarction, stroke, renal disease, and atrial fibrillation, with no observed increase in thromboembolic complications.93 Single-dose (1 g) intravenous TXA achieves comparable efficacy to double-dose regimens, supporting protocol simplification.91
Complementary blood conservation measures include active prevention of intraoperative hypothermia, which independently increases blood loss and transfusion requirements,94 and avoidance of routine closed-suction drain placement, which has not demonstrated benefit in reducing total blood loss or infection risk and may paradoxically increase transfusion needs and delay straight-leg raising recovery.134 Bipolar sealing devices have similarly failed to demonstrate superiority over standard electrocautery for blood loss or functional outcomes in arthroplasty.135 Preoperative hemoglobin optimization is critical: when hemoglobin falls below 135 g/L, transfusion risk increases significantly and progressively; moreover, hemoglobin values deviating from the 137–141 g/L range (in either direction) are associated with increased 30-day emergency visits and readmissions.136
Prevention of OI, PONV, and Urinary Retention
OI is a frequently underrecognized barrier to early mobilization following THA, with an overall incidence of approximately 25%, significantly exceeding that following TKA.41 Risk factors include female sex, THA (versus TKA), and bupivacaine-based spinal anesthesia.41,137 Preliminary investigation of the vasopressor midodrine (10 mg) has demonstrated a significant pressor response and potential reduction in adverse mobility events, offering a potential pharmacological strategy for refractory OI.107
PONV risk factors in the arthroplasty population include female sex, history of motion sickness, migraine history, and lower BMI.105,106 Risk-stratified, multimodal antiemetic prophylaxis is essential within SDD protocols. Urinary retention risk factors encompass advanced age, male sex, benign prostatic hyperplasia, opioid use, and patient-controlled analgesia.108 Routine indwelling catheterization should be avoided or removed within 48 hours, with ultrasound-guided bladder volume monitoring and intermittent catheterization as the preferred management strategy.108
Surgical Site Infection Prevention
Surgical site infection (SSI) prevention requires attention to multiple perioperative details. Razor shaving significantly increases SSI risk relative to no hair removal, clippers or depilatory agents should be used while necessary.109 Preoperative smoking cessation of at least four weeks also significantly reduces wound infection rates.110 Current evidence supports perioperative antibiotic prophylaxis for THA but does not support continuation beyond 24 hours.111 Postoperative glycemic control is critical: in non-diabetic patients, first-postoperative-morning blood glucose ≥ 137 mg/dL is linearly associated with increasing periprosthetic joint infection risk.112 Allogenic blood transfusion independently increases both superficial and deep wound infection risk, further reinforcing the importance of comprehensive blood conservation strategies.113
Regarding venous thromboembolism screening, a noteworthy temporal trend has been documented that as LOS has shortened, the rate of inpatient lower-extremity ultrasonography has declined dramatically (from 7.0% in 2010 to 0.3% in 2020), yet the two-week postoperative DVT diagnosis rate has remained stable.138 This suggests that reduced LOS has not increased DVT miss rates and may have curtailed unnecessary screening.
Functional Status and Sarcopenia as Outcome Predictors
Patient functional reserve and muscle strength represent powerful predictors of early recovery quality and complication risk, with particular relevance to the ageing THA population. Severe preoperative dependence in activities of daily living (ADL) is significantly associated with 30-day readmission following THA.51 Poor ADL recovery during post-discharge home care or rehabilitation independently elevates rehospitalization risk.139–141 Grip strength, as a simple and reliable surrogate marker of systemic muscle status, predicts a constellation of adverse outcomes including pressure injury, transfusion, urinary tract infection, prolonged LOS, unplanned readmission, reduced home discharge probability, and inferior hip function and quality-of-life recovery.44,45 Preoperative walking speed has also been identified as an independent predictor of six-month functional recovery and quality of life following hip fracture surgery.142 These findings collectively support the incorporation of functional assessments such as ADL dependency screening, grip strength measurement, TUG testing, and LEFS scoring, into the preoperative evaluation algorithm for SDD THA candidates, enabling targeted prehabilitation or pathway modification for high-risk individuals.
Early Rehabilitation Strategies and Functional Recovery Trajectories
Early Mobilization as the ERAS Cornerstone
Early postoperative mobilization is the main objective of the ERAS pathway and the critical gateway to successful SDD. A large prospective cohort study across 131 Spanish hospitals demonstrated that 69.3% of THA/TKA patients achieved mobilization within 24 hours, with multivariable analysis identifying local anesthesia use, higher preoperative hemoglobin, and avoidance of urinary catheters, surgical drains, and epidural analgesia as significant independent facilitators.98 Surgical start time is an additional modifiable determinant. Earlier start times (before 9:00 AM) significantly increase the probability of same-day discharge.143 A randomized controlled feasibility study confirmed that day-zero mobilization (within hours of surgery) is safe and effective, accelerating functional milestone achievement and promoting earlier discharge.101 Importantly, achievement of walking-level rehabilitation has been identified as a strong independent predictor of ambulatory capacity at discharge.142
Objective Measurement of Recovery Trajectories Using Digital Health Technology
The objective characterization of postoperative recovery trajectories has been revolutionized by wearable sensor technology and smartphone-based platforms. A systematic review and meta-analysis confirmed the efficacy of lower-limb wearable devices in assessing recovery following THA and TKA, with capacity to monitor step count, gait velocity, standing duration, gait stability, and estimated six-minute walk test performance.144 A prospective study utilizing wearable accelerometry to track daily ambulatory function over one year following THA revealed a non-linear recovery trajectory: mean daily step count demonstrated significant improvement from six weeks postoperatively onward, with continued gains at six and twelve months; gait velocity showed a transient decline at six weeks due to surgical trauma and protective behavior, before significant improvement at six and twelve months; stability metrics improved notably at twelve months.145 These objective data delineate the characteristic multiphasic recovery pattern: an initial period focused on pain control and basic mobility restoration, an intermediate phase (3–6 months) of rapid gait parameter and activity volume improvement, and a late phase beyond 6 months of stabilization and further movement optimization (Figure 3).
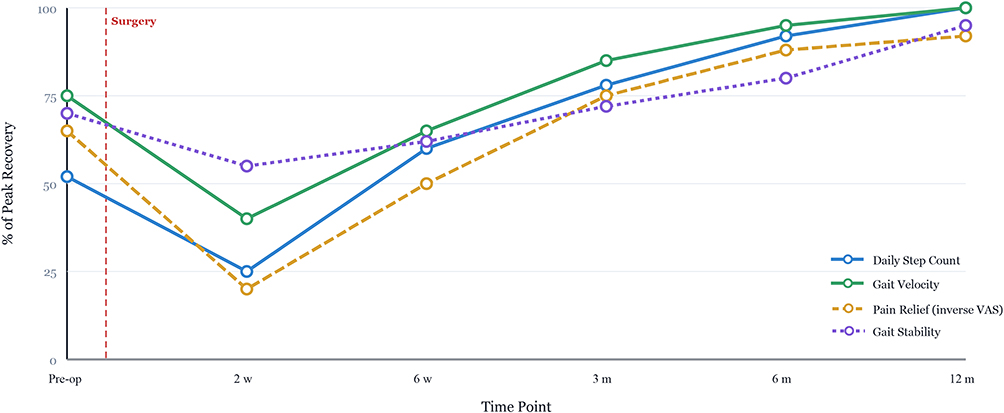 |
Figure 3 Evidence-Based Schematic Synthesis of the Non-Linear, Multiphasic Recovery Trajectory Following THA. Notes: This figure provides a conceptual visualization of recovery patterns synthesized from contemporary wearable sensor and patient-reported data. Recovery metrics including daily step count, gait velocity, pain relief (inverse VAS), and gait stability are plotted as percentage of peak recovery over a 12-month postoperative period. The trajectory is characterized by three distinct phases: (1) an acute recovery phase (0–6 weeks) featuring an initial decline attributable to surgical trauma and protective behavior, followed by early functional restoration driven by day-zero mobilization protocols; (2) a rapid progress phase (6 weeks to 6 months) during which gait parameters and activity volumes demonstrate accelerated improvement; and (3) a plateau phase (6–12 months) in which metrics approach peak values with continued optimization of movement patterns and stability. The dashed vertical line indicates the time of surgery. |
Remote vital signs monitoring has demonstrated particular value during the acute post-discharge period. Through wearable-to-virtual-response-center data transmission, medical teams can provide real-time surveillance and early intervention for physiological deviations, effectively reducing unplanned readmissions and emergency department visits.114 A prospective randomized trial evaluating a smartphone-based rehabilitation platform demonstrated that early functional outcomes were comparable to conventional rehabilitation, while significantly reducing outpatient physiotherapy utilization (from 55.4% to 34.0%) without increasing complications, providing a more flexible, lower-cost rehabilitation alternative compatible with the SDD model.117 These characteristic patterns, though synthesized into a schematic representation in Figure 3 to aid clinical visualization, are fundamentally derived from objective longitudinal evidence documenting the multi-phasic nature of functional restoration.
Activity Restrictions and Individualized Rehabilitation Paradigms
Longstanding postoperative hip precaution protocols to prevent dislocation are being re-evaluated. A retrospective cohort study comparing standard versus relaxed hip precautions following posterolateral-approach THA found no statistically significant difference in three-month dislocation rates.146 This finding is corroborated by a comprehensive review concluding that routine hip precaution recommendations may be unnecessary for elective primary THA.147 These data support permitting SDD patients to engage in earlier, more autonomous functional activity within a safety framework.
The optimal intensity and delivery model of postoperative rehabilitation is evolving toward individualized, goal-directed strategies. A randomized controlled trial published in the BMJ demonstrated that for TKA patients at predicted high risk of poor recovery, an intensive 18-session supervised outpatient physiotherapy program yielded no clinically meaningful advantage over a single physiotherapy assessment followed by home-based exercise at 52-week follow-up across the Oxford Knee Score, pain, and functional satisfaction outcomes.118 A Delphi consensus study recommended that regardless of recovery status, outpatient rehabilitation should commence within one week postoperatively at a frequency of twice weekly during the first month, with subsequent frequency adjustments guided by individual recovery trajectory.119 Telerehabilitation was endorsed as appropriate for most patients, though not for those with slow recovery.119 These principles support a rehabilitation model that prioritizes high-quality patient education and clear home-based guidance over high-frequency supervised attendance, while preserving the flexibility to intensify support for patients demonstrating suboptimal recovery trajectories.
Rehabilitation Resource Variability and Policy Implications
Significant variability exists in postoperative rehabilitation resource utilization. A systematic review documented that outpatient physiotherapy utilization rates following TKA range from 16.7% to 84.5%.148 Patient characteristics influence rehabilitation including female patients, TKA (versus THA), and those requiring inpatient physiotherapy tend to receive more outpatient sessions, while older patients and those with depression histories use fewer services.149 At the health system level, bundled payment implementation has been projected to substantially reduce skilled nursing facility referrals while increasing home health care utilization, which is a shift that may be accompanied by decreased functional recovery and reduced treatment volume.150 This cautionary finding underscores the need for vigilance in ensuring that cost-containment policies do not inadvertently compromise functional outcomes.
Patient-Reported Outcomes and Functional Assessment in Monitoring Recovery Quality
Patient-Reported Outcome Measures in SDD-THA
Patient-reported outcome measures (PROMs) have become indispensable for capturing the patient perspective on recovery quality, complementing objective clinical assessments. Instruments including the Oxford Hip Score (OHS), Hip Disability and Osteoarthritis Outcome Score Joint Replacement (HOOS-JR), and Quality of Recovery-15 (QoR-15) provide multidimensional assessment of pain, function, and health-related quality of life.151,152 Studies consistently demonstrate significant PROMs improvement from three months to one-year post-THA.28,153 Crucially, early discharge does not appear to compromise patient-reported outcomes. A prospective study in planned SDD patients found no significant differences in postoperative day 1–7 pain scores, morphine consumption, or one-year OHS between patients discharged on the day of surgery and those who stayed overnight.154
A prospective investigation of the relationship between patient expectations and outcomes revealed that high preoperative expectations are associated with greater objective functional improvement but also greater unmet expectation as improvements frequently fall short of the magnitude anticipated, generating subjective dissatisfaction despite objectively favorable recovery.155 Furthermore, surgeon expectations have been shown to influence patient expectations and, in turn, objective outcomes.155 These findings highlight the limitations of relying exclusively on objective metrics and the importance of integrating expectation management into preoperative education.
Functional Assessment Tools for Risk Stratification
Standardized functional assessment instruments serve dual roles: preoperative risk stratification and postoperative recovery monitoring. The LEFS has demonstrated significant associations with THA surgical outcomes across multiple dimensions. Patients in the highest preoperative LEFS quartile achieve shorter LOS, higher SDD rates, greater independent ambulation at discharge, and higher home discharge rates.43 Grip strength measurement offers additional predictive power: in female TKA patients, preoperative grip strength exceeding 19 kg predicts adoption of a more efficient stair ascent pattern at one year.156 These assessments can therefore inform individualized perioperative care plans and resource allocation.
Digital PROM Platforms and Real-Time Alert Systems
The digitalization of PROM collection enables continuous, remote recovery surveillance with the capacity for automated early-warning intervention. A randomized controlled trial protocol has described a system in which digital PROM data are collected at regular intervals from THA/TKA patients, with algorithm-defined thresholds triggering alerts when recovery deviates from expected trajectories.115 Research assistants then contact the patient and physician to investigate the deviation and potentially adjust the management plan. A secondary analysis of a randomized trial (the Promoting Quality study) demonstrated that PROM-based monitoring with alerts significantly reduced post-surgical healthcare utilization, providing evidence that this approach can both improve care quality and contain costs.116 Such systems provide a viable framework for remote follow-up and precision intervention following SDD-THA.
Social Support and Its Association with Recovery Outcomes
A systematic review and meta-analysis confirmed that social support is a prognostic factor for selected patient-reported outcomes after joint replacement, with positive effects on long-term WOMAC scores and Oxford Knee Scores.157 These findings reinforce the importance of evaluating social network adequacy and home support systems as part of the comprehensive SDD assessment. Preoperative identification of patients with insufficient support should prompt proactive planning for community care resources or consideration of alternative surgical management models.
Healthcare Policy, Economic Evaluation, and Care Model Transformation
Policy and Administrative Consequences
The growth of SDD-THA is inherently associated with the reform of healthcare reimbursement. The CMS removal of THA from the inpatient-only list triggered a dramatic increase in outpatient-designated procedures, which combined with COVID-19-related hospital capacity pressures, resulted in over 50% of all THA and TKA procedures being completed as outpatient by the end of 2020.12 The transition from fee-for-service to value-based alternative payment models, particularly bundled payment programs, has fundamentally altered perioperative decision-making by incentivizing cost containment across the entire episode of care.150
However, the administrative implementation of these policy shifts has generated unintended consequences. The “two-midnight rule,” which classifies anticipated stays shorter than two midnights as outpatient, has compelled many hospitals to designate all THA procedures as outpatient to avoid audit and reimbursement denial risk.158 Surgeon surveys reveal that over 80% consider these classification changes to have increased administrative burden, while over 60% have encountered patients facing unexpected out-of-pocket costs due to outpatient designation.159 Patients classified as “outpatient” differ systematically from “inpatient” patients in baseline characteristics, average LOS, and discharge disposition.160 When patients requiring short-term observation are forced into outpatient classification, the resulting financial burden may fall disproportionately on the patient.161
Health-Economic Evaluation of SDD-THA
From a health-economic perspective, SDD-THA demonstrates favorable cost-effectiveness. Cost-utility analysis from a societal perspective, using a willingness-to-pay threshold of $50,000 per quality-adjusted life year, indicates that outpatient THA is more cost-effective than inpatient THA.162 Time-driven activity-based costing reveals lower mean facility costs for ambulatory surgery center (ASC)-based THA compared with hospital-based inpatient THA, primarily attributable to personnel cost reductions.163 However, CMS reimbursement reductions following the inpatient-only list removal substantially exceed the actual cost savings achievable, potentially undermining institutional incentives for ASC-based SDD programs.163
A patient-level value analysis has demonstrated that HOOS-JR improvement correlates weakly with total episode-of-care cost, whereas surgical setting and discharge destination are the primary determinants of “value”.151 THA performed at an ASC with home discharge generates substantially higher value than hospital-based THA with skilled nursing facility discharge. This emphasizes that value optimization requires comprehensive pathway redesign, not merely surgical technique refinement.
Safety of Ambulatory Surgery Center-Based THA
The safety of the ASC as an operative venue for THA has been substantiated by accumulating evidence. Comparative analyses of near-elderly, non-Medicare patients demonstrate lower readmission and complication rates for ASC-based versus hospital outpatient department-based arthroplasty.164 Private practice experience confirms that enhanced recovery pathways incorporating multimodal analgesia can achieve SDD rates exceeding 96%, with significantly reduced postoperative opioid consumption and no increase in complication rates with expanding SDD volumes.165 Novel “hyperspecialty” ASCs with extended care suites have demonstrated safety profiles equivalent to inpatient arthroplasty.26 Opioid-related adverse drug events are associated with increased inpatient mortality, prolonged LOS, higher costs, and elevated 30-day readmission rates, reinforcing the centrality of opioid-minimizing strategies regardless of surgical venue.166
Conclusions and Future Perspectives
Synthesis of Evidence and Clinical Paradigm Shift
SDD-THA has matured into an evidence-supported paradigm that, when integrated within rigorous ERAS-driven pathways, achieves clinical outcomes equivalent or superior to traditional inpatient management in appropriately selected candidates. Early recovery is a multidimensional, non-linear trajectory that can be objectively characterized via wearable technology.144,145 This process is governed by a synergistic interplay between patient-intrinsic factors such as functional reserve and resilience, and modifiable perioperative strategies, including motor-sparing anesthesia, multimodal analgesia, and protocolized mobilization.15,28,32,41,44,98 Successful implementation is predicated upon the systematic integration of risk-stratified selection utilizing validated tools like OARA and RAPT scores, and seamless digital transitions to home-based recovery.32,54,56,114,117
A fundamental paradigm shift is required: transitioning from the administrative goal of shortening hospital length of stay (LOS) to the clinical priority of optimizing recovery quality as the definitive endpoint. Fast-track protocols that prioritize discharge velocity over comprehensive physiological restoration risk deviating from the foundational ERAS objectives of minimizing complications and maximizing functional gains.10,167 Consequently, future SDD-THA pathways must anchor their success metrics to “optimal-recovery-quality-guided safe discharge,” focusing on the control of perioperative pathophysiology and the promotion of early functional independence.121,168,169
Limitations of Current Evidence and Future Frontiers
While current evidence is predominantly positive, it remains subject to selection bias, as most literature focuses on low-risk populations at high-volume centers. A relative paucity of data exists regarding SDD outcomes in complex populations, including those with severe obesity, cognitive impairment, or inadequate social support. Furthermore, the long-term impact of SDD on implant survivorship and patient-reported quality of life beyond the first year remains to be fully elucidated through larger, registry-based longitudinal studies.
To transcend current standardized protocols, several critical frontiers warrant prioritization. First, precision perioperative medicine may eventually integrate genomic and multi-omics data, such as identifying genetic polymorphisms like IL-6-174G>C that influence analgesic needs, with AI algorithms to design individualized SDD pathways.58,59,170 Second, integrated digital ecosystems via developing interoperable platforms that synthesize electronic health records, wearable-derived kinetics, and digital PROMs into real-time clinical decision support for both patients and care teams114–117,144 (Figure 4). Third, long-term outcome evaluation through national arthroplasty registries and extended follow-up studies is needed to determine whether the SDD model influences implant survivorship, long-term functional trajectories, and patient quality of life beyond the early postoperative period. Fourth, expanding research on the socioeconomic and psychological consequences of SDD on informal caregivers, who assume a pivotal role in home-based recovery.48,49 Finally, policy refinement must ensure alignment between reimbursement incentives and clinical quality standards, preventing the inappropriate shifting of financial burdens to patients.150,158,161
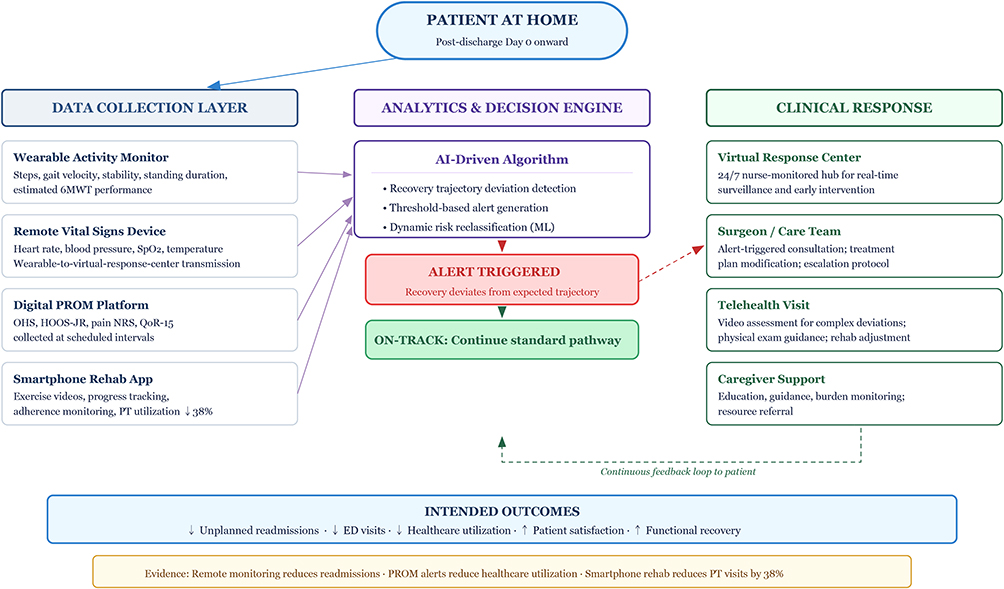 |
Figure 4 Proposed Conceptual Framework for an Integrated Digital Health Ecosystem. Abbreviations: SDD, same-day discharge; THA, total hip arthroplasty; 6MWT, six-minute walk test; OHS, Oxford Hip Score; HOOS-JR, Hip Disability and Osteoarthritis Outcome Score Joint Replacement; NRS, numeric rating scale; QoR-15, Quality of Recovery-15; PT, physical therapy; ML, machine learning; PROM, patient-reported outcome measure. Notes: This schematic integrates current evidence-based digital tools into a unified clinical model for remote post-discharge surveillance and intervention. Arrows denote the direction of data transmission and feedback loops within the ecosystem. In the “Intended Outcomes” section, ↑ indicates an increase or improvement, and ↓ indicates a reduction or decrease in the respective metric. |
Conclusions
The paradigm of SDD-THA holds transformative potential for addressing the escalating global demand for hip arthroplasty in an ageing population. Realizing this potential is dependent upon a sustained focus on patient-centered recovery quality—transcending reductive LOS metrics to embrace a holistic vision of functional independence and sustainable healthcare value. Through continued multi-disciplinary research collaboration, clinical pathway refinement, and health system innovation, SDD-THA has the potential to become a cornerstone of surgical practice, enabling more individuals to safely and comfortably regain quality of life following hip replacement surgery.
Abbreviations
THA, Total hip arthroplasty; OECD, Organisation for Economic Co-operation and Development; SDD, same-day discharge; ERAS, enhanced recovery after surgery; LOS, length of stay; CMS, Centers for Medicare and Medicaid Services; PONV, postoperative nausea and vomiting; OI, orthostatic intolerance; TKA, total knee arthroplasty; ASA, American Society of Anesthesiologists; CCI, Charlson Comorbidity Index; TUG, Timed Up and Go; LEFS, Lower Extremity Functional Scale; OARA, Outpatient Arthroplasty Risk Assessment; BMI, body mass index; RAPT, Risk Assessment and Prediction Tool; PENG, pericapsular nerve group; ESP, erector spinae plane; QLB, quadratus lumborum block; LIA, local infiltration analgesia; TXA, Tranexamic acid; SSI, surgical site infection; ADL, activities of daily living; PROMs, patient-reported outcome measures; OHS, Oxford Hip Score; HOOS-JR, Hip Disability and Osteoarthritis Outcome Score Joint Replacement; QoR-15, Quality of Recovery-15; ACS, ambulatory surgery center.
Acknowledgments
Authors thank Home for Researchers editorial team (www.home-forresearchers.com) for improving the English language in this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (No.82502974), Scientific Research and Innovation Platform for Intelligent and Precise Treatment of Bone and Joint Diseases in Shaanxi Province (No. 2024PT-13), Youth Top-Notch Talent Support Program of Honghui Hospital, Xi’an Jiaotong University (ynrc2024044), and the Natural Science Basic Research Program of Shaanxi Province (No. 2025JC-YBQN-1113 and 2025JC-YBQN-1181). The funding source had no influence on the study design, data collection, analysis, or interpretation of the findings.
Disclosure
The authors declare that they have no conflicts of interest to disclose for this work.
References
1. Price AJ, Alvand A, Troelsen A, et al. Knee replacement. Lancet. 2018;392(10158):1672–23. doi:10.1016/S0140-6736(18)32344-4
2. Schwartz AM, Farley KX, Guild GN, et al. Projections and epidemiology of revision hip and knee arthroplasty in the United States to 2030. J Arthroplasty. 2020;35(6S):S79–S85. doi:10.1016/j.arth.2020.02.030
3. Singh JA, Yu S, Chen L, et al. Rates of total joint replacement in the United States: future projections to 2020-2040 using the National Inpatient Sample. J Rheumatol. 2019;46(9):1134–1140. doi:10.3899/jrheum.170990
4. Shichman I, Roof M, Askew N, et al. Projections and epidemiology of primary hip and knee arthroplasty in medicare patients to 2040-2060. JB JS Open Access. 2023;8(1):e2200112.
5. Pabinger C, Lothaller H, Portner N, et al. Projections of hip arthroplasty in OECD countries up to 2050. Hip Int. 2018;28(5):498–506. doi:10.1177/1120700018757940
6. Sloan M, Premkumar A, Sheth NP. Future demand for total joint arthroplasty drives renewed interest in arthroplasty fellowship. HSS J. 2020;16(Suppl 2):210–215. doi:10.1007/s11420-019-09678-y
7. Kopp-Mulberg FE, Naik H. Arthritis: knee and hip arthroplasty. FP Essentials. 2025;548:13–17.
8. Vehmeijer SBW, Husted H, Kehlet H. Outpatient total hip and knee arthroplasty. Acta Orthop. 2018;89(2):141–144. doi:10.1080/17453674.2017.1410958
9. Osman B, Devarajan J, Skinner A, et al. Driving forces for outpatient total hip and knee arthroplasty with enhanced recovery after surgery protocols: a narrative review. Curr Pain Headache Rep. 2024;28(10):971–983. doi:10.1007/s11916-024-01266-y
10. Sivaloganathan S, Blakeney WG, Vendittoli PA. Modernizing total hip arthroplasty perioperative pathways: the implementation of ERAS-outpatient protocol. J Clin Med. 2022;11(12):3293. doi:10.3390/jcm11123293
11. Osman BM, Tieu TG, Caceres YG, et al. Current trends and future directions for outpatient total joint arthroplasty: a review of the anesthesia choices and analgesic options. J Am Acad Orthop Surg Glob Res Rev. 2023;7(9):e2200259.
12. Richardson MK, Wier J, Liu KC, et al. Same-day total joint arthroplasty in the United States from 2016 to 2020: the impact of the medicare inpatient only list and the COVID-19 pandemic. J Arthroplasty. 2024;39(4):858–863.e2. doi:10.1016/j.arth.2023.10.025
13. Chen AZ, Shen TS, Bovonratwet P, et al. Total joint arthroplasty during the COVID-19 pandemic: a scoping review with implications for future practice. Arthroplast Today. 2021;8:15–23. doi:10.1016/j.artd.2020.12.028
14. Sterne J, Crone A, Baker G, et al. High-volume day-case hip arthroplasty in a district general hospital. Bone Joint Open. 2025;6(9):1122–1128. doi:10.1302/2633-1462.69.BJO-2024-0235.R1
15. Rodriguez S, Shen TS, Lebrun DG, et al. Ambulatory total hip arthroplasty: causes for failure to launch and associated risk factors. Bone Jt Open. 2022;3(9):684–691. doi:10.1302/2633-1462.39.BJO-2022-0106.R1
16. Kabiri M, Brauer M, Shafrin J, et al. Long-term health and economic value of improved mobility among older adults in the United States. Value Health. 2018;21(7):792–798. doi:10.1016/j.jval.2017.12.021
17. Debbi EM, Mosich GM, Bendich I, et al. Same-day discharge total hip and knee arthroplasty: trends, complications, and readmission rates. J Arthroplasty. 2022;37(3):444–448.e1. doi:10.1016/j.arth.2021.11.023
18. Feder OI, Lygrisse K, Hutzler LH, et al. Outcomes of same-day discharge after total hip arthroplasty in the medicare population. J Arthroplasty. 2020;35(3):638–642. doi:10.1016/j.arth.2019.09.040
19. Turcotte JJ, Menon N, Aja JM, et al. Preoperative predictors of patients requiring inpatient admission for total hip arthroplasty following removal from the medicare inpatient-only list. J Arthroplasty. 2020;35(8):2109–2113.e1. doi:10.1016/j.arth.2020.03.038
20. Rodriguez S, Lebrun DG, Shen TS, et al. Predicting total knee arthroplasty outpatient discharge: surgeons versus insurance companies. J Arthroplasty. 2022;37(8S):S766–S770. doi:10.1016/j.arth.2022.03.037
21. Buller LT, Hubbard TA, Ziemba-Davis M, et al. Safety of same and next day discharge following revision hip and knee arthroplasty using modern perioperative protocols. J Arthroplasty. 2021;36(1):30–36. doi:10.1016/j.arth.2020.07.062
22. Yang J, Olsen AS, Serino J, et al. Similar 90-day outcomes among inpatient and outpatient arthroplasties: a single-surgeon matched cohort analysis. Bone Joint J. 2021;103-B(7 Supple B):84–90. doi:10.1302/0301-620X.103B7.BJJ-2020-2341.R1
23. Toy PC, Fournier MN, Throckmorton TW, et al. Low rates of adverse events following ambulatory outpatient total hip arthroplasty at a free-standing surgery center. J Arthroplasty. 2018;33(1):46–50. doi:10.1016/j.arth.2017.08.026
24. Sershon RA, McDonald JF, Ho H, et al. Outpatient total hip arthroplasty performed at an ambulatory surgery center vs hospital outpatient setting: complications, revisions, and readmissions. J Arthroplasty. 2019;34(12):2861–2865. doi:10.1016/j.arth.2019.07.032
25. Shah RR, Cipparrone NE, Gordon AC, et al. Is it safe? Outpatient total joint arthroplasty with discharge to home at a freestanding ambulatory surgical center. Arthroplast Today. 2018;4(4):484–487.
26. Goh GS, D’Amore T, Courtney PM, et al. Total joint arthroplasty at a novel “hyperspecialty” ambulatory surgical center with extended care suites is as safe as inpatient arthroplasty. Arthroplast Today. 2022;16:242–246.e1. doi:10.1016/j.artd.2022.05.005
27. Kelly MP, Calkins TE, Culvern C, et al. Inpatient versus outpatient hip and knee arthroplasty: which has higher patient satisfaction? J Arthroplasty. 2018;33(11):3402–3406. doi:10.1016/j.arth.2018.07.025
28. Hardy A, Courgeon M, Pellei K, et al. Improved clinical outcomes of outpatient enhanced recovery hip and knee replacements in comparison to standard inpatient procedures. Orthop Traumatol Surg Res. 2022;108(6):103236. doi:10.1016/j.otsr.2022.103236
29. Hardy A, Gervais-Hupé J, Desmeules F, et al. Comparing ERAS-outpatient versus standard-inpatient hip and knee replacements: a mixed methods study. BMC Musculoskelet Disord. 2021;22(1):978. doi:10.1186/s12891-021-04847-9
30. Radtke LE, Blackburn BE, Kapron CR, et al. Outpatient total joint arthroplasty at a high-volume academic center: an analysis of failure to launch. J Arthroplasty. 2024;39(9S2):S134–S142. doi:10.1016/j.arth.2024.01.027
31. Keulen MHF, Asselberghs S, Boonen B, et al. Predictors of (un)successful same-day discharge in selected patients following outpatient hip and knee arthroplasty. J Arthroplasty. 2020;35(8):1986–1992. doi:10.1016/j.arth.2020.03.034
32. Ziemba-Davis M, Caccavallo P, Meneghini RM. Outpatient joint arthroplasty-patient selection: update on the outpatient arthroplasty risk assessment score. J Arthroplasty. 2019;34(7S):S40–S43. doi:10.1016/j.arth.2019.01.007
33. Turcotte JJ, Menon N, Kelly ME, et al. Preoperative predictors of same-day discharge after total knee arthroplasty. Arthroplast Today. 2021;7:182–187. doi:10.1016/j.artd.2020.12.006
34. Connolly P, Thomas J, Bieganowski T, et al. Outpatient vs. inpatient designation in total hip arthroplasty: can we predict who will require hospitalization? Arch Orthop Trauma Surg. 2024;144(8):3851–3856. doi:10.1007/s00402-024-05502-3
35. Nelson CL, Sheth NP, Higuera Rueda CA, et al. Impact of chronic opioid use on postoperative mobility recovery and patient-reported outcomes: a propensity-matched study. J Arthroplasty. 2024;39(8S1):S148–S153. doi:10.1016/j.arth.2024.02.032
36. Gong MF, McElroy MJ, Li WT, et al. Reasons and risk factors for failed same-day discharge after total joint arthroplasty. J Arthroplasty. 2024;39(6):1468–1473. doi:10.1016/j.arth.2023.11.032
37. Bovonratwet P, Chen AZ, Shen TS, et al. What are the reasons and risk factors for 30-day readmission after outpatient total hip arthroplasty? J Arthroplasty. 2020;36(7S):S258–S263.e1. doi:10.1016/j.arth.2020.10.011
38. Van Horne A, Van Horne J. Patient-optimizing enhanced recovery pathways for total knee and hip arthroplasty in medicare patients. Arthroplast Today. 2019;5(4):497–502. doi:10.1016/j.artd.2019.08.008
39. Adachi RN, Wong KK, Buchner BR, et al. Tempering expectations for outpatient total knee arthroplasty for patients over 70. J Arthroplasty. 2022;37(4):704–708. doi:10.1016/j.arth.2022.01.004
40. Gazendam AM, Tushinski D, Patel M, et al. Causes and predictors of failed same-day home discharge following primary hip and knee total joint arthroplasty: a Canadian perspective. Hip Int. 2023;33(4):576–582. doi:10.1177/11207000221111101
41. Kurkis GM, Dennis DA, Johnson RM, et al. Incidence and risk factors of orthostasis after primary Hip and knee arthroplasty. J Arthroplasty. 2022;37(6S):S70–S75. doi:10.1016/j.arth.2022.01.035
42. Oosting E, Kapitein PJC, de Vries SV, et al. Predicting short stay total hip arthroplasty by use of the timed up and go-test. BMC Musculoskelet Disord. 2021;22(1):361. doi:10.1186/s12891-021-04240-6
43. Turcotte JJ, Kelly ME, Fenn AB, et al. The role of the lower extremity functional scale in predicting surgical outcomes for total joint arthroplasty patients. Arthroplasty. 2022;4(1):3. doi:10.1186/s42836-021-00106-3
44. Long G, Chao C, Ming-Sheng T, et al. Low grip strength associated with clinical outcomes after total hip arthroplasty—a prospective case-control study. Orthop Surg. 2021;13(5):1488–1495. doi:10.1111/os.13007
45. Selakovic I, Dubljanin-Raspopovic E, Markovic-Denic L, et al. Can early assessment of hand grip strength in older hip fracture patients predict functional outcome? PLoS One. 2019;14(8):e0213223. doi:10.1371/journal.pone.0213223
46. Young S, Osman B, Shapiro FE. Safety considerations with the current ambulatory trends: more complicated procedures and more complicated patients. Korean J Anesthesiol. 2023;76(5):400–412. doi:10.4097/kja.23078
47. Rajan N, Rosero EB, Joshi GP. Patient selection for adult ambulatory surgery: a narrative review. Anesth Analg. 2021;133(6):1415–1430. doi:10.1213/ANE.0000000000005605
48. Sontag-Milobsky IL, Selph TJ, Madhan A, et al. Caring for the caregiver: caregiver preparation and stress following total joint arthroplasty. J Arthroplasty. 2025;S0883-5403(25).
49. Page BM, Urbach DR, Wolfstadt JI, et al. Impact of outpatient total hip or knee replacement on informal caregivers at home: a scoping review. Can J Surg. 2023;66(2):E150–E155. doi:10.1503/cjs.010022
50. Kim AG, Sanghvi P, Rizk AA, et al. Resilience as a psychiatric factor affecting outcomes after total joint arthroplasty: a systematic review. Arthroplasty. 2024;6(1):16. doi:10.1186/s42836-024-00240-8
51. Falvey JR, Bade MJ, Hogan C, et al. Preoperative activities of daily living dependency is associated with higher 30-day readmission risk for older adults after total joint arthroplasty. Clin Orthop Relat Res. 2020;478(2):231–237. doi:10.1097/CORR.0000000000001040
52. Shen TS, Rodriguez S, LeBrun DG, et al. Reasons and risk factors for failed same-day discharge after primary total knee arthroplasty. J Arthroplasty. 2023;38(4):668–672. doi:10.1016/j.arth.2022.10.044
53. Neuman MD, Feng R, Carson JL, et al. Spinal anesthesia or general anesthesia for hip surgery in older adults. N Engl J Med. 2021;385(22):2025–2035. doi:10.1056/NEJMoa2113514
54. Deckard ER, Meneghini RM. The “outpatient arthroplasty risk assessment” score for same day outpatient primary total joint arthroplasty: a multicenter study. J Arthroplasty. 2025;40(11):2859–2865. doi:10.1016/j.arth.2025.05.048
55. Buller LT, Deckard ER, Meneghini RM, et al. The predictability of the outpatient arthroplasty risk assessment score on clinical outcomes following revision total joint arthroplasty: a preliminary registry analysis. J Arthroplasty. 2025;40(9S1):S344–S349. doi:10.1016/j.arth.2025.04.093
56. Moore MG, Brigati DP, Crijns TJ, et al. Enhanced selection of candidates for same-day and outpatient total knee arthroplasty. J Arthroplasty. 2020;35(3):628–632. doi:10.1016/j.arth.2019.09.050
57. Oeding JF, Bosco JA, Carmody M, et al. RAPT scores predict inpatient versus outpatient status and readmission rates after IPO changes for total joint arthroplasty. J Arthroplasty. 2022;37(11):2140–2148. doi:10.1016/j.arth.2022.05.037
58. Lopez CD, Ding J, Trofa DP, et al. Machine learning model developed to aid in patient selection for outpatient total joint arthroplasty. Arthroplast Today. 2022;13:13–23. doi:10.1016/j.artd.2021.11.001
59. Kugelman DN, Teo G, Huang S, et al. A novel machine learning predictive tool assessing outpatient or inpatient designation for medicare patients undergoing total hip arthroplasty. Arthroplast Today. 2021;8:194–199. doi:10.1016/j.artd.2021.03.001
60. Mast NH, Oeste CL, Hens D, et al. Assessing total hip arthroplasty outcomes and generating an orthopedic research outcome database via a natural language processing pipeline. JMIR Med Inform. 2025;13:e64705. doi:10.2196/64705
61. Keulen MHF, Asselberghs S, Bemelmans YFL, et al. Reasons for unsuccessful same-day discharge following outpatient Hip and knee arthroplasty: 5½ years’ experience. J Arthroplasty. 2020;35(9):2327–2334.e1. doi:10.1016/j.arth.2020.04.064
62. Fraser JF, Danoff JR, Manrique J, et al. Identifying reasons for failed same-day discharge following primary total Hip arthroplasty. J Arthroplasty. 2018;33(12):3624–3628. doi:10.1016/j.arth.2018.08.003
63. Changjun C, Jingkun L, Yun Y, et al. Enhanced recovery after total joint arthroplasty: a contemporary systematic review. Orthop Surg. 2023;15(5):1228–1240. doi:10.1111/os.13710
64. Ripollés-Melchor J, Abad-Motos A, Díez-Remesal Y, et al. Association between use of enhanced recovery after surgery protocol and postoperative complications in total hip and knee arthroplasty in the POWER2 study. JAMA Surg. 2020;155(4):e196024. doi:10.1001/jamasurg.2019.6024
65. van Eck CF, Toor A, Banffy MB, et al. Web-based education prior to outpatient orthopaedic surgery enhances early patient satisfaction scores. Orthop J Sports Med. 2018;6(1):2325967117751418. doi:10.1177/2325967117751418
66. Camillieri S, Anonymous. Does participation in virtual or in-person preoperative education relate to reduced length of stay after total joint arthroplasty? HSS J. 2023;20(1):83–89. doi:10.1177/15563316231208454
67. Greenberg JA, Zwiep TM, Sadek J, et al. Clinical practice guideline: evidence, recommendations and algorithm for the preoperative optimization of anemia, hyperglycemia and smoking. Can J Surg. 2021;64(5):E491–E509. doi:10.1503/cjs.011519
68. Li S, Si H, Zhang S, et al. Does diabetes mellitus impair the clinical results of total knee arthroplasty under enhanced recovery after surgery? J Orthop Surg Res. 2023;18(1):490. doi:10.1186/s13018-023-03982-4
69. MacMahon A, Rao SS, Chaudhry YP, et al. Preoperative patient optimization in total joint arthroplasty—the paradigm shift from preoperative clearance: a narrative review. HSS J. 2022;18(3):418–427. doi:10.1177/15563316211030923
70. Cook MJ, Lunt M, Board T, et al. The impact of frailty on short-term mortality following primary total Hip and knee arthroplasty due to osteoarthritis. Age Ageing. 2022;51(6):afac118. doi:10.1093/ageing/afac118
71. Gianotti L, Biffi R, Sandini M, et al. Preoperative oral carbohydrate load versus placebo in major elective abdominal surgery (PROCY). Ann Surg. 2018;267(4):623–630. doi:10.1097/SLA.0000000000002325
72. Suh S, Hetzel E, Alter-Troilo K, et al. The influence of preoperative carbohydrate loading on postoperative outcomes in bariatric surgery patients. Surg Obes Relat Dis. 2021;17(8):1480–1488. doi:10.1016/j.soard.2021.04.014
73. Rajan S, Rahman AA, Kumar L. Preoperative oral carbohydrate loading: effects on intraoperative blood glucose levels, post-operative nausea and vomiting. J Anaesthesiol Clin Pharmacol. 2021;37(4):622–627. doi:10.4103/joacp.JOACP_382_19
74. Wang M, Meng L, Ma X, et al. Effect of warmed ropivacaine versus room temperature ropivacaine administered spinal anesthesia on recovery of lower limb muscle strength following total knee or Hip replacement. BMC Anesthesiol. 2025;25(1):409. doi:10.1186/s12871-025-03294-6
75. Contino V, Abrams JH, Arumugam S, et al. Spinal anesthesia using ropivacaine leads to earlier ambulation after total hip arthroplasty. Orthopedics. 2021;44(3):e343–e346. doi:10.3928/01477447-20210414-04
76. Wyles CC, Pagnano MW, Trousdale RT, et al. More predictable return of motor function with mepivacaine versus bupivacaine spinal anesthetic in total hip and total knee arthroplasty. J Bone Joint Surg Am. 2020;102(18):1609–1615. doi:10.2106/JBJS.20.00231
77. Schwenk ES, Kasper VP, Smoker JD, et al. Mepivacaine versus bupivacaine spinal anesthesia for early postoperative ambulation. Anesthesiology. 2020;133(4):801–811. doi:10.1097/ALN.0000000000003480
78. Calkins TE, McClatchy SG, Rider CM, et al. Mepivacaine vs bupivacaine spinal anesthesia in total hip arthroplasty at an ambulatory surgery center. J Arthroplasty. 2021;36(11):3676–3680. doi:10.1016/j.arth.2021.07.014
79. Gilreath N, Liu J, Daher M, et al. Spinal anesthesia in same-day discharge total hip arthroplasty: chloroprocaine versus mepivacaine. Hip Pelvis. 2025;37(4):262–268. doi:10.5371/hp.2025.37.4.262
80. Anger M, Valovska T, Beloeil H, et al. PROSPECT guideline for total hip arthroplasty: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021;76(8):1082–1097. doi:10.1111/anae.15498
81. Lex JR, Edwards TC, Packer TW, et al. Perioperative systemic dexamethasone reduces length of stay in total joint arthroplasty: a systematic review and meta-analysis. J Arthroplasty. 2020;36(3):1168–1186. doi:10.1016/j.arth.2020.10.010
82. Verret M, Lauzier F, Zarychanski R, et al. Perioperative use of gabapentinoids for the management of postoperative acute pain: a systematic review and meta-analysis. Anesthesiology. 2020;133(2):265–279. doi:10.1097/ALN.0000000000003428
83. Lin DY, Morrison C, Brown B, et al. Pericapsular nerve group (PENG) block provides improved short-term analgesia compared with the femoral nerve block in hip fracture surgery. Reg Anesth Pain Med. 2021;46(5):398–403. doi:10.1136/rapm-2020-102315
84. Remily EA, Hochstein SR, Wilkie WA, et al. The pericapsular nerve group block: a step towards outpatient total hip arthroplasty? Hip Int. 2020;32(3):318–325. doi:10.1177/1120700020978211
85. Xu L, Leng JC, Elsharkawy H, et al. Replacement of fascia iliaca catheters with continuous erector spinae plane blocks within a clinical pathway facilitates early ambulation after total hip arthroplasty. Pain Med. 2020;21(10):2423–2429. doi:10.1093/pm/pnaa243
86. Blackwell RE, Kushelev M, Norton J, et al. A comparative analysis of the quadratus lumborum block versus femoral nerve and fascia iliaca blocks in hip arthroscopy. Arthrosc Sports Med Rehabil. 2021;3(1):e7–e13. doi:10.1016/j.asmr.2020.08.002
87. Kikuchi M, Mihara T, Mizuno Y, et al. Anterior quadratus lumborum block for postoperative recovery after total hip arthroplasty: a study protocol for a single-center, double-blind, randomized controlled trial. Trials. 2020;21(1):142. doi:10.1186/s13063-020-4090-0
88. Thompson J, Long M, Rogers E, et al. Fascia iliaca block decreases hip fracture postoperative opioid consumption. J Orthop Trauma. 2020;34(1):49–54. doi:10.1097/BOT.0000000000001634
89. Wang Q, Yang Y, Yang Z, et al. Analgesic effects of ultrasound-guided iliohypogastric/ilioinguinal nerve block combined with lateral femoral cutaneous nerve block in total hip arthroplasty via direct anterior approach: a Retrospective Cohort Study. Orthop Surg. 2021;13(3):920–931. doi:10.1111/os.12795
90. Fillingham YA, Ramkumar DB, Jevsevar DS, et al. The efficacy of tranexamic acid in total Hip arthroplasty: a network meta-analysis. J Arthroplasty. 2018;33(10):3083–3089.e4. doi:10.1016/j.arth.2018.06.023
91. Yang YZ, Cheng QH, Zhang AR, et al. Efficacy and safety of single- and double-dose intravenous tranexamic acid in Hip and knee arthroplasty: a systematic review and meta-analysis. J Orthop Surg Res. 2023;18(1):593. doi:10.1186/s13018-023-03929-9
92. Juraj M, Jaroslav V, Gažová A, et al. Evaluation of efficacy and safety of systemic and topical intra-articular administration of tranexamic acid in primary unilateral total hip arthroplasty. Medicine. 2021;100(26):e26565. doi:10.1097/MD.0000000000026565
93. Poeran J, Chan JJ, Zubizarreta N, et al. Safety of tranexamic acid in hip and knee arthroplasty in high-risk patients. Anesthesiology. 2021;135(1):57–68. doi:10.1097/ALN.0000000000003772
94. Pan P, Song K, Yao Y, et al. The impact of intraoperative hypothermia on blood loss and allogenic blood transfusion in total knee and hip arthroplasty. Biomed Res Int. 2020;2020(1):1096743. doi:10.1155/2020/1096743
95. Ackermann W, Fan Q, Parekh AJ, et al. Forced-air warming and resistive heating devices: updated perspectives on safety and surgical site infections. Front Surg. 2018;5:64. doi:10.3389/fsurg.2018.00064
96. Roumeliotis L, Graham NM. Barbed suture and glue in skin closure during lower limb arthroplasty: reduced delayed discharge due to wound exudate. J Wound Care. 2019;28(11):784–789. doi:10.12968/jowc.2019.28.11.784
97. Rui M, Zheng X, Sun SS, et al. A prospective randomised comparison of 2 skin closure techniques in primary total hip arthroplasty surgery. Hip Int. 2018;28(1):101–105. doi:10.5301/hipint.5000534
98. Ripollés-Melchor J, Aldecoa CS, Fernández-García R, et al. Early mobilization after total hip or knee arthroplasty: a substudy of the POWER.2 study. Braz J Anesthesiol. 2023;73(1):54–71. doi:10.1016/j.bjane.2021.05.008
99. Frassanito L, Vergari A, Nestorini R, et al. Enhanced recovery after surgery (ERAS) in hip and knee replacement surgery. Musculoskelet Surg. 2020;104(1):87–92. doi:10.1007/s12306-019-00603-4
100. Morrell AT, Layon DR, Scott MJ, et al. Enhanced recovery after primary total hip and knee arthroplasty: a systematic review. J Bone Joint Surg Am. 2021;103(20):1938–1947. doi:10.2106/JBJS.20.02169
101. Efford CM, Samuel D. Does rapid mobilisation as part of an enhanced recovery pathway improve length of stay, return to function and patient experience post primary total hip replacement? Disabil Rehabil. 2022;45(25):4252–4258. doi:10.1080/09638288.2022.2148298
102. Chassery C, Atthar V, Marty P, et al. Opioid-free versus opioid-sparing anaesthesia in ambulatory total hip arthroplasty: a randomised controlled trial. Br J Anaesth. 2023;132(2):352–358. doi:10.1016/j.bja.2023.10.031
103. Zhang Q, Chen Y, Li Y, et al. Enhanced recovery after surgery in patients after hip and knee arthroplasty: a systematic review and meta-analysis. Postgrad Med J. 2024;100(1181):159–173. doi:10.1093/postmj/qgad125
104. Berg AR, Lakra A, Jennings EL, et al. Transdermal scopolamine as an adjunct to multimodal pain management in patients undergoing total joint arthroplasty. J Arthroplasty. 2019;34(7S):S159–S163. doi:10.1016/j.arth.2019.03.028
105. Jin Z, Gan TJ, Bergese SD. Prevention and treatment of postoperative nausea and vomiting: a review of current recommendations and emerging therapies. Ther Clin Risk Manag. 2020;16:1305–1317. doi:10.2147/TCRM.S256234
106. Wang Y, Yang Q, Lin J, et al. Risk factors of postoperative nausea and vomiting after total hip arthroplasty or total knee arthroplasty. Ann Transl Med. 2020;8(17):1088. doi:10.21037/atm-20-5486
107. Smits M, Lin S, Rahme J, et al. Blood pressure and early mobilization after total hip and knee replacements: a pilot study on the impact of midodrine hydrochloride. JBJS Open Access. 2019;4(2):e0048. doi:10.2106/JBJS.OA.18.00048
108. Cha YH, Lee YK, Won SH, et al. Urinary retention after total joint arthroplasty of hip and knee: systematic review. J Orthop Surg. 2020;28(1):2309499020905134. doi:10.1177/2309499020905134
109. Tanner J, Melen K. Preoperative hair removal to reduce surgical site infection. Cochrane Database Syst Rev. 2021;8(8):CD004122. doi:10.1002/14651858.CD004122.pub5
110. Xu B, Anderson DB, Park ES, et al. The influence of smoking and alcohol on bone healing: systematic review and meta-analysis. EClinicalMedicine. 2021;42:101179. doi:10.1016/j.eclinm.2021.101179
111. Siddiqi A, Forte SA, Docter S, et al. Perioperative antibiotic prophylaxis in total joint arthroplasty: a systematic review and meta-analysis. J Bone Joint Surg Am. 2019;101(9):828–842. doi:10.2106/JBJS.18.00990
112. Kheir MM, Tan TL, Kheir M, et al. Postoperative blood glucose levels predict infection after total joint arthroplasty. J Bone Joint Surg Am. 2018;100(16):1423–1431. doi:10.2106/JBJS.17.01316
113. Taneja A, El-Bakoury A, Khong H, et al. Association between allogeneic blood transfusion and wound infection after total hip or knee arthroplasty. J Bone Jt Infect. 2019;4(2):99–105. doi:10.7150/jbji.30636
114. DeRogatis MJ, Pellegrino AN, Wang N, et al. Enhancing recovery and reducing readmissions: the impact of remote monitoring on acute postoperative care in outpatient total joint arthroplasty. J Orthopaedics. 2024;58:111–116. doi:10.1016/j.jor.2024.06.028
115. Kuklinski D, Oschmann L, Pross C, et al. The use of digitally collected patient-reported outcome measures for newly operated patients with total knee and hip replacements to improve post-treatment recovery: study protocol for a randomized controlled trial. Trials. 2020;21(1):322. doi:10.1186/s13063-020-04252-y
116. Ehlig D, Schöner L, Geissler A, et al. PROM-based monitoring and alerts reduce post-surgery healthcare utilization of patients undergoing joint replacement: a secondary analysis of the Promoting Quality RCT. Eur J Health Econ. 2025;27(2):391–410. doi:10.1007/s10198-025-01810-6
117. Crawford DA, Lombardi AV, Berend KR, et al. Early outcomes of primary total hip arthroplasty with use of a smartphone-based care platform: a prospective randomized controlled trial. Bone Joint J. 2021;103-B(7 Supple B):91–97. doi:10.1302/0301-620X.103B7.BJJ-2020-2402.R1
118. Hamilton DF, Beard DJ, Barker KL, et al. Targeting rehabilitation to improve outcomes after total knee arthroplasty in patients at risk of poor outcomes: randomised controlled trial. BMJ. 2020;371:m3576. doi:10.1136/bmj.m3576
119. Graber J, Churchill L, Struessel T, et al. Expert consensus for the use of outpatient rehabilitation visits after total knee arthroplasty: a Delphi study. J Orthop Sports Phys Ther. 2023;53(9):566–574. doi:10.2519/jospt.2023.11840
120. Soffin EM, Gibbons MM, Wick EC, et al. Evidence review for the agency for healthcare research and quality safety program: focus on anesthesiology for hip fracture surgery. Anesth Analg. 2019;128(6):1107–1117. doi:10.1213/ANE.0000000000003925
121. Wainwright TW, Gill M, McDonald DA, et al. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: ERAS society recommendations. Acta Orthop. 2020;91(1):3–19. doi:10.1080/17453674.2019.1683790
122. Kumar V, Patel S, Baburaj V, et al. Does robotic-assisted surgery improve outcomes of total hip arthroplasty compared to manual technique? Postgrad Med J. 2023;99(1171):375–383. doi:10.1136/postgradmedj-2021-141135
123. Lu H, Sun H, Xiao Q, et al. Perioperative safety and efficacy of robot-assisted total hip arthroplasty in ERAS-managed patients: a pilot study. J Orthop Surg Res. 2023;18(1):696. doi:10.1186/s13018-023-04180-y
124. LeBrun DG, LaValva SM, Waddell BS, et al. No effect of surgical approach on discharge outcomes in outpatient total Hip arthroplasty. HSS J. 2021;18(3):338–343. doi:10.1177/15563316211055069
125. Ezzibdeh R, Korth MJS, Arora P, et al. Case-controlled analysis of the direct superior and mini-posterior approach for total Hip arthroplasty. Surg Technol Int. 2021;37:353–359.
126. Memtsoudis SG, Cozowicz C, Bekeris J, et al. Anaesthetic care of patients undergoing primary hip and knee arthroplasty: consensus recommendations from the ICAROS group. Br J Anaesth. 2019;123(3):269–287. doi:10.1016/j.bja.2019.05.042
127. Li WX, Luo RY, Chen C, et al. Effects of propofol, dexmedetomidine, and midazolam on postoperative cognitive dysfunction in elderly patients. Chin Med J. 2019;132(4):437–445. doi:10.1097/CM9.0000000000000098
128. Hickman SR, Mathieson KM, Bradford LM, et al. Randomized trial of oral versus intravenous Acetaminophen for postoperative pain control. Am J Health Syst Pharm. 2018;75(6):367–375. doi:10.2146/ajhp170064
129. Mittal A, Tamer P, Shah I, et al. Postoperative acute kidney injury with dual NSAID use after outpatient primary total joint arthroplasty. J Am Acad Orthop Surg. 2022;30(14):676–681. doi:10.5435/JAAOS-D-21-00934
130. Yayac M, Li WT, Ong AC, et al. The efficacy of liposomal bupivacaine over traditional local anesthetics in periarticular infiltration and regional anesthesia during total knee arthroplasty: a systematic review and meta-analysis. J Arthroplasty. 2019;34(9):2166–2183. doi:10.1016/j.arth.2019.04.046
131. Choi YM, Choi EJ, Ri HS, et al. The effect of dexmedetomidine and midazolam on combined spinal-epidural anesthesia in patients undergoing total knee arthroplasty. Anesth Pain Med. 2020;15(1):111–119. doi:10.17085/apm.2020.15.1.111
132. Lee C, Lee C, So C, et al. Impact of dexmedetomidine on tourniquet-induced systemic effects in total knee arthroplasty under spinal anesthesia. Biomed Res Int. 2020;2020:4208597. doi:10.1155/2020/4208597
133. Holland CT, Meyers AJ, Lum ZC, et al. Intravenous dexmedetomidine use in total hip arthroplasty may lead to elevated rates of hypotension. Cureus. 2023;15(8):e43768. doi:10.7759/cureus.43768
134. Zhang Q, Liu L, Sun W, et al. Are closed suction drains necessary for primary total knee arthroplasty? A systematic review and meta-analysis. Medicine. 2018;97(30):e11290. doi:10.1097/MD.0000000000011290
135. Pasqualotto S, Demey G, Michelet A, et al. Bipolar sealers do not improve blood loss or functional outcomes of primary total knee arthroplasty. J Knee Surg. 2020;33(1):62–66. doi:10.1055/s-0038-1676516
136. Grammatopoulos G, McIsaac DI, Beaulé PE, et al. Shape of the association between preoperative hemoglobin level and postoperative outcomes in patients undergoing primary arthroplasty. Can J Surg. 2022;65(1):E25–E37. doi:10.1503/cjs.020720
137. Memtsoudis SG, Mörwald EE, Fields K, et al. Changes in the augmentation index and postoperative orthostatic intolerance in orthopedic surgery. Can J Anaesth. 2018;65(9):1012–1028. doi:10.1007/s12630-018-1149-4
138. Sequeira SB, Kamalapathy PN, Burke JF, et al. The utilization of postoperative inpatient ultrasound for lower extremity deep venous thrombosis following total hip arthroplasty has decreased dramatically over the past decade. J Arthroplasty. 2022;37(10):2071–2075. doi:10.1016/j.arth.2022.05.007
139. Middleton A, Downer B, Haas A, et al. Functional status is associated with 30-day potentially preventable readmissions following skilled nursing facility discharge. J Am Med Dir Assoc. 2018;19(4):348–354.e4. doi:10.1016/j.jamda.2017.12.003
140. Middleton A, Graham JE, Ottenbacher KJ. Functional status is associated with 30-day potentially preventable hospital readmissions after inpatient rehabilitation. Arch Phys Med Rehabil. 2018;99(6):1067–1076. doi:10.1016/j.apmr.2017.05.001
141. Falvey J, Bade MJ, Forster JE, et al. Poor recovery of activities-of-daily-living function is associated with higher rates of postsurgical hospitalization after total joint arthroplasty. Phys Ther. 2021;101(11):pzab189. doi:10.1093/ptj/pzab189
142. Kang MJ, Kim BR, Lee SY, et al. Factors predictive of functional outcomes and quality of life in patients with fragility hip fracture. Medicine. 2023;102(7):e32909. doi:10.1097/MD.0000000000032909
143. Martinkovich SC, Trott GL, Garay M, et al. Patient characteristics and surgical start time affect length of stay following anterior total hip arthroplasty. J Arthroplasty. 2020;35(8):2114–2118. doi:10.1016/j.arth.2020.03.049
144. Garabedian M, Legler J, Benzouak T, Baskaran S, Mutch J, Albers A. Efficacy of lower-limb wearables to assess recovery following total Hip or knee arthroplasty: a systematic review and meta-analysis. J Arthroplasty. 2025;S0883-5403(25).
145. Wu KA, Dilbone ES, Kugelman DN, et al. The impact of total hip arthroplasty on daily ambulatory function: a prospective study. J Arthroplasty. 2025;40(9S1):S253–S258. doi:10.1016/j.arth.2025.04.089
146. Brown ML, Ezzet KA. Relaxed hip precautions do not increase early dislocation rate following total hip arthroplasty. J Am Acad Orthop Surg. 2020;28(10):e440–e447. doi:10.5435/JAAOS-D-19-00261
147. Fortier LM, Rockov ZA, Chen AF, et al. Activity recommendations after total hip and total knee arthroplasty. J Bone Joint Surg Am. 2021;103(5):446–455. doi:10.2106/JBJS.20.00983
148. Jacobs H, Seeber GH, Allers K, et al. Utilisation of outpatient physiotherapy in patients following total knee arthroplasty—a systematic review. BMC Musculoskelet Disord. 2021;22(1):711. doi:10.1186/s12891-021-04600-2
149. Wu C, McAdam A, Siverling S, et al. Factors associated with higher utilization of outpatient physical therapy for patients who have undergone primary total joint arthroplasty. HSS J. 2024;20(1):51–56. doi:10.1177/15563316231210556
150. Zogg CK, Falvey JR, Dimick JB, et al. Changes in discharge to rehabilitation: potential unintended consequences of medicare THA/TKA bundled payments. J Arthroplasty. 2019;34(6):1058–1065.e4. doi:10.1016/j.arth.2019.01.068
151. Doxey SA, Huyke-Hernández FA, Davidson S, et al. Patient-level value analysis in total hip arthroplasty: optimizing the value of care delivery. J Bone Joint Surg Am. 2024;106(24):2338–2346. doi:10.2106/JBJS.24.00130
152. Aloziem OU, Williams BA, Mikolic JM, et al. Assessing common content and responsiveness of the QoR-15 and the SF-8 in the context of recovery from regional anesthesia for joint replacement. Mil Med. 2023;188(11–12):e3469–e3476. doi:10.1093/milmed/usad191
153. Vendittoli PA, Pellei K, Desmeules F, et al. Enhanced recovery short-stay hip and knee joint replacement program improves patients outcomes while reducing hospital costs. Orthop Traumatol Surg Res. 2019;105(7):1237–1243. doi:10.1016/j.otsr.2019.08.013
154. Husted CE, Husted H, Ingelsrud LH, et al. Are functional outcomes and early pain affected by discharge on the day of surgery following total hip and knee arthroplasty? Acta Orthop. 2020;92(1):62–66. doi:10.1080/17453674.2020.1836322
155. Hafkamp FJ, de Vries J, Gosens T, et al. High pre-operative expectations precede both unfulfilled expectations and clinical improvement after total hip and total knee replacement. J Arthroplasty. 2020;35(7):1806–1812. doi:10.1016/j.arth.2020.02.061
156. Hashimoto S, Hatayama K, Terauchi M, et al. Preoperative hand-grip strength can be a predictor of stair ascent and descent ability after total knee arthroplasty in female patients. J Orthop Sci. 2020;25(1):167–172. doi:10.1016/j.jos.2019.03.003
157. Wylde V, Kunutsor SK, Lenguerrand E, et al. Is social support associated with patient-reported outcomes after joint replacement? A systematic review and meta-analysis. Lancet Rheumatol. 2019;1(3):e174–e186. doi:10.1016/S2665-9913(19)30050-5
158. Yates AJ, Kerr JM, Froimson MI, et al. The unintended impact of the removal of total knee arthroplasty from the center for medicare and medicaid services inpatient-only list. J Arthroplasty. 2018;33(12):3602–3606. doi:10.1016/j.arth.2018.09.043
159. Krueger CA, Kerr JM, Bolognesi MP, et al. The removal of total hip and total knee arthroplasty from the inpatient-only list increases the administrative burden of surgeons. J Arthroplasty. 2020;35(10):2772–2778. doi:10.1016/j.arth.2020.04.079
160. Yayac M, Schiller N, Austin MS, et al. 2020 John N. Insall Award: removal of total knee arthroplasty from the inpatient-only list adversely affects bundled payment programmes. Bone Joint J. 2020;102-B(6_Supple_A):19–23. doi:10.1302/0301-620X.102B6.BJJ-2019-1369
161. Iorio R, Barnes CL, Vitale MP, et al. Total knee replacement: the inpatient-only list and the two midnight rule. J Arthroplasty. 2020;35(6S):S28–S32. doi:10.1016/j.arth.2020.01.007
162. Rosinsky PJ, Go CC, Bheem R, et al. The cost-effectiveness of outpatient surgery for primary total hip arthroplasty in the United States. Hip Int. 2021;31(5):572–581. doi:10.1177/1120700020952776
163. Lynch JC, Yayac M, Krueger CA, et al. Amount of CMS reduction in facility reimbursement following removal of total hip arthroplasty from the inpatient-only list far exceeds reduction in actual care cost. J Arthroplasty. 2021;36(7):2276–2280. doi:10.1016/j.arth.2020.08.038
164. Carey K, Morgan JR, Lin MY, et al. Patient outcomes following total joint replacement surgery: a comparison of hospitals and ambulatory surgery centers. J Arthroplasty. 2020;35(1):7–11. doi:10.1016/j.arth.2019.08.041
165. Van Horne J, Van Horne A, Liao N, et al. Migration of hospital total hip and knee arthroplasty procedures to an ambulatory surgery center setting and postsurgical opioid use. Am Health Drug Benefits. 2022;15(1):21–29. doi:10.1097/MD.0000000000007190
166. Shafi S, Collinsworth AW, Copeland LA, et al. Association of opioid-related adverse drug events with clinical and cost outcomes among surgical patients. JAMA Surg. 2018;153(8):757–763. doi:10.1001/jamasurg.2018.1039
167. Kehlet H. Enhanced postoperative recovery: good from afar, but far from good? Anaesthesia. 2020;75(S1):e54–e61. doi:10.1111/anae.14860
168. Changjun C, Xin Z, Yue L, et al. Key elements of enhanced recovery after total joint arthroplasty: a reanalysis of the enhanced recovery after surgery guidelines. Orthop Surg. 2023;15(3):671–678. doi:10.1111/os.13623
169. Galbraith AS, McGloughlin E, Cashman J. Enhanced recovery protocols in total joint arthroplasty: a review of the literature and their implementation. Ir J Med Sci. 2018;187(1):97–109. doi:10.1007/s11845-017-1641-9
170. Białecka M, Jurewicz A, Machoy-Mokrzyńska A, et al. Effect of interleukin 6 −174G>C gene polymorphism on opioid requirements after total hip replacement. J Anesth. 2016;30(4):562–567. doi:10.1007/s00540-016-2167-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Pericapsular Nerve Group Block with Wound Infiltration vs Modified Supra-Inguinal Fascia Iliaca Block on Postoperative Analgesia in Adult Patients Undergoing Total Hip Arthroplasty – A Randomized Clinical Trial
Huang Y, Peng S, Wang J, Liu L, Dong CS
Journal of Pain Research 2025, 18:2679-2688
Published Date: 24 May 2025