Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Optimizing Drug Procurement Using ABC-VEN: A Narrative Review and Conceptual Framework
Authors Heryanto D ![]() , Amalia E
, Amalia E ![]() , Kautsar AP
, Kautsar AP ![]()
Received 25 April 2026
Accepted for publication 25 June 2026
Published 14 July 2026 Volume 2026:19 619681
DOI https://doi.org/10.2147/JMDH.S619681
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Dikky Heryanto,1 Eri Amalia,2 Angga Prawira Kautsar1,2
1Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, Indonesia; 2Department Pharmaceutics and Technology of Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, Indonesia
Correspondence: Angga Prawira Kautsar, Department Pharmaceutics and Technology of Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, Indonesia, Email [email protected]
Abstract: Drug procurement represents a substantial component of healthcare expenditure, particularly in low- and middle-income countries (LMICs). While ABC-VEN analysis remains important for balancing economic and clinical priorities, existing literature lacks critical evaluation of its cross-country adaptability and methodological rigor. This study aims to synthesize international evidence on ABC-VEN application within healthcare facilities to identify structural knowledge gaps and comparative findings. A structured narrative review was conducted using literature from PubMed, Scopus, Taylor & Francis and Google Scholar. To improve reporting transparency, study selection was mapped using a PRISMA 2020 framework. Studies included were those that applied the ABC-VEN method in hospitals and primary healthcare centers. This review also proposes a conceptual framework to explain how ABC-VEN supports procurement decision-making across different healthcare settings. The method also facilitates the identification of wasteful spending and ensures more stringent monitoring of critical drug categories. The synthesis of 19 included studies showed that Category I expenditures consistently consumed 71.69% to 90% of pharmaceutical budgets. However, the review revealed substantial heterogeneity in methodological execution, lack of reviewer transparency, and an absence of formal quality appraisal across the existing literature. While the ABC-VEN matrix offers a valuable baseline for resource allocation, its operational effectiveness is highly dependent on institutional capacity and geographic context. This review provides a novel conceptual framework that transitions ABC-VEN from a static classification model into a dynamic decision-support mechanism, emphasizing the need for standardized implementation to achieve sustainable medicine availability.
Keywords: drug procurement, ABC-VEN, drug expenditure, inventory management, healthcare services
Introduction
Drug procurement constitutes one of the most significant expenditures in healthcare facilities, particularly in low- and middle-income countries (LMICs), where it may absorb 40% to 50% of total hospital budgets.1,2 Even in high-income or upper-middle-income settings, inefficient procurement and lack of supply chain integration remain persistent challenges affecting healthcare quality and cost-efficiency.3 Inadequate forecasting, stockouts, overstocking, and expired medicines can increase operational costs and compromise the continuity of patient care.4,5 Excess inventory alone has been reported to account for up to 20%–40% of annual drug stock value, highlighting the need for effective inventory control and procurement planning strategies.6
To address these challenges, various inventory management techniques have been developed, including Always Better Control (ABC), Vital, Essential, Non-essential (VEN), Fast, Slow, Non-moving (FSN), High-Medium-Low cost (HML), and Seasonal and Off-seasonal (SOS).1,7 Among these methods, ABC and VEN are the most widely implemented in healthcare settings. However, each method has inherent limitations. ABC analysis prioritizes medicines based on expenditure but does not account for clinical importance. whereas VEN analysis emphasizes therapeutic criticality without considering financial implications.8,9 Consequently, neither approach alone provides a sufficiently balanced basis for procurement decision-making.10
The ABC-VEN matrix was developed to overcome these limitations by integrating economic and clinical considerations into a single prioritization framework.11 Previous studies have reported its application in hospitals, primary healthcare facilities, and specialized treatment centers, demonstrating benefits in expenditure control, inventory prioritization, and medicine availability.2,12,13 Nevertheless, the available evidence remains fragmented and largely restricted to single-facility evaluations or local procurement audits. In addition, substantial methodological variation exists in the classification of vital and essential medicines, which is often influenced by local formularies, epidemiological priorities, and institutional practices. These differences create inconsistencies in implementation and limit the comparability and transferability of findings across healthcare settings.
A comparative synthesis across countries is therefore needed to address several unresolved questions. Existing studies rarely examine how differences in healthcare infrastructure, procurement systems, resource availability, and policy environments influence the implementation and outcomes of ABC-VEN. As a result, it remains unclear whether the reported benefits primarily reflect the effectiveness of the ABC-VEN framework itself or the contextual characteristics of the healthcare systems in which it is applied. Identifying recurring implementation patterns, methodological differences, and operational challenges may provide valuable insights for healthcare managers and policymakers seeking to optimize pharmaceutical resource allocation.
Beyond summarizing existing evidence, this review aims to advance current knowledge by examining ABC-VEN from a broader decision-making perspective. To our knowledge, this is among the first reviews to comparatively synthesize international experiences while proposing a conceptual framework that positions ABC-VEN as a decision-support mechanism rather than merely an inventory classification tool. By integrating findings from diverse healthcare settings, this review aims to provide a more comprehensive understanding of how ABC-VEN can support procurement planning, strengthen inventory governance, and improve the efficient use of pharmaceutical resources.
Materials and Methods
This study employed a structured narrative review approach to synthesize international evidence on the application of the ABC-VEN method in drug procurement planning. To minimize selection bias and enhance reporting transparency, a systematic search and screening procedure was executed. A structured non-systematic narrative review was conducted using four primary health science databases: PubMed, Scopus, Taylor & Francis, and Google Scholar, with no restrictions on publication year. A comprehensive database search was conducted in August 2025 using the following keywords in the advanced search function: (“ABC-VEN” OR “ABC analysis” OR “VEN analysis”) AND “drug procurement” AND (“hospital drug procurement” OR “primary health center”) were used to focus the search on healthcare facilities. The American English spelling “health center” was selected as the operational standard for this paper. Reference lists of relevant articles were also examined to identify additional studies.
Review Process and Transparency
To ensure methodological rigor, the study screening and eligibility processes were conducted independently by two reviewers (DH and APK). Disagreements regarding article inclusion were resolved via consensus, with a third reviewer (EA) serving as a moderator when an agreement could not be reached initially.
Study Eligibility Criteria
Articles were included if they applied the ABC, VEN, or ABC-VEN method in drug procurement or inventory management within healthcare facilities, particularly hospitals or primary health centers. Studies were excluded if they examined private sector supply chains unrelated to public healthcare procurement and did not clearly describe the methodology or outcomes related to the ABC-VEN application. Inclusion criteria contain peer-reviewed journal articles published in English or Indonesian; study designs involving retrospective, cross-sectional, or observational data; settings restricted to public/private hospitals or public primary health centers; and clear operationalization of combined ABC-VEN matrix methodologies.
Exclusion Criteria is dissertations, book chapters, conference abstracts, studies focusing exclusively on private retail commercial supply chains unrelated to institutional public healthcare procurement, review article, or papers lacking defined expenditure outcomes.
Data Extraction and Analytical Synthesis
A total of 584 records were identified through database searching. After the removal of 16 duplicate records, 568 articles were screened based on titles and abstracts. Of these, 548 records were excluded for not meeting the eligibility criteria, leaving 20 articles for full-text assessment. Following full-text review, one article was excluded because it did not satisfy the inclusion criteria. Consequently, 19 studies met all eligibility criteria and were included in the final synthesis. The study selection process is summarized in the PRISMA flow diagram (Figure 1).
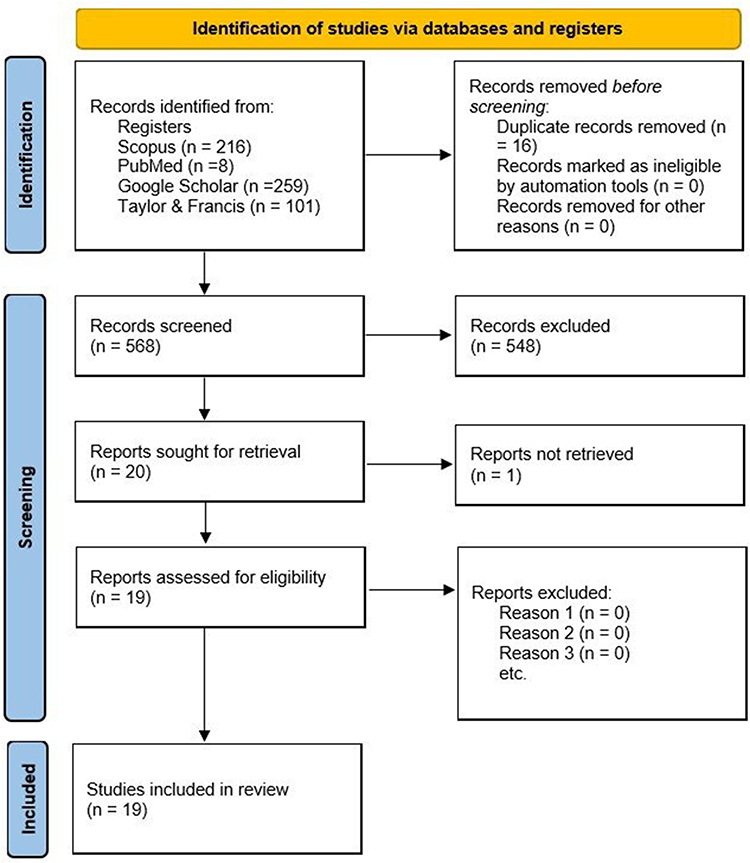 |
Figure 1 PRISMA flow diagram of the current study. |
A narrative synthesis was performed to describe the application and impact of the ABC-VEN method. Key findings from each included study were extracted, including healthcare setting, analysis period, country of origin, and reported annual drug expenditures (ADE) by category, as presented in the reviewed articles. These expenditures reflect the financial classification of drug items into categories I, II, and III, based on their placement in the ABC-VEN matrix. The synthesis aimed to compare implementation experiences across countries and highlight recurring patterns in procurement outcomes, budget efficiency, and inventory prioritization.
Results
A total of 19 eligible studies were included in the final synthesis after a multi-stage screening process mapped in the PRISMA-style flow framework (Figure 1). These studies applied the ABC, VEN, or ABC-VEN analysis methods in various healthcare settings across 11 countries, predominantly within LMICs. Table 1 summarizes the characteristics of the included studies, including authorship, country of study, study period, healthcare setting, study design, and the type of procurement analysis applied.
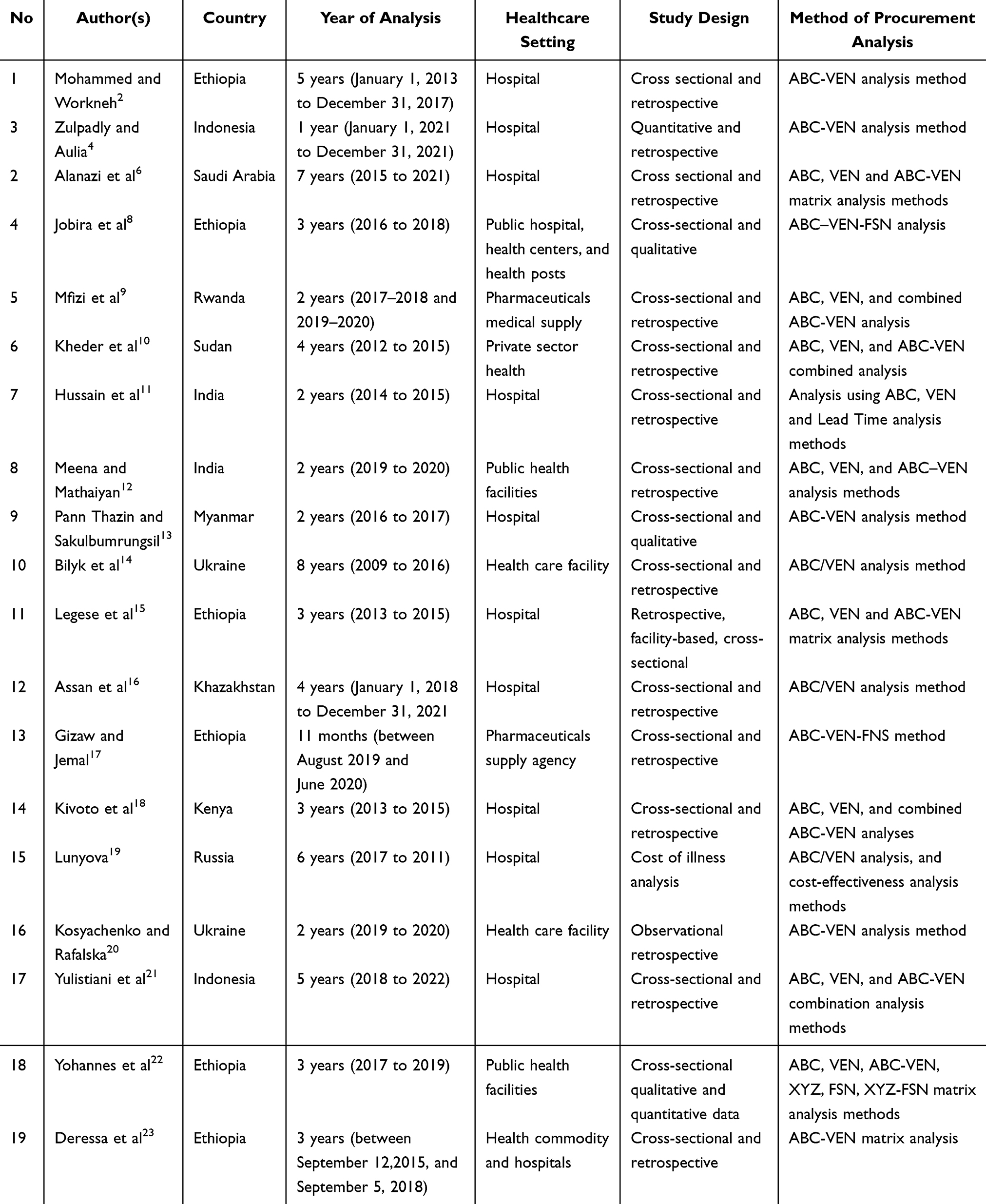 |
Table 1 Study Characteristics |
Most studies were conducted in public hospitals (eg., in Ethiopia, India, Kenya, and Indonesia), while a few included broader supply systems such as pharmaceutical supply agencies or national-level distributors. The majority employed retrospective or cross-sectional designs, using inventory data from periods ranging between one and eight years. While some studies used only the ABC-VEN matrix, others incorporated additional analyses such as FSN, often to strengthen prioritization and stock monitoring.
Comparative Synthesis of Budgetary Expenditures Across Contextual Settings
The synthesis of 19 articles shows that pharmaceutical expenditures have a structured variation based on the complexity of institutions and health policies of a region. Items in Category I (consisting of high-cost and clinically critical drugs comprising AV, AE, AN, BV, and CV) consistently absorb the majority of available funds, ranging from 71.65% to 91.60% of the total ADE. The proportion distribution across inter-cluster comparisons is illustrated in Figure 2. The in-depth comparison can be seen in Table 2, which stratifies Category I ADE, indicating that the driving factors behind the highly context-dependent figures are:
 |
Table 2 Stratification and Driving Factors of Category I Pharmaceutical Expenditures |
 |
Figure 2 Comparative visualization of Category I expenditure ranges across international healthcare settings. |
Cluster 1: Public Tertiary and Referral Systems (LMIC Context)
Healthcare systems in Sub-Saharan Africa and South Asia, which are classified within Cluster 1, exhibit exceptionally high Category I expenditures, ranging from 84.00% to 91.60%. This pattern occurs due to severe fiscal limitations, forcing these institutions to adopt a strict procurement stance by limiting the purchase of Class non-essential (N) items to prevent shortages and stockouts of vital medicines amid an unstable supply chain.2,11
Cluster 2: Decentralized and Primary Care Services
Community health centers and district polyclinics classified within Cluster 2 demonstrate Category I expenditures ranging from 74.30% to 83.50%. Lower and more variable budget utilization is heavily influenced by local epidemiological shifts and seasonal infectious disease spikes, which can complicate procurement management in primary care facilities due to a lack of tools for automated planning and fluctuations in community demand.2,14,24
Cluster 3: Specialized and Mixed Networks
Specialized oncology centers classified as (Cluster 3) show the lowest relative percentage of Category I (71.65%–78.50%). In context, this does not indicate lower spending, but rather reflects the extraordinarily high baseline cost of complex therapy regimens (eg., targeted chemotherapy and specialized biological drugs), which mathematically flatten the percentage variance between ABC-VEN classes across the remainder of the formulary.19,20
Structured Evaluation of Strengths and Limitations of the ABC-VEN Matrix
The synthesized findings demonstrate the robust utility and operational limitations of this integrated ABC-VEN matrix in various international settings. The primary strength of this matrix lies in its consistent ability to safeguard in maintaining high-cost, high-volume, and clinically critical inventories, thereby preventing budgetary inefficiencies in non-combined ABC or VEN analyses. During supply chain disruptions (such as post-pandemic turbulence), this method serves as a quick administrative instrument for budget reallocation.
A primary limitation of this method remains the unresolved challenge of high subjectivity in determining the boundary between Vital and Essential medicines across several countries. Moreover, since data collection in 80% of the reviewed studies remains retrospective, this method operates as a post-event audit (ex-post audit) rather than a prospective forecasting instrument, which significantly limits the capacity to mitigate real-time stockouts.
Table 3 presents a synthesis of findings from these studies, with a particular focus on reported ADEs classified by ABC-VEN categories I, II, and III. A consistent pattern emerged across countries: Category I drugs, which include vital and high-cost or high-priority items (eg., AV, AE, AN), accounted for the largest share of drug budgets, typically ranging from 74% to 90% of total expenditures. For example, studies in Ethiopia,2 Rwanda,9 and Myanmar13 reported over 84% of annual expenditures allocated to Category I items. In contrast, Category II drugs (eg., BE, CE, BN) represented between 9% and 25%, while Category III drugs (eg., CN), considered non-essential and low-priority, typically consumed less than 3% of the total drug budget. These proportions are visualized in Figure 3, which summarizes the average distribution of annual drug expenditure across the three ABC-VEN categories based on the reviewed studies.
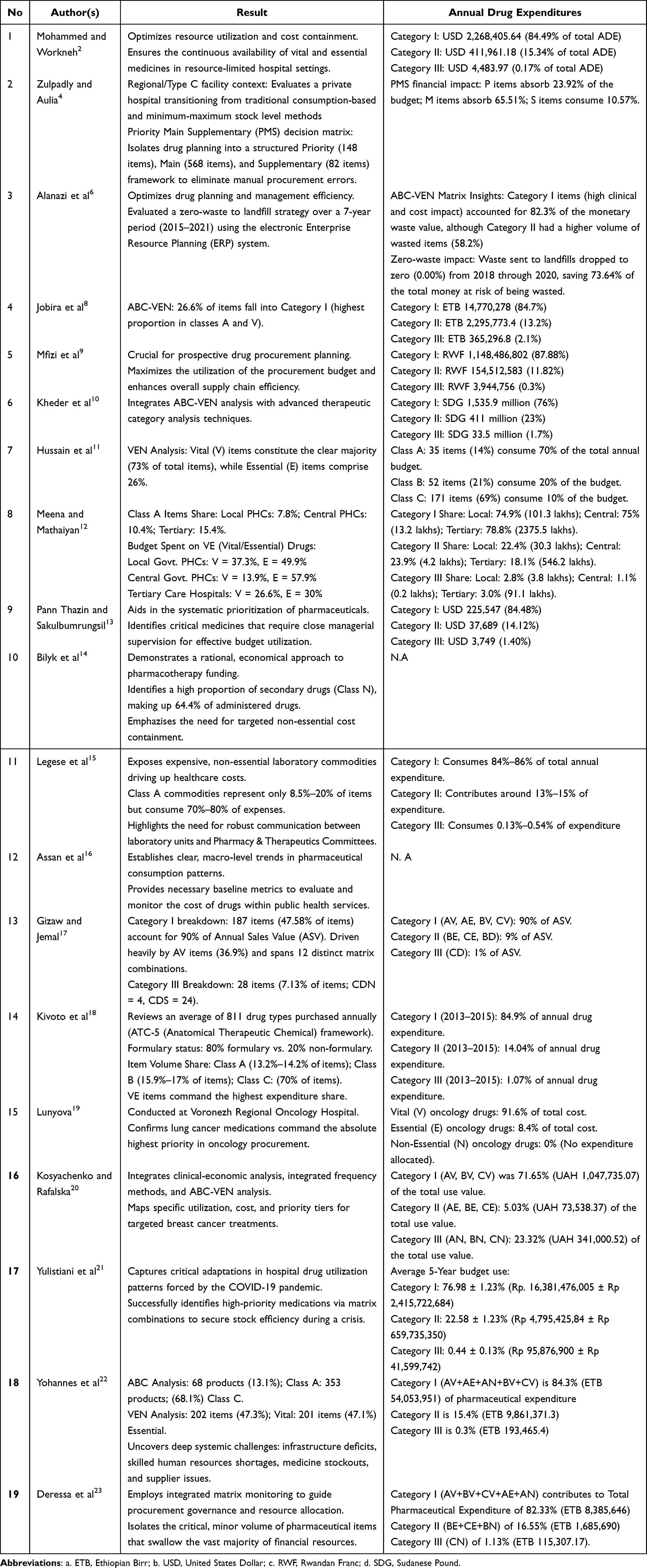 |
Table 3 Review of ABC-VEN Method in Different Countries |
 |
Figure 3 Average distribution of annual drug expenditure by ABC-VEN category (I, II, III) based on synthesis of 19 reviewed studies across LMIC healthcare settings. |
These findings highlight a common trend across LMICs. A small proportion of critical drug items consumes the majority of financial resources, underscoring the need for careful prioritization and strict monitoring of Category I drugs. Moreover, the ABC-VEN method was also effective in identifying excess spending on non-essential drugs and in guiding inventory streamlining. Several studies (eg.,)4,6,21 also reported reductions in expired or wasteful stock following the adoption of ABC-VEN-informed planning.
Overall, the ABC-VEN matrix provided a structured framework for classifying and prioritizing drug items based on both economic value and clinical necessity. Its implementation across diverse settings demonstrated consistency in expenditure patterns, supporting its applicability as a decision-making tool in drug procurement planning in resource-constrained environments.
Conceptual Framework for ABC-VEN-Based Drug Procurement Decision-Making
To provide a more comprehensive understanding of how the ABC-VEN method contributes to drug procurement efficiency, this review proposes a conceptual framework that positions ABC-VEN as a decision-support tool within healthcare supply systems. The framework begins with key inputs, including drug inventory data, budget constraints, disease burden, and procurement policies. These inputs are processed through two complementary classification approaches: ABC analysis, which prioritizes drugs based on economic value, and VEN analysis, which classifies drugs according to their clinical importance.
The integration of these two approaches generates the ABC-VEN matrix, which categorizes drugs into priority groups (Category I, II, and III), enabling targeted monitoring and resource allocation. The resulting outputs support procurement decision-making by identifying high-priority drugs that require strict control and continuous availability. Ultimately, this process leads to improved outcomes, including more efficient budget utilization, reduced inventory waste, and enhanced availability of essential medicines.
Importantly, this framework highlights that the effectiveness of the ABC-VEN method lies not only in its classification function but also in its role as a structured mechanism for aligning financial and clinical priorities within drug supply systems, particularly in resource-constrained settings.
ABC Method
The ABC method is implemented by calculating the estimated budget amount by multiplying the number of goods by their price value, then sorting the results in descending order.25,26 The next step is to calculate the cumulative value of the cost allocated to each item. The ABC analysis separates inventory items into three groups as follows:10,27
- Class A represents the item with the highest annual budget use (70–80% of the total value of inventory expenditure).
- Class B consists of drugs with a moderate utilization value (15–20% of the total value of inventory expenditure).
- Class C consists of drugs with the lowest frequency of consumption value (5–10% of the total inventory expenditure value).
The limitation of the ABC method analysis is that it relies solely on the range of budget values and the consumption levels of goods.28 This means that items with low but essential use values and volumes, which can save lives, might be considered unimportant in health centers or hospitals because they are not categorized as A.29,30 Therefore, additional parameters are necessary. In this case, another parameter used is the level of criticality of the item.
VEN Method
The VEN analysis is categorized based on the critical level of the item or drug for the patient into three categories: vital, essential, and non-essential.1
- The vital (V) category is given to items that have the potential to save lives or are of great importance in healthcare as well as the prevention of death or disability of patients, in addition, it can also be given to items that have the side effects of withdrawal syndrome so the item should always be available.
- The essential (E) category is given to items that are effective against less severe but still significant disease. Where this item is not very important to provide basic health care and can be replaced in a certain way.
- The non-essential (N) category is given to items that are effective for mild illness and have low therapeutic benefit.
The weakness of the VEN analysis is that essential medicines will not be prioritized for purchase even if they move quickly.7 Shortages or unavailability of low-cost but indispensable items can have a significant impact on hospital services.31
Analysis of ABC-VEN Matrix
At the planning stage, analysis is needed to ensure the availability of medicines and budget efficiency. The combination of ABC-VEN analysis is used to overcome weaknesses in ABC and VEN analysis in planning, namely by grouping drugs according to their importance and value of use. Drug control using the ABC-VEN method can improve drug management to be more effective and efficient.24 This analysis was formulated by conducting a cross-combination of ABC and VEN analysis, which will be divided into three new groups. The first letter in the subcategory indicates its position in the ABC analysis, while the second letter indicates its position in the VEN analysis.8
- Category I consists of all vital commodities and of high value (AV, BV, CV, AE, AN). These items are essential for hospitals, both financially and in terms of health services. Products in this category require close supervision and a high level of vigilance.
- Category II includes the remaining items from groups E and B (BE, CE, BN), which are essential and of lesser value compared to Category I. Stock control of items in this category should be carried out periodically.
- Category III consists of non-essential groups and items with the lowest value (CN).
Although some existing literature shows that the majority of ABC-VEN matrix usage is as a method for conducting logistics audits including in hospitals and medical supplies,9,23 this research extends the existing literature by conceptualizing the ABC-VEN method, which can be explicitly integrated into decision support mechanisms in procurement planning.
Discussion
The most consistent finding across the reviewed studies was the dominant contribution of Category I medicines to total drug expenditures, regardless of healthcare setting or country context. This pattern suggests that drug procurement systems consistently allocate the largest proportion of resources to medicines that are both clinically critical and economically significant. The recurrence of this finding across diverse healthcare environments supports the proposed conceptual framework, in which the ABC-VEN matrix functions as a decision-support mechanism that integrates financial and clinical priorities. Rather than serving solely as an inventory classification tool, ABC-VEN provides a structured approach for identifying medicines that require the highest level of procurement attention and resource allocation.
The predominance of Category I medicines observed across studies reflects the concentration of healthcare expenditures on drugs that are both clinically important and financially demanding. In several settings, Category I items accounted for more than 80% of total pharmaceutical expenditures despite representing a relatively small proportion of inventory items. This finding highlights the importance of prioritizing procurement oversight and inventory control for a limited number of high-impact medicines, as inefficiencies within this category may have substantial clinical and financial consequences.18,19
The consistent concentration of expenditure within Category I also illustrates the value of integrating economic and clinical dimensions in procurement decision-making. Standalone ABC analysis may overlook low-cost but clinically essential medicines, whereas VEN classification does not explicitly account for budgetary constraints. By combining these approaches, the ABC-VEN matrix provides a structured mechanism for balancing resource efficiency with therapeutic priorities, thereby supporting more rational procurement planning and resource allocation.11,31
Despite the consistency of expenditure patterns, the review identified substantial methodological variation across studies that may limit the comparability of findings. One of the most prominent challenges concerns the classification of medicines within the VEN framework. In many settings, the distinction between Vital and Essential medicines remains dependent on local formularies, epidemiological priorities, and expert judgement rather than standardized criteria. As a result, similar medicines may be categorized differently across healthcare systems, creating challenges for cross-country comparisons and limiting the transferability of procurement recommendations.2,11
The relative importance of each component within this framework may vary between LMIC and non-LMIC settings, where differences in resource availability, procurement systems, and policy environments influence the implementation and impact of ABC-VEN-based decision-making. In LMIC settings, the reliance on ABC-VEN is primarily driven by constrained financial resources and the need to ensure the availability of essential medicines, whereas in non-LMIC settings, the method may function more as an optimization tool within established procurement and supply chain systems.2,12,32 These findings underscore the crucial role of prioritization tools, such as the ABC-VEN matrix, in identifying the most impactful drug categories and informing procurement decisions accordingly. In addition, the findings also suggest that procurement policies should integrate both expenditure-based and clinical-priority criteria to ensure efficient allocation of limited pharmaceutical resources across diverse healthcare settings.
Beyond classification, the ABC-VEN method also facilitates decision-making for specific clinical areas. In oncology settings, the matrix helped prioritize high-cost chemotherapy drugs with a high therapeutic impact.19,20 Additionally, several studies have observed reductions in expired or wasted inventory following the implementation of ABC-VEN-guided planning, supporting its value in optimizing stock levels and minimizing waste.6,21 These findings indicate that the utility of ABC-VEN extends beyond expenditure monitoring and may support service-specific procurement optimization.
The practical value of ABC-VEN becomes particularly evident during periods of supply chain disruption. During the COVID-19 pandemic, several LMIC countries experienced shortages of medicines caused by poor inventory management in some hospitals.33 The method’s relevance also extends to dynamic contexts. ABC-VEN was utilized to evaluate shifts in drug use patterns following the COVID-19 pandemic, demonstrating its effectiveness in capturing evolving demand and informing responsive procurement strategies.21 Furthermore, by combining ABC-VEN with other approaches such as FSN, healthcare facilities can further enhance procurement accuracy by incorporating stock movement and consumption variability into planning.17,22
Despite its methodological simplicity, the implementation of the ABC-VEN matrix in routine procurement workflows continues to face several operational challenges, particularly in resource-constrained settings. In most public health centers, the inventory recording process is still managed manually without using an automated recording system, through unintegrated spreadsheets.2,11
More than 80% of the studies used for data analysis were based on retrospective annual expenditures.2,15,22 Consequently, while this historical approach is useful for routine planning, temporary operational mismatches may occur when facing sudden events, seasonal demand spikes, or emerging pandemics.21,33 Beyond methodological constraints, successful implementation also depends on organizational capacity and multidisciplinary collaboration. The process of implementing the effective ABC-VEN requires collaboration among practitioners, for instance, clinical pharmacists, financial officers, and medical directors. The shortage of trained human resources in pharmaceutical logistics at public health facilities can hinder the administrative process in the implementation of this combined method.8,12
The proposed conceptual framework extends the traditional use of ABC-VEN by integrating contextual factors such as disease burden, formulary changes, and supply chain conditions into procurement decision-making. This framework aligns economic considerations with clinical priorities by linking adjustments between stock shortage indicators for essential medicines and ensuring the fiscal sustainability of an institution. By extending the use of retrospective expenditure data into a broader decision-making process, the framework may support more prospective procurement planning and inventory governance.
Despite these strengths, this review has some limitations. As a narrative review, it lacks formal quality appraisal and may be prone to selection bias. Geographic representation was also uneven. Although studies from Asia, Africa, and Eastern Europe were included, no studies from Latin America or North America were identified, which limited the generalizability of the findings to other healthcare systems. Moreover, while ABC-VEN was a common framework, classification approaches (eg., AV/AE/AN vs. P/M/T) varied across studies, potentially reducing the comparability of results. These limitations should be taken into account when interpreting the findings of this review.
Conclusion
This review demonstrates that the ABC-VEN method is a widely used approach for supporting drug procurement planning and inventory management across diverse healthcare settings. By integrating economic and clinical priorities, the method consistently facilitates the identification of high-priority medicines, supports rational resource allocation, and contributes to reducing waste while maintaining the availability of essential drugs. Although the evidence is largely derived from single-center and descriptive studies with substantial methodological variation, the overall findings suggest that ABC-VEN remains a practical decision-support tool for healthcare managers and policymakers, particularly in resource-constrained settings. Future research should focus on developing standardized implementation frameworks and generating higher-quality comparative evidence to strengthen the generalizability of findings across healthcare systems.
Acknowledgments
The authors gratefully acknowledge the support from the Faculty of Pharmacy of the Universitas Padjadjaran. We also acknowledge support from the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology, managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Management Sciences for Health. 2012. MDS-3: managing access to medicines and health technologies. Arlington, VA: Management Sciences for Health. Avaliable from: https://msh.org/wp-content/uploads/2014/01/mds3-jan2014.pdf.
2. Mohammed SA, Workneh BD. Critical analysis of pharmaceuticals inventory management using the abc-ven matrix in dessie referral hospital, ethiopia. Integr Pharm Res Pract. 2020;9:113–14. doi:10.2147/iprp.s265438
3. Budgett A, Gopalakrishnan M, Schneller E. Procurement in public & private hospitals in Australia and Costa Rica–a comparative case study. Health Systems. 2017;6(1):56–67. doi:10.1057/s41306-016-0018-z
4. Zulpadly F, Aulia FN. Evaluation of Medication Planning with ABC-VEN Analysis at Indriati Solo Baru Hospital. J. Manaj. Pelayanan Farm. 2024;14(1):26. doi:10.22146/jmpf.86600
5. Indarti TR, Satibi S, Yuniarti E. Pengendalian persediaan obat dengan minimum-maximum stock level di instalasi Farmasi RSUP Dr. Sardjito Yogyakarta. J. Manaj. Pelayanan Farm. 2019;9(3):192. doi:10.22146/jmpf.45295
6. Alanazi MQ, Alkhadhairi EK, Alrumi WH, Alajlan SA. Reducing Pharmaceutical and Non-Pharmaceutical Inventory Waste in Tertiary Hospital: impact of ABC-VEN Analysis in a Zero-Waste Strategy Over 7 Years. Risk Manag Healthc Policy. 2024;17:2659–2675. doi:10.2147/RMHP.S467230
7. Nguyen PH, Dang TVK, Nguyen PT, TMH V, Nguyen TTM. 5-year inventory management of drug products using ABC-VEN analysis in the pharmacy store of a specialized public hospital in Vietnam. Pharmacia. 2022;69(2):517–525. doi:10.3897/pharmacia.69.e84348
8. Jobira T, Abuye H, Jemal A, Gudeta T. Evaluation of pharmaceuticals inventory management in selected health facilities of west arsi zone, Oromia, Ethiopia. Integr Pharm Res Pract. 2021;10:1–11. doi:10.2147/iprp.s298660
9. Mfizi E, Niragire F, Bizimana T, Mukanyangezi MF. Analysis of pharmaceutical inventory management based on ABC-VEN analysis in Rwanda: a case study of Nyamagabe district. J Pharm Policy Pract. 2023;16(1). doi:10.1186/s40545-023-00540-5
10. Kheder SI, Awad MM, Hamid K. Prioritization of medicine importation by the private sector in sudan: evidence from a data analysis, 2012-2015. Value Health Reg Issues. 2020;22:27–34. doi:10.1016/j.vhri.2019.11.007
11. Hussain M, Siddharth V, Arya SABC. VED and lead time analysis in the surgical store of a public sector tertiary care hospital in Delhi. Indian J Public Health. 2019;63(3):194–198. doi:10.4103/ijph.IJPH_282_18
12. Meena DK, Mathaiyan J. Assessment of drug inventory using ABC–VED matrix analysis in selected public health facilities of Puducherry, India. J Family Med Prim Care. 2025;14(4):1389–1394. doi:10.4103/jfmpc.jfmpc_1544_24
13. Pann Thazin M, Sakulbumrungsil R. Analysis of pharmaceutical inventory management in a state hospital in myanmar. Thai J Pharm Sci. 2022;46(2). Available from http://www.tjps.pharm.chula.ac.th.
14. Bilyk I, Fedyak I, Ivaniulyk I, Havryshchuk L. Clinical and economic estimation of children’s pharmacotherapy with meningococcial infections in Ukraine. Pharmacia. 2019;66(3):157–160. doi:10.3897/PHARMACIA.66.E35186
15. Legese N, Teshome D, Gedif T. Inventory management of health commodities in a tertiary teaching hospital in ethiopia. Front Pharmacol. 2022;13. doi:10.3389/fphar.2022.763909
16. Assan A, Moldaliyev I, Kerimbayeva Z, et al. A retrospective analysis of pharmacotherapy in Kazakhstan: assessment of the rational prescription and use of antibiotics in the nephrology department of a multidisciplinary hospital. Electron. J. Gen. Med. 2022;19(6):em422. doi:10.29333/ejgm/12576
17. Gizaw T, Jemal A. How is Information from ABC–VED–FNS matrix analysis used to improve operational efficiency of pharmaceuticals inventory management? a cross-sectional case analysis. Integr Pharm Res Pract. 2021;10:65–73. doi:10.2147/iprp.s310716
18. Kivoto PM, Mulaku M, Ouma C, et al. Clinical and financial implications of medicine consumption patterns at a leading referral hospital in kenya to guide future planning of care. Front Pharmacol. 2018;9:9. doi:10.3389/fphar.2018.01348
19. Lunyova YA. Pharmacoeconomic evaluation of drug supply for chemotherapy in small cell lung cancer. Res. Results Pharmacol. 2023;9(3):1–9. doi:10.18413/rrpharmacology.9.10037
20. Kosyachenko K, Rafalska Y. Analysis of pharmaceutical supply of breast cancer patients. Sci.: Pharm. Sci. 2023;2023(3):87–94. doi:10.15587/2519-4852.2023.283490
21. Yulistiani Y, Hamidi NF, Utomo FN, Hamidah KF. Shifts in drugs use after the COVID-19 pandemic based on the analysis of ABC, VEN and ABC-VEN matrix. Pharmacia. 2023;70(4):1315–1322. doi:10.3897/pharmacia.70.e113558
22. Yohannes T, Boche B, Birhanu N, Gudeta T. Matrix analyses of pharmaceutical products for the years 2017 to 2019 among public health facilities in Hadiya zone, Ethiopia: a cross-sectional descriptive study. BMC Health Serv Res. 2022;22(1). doi:10.1186/s12913-022-07568-4
23. Deressa MB, Beressa TB, Jemal A. Analysis of Pharmaceuticals Inventory Management Using ABC-VEN Matrix Analysis in Selected Health Facilities of West Shewa Zone, Oromia Regional State, Ethiopia. Integr Pharm Res Pract. 2022;11:47–59. doi:10.2147/iprp.s354810
24. Rofiq A, Oetari O, Widodo GP. Analisis Pengendalian Persediaan Obat Dengan Metode ABC, VEN dan EOQ di Rumah Sakit Bhayangkara Kediri. JPSCR. 2020;5(2):97. doi:10.20961/jpscr.v5i2.38957
25. Mousnad MA, Ibrahim MIM, Palaian S, Shafie AA. Medicine expenditures in Sudan National Health Insurance Fund: an ABC-VEN analysis of 5-year medicine consumption. J Pharm Health Serv Res. 2016;7(3):165–171. doi:10.1111/jphs.12136
26. Singh S, Gupta AK, Latika L, Devnani M. ABC and VED analysis of the pharmacy store of a tertiary care, Academic Institute of the Northern India to identify the categories of drugs needing strict management control. J Young Pharm. 2015;7(2):76–80. doi:10.5530/jyp.2015.2.4
27. Kastanioti C, Mavridoglou G, Karanikas H, Polyzos N. ABC analysis: a tool of effectively controlling pharmaceutical expenditure in Greek NHS hospitals. J Pharm Health Serv Res. 2016;7(3):173–179. doi:10.1111/jphs.12137
28. Antonoglou D, Kastanioti C, Niakas D. ABC and VED analysis of medical materials of a general military hospital in greece. J Health Manag. 2017;19(1):170–179. doi:10.1177/0972063416682643
29. Taddele BW, Wondimagegn AA, Asfaw Asaro M, Sorato MM, Gedayi BG, Hailesilase AA. ABC-VEN matrix analysis of the pharmacy store in a secondary level health care facility in arbaminch town, southern ethiopia. J Young Pharm. 2019;11(2):182–185. doi:10.5530/jyp.2019.11.38
30. Dhodi D, Sinha S, Desai S, Vable M. Always, better, and control-vital essential and desirable analysis of pharmacy store of tertiary care teaching hospital, Mumbai. Natl J Physiol Pharm Pharmacol. 2021;1. doi:10.5455/njppp.2021.11.03072202131052021
31. Yilmaz F. The drug inventories evaluation of healthcare facilities using ABC and VED analyzes. Istanbul J. Pharm. 2019;48(2):43–48. doi:10.5152/IstanbulJPharm.2018.398141
32. George S, Elrashid S. Inventory Management and Pharmaceutical Supply Chain Performance of Hospital Pharmacies in Bahrain: a Structural Equation Modeling Approach. Sage Open. 2023;13(1). doi:10.1177/21582440221149717
33. Jifar WW, Geneti GB, Dinssa SD. The Impact of COVID-19 on Pharmaceutical Shortages and Supply Disruptions for Non-Communicable Diseases Among Public Hospitals of South West, Oromia, Ethiopia. J Multidiscip Healthc. 2022;15:1933–1943. doi:10.2147/JMDH.S377319
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.