Back to Journals » Advances in Medical Education and Practice » Volume 16
Optimal Working Hours in the 2024 Physician Work Reform: Insights from a Residency Program Director
Authors Shikino K ![]() , Nishizaki Y, Kataoka K
, Nishizaki Y, Kataoka K ![]() , Nagasaki K, Kobayashi H, Shimizu T
, Nagasaki K, Kobayashi H, Shimizu T ![]() , Tokuda Y
, Tokuda Y ![]()
Received 15 May 2025
Accepted for publication 12 August 2025
Published 20 August 2025 Volume 2025:16 Pages 1461—1468
DOI https://doi.org/10.2147/AMEP.S540698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
Kiyoshi Shikino,1,2,* Yuji Nishizaki,3,* Koshi Kataoka,3 Kazuya Nagasaki,4 Hiroyuki Kobayashi,4 Taro Shimizu,5 Yasuharu Tokuda6,7
1Department of Community-oriented Medical Education, Chiba University Graduate School of Medicine, Chiba, Japan; 2Department of General Medicine, Chiba University Hospital, Chiba, Japan; 3Division of Medical Education, Juntendo University School of Medicine, Tokyo, Japan; 4Department of Internal Medicine, Mito Kyodo General Hospital, University of Tsukuba, Ibaraki, Japan; 5Department of Diagnostic and Generalist Medicine, Dokkyo Medical University Hospital, Tochigi, Japan; 6Muribushi Okinawa for Teaching Hospitals, Okinawa, Japan; 7Tokyo Foundation for Policy Research, Tokyo, Japan
*These authors contributed equally to this work
Correspondence: Kiyoshi Shikino, Department of Community-oriented Medical Education, Chiba University Graduate School of Medicine, 1-8-1, Inohana, Chu-pu-ku, Chiba, Japan, Tel +81-43-222-7171, Email [email protected]
Purpose: The recently instituted Japan 2024 physician workstyle reform imposed upper limits on monthly overtime hours. However, the interpretation of these limits by different training hospitals for postgraduate medical trainees (PGY1– 2) and their supervisors remains unclear. This study aimed to quantify program directors’ perceptions of the “optimal” monthly overtime hours for: (1) achieving educational milestones (Q1), (2) maintaining trainees’ well-being (Q2), and (3) complying with trainees’ limits through supervisors’ workload (Q3), and to compare urban and rural hospitals.
Patients and Methods: We conducted a cross-sectional, web-based survey of all accredited postgraduate training programs (N = 644) between March 1 and April 30, 2024. Program directors responded to three single-choice questions, selecting a monthly overtime band (none, 10, 20, … 100 h/month). Hospitals were classified as urban or rural based on the Ministry of Health, Labor, and Welfare criteria. Linear trends across categories were tested using the Cochran–Armitage trend test.
Results: A total of 151 directors responded (response rate: 23%). Across Q1–Q3, 40 h/month was the most frequently selected time (21– 23%). However, the proportion endorsing ≥ 60 h/month was significantly higher in urban than in rural hospitals (Q1: 43% vs 23%, p = 0.0347; Q2: 34% vs 23%, p = 0.0419; Q3: 40% vs 27%, p = 0.0405). Notably, urban programs were twice as likely to consider ≥ 80 h/month appropriate for both trainees’ well-being (21% vs 6%, p = 0.0066) and supervisors (21% vs 7%, p = 0.0137).
Conclusion: Although 40 h/month is the most frequent response by program directors, those from urban hospitals more commonly viewed extended hours acceptable, even exceeding the “A tier” limit of 45 h. Policy initiatives should tailor workload mitigation and task-shifting strategies to urban hospitals to safeguard the well-being of trainees and supervisors.
Keywords: clinical competence, duty hours, medical education reform, program director perspectives, residency training, well-being
Introduction
Physician work-hour regulation has become a critical issue globally over the past two decades, as extended shifts have been linked to impaired clinician performance, compromised patient safety, and increased burnout among trainees.1,2 In response, the United States implemented duty-hour restrictions in 2003, followed by the European Union’s Working Time Directive in 2009.3 These policy changes triggered an international dialogue on how to balance the dual demands of clinical service and residency training education.4–6
In Japan, the urgency of this issue has intensified with the implementation of the 2024 physician workstyle reform, which legally enforces a tiered system for monthly overtime: Tier A (≤ 45 h), Tier B (≤ 60 h), and Tier C (≤ 80 h under limited exemption).7–9 However, the application of these regulations faces major structural barriers. Urban hospitals often manage higher patient volumes, complex cases, and emergency surges,10 making full compliance with the caps challenging. Conversely, rural hospitals may suffer from understaffing, but their workloads tend to be more predictable.11 Previous studies have examined actual duty hours and their associations with outcomes such as mental health and examination scores,12 but the contextual differences across institutions make it difficult to establish a universal standard for acceptable working hours.
Although prior research in Japan has explored correlations between resident duty hours and outcomes like examination performance and burnout, it has not investigated how program directors interpret and implement the new duty-hour regulations in practice. Specifically, the way these educational leaders balance competing priorities of education, resident well-being, and supervisor workload—particularly in the early stages of the 2024 reform’s rollout—remains underexplored. This is a critical gap in knowledge, especially as recent policy reports and national discussions have emphasized inconsistencies in implementation across institutions, regions, and specialties.
Therefore, this study aimed to explore program directors’ perceptions of appropriate monthly overtime limits for residents in Japan, focusing on (1) optimal hours for achieving educational milestones, (2) maintaining resident well-being, and (3) supervisor workload needed to comply with regulations. By examining these perspectives, the study contributes to ongoing debates in medical education and workforce reform and offers insights to inform tailored implementation strategies within Japan and internationally.
Methods
Research Procedure and Samples
We conducted a cross-sectional, web-based survey targeting program directors of all 644 hospitals in Japan certified for postgraduate residency training by the Ministry of Health, Labour and Welfare (MHLW) and the Japan Organization of Advancing Medical Education Program (JAMEP).
This constituted a total population (census) sampling method, in which one program director per accredited hospital was invited to participate. This approach was intentionally selected to maximize diversity across institutional contexts (geographical location, hospital size, and function) and to minimize sampling bias. By surveying the entire population of eligible training hospitals, this method enhances the generalizability of the findings to the national level.
The survey was administered via Email between March 1 and April 30, 2024, with follow-up reminders sent after 2 weeks. Participation was voluntary and anonymous.
A total of 151 program directors responded, yielding a response rate of 23.4%. Of these, 98 (65%) were affiliated with rural hospitals and 53 (35%) with urban hospitals, as defined by MHLW-designated medical care area codes. This classification aligns with national health policy frameworks. The only inclusion criterion was certification as a postgraduate residency training hospital by MHLW and JAMEP. One program director per hospital was targeted. No further exclusion criteria were applied.
Ethics Approval and Informed Consent
This study was approved by the Ethics Review Board of the Japan Institute for the Advancement of Medical Education Program (Approval No. 23–27). All participants provided written informed consent prior to participation.
Questionnaire Items
The questionnaire consisted of three items (Q1–Q3), each asking respondents to select the single best overtime band (None, 10, 20, …, ≥ 100 h) under distinct scenarios: educational attainment (Q1), maintaining resident well-being (Q2), and managing supervisor workload to comply with resident duty limits (Q3). For Q2, the term “well-being” was not formally defined but was intended to encompass a broad spectrum, including mental health, burnout risk, fatigue, and work–life balance, consistent with prior literature. Although subjective, this construct aligns with established well-being dimensions used in physician studies, such as the Maslach Burnout Inventory and General Health Questionnaire. Urban/rural status was determined using MHLW medical care area codes.
Statistical Analysis
Descriptive statistics (frequencies and percentages) were used to summarize respondent characteristics and survey responses. Stratified results by urban/rural classification were reported where applicable. Because our primary aim was to describe directors’ perceptions rather than test causal hypotheses, we did not introduce statistical control variables or fit multivariable models. Nevertheless, we acknowledge that contextual factors—such as hospital size, patient volume, or specialty mix—could influence responses; these potential confounders are considered qualitatively in the Limitations and Future Directions sections. The distributions of answers were summarized as frequencies and percentages. For each question, we applied the Cochran–Armitage test to assess the monotonic trends across the overtime bands. For secondary analysis, categories were dichotomized into “≤ 70 h (A/B tier)” vs “≥ 80 h (C tier or above)”. The Fisher’s exact test was applied to compare proportions. Significance was set at a two-sided p < 0.05. All analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Respondent Characteristics
Of the 151 program directors who responded, 98 (65%) were affiliated with rural hospitals and 53 (35%) with urban hospitals. This reflects a slight overrepresentation of rural hospitals, as nationally, accredited residency hospitals are more concentrated in urban areas. The median number of trainees per hospital was 6 (IQR, 4–10). No further individual or institutional demographic data (eg, sex, specialty, or hospital bed count) were collected. As the study employed a census approach targeting all accredited hospitals across Japan, the sample included a diverse range of settings. Although participation was voluntary, the inclusion of both urban and rural institutions enhances the representativeness of perspectives.
Optimal Overtime for Educational Attainment (Q1)
The distribution of responses regarding the optimal number of monthly overtime hours for achieving educational goals is shown in Figure 1. Among all respondents, 40 hours per month was the most frequently selected option (22%), followed by 60 hours (17%) and 20 hours (15%) (Table 1). Notably, response patterns varied between urban and rural hospitals in urban settings, 60 hours per month was chosen by 23%, whereas in rural hospitals, 40 hours was the most common response (22%). These findings suggest a tendency among urban directors to accept longer working hours for educational purposes.
 |
Table 1 Preferred Overtime Hours for Educational Attainment (Q1) by Setting |
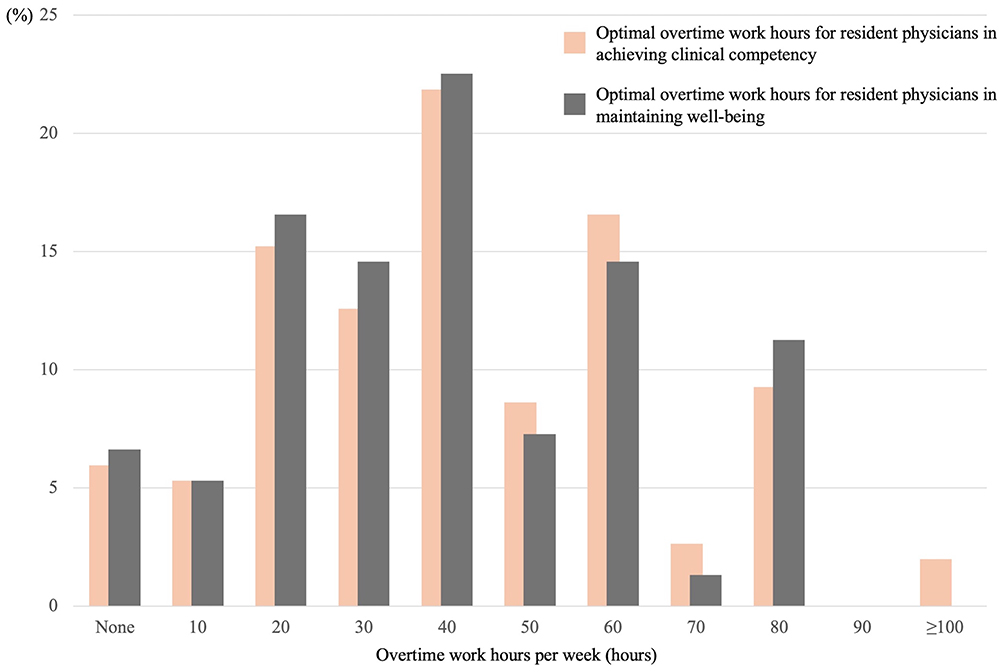 |
Figure 1 Distributions of responses for Q1 & Q2, showing the gap between the program directors’ perspectives on optimal overtime work hours for resident physicians: Balancing achieving clinical competency and well-being. |
Optimal Overtime for Well-Being (Q2)
Figure 2 illustrates directors’ perceptions regarding the relationship between overtime hours and residents’ clinical competence. Overall, 67% of respondents considered moderate overtime (40–60 h/month) enhanced clinical learning (Table 2). In contrast, both minimal overtime (<20 h/month) and excessive overtime (>80 h/month) were associated with decreased perceived effectiveness. While this trend was consistent across regions, rural hospital directors more frequently viewed shorter overtime hours (20–40 h/month) as sufficient for maintaining educational quality.
 |
Table 2 Preferred Overtime Hours for Wellbeing (Q2) by Setting |
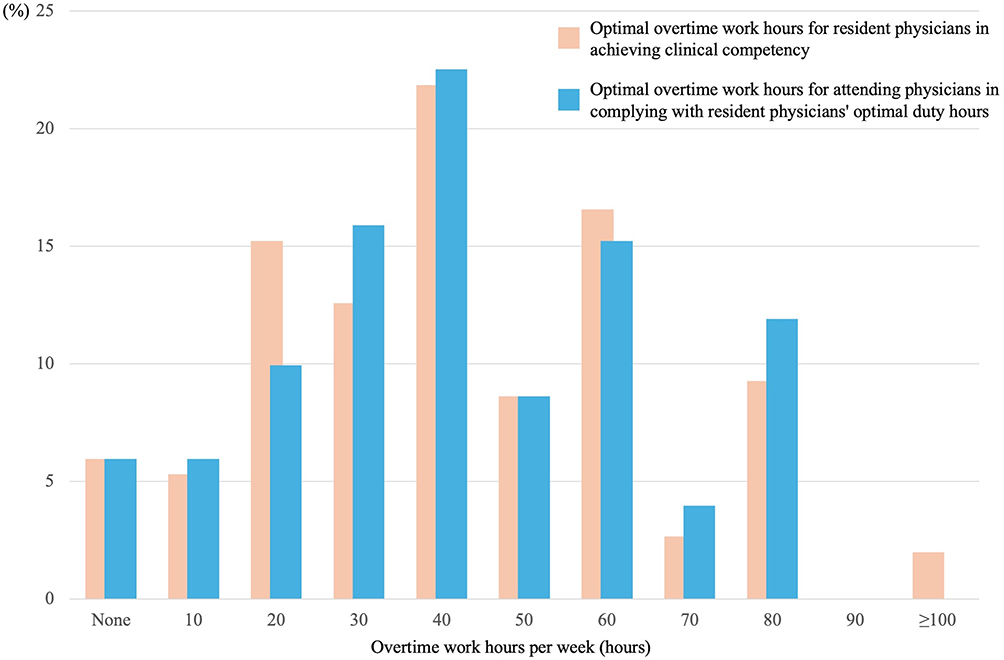 |
Figure 2 Distributions of responses for Q3, showing the gap between program directors’ perspectives on optimal overtime work hours for resident physicians: Balancing resident physicians’ clinical competency achievement and attending physicians’ compliance. |
Supervisors’ Overtime to Uphold Trainee Limits (Q3)
Responses regarding the impact of overtime on physician well-being are summarized in Figure 1. Most directors indicated that excessive overtime (>80 h/month) negatively impacted well-being (Table 3). By contrast, 30–40 h/month was most frequently associated with positive outcomes. Urban directors were more likely than their rural counterparts to tolerate higher overtime levels, with urban respondents considering 60 h/month acceptable for balancing training and well-being, compared to rural respondents. The linear trend analysis also reached significance (p = 0.0405), confirming the consistency of this urban–rural divide across all three questions. The survey instrument was developed in Japanese, based on a literature review and expert consensus among medical educators and program directors. It included demographic questions and three main items assessing the perceived optimal number of monthly overtime hours for resident education, well-being, and supervision.
 |
Table 3 Preferred Overtime Hours for Supervisors (Q3) by Setting |
Discussion
This nationwide survey showed that program directors most frequently identified 40 h/month as the optimal amount of overtime, suggesting a convergence around this threshold. This clustering may partially reflect social desirability bias, as 40 hours corresponds to the legally sanctioned upper limit of the “A tier” overtime threshold. However, the interpretation of this finding warrants caution, given the study’s limitations, including a modest 23% response rate and the overrepresentation of rural hospitals. These factors may affect the external validity, and further research is needed to confirm whether the observed patterns hold across the broader population of training programs in Japan. Directors may have selected this figure to align with perceived policy expectations rather than institutional realities. Future studies integrating actual duty logs or triangulating with resident-reported well-being scores could help clarify whether this threshold reflects genuine consensus or normative pressures. This finding underscores a tension between national policy and local realities, indicating that the regulatory “universal” model may inadequately capture the heterogeneity of clinical workloads across Japan.
Moreover, the 40 h/month selection as a balance point warrants interpretation in light of existing performance data. For instance, Nagasaki et al (2022)13 demonstrated that residents working within 60–80 h/month showed no deterioration in GM-ITE scores, suggesting that moderate overtime may be educationally neutral or even beneficial. Our results support these findings by demonstrating the directors’ implicit belief in a trade-off zone rather than a strict cut-off; however, further investigation is required to confirm whether the perceived optimal hours align with actual training outcomes.
Actual working hour studies report a median resident overtime of 70–80 h in metropolitan tertiary centers, corroborating directors’ high tolerance.14,15 Rural hospitals, which have lower patient volumes but still experience staffing shortages, nevertheless aspire to keep hours within A–B tiers, echoing US duty-hour reforms targeting ≤ 80 h16 Our data extend these observations by demonstrating that perceptions, not just recorded hours, follow the same geographic gradient, aligning with reports from South Korea and Taiwan, where urban academic centers similarly endorse prolonged duty hours to sustain service throughput.14,17
Several contextual factors may explain the observed urban–rural gap.16,18 First, urban hospitals face a higher influx of emergency cases and subspecialty referrals, creating service demands that normalizes extended shifts.15 Second, the high case mix complexity and diversity in metropolitan centers necessitate sustained direct supervision and bedside teaching, which program directors may view as requiring longer duty hours to snsure adequate clinical exposure and competence acquisition.19 Third, the multi-layered hierarchical cultures in large hospitals can diffuse responsibility, inadvertently inflating the clock-in times for trainees and supervisors.20 Conversely, rural training programs that incorporate a longitudinal continuity experience—such as scheduled half‑day sessions at free or community‑based clinics—may promote graduates’ likelihood of practicing in underserved or rural areas after completion.21
Practical Implications
Policies predicated on uniform-hour caps may be resisted in urban centers unless coupled with service redesigns such as night float systems, APP integration, or regional load balancing. Moreover, our data indicate that directing compliance burdens onto supervisors risks perpetuating overwork and undermining the intent of reform. A differentiated implementation strategy, analogous to the US ACGME’s “flexible compliant schedules” pilot, could further permit urban institutions to adopt transitional models contingent upon demonstrable fatigue-risk management plans and objective learning outcomes. Additionally, task-shift interventions, such as pharmacist-led medication reconciliation and tele-hospitalist coverage, already piloted in select Tokyo hospitals, warrant broader evaluation as a means of decoupling educational exposure from the service load.
Limitations
Despite the valuable insights provided by this study, several limitations must be acknowledged. First, the low response rate of 23% raises the possibility of non-response bias, potentially limiting the generalizability of the findings. The overrepresentation of rural hospitals (65%), compared to their actual proportion among accredited training hospitals, may reflect differential response behavior and could skew the findings toward the perspectives of directors working in rural settings. As a result, caution is warranted in generalizing these results to all residency training institutions in Japan. Future studies using stratified sampling and efforts to increase response rates are needed to enhance representativeness. Future studies with higher response rates and weighted sampling may help ensure greater representativeness. It is also possible that program directors who chose to participate may have had stronger opinions or different experiences than those who did not, which may have skewed the results. Second, the study sample was drawn exclusively from hospitals participating in the 2023 GM-ITE and may therefore not fully represent all residency training institutions in Japan. Hospitals that prioritize structured training and assessment, such as those involved in GM-ITE, may differ in their work-hour policies and educational approaches compared with non-participating institutions. Third, the study relied on self-reported data, possibly subject to social desirability bias. Program directors may have provided responses that aligned with regulatory expectations or institutional policies rather than actual practice. Future research incorporating objective measures such as duty-hour logs or resident feedback would provide a more comprehensive understanding of actual working conditions. Fourth, the survey did not explore any potential regional variations or specialty-specific differences in duty hour preferences. Indeed, training demands and workload expectations, which were not explicitly considered in the present study, may vary across medical specialties and geographic regions. Fifth, the study’s cross-sectional design limited its ability to establish causality or track changes over time. Longitudinal studies are, therefore, required to assess the long-term impact of duty-hour reforms on resident training, well-being, and patient care outcomes. Despite these limitations, this study offers valuable insights for residency program directors and provides a foundation for further research and policy discussions on optimizing resident work hours in Japan. Finally, although hospitals were dichotomized into “urban” and “rural” settings based on MHLW medical area codes, this classification may not fully capture institutional heterogeneity. For example, some urban hospitals may be small-scale community facilities, whereas certain rural hospitals may function as high-volume regional centers. Future studies should consider sensitivity analyses using additional stratification variables such as hospital bed count, emergency case volume, or number of residents to enhance robustness and generalizability.
Future Directions
Building on these limitations, several directions for future research are warranted. First, future studies should aim to improve sampling methods, using stratified random sampling with weighting for urban–rural distribution, to ensure greater generalizability of findings across different hospital settings and regions. Second, longitudinal studies are essential to evaluate how changes in duty-hour policies influence resident competence, well-being, and patient outcomes over time. Third, incorporating resident perspectives, including qualitative interviews and structured feedback, would help contextualize program directors’ views and uncover gaps between policy and practice. Fourth, future investigations should explore specialty-specific and regional variations in duty-hour preferences and training structures, as these may have significant implications for the implementation of nationwide policies. Lastly, triangulating self-reported data with objective indicators—such as electronic duty logs, resident evaluations, or patient care metrics—could provide a more nuanced understanding of how work hours influence both education and healthcare delivery.
Conclusion
Overall, our survey results showed that 40 h per month is perceived as ensuring an optimal balance between the education and well-being of Japanese PGY1–2 trainees. Nonetheless, urban program directors frequently endorse overtime levels exceeding the national Tier A thresholds for trainees and supervisors. To reconcile educational imperatives with work-style reform mandates, we recommend several policy adaptations such as flexible compliance models for urban institutions, region-specific duty-hour targets, and expansion of task-shifting initiatives. These strategies can promote sustainable implementation while safeguarding the well-being of both trainees and supervisors.
Based on our findings, we propose several policy optimization strategies. First, for high-volume urban hospitals that tolerate extended duty hours, flexible compliance models—such as night float systems, staggered shifts, and fatigue risk management plans—should be implemented. Second, context-sensitive duty-hour thresholds should be introduced, allowing for regional and institutional variation rather than uniform caps. Third, task-shifting approaches, including advanced practice provider (APP) integration, tele-supervision, and pharmacist-led support, should be expanded to reduce supervisory burden without compromising resident education. Lastly, reforms should incorporate continuous monitoring of resident outcomes (eg, burnout, satisfaction, and learning progress) to support adaptive, evidence-informed policy implementation.
Acknowledgments
We thank the members of JAMEP for their valuable assistance. We would also like to thank Editage for English language editing.
Funding
This study was supported by Health, Labor, and Welfare Policy Research Grants for Region Medical (Grant No. 24IA2016) from the Ministry of Health, Labor, and Welfare (MHLW). The funder had no role in the design or conduct of the study; the collection, management, analysis, or interpretation of the data; the preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Disclosure
KS received honorarium from JAMEP for exam preparation for the GM-ITE. YN received honorarium from JAMEP as a GM-ITE project manager. YT is the director of JAMEP, and has received honorarium from JAMEP as a speaker of JAMEP lectures. HK received an honorarium from JAMEP as a speaker for the JAMEP lecture. TS received honorarium from JAMEP as an exam preparer for GM-ITE. The authors report no other conflicts of interest in this work.
References
1. Weaver MD, Sullivan JP, Landrigan CP, Barger LK. Systematic review of the impact of physician work schedules on patient safety with meta-analyses of mortality risk. Jt Comm J Qual Patient Saf. 2023;49(11):634–647. doi:10.1016/j.jcjq.2023.06.014
2. Weaver MD, Landrigan CP, Sullivan JP, et al. The association between resident physician work-hour regulations and physician safety and health. Am J Med. 2020;133(7):e343–e354. doi:10.1016/j.amjmed.2019.12.053
3. Wyman MG, Huynh R, Owers C. The European Working Time Directive: will modern surgical training in the United Kingdom be sufficient? Cureus. 2022;14(1):e21797. doi:10.7759/cureus.21797
4. Philibert I, Chang B, Flynn T, et al. The 2003 common duty hour limits: process, outcome, and lessons learned. J Grad Med Educ. 2009;1(2):334–337. doi:10.4300/JGME-D-09-00076.1
5. Bolster L, Rourke L. The effect of restricting residents’ duty hours on patient safety, resident well-being, and resident education: an updated systematic review. J Grad Med Educ. 2015;7(3):349–363. doi:10.4300/JGME-D-14-00612.1
6. Salgado SM, Katz JT, Pelletier SR, et al. Impact of extended duty hours on perceptions of care and objective patient outcomes. J Patient Saf. 2022;18(6):e938–e946. doi:10.1097/PTS.0000000000000988
7. Ishikawa M. Overwork among resident physicians: national questionnaire survey results. BMC Med Educ. 2022;22(1):729. doi:10.1186/s12909-022-03789-7
8. Nagasaki K, Kobayashi H. The effects of resident work hours on well-being, performance, and education: a review from a Japanese perspective. J Gen Fam Med. 2023;24(6):323–331. doi:10.1002/jgf2.649
9. Le AB, Balogun AO, Smith TD. Long work hours, overtime, and worker health impairment: a cross-sectional study among stone, sand, and gravel mine workers. Int J Environ Res Public Health. 2022;19(13):7740. doi:10.3390/ijerph19137740
10. Shen HN, Lu CL, Li CY. Higher hospital caseload is associated with better treatment outcomes of patients with pleural infection. Tohoku J Exp Med. 2014;232(4):285–292. doi:10.1620/tjem.232.285
11. Borowiak E, Kostka J, Kostka T. Comparative analysis of the expected demands for nursing care services among older people from urban, rural, and institutional environments. Clin Interv Aging. 2015;10:405–412. doi:10.2147/CIA.S72534
12. Nagasaki K, Kobayashi H, Nishizaki Y, et al. Association of sleep quality with duty hours, mental health, and medical errors among Japanese postgraduate residents: a cross-sectional study. Sci Rep. 2024;14(1):1481. doi:10.1038/s41598-024-51353-8
13. Nagasaki K, Nishizaki Y, Shinozaki T, et al. Impact of the resident duty hours on in-training examination score: a nationwide study in Japan. Med Teach. 2022;44(4):433–440. doi:10.1080/0142159X.2021.2003764
14. Jena AB, Schoemaker L, Bhattacharya J. Exposing physicians to reduced residency work hours did not adversely affect patient outcomes after residency. Health Aff. 2014;33(10):1832–1840. doi:10.1377/hlthaff.2014.0318
15. Fujikawa H, Tamune H, Nishizaki Y, et al. Association between residents’ work hours and patient care ownership: a nationwide cross-sectional study in Japan. BMC Med Educ. 2022;25(1):385. doi:10.1186/s12909-025-06941-1
16. Nagasaki K, Nisizaki Y, Shimizu T, et al. Educational environment changes toward resident duty hour restrictions in Japan. Sci Rep. 2025;15(1):16925. doi:10.1038/s41598-025-00347-1
17. Sasnal M, Jensen RM, Mai UT, et al. Strategies to foster stakeholder engagement in residency coaching: a CFIR-Informed qualitative study across diverse stakeholder groups. Med Educ Online. 2024;29(1):2407656. doi:10.1080/10872981.2024.2407656
18. Ministry of Health, Labour and Welfare. Summary of Static/Dynamic Surveys of Medical Institutions and Hospital Report. Tokyo: MHLW; 2024.
19. Ouyang D, Chen JH, Krishnan G, et al. Patient Outcomes When Housestaff Exceed Eighty Hours per Week. Am J Med. 2016;129(9):993–999. doi:10.1016/j.amjmed.2016.03.023
20. Morita S, Yamada R, Okada Y, et al. Facing hierarchy: a qualitative study of residents’ experiences in an obstetrical simulation scenario. Adv Simul (Lond). 2022;7:34. doi:10.1186/s41077-022-00232-1
21. Petrany SM, Gress T, Poole D. A Free Clinic Continuity Experience During Residency Is Associated With Practice in Underserved Areas. J Grad Med Educ. 2017;9(5):595–599. doi:10.4300/JGME-D-17-00019.1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.