Back to Journals » Drug Design, Development and Therapy » Volume 19
Optimal Programmed Intermittent Epidural Bolus Interval for Video-Assisted Thoracic Surgery Lobectomy: A Biased-Coin Up-Down Study of Ropivacaine-Sufentanil
Authors Feng C ![]() , Wen J, Lai G, Lu X, Luo G, Lu Y, Li W, Lai R
, Wen J, Lai G, Lu X, Luo G, Lu Y, Li W, Lai R ![]()
Received 3 May 2025
Accepted for publication 12 August 2025
Published 20 August 2025 Volume 2025:19 Pages 7207—7214
DOI https://doi.org/10.2147/DDDT.S538163
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Chengfei Feng,1,* Jijin Wen,2,* Guozhong Lai,3,* Xiaofan Lu,2 Guanli Luo,2 Yali Lu,2 Wei Li,2 Renchun Lai2
1Department of Anesthesiology, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-Sen University, Guangdong Provincial Key Laboratory of Ophthalmology Visual Science, Guangdong Provincial Clinical Research Center for Ocular Disease, Guangzhou, 510060, People’s Republic of China; 2Department of Anesthesiology, State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-Sen University Cancer Center, Guangzhou, 510060, People’s Republic of China; 3Department of Anesthesiology, Guangzhou Women and Children’s Medical Center, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Renchun Lai, Email [email protected] Wei Li, Email [email protected]
Purpose: Programmed intermittent epidural bolus (PIEB) is a novel epidural anesthesia technique for video-assisted thoracic surgery (VATS). However, the optimal setting of the PIEB parameters remains to be determined. This study aimed to determine the optimal time interval for the PIEB regimen of 10 mL ropivacaine 0.15% with sufentanil 0.4 μg/mL within 24 hours of VATS lobectomy.
Patients and Methods: We conducted a double-blind, sequential allocation trial with a biased-coin up-down design. 42 patients scheduled for VATS lobectomy were enrolled in the study. All participants received a fixed programmed bolus dose of 10 mL of 0.15% ropivacaine combined with 0.4 μg/mL sufentanil. The PIEB interval was initially set at 180 minutes for the first patient and adjusted for subsequent patients according to the biased-coin design, with intervals of 180, 150, 120, and 90 minutes (corresponding to groups 180, 150, 120, and 90, respectively). The primary outcome was the achievement of effective analgesia, defined as the absence of any requirement for patient-controlled epidural analgesia (PCEA) or additional rescue analgesic interventions within 24 hours after the loading dose. Secondary outcomes included the documentation of postoperative adverse effects, such as nausea, vomiting, hypotension, pruritus, and dizziness.
Results: A total of 40 patients were included in the study. Using Isotonic Regression analysis, the estimated effective interval for 90% (EI90) of patients was determined to be 97.4 minutes (95% confidence interval [CI]: 91.6– 103.1 minutes). The incidence of postoperative hypotension varied significantly across groups, with the highest probability observed in group 90 (64.3%), followed by group 120 (18.8%) and group 150 (11.1%).
Conclusion: The estimated effective interval for the EI90 between PIEB of 10 mL of ropivacaine 0.15% with sufentanil 0.4 μg/mL was approximately 100 minutes.
Trial Registration: Chinese Clinical Trial Registry, ChiCTR2300077174.
Keywords: epidural analgesia, programmed intermittent epidural bolus, time interval, video-assisted thoracic surgery lobectomy
Introduction
The efficacy of continuous epidural infusion (CEI) of local anesthetics combined with patient-controlled analgesia (PCA) as a postoperative analgesic approach for video-assisted thoracic surgery (VATS) has been well established.1 However, CEI may lead to increased local anesthetic consumption and restricted drug distribution, potentially resulting in suboptimal postoperative analgesia and recovery quality for VATS patients.2
Programmed intermittent epidural bolus (PIEB) is an advanced epidural analgesia technique that administers local anesthetic boluses into the epidural space at predetermined intervals. In the realm of obstetric analgesia, PIEB has progressively replaced CEI and has become a widely adopted method. Comparative studies between PIEB and CEI have demonstrated that PIEB not only reduces the incidence of adverse events but also enhances maternal satisfaction and decreases local anesthetic consumption.3–9
Despite its proven benefits in obstetric care, research on the application of PIEB for postoperative analgesia in thoracic surgery is limited. Only two studies have explored this area, both indicating that PIEB, compared to CEI, reduces local anesthetic usage, alleviates nighttime pain, and improves sleep quality following thoracotomy.10,11 However, these studies had significantly different protocols and did not include patients undergoing VATS. Additionally, both studies incorporated PCEA as a supplementary postoperative analgesic method. Consequently, the optimal parameters for drug delivery when PIEB is employed as the sole analgesic technique remain undefined.
To address this gap, we designed a study to determine the optimal time interval between fixed boluses of an epidural mixture using PIEB as the sole analgesic technique. We hypothesize that the optimal time interval for achieving effective analgesia in 90% of patients receiving PIEB with 10 mL of 0.15% ropivacaine and 0.4 μg/mL sufentanil within 24 hours post-VATS lies between 90 and 180 minutes. This study aims to refine the application of PIEB in VATS, potentially improving postoperative outcomes and patient comfort.
Materials and Methods
Study Design
This prospective, double-blind, sequential allocation trial was approved by the Ethical Committee Sun Yat-sen University Cancer Center (SL-B2023-353-02). Written informed consent was obtained from all participants. It was registered at the Chinese Clinical Trial Registry (ChiCTR2300077174, principal investigator: Renchun Lai, date of registration: November 1st, 2023) before patient enrollment. This study was conducted following the Declaration of Helsinki.
Participants
Patients eligible for participation were those diagnosed with lung cancer and scheduled to undergo VATS lobectomy at the Sun Yat-sen University Cancer Center between November 2023 and February 2024. Additional inclusion criteria included: (1) age over 18 years, (2) American Society of Anesthesiologists (ASA) physical status of I–III, (3) no participation in other clinical studies within the preceding three months. Patients were excluded from the study if they met any of the following conditions: (1) allergy or hypersensitivity to local anesthetics (eg, ropivacaine or lidocaine) or opioids (eg, sufentanil), (2) scheduled for bilateral thoracic surgery, (3) history of previous thoracic surgery, (4) contraindications to nerve block procedures, (5) history of chronic pain or ongoing pain treatment. The study was discontinued under the following circumstances: (1) inability to complete the planned treatment due to adverse events, such as complications from the puncture procedure or dislodgement of the epidural catheter, (2) conversion of thoracoscopic surgery to open thoracotomy, (3) absence of postoperative chest drainage, (4) patient request to withdraw from the study.
Anesthetic Procedure
Under standard monitoring, thoracic epidural puncture was performed at the T6-7 or T7-8 interspace with the patient in the lateral decubitus position. To ensure consistency in puncture level, all patients underwent preprocedural spinal ultrasound assessment.12 All epidural catheter placements were performed by an experienced anesthesiologist. The epidural space was identified using a 17-gauge Tuohy needle and the loss-of-resistance-to-saline technique. A 19-gauge multiport wire-reinforced epidural catheter (Arrow FlexTip Plus®; Arrow International Inc., Reading, PA) was then advanced 5 cm into the epidural space. After a 3-mL test dose of 1% lidocaine confirmed proper placement, the catheter was secured.
General anesthesia was induced with intravenous sufentanil (0.3 μg/kg), propofol (1.5–2 mg/kg), and cisatracurium (0.2 mg/kg) and maintained with sevoflurane (2–3%) and a cisatracurium infusion (2 μg/kg/min). After endotracheal intubation and hemodynamic stabilization, a 10 mL bolus of 0.2% ropivacaine (20 mg ropivacaine + 10 μg sufentanil) was administered as an epidural loading dose. An blinded research assistant prepared and activated a portable electronic infusion pump (Model: REHN 11, Renxian Medical Technology Co., Ltd., Jiangsu, China), which was then connected to the epidural catheter. To maintain blinding, the pump was concealed under an opaque paper cover, preventing investigators, nursing staff, and participants from identifying the device. Throughout the procedure, bispectral index (BIS) and noxious stimulation index (NOX) were continuously monitored, with target ranges of 40–60 for BIS and 30–50 for NOX to ensure adequate anesthesia depth and nociception-antinociception balance.
Group Allocation
The maintenance solution consisted of 0.15% ropivacaine with sufentanil (0.4 μg/mL). All subjects received a fixed PIEB dose of 10 mL delivered at 300 mL/h. The time for the first bolus was determined based on the interval time assigned to the patient. Subsequent intervals were adjusted using a biased coin allocation method based on the previous patient's response. The investigated interval times were 180, 150, 120, and 90 minutes, corresponding to groups 180, 150, 120, and 90, respectively. Consequently, the total volume of ropivacaine administered via PIEB ranged from 3.3 mL/hour (group 180) to 6.7 mL/hour (group 90), equivalent to an hourly dose of 5–10 mg of ropivacaine. For the first patient, the interval was set at 180 minutes. If a patient did not respond successfully to the PIEB regimen, the interval for the next patient was shortened by 30 minutes. Conversely, if the response was successful, the interval for the subsequent patient was lengthened by 30 minutes with a probability of 1/9; otherwise, it remained unchanged. In cases where group 180 had a successful response, or group 90 had a failed response, the interval for subsequent patients was held constant until the biased-coin algorithm dictated an increase or decrease, respectively. After each successful response, the biased-coin allocation was executed using a computer-generated randomization list prepared by the statistician. A research assistant, who had access to the program, entered the data, determined the next patient’s interval, and configured the delivery system. To maintain blinding, the device was concealed with paper, preventing investigators, nurses, and participants from viewing the settings.
The infusion pump was programmed to deliver 5 mL PCEA boluses of the study solution, with a 30 minute lockout period and a maximum allowable dose of 20 mL/h. Participants were instructed to self-administer PCEA boluses as needed for breakthrough pain. Any utilization of PCEA was interpreted as failure to achieve adequate analgesia with the programmed PIEB protocol, resulting in classification as a treatment failure for that particular PIEB interval.
Routine monitoring was conducted for the first 24 hours, with non-invasive blood pressure measured every 5 minutes initially and extended to 10–30 minutes if no hypotension occurred. Hypotension was defined as either a systolic blood pressure (SBP) < 90 mmHg or a ≥ 20% decrease in SBP from baseline values. Hypotension was managed with fluid resuscitation, vasoactive medications, or temporary cessation of the analgesic pump, which was restarted after symptom resolution.
Outcomes
Outcome assessments were performed by a blinded investigator. The primary outcome was effective analgesia, defined as the absence of PCEA requests or supplemental analgesic requirements during the first 24 hours following the loading dose. The secondary endpoints were the occurrence of postoperative adverse effects, including nausea, vomiting, hypotension, and dizziness, which were documented. The quality of recovery-15 (QoR-15) score was recorded at 24 hours postoperatively. The patients who did not achieve effective analgesia were recorded with the time of the first PCEA use in the 24 hour postoperative period and the total number of PCEA. The highest pain intensity experienced in the 24-hour postoperative period was evaluated using a verbal numeric rating scale (VNRS).
Additional data recorded included age, gender, body mass index (BMI), ASA classification, history of hypertension, diabetes mellitus, coronary artery disease, smoking, and preoperative radiotherapy or chemotherapy.
Sample Size Calculation
For dose-finding studies based on the biased-coin up-and-down design, simulation studies suggest that enrolling at least 20–40 patients will provide stable estimates of the target dose in most cases.13,14 Therefore, we decided to enroll 40 patients in this study.
Statistical Analysis
The study population was summarized descriptively. The effective interval of PIEB in EI90 and its 95% CI can be estimated using two non-parametric methods: the truncated Dixon and Mood method and the isotonic regression method with the pooled-adjacent-violators algorithm approach. In general, the estimate based on the isotonic regression method exhibits a smaller bias and mean square error in comparison to the Dixon and Mood estimator, although a wider CI is expected. Therefore, this study used the isotonic regression method to estimate the EI90 and its 95% CI.
A descriptive analysis was conducted to examine the patients’ characteristics and secondary outcomes across various time interval groups. Statistical analyses were performed with R 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 42 patients were enrolled in the study, conducted between November 1, 2023, and February 29, 2024. Two participants were subsequently excluded: one due to an intraoperative procedural change and another due to postoperative epidural catheter dislodgement. Consequently, data analysis was performed on the remaining 40 patients. Demographic characteristics are summarized in Table 1.
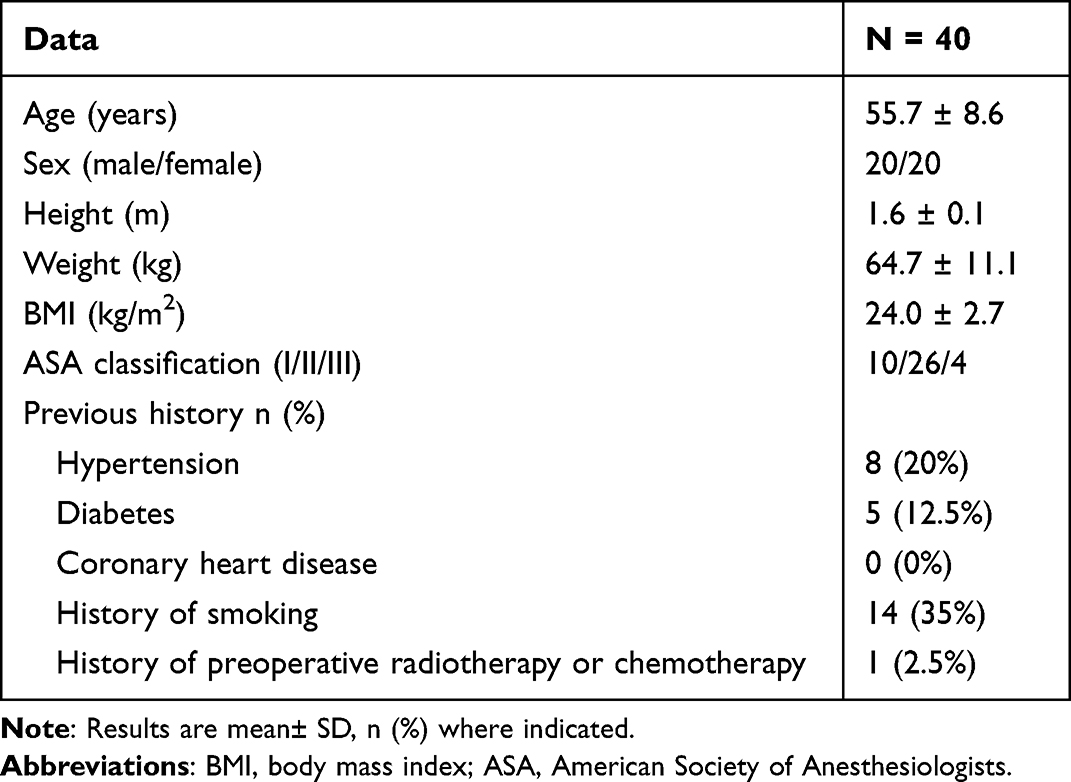 |
Table 1 Patient Characteristics |
Using isotonic regression, the estimated EI90 for programmed intermittent epidural bolus (PIEB) intervals was 97.4 minutes (95% CI: 91.6–103.1). This estimate demonstrated sufficient precision to support the primary hypothesis, as the entire CI fell within the predefined clinically acceptable range of 90–180 minutes. The patient allocation sequence and responses to varying PIEB intervals are illustrated in Figure 1.
 |
Figure 1 CONSORT flow diagram. The patient sequence number (x-axis) orders patient exposures using the bias coin up-and-down design. The assigned PIEB interval times (y-axis) are 180, 150, 120, and 90 minutes. An effective PIEB interval time is indicated by a green dot, while an ineffective one is indicated by a red triangle. Abbreviations: CONSORT, Consolidated Standards of Reporting Trials; PIEB, programmed intermittent epidural bolus. |
The study demonstrated effective analgesia rates of 92.9% in group 90 and 81.3% in group 120. Response rates for each interval, along with adjusted values, were detailed in Table 2. Additionally, Table 3 presented the time to PCEA request after the loading dose in patients who did not respond to the protocol.
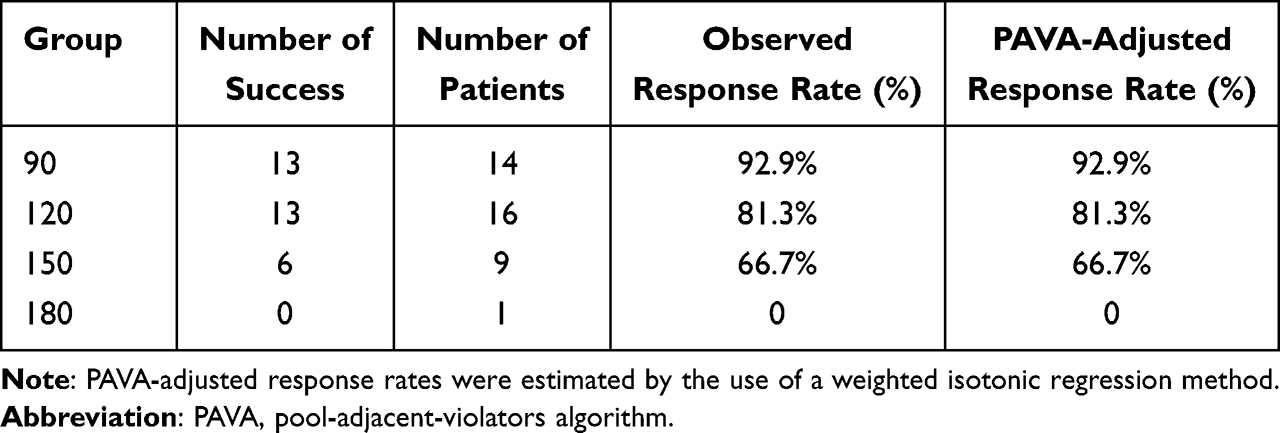 |
Table 2 Observed and PAVA-Adjusted Response Rate |
 |
Table 3 Time to PCEA Request, Total Number of PCEAs, and Highest NRS Score Within 24 h in Cases of Failure of the PIEB Regimen |
The incidence of postoperative hypotension varied significantly among groups, occurring in 64.3% of patients in group 90, compared to 18.8% in group 120 and 11.1% in group 150. All hypotensive episodes resolved following fluid therapy or vasoactive medication, with no associated adverse events or discontinuation of analgesic pumps. During the postoperative period, pruritus was reported by approximately 50% of patients, most commonly affecting the abdominal and forearm regions. Table 4 summarized the incidence of nausea/vomiting, pruritus, hypotension, and dizziness across subgroups. To assess postoperative recovery quality, we utilized the QoR-15 scale. The QoR-15 scores for each subgroup were detailed in Table 5.
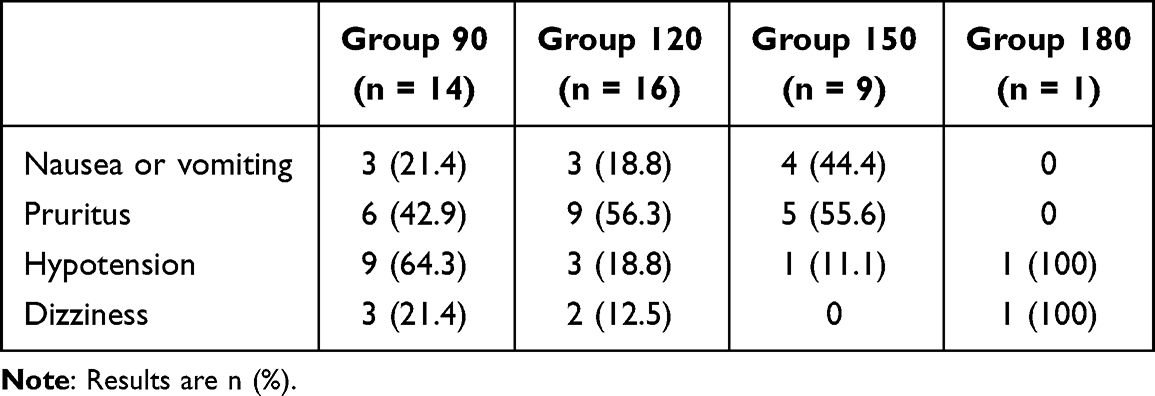 |
Table 4 Nausea or Vomiting, Pruritus, Hypotension, and Dizziness |
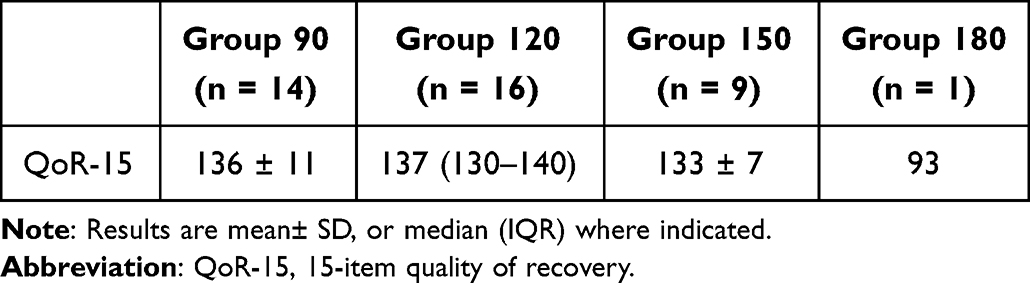 |
Table 5 Postoperative QoR-15 |
Discussion
Our study demonstrated that for patients undergoing VATS lobectomy, PIEB interval of approximately 100 minutes using 10 mL of 0.15% ropivacaine combined with 0.4 μg/mL sufentanil provided effective analgesia for 90% of patients during the first 24 postoperative hours. This regimen corresponds to an hourly ropivacaine consumption of 9 mg.
Previous randomized controlled trials investigating PIEB versus CEI for post-thoracic surgery analgesia have employed varying PIEB protocols. Higashi et al10 utilized a regimen of 5 mL 0.2% ropivacaine with 2 μg/mL fentanyl administered at 90 minute intervals. Notably, all patients in their PIEB group required supplemental PCEA and failed to achieve the effective analgesia threshold as defined in our current study. In contrast, Lee et al11 implemented a 180 minute interval protocol using 3 mL of 0.2% levobupivacaine with 3 μg/mL fentanyl, reporting a mean PCEA usage of 16.3 ± 8.3 times during the 48-hour postoperative period. Given these substantial protocol variations in existing literature, we selected a time range of 90–180 minutes based on prior studies and systematically evaluated four distinct intervals. Our study employed a PIEB regimen featuring 10 mL of 0.15% ropivacaine combined with 0.4 μg/mL sufentanil, delivered at a fixed infusion rate of 300 mL/h. This larger bolus volume compared to previous thoracic PIEB regimens was specifically designed to: (1) ensure adequate ropivacaine delivery for sustained analgesia, (2) minimize breakthrough pain, and (3) reduce or eliminate the need for supplemental PCEA.
Our findings indicated that shorter PIEB intervals (90 minutes) might be associated with an increased incidence of hypotension compared to longer intervals. However, the small sample size in our study limited the generalizability of these results, necessitating further investigation in larger cohorts. Future research should also explore whether reducing the bolus volume while maintaining the PIEB interval can preserve analgesic efficacy while potentially mitigating hypotensive effects.
It could be argued that the EI90 dose may have been excessive for certain patients. This study aimed to investigate the pharmacodynamic properties of PIEB when used as the sole analgesic technique following thoracic surgery. In prior studies, the concurrent use of PCEA with PIEB introduced a confounding variable, obscuring the desired pharmacodynamic data. While the EI90 might lead to a mild overdose in some individuals, it could also reduce the risk of breakthrough pain and the consequent need for repeated PCEA interventions.
A meta-analysis determined that the minimal clinically important difference (MCID) for QoR-15 scores was 6.15 However, given the small sample size in this study, whether varying time intervals influence postoperative QoR-15 scores remains to be confirmed in randomized controlled trials.
Our study has several limitations. First, the cohort exclusively comprised patients undergoing VATS lobectomy for lung cancer; thus, the findings may not generalize to other thoracoscopic procedures or open thoracotomy. Second, the observed EI90 likely reflects the specific combination of 0.15% ropivacaine and 0.4 μg/mL sufentanil. Despite equivalent hourly doses of local anesthetic, differences in drug concentration, bolus volume, and infusion rate could yield divergent EI90 values. Furthermore, the EI90s of analgesic combinations of different types of local anesthetic drugs and opioids required further investigation. For instance, bupivacaine had been demonstrated to exhibit disparate analgesic efficacy and pharmacological properties compared to ropivacaine in epidural analgesia,16,17 which could potentially result in disparate EI90s. Finally, as patient assessments were limited to the first 24 hours post-loading dose, later variations in local anesthetic requirements could further influence EI90 determinations.
Conclusion
Our study estimated the EI90 interval for PIEB with 10 mL of 0.15% ropivacaine plus 0.4 μg/mL sufentanil to be approximately 100 minutes in patients undergoing VATS lobectomy. While these findings provided initial pharmacodynamic data for this specific regimen, further validation through large-scale randomized controlled trials was warranted to confirm its clinical applicability across different surgical populations and analgesic combinations.
Data Sharing Statement
The individual deidentified participant data, the study protocol, and the statistical analysis plan can be accessed from the corresponding author (Renchun Lai, [email protected]) upon reasonable request.
Acknowledgment
We would like to thank the nursing staff and the clinical partners who were not directly involved in conducting this trial but without whom its successful completion would not have been possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no known competing financial interests or personal relationships that influenced this study.
References
1. Joshi GP, Bonnet F, Shah R, et al. A systematic review of randomized trials evaluating regional techniques for postthoracotomy analgesia. Anesth Analg. 2008;107:1026–1040. doi:10.1213/01.ane.0000333274.63501.ff
2. Rjc van den B, Jmc P, Jsha K, et al. Continuous erector spinae plane block versus thoracic epidural analgesia in video-assisted thoracoscopic surgery: a prospective randomized open-label non-inferiority trial. Reg Anesth Pain Med. 2025;50:11–19. doi:10.1136/rapm-2023-105047
3. Carvalho B, George RB, Cobb B, McKenzie C, Riley ET. Implementation of programmed intermittent epidural bolus for the maintenance of labor analgesia. Anesth Analg. 2016;123:965–971. doi:10.1213/ANE.0000000000001407
4. Chua SM, Sia AT. Automated intermittent epidural boluses improve analgesia induced by intrathecal fentanyl during labour. Can J Anesth. 2004;51:581–585. doi:10.1007/BF03018402
5. Capogna G, Camorcia M, Stirparo S, Farcomeni A. Programmed intermittent epidural bolus versus continuous epidural infusion for labor analgesia: the effects on maternal motor function and labor outcome. A randomized double-blind study in nulliparous women. Anesth Analg. 2011;113:826–831. doi:10.1213/ANE.0b013e31822827b8
6. Fettes PD, Moore CS, Whiteside JB, McLeod GA, Wildsmith JA. Intermittent vs continuous administration of epidural ropivacaine with fentanyl for analgesia during labour. Br J Anesth. 2006;97:359–364. doi:10.1093/bja/ael157
7. Wong CA, Ratliff JT, Sullivan JT, Scavone BM, Toledo P, McCarthy RJ. A randomized comparison of programmed intermittent epidural bolus with continuous epidural infusion for labor analgesia. Anesth Analg. 2006;102:904–909. doi:10.1213/01.ane.0000197778.57615.1a
8. Wong CA, McCarthy RJ, Hewlett B. The effect of manipulation of the programmed intermittent bolus time interval and injection volume on total drug use for labor epidural analgesia: a randomized controlled trial. Anesth Analg. 2011;112:904–911. doi:10.1213/ANE.0b013e31820e7c2f
9. Sia AT, Lim Y, Ocampo C. A comparison of a basal infusion with automated mandatory boluses in parturient-controlled epidural analgesia during labor. Anesth Analg. 2007;104:673–678. doi:10.1213/01.ane.0000253236.89376.60
10. Higashi M, Shigematsu K, Nakamori E, Sakurai S, Yamaura K. Efficacy of programmed intermittent bolus epidural analgesia in thoracic surgery: a randomized controlled trial. BMC Anesthesiol. 2019;19:107. doi:10.1186/s12871-019-0780-0
11. Lee SS, Baek JH, Park SJ, Kim HJ, Kim HY, Byeon GJ. Comparison of programmed intermittent epidural bolus injection and continuous epidural injection in controlling nighttime pain and improving sleep quality after thoracotomy. Medicine. 2022;101:e31684. doi:10.1097/MD.0000000000031684
12. Huang C, Chen Y, Kou M, et al. Evaluation of a modified ultrasound-assisted technique for mid-thoracic epidural placement: a prospective observational study. BMC Anesthesiol. 2024;24:31. doi:10.1186/s12871-024-02415-x
13. Stylianou M, Flournoy N. Dose finding using the biased coin up-and-down design and isotonic regression. Biometrics. 2002;58:171–177. doi:10.1111/j.0006-341X.2002.00171.x
14. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107:144–152. doi:10.1097/01.anes.0000267514.42592.2a
15. Kleif J, Waage J, Christensen KB, Gögenur I. Systematic review of the QoR-15 score, a patient- reported outcome measure measuring quality of recovery after surgery and anaesthesia. Br J Anesth. 2018;120:28–36. doi:10.1016/j.bja.2017.11.013
16. Heid F, Schmidt-Glintzer A, Piepho T, Jage J. Epidural ropivacaine -- where are the benefits? A prospective, randomized, double-blind trial in patients with retropubic prostatectomy. Acta Anesthesiol Scand. 2007;51:294–298. doi:10.1111/j.1399-6576.2006.01259.x
17. Ngan Kee WD, Ng FF, Khaw KS, Tang SPY, Koo AGP. Dose-response curves for intrathecal bupivacaine, levobupivacaine, and ropivacaine given for labor analgesia in nulliparous women. Reg Anesth Pain Med. 2017;42:788–792. doi:10.1097/AAP.0000000000000657
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.