Back to Journals » Drug Design, Development and Therapy » Volume 20
Optimal Piperacillin/Tazobactam Dosing in Adults with Low Body Weight: A Population Pharmacokinetic and Simulation-Based Study
Authors Tseng YJ, Juan L ![]() , Tai CH, Wu CC
, Tai CH, Wu CC ![]()
Received 26 February 2026
Accepted for publication 29 April 2026
Published 5 May 2026 Volume 2026:20 602835
DOI https://doi.org/10.2147/DDDT.S602835
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Yu-Ju Tseng,1,2 Liang Juan,2,3 Chih-Hsun Tai,1,2 Chien-Chih Wu1,2
1Department of Pharmacy, National Taiwan University Hospital, College of Medicine, National Taiwan University, Taipei, Taiwan; 2School of Pharmacy, College of Medicine, National Taiwan University, Taipei, Taiwan; 3Department of Clinical Pharmacology and Therapeutics, Kyoto University Hospital, Kyoto, Japan
Correspondence: Chien-Chih Wu, Department of Pharmacy, National Taiwan University Hospital, College of Medicine, National Taiwan University, 7 Chung Shan S. Road, Taipei, Taiwan, Email [email protected]
Background: Pharmacokinetic (PK) evidence for optimal piperacillin/tazobactam (TZP) dosing in adults with low body weight (LBW) is limited, and current dosing strategies are typically extrapolated from general populations. Physiological alterations associated with LBW including reduced muscle mass, altered body water distribution and potential for impaired renal function may affect drug exposure, increasing the risk of subtherapeutic treatment or toxicity. This study developed a population PK model of TZP in adults with LBW, and dosing strategies in this population were evaluated on the basis of efficacy and neurotoxicity considerations.
Methods: Adults with a body mass index ≤ 18.5 kg/m2 receiving TZP were enrolled in a prospective observational study. Plasma piperacillin concentrations obtained during therapeutic drug monitoring were analyzed through nonlinear mixed-effects modeling. Structural models and covariates, particularly estimated renal function, were evaluated. Monte Carlo simulations were performed to assess the probability a patient would achieve the PK/PD target of 100% time above the minimum inhibitory concentration (100% fT > MIC). To evaluate safety, the probability that piperacillin would exceed a trough concentration of 361 mg/L associated with drug-related neurotoxicity was assessed.
Results: This study included 29 patients (55 samples). A one compartment model adequately described piperacillin PK, and renal function estimated according to the 2021 CKD-EPI creatinine-cystatin C equation best explained piperacillin clearance. Body weight did not significantly improve model performance. The estimated typical values were 4.89 L/hr [relative standard error (RSE) 19.0%] for clearance and 11.95 L (RSE 36.5%) for volume of distribution, with an eGFR exponent of 1.12 on clearance. In addition, simulations indicated that prolonged infusion and increased dosing frequency improved target attainment, particularly at higher MICs and in patients with preserved or augmented renal clearance. Conversely, patients with renal dysfunction achieved PK/PD targets at lower dosing regimens and exhibited a reduced likelihood of exceeding the neurotoxicity threshold.
Conclusion: In adults with LBW, renal function and PK/PD principles should guide TZP dosing. Model-informed strategies to optimize infusion duration and dosing frequency may improve efficacy and limit neurotoxicity.
Keywords: piperacillin/tazobactam, low body weight, population pharmacokinetics, monte carlo simulation
Introduction
Piperacillin/tazobactam (TZP) is a broad-spectrum antimicrobial agent widely used to treat severe community-acquired and nosocomial infections, including sepsis, pneumonia, and intra-abdominal infections.1,2 Piperacillin exhibits time-dependent bactericidal activity. The pharmacokinetic/pharmacodynamic (PK/PD) index value most closely associated with bactericidal efficacy is the proportion of the dosing interval during which free drug concentrations exceed the minimum inhibitory concentration (fT > MIC).3 In critically ill patients, providers may recommend more aggressive targets, such as 100% fT > MIC or even 100% fT > 4 × MIC, to maximize bacterial killing and suppress resistance.4,5 Piperacillin is a hydrophilic compound with limited protein binding that is predominantly eliminated through renal excretion, rendering piperacillin exposure highly sensitive to changes in renal function, volume of distribution (Vd), and infusion strategy.6 Consequently, prolonged or continuous infusion regimens have been increasingly adopted to improve PK/PD target attainment, particularly in patients with augmented renal clearance or high pathogen MICs.7 Given the significant PK variability and the risk of underexposure in this subpopulation, individualized dosing regimens guided by renal function are crucial to optimize therapeutic outcomes.8
In adults, TZP is administered through a fixed dosing regimen; however, body weight substantially affects the PK parameters of TZP. In patients with obesity, multiple population PK studies have demonstrated an elevated piperacillin Vd, with this elevation largely driven by increased extracellular fluid and cardiac output.9 Chung et al reported an approximately 25% to 40% increase in piperacillin Vd in patients with compared with in those without obesity; clearance (CL) was modestly elevated and strongly correlated with creatinine CL (CLCr) rather than total body weight.6 These PK alterations translate into lower peak concentrations and an increased risk of subtherapeutic exposure, particularly under standard intermittent infusions.
In contrast to those for patients with obesity, PK data for patients with low body weight (LBW) are limited. LBW is frequently associated with reduced muscle mass, altered total body water composition, hypoalbuminemia, and decreased renal CL. These physiological alterations may predispose patients to either supratherapeutic drug concentrations and toxicity or to subtherapeutic exposure, given the greater Vd in critical illness settings.4,10,11 Importantly, alterations in body size and composition may also lead to systematic differences in drug CL that are not adequately captured by conventional weight-based scaling. In a comparative population PK study, unscaled total CL and Vd were substantially lower in patients with reduced body size, primarily reflecting differences in body composition rather than intrinsic elimination capacity.12 Although these factors may contribute PK variability, relevant antibiotic PK data and concentration distribution in patients with low body weight remain limited. In a large analysis of adults receiving aminoglycosides, including underweight patients with a body mass index (BMI) as low as 11.3 kg/m2, the Vd indexed to total body weight or ideal body weight varied substantially across weight strata, whereas only lean body weight provided a stable estimate across the full BMI range, indicating that standard weight-based extrapolation misrepresents drug distribution in patients at weight extremes.13 Similarly, a retrospective study of patients receiving vancomycin reported that the dose required to attain an area under the concentration-time curve (AUC) of 400 μg·h/mL was substantially higher in underweight than in obese elderly patients with preserved renal function, underscoring that actual body weight based dosing guidelines may systematically underdose underweight individuals.14 Furthermore, a prospective observational study in individuals with LBW receiving TZP demonstrated considerable interindividual variability. A substantial proportion of participants failed to achieve PK/PD targets despite receiving standard dosing.15 Notably, population PK models specific to LBW adults are lacking, and dosing recommendations remain reliant on extrapolations from normal-weight or obese populations. In this study, we developed a population PK model for TZP in adults with LBW and performed Monte Carlo simulations to tailor dosing strategies to renal function, enabling safer and more effective therapy.
Methods
Study Design and Population
This prospective observational PK study was conducted at National Taiwan University Hospital (NTUH) between January 2020 and December 2022. Adult patients aged 20 years or older (reflecting the legal definition of adulthood in Taiwan at the time of enrollment) with a BMI of 18.5 kg/m2 or lower who received TZP were eligible for inclusion. Patients who developed acute kidney injury during antibiotic therapy or required renal replacement therapy for acute illness were excluded. This study protocol was approved by the Institutional Review Board (approval number: 201907124RINC) of NTUH, and informed consent was acquired from all participants or a legal representative before enrollment. This study was conducted in accordance with the Declaration of Helsinki.
The demographic and clinical data that were collected on the day of therapeutic drug monitoring (TDM) included age, sex, height, body weight, serum creatinine level, serum cystatin C level, comorbidities, Charlson Comorbidity Index score, and intensive care unit (ICU) admission. TZP-related data, including dose, dosing interval, and infusion duration, were also recorded.
Drug Administration and Sampling
At our institution, TZP dosing is primarily guided by renal function, with a standard infusion regimen of 4500 mg every 6 hours for 1 hour administered to patients with a CLCr ≥ 40 mL/min. Dose modifications related to LBW were not protocolized and were left to the clinical judgment of the treating physician. Blood samples were obtained for PK analysis after administration of at least four consecutive doses to ensure a steady-state condition. Two samples were randomly collected within a dosing interval. Total plasma concentrations of piperacillin were measured, and the total concentrations were multiplied by the reported unbound fraction of 0.7 to determine free drug concentrations.
Bioanalytical Assay
Total plasma concentrations of piperacillin were quantified through a validated ultra high-performance liquid chromatography–electrospray ionization–tandem mass spectrometry method. Plasma samples were prepared through protein precipitation with acetonitrile followed by centrifugation. TZP-d5 was used as the internal standard. The supernatant was diluted with deionized water before analysis. Chromatographic separation was performed on an Agilent 1290 ultra high-performance liquid chromatography system coupled to a QTrap 6500 triple quadrupole mass spectrometer (Sciex) with a Kinetexbiphenyl column (2.1 × 100 mm, 2.6 μm). The mobile phase consisted of 0.1% formic acid in water and methanol, delivered at a flow rate of 0.5 mL/min with gradient elution. Detection was conducted in positive ionization mode through scheduled multiple reaction monitoring.
Population PK Modeling
For population PK analysis, we performed nonlinear mixed-effects modeling in Monolix (version 2024R1; Lixoft, Antony, France).16 One- and two-compartment structural models with first order elimination were evaluated. Exponential error models were used to capture interindividual variability, and residual unexplained variability was assessed through additive, proportional, and combined error structures.
Covariate analysis involved a stepwise forward inclusion and backward elimination approach. Candidate covariates included age, sex, BMI, total body weight, CLCr (calculated according to the Cockcroft–Gault equation), and the estimated glomerular filtration rate (derived from the 2012 CKD-EPI Cystatin C Equation [eGFRCys] and 2021 CKD-EPI Creatinine-Cystatin C Equation [eGFRCre-Cys]).17–19 Body weight was evaluated using allometric scaling with fixed exponents of 0.75 on CL and 1.0 on Vd, consistent with established allometric theory. Covariates were retained on the basis of whether they caused a reduction in the objective function value (OFV) of at least 3.84 (p < 0.05) during forward inclusion and an increase of more than 6.63 (p < 0.01) during backward elimination.
Standard diagnostic procedures were performed to assess model performance, including observed versus predicted concentration plots, individual weighted residuals, and visual predictive check. This study noted an absence of systematic bias and concordance between observed and simulated concentrations that indicated model adequacy.
Monte Carlo Simulations
Monte Carlo simulations were performed with Simulx (version 2024R1; Lixoft, Antony, France) to evaluate the probability of target attainment (PTA) across a range of dosing regimens. The primary PK/PD target was set at 100% fT > MIC, consistent with current international recommendations for β-lactam therapy in critically ill patients and supported by clinical outcome data indicating improved cure rates when this stringent target is achieved.5,20 Pseudomonas aeruginosa was selected as the reference pathogen because it is one of the most common and virulent Gram-negative organisms causing nosocomial infections, is associated with substantially elevated mortality in critically ill patients, and presents one of the most demanding PK/PD dosing challenges among pathogens typically covered by empirical TZP therapy.21 The clinical breakpoint for this pathogen was therefore adopted as the target MIC to provide conservative dosing guidance applicable across a broad pathogen spectrum. A total of 1000 virtual patients were simulated per scenario. Target attainment was defined on the basis of the final simulated trough concentration for each individual. Under the assumption of a one compartment model with first order elimination and monotonic concentration decline between doses, the simulated free concentration at the end of each dosing interval (trough) represents the minimum exposure. Therefore, a trough free concentration exceeding the MIC implies that the free concentration remained above the MIC throughout the entire dosing interval, satisfying the 100% fT > MIC target. Target attainment was accordingly defined on the basis of the final simulated trough free concentration for each virtual patient.
Simulated dosing regimens spanned piperacillin doses of 2250 mg every 12 hours to 4500 mg every 6 hours, with these administered as either intermittent infusions (1 hour) or prolonged infusions (4 hours). Additional simulations were conducted to quantify the probability that piperacillin would exceed a trough concentration of 361 mg/L. This threshold was reported to be associated with a 50% risk of piperacillin-related neurotoxicity.22 Regimens with a probability >10% of exceeding this threshold were flagged on the heatmap as an indicator of elevated safety concern. The 10% cutoff was selected as a pragmatic safety signal, consistent with the conventional 90% probability benchmark used for PK/PD target attainment in simulation-based studies. All simulations were performed under the assumption of no interindividual variability in covariates, a simplifying approach adopted to isolate the effect of renal function strata on dosing requirements and produce interpretable dosing heatmaps. The robustness of PTA results in regard to the parameter variabilities was evaluated using the parameter uncertainty propagation analysis.
Results
Patient Characteristics
A total of 29 adults with 55 blood samples were included in the final PK analysis. Only one blood sample was collected from three patients because of clinical care–related constraints. The cohort predominantly comprised older adults, with a median age of 64 years, and approximately half of the patients were men. The median body weight was 42 kg, indicating pronounced LBW, and one-fifth of the participants had a BMI of 15 kg/m2 or lower. The participants’ baseline characteristics are summarized in Table 1.
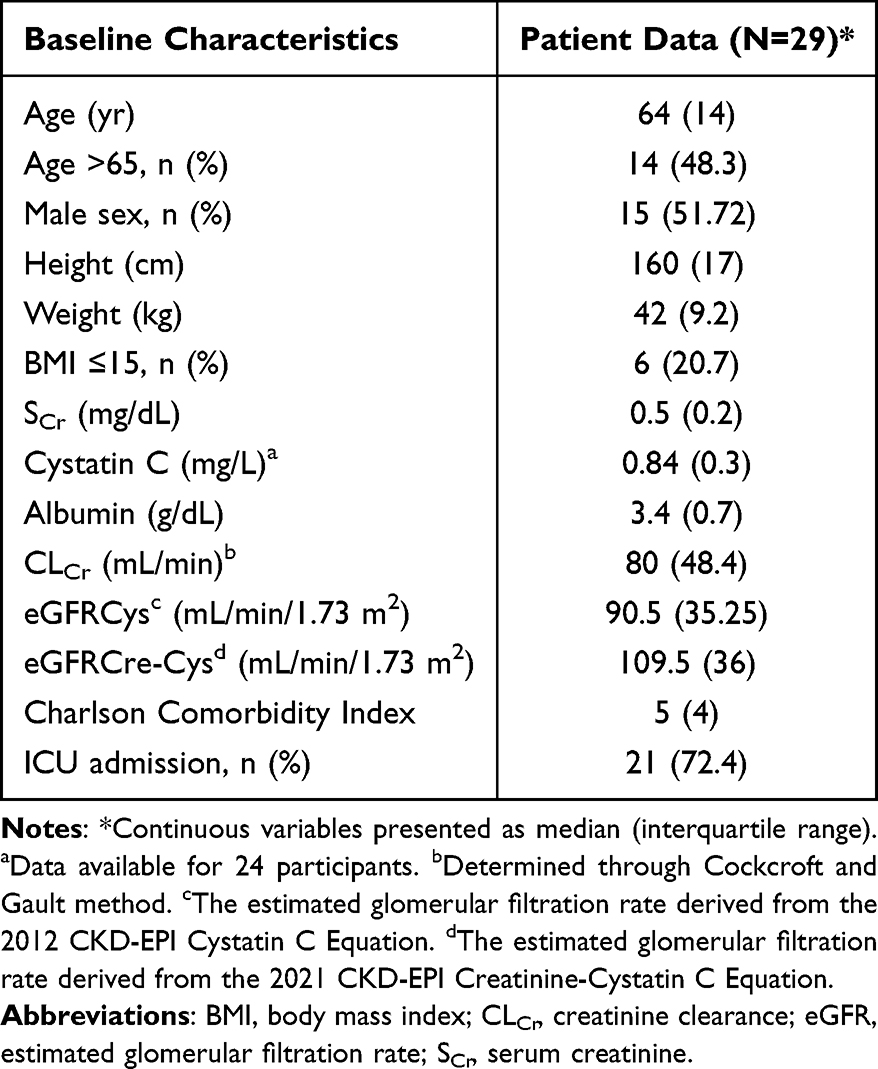 |
Table 1 Demographic and Clinical Characteristics of Enrolled Patients |
Population PK Modeling
A one compartment model with first order elimination and a proportional residual error structure adequately described piperacillin PK. (Supplementary Table 1) The base model supported interindividual variability in CL and Vd. In the covariate analysis, renal function indices for CL significantly improved model performance. Log transformed CLCr, eGFRCys, and eGFRCre-Cys yielded OFV reductions of 6.48, 10.50, and 12.13, respectively. The eGFRCre-Cys provided the greatest improvement in model fit and was therefore selected as the renal function descriptor for CL in the final model. (Supplementary Table 2) No additional covariates met the predefined criteria for retention after adjustment for renal function.
The final population PK model incorporated eGFRCre-Cys as a covariate descriptor of CL, which we modeled using a power function normalized to the median eGFR value (CL = tvCL × (eGFR/104.368)βCL × expηCL. Vd was input as a fixed parameter without covariates (V = tvV). Given the excessive shrinkage (83.2%) observed for interindividual variability in Vd, this random effect was removed from the final model. Incorporating renal function reduced unexplained interindividual variability in CL. The parameter estimates for the final model are summarized in Table 2.
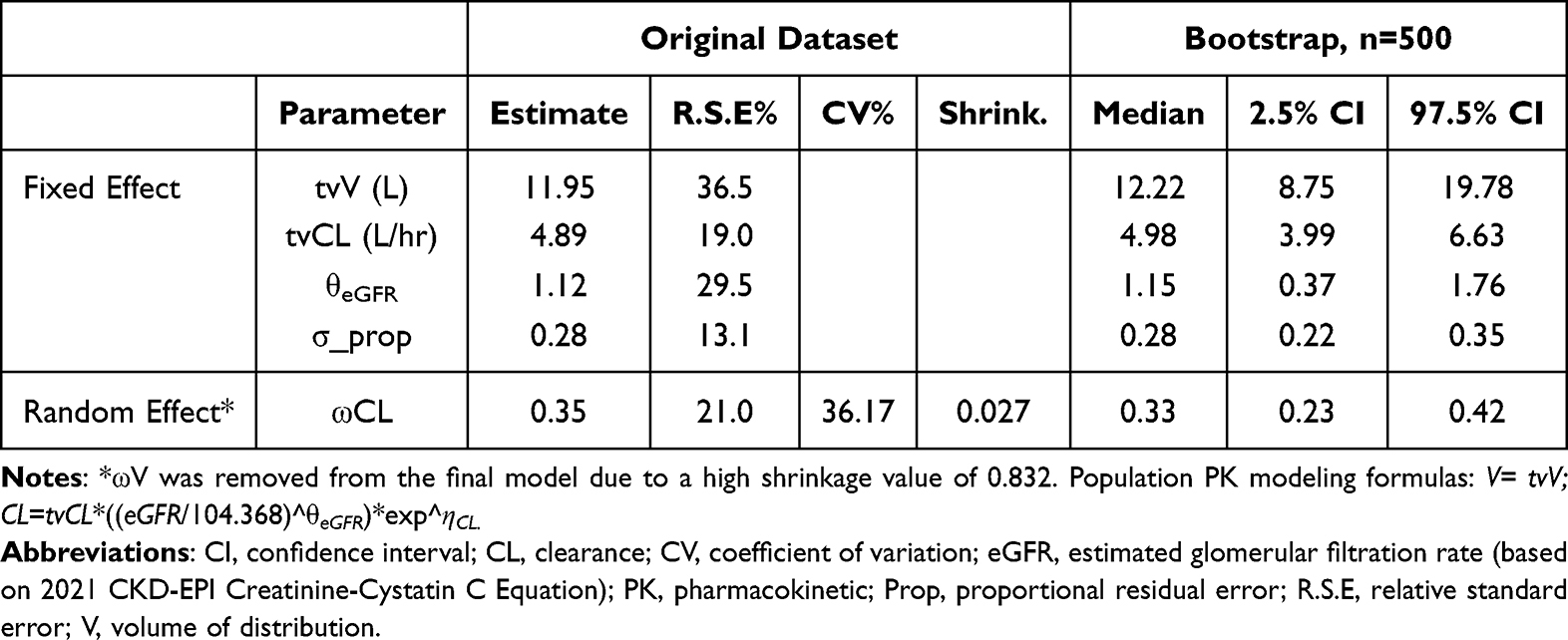 |
Table 2 Parameter Estimates of Final Population PK Model of Piperacillin in Adults with Low Body Weight |
Goodness of fit diagnostics indicated acceptable model performance. Observed concentrations demonstrated good agreement with both population- and individual-level predicted concentrations without evidence of systematic bias (Figure 1). Individual weighted residuals were symmetrically distributed near zero across timepoints after dose and predicted concentrations, indicating no significant model misspecification (Figure 2). Visual predictive checks based on 1000 Monte Carlo simulations indicated that the median and 5th to 95th percentile prediction intervals adequately captured the central tendency and variability of the observed concentration–time data (Supplementary Figure 1), supporting the adequacy of the final model.
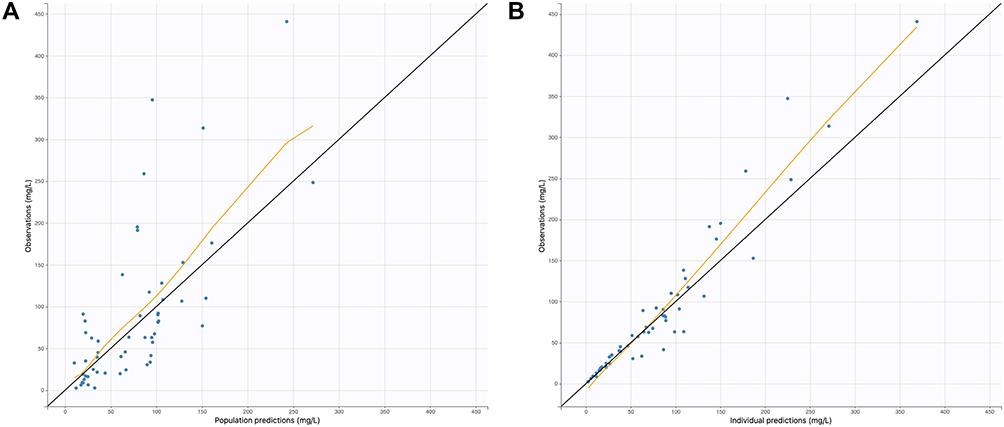 |
Figure 1 Goodness-of-fit plots for final population pharmacokinetic model. (A) Observed vs population-predicted concentrations. (B) Observed vs individual-predicted concentrations. |
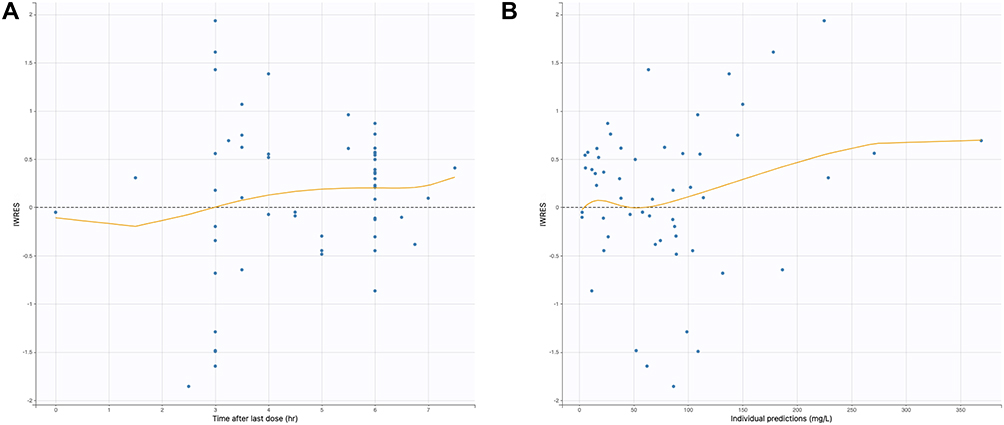 |
Figure 2 Individual weighted residuals (IWRES) versus time and predicted concentrations in the final population pharmacokinetic model. (A) IWRES vs. time. (B) IWRES vs. individual predictions. |
Monte Carlo Simulations for Target Attainment and Neurotoxicity
We performed Monte Carlo simulations for TZP by using the final population PK model, revealing marked variability in the PTA across dosing regimens, infusion strategies, MIC values, and renal function strata (Figure 3, Supplementary Figure 2 and 3). Intermittent infusion at a total daily dose of 2250 mg administered every 12 hours was associated with a rapid decline in PTA as MIC increased, particularly in patients with preserved renal function. Prolonged infusion at the same dosing frequency improved PTA at lower MIC values but remained insufficient at MIC ≥ 16 mg/L in patients with a high eGFR. A dosing frequency of every 6–8 hours increased the PTA across renal function categories, with prolonged infusion consistently outperforming intermittent infusion, especially at MIC values of 8–16 mg/L. However, in patients with eGFR > 100 mL/min/1.73 m2, prolonged infusion of 3375–4500 mg every 6 hours was required to achieve optimal PTA.
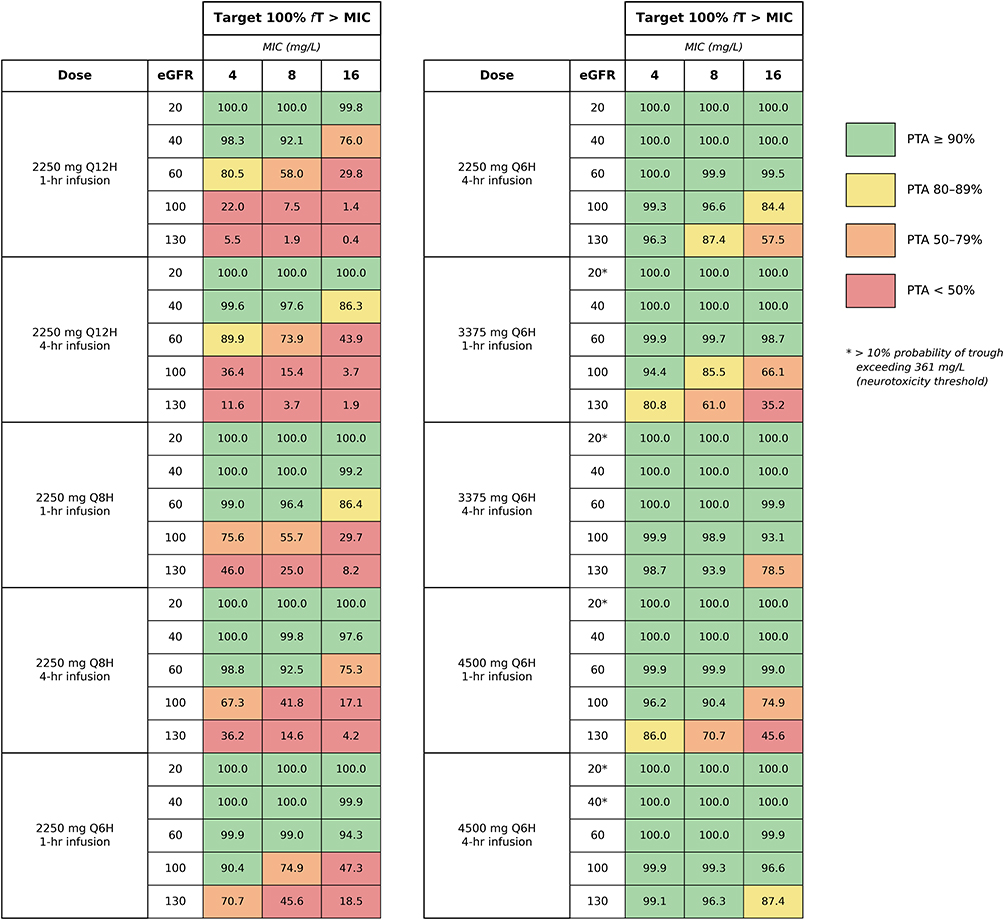 |
Figure 3 Probability of target attainment (100% fT>MIC) at different MIC values and neurotoxicity risk for piperacillin under different dosing regimens and renal function strata. *>10% probability of trough concentrations exceeding 361 mg/L. |
Across simulated scenarios, the probability of piperacillin exceeding the trough concentration threshold associated with drug-related neurotoxicity was generally low. Nevertheless, higher total daily doses administered as prolonged infusions were associated with an increased probability of threshold crossing, particularly in patients with reduced renal function (eGFR ≤ 40 mL/min/1.73 m2), indicating a trade-off between optimal target attainment and elevated systemic exposure (Figure 3).
Parameter Uncertainty Propagation Analysis
To evaluate the robustness of the primary PTA estimates to imprecision in the estimated PK parameters, uncertainty propagation was performed in Simulx with 100 replicates. The analysis revealed a consistent pattern: when a dosing regimen was appropriately matched to a patient’s renal function stratum, the 95% confidence interval (CI) of the PTA was narrow, supporting the reliability of the model based recommendation. In contrast, when a regimen was mismatched to renal function, the 95% CI widened substantially, indicating that parameter uncertainty could not support that regimen for the given renal function category. For example, TZP 2250 mg q12h produced reliable PTA estimates only in patients with eGFR ≤ 20 mL/min/1.73 m2, whereas TZP 4500 mg q6h as prolonged infusion produced reliable estimates in patients with eGFR ≥ 60 mL/min/1.73 m2 (Supplementary Table 3).
Discussion
We developed a population PK model of TZP in adults with LBW and evaluated optimal dosing strategies through Monte Carlo simulations. Renal function, which was best captured by the eGFRCre-Cys metric, was the primary determinant of piperacillin CL. Body weight did not independently contribute to PK variability after consideration of renal function. Simulation analyses further indicated that the dosing frequency and infusion strategy rather than the total daily dose alone primarily influenced the attainment of stringent PD targets. Prolonged infusion and more frequent dosing substantially increased the probability that a patient would achieve 100% fT > MIC, particularly in individuals with preserved or augmented renal CL. Excessive dose escalation was associated with an increased risk of supratherapeutic exposure in patients with impaired renal function. Collectively, these findings underscore the need to consider renal function in PK/PD-guided dosing strategies for TZP in adults with LBW.
We observed a comparable Vd but generally lower CL in this study relative to values reported in other studies for the general adult population.12,23 While direct pathophysiological analogies should be drawn cautiously, the observation by Bulitta et al that piperacillin PK differences between cystic fibrosis patients and healthy volunteers largely disappeared after normalization to lean body mass is mechanistically relevant in supporting the broader principle that body size and composition can substantially explain PK variability that may otherwise be attributed to disease-specific factors.12 Population PK studies of patients with and without obesity further support the effects of extreme body size on piperacillin PK. Chung et al reported an approximately 25% to 40% elevation in piperacillin Vd in patients with versus without obesity, whereas CL was only modestly higher and remained primarily driven by renal function.6 These alterations resulted in lower peak concentrations and an increased risk of subtherapeutic exposure under standard dosing regimens. In consideration of these findings, the absence of body weight as a significant covariate in our model is likely attributable to the restricted body weight range of our cohort, which exclusively included patients with LBW. Although significant weight-related effects could not be identified within this population, evidence indicates that both high and low extreme body size can meaningfully alter piperacillin PK, indicating a need for individualized dosing strategies rather than uniform fixed dosing in these patient groups.6,12
Renal function was the greatest determinant of piperacillin CL in our population PK model. Among the renal function descriptors we evaluated, eGFRCre-Cys best characterized the interindividual variability in CL. This finding is physiologically plausible, given that serum creatinine is largely derived from skeletal muscle metabolism and is therefore strongly influenced by body weight and muscle mass.24 In patients with LBW or sarcopenia, creatinine-based equations may overestimate the eGFR, potentially mischaracterizing renal drug elimination. By contrast, cystatin C is produced at a relatively constant rate by all nucleated cells and is minimally affected by muscle mass or body composition, rendering it a more robust marker of renal function in this population.25 Previous PK studies have demonstrated that cystatin C–based renal function estimates correlate more closely than the results of creatinine-based equations do with the CL of renally eliminated drugs, such as gentamicin and vancomycin.26,27 Cystatin C–based renal function assessment has also been associated with improved vancomycin target attainment and a lower incidence of cefepime-related neurotoxicity.28,29 Collectively, these findings support the use of cystatin C–based renal function evaluation to guide piperacillin dosing in patients with LBW. This approach can enable optimization of PK/PD target attainment and minimization of toxicity risk.
Our Monte Carlo simulation results indicated that relative to the general adult population, the dosing requirements for TZP in patients with LBW differ according to renal function. In patients with impaired renal function (eGFR < 40 mL/min/1.73 m2), slightly lower doses were sufficient to achieve pharmacodynamic targets, reflecting reduced CL and an increased susceptibility to drug accumulation in this population.30 Conversely, in patients with LBW and preserved renal function (eGFR > 60 mL/min/1.73 m2), dosing requirements were largely comparable to those recommended for general adult populations, suggesting that LBW alone does not necessitate routine dose reduction in the presence of normal renal function. Simulation analyses further indicated that in patients with preserved or augmented renal CL, prolonged infusion was essential to attain PK/PD targets and prevent excessive exposure.31 Prolonged infusion stabilized plasma concentrations, increasing the probability that stringent targets, such as 100% fT > MIC, would be achieved. Conversely, intermittent administration was associated with greater variability and a higher risk of either subtherapeutic exposure or drug accumulation.20 Implementation of prolonged infusion, however, requires reliable and dedicated intravenous access, which may be challenging in LBW patients with limited venous reserves. Additionally, drug compatibility must be carefully considered when administering concomitant medications.
β-Lactam induced neurotoxicity occurs in approximately 10–15% of ICU patients and encompasses a wide spectrum of clinical manifestations, ranging from confusion, encephalopathy, and hallucinations to myoclonus, convulsions, and non-convulsive status epilepticus.32 These manifestations are often underdiagnosed in the ICU setting because they overlap with conditions commonly observed in critically ill patients, such as delirium, sepsis-associated encephalopathy, and metabolic disturbances, making prompt recognition clinically challenging; therefore, TDM represents a feasible alternative approach.33 Although we applied a relatively broad toxicity threshold, total piperacillin concentrations approaching 150 mg/L should prompt dosing reassessment, even in the absence of overt neurological symptoms.34 It should be acknowledged that the neurotoxicity threshold of 361 mg/L applied in our simulations is subject to substantial uncertainty. Lower concentration thresholds (157.2 mg/L) associated with neurotoxicity have also been described in the literature among critically ill patients receiving continuous TZP infusion.35 The variability among published thresholds likely reflects differences in patient populations, infusion regimens, analytical methods, and definitions of neurotoxic events. Accordingly, the toxicity predictions derived from our simulations should be interpreted with caution. The probability of trough concentrations exceeding 361 mg/L should therefore be regarded as an indicative safety signal rather than a definitive predictor of neurotoxicity risk. Given the narrow margin between efficacy and toxicity in patients with LBW, routine TDM is an integral component of piperacillin therapy in this population.15 TDM enables individualized dose adjustment to ensure adequate PK/PD target attainment and minimize the risk of toxic drug exposure, ensuring safer TZP treatment in patients with LBW.
Several limitations of this study should be acknowledged. First, the single-center design, relatively small sample size, and limited number of PK samples per patient may have limited the precision of our parameter estimation and constrained the generalizability of the findings. Nevertheless, the study population was well-characterized, and the final model demonstrated acceptable goodness of fit and stability, supporting the validity of the primary PK conclusions. Second, the study cohort exclusively comprised patients with LBW, with a narrow range for patient body size. This design was selected to address our specific research question but limited our ability to formally identify body weight as a covariate within PK parameters. Consequently, we could only perform indirect comparisons with normal-weight and obese populations reported on in previously published studies rather than with internal controls. Future prospective multicenter population PK studies enrolling patients across the full body weight spectrum are needed to provide the statistical power required to formally identify body weight as an independent PK covariate after adjustment for renal function. Furthermore, patients who developed acute kidney injury or required renal replacement therapy were excluded to maintain stable renal function for PK parameter estimation. While this design choice improves the reliability of the model, it limits the generalizability of our findings to critically ill LBW patients with unstable or rapidly changing renal function, who may represent a particularly high-risk subgroup warranting tailored investigation in future studies. Third, LBW was defined solely on the basis of BMI ≤ 18.5 kg/m2 in accordance with WHO classification. While this approach is practical and widely applied, BMI does not fully capture variations in body composition such as sarcopenia, cachexia, or altered fat-free mass, which are particularly relevant in the elderly cohort represented in this study. Future studies incorporating direct measures of body composition may better characterize the PK impact of specific body composition alterations in this population. Fourth, the use of a fixed unbound fraction to derive free piperacillin concentrations represents a simplification because free piperacillin concentrations were not measured in this study. Although piperacillin is a low to moderately protein-bound antibiotic and albumin variability has been shown to have limited influence on its unbound fraction in critically ill patients,36 hypoalbuminemia in LBW patients could theoretically introduce some variability in free drug exposure that is not captured by our model. Future studies incorporating direct free-concentration measurement would help further refine PK/PD target attainment estimates in this population. Fifth, blood sampling was performed in alignment with routine clinical TDM procedures, typically yielding two samples per dosing interval at clinically convenient time points rather than through a PK-optimized sampling design. This constraint limited the ability to robustly discriminate between one and two compartment structural models. While the final one compartment model demonstrated acceptable fit and diagnostic performance, mild trends observed in the goodness of fit diagnostics including scatter at higher concentrations in the observed versus predicted plots and a slight upward trend in the locally estimated scatterplot smoothing smoother of the Individual weighted residuals (IWRES) plots are most plausibly attributable to the sparse and clinically constrained sampling design rather than to fundamental structural misspecification. Although additive, proportional, and combined residual error structures were evaluated during model development and the proportional error model provided the best overall fit, we acknowledge that the IWRES distribution exhibits a mild asymmetry with a few more extreme negative residuals. Given the limited sample size, a small number of influential data points can disproportionately shape the tails of the residual distribution. Future studies with richer sampling and larger cohorts would permit a more definitive characterization of residual error behavior. The RSE of 36.5% for Vd also reflects meaningful imprecision arising from the sparse sampling design. The selection of a one compartment model may also limit the ability to fully characterize early distribution phase and peak concentrations, particularly for prolonged infusion regimens. However, as piperacillin is a time-dependent antibiotic whose PK/PD efficacy is driven by %fT > MIC rather than Cmax, and as our primary simulation endpoint (100% fT > MIC) is determined by trough level behavior governed mainly by CL, the impact of this structural simplification on our dosing recommendations is expected to be limited. Sixth, we performed Monte Carlo simulations based on PK/PD targets and toxicity thresholds derived from the literature, which may not fully capture interindividual susceptibility to adverse effects. Although conservative assumptions were applied, neurotoxicity may develop at lower than usual concentrations in certain patients, particularly those with multiple predisposing factors. In addition, the primary Monte Carlo simulations assumed no interindividual variability in covariates, a simplification applied to generate interpretable dosing heatmaps by isolating the effect of renal function strata. Parameter uncertainty propagation was performed to address this limitation and confirmed that the dosing recommendations were robust within each renal function category when regimens were appropriately matched. Nonetheless, model informed initial dosing should be combined with TDM in clinical practice to account for individual variability not fully captured in the simulation framework. Finally, the dosing strategies proposed in this study are based on simulation results rather than prospectively validated clinical outcomes. Prospective studies incorporating standardized dosing, TDM, and clinical efficacy and safety endpoints are warranted to confirm the clinical applicability and outcome benefits of these recommendations in patients with LBW.
Conclusion
We developed a population PK model of TZP in adults with LBW, revealing renal function as the primary determinant of piperacillin CL in this population. Monte Carlo simulations indicated that prolonged infusion and increased dosing frequency were more effective than empirical dose escalation in achieving PK/PD targets in patients with preserved or augmented renal CL, whereas lower doses were sufficient in those with impaired renal function.
In routine clinical practice, these findings support a practical model-informed dosing approach for LBW patients. Cystatin C–based renal function assessment (eGFRCre-Cys) should be incorporated into initial dose selection rather than relying solely on creatinine-based equations, which may overestimate renal CL in this population with reduced muscle mass. Infusion duration and dosing frequency can then be tailored to the estimated renal function. Where institutional resources permit, routine TDM of piperacillin is recommended to confirm adequate target attainment and avoid accumulation. Where routine TDM is not feasible, selective TDM should be performed in clinical situations in which the efficacy-toxicity balance is less certain, specifically: (i) patients receiving higher than standard doses for their renal function category, in whom accumulation and neurotoxicity risk cannot be confidently excluded; (ii) patients receiving lower than standard doses, in whom adequate target attainment is not guaranteed; and (iii) patients developing acute kidney injury or receiving continuous kidney replacement therapy, whose PK is expected to deviate substantially from the population modeled in the present study, which excluded these patients. Together, this cystatin C-informed initial dosing and targeted TDM framework provides a clinically actionable strategy to optimize efficacy and minimize toxicity in this vulnerable population.
Data Sharing Statement
The datasets used and/or analyzed during the current study can be obtained from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board (201907124RINC) of NTUH, and informed consent was acquired from all participants or a legal representative before enrollment.
Acknowledgments
We would like to acknowledge the use of OpenAI’s ChatGPT (version 5.2, accessed on February 25, 2026) for assistance in translating, editing grammar, and refining the phrasing and readability of this manuscript. The AI tool was not used for data analysis, interpretation of results, or generation of scientific content. The content, analysis, and conclusions presented remain entirely the responsibility of the authors.
Funding
This study was supported by research grants from National Taiwan University Hospital (NTUH 109-S4618). The funders played no role in the study design, data collection and analysis, preparation of the manuscript, or decision to publish.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gin A, Dilay L, Karlowsky JA, Walkty A, Rubinstein E, Zhanel GG. Piperacillin-tazobactam: a beta-lactam/beta-lactamase inhibitor combination. Expert Rev Anti Infect Ther. 2007;5(3):365–12. doi:10.1586/14787210.5.3.365
2. Drawz SM, Bonomo RA. Three decades of beta-lactamase inhibitors. Clin Microbiol Rev. 2010;23(1):160–201. doi:10.1128/CMR.00037-09
3. Kim MK, Xuan D, Quintiliani R, Nightingale CH, Nicolau DP. Pharmacokinetic and pharmacodynamic profile of high dose extended interval piperacillin-tazobactam. J Antimicrob Chemother. 2001;48(2):259–267. doi:10.1093/jac/48.2.259
4. Roberts JA, Paul SK, Akova M, et al. DALI: defining antibiotic levels in intensive care unit patients: are current beta-lactam antibiotic doses sufficient for critically ill patients? Clinl Infect Dis. 2014;58(8):1072–1083. doi:10.1093/cid/ciu027
5. Abdul-Aziz MH, Alffenaar JC, Bassetti M, et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: a position paper. Intensive Care Med. 2020;46(6):1127–1153. doi:10.1007/s00134-020-06050-1
6. Chung EK, Cheatham SC, Fleming MR, Healy DP, Shea KM, Kays MB. Population pharmacokinetics and pharmacodynamics of piperacillin and tazobactam administered by prolonged infusion in obese and nonobese patients. J Clin Pharmacol. 2015;55(8):899–908. doi:10.1002/jcph.505
7. Tilanus A, Drusano G. Optimizing the use of beta-lactam antibiotics in clinical practice: a test of time. Open Forum Infect Dis. 2023;10(7):ofad305. doi:10.1093/ofid/ofad305
8. Shi A-X, Qu Q, Zhuang -H-H, et al. Individualized antibiotic dosage regimens for patients with augmented renal clearance. Front Pharmacol. 2023;Volume:14–2023. doi:10.3389/fphar.2023.1137975
9. Märtson AG, Barber KE, Crass RL, et al. The pharmacokinetics of antibiotics in patients with obesity: a systematic review and consensus guidelines for dose adjustments. Lancet Infect Dis. 2025;25(9):e504–e15. doi:10.1016/S1473-3099(25)00155-0
10. McLeay SC, Morrish GA, Kirkpatrick CM, Green B. The relationship between drug clearance and body size: systematic review and meta-analysis of the literature published from 2000 to 2007. Clin Pharmacokinet. 2012;51(5):319–330. doi:10.2165/11598930-000000000-00000
11. Jang SM, Shaw AR, Mueller BA. Size matters: the influence of patient size on antibiotics exposure profiles in critically ill patients on continuous renal replacement therapy. Antibiotics. 2021;10(11):1390. doi:10.3390/antibiotics10111390
12. Bulitta JB, Duffull SB, Kinzig-Schippers M, et al. Systematic comparison of the population pharmacokinetics and pharmacodynamics of piperacillin in cystic fibrosis patients and healthy volunteers. Antimicrob Agents Chemother. 2007;51(7):2497–2507. doi:10.1128/AAC.01477-06
13. Pai MP, Nafziger AN, Bertino JS. Simplified estimation of aminoglycoside pharmacokinetics in underweight and obese adult patients. Antimicrob Agents Chemother. 2011;55(9):4006–4011. doi:10.1128/AAC.00174-11
14. Sakurai N, Kawaguchi H, Kuwabara G, et al. Body mass index of elderly patients with normal renal function as a determining factor for initial vancomycin regimen designing. Chemotherapy. 2022;67(3):193–200. doi:10.1159/000522455
15. Tseng YJ, Tai CH, Chen GY, et al. Navigating pharmacokinetic and pharmacodynamics challenges of β-lactam antibiotics in patients with low body weight: efficacy, toxicity, and dosage optimization. Ther Adv Drug Saf. 2025;16:1–12. doi:10.1177/20420986251320414
16. Lixoft. Monolix® user guide. Antony, France: Lixoft SAS; 2024. Available from: https://monolix.lixoft.com/.
17. Inker LA, Schmid CH, Tighiouart H, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367(1):20–29. doi:10.1056/NEJMoa1114248
18. Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737–1749. doi:10.1056/NEJMoa2102953
19. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. doi:10.1159/000180580
20. Hong LT, Downes KJ, FakhriRavari A, et al. International consensus recommendations for the use of prolonged-infusion beta-lactam antibiotics: endorsed by the American College of Clinical Pharmacy, British Society for Antimicrobial Chemotherapy, Cystic Fibrosis Foundation, European Society of Clinical Microbiology and Infectious Diseases, Infectious Diseases Society of America, Society of Critical Care Medicine, and Society of Infectious Diseases Pharmacists. Pharmacotherapy. 2023;43(8):740–777. doi:10.1002/phar.2842
21. Babich T, Naucler P, Valik JK, et al. Risk factors for mortality among patients with pseudomonas aeruginosa bacteraemia: a retrospective multicentre study. Int J Antimicrob Agents. 2020;55(2):105847. doi:10.1016/j.ijantimicag.2019.11.004
22. Imani S, Buscher H, Marriott D, Gentili S, Sandaradura I. Too much of a good thing: a retrospective study of beta-lactam concentration-toxicity relationships. J Antimicrob Chemother. 2017;72(10):2891–2897. doi:10.1093/jac/dkx209
23. Batra VK, Morrison JA, Lasseter KC, Joy VA. Piperacillin kinetics. Clin Pharmacol Ther. 1979;26(1):41–53. doi:10.1002/cpt197926141
24. Kidney Disease: Improving Global Outcomes CKDWG. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4S):S117–S314. doi:10.1016/j.kint.2023.10.018
25. Teaford HR, Barreto JN, Vollmer KJ, Rule AD, Barreto EF. Cystatin C: a primer for pharmacists. Pharmacy. 2020;8(1):35. doi:10.3390/pharmacy8010035
26. Chin PK, Chew-Harris JS, Florkowski CM, Begg EJ. The performance of contemporary cystatin C-based GFR equations in predicting gentamicin clearance. Br J Clin Pharmacol. 2015;79(2):268–277. doi:10.1111/bcp.12501
27. Mohd Tahir NA, Mohd Saffian S, Islahudin FH, Abdul Gafor AH, Makmor-Bakry M. A meta-analysis on the performance of cystatin C- versus creatinine-based eGFR equations in predicting vancomycin clearance. J Korean Med Sci. 2020;35(37):e306. doi:10.3346/jkms.2020.35.e306
28. Frazee EN, Rule AD, Herrmann SM, et al. Serum cystatin C predicts vancomycin trough levels better than serum creatinine in hospitalized patients: a cohort study. Crit Care. 2014;18(3):R110. doi:10.1186/cc13899
29. Kim M-C, Kim SO, Kim S-H, et al. Efficacy and safety of cystatin C-Guided renal dose adjustment of cefepime treatment in hospitalized patients with pneumonia. J Clin Med. 2020;9(9):2803. doi:10.3390/jcm9092803
30. Sanford guide to antimicrobial therapy. Piperacillin/tazobactam. Available from: https://web.sanfordguide.com/.
31. Sjövall F, Alobaid AS, Wallis SC, Perner A, Lipman J, Roberts JA. Maximally effective dosing regimens of meropenem in patients with septic shock. J Antimicrob Chemother. 2017;73(1):191–198. doi:10.1093/jac/dkx330
32. Roger C, Louart B. Beta-Lactams toxicity in the intensive care unit: an underestimated collateral damage? Microorganisms. 2021;9(7):1505. doi:10.3390/microorganisms9071505
33. Suttels V, André P, Thoma Y, et al. Therapeutic drug monitoring of cefepime in a non-critically ill population: retrospective assessment and potential role for model-based dosing. JAC Antimicrob Resist. 2022;4(2):dlac043. doi:10.1093/jacamr/dlac043
34. Roberts JA, Joynt GM, Lee A, et al. The effect of renal replacement therapy and antibiotic dose on antibiotic concentrations in critically ill patients: data from the multinational sampling antibiotics in renal replacement therapy study. Clinl Infect Dis. 2021;72(8):1369–1378. doi:10.1093/cid/ciaa224
35. Quinton MC, Bodeau S, Kontar L, et al. Neurotoxic concentration of piperacillin during continuous infusion in critically ill patients. Antimicrob Agents Chemother. 2017;61(9). doi:10.1128/AAC.00654-17
36. Colman S, Stove V, De Waele JJ, Verstraete AG. Measuring unbound versus total piperacillin concentrations in plasma of critically ill patients: methodological issues and relevance. Therapeutic Drug Monitoring. 2019;41(3):325–330. doi:10.1097/FTD.0000000000000602
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.