Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Optimal Medical Therapy for Secondary Prevention of Acute Coronary Syndrome: A Retrospective Study from a Tertiary Hospital in Sudan
Authors Ahmed KO ![]() , Ahmed AM, Wali MB, Ali AH, Azhari MM, Babiker A, Yousef BA
, Ahmed AM, Wali MB, Ali AH, Azhari MM, Babiker A, Yousef BA ![]() , Muddather HF
, Muddather HF ![]()
Received 4 February 2022
Accepted for publication 1 April 2022
Published 8 April 2022 Volume 2022:18 Pages 391—398
DOI https://doi.org/10.2147/TCRM.S361129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Kannan O Ahmed,1 Ashraf M Ahmed,1 Mojahed B Wali,1 Ali H Ali,1 Mustafa M Azhari,1 Anas Babiker,2 Bashir A Yousef,3 Hiba F Muddather1
1Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmacy, University of Gezira, Wad Medani, Sudan; 2Department of Cardiology, Royal Care International Hospital, Khartoum, Sudan; 3Department of Pharmacology, Faculty of Pharmacy, University of Khartoum, Khartoum, Sudan
Correspondence: Kannan O Ahmed, Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmacy, University of Gezira, Wad Medani, Sudan, Tel +249 121860001, Fax +249 511861180, Email [email protected]
Background: Five-medication regimen is recommended for patients after acute coronary syndrome (ACS) as a secondary prevention strategy at discharge to reduce recurrence and improve mortality.
Objective: This study aimed to assess prescribing of optimal medical therapy (OMT) as five-medication regimens for secondary prevention at discharge after ACS in Sudan.
Methods: A retrospective cohort study was performed at a tertiary hospital located in Wad Medani, Sudan, in the period between January and December 2019. Data were collected from patients’ files. OMT was defined as a combination of five medications; aspirin and P2Y12 inhibitors, statins, beta-blockers (BBs), and angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs) or if a valid contraindication was documented.
Results: Of the 619 patients throughout the study period, 591 were selected based on inclusion and exclusion criteria. The median age of patients was 60 years, and 58.9% of patients were male. Diabetes (44.5%) and hypertension (42%) were the most common risk factors. Most patients (58.4%) were diagnosed with ST-segment elevation myocardial infarction. About 99.7% of patients were on aspirin, 99.5% on statins, 97% on clopidogrel, 96.8% on dual antiplatelet therapy, 70.4% on BBs, and 57.9% on ACEIs/ARBs. OMT for secondary prevention was prescribed to 267 (45.2%) patients with ACS at discharge.
Conclusion: Although prescriptions for all five guideline-recommended medications after ACS were suboptimal, the study showed a positive trend in prescribing most individual medications.
Keywords: acute coronary syndrome, discharge, optimal medical therapy, secondary prevention, Sudan
Introduction
Cardiovascular diseases are one of the leading causes of death worldwide and remain a substantial contributor to morbidity, mortality, and healthcare expenditure.1 In Sudan, around 12% of people die of cardiovascular diseases.2 Acute coronary syndrome (ACS) is a serious cardiovascular disease in which atheroma, thrombosis, or spasm of coronary arteries obstruct the oxygenated blood supply to the heart, leading to myocardial ischemia.3 ACS is classified as non-ST segment elevation ACS (NSTACS) or ST-segment elevation ACS (STACS);4 both of them are life-threatening and the leading cause of death in developed and developing countries. The mortality of ACS was estimated at 7.5 million deaths.5
Management of ACS depends on occlusion and time of onset symptoms. It includes immediate reperfusion through thrombolytic therapy or percutaneous coronary intervention (PCI), antiplatelets and anticoagulants, and in some instances, ACS can be approached by coronary artery bypass grafting surgery.3,6 After the acute phase of ACS, secondary prevention treatments including cardioprotective medications (beta-blockers [BBs], antiplatelet drugs, angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers [ACEIs/ARBs], and statins) and behavioral advices such as smoking cessation and exercise are effective in decreasing the risk of subsequent cardiovascular events, risk of hospital admission, and death.7,8
Regular usage and correct administration of secondary prevention medications increase the quality of life and lower the risk of repeated ischemic events and mortality for ACS patients.9 The American Heart Association/American College of Cardiology (AHA/ACC) guidelines and the European Society of Cardiology (ESC) recommend that all patients should be prescribed with secondary prevention medications prior to discharge.10,11 However, several reports have shown large gaps between the recommended and the prescribed dose of secondary prevention medications after ACS.12–15 To our knowledge, there is no published study that evaluates the optimization of secondary prevention medications for ACS Sudanese patients. Therefore, the current study aims to help fill the gap and assess the drug used for secondary prevention for Sudanese patients with ACS at the discharge point.
Methods
Study Setting
The study was conducted at Medani Heart Center, which is a tertiary hospital, located in Wad Medani, Gezira State, Sudan. It provides free health care that serves the inhabitants of Gezira state and receives referral patients from neighboring states within the central region. The Medani Heart Center has 100 beds in three separate fundamental sites of the center that are composed of the ICU (intensive care unit), the CCU (cardiac care unit), and the HDU (high dependency unit), which also contains wards for both internal medicine and surgery services. In addition, it is equipped with a cardiac catheterization lab.
Study Design and Patient Selection
An observational retrospective single-center study was conducted by reviewing the patients’ medical files between January and December 2019. Patients 18 years and older who were admitted to Medani Heart Center with a diagnosis of STACS or NSTACS during the study period were included. Patients were excluded if they had stable angina, died during hospitalization, transferred to other healthcare facilities, or refused to receive secondary prevention medications. If patients were admitted more than once during the study, only their first admission was included.
Data Collection
Data were retrieved from patients’ medical files using a structured data collection sheet. These data included patients’ demographics (age, gender, marital status, education, occupation, and residence), clinical characteristics (primary diagnosis, past medical history, and baseline risk factors), laboratory investigations, medications used, and their doses on the day of discharge.
The primary endpoint of the study was prescribing secondary prevention medications at discharge. Appropriate secondary prevention medications, for the purpose of the study, were defined as being prescribed all five guideline-recommended medications (statin, ACEIs/ARBs, dual antiplatelet therapy, and beta-blocker) at discharge or if a clinical contraindication to one or more of the secondary prevention medications was documented in the patients’ files.
Data Analysis
All analyses were performed using the Statistical Package for Social Sciences (SPSS) version 26 (SPSS Inc., Chicago, IL). Descriptive statistics were performed; categorical variables were expressed in percentages and/or frequencies, while continuous variables were summarized as median and means. Association between variables was carried out using the Student’s t-test and chi-square test. P value of less than 0.05 was considered statistically significant in all analyses.
Ethical Considerations
Ethical approval (HS-ERC-10-21) was obtained from the Health-Sector Ethical Review Committee, University of Gezira, in accordance with the Declaration of Helsinki. Due to the study’s retrospective nature, informed consent was waived, and collected data were also assured of strict privacy and confidentiality and the names and other personal identifiers of patients were not being registered.
Results
A total number of 619 ACS patients within the study period were initially identified from the hospital medical files, of which 591 patients were eligible to be included in the study and 28 patients were excluded. The reasons for exclusion were death before discharge (n = 19, 67.8%), transferred to other healthcare facilities (n = 4, 14.3%), refusal to receive secondary prevention medications (n = 3, 10.7%), diagnosed with stable angina (n = 1, 3.6%), and incomplete medical file (n = 1, 3.6%).
The median age of the patients was 60 years (range 19–100 years), and 348 (58.9%) patients were male. The majority of patients were married (n = 563, 95.3%). Moreover, approximately one-third of patients were illiterate, and more than half of the patients were residents of rural areas. The descriptive characteristics of patients are shown in Table 1.
 |
Table 1 Demographic and Clinical Characteristics of the Study Population (N = 591) |
Regarding disease characteristics, as demonstrated in Table 1, the baseline cardiac risk factors included hypertension in 246 (42%) patients, diabetes mellitus in 261 (44.5%) patients, current smoker 81 (13.9%) and, 117 (23.1%) patients had a family history of cardiac diseases. Of the whole group, 345 (58.4%) patients having the diagnosis of ST-segment elevation myocardial infarction (STEMI), 113 (19.1%) patients having non–ST-segment elevation myocardial infarction (NSTEMI), and 133 (22.5%) patients having unstable angina (UA). Of the total 591 patients, only 165 (27.9%) patients underwent percutaneous coronary intervention (PCI) during the hospitalization with or without stent implantation, whereas 426 (72.1%) patients did not undergo an invasive procedure and were treated medically. With regard to the laboratory investigations, the majority of patients neither underwent liver function tests (LFT) 539 (91.2%) nor lipid profile (LP) test (n = 585, 99%) (Table 1).
Among the 591 patients, 267 (45.2%) patients received all five guideline-recommended medications at hospital discharge, as shown in Table 2. The most common prescribed medications were aspirin (n = 589, 99.7%), statins (n = 588, 99.5%), clopidogrel (n = 573, 97%), BBs (n = 416, 70.4%), and ACEIs and/or ARBs (n = 342, 57.9%). Of note, most of the patients were received dual antiplatelet therapy (DAPT) (n = 576, 96.8%). Of them, ticagrelor was prescribed only in 4 patients (0.68%). Concerning optimal dosing, all patients prescribed antiplatelet received optimal doses, aspirin 75–100 mg and/or clopidogrel 75 mg daily. Of the patients who received a statin, 98.6% were prescribed a high-intensity statin (92.5% atorvastatin and 6.1% rosuvastatin).
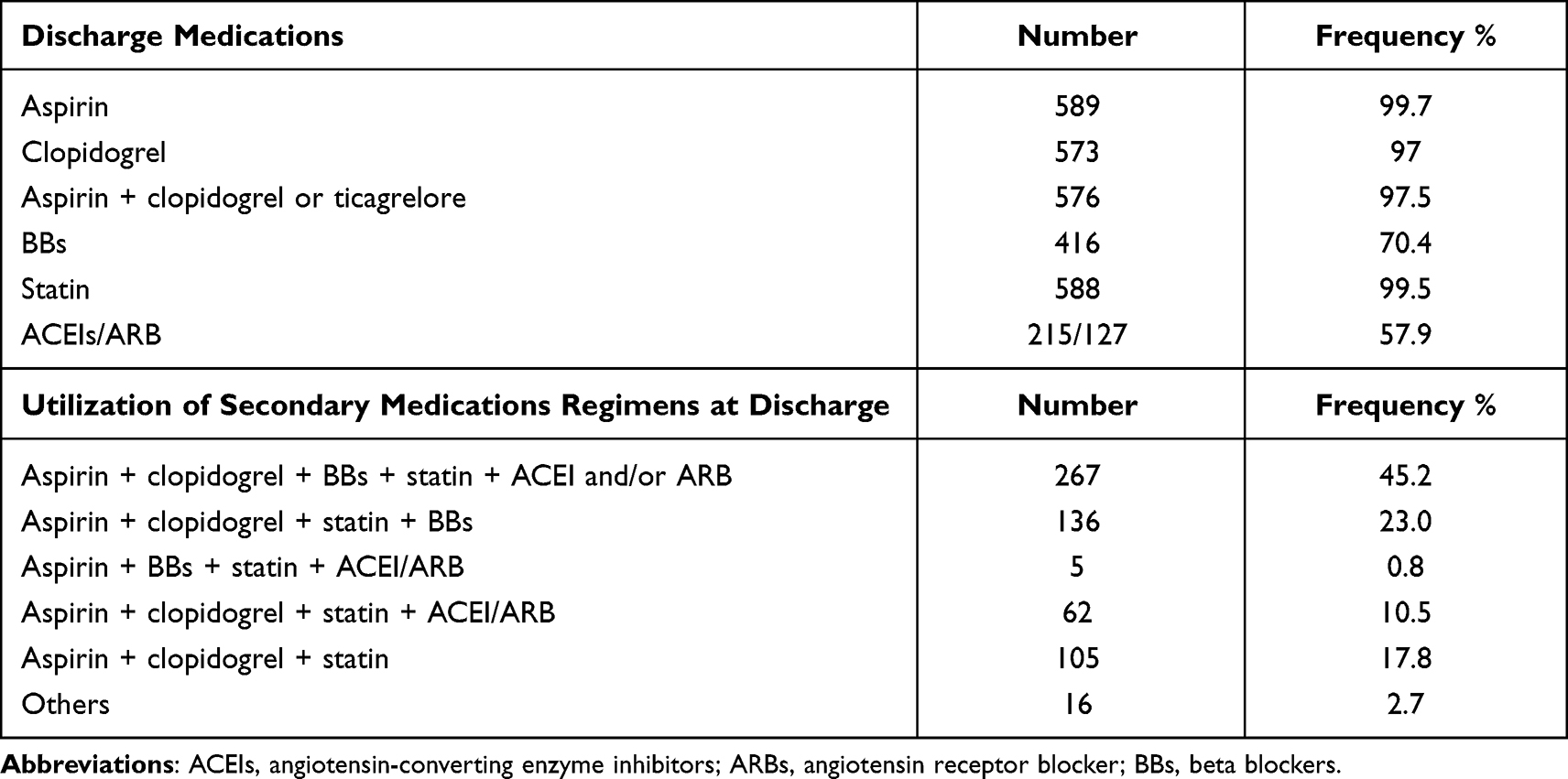 |
Table 2 Trend and Utilization of Discharge Secondary Medications and Medications Regimens Among the Study Population (N = 591) |
Chi-square analysis between baseline characteristics and five-drug combination therapy revealed statistically significant associations between the use of five-drug combination therapy and the number of comorbidities, hypertension, and diabetes mellitus (Table 3). Patients with two or more comorbidities were more likely to receive all five medications than those with one or no comorbid diseases (p = 0.001). Additionally, hypertensive patients were more likely to receive the five-drug combination therapy than non-hypertensive patients (p = 0.001). Furthermore, non-diabetic patients were less likely to receive all five medications than diabetic patients (p = 0.025), whereas there were statistically insignificant associations (p > 0.05) between the use of all five medications and socio-demographics (gender, age), type of ACS, and PCI intervention (Table 3).
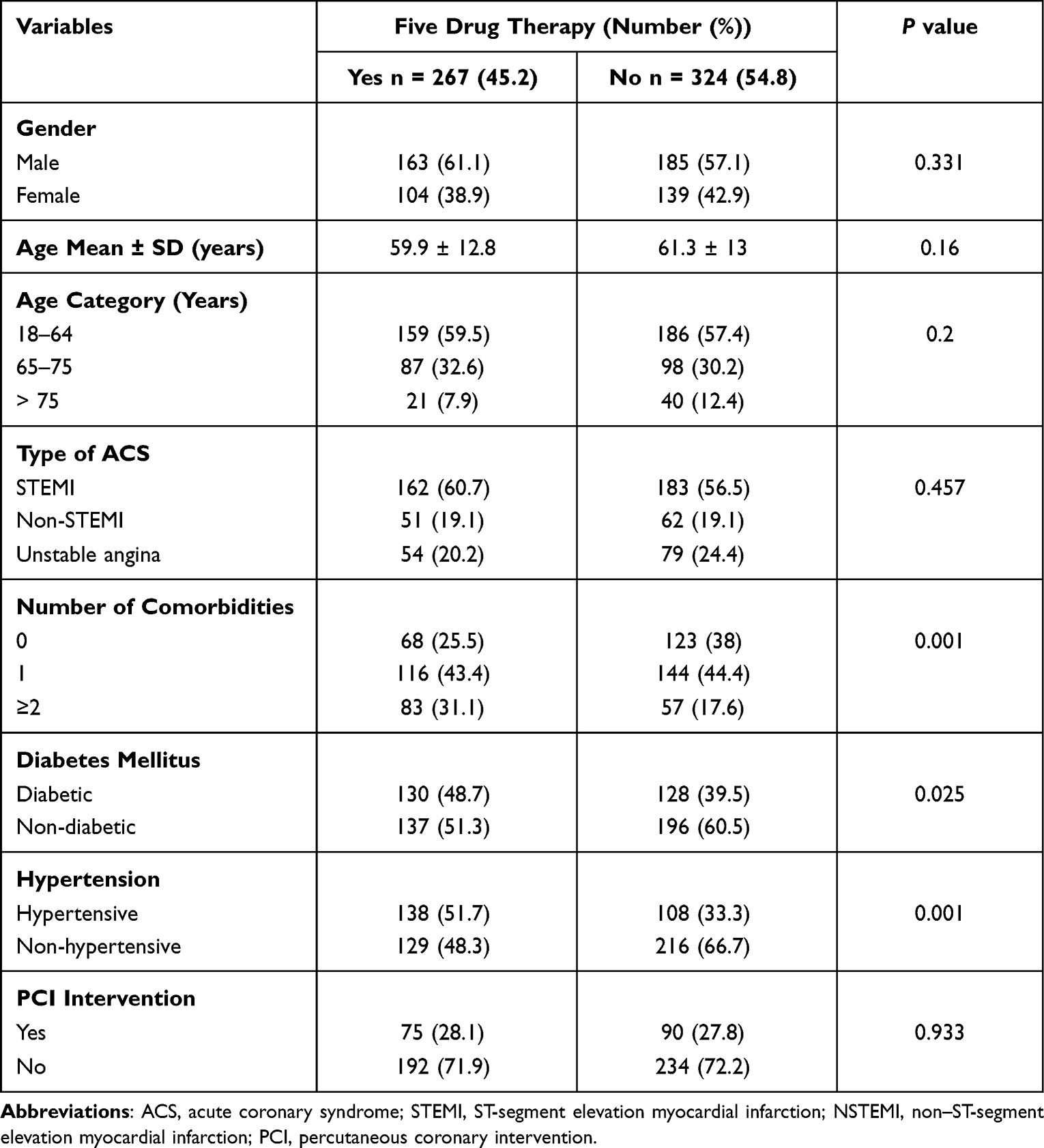 |
Table 3 Baseline Characteristics and Five-Drug Combination Therapy (N = 591) |
Discussion
In Sudan, there is a lack of studies evaluating ACS secondary prevention, as well as an increase in the number of ACS patients, that lead to increased death. The discharge remains the utmost important point to check the suitability of secondary prevention, the headway to prevent recurrence of the ACS, and ultimately the mortality.16 Thus, we conducted the first study in Sudan to address the secondary pharmacotherapy prevention to detect the gaps between the recommended and what is prescribed for ACS medications at the time of discharge.
The study showed that the median age of patients was 60 years, males were dominated, hypertension and diabetes mellitus patients were the common risk factors, and these findings were similar to previous Sudanese studies.2,17 The mean age in the present study was higher than studies conducted in neighboring countries,18,19 and significantly lower than the European population.20 About clinical diagnosis of ACS, 58.4%, 22.5%, or 19.1% of patients in this study were diagnosed with STEMI, UA, or NSTEMI, respectively, which was consistent with the previous studies.13,14 Moreover, the study showed that 3.1% of patients died before hospital discharge, which was much lower than previously published reports from Egypt and Ethiopia.18
Medications used in secondary prevention of ACS affect kidney functions in various mechanisms. This information is composed of the importance of kidney function tests in the dosing of medications.21 Our data revealed that almost all patients were tested for renal functions, and it was normal in nearly all the patients. Despite that, the study highlighted alarming issues regarding requested laboratory investigations; for instance, in 91.2% of patients, LFT was not performed. The LFT is very important in ACS patients, since they could start high-intensity statins therapy, which is known to cause hepatotoxicity that is normally monitored through baseline and thereafter.16 Similarly, LP was not documented in 99% of patients; by implementing the recommended strategy, the lowest is best regarding the LDL-cholesterol; this necessitates those physicians, and clinical pharmacists are aware of the baseline and the target of LDL-Cholesterol in ACS. A reduction of ≥50% LDL-Cholesterol from baseline and goal of <1.4 mmol/L (<55 mg/dL), so it is crucial to perform and document the lipid test.22
In this study, less than half (45.2%) of patients received all the five guideline-recommended medications; previous reports varied significantly as 43.7% in Thailand,23 62.9% in Lebanon,24 60% in Iraq,14 and 76% in Korea13 were discharged on optimal five recommended secondary prevention medications. The variation between results might be due to the study time points, study designs, and the definition of optimal pharmacotherapy secondary prevention. For instance, some researchers defined the optimal secondary prevention based on any four of the following drugs: aspirin or P2Y12 inhibitors, ACEIs or ARBs, BBs, and statins. By this definition, the results given were overestimated compared to the five drugs’ definition. Furthermore, our study was retrospective, which was faced by underestimating actual secondary prevention since many valid contraindications might not be documented in the patients’ files. Generally, our study results were suboptimal against the AHA/ACC guidelines, and other guidelines recommended that the adherence rate to secondary prevention medications be at least 60% after accounting for valid contraindications.14
Our study noted statistical differences in the use of secondary prevention therapy at discharge based on the number and type of the comorbid diseases. Hypertensive patients and diabetic patients were more likely to receive five-drug combination therapy than non-hypertensive and non-diabetic patients. Similar findings were also observed in previous studies, in which Hypertension and diabetes mellitus were statistically associated with receiving all five medications at discharge.14,25,26 Noteworthy from this study, about 44.5% of ACS patients had diabetes which is known as a strong risk factor for ACS and other cardiovascular diseases, this will provide a great opportunity to work at the primary prevention level by implementing the multifactorial intervention at primary health care level for Sudanese diabetic patients.27
Following an ACS, for life antiplatelet therapy with low-dose aspirin (75–100 mg) is the treatment of choice; clopidogrel (75 mg) is the alternative for patients with aspirin intolerance. For dual therapy with aspirin, the latest European and American guidelines highly recommend the novel antiplatelets ticagrelor or prasugrel, and clopidogrel is reserved for patients with contraindications or if it is not available in the country, generally recommended for one year.16 Our study denoted that 99.7% of patients were on aspirin and 97% on clopidogrel; this is in line with studies conducted in Iraq, Lebanon, and Korea. Yet, these percentages were higher than Ethiopian and Bangladesh studies.13,14,20,24,28 Similarly, 97.5% were on dual antiplatelet aspirin plus clopidogrel or ticagrelor (only in four patients), which was agreed with Iraqi and Bangladesh studies.14,20 The low utilization of ticagrelor might be justified by higher cost, and it is not included in governmental and private insurance in Sudan.
Guidelines highly recommend the use of oral BBs in hemodynamically stable ACS patients within the first 24 hours for a survival benefit compared with a delayed one.16 Our study found 70.4% of patients were discharged on BBs; this was remarkably lower than the utilization percentages reported in the previous studies.13,14,24 The lower percentage of prescribed BBs in the current study might be due to the hospital’s documentation system, in which clinical contraindications were not documented in the patients’ files, considering the retrospective nature of our study.
All patients with established atherosclerotic cardiovascular disease as ACS are classified as having a very high risk of fatal or nonfatal cardiovascular events in the next ten years.22 Thus, for secondary prevention, high-intensity statins therapy (atorvastatin 40–80 mg or rosuvastatin 20–40 mg) must be started regardless of LDL-C levels.16 In the present study, 99.5% of patients were using statin; this was higher than previously published reports.13,14,20,24,28 Furthermore, ACEIs (or ARBs in cases of intolerance to ACEIs) are recommended in patients with anterior infarction, heart failure with reduced LVEF (<40%), diabetes, or chronic kidney disease (CKD) unless contraindicated in order to reduce cardiovascular mortality and cardiovascular morbidity.16 In this study, 57.9% of patients were on either ACEIs or ARBs, compared with the literature; it was considered lower than other reports.13,14,24
The current study has several strengths, including: 1) this is the first study that assessed pharmacotherapy secondary prevention after ACS for one-year period in Sudan, which faced many challenges in the weak health care system, 2) The investigation is extracted from real-world data of the largest cardiac center outside Khartoum state. It provides cardiac services for Middle, West, and South inhabitants; thus, this data can help for national, sub-Saharan Africa, and global community to understand the treatment and other clinical characteristics among Sudanese patients with ACS, and 3) the study provides data for quality and policymakers towards the improvement of documentation systems and to a step for the establishment of guidelines that suit our context. Moreover, there is a great opportunity to optimize care for patients with cardiovascular disease including ACS by addition of a clinical pharmacist to the multidisciplinary team at Medani Heart Center, who showed positive impact in anticoagulation clinic and heart failure clinic in other cardiac centers in Khartoum, Sudan.29,30
The present study has some limitations. Due to the study’s retrospective nature, some data of eligible patients were missed. For example, heart failure was not documented among comorbidities; also, we did not find any documented contraindication or medication intolerance for secondary prevention medications. Secondly, due to a cross-sectional study’s design, no patients’ follow-up were performed; hence, we did not know the adherence rate after 6 months and forward after discharge. Further limitations of our study include that it was a single institutional study that could not generalize to other patients treated in other hospitals, and the patients’ adherence to these medications was not assessed. Therefore, further prospective cohort and multicenter studies were extremely needed.
Conclusion
Around 45.2% of patients received the recommended secondary prevention medications at discharge from the hospital. Although this percentage was suboptimal, the data showed a positive trend in prescribing most individual medications. Our findings necessitate the implementation of strategies to optimize prescribing.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Isma’eel H, Mohanna Z, Hamadeh G, et al. The public cost of 3 statins for primary prevention of cardiovascular events in 7 Middle East countries: not all of them can afford it. Int J Cardiol. 2012;155(2):316–318. doi:10.1016/j.ijcard.2011.12.011
2. Mirghani HO, Elnour MA, Taha AM, Elbadawi AS. Gender inequality in acute coronary syndrome patients at Omdurman Teaching Hospital, Sudan. J Fam Community Med. 2016;23(2):100. doi:10.4103/2230-8229.181007
3. Kumar A, Cannon CP. Acute coronary syndromes: diagnosis and management, part I.
4. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes: the task force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J. 2020;41(3):407–477. doi:10.1093/eurheartj/ehz425
5. WHO’s Global Health. Leading causes of death and disability. Leading causes of death and disability; 2020. Available from: https://www.who.int/data/stories/leading-causes-of-death-and-disability-2000-2019-a-visual-summary.
6. Neumann F-J, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165. doi:10.1093/eurheartj/ehy394
7. Chow CK, Brieger D, Ryan M, Kangaharan N, Hyun KK, Briffa T. Secondary prevention therapies in acute coronary syndrome and relation to outcomes: observational study. Heart Asia. 2019;11(1):e011122. doi:10.1136/heartasia-2018-011122
8. Clark AM, Hartling L, Vandermeer B, McAlister FA. Meta-analysis: secondary prevention programs for patients with coronary artery disease. Ann Intern Med. 2005;143(9):659–672. doi:10.7326/0003-4819-143-9-200511010-00010
9. Members WG, Roger VL, Go AS, et al. Heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation. 2012;125(1). e2–e220.
10. Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016;68(10):1082–1115. doi:10.1016/j.jacc.2016.03.513
11. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
12. Arnold SV, Spertus JA, Masoudi FA, et al. Beyond medication prescription as performance measures: optimal secondary prevention medication dosing after acute myocardial infarction. J Am Coll Cardiol. 2013;62(19):1791–1801. doi:10.1016/j.jacc.2013.04.102
13. Byeon HJ, Yang Y-M, Choi EJ. Optimal medical therapy for secondary prevention after an acute coronary syndrome: 18-month follow-up results at a tertiary teaching hospital in South Korea. Ther Clin Risk Manag. 2016;12:167. doi:10.2147/TCRM.S99869
14. Nassr OA, Forsyth P, Johnson CF. Evaluation of discharge prescriptions for secondary prevention in patients with acute coronary syndromes in Iraq. Pharm Pract. 2019;17(1):1372. doi:10.18549/PharmPract.2019.1.1372
15. Grall S, Biere L, Le Nezet M, et al. Relationship between beta-blocker and angiotensin-converting enzyme inhibitor dose and clinical outcome following acute myocardial infarction. Circ J. 2015;2015:
16. Collet J-P, Thiele H, Barbato E, et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2021;42(14):1289–1367. doi:10.1093/eurheartj/ehaa575
17. Elhassan O, Mohamed S, Ibnouf M. Adherence of Sudanese coronary artery disease patients to secondary prevention medications at Elshaab Teaching Hospital, Sudan. Sud J Med Sci. 2014;9(2):111–116.
18. Fanta K, Daba FB, Tegene E, Melaku T, Fekadu G, Chelkeba L. Management quality indicators and in-hospital mortality among acute coronary syndrome patients admitted to tertiary hospitals in Ethiopia: prospective observational study. BMC Emerg Med. 2021;21(1):1–9. doi:10.1186/s12873-021-00433-3
19. Thabet N, Dina L, Samir A, et al. Evaluation of secondary prevention in Egyptian patients after primary percutaneous coronary intervention. Eur J Prev Cardiol. 2021;28(Supplement_1):
20. Hasdai D, Behar S, Wallentin L, et al. A prospective survey of the characteristics, treatments and outcomes of patients with acute coronary syndromes in Europe and the Mediterranean basin; the Euro Heart Survey of Acute Coronary Syndromes (Euro Heart survey ACS). Eur Heart J. 2002;23(15):1190–1201. doi:10.1053/euhj.2002.3193
21. Agustina PS, Yunir E, Prawiroharjo P, Damanik J, Sauriasari R. Comparison of effects of ACEIs and ARBs on albuminuria and hyperkalemia in Indonesian hypertensive type 2 diabetes mellitus patients. Int J Hypertens. 2020;2020.
22. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Atherosclerosis. 2019;290:140–205.
23. Wongsalap Y, Kengkla K, Poolpun D, Saokaew S. Trends in optimal medical therapy at discharge and clinical outcomes in patients with acute coronary syndrome in Thailand. J Cardiol. 2021;77(6):669–676. doi:10.1016/j.jjcc.2020.12.015
24. Sheikh-Taha M, Hijazi Z. Evaluation of proper prescribing of cardiac medications at hospital discharge for patients with acute coronary syndromes (ACS) in two Lebanese hospitals. SpringerPlus. 2014;3(1):1–6. doi:10.1186/2193-1801-3-159
25. Tra J, van der Wulp I, Appelman Y, de Bruijne MC, Wagner C. Adherence to guidelines for the prescription of secondary prevention medication at hospital discharge after acute coronary syndrome: a multicentre study. Neth Heart J. 2015;23(4):214–221. doi:10.1007/s12471-015-0664-y
26. Al-Zakwani I, Sulaiman K, Za’abi M, et al. Impact of evidence-based cardiac medications on short and long-term mortality in 7567 acute coronary syndrome patients in the Gulf RACE-II registry. Int J Clin Pharmacol Ther. 2012;50(6):418–425. doi:10.5414/CP201667
27. Sasso FC, Pafundi PC, Simeon V, et al. Efficacy and durability of multifactorial intervention on mortality and MACEs: a randomized clinical trial in type-2 diabetic kidney disease. Cardiovasc Diabetol. 2021;20(1):145. doi:10.1186/s12933-021-01343-1
28. Tsegaye T, Gishu T, Habte MH, Bitew ZW. Recovery rate and predictors among patients with acute coronary syndrome in Addis Ababa, Ethiopia: a retrospective cohort study. Res Rep Clin Cardiol. 2021;12:9–21.
29. Ahmed NO, Osman B, Abdelhai YM, El-Hadiyah TMH. Impact of clinical pharmacist intervention in anticoagulation clinic in Sudan. Int J Clin Pharm. 2017;39(4):769–773. doi:10.1007/s11096-017-0475-x
30. Ahmed KO, Eldin IT, Yousif M, et al. Clinical pharmacist’s intervention to improve medication titration for heart failure: first experience from Sudan. Integr Pharm Res Pract. 2021;10:135. doi:10.2147/IPRP.S341621
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.