Back to Journals » Journal of Pain Research » Volume 11
Optimal management of orthodontic pain
Authors Topolski F, Moro A ![]() , Correr GM, Schimim SC
, Correr GM, Schimim SC
Received 1 October 2017
Accepted for publication 23 December 2017
Published 16 March 2018 Volume 2018:11 Pages 589—598
DOI https://doi.org/10.2147/JPR.S127945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Francielle Topolski,1 Alexandre Moro,1,2 Gisele Maria Correr,3 Sasha Cristina Schimim1
1Department of Orthodontics, Positivo University, Curitiba, Paraná, Brazil; 2Department of Orthodontics, Federal University of Paraná, Curitiba, Paraná, Brazil; 3Department of Restorative Dentistry, Positivo University, Curitiba, Paraná, Brazil
Abstract: Pain is an undesirable side effect of orthodontic tooth movement, which causes many patients to give up orthodontic treatment or avoid it altogether. The aim of this study was to investigate, through an analysis of the scientific literature, the best method for managing orthodontic pain. The methodological aspects involved careful definition of keywords and diligent search in databases of scientific articles published in the English language, without any restriction of publication date. We recovered 1281 articles. After the filtering and classification of these articles, 56 randomized clinical trials were selected. Of these, 19 evaluated the effects of different types of drugs for the control of orthodontic pain, 16 evaluated the effects of low-level laser therapy on orthodontic pain, and 21 evaluated other methods of pain control. Drugs reported as effective in orthodontic pain control included ibuprofen, paracetamol, naproxen sodium, aspirin, etoricoxib, meloxicam, piroxicam, and tenoxicam. Most studies report favorable outcomes in terms of alleviation of orthodontic pain with the use of low-level laser therapy. Nevertheless, we noticed that there is no consensus, both for the drug and for laser therapy, on the doses and clinical protocols most appropriate for orthodontic pain management. Alternative methods for orthodontic pain control can also broaden the clinician’s range of options in the search for better patient care.
Keywords: tooth movement, pain control, drug therapy, laser therapy
Introduction
Orthodontic tooth movement is a result of the application of forces to the teeth. The orthodontic forces promote tooth displacement in the periodontal ligament space, leading to the formation of areas of compression and traction. These stimuli trigger a series of tissue reactions that result in bone remodeling of the alveolus through the processes of bone resorption and apposition, thus permitting changes in tooth positioning.1 These processes are accompanied by a stimulation of nerve endings in the periodontal ligament and an inflammatory process, which most often results in pain.2
Pain is one of the most important side effects of orthodontic tooth movement and one of the factors that discourage patients the most from starting orthodontic treatment. In addition, it is among the main causes for treatment withdrawal.2–4 However, despite the relevance of pain in the clinical practice of orthodontics, this symptom is frequently underestimated and receives little attention. Considering the importance of pain control to promote patient well-being and avoid orthodontic treatment withdrawal, this study aimed to identify, through an analysis of the scientific literature, the best method for managing orthodontic pain.
Materials and methods
The methodological procedures used to conduct this research were guided by the Knowledge Development Process – Constructivist (ProKnow-C) process.5 The research was carried out in August 2017 according to the procedure outlined in Figure 1. Initially, the most representative keywords for the studied subject were defined. The terms underwent a test of adherence, in which the results that each keyword generated when searched in databases were assessed. The keyword selection was validated by a researcher with experience in the area. The following keyword combinations were used: “tooth movement” AND pain and orthodontic* AND pain. We searched the MEDLINE via PubMed and Science Direct databases. The search was directed toward scientific articles published in the English language. There was no restriction on the date of publication.
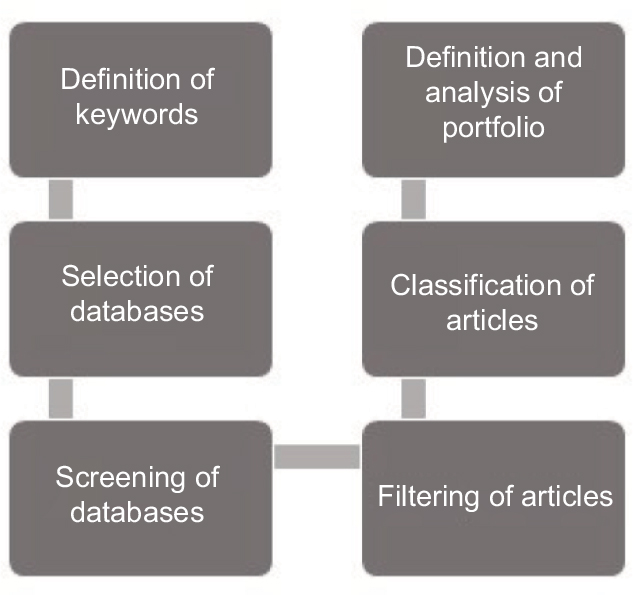 | Figure 1 Methodological stages. |
The retrieved articles were exported using EndNote X6 software. The articles were filtered and classified using the software features. Duplicate articles were identified and deleted. The others were classified through analyses of titles, abstracts, and keywords. Scientific articles that evaluated different methods of orthodontic pain management were selected. The selected articles were subjected to a more careful classification, from which only the randomized clinical trials were retained. These studies, which correspond to the final portfolio of selected articles, were comprehensively analyzed.
Results
We recovered 1281 articles. Of these, 342 were duplicates and were excluded. The other 939 were classified on the basis of analyses of titles, abstracts, and keywords. Of these, 12 were not scientific articles and 820 were not aligned with the objective of this study. The other 107 articles were selected and subjected to a new classification, in which only randomized clinical trials were selected: 56 articles remained. Of these, 19 evaluated the effects of different types of drugs to manage orthodontic pain, 16 evaluated the effects of low-level laser therapy (LLLT), and the other 21 studies evaluated other types of intervention (Figure 2). Table 1 shows the selected articles, their general methods, and the main outcomes.
 | Figure 2 Flowchart of filtering and classification of articles. |
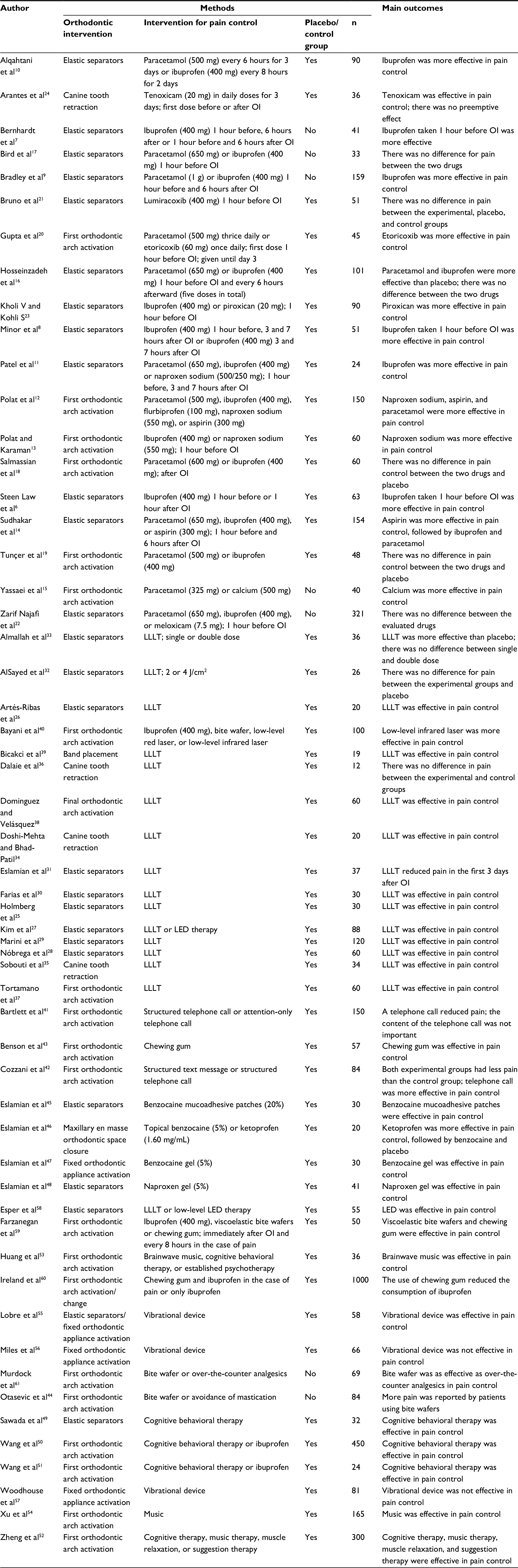 | Table 1 Selected articles Abbreviations: LED, light-emitting diode; LLLT, low-level laser therapy; OI, orthodontic intervention. |
Systematic analysis
Drug therapy
Several studies have evaluated the effects of different types of drugs on the control of orthodontic pain. Steen Law et al6 compared three groups of patients subjected to the insertion of elastic separators. One group used ibuprofen 1 hour before and placebo 1 hour after the procedure; another group was administered placebo 1 hour before and ibuprofen 1 hour after the procedure, and the third group received only placebo 1 hour before and 1 hour after the procedure. The group that received the drug before the separator placement experienced less pain when compared to the other groups. Bernhardt et al7 compared the use of ibuprofen administered only before the separator placement, both before and after the separator placement, and only after the separator placement. They observed that administration before the procedure was more effective in pain control. Minor et al8 compared a group of patients who received ibuprofen both before and after separator placement with one group that received the drug only after the procedure and with another group that received only placebo. The group receiving the drug in both the preoperative and postoperative periods had a more effective pain reduction.
Bradley et al9 compared the effects of paracetamol and ibuprofen administered 1 hour before and 6 hours after the placement of elastic separators and concluded that ibuprofen had a greater effect on orthodontic pain control. Alqahtani et al10 also observed that ibuprofen was more effective than paracetamol. In this study, patients were administered either paracetamol or ibuprofen after the insertion of elastic separators. Patel et al11 observed that ibuprofen had a greater effect on orthodontic pain reduction compared to both paracetamol and naproxen sodium. In this study, patients were administered paracetamol, naproxen, or ibuprofen 1 hour before the procedure. The same drug initially administered was again administered 3 and 7 hours after the insertion of elastic separators. The group that used ibuprofen had better pain reduction when compared with the placebo group. However, the groups that used paracetamol and naproxen sodium did not present any differences in terms of pain reduction from the group that used placebo.
In contrast, Polat et al,12 when comparing the effects of ibuprofen and naproxen sodium administered separately 1 hour before orthodontic arch activation, found that naproxen sodium was more effective in pain control. In another study, Polat and Karaman13 compared the effects of ibuprofen, flurbiprofen, paracetamol, naproxen sodium, and aspirin. The authors reported that all the drugs used were more effective compared to the placebo; however, naproxen sodium, aspirin, and paracetamol yielded better results.
Sudhakar et al14 compared the effects of paracetamol, ibuprofen, aspirin, and placebo initially administered 1 hour before the insertion of elastic separators and every 6 hours after the insertion of elastic separators. They reported that all drugs had effects superior to placebo and that the best results were observed in the group that used aspirin, followed by the group that used ibuprofen. Paracetamol generated less pain reduction compared to the other drugs tested. Yassaei et al15 observed that calcium was more effective for orthodontic pain control than paracetamol.
Hosseinzadeh et al16 compared the effects of paracetamol and ibuprofen administered 1 hour before the insertion of elastic separators and every 6 hours after their insertion. The authors concluded that there was a reduction in pain perception in both groups compared to placebo. There was no difference in pain reduction between the groups that were administered the two drugs, as reported by the patients. Bird et al17 also compared the effects of paracetamol and ibuprofen administered 1 hour prior to separator placement. The authors did not observe a difference between the two groups. In this study, no control group was used. Two other studies18,19 reported no difference in orthodontic pain with paracetamol, ibuprofen, or placebo administration.
The other drugs tested were etoricoxib, lumiracoxib, meloxicam, piroxicam, and tenoxicam. Gupta et al20 compared the effects of administration of paracetamol, etoricoxib, and placebo 1 hour before and 3 days after the first orthodontic arch was installed. They concluded that etoricoxib was more effective in reducing pain. Bruno et al21 evaluated the effect of lumiracoxib administered 1 hour before the separator insertion. They did not observe a difference in pain perception between the group that was treated with the drug and the group that was administered placebo. Zarif Najafi et al22 compared the effects of paracetamol, ibuprofen, and meloxicam administered 1 hour before the separator insertion. The authors did not observe a difference in efficacy among the tested drugs. In this study, no control group was used. Kholi and Kohli23 evaluated the effects of ibuprofen and piroxicam administered 1 hour prior to the insertion of elastic separators. The authors observed that piroxicam was more effective in pain control than ibuprofen. Arantes et al24 evaluated tenoxicam administered to one group before the activation of the device to upper canine retraction and to another group after the procedure. The effects of these drugs were then compared with the placebo. The authors reported that the tenoxicam-treated groups had less pain than the placebo group, regardless of the time of administration.
Laser therapy
The reduction in pain perception after insertion of elastic separators by the effect of LLLT was reported by Holmberg et al,25 Artés-Ribas et al,26 Kim et al,27 Nóbrega et al,28 Marini et al,29 and Farias et al.30 Eslamian et al31 observed that the application of LLLT was effective in reducing pain during the first 3 days after separator insertion. After this period, the pain was of low intensity and presented marked variation in both the treatment and control groups. AlSayed et al32 did not observe a reduction in orthodontic pain after insertion of elastic separators by the effect of LLLT.
Almallah et al33 tested the effect of LLLT after separator insertion by comparing a protocol with a single application, which was administered immediately after separator insertion, and another with double application, which was administered immediately after the separator insertion and once again after 24 hours. The authors reported that LLLT was effective in reducing pain, with no significant differences between the single and double application protocols.
Other studies have evaluated the effect of LLLT on orthodontic pain during canine retraction. Doshi-Mehta and Bhad-Patil34 observed an average increase of 30% in the rate of tooth movement, as well as a reduction in pain perception in patients subjected to laser application. A positive effect on pain reduction was also reported by Sobouti et al.35 Dalaie et al,36 on the contrary, did not observe any differences either with the movement rate or with the pain perception when compared to control group.
Tortamano et al37 evaluated the effect of LLLT after insertion of the first orthodontic arch, while Dominguez and Velásquez38 evaluated the effect of LLLT after activation of the final orthodontic arch. Both reported reductions in orthodontic pain in patients subjected to laser application. Bicakci et al39 observed that LLLT after activation of the fixed appliance led to a reduction both in the perceived pain by patients and in the levels of prostaglandins expressed in the crevicular fluid.
Bayani et al40 compared the effects of ibuprofen, bite wafer, low-level red laser, and low-level infrared laser on orthodontic pain after activation of the first orthodontic arch. They concluded that low-level infrared laser was more effective in pain control.
Other methods of orthodontic pain control
Some studies have evaluated other methods of orthodontic pain control. Bartlett et al41 and Cozzani et al42 found that a telephone call from the dental office after consultation might be effective in reducing orthodontic pain. Benson et al43 observed a positive effect of using chewing gum on orthodontic pain control. Otasevic et al44 reported a reduction in orthodontic pain with the use of bite wafers.
Some studies have tested the use of topical drugs. Eslamian et al45 observed that the use of benzocaine mucoadhesive plaster (20%) reduced pain due to the insertion of an elastic separator. Eslamian et al46 found that topical application of 5% benzocaine gel and ketoprofen (1.60 mg/mL) reduced the pain resulting from loop activation for mass dental retraction. In this study, the ketoprofen gel was more effective than the benzocaine gel. Eslamian et al47 also reported a reduction in orthodontic pain with the application of 5% benzocaine gel. Eslamian et al48 observed a reduction in pain due to the insertion of an elastic separator in patients who were treated with topical application of naproxen 5%.
Cognitive behavioral therapy was a method identified as effective in controlling orthodontic pain by Sawada et al,49 Wang et al,50,51 and Zheng et al.52 The latter also reported positive results with music therapy, muscle relaxation therapy, and suggestion therapy. The positive effect of music on orthodontic pain reduction was also reported by Huang et al53 and Xu et al.54
Studies have also evaluated the influence of vibratory devices on orthodontic pain control. Lobre et al55 and Miles et al56 reported positive results of pain reduction, whereas Woodhouse et al57 did not observe any difference between patients undergoing therapy with this type of device and the control group during the initial orthodontic alignment.
Esper et al58 verified that low-level light-emitting diode therapy was more effective than LLLT in orthodontic pain control after insertion of orthodontic separator.
A few studies have compared the efficacy of drugs with that of nonpharmacologic methods with respect to pain control. Farzanegan et al59 compared the use of ibuprofen, soft viscoelastic bite wafer, hard viscoelastic bite wafer, chewing gum, and placebo administered immediately after and then every 8 hours in the case of pain after the initial orthodontic arch was installed. The authors concluded that ibuprofen might be replaced by nonpharmacologic methods tested for orthodontic pain control. Ireland et al60 found that the use of chewing gum might reduce the consumption of ibuprofen for orthodontic pain control. Murdock et al61 reported that the use of bite wafer after the initial orthodontic arch insertion was as effective as the consumption of analgesics in the control of orthodontic pain.
Discussion
This study aimed to investigate the best methods of orthodontic pain control. The methodological strategy used was the review of scientific literature oriented by the Knowledge Development Process – Constructivist (ProKnow-C).5 This process involves the careful selection of keywords as well as a thorough search of databases pertinent to this study. The cross-checking of keywords guarantees the specificity of the search with respect to the research topic.
The analysis of the final portfolio of articles revealed that studies evaluating different types of medications for orthodontic pain control were the most prevalent. The most frequently searched drugs were ibuprofen and paracetamol. The results of the studies comparing the effects of these two drugs on orthodontic pain control have been quite contradictory. A few studies showed that ibuprofen was more effective,9–11,14 while another study presented that paracetamol produced better results in terms of pain control.13 A few other studies posited that there is no difference between them in terms of pain reduction16,17 and that neither is effective in the control of orthodontic pain.18,19 A few studies suggested that the preemptive effect of ibuprofen was more important than its postoperative administration.6–8
Patel et al11 observed that ibuprofen had a greater effect on orthodontic pain compared to naproxen sodium, in contrast to the study by Polat et al,12 who observed that naproxen sodium was more effective than ibuprofen. The efficacies of aspirin,13,14 etoricoxib,20 meloxicam,22 piroxicam,23 and tenoxicam24 were also evaluated; these drugs were found to be effective in reducing orthodontic pain. Lumiracoxib, however, was not effective.21
The studies that involved the administration of these drugs presented a great variability, not only in terms of the results found but also in terms of the methodology used. Studies with ibuprofen consistently used a 400 mg dose. However, there was a substantial variation in terms of dose with respect to the other drugs. The drug administration protocols were also quite varied, as were the periods of pain data collection.
Studies evaluating the effect of LLLT on the control of orthodontic pain also presented considerable variations in relation to the design, type, and protocol of laser application. The majority of such studies, however, reported favorable results.25–31,33–35,37–40
In addition to drug administration and laser therapy, other methods of orthodontic pain control have been researched and shown to be effective. It is worth noting that a telephone call from the dental office after consultation,41,42 topical application of benzocaine and ketoprofen,45–48 cognitive behavioral therapy,49–52 muscle relaxation,52 suggestion therapy,52 music,52–54 vibratory devices,55,56 chewing gum,43,59,60 and bite wafers59,61,44 have all been shown to be effective in terms of orthodontic pain control.
Different methods of inducing tooth movement were used in the studies, including the use of separators, canine retraction, and dental alignment with fixed appliance. These methods can generate different intensities of force and, consequently, different intensities of pain, which make it difficult to compare the results. The individual variability and subjectivity inherent in the study of pain are also limiting factors in this type of research. Studies, in general, do not present details about the patients’ initial malocclusion.
Most of the studies used a visual analog scale as a method to assess pain. However, a great variation was observed in relation to the moment when the pain was evaluated, specifically in relation to the time periods after orthodontic intervention and to the activity the patient was performing during pain assessments.
Some studies evaluated the effect of interventions for pain relief on tooth movement. Arantes et al24 did not observe the influence of tenoxican administration on tooth movement. Dalaie et al36 also did not observe differences related to tooth movement with LLLT application. Miles at al56 found that the vibratory device used, besides not promoting pain relief, did not influence tooth movement. On the contrary, Doshi-Mehta and Bhad-Patil34 observed that the application of LLLT, in addition to reducing pain, promoted an increase in the rate of tooth movement.
Most of the studies used samples of adolescents from both sexes. Some of them also included adults. There were no differences in pain perception related to the age group. Cozzani et al42 reported that female subjects appeared to be more sensitive to pain than male subjects. Xu et al54 observed a greater effect on pain relief for the male subjects than for the female subjects.
Conclusion
Analysis of the scientific literature allows us to conclude that the main methods of orthodontic pain control are drug administration and the application of LLLT.
With respect to drug administration, positive results were obtained in terms of pain control with the use of ibuprofen, paracetamol, naproxen sodium, aspirin, etoricoxib, meloxicam, piroxicam, and tenoxicam. Nevertheless, there is no consensus on the most effective dose and the protocol to be used.
With respect to LLLT, although most studies report favorable results in terms of pain reduction, there is a need to establish an ideal clinical protocol.
Alternative nonpharmacologic methods for orthodontic pain control are also effective and can broaden the clinician’s range of options in the search for better patient care.
Disclosure
The authors report no conflicts of interest in this work.
References
Krishnan V, Davidovitch Z. Cellular, molecular, and tissue-level reactions to orthodontic force. Am J Orthod Dentofacial Orthop. 2006;129(4):469.e1–32. | ||
Krishnan V. Orthodontic pain: from causes to management – a review. Eur J Orthod. 2007;29(2):170–179. | ||
Brown DF, Moerenhout RG. The pain experience and psychological adjustments to orthodontic treatment of preadolescents, adolescents and adults. Am J Orthod Dentofacial Orthop. 1991;100(4):349–356. | ||
Kluemper GT, Hiser DG, Rayens MK, Jay MJ. Efficacy of a wax containing benzocaine in the relief of oral mucosal pain caused by orthodontic appliances. Am J Orthod Dentofacial Orthop. 2002;122(4):359–365. | ||
Marafon AD, Ensslin L, Ensslin SR, Lacerda RT. Revisão sistêmica da literatura internacional sobre avaliação de desempenho na gestão de P&D. Revista Gestão Industrial. 2012;8(3):1–43. | ||
Steen Law SL, Southard KA, Law AS, Logan HL, Jakobsen JR. An evaluation of preoperative ibuprofen for treatment of pain associated with orthodontic separator placement. Am J Orthod Dentofacial Orthop. 2000;118(6):629–635. | ||
Bernhardt MK, Southard KA, Batterson KD, Logan HL, Baker KA, Jakobsen JR. The effect of preemptive and/or postoperative ibuprofen therapy for orthodontic pain. Am J Orthod Dentofacial Orthop. 2001;120(1):20–27. | ||
Minor V, Marris CK, McGorray SP, et al. Effects of preoperative ibuprofen on pain after separator placement. Am J Orthod Dentofacial Orthop. 2009;136(4):510–517. | ||
Bradley RL, Ellis PE, Thomas P, Bellis H, Ireland AJ, Sandy JR. A randomized clinical trial comparing the efficacy of ibuprofen and paracetamol in the control of orthodontic pain. Am J Orthod Dentofacial Orthop. 2007;132(4):511–517. | ||
Alqahtani N, Alwakeel A, Alzamil A, et al. Comparison of two analgesics used for pain relief after placement of orthodontic separators. Saudi Pharm J. 2017;25(8):1169–1174. | ||
Patel S, McGorray SP, Yezierski R, Fillingim R, Logan H, Wheeler TT. Effects of analgesics on orthodontic pain. Am J Orthod Dentofacial Orthop. 2011;139(1):e53–e58. | ||
Polat O, Karaman AI, Durmus E. Effects of preoperative ibuprofen and naproxen sodium on orthodontic pain. Angle Orthod. 2005;75(5):791–796. | ||
Polat O, Karaman AI. Pain control during fixed orthodontic appliance therapy. Angle Orthod. 2005;75(2):214–219. | ||
Sudhakar V, Vinodhini TS, Mohan AM, Srinivasan B, Rajkumar BK. The efficacy of different pre- and post-operative analgesics in the management of pain after orthodontic separator placement: a randomized clinical trial. J Pharm Bioallied Sci. 2014;6(Suppl 1):S80–S84. | ||
Yassaei S, Vahidi A, Farahat F. Comparison of the efficacy of calcium versus acetaminophen on reduction of orthodontic pain. Indian J Dent Res. 2012;23(5):608–612. | ||
Hosseinzadeh Nik T, Shahsavari N, Ghadirian H, Ostad SN. Acetaminophen versus liquefied ibuprofen for control of pain during separation in orthodontic patients: a randomized triple blinded clinical trial. Acta Med Iran. 2016;54(7):418–421. | ||
Bird SE, Williams K, Kula K. Preoperative acetaminophen vs ibuprofen for control of pain after orthodontic separator placement. Am J Orthod Dentofacial Orthop. 2007;132(4):504–510. | ||
Salmassian R, Oesterle LJ, Shellhart WC, Newman SM. Comparison of the efficacy of ibuprofen and acetaminophen in controlling pain after orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2009;135(4):516–521. | ||
Tunçer Z, Polat-Ozsoy O, Demirbilek M, Bostanoglu E. Effects of various analgesics on the level of prostaglandin E2 during orthodontic tooth movement. Eur J Orthod. 2014;36(3):268–274. | ||
Gupta M, Kandula S, Laxmikanth SM, Vyavahare SS, Reddy SB, Ramachandra CS. Controlling pain during orthodontic fixed appliance therapy with non-steroidal anti-inflammatory drugs (NSAID): a randomized, double-blinded, placebo-controlled study. J Orofac Orthop. 2014;75(6):471–476. | ||
Bruno MB, Bruno MA, Krymchantowski AV, da Motta AF, Mucha JN. A double-blind, randomized clinical trial assessing the effects of a single dose of preemptive anti-inflammatory treatment in orthodontic pain. Prog Orthod. 2011;12(1):2–7. | ||
Zarif Najafi H, Oshagh M, Salehi P, Babanouri N, Torkan S. Comparison of the effects of preemptive acetaminophen, ibuprofen, and meloxicam on pain after separator placement: a randomized clinical trial. Prog Orthod. 2015;16:34. | ||
Kohli SS, Kohli VS. Effectiveness of piroxicam and ibuprofen premedication on orthodontic patients’ pain experiences. Angle Orthod. 2011;81(6):1097–1102. | ||
Arantes GM, Arantes VM, Ashmawi HA, Posso IP. Tenoxicam controls pain without altering orthodontic movement of maxillary canines. Orthod Craniofac Res. 2009;12(1):14–19. | ||
Holmberg PF, Sánchez CZ, Suarez RF, Vidal PS. Uso del láser terapéutico en el control del dolor en ortodoncia. Rev Clín Periodoncia Implantol Rehabil Oral. 2011;4(3):114–116. | ||
Artés-Ribas M, Arnabat-Dominguez J, Puigdollers A. Analgesic effect of a low-level laser therapy (830 nm) in early orthodontic treatment. Lasers Med Sci. 2013;28(1):335–341. | ||
Kim WT, Bayome M, Park JB, Park JH, Baek SH, Kook YA. Effect of frequent laser irradiation on orthodontic pain. A single-blind randomized clinical trial. Angle Orthod. 2013;83(4):611–616. | ||
Nóbrega C, da Silva EM, de Macedo CR. Low-level laser therapy for treatment of pain associated with orthodontic elastomeric separator placement: a placebo-controlled randomized double-blind clinical trial. Photomed Laser Surg. 2013;31(1):10–16. | ||
Marini I, Bartolucci ML, Bortolotti F, Innocenti G, Gatto MR, Alessandri Bonetti G. The effect of diode superpulsed low-level laser therapy on experimental orthodontic pain caused by elastomeric separators: a randomized controlled clinical trial. Lasers Med Sci. 2015;30(1):35–41. | ||
Farias RD, Closs LQ, Miguens SA Jr. Evaluation of the use of low-level laser therapy in pain control in orthodontic patients: a randomized split-mouth clinical trial. Angle Orthod. 2016;86(2):193–198. | ||
Eslamian L, Borzabadi-Farahani A, Hassanzadeh-Azhiri A, Badiee MR, Fekrazad R. The effect of 810-nm low-level laser therapy on pain caused by orthodontic elastomeric separators. Lasers Med Sci. 2014;29(2):559–564. | ||
AlSayed H, Sultan K, Hamadah O. Evaluating low-level laser therapy effect on reducing orthodontic pain using two laser energy values: a split-mouth randomized placebo-controlled trial. Eur J Orthod. Epub 2017 May 2. | ||
Almallah MM, Almahdi WH, Hajeer MY. Evaluation of low level laser therapy on pain perception following orthodontic elastomeric separation: a randomized controlled trial. J Clin Diagn Res. 2016;10(11):ZC23–ZC28. | ||
Doshi-Mehta G, Bhad-Patil WA. Efficacy of low-intensity laser therapy in reducing treatment time and orthodontic pain: a clinical investigation. Am J Orthod Dentofacial Orthop. 2012;141(3):289–297. | ||
Sobouti F, Khatami M, Chiniforush N, Rakhshan V, Shariati M. Effect of single-dose low-level helium-neon laser irradiation on orthodontic pain: a split-mouth single-blind placebo-controlled randomized clinical trial. Prog Orthod. 2015;16:32. | ||
Dalaie K, Hamedi R, Kharazifard MJ, Mahdian M, Bayat M. Effect of low-level laser therapy on orthodontic tooth movement: a clinical investigation. J Dent (Tehran). 2015;12(4):249–256. | ||
Tortamano A, Lenzi DC, Haddad AC, Bottino MC, Dominguez GC, Vigorito JW. Low-level laser therapy for pain caused by placement of the first orthodontic archwire: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2009;136(5):662–667. | ||
Domínguez A, Velásquez SA. Effect of low-level laser therapy on pain following activation of orthodontic final archwires: a randomized controlled clinical trial. Photomed Laser Surg. 2013;31(1):36–40. | ||
Bicakci AA, Kocoglu-Altan B, Toker H, Mutaf I, Sumer Z. Efficiency of low-level laser therapy in reducing pain induced by orthodontic forces. Photomed Laser Surg. 2012;30(8):460–465. | ||
Bayani S, Rostami S, Ahrari F, Saeedipouya I. A randomized clinical trial comparing the efficacy of bite wafer and low level laser therapy in reducing pain following initial arch wire placement. Laser Ther. 2016;25(2):121–129. | ||
Bartlett BW, Firestone AR, Vig KW, Beck FM, Marucha PT. The influence of a structured telephone call on orthodontic pain and anxiety. Am J Orthod Dentofacial Orthop. 2005;128(4):435–441. | ||
Cozzani M, Ragazzini G, Delucchi A, et al. Self-reported pain after orthodontic treatments: a randomized controlled study on the effects of two follow-up procedures. Eur J Orthod. 2016;38(3):266–271. | ||
Benson PE, Razi RM, Al-Bloushi RJ. The effect of chewing gum on the impact, pain and breakages associated with fixed orthodontic appliances: a randomized clinical trial. Orthod Craniofac Res. 2012;15(3):178–187. | ||
Otasevic M, Naini FB, Gill DS, Lee RT. Prospective randomized clinical trial comparing the effects of a masticatory bite wafer and avoidance of hard food on pain associated with initial orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2006;130(1):6.e9–e15. | ||
Eslamian L, Borzabadi-Farahani A, Edini HZ, Badiee MR, Lynch E, Mortazavi A. The analgesic effect of benzocaine mucoadhesive patches on orthodontic pain caused by elastomeric separators, a preliminary study. Acta Odontol Scand. 2013;71(5):1168–1173. | ||
Eslamian L, Borzabadi-Farahani A, Gholami H. The effect of benzocaine and ketoprofen gels on pain during fixed orthodontic appliance treatment: a randomized, double-blind, crossover trial. Aust Orthod J. 2016;32(1):64–72. | ||
Eslamian L, Gholami H, Mortazavi SA, Soheilifar S. Effect of 5% benzocaine gel on relieving pain caused by fixed orthodontic appliance activation. A double-blind randomized controlled trial. Orthod Craniofac Res. 2016;19(4):190–197. | ||
Eslamian L, Kianipour A, Mortazavi SAR. The analgesic efficacy of 5% naproxen gel for pain associated with orthodontic separator placement: a randomized double-blind controlled trial. Anesth Pain Med. 2017;7(2):e42708. | ||
Sawada A, Usui N, Shimazaki K, Taira M, Ono T. The effects of cognitive behavioral therapy on experimental orthodontic pain. Orthodontic Waves. 2015;74(1):10–14. | ||
Wang J, Jian F, Chen J, et al. Cognitive behavioral therapy for orthodontic pain control: a randomized trial. J Dent Res. 2012;91(6):580–585. | ||
Wang J, Wu D, Shen Y et al. Cognitive behavioral therapy eases orthodontic pain: EEG states and functional connectivity analysis. Oral Dis. 2015;21(5):572–582. | ||
Zheng Q, Zhang LH, Huang L, Wang GP, Yuan XP, Xu XM. [Effects of different psychological interventions on relieving orthodontic pain in patients with different personalities: a preliminary study]. Shanghai Kou Qiang Yi Xue. 2016;25(1):91–96. Chinese. | ||
Huang R, Wang J, Wu D, et al. The effects of customized brainwave music on orofacial pain induced by orthodontic tooth movement. Oral Dis. 2016;22(8):766–774. | ||
Xu X, Zhang L, Jiang Y, Huang Y, Huang S, Yang S. Clinical research of music in relieving orthodontic pain. Hua Xi Kou Qiang Yi Xue Za Zhi. 2013;31(4):365–368. | ||
Lobre WD, Callegari BJ, Gardner G, Marsh CM, Bush AC, Dunn WJ. Pain control in orthodontics using a micropulse vibration device: a randomized clinical trial. Angle Orthod. 2016;86(4):625–630. | ||
Miles P, Smith H, Weyant R, Rinchuse DJ. The effects of a vibrational appliance on tooth movement and patient discomfort: a prospective randomized clinical trial. Aust Orthod J. 2012;28(2):213–218. | ||
Woodhouse NR, DiBiase AT, Johnson N, et al. Supplemental vibrational force during orthodontic alignment: a randomized trial. J Dent Res. 2015;94(5):682–689. | ||
Esper MA, Nicolau RA, Arisawa EA. The effect of two phototherapy protocols on pain control in orthodontic procedure: a preliminary clinical study. Lasers Med Sci. 2011;26(5):657–563. | ||
Farzanegan F, Zebarjad SM, Alizadeh S, Ahrari F. Pain reduction after initial archwire placement in orthodontic patients: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2012;141(2):169–173. | ||
Ireland AJ, Ellis P, Jordan A, et al. Comparative assessment of chewing gum and ibuprofen in the management of orthodontic pain with fixed appliances: a pragmatic multicenter randomized controlled trial. Am J Orthod Dentofacial Orthop. 2016;150(2):220–227. | ||
Murdock S, Phillips C, Khondker Z, Hershey HG. Treatment of pain after initial archwire placement: a noninferiority randomized clinical trial comparing over-the-counter analgesics and bite-wafer use. Am J Orthod Dentofacial Orthop. 2010;137(3):316–323. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.