")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Optimal management of Ménière’s disease
Authors Foster C
Received 11 November 2014
Accepted for publication 20 January 2015
Published 25 February 2015 Volume 2015:11 Pages 301—307
DOI https://doi.org/10.2147/TCRM.S59023
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Garry Walsh
Carol A Foster
Department of Otolaryngology, University of Colorado School of Medicine, Aurora, Colorado, USA
Abstract: Confusion in the nomenclature of Ménière’s disease and lack of a standard definition of the disorder until 1995 has hampered accurate assessment of treatment efficacy since the presently defined disorder was first described in 1938. The lack of a widely accepted mechanism of the disease has also delayed the development of rational treatments. Past treatments have focused on relieving elevated pressures in the hydropic ear and more recently on treatment of underlying migraine. Present dietary methods of control include sodium restriction and migraine trigger elimination. Pharmacologic treatments include diuretics, migraine prophylactic medications, histamine analogs, and oral steroids. Surgical procedures include intratympanic steroid perfusion, shunts, and ablative procedures when conservative treatments fail. External pressure devices are also used. Evidence of efficacy is lacking for most interventions other than ablation.
At our institution, Ménière’s disease is treated as a cerebrovascular disorder. Control of risk factors for cerebrovascular ischemia is combined with treatment of pressure dysfunction in the hydropic ear. Screening for risk factors is performed at presentation. Migraine, dyslipidemia, obesity, diabetes, sleep apnea, hypertension, and atherosclerosis are among the major factors that often require medical management. Migraine prophylactic medications, magnesium supplementation, sodium restriction, migraine trigger elimination, diuretics, anticoagulants, and antihypertensives are among the treatments used initially. Steroids administered orally or intratympanically are used if control is not achieved medically, and ablation remains the definitive treatment in unilateral cases experiencing treatment failure.
Keywords: endolymphatic hydrops, migraine, cerebrovascular disorders, ischemia
Introduction
Progress in controlling the symptoms of Ménière’s disease has been frustratingly slow. For the first few decades after Meniere identified the ear as the source of vertigo spells in 1861, his name was applied indiscriminately to a host of chronic dizziness disorders that lacked a common pathology. It was not until the 1938 description of the disorder by Hallpike and Cairns1 that the definition of the disease began to approach its present form, and only since the 1995 American Academy of Otolaryngology-Head and Neck Surgery (AAOHNS) criteria2 has a clear, unambiguous, and sufficiently narrow definition of the disorder been available to researchers. This confusion in nomenclature means that many articles purporting to treat Ménière’s disease over the past 75 years have included patients with unrelated disorders, interfering with proper assessment of treatment efficacy.
A second factor that has impaired treatment progress is the lack of consensus on a mechanism for the disorder. There have been two major opposing factions since the Hallpike and Cairns paper was published.1 One broad group believes that endolymphatic hydrops and Ménière’s disease are synonymous and that treatments directed at hydrops should be sufficient to control symptoms.3 Within this “hydrops group”, it is currently believed that the onset of hydrops is probably multifactorial, including viral infection, autoimmunity, and other disorders as causes. Since the 1950s, the spells have been ascribed to sudden silencing of the inner ear due to contamination of the perilymph with endolymph after rupture of the membrane,3 although this mechanism has been seriously questioned over the past few decades.4 There is no longer a clear consensus on the mechanism by which hydrops results in attacks in this group, but treatments continue to focus on decompressing the hydropic ear either through medications or by surgical intervention.
The other major group, the “migraine group” believed early on that migraine explains many cases of the disorder, perhaps through the mechanism of ischemia due to vasospasm.5,6 Some researchers have rejected hydrops as causal in the disorder.7 Genetic factors or the presence of an ion channelopathy have been invoked to explain the association.8 Treatment strategies involve using medications to prevent migraine-associated vasospasm or neurosensory disturbances.9
Both sides have developed a considerable arsenal of papers supporting their positions. In the absence of consensus, treatments for Ménière’s disease have been based on empirical success with patients rather than on a formal pathologic rationale. At the University of Colorado, we combine treatments from both groups along with additional treatments because we believe that Ménière’s disease results from a combination of hydrops with a variety of risk factors for cerebrovascular disease, including maladies as disparate as migraine, sleep apnea, atherosclerosis, and autoimmune disorders.10,11 We have hypothesized that hydrops acts as an intermittent Starling resistor to lower perfusion pressure in the inner ear, which is additive with other causes of lowered perfusion such as cerebrovascular diseases. In our theory, progressive damage is attributed to calyceal and dendritic ischemia–reperfusion injury (excitotoxicity). The treatments we advocate are directed at mitigating the vascular risk factors that trigger spells and also at lowering pressure fluctuations in the affected ear.
The current AAOHNS definition of the disorder describes a very specific type of hours-long attack, during which the sufferer experiences acute hearing loss, roaring tinnitus, a sensation of fullness in the ear, and intense vertigo with the illusion of environmental rotation. Over time, a progressive hearing loss develops in the affected ear. No treatment has thus far been shown to stop the inevitable progression to deafness in the afflicted ear. Vertigo spells can be controlled with high efficacy, but the favored means are destructive: gentamicin ablation, vestibular neurectomy, and labyrinthectomy. The rationale for these treatments is to functionally disconnect the labyrinth, relieving the most intrusive symptom of vertigo, after which the ear continues to follow its progressive downhill audiologic course. Destructive procedures are not usually used in bilateral cases because this results in the disabling symptom of oscillopsia.
Given the destructive nature of the most effective procedures, treating physicians usually prefer to temporize for months or years after a case presents itself. Delaying destructive treatments allows time to ascertain that only one ear is involved; it provides time for interim treatments that, if successful, may render destruction unnecessary, and it allows repeated testing to ensure that the ear is inevitably declining. This review will focus on these interim treatments.
Dietary methods
Sodium restriction
This has been widely used to control symptoms of Ménière’s disease since 1931.12 Reduction of dietary sodium combined with diuretics has been reported to slow progression of hearing loss in Ménière’s disease.13 Some advocate moderate regulation of sodium intake rather than harsh restriction.9 The literature lacks controlled studies of this therapy based on modern Ménière’s disease definitions.
Therapeutic rationale
Members of the hydrops group were early advocates of this treatment because it was thought to lower pressure in the hydropic ear, reducing the risk of membrane rupture. Sodium restriction has not been advocated as a migraine treatment, but reduction of monosodium glutamate intake as a part of sodium restriction maybe helpful in migraine because glutamate is a known trigger for migraine.14 A low-sodium diet is also useful in controlling hypertension, a vascular risk factor.15
Migraine trigger elimination
Common migraine food triggers include monosodium glutamate, chocolate, red wine, fermented dairy products including yogurt, and aged or pickled foods.16 Trigger elimination is advocated as treatment for migraine-associated vestibular disorders,17 but controlled studies demonstrating the efficacy of this treatment in Ménière’s disease are lacking.
Therapeutic rationale
The migraine group recommends avoidance of these foods with the belief that Ménière’s disease will fluctuate and worsen if migraines are uncontrolled.9 There is no expectation that these triggers modify hydrops, but they are often included in dietary regimens for hydrops control based on their empiric efficacy.18 Our protocol is to recommend avoidance of these food triggers in patients with migraine headaches, aura, or in Ménière’s patients under the age of 50 years because migraine is the most common vascular risk factor in that group.
Pharmacologic methods
Diuretics
A combination of hydrochlorothiazide and triamterene is the most commonly used medical treatment for Ménière’s disease. Acetazolamide, furosemide, and spironolactone are also used by some. Combining these with sodium restriction has slowed progression of hearing loss.13 A recent Cochrane review regarding diuretics in Ménière’s disease noted that no articles supporting diuretic use that meet accepted review standards are presently available in the literature.19
Therapeutic rationale
Like the sodium-restricted diet described earlier, diuretics have been used in the belief that pressures in the hydropic ear may be reduced by the drug. Acetazolamide is also used in the treatment of migraine with aura, so it has been used by both the hydrops and migraine groups. In our center, we use hydrochlorothiazide with triamterene in Ménière’s disease patients without migraine, particularly for those with hypertension and atherosclerosis. Acetazolamide is used for those who have migraine with aura or as a second-line agent in patients with migraine who do not respond to other migraine prophylactic medications. There is a risk for renal calculi with this medication, so patients are advised to increase fluid and citrus intake.
Migraine prophylactic medications
Amitriptyline, beta blockers, calcium channel blockers, acetazolamide, and topiramate are commonly used in the prevention of migraine headaches14 and are also used for vestibular symptoms in migraineurs.17 Migraine prophylactic medications are used by some centers for Ménière’s disease but controlled studies are lacking.
Therapeutic rationale
Migraine and hydrops have not been shown to be causally related, so migraine prophylactic medications are generally used only by the migraine group with the belief that vasospasm and other migraine phenomena can be controlled by these drugs. Calcium channel blockers such as verapamil, and in Europe, flunarizine, are effective in migraineurs.20 The carbonic anhydrase inhibitors have some diuretic effects and so may impact hydrops directly in addition to treating migraine. The blockers are also used in the treatment of hypertension and so may be of use in Ménière’s patients who also have migraine and hypertension.
Histamine and related medications
Histamine was first advocated over 50 years ago by the migraine group because the intense facial flushing it causes was hoped to reflect increased perfusion to the ear. This has not stood the scrutiny of time. Niacin was also used for a similar reason, and like histamine it has faded from use.
Betahistine is a modern analog, although the mechanism of action has been attributed to central vestibular effects as well as to vascular effects. Recent work suggests that it has positive effects on cochlear blood flow.21 A 2001 Cochrane review has found no definitive evidence of efficacy in the treatment of the vertigo spells, and no effect on hearing or tinnitus.22 It continues to be a popular drug in Europe and Canada, but is not approved in the United States based on lack of efficacy.
Oral steroids
Oral steroids have been used for treatment with the belief that inflammation or immunologic factors or a direct effect on the vestibular nucleus may reduce the severity of spells.23 This study using 18 months of steroid treatment reported a 50% improvement in vertigo spell frequency.
Intratympanic perfusion
Steroids
Intratympanic steroids have been noted to have a calming effect on Ménière’s ears.24 The number and severity of spells seem to decrease for up to 2 years after use.25
Therapeutic rationale
Steroids are not useful in migraine and there is no plausible mechanism for alteration of hydropic distention by steroids. Improvement in Ménière’s disease has been hypothesized to occur when hydrops is due to inflammation or autoimmune factors.24 Steroids are used to reduce edema after ischemic stroke,26 so steroid-responsive Ménière’s disease also supports ischemia as a mechanism of attacks. Steroids are also used successfully to treat sudden sensorineural hearing loss,27 with improvement attributed to a reduction in inflammation and improvement in blood flow to the cochlea.28
Surgery directed at hydrops
Surgeries to relieve distention of the endolymphatic system
Endolymphatic shunts of various kinds, cochleosacculotomy, and endolymphatic sac decompressions have been used for many decades. Improvement in vertigo control has been achieved in about two-thirds of treated patients.29 This is similar to the improvement seen in nonsurgically treated cases over time.30 None have been shown to be as effective as destructive procedures.31 The possibility that any improvement found in prior studies is due to the placebo effect has been repeatedly raised.32 On autopsy studies, shunts have been found to be malpositioned or occluded, suggesting that any impact might be temporary.33
Shunt procedures are still popular and are the major nondestructive surgical treatment for the disorder. Over 80% of otologists use shunts for medically refractory Ménière’s disease. They are appealing for patients with bilateral Ménière’s because ablative procedures cannot be used in that group. There is no evidence that shunts alter the natural history of the disease.30
Therapeutic rationale
The migraine group does not advocate these surgeries because they believe hydrops is not a critical factor in causation of attacks. The hydrops group, however, has long felt that elevated endolymph pressures cause the distention of hydrops, and so have devised these treatments to shunt endolymph and relieve this pressure. At the University of Colorado, shunts are performed infrequently, more often in those with bilateral disease, and when control cannot be achieved with treatment of vascular risk factors. Complete, lifelong control of vertigo is rarely achieved by shunting.
Devices
External pressure device (Menniett)
While a trend toward improvement in vertigo has been identified with this device,34,35 improvement also occurs in the natural history of the disease.30 A long-term follow-up showed 75% improvement in frequency and severity of spells,36 which is similar to the improvement in untreated patients. This is a relatively expensive device, and a cost–benefit analysis is lacking.
Therapeutic rationale
This device is advocated by the hydrops group and the purported mechanism of action is either transmission of pulsed pressure to the endolymph space, presumably relieving hydrops by massaging fluid out of the endolymph space, or another as yet unknown mechanism.35
Suppressant medications
Benzodiazepines, meclizine, other antihistamines such as promethazine or diphenhydramine, and transdermal scopolamine patches have all been used to control the sensation of vertigo during acute attacks. These medications have no effect on the progression of the disorder. However, they are useful in controlling vegetative symptoms during attacks and can help patients during the interval before ablative surgery is contemplated.37 Transdermal scopolamine patches require 4 hours to reach a therapeutic blood level of scopolamine and continue to release drug for 72 hours,38 which is a poor match for typical Ménière’s attacks of sudden onset and duration of a few hours. Meclizine is often useful to reduce nausea for milder spells, oral benzodiazepines are well tolerated for more severe spells, and promethazine suppositories can be used for the most severe spells with intractable vomiting.
The University of Colorado protocol
The cornerstone of our treatment protocol is the identification and control of disorders that impair cerebral and inner ear vascular perfusion. Patients with a history of classic Ménière’s attacks are screened for a number of common vascular disorders (Table 1). Initial screening is by history and examination. All patients with this diagnosis undergo magnetic resonance imaging of the internal auditory canals as part of the screening process.
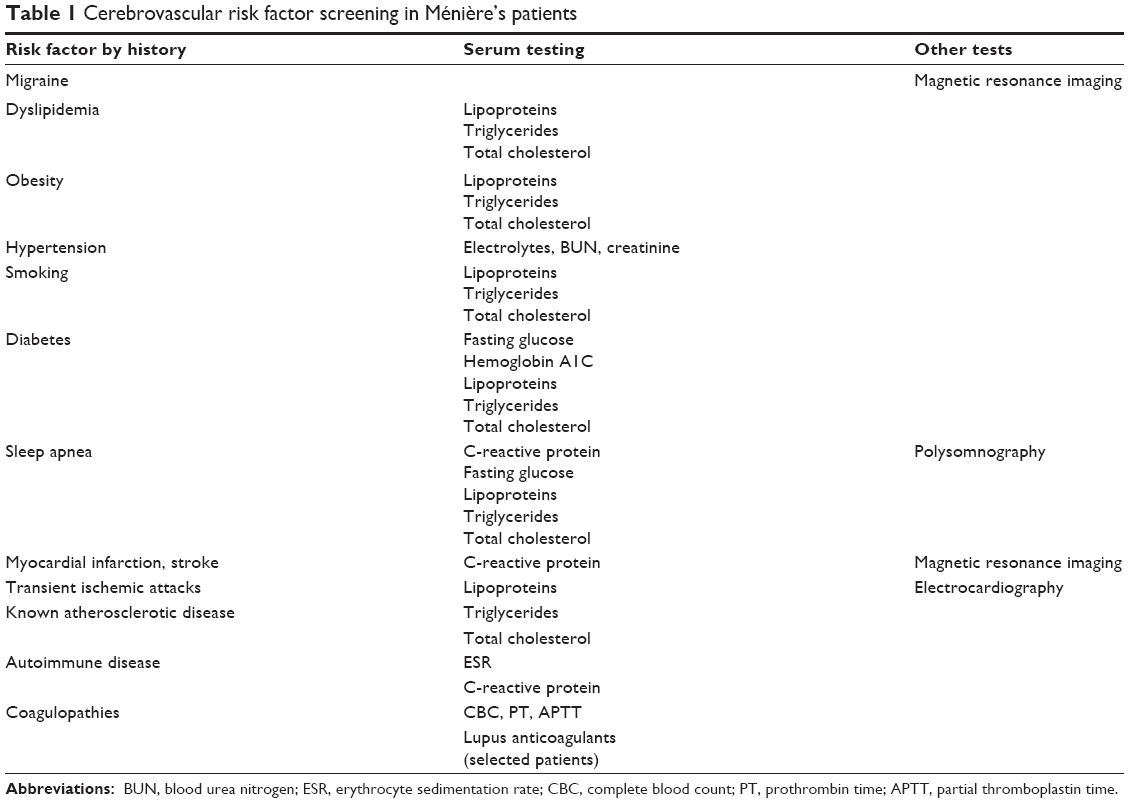 | Table 1 Cerebrovascular risk factor screening in Ménière’s patients |
Migraine is closely associated with Ménière’s attacks in adults under the age of 50 years. Serum testing is only done in these younger patients when there is no personal or family history of migraine or when other vascular risk factors are evident in the history or on examination. All obese patients and those over the age of 50 years receive serum screening consisting of a standard metabolic panel (glucose, blood urea nitrogen, creatinine, electrolytes), complete blood count, erythrocyte sedimentation rate, C-reactive protein, lipid screening (cholesterol, lipoprotein profile, triglycerides), and coagulation screening (platelets, prothrombin time, activated partial thromboplastin time, fibrinogen). Additional selected tests may be performed on patients with more complex disorders, such as autoimmune disease.
Treatments are tailored to the underlying vascular risk factor (Table 2). Migraine patients and all patients under the age of 50 years without other known vascular disorders are managed with migraine trigger elimination and daily magnesium supplements. Those who continue to have attacks are given migraine prophylactic medications. All patients over the age of 50 years are given diuretics, daily low-dose aspirin (80 mg), and magnesium supplementation. Modest sodium restriction (2,000 mg/day) is also recommended. Each identified vascular risk factor is treated either in our clinic or by coordination with the patient’s other care providers. Transtympanic or oral steroids are used after initial treatment failure in all groups. Four or more classic unilateral attacks during a year or more of treatment is considered inadequate control, and these patients are usually referred for ablative procedures. Because bilateral ablation is disabling, bilateral patients who fail conservative treatment may be offered other options such as shunting and pressure devices.
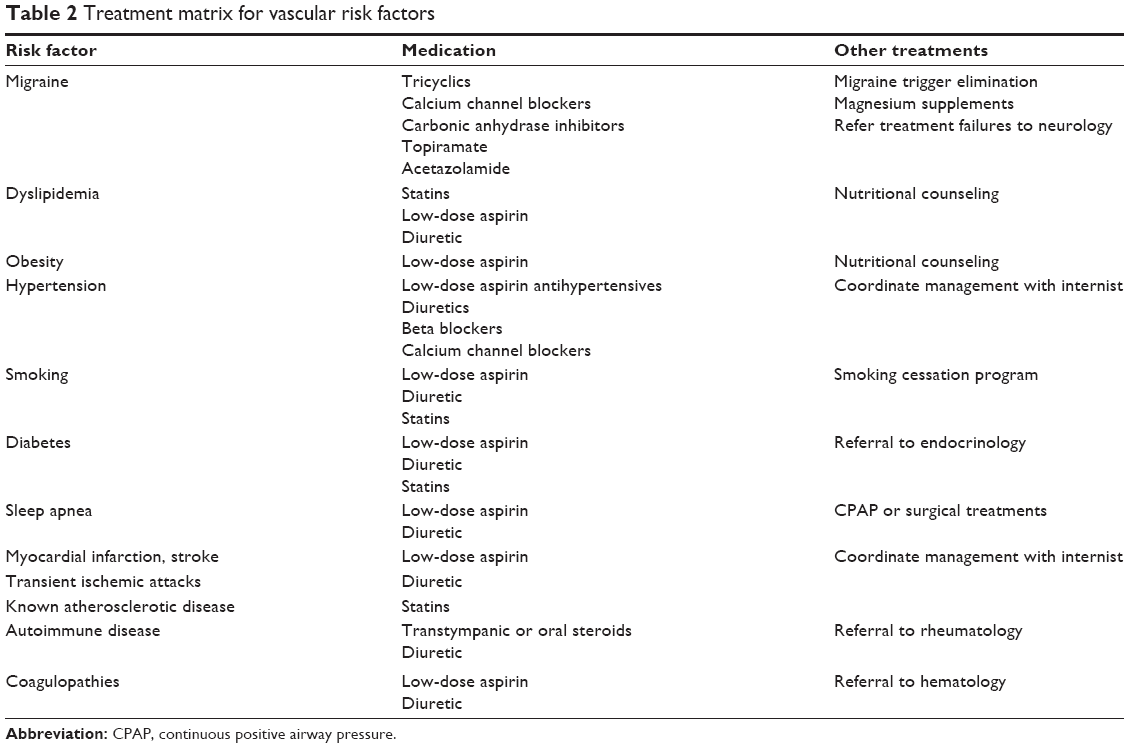 | Table 2 Treatment matrix for vascular risk factors |
Disclosure
The author has no conflict of interest to report regarding this work.
References
Hallpike C, Cairns H. Observations on the pathology of Ménière’s syndrome. J Laryngol Otol. 1938;53:625–654. | ||
Committee on Hearing and Equilibrium. Committee on hearing and equilibrium guidelines for the diagnosis and evaluation of therapy in Ménière’s disease otolaryngology. Head Neck Surg. 1995;113:181–185. | ||
Schuknecht HF. Pathophysiology of endolymphatic hydrops. Arch Otorhinolaryngol. 1976;212(4):253–262. | ||
Brown DH, McClure JA, Downar-Zapolski Z. The membrane rupture theory of Ménière’s disease – is it valid? Laryngoscope. 1988;98(6):599–601. | ||
Radtke A, Lempert T, Gresty MA, Brookes GB, Bronstein AM, Neuhauser H. Migraine and Ménière’s disease: is there a link? Neurology. 2002;59(11):1700–1704. | ||
Cha YH, Brodsky J, Ishiyama G, Sabatti C, Baloh RW. The relevance of migraine in patients with Ménière’s disease. Acta Otolaryngol. 2007;127(12):1241–1245. | ||
Merchant S, Adams J, Nadol J. Pathophysiology of Ménière’s syndrome: are symptoms caused by endolymphatic hydrops? Otol Neurotol. 2005;26:74–81. | ||
Baloh RW. Migraine and vertigo: epidemiology, genetics, and mechanism(s). Headache Curr. 2006;3(1):1–7. | ||
Rauch SD. Clinical hints and precipitating factors in patients suffering from Ménière’s disease. Otolaryngol Clin North Am. 2010;43(5):1011–1017. | ||
Foster CA, Breeze RE. The Meniere attack: an ischemia/reperfusion disorder of inner ear sensory tissues. Med Hypotheses. 2013;81(6):1108–1115. | ||
Foster CA, Breeze RE. Endolymphatic hydrops in Ménière’s disease: cause, consequence, or epiphenomenon? Otol Neurotol. 2013;34(7):1210–1214. | ||
Gates G. Ménière’s disease: medical therapy. In: Harris JP, editor. Ménière’s Disease. The Hague, Netherlands: Kugler publications; 1999:329–340. | ||
Santos PM, Hall RA, Snyder JM, Hughes LF, Dobie RA. Diuretic and diet effect on Ménière’s disease evaluated by the 1985 Committee on Hearing and Equilibrium guidelines. Otolaryngol Head Neck Surg. 1993;109(4):680–689. | ||
Chan K, MaassenVanDenBrink A. Glutamate receptor antagonists in the management of migraine. Drugs. 2014;74(11):1165–1176. | ||
Ha SK. Dietary salt intake and hypertension. Electrolyte Blood Press. 2014;12(1):7–18. | ||
Sun-Edelstein C, Mauskop A. Foods and supplements in the management of migraine headaches. Clinical J Pain. 2009;25(5):446–452. | ||
Bisdorff AR. Management of vestibular migraine. Ther Adv Neurol Disord. 2011;4(3):183–191. | ||
Sajadi H, Paparella MM. How I do it: medical management of Ménière’s disease. In: Harris JP, editor. Ménière’s Disease. The Hague, Netherlands: Kugler publications; 1999:343–345. | ||
Thirlwall AS, Kundu S. Diuretics for Ménière’s disease or syndrome. Cochrane Database Syst Rev. 2006;(3):Cd003599. | ||
Yacovino DA, Hain TC. Medical management of vertigo. In: Dispenza F, De Stefano A, editors. Textbook of Vertigo: Diagnosis and Management. New Delhi: Jaypee Brothers Medical Publishers; 2014:219–236. | ||
Ihler F, Bertlich M, Sharaf K, Strieth S, Strupp M, Canis M. Betahistine exerts a dose-dependent effect on cochlear stria vascularis blood flow in Guinea pigs in vivo. PLoS One. 2012;7(6):e39086. | ||
James A, Burton Martin J. Betahistine for Ménière’s Disease or Syndrome. Cochrane Database of Systematic Reviews. Hoboken, NJ: John Wiley & Sons, Ltd; 2001. | ||
Morales-Luckie E, Cornejo-Suarez A, Zaragoza-Contreras MA, Gonzalez-Perez O. Oral administration of prednisone to control refractory vertigo in Ménière’s disease: a pilot study. Otol Neurotol. 2005;26(5):1022–1026. | ||
Barrs DM, Keyser JS, Stallworth C, McElveen JT. Intratympanic steroid injections for intractable Ménière’s disease. Laryngoscope. 2001;111(12):2100–2104. | ||
Phillips JS, Westerberg B. Intratympanic steroids for Ménière’s disease or syndrome. Cochrane Database Syst Rev. 2011;(7):Cd008514. | ||
Norris JW. Steroids may have a role in stroke therapy. Stroke. 2004;35(1):228–229. | ||
Stachler RJ, Chandrasekhar SS, Archer SM, et al; American Academy of Otolaryngology-Head and Neck Surgery. Clinical practice guideline: sudden hearing loss. Otolaryngol Head Neck Surg. 2012;146(3 suppl):S1–S35. | ||
Doyle KJ, Bauch C, Battista R, et al. Intratympanic steroid treatment: a review. Otol Neurotol. 2004;25(6):1034–1039. | ||
Brinson GM, Chen DA, Arriaga MA. Endolymphatic mastoid shunt versus endolymphatic sac decompression for Ménière’s disease. Otolaryngol Head Neck Surg. 2007;136(3):415–421. | ||
Silverstein H, Smouha E, Jones R. Natural history vs surgery for Ménière’s disease. Otolaryngol Head Neck Surg. 1989;100(1):6–16. | ||
Hillman TA, Chen DA, Arriaga MA. Vestibular nerve section versus intratympanic gentamicin for Ménière’s disease. Laryngoscope. 2004;114(2):216–222. | ||
Bretlau P, Thomesen J, Tos M, Johnsen NJ. Placebo effect in surgery for Ménière’s disease: nine-year follow-up. Otol Neurotol. 1989;10(4):259–261. | ||
Chung JW, Fayad J, Linthicum F, Ishiyama A, Merchant SN. Histopathology after endolymphatic sac surgery for Ménière’s syndrome. Otol Neurotol. 2011;32(4):660–664. | ||
Thomsen J, Sass K, Odkvist L, Arlinger S. Local overpressure treatment reduces vestibular symptoms in patients with Ménière’s disease: a clinical, randomized, multicenter, double-blind, placebo-controlled study. Otol Neurotol. 2005;26(1):68–73. | ||
Gates GA, Green JD Jr, Tucci DL, Telian SA. The effects of transtympanic micropressure treatment in people with unilateral Ménière’s disease. Arch Otolaryngol Head Neck Surg. 2004;130(6):718–725. | ||
Dornhoffer JL, King D. The effect of the Meniett device in patients with Ménière’s disease: long-term results. Otol Neurotol. 2008;29(6):868–874. | ||
Foster CA, Baloh RW. Drug therapy for vertigo. In: Baloh RW, Halmagyi GM, editors. Disorders of the Vestibular System. New York: Oxford University Press; 1996:541–550. | ||
Antor MA, Uribe AA, Erminy-Falcon N, et al. The effect of transdermal scopolamine for the prevention of postoperative nausea and vomiting. Front Pharmacol. 2014;5:55. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.