Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Optimal Discharge Education: Evidence for Enhancing Family Preparedness for Premature Infants
Authors Zhang L ![]() , He J, Zhou Y
, He J, Zhou Y ![]() , Li X
, Li X
Received 31 December 2024
Accepted for publication 14 April 2025
Published 8 May 2025 Volume 2025:18 Pages 2551—2563
DOI https://doi.org/10.2147/JMDH.S515110
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract of “Enhancing Family Preparedness for Premature Infants” [515110].
Views: 184
Lingping Zhang,1,2 Junjie He,3 Yue Zhou,3 Xiaomei Li1
1School of Nursing, Health Science Center, Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 2Department of Neonatology, Children’s Medical Center, the Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China; 3Department of Pediatrics, Southwest Medical University, Luzhou, Sichuan, People’s Republic of China
Correspondence: Xiaomei Li, School of Nursing, Health Science Center, Xi’an Jiaotong University, #76, Yanta West Road, Xi’an, Shaanxi, 710061, People’s Republic of China, Email [email protected]
Objective: The study aimed to systematically search, screen, evaluate, and synthesize evidence regarding the effectiveness of discharge education in enhancing family preparedness for premature infants. The ultimate goal was to provide evidence-based references for implementing discharge education for family caregivers, thereby improving families’ discharge readiness and enhancing home care and infant health.
Methods: Systematic searches were conducted across BMJ Best Practice, UpToDate, the Cochrane Library, and other relevant databases from October 2014 to October 2024. The collected literature comprised clinical decisions, guidelines, expert consensuses, systematic reviews, meta-analyses, best practices, and randomized controlled trials related to discharge education for enhancing family preparedness for premature infants. Relevant evaluation tools were selected based on the type of literature to assess methodological quality, and the evidence was extracted, summarized, and organized.
Results: A total of 1724 documents were searched. Ultimately, ten pieces of literature were selected based on the inclusion and exclusion criteria, comprising one clinical decision, one guideline, one expert consensus, two systematic reviews, one meta-analysis, one best practice, and three randomized controlled trials. From these literature, a total of thirty-three pieces of evidence were extracted and synthesized across five domains: assessment, planning, implementation, evaluation, and support.
Conclusion: This study synthesized evidence on discharge education for premature infant’ families, revealing key insights for clinical practice. It emphasized tailored education plans, early family involvement, multidisciplinary collaboration, and diverse teaching methods. Implementing these practices is expected to improve families’ discharge readiness, thereby promoting better infant health.
Keywords: discharge education, family preparedness, premature infants, evidence synthesis
Introduction
Premature infants, defined as newborns delivered before 37 weeks of gestation, face heightened nursing challenges because of their incomplete physiological development.1 Due to the immaturity of their physiological systems, these infants frequently encounter challenges such as high risk of infection, difficulties with feeding, and neurodevelopmental concerns. Therefore, they necessitate more meticulous and professional care post-discharge.2–4 However, in reality, parents of premature infants frequently lack adequate preparedness at discharge, being deficient in essential nursing knowledge and skills to effectively address the various health challenges their infants may encounter at home.5,6
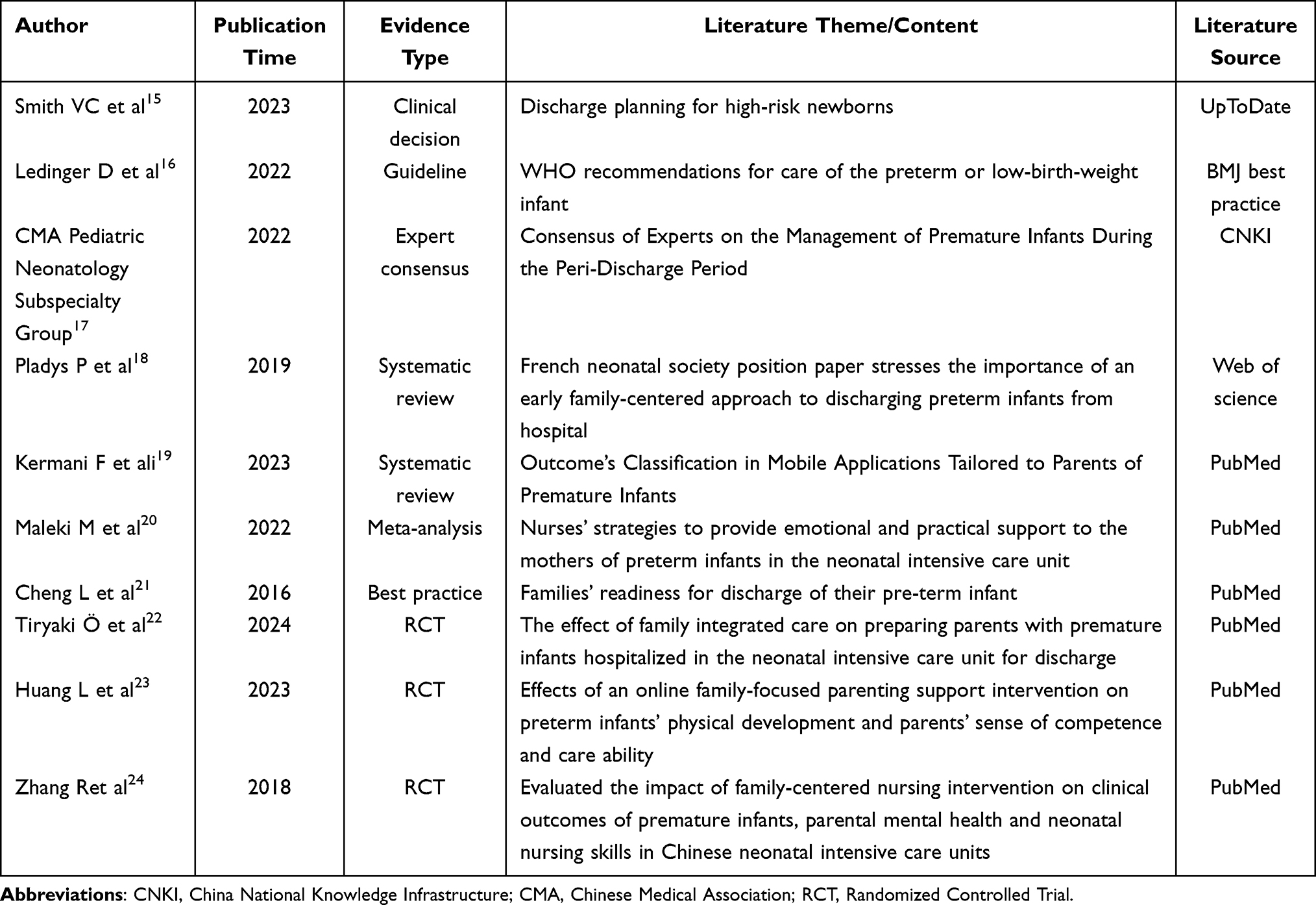 |
Table 1 Characteristics of the Included Studies (n=10) |
Discharge education is a crucial bridge connecting hospitals and families, which is pivotal in enhancing the family’s preparedness for premature infants. Research indicates that systematic discharge education can empower parents with skills in daily nursing techniques and knowledge of disease observation and prevention for premature infants.7,8 This facilitates better care for premature infants within the family setting, reducing rehospitalization rates and alleviating parents’ psychological stress, bolstering their confidence in parenting.9
Nonetheless, the current state of discharge education for families of premature infants leaves much to be desired. The absence of standardized discharge preparation protocols results in inconsistent educational content provided by healthcare professionals and different hospitals, failing to meet the practical needs of premature infant families.10 Inadequate discharge preparedness impacts their caregiving knowledge and abilities, potentially hindering the successful transition of premature infants from the neonatal intensive care unit (NICU) to the home environment, which may ultimately adversely affect the infants’ long-term healthy growth.
Consequently, an evidence-synthesis study on discharge education is urgently needed. By systematically reviewing and analyzing existing research findings, we aimed to extract systematic, effective, and practical evidence to inform discharge education practices, thereby providing a strong foundation for developing discharge education programs. This research was essential in enhancing families’ discharge preparedness, improving the health outcomes of premature infants, and fostering the standardization of discharge education practices.
Materials and Methods
Study Design and Setting
This study utilized the PIPOST framework to formulate evidence-based inquiries, with the inclusion criteria delineated according to specific parameters. a) Population: The target demographic for the application of evidence was families of premature infants. b) Intervention: The intervention method involved discharge education services to enhance families’ readiness for preterm discharge. c) Professional: The professionals responsible for implementing the evidence encompassed nurses and physicians within neonatal departments. d) Outcomes: Pertaining to families’ preparation for the discharge and subsequent care of premature infants. e) Setting: The settings for evidence application were neonatal departments in hospitals and associated caregiving institutions. f) Type of evidence: The types of evidence selected for analysis include clinical decisions, guidelines, best practices, expert consensuses, systematic reviews, meta-analyses, and randomized controlled trials (RCTs). Exclusion Criteria: Considering the primary focus of this evidence synthesis on discharge education for enhancing family preparedness for premature infants, any evidence that does not pertain to this central theme was excluded from consideration. This study has been registered with the Evidence-Based Nursing Center of Fudan University (ES20246804).
Evidence Search Strategy
To identify pertinent literature, the search strategy was designed in accordance with the “6S” hierarchy of evidence resources, adhering to a top-down search approach.11 Systematic electronic searches were executed on various platforms, encompassing BMJ Best Practice, UpToDate, the Cochrane Library. The scope of the search was further broadened to encompass evidence-based resource databases from the Registered Nurses’ Association of Ontario (RNAO), the Scottish Intercollegiate Guidelines Network (SIGN), the Global Initiative for Nursing (GIN), the National Institute for Health and Clinical Excellence (NICE), and the Joanna Briggs Institute (JBI). Additional searches were conducted in comprehensive databases, notably PubMed, the American Academy of Pediatrics (AAP), and Web of Science. Moreover, the investigation extended to Chinese databases, including CNKI (China National Knowledge Infrastructure), VIP (Vip Information), and Wanfang Database.
The English search terms encompassed phrases such as “premature/preterm infant/prematurity”, “parents/caregivers/family” and “discharge preparation/discharge readiness/discharge teaching/discharge education”. The specific English search strategy was as follows: ((((((((((premature[Title/Abstract]) OR (preterm infant[Title/Abstract])) OR (prematurity[Title/Abstract]))) AND (parents[Title/Abstract])) OR (caregivers[Title/Abstract])) OR (family[Title/Abstract])) AND (discharge preparation[Title/Abstract])) OR (discharge teaching[Title/Abstract])) OR (discharge readiness[Title/Abstract])) OR (discharge education[Title/Abstract]). Correspondingly, the Chinese search utilized semantically aligned keywords with the English search terms.
The search period was set from October 2014 to October 2024. The flowchart of literature screening is shown in Figure 1.
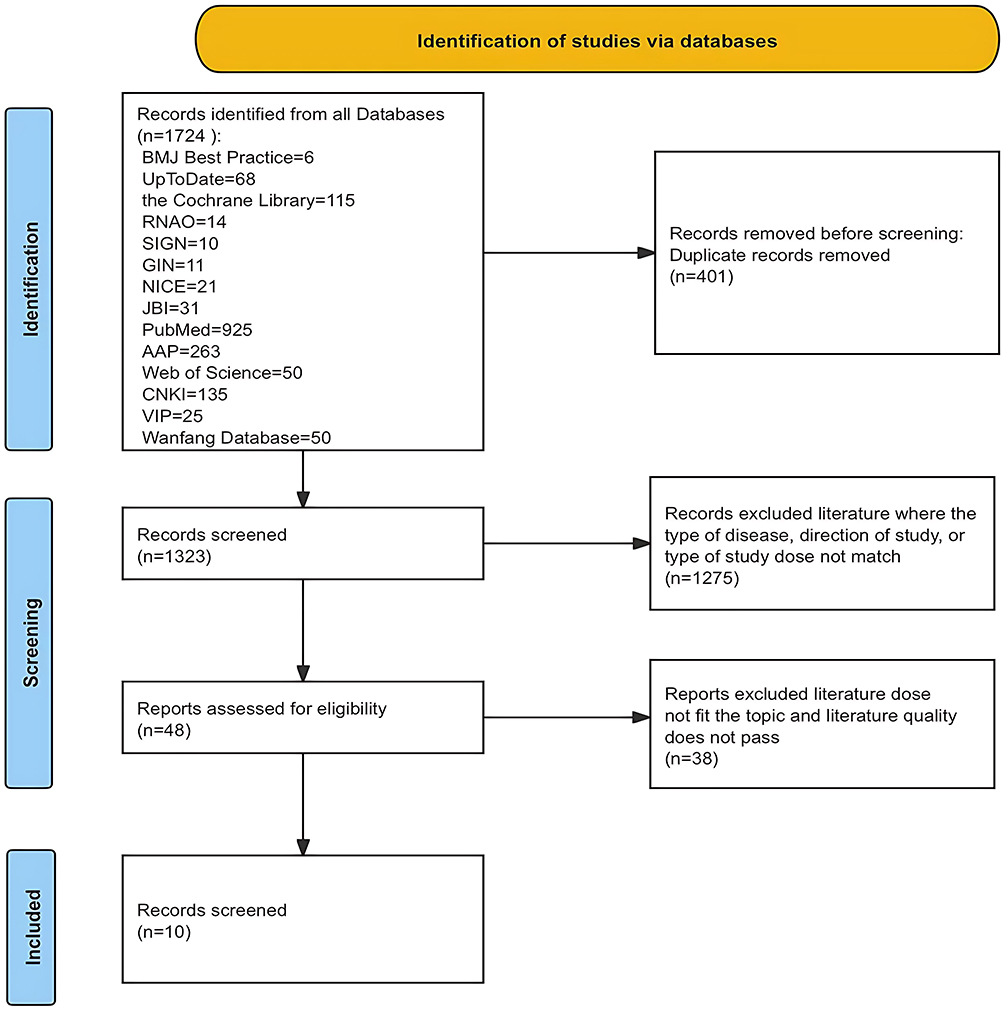 |
Figure 1 The flowchart of literature screening. |
Quality Assessment of Evidence
The research team conducted a meticulous assessment of the evidence quality, carefully selecting evaluation instruments that were specifically tailored to the distinct formats of the presented evidence. The quality of clinical decision was evaluated using the Critical Appraisal for Summaries of Evidence (CASE) tool.12 The Appraisal of Guidelines for Research and Evaluation II (AGREE II)13 was employed for the appraisal of guidelines. Both expert consensuses and best practices were assessed using the evaluation criteria for opinion and consensus statements developed by the JBI Evidence-Based Healthcare Center in Australia.25, The included systematic reviews and meta-analyses were evaluated using JBI’s quality assessment tool for systematic review literature.26 RCTs were assessed for quality using JBI’s RCT evaluation tool.26 Any discrepancies that emerged among the evaluators were resolved through deliberative consultation with a third experienced team member, leading to a unanimous conclusion.
Evidence Extraction, Summarization, and Grading
The literature was rigorously reviewed post-screening, with evidence extracted and summarized independently by two researchers. Disagreements were resolved through discussion with a third researcher. All involved personnel were trained in evidence-based nursing methodology. The evidence-based team comprehensively summarized the evidence based on the following principles: (I) For consistent content, preference was given to more comprehensible sentences; (II) Multiple complementary sources were integrated into single pieces of evidence; (III) In case of conflicting conclusions from different sources, priority was given to evidence-based on quality, credibility, and the most recent authoritative publications. Evidence was graded using the ‘2014 JBI Evidence Hierarchy and Recommendation Levels’.14 For the included clinical decision, guideline, expert consensus, systematic reviews, meta-analysis, and best practice the original sources were traced back for classification.
Results
Results of Literature Screening
In this study, a total of 1724 documents were searched. Ten documents were ultimately included after removing duplicates and conducting a thorough review of titles, abstracts, and full texts. The evidence screening process is shown in Figure 1.
General Characteristics of the Included Literature
The selected literature comprised of one clinical decision,15 one guideline,16 one expert consensus,17 two systematic reviews,18,19 one meta-analysis,20 one best practice,21 and three randomized controlled trials.22–24 Table 1 presents an overview of the essential characteristics of the included literature.
Quality Evaluation Results of the Included Studies
Quality Evaluation Results of the Clinical Decision
The CASE worksheet assessed the quality of the included clinical decision.15 The evaluation results for items 4 and 5 were “Not completely” while the remaining items were all rated as “Yes” The overall quality of this clinical decision was deemed moderate, and it was approved for inclusion. Details are provided in Table 2.
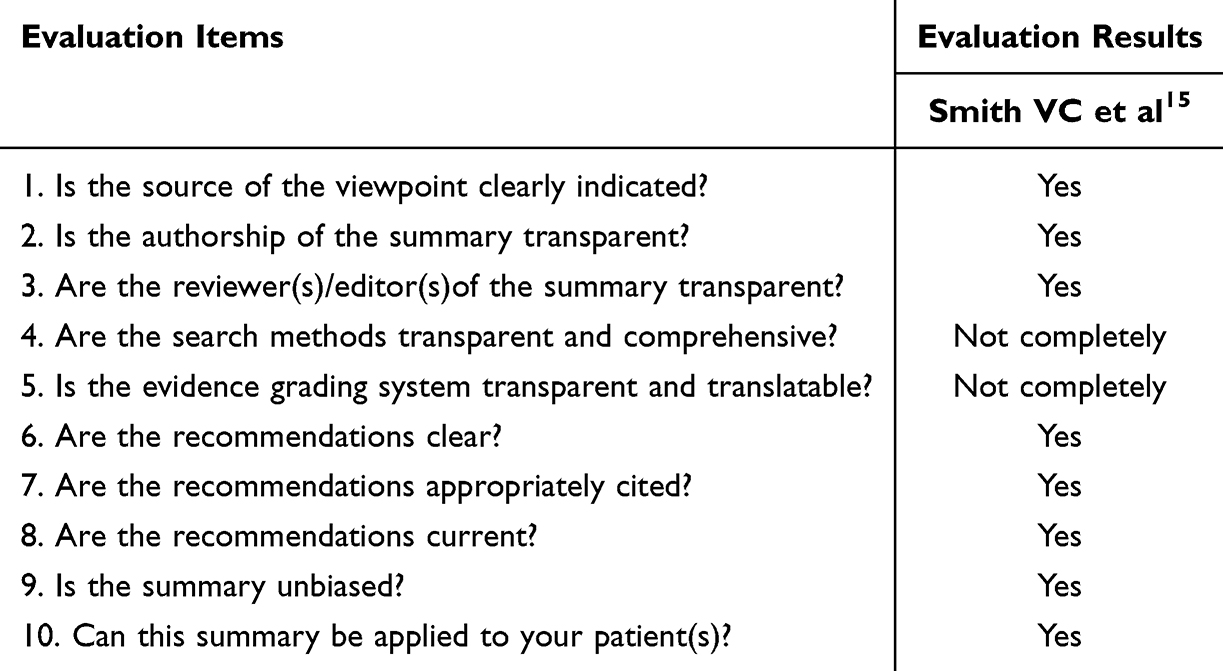 |
Table 2 Quality Evaluation Results of the Clinical Decision (n=1) |
Quality Evaluation Results of the Guideline
This study included one guideline.16 Detailed evaluation results and recommendation levels for various domains of the guideline are shown in Table 3.
 |
Table 3 Quality Evaluation Results of the Guideline (n=1) |
Quality Evaluation Results of the Expert Consensus and Best Practice
One expert consensus17 and one best practice21 were included. The overall quality is high, allowing inclusion. For details, refer to Table 4.
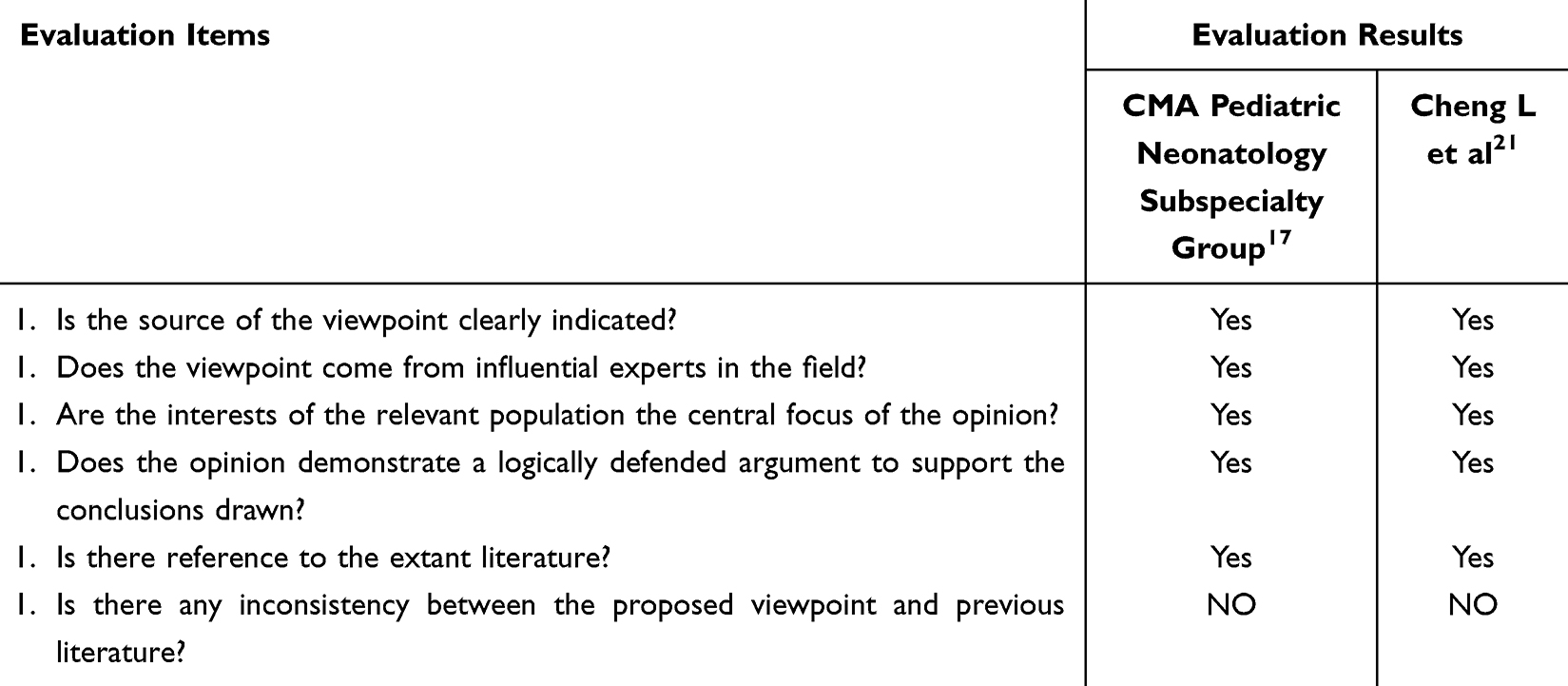 |
Table 4 Quality Evaluation Results of the Expert Consensus and Best Practice (n=2) |
Quality Evaluation Results of the Systematic Reviews and Meta-Analysis
Two systematic reviews18,19 and one meta-analysis20 were included. They demonstrated high quality in multiple aspects and were all included. Details are provided in Table 5.
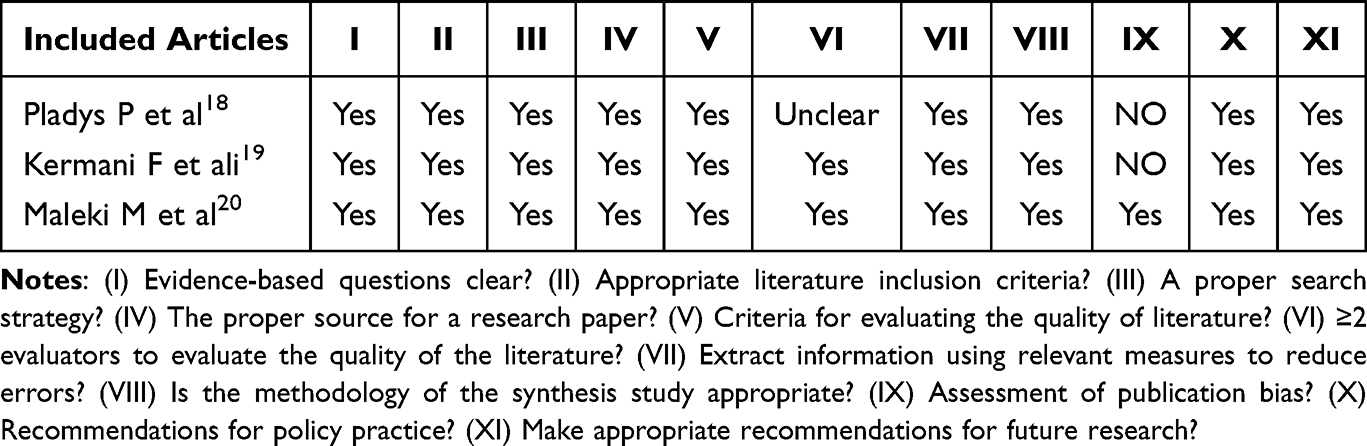 |
Table 5 Quality Evaluation Results of Systematic Reviews and Meta-Analysis (n=3) |
Quality Evaluation Results of the Randomized Controlled Trials
The present study has incorporated three randomized controlled trials,22–24 and the results of their quality assessments are presented in Table 6.
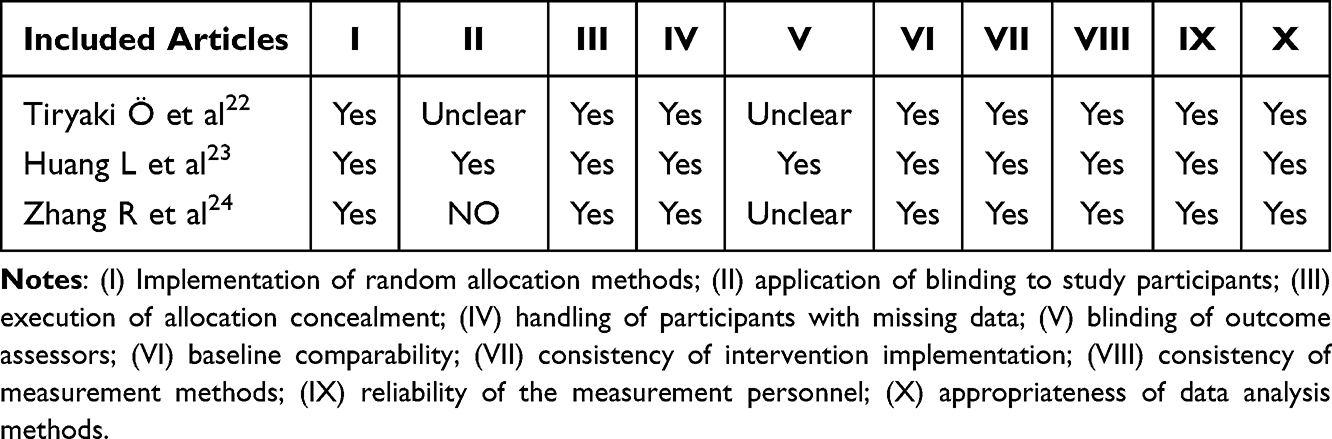 |
Table 6 Quality Evaluation Results of the Randomized Controlled Trials (n=3) |
Summary of Evidence
This study, through a systematic search, screening, and evaluation of relevant literature, has identified 33 key pieces of evidence that collectively shed light on critical aspects of discharge education across five themes: assessment, planning, implementation, evaluation, and support. In the assessment phase, the evidence underscores the importance of promptly identifying and engaging the primary caregiver, as well as assessing the unique needs of diverse families, to tailor education effectively. For the planning phase, forming a multidisciplinary team and developing an individualized education plan are key steps to ensure family caregivers systematically acquire the necessary knowledge and skills. During the implementation phase, the early involvement of family caregivers and the utilization of diverse teaching methods are crucial factors that facilitate their proficiency in performing caregiving tasks. In the evaluation phase, systematic evaluation and feedback mechanisms are essential to ensure the effectiveness of the education provided. Lastly, in terms of support, providing practical educational materials and online platforms reinforces family caregivers’ nursing abilities and boosts their confidence. Tables 7 and 8 detail the primary evidence and their respective sources identified in this study.
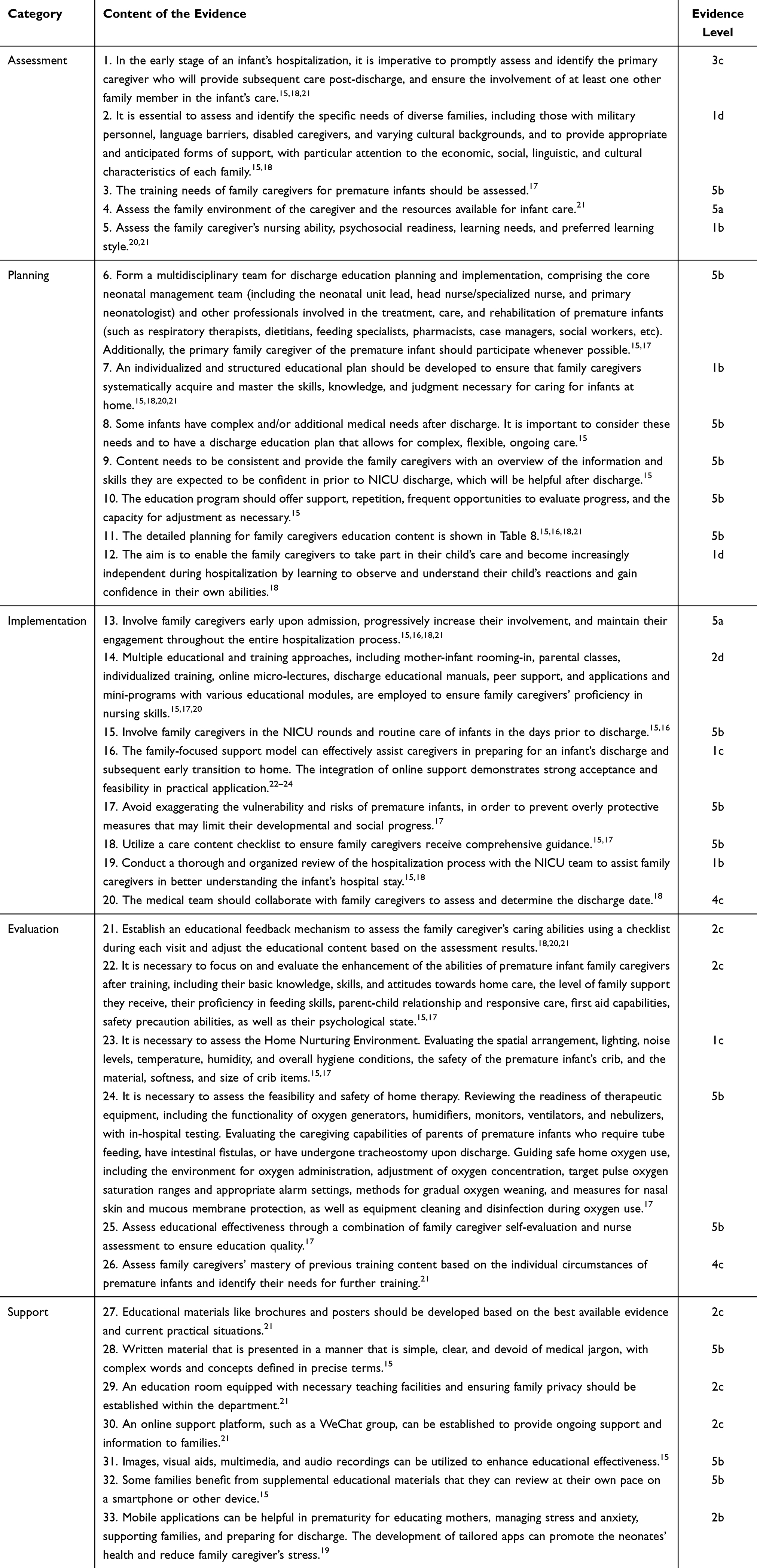 |
Table 7 The Best Evidence Content and Rating for Discharge Education to Enhance Family Preparedness for Premature Infants |
 |
Table 8 The Detailed Planning for Family Caregiver’s Education Content |
Discussion
Discharge preparation services, originating from the continuous care and referral system in the United States, represent a novel care model that has emerged in recent years. They play a crucial role in ensuring patient safety upon discharge and the sustainability of home-based rehabilitation care and have become a focal point of attention among international nursing scholars.27 Discharge education is a key aspect of discharge preparation and sets the stage for a successful transition.28 This study provides a comprehensive summary of the optimal discharge education practices to enhance family preparedness for the care of premature infants. Through a systematic review and analysis of existing research findings, we have distilled key, evidence-based recommendations that encompass assessment, planning, implementation, evaluation, and support.
Assessment for Discharge Education
Evidence 1–5 summarizes the content that should be assessed before conducting education on discharge preparation for family caregivers of premature infants. Evidence 1 suggests that during the initial hospitalization of the infant, it is crucial to promptly assess and identify the primary caregiver who will provide subsequent care after discharge and to actively involve at least one other family member in the infant’s care. This plays a pivotal role in ensuring effective post-discharge care. Evidence 2 emphasizes that recognizing the unique needs of diverse families, such as those with military personnel or language barriers, facilitates the provision of tailored support that accommodates economic, social, linguistic, and cultural differences. This approach acknowledges that effective discharge education must be culturally sensitive and adaptable Evidence 3–5 highlights that assessing the training needs of family caregivers for premature infants is essential to ensure they are adequately prepared to provide appropriate care. This assessment should be comprehensive, encompassing technical skills related to infant care and emotional and psychological support for the caregivers themselves. By understanding the specific challenges each family faces, healthcare providers can better equip family caregivers with the knowledge they need to navigate the complexities of caring for a premature infant.
Planning for Discharge Education
The evidence from 6 to 12 summarizes key recommendations for discharge education plans for family caregivers of premature infants. Evidence 6 emphasizes forming a multidisciplinary team comprising the core neonatal team and other professionals involved in treatment, nursing, and rehabilitation while also striving to involve primary family caregivers whenever possible. Evidence 7 to 10 advocates for a personalized, structured educational plan to ensure family caregivers systematically learn necessary skills. Given that some premature infants have complex or additional medical needs, the educational plan should be flexible to support continuous care. The education content needs to be consistent to avoid confusing family caregivers. It should also provide opportunities for repeated practice, progress assessments, and necessary adjustments. This iterative process reinforces learning and allows for identifying and resolving any gaps or misunderstandings in the caregivers’ knowledge or skills. Evidence 11 details educational content planning to empower family caregivers during hospitalization. Evidence 12 clarifies that the goal is to adequately prepare family caregivers for home care, promoting positive outcomes for infants and families. These recommendations aim to enhance family caregivers’ confidence and abilities, ensuring they are well-prepared to manage their infant’s care at home. By adopting a comprehensive and individualized approach to discharge education, healthcare providers can empower family caregivers to provide the best possible care for their premature infants, ultimately leading to improved health outcomes and a smoother transition from hospital to home.
Implementation of Discharge Education
In the implementation phase of discharge education, Evidence 13–20 collectively suggests operational recommendations. Some parents mentioned that the short notice before discharge resulted in hurried and inadequate preparation for discharge.29 Evidence 13 recommends early engagement of family caregivers upon premature infant admission, with a gradual introduction of educational content to ensure adequate time for acquiring essential knowledge and skills. Evidence 14 proposes adopting diverse teaching methods, encompassing mother-infant rooming-in, parental education classes, individualized training, online micro-lectures, discharge manuals, peer support, and educational apps/mini-programs, to guarantee family caregivers’ proficiency in caregiving tasks. Internationally, bedside teaching is one of the most effective ways of teaching. Bedside teaching involves demonstrating to the family how to perform a task, assessing their understanding, and having them perform the task.30 Evidence 15 suggests involving family caregivers in the infant’s rounds and routine care within healthcare facilities pre-discharge, facilitating a smooth transition to home care. Evidence 16 advocates for a family-centered support model enhanced by online resources, demonstrating adaptability and efficacy. Evidence 17 emphasizes the importance of avoiding exaggerating premature infants’ vulnerability and risks to prevent overly protective measures that could impede their developmental and social milestones. Evidence 18–20 recommends utilizing a care content checklist to ensure comprehensive guidance. Family caregivers engage in collaborative reviews of the infant’s hospital stay and conduct joint assessments with the healthcare team to determine the discharge date, thereby fostering an understanding of the hospitalization process and facilitating informed decision-making regarding discharge.
Evaluation for Discharge Education
The evaluation and feedback of the educational process are vital for ensuring its effectiveness. Evidence 21 suggests that by employing a checklist during each visit, family caregivers’ abilities can be systematically assessed, allowing for tailored adjustments to the educational content. This approach ensures individualized training for family caregivers, enhancing their proficiency in various aspects of premature infant care. Evidence 22–24 recommends a comprehensive evaluation of family caregivers’ skill enhancement, the home nurturing environment, and the feasibility and safety of home-based treatment during discharge education. This ensures a smooth transition for premature infants to the home environment and proper care and treatment. Evidence 25 mentions that integrating family caregivers’ self-assessment with nurse evaluation offers a multi-dimensional perspective on the effectiveness of the education. Evidence 26 further suggests assessing family caregivers’ needs for further training based on previous evaluations. These appraisals enable personalized adjustments to discharge education, confirming caregivers’ discharge readiness and the suitability and safety of the home nurturing environment, thereby providing a solid foundation for the smooth transition of premature infants from hospital to home.
Support for Discharge Education
Practical educational support forms the cornerstone of the overall educational process. Evidence 27–28 suggests that educational materials such as brochures and posters can be developed based on the best available evidence and current practical situations to ensure families receive accurate and practical information. These materials should be presented concisely and clearly, avoiding medical jargon and providing precise definitions for complex terms and concepts. Evidence 29–32 indicates that some families can benefit from supplementary educational materials, allowing them to review on smartphones or other devices at their own pace. Mobile applications can be beneficial in prematurity for educating family caregivers. Establishing online support platforms, such as WeChat groups, can facilitate continuous information dissemination and support to families. Using images, visual aids, multimedia, and audio recordings can significantly enhance the effectiveness of education. Evidence 33 recommends setting up an education room within the department, equipped with necessary teaching facilities, to protect family privacy. The Integrated theory of health behavior change highlights instrumental support as a key facilitator of health behaviors, and these evidence provide valuable guidance for the refinement/development of support tools.31
The evidence presented encompasses 33 key recommendations for optimal discharge education practices to enhance family caregivers’ preparedness to care for premature infants. These recommendations span assessment, planning, implementation, evaluation, and support, underscoring the significance of a holistic and personalized approach. They emphasize the importance of identifying primary caregivers early, assessing their unique needs, and developing tailored, structured educational plans. Implementing these plans through diverse teaching methods is crucial, highlighting the need for a multidisciplinary team approach and early engagement of family caregivers. Furthermore, the evidence stresses the importance of consistent and flexible educational content, regular evaluation and feedback, and effective educational support, including evidence-based materials and online platforms. These elements are essential to ensure high-quality care for premature infants and their families as they transition from hospital to home.
Limitations
This study included ten documents, which may limit the comprehensiveness of the evidence. Therefore, the conclusions drawn should be interpreted cautiously and may require further validation through more extensive and diverse studies.
Conclusion
This study systematically synthesized evidence regarding the effectiveness of discharge education for premature infants’ families. The findings revealed several key insights that form a comprehensive framework for clinical practice. The study highlighted the importance of tailored, individualized discharge education plans that address the unique needs of each family. The early involvement of families, multidisciplinary team collaboration, and the use of diverse teaching methods are crucial for helping families acquire necessary nursing knowledge and skills. Implementing these evidence-based practices is expected to significantly improve families’ discharge readiness, enhance their ability to care for their premature infants, and ultimately promote better infant health outcomes.
Abbreviations
PIPOST, Population, intervention, professional, outcome, setting, type of evidence; RNAO, the Registered Nurses’ Association of Ontario; SIGN, the Scottish Intercollegiate Guidelines Network; GIN, the Global Initiative for Nursing; NICE, National Institute for Health and Care Excellence; JBI, Joanna Briggs Institute; AAP, the American Academy of Pediatrics; CNKI, China National Knowledge Infrastructure; VIP, Vip Information; CASE, the Critical Appraisal for Summaries of Evidence; AGREE II, The Appraisal of Guidelines for Research and Evaluation II.
Acknowledgments
We express our gratitude to the corresponding author and the team members for their diligent efforts. Additionally, we acknowledge the support provided by the Sichuan Provincial College Students’ Innovation and Entrepreneurship Training Program [grant numbers 202310632044, 2023].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Organization WH. Preterm birth[EB/QL]. Available from: https://www.who.int/news-room/fact-sheets/detail/preterm-birth.
2. Collins A, Weitkamp JH, Wynn JL. Why are preterm newborns at increased risk of infection. Arch Dis Child Fetal Neonatal Ed. 2018;103(4):F391–F394. doi:10.1136/archdischild-2017-313595
3. Astuti DD, Rohsiswatmo R, Wanda D, Utari DM. Experiences of Indonesian nurses in improving preterm oral feeding readiness in special care units: a qualitative descriptive study. Belitung Nurs J. 2023;9(5):478–488. doi:10.33546/bnj.2772
4. Li HL, Chen LL, Qian G, et al. A birth cohort study of neurodevelopmental outcomes from birth to 2 years of age in preterm infants under 34 weeks of gestation. J Healthc Eng. 2022;2022:7496785. doi:10.1155/2022/7496785
5. Dai K, Fan X, Shi H, et al. Application of family-centered empowerment model in primary caregivers of premature infants: a quasi-experimental study. Front Pediatr. 2023;11:1137188. doi:10.3389/fped.2023.1137188
6. Zheng QM, Hua WZ, Yan J, Zhou JX, Jiang LP. Analysis of status and influencing factors of parents’ discharge preparation for preterm infants in intensive care unit. Chin J Prac Nurs. 2021;37(25):1979–1984. doi:10.3760/cma.j.cn211501-20210518-01425
7. Meng L, Lingling Z, Haihong Z, Xiaobai Z, Dandan H, Shaoyan W. Readiness for hospital discharge and its correlation with the quality of discharge teaching among the parents of premature infants in NICU. Appl Bionics Biomech. 2022;2022:4924021. doi:10.1155/2022/4924021
8. Hua W, Yuwen W, Simoni JM, Yan J, Jiang L. Parental readiness for hospital discharge as a mediator between quality of discharge teaching and parental self-efficacy in parents of preterm infants. J Clin Nurs. 2020;29(19–20):3754–3763. doi:10.1111/jocn.15405
9. Jefferies AL. Canadian paediatric society FaNC. Going home: facilitating discharge of the preterm infant. Paediatr Child Health. 2014;19(1):31–42. doi:10.1093/pch/19.1.31
10. Fu JX, Zhou YH, Chen MZ. Family readiness for preterm infant discharge: a review. Chin Nurs Manage. 2019;19(7):1074–1078. doi:10.3969/j.issn.1672-1756.2019.07.024
11. Alper BS, Haynes RB. EBHC pyramid 5.0 for accessing preappraised evidence and guidance. Evid Based Med. 2016;21(4):123–125. doi:10.1136/ebmed-2016-110447
12. Foster MJ, Shurtz S. Making the critical appraisal for summaries of evidence (CASE) for evidence-based medicine (EBM): critical appraisal of summaries of evidence. J Med Libr Assoc. 2013;101(3):192–198. doi:10.3163/1536-5050.101.3.008
13. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010;182(18):E839–842. doi:10.1503/cmaj.090449
14. Wang CQ, Hu Y. JBI evidence pregrading and evidence recommendation level system (2014 Edition). J Nurs Contin Educ. 2015;30(11):964–967.
15. Smith VC, Stewart J. Discharge planning for high-risk newborns. UpToDate. 2023;2023:1.
16. Ledinger D, Nußbaumer-Streit B, Gartlehner G. WHO recommendations for care of the preterm or low-birth-weight Infant. Gesundheitswesen. 2024;86(4):289–293. doi:10.1055/a-2251-5686
17. Subspecialty Group of Neonatology, Society of Pediatrics, Chinese Medical Association, Editorial Board of Chinese Journal of Neonatology, Society of Neonatal Nursing of China Medicine Education Association. Management on safe discharge for preterm infants (medical staff version): experts consensus. Chin J Neonatol. 2022;37(5):385–394. doi:10.3760/cma.j.issn.2096-2932.2022.05.001.
18. Pladys P, Zaoui C, Girard L, et al. French neonatal society position paper stresses the importance of an early family-centred approach to discharging preterm infants from hospital. Acta Paediatr. 2020;109(7):1302–1309. doi:10.1111/apa.15110
19. Kermani F, Kahouei M, Valinejadi A, Sadeghi M, Momeni M, Pahlevanynejad S. Outcome’s classification in mobile applications tailored to parents of premature infants: a systematic review. Iran J Public Health. 2023;52(8):1642–1655. doi:10.18502/ijph.v52i8.13402
20. Maleki M, Mardani A, Harding C, Basirinezhad MH, Vaismoradi M. Nurses’ strategies to provide emotional and practical support to the mothers of preterm infants in the neonatal intensive care unit: a systematic review and meta-analysis. Womens Health. 2022;18:17455057221104674. doi:10.1177/17455057221104674
21. Cheng L, Zhang Y, Gu Y, Lu C, Liu Q, Yuan H. Families’ readiness for discharge of their pre-term infant: a best practice implementation project. JBI Database System Rev Implement Rep. 2016;14(9):367–380. doi:10.11124/JBISRIR-2016-003087
22. Tiryaki Ö, Çınar N, Caner İ. The effect of family integrated care on preparing parents with premature infants hospitalized in the neonatal intensive care unit for discharge. J Perinatol. 2024;44(7):1014–1021. doi:10.1038/s41372-024-01931-5
23. Huang L, Zhao BY, Li XT, et al. Effects of an online family-focused parenting support intervention on preterm infants’ physical development and parents’ sense of competence and care ability: a randomized controlled trial. Int J Nurs Stud. 2024;149:104625. doi:10.1016/j.ijnurstu.2023.104625
24. Zhang R, Huang RW, Gao XR, et al. Involvement of parents in the care of preterm infants: a pilot study evaluating a family-centered care intervention in a Chinese neonatal ICU. Pediatr Crit Care Med. 2018;19(8):741–747. doi:10.1097/PCC.0000000000001586
25. Martha A, Klugarova J, Yan H, et al. Chapter 4: Systematic Reviews of Text and Opinion. Australia: JBI; 2019.
26. Hu Y, Hao YF. Evidence-Based Nursing.
27. Yu YT, Xiao F, Chen JR, et al. Research progress in clinical practice of discharge preparation services. Chin J Prac Nurs. 2018;34(2):139–143. doi:10.3760/cma.j.issn.1672-7088.2018.02.014
28. Weiss ME, Sawin KJ, Gralton K, et al. Discharge Teaching, Readiness for Discharge, and Post-discharge Outcomes in Parents of Hospitalized Children. J Pediatr Nurs. 2017;34:58–64. doi:10.1016/j.pedn.2016.12.021
29. Hua W, Wang L, Li C, Simoni JM, Yuwen W, Jiang L. Understanding preparation for preterm infant discharge from parents’ and healthcare providers’ perspectives: challenges and opportunities. J Adv Nurs. 2021;77(3):1379–1390. doi:10.1111/jan.14676
30. Smith H, Harvey C, Portela A. Discharge preparation and readiness after birth: a scoping review of global policies, guidelines and literature. BMC Pregnancy Childbirth. 2022;22(1):281. doi:10.1186/s12884-022-04577-3
31. Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec. 2009;23(3):161–170;quiz171–172. doi:10.1097/NUR.0b013e3181a42373
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.