Back to Journals » Clinical Ophthalmology » Volume 17
Optical-Quality Analysis and Defocus-Curve Simulations of a Novel Hydrophobic Trifocal Intraocular Lens
Authors Łabuz G, Yan W, Khoramnia R ![]() , Auffarth GU
, Auffarth GU ![]()
Received 18 October 2023
Accepted for publication 20 November 2023
Published 18 December 2023 Volume 2023:17 Pages 3915—3923
DOI https://doi.org/10.2147/OPTH.S445461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Grzegorz Łabuz, Weijia Yan, Ramin Khoramnia, Gerd U Auffarth
The David J. Apple Center for Vision Research, Department of Ophthalmology, University Hospital Heidelberg, Heidelberg, 69120, Germany
Correspondence: Grzegorz Łabuz, Universitätsklinikum Heidelberg, Im Neuenheimer Feld 400, Heidelberg, 69120, Germany, Tel +49 6221 56-6613, Fax +49 6221 56-8229, Email [email protected]
Purpose: The optical function of a novel refractive-diffractive trifocal intraocular lens (IOL) was tested in vitro to provide preclinical metrics that predict postoperative performance and may guide patient selection.
Methods: Fundamental optical characteristics of a trifocal hydrophobic-acrylic IOL with a C-loop haptic configuration (AT ELANA 841P, Carl Zeiss Meditec) were assessed using a fully automated optical test device under both monochromatic and polychromatic conditions combined with increased or compensated spherical aberration (SA). The area under the modulation transfer function (MTFa) was calculated across a defocus range from +1D to − 3.5D and used to simulate visual acuity (VA). A polychromatic point spread function (PSF) was employed to assess the light distribution and identify photic phenomena.
Results: The highest MTFa values were obtained under monochromatic conditions using an SA-neutral corneal model. Nevertheless, after introducing SA and polychromatic light, the IOL performance remained good. Simulated VA values were 0.00 logMAR for distance, 0.1 logMAR at 100 cm, and progressively improving to 0.05 logMAR at 40 cm from the intermediate point. The light-spread analysis confirmed halos around the PSF center, which is a characteristic of trifocal technology.
Conclusion: AT ELANA 841P demonstrated good optical performance across various distances, independently of spectral and SA conditions, resulting in good simulated VA. Although light spread resembles standard trifocal IOLs, clinical studies are essential to confirm these laboratory results.
Keywords: intraocular lenses, presbyopia correction, optical quality, modulation transfer function
Introduction
The growing emphasis on an active lifestyle and the widespread use of screen-based devices in daily activities highlights the increasing demand for good vision across various distances, regardless of age. Vision is notably compromised following crystalline lens extraction and the implantation of a monofocal intraocular lens (IOL) due to its inability to change the eye’s focus.1 This deficiency has been addressed by the introduction of IOLs with multifocal optics, first in the form of bifocal IOLs offering reading without glasses in addition to distance vision.2 Later, more complex trifocal designs were introduced, such as FineVision (PhysIOL), AT LISA tri 839 MP (Carl Zeiss Meditec), and PanOptix (Alcon), among others,3–5 to address the challenge of inadequate intermediate vision.2 Furthermore, in an effort to reduce photic phenomena associated with bifocal and trifocal designs, extended-depth-of-focus (EDoF) technology was launched, however, at the expense of near vision.6 Still, a recent meta-analysis found no statistically significant difference between patients receiving multifocal versus EDOF IOLs in terms of halo and glare perception.7
AT ELANA 841P (Carl Zeiss Meditec) is a recently introduced trifocal IOL with a diffractive-refractive design and aberration-neutral optics. It is placed on a hydrophobic acrylic platform, which differs from its predecessor – AT LISA tri, an established hydrophilic-trifocal model. Hydrophobic and hydrophilic acrylate materials have undergone comprehensive validation for their safety in scientific investigations and clinical applications.8–10 Still, the change of material and altered asphericity may weaken optical performance under various conditions; particularly, the impact of chromatic and spherical aberrations needs to be considered. Besides, deciding how to apply this new technology in routine cataract and refractive surgery requires the surgeon to take a personalized approach guided by scientific data. Laboratory evaluation with visual-function simulation provides comprehensive information about distinct characteristics of new lenses, offering guidance for clinicians.
In this comprehensive investigation, the image quality metrics of the AT ELANA 841P were experimentally assessed using two corneal models in monochromatic and polychromatic light. Measurements were made of the modulation transfer function (MTF), recording resolution-test chart photographs, simulating visual acuity (VA) effects, and applying the point spread function (PSF) to characterize the spread of light and thus assess the IOL’s susceptibility to dysphotopsia.
Materials and Methodology
Intraocular Lenses
The AT ELANA 841P (Carl Zeiss Meditec, Berlin, Germany) is presented in Figure 1. According to the manufacturer, it is made of heparin-coated hydrophobic acrylic material that has a refractive index of 1.49 and an Abbe number of 51, also used in a monofocal CT LUCIA 621 model. The lens has a C-loop haptic, a 6.00-mm diameter, aspheric aberration-neutral optics, and a full-diffractive design. This non-apodized trifocal IOL is characterized by add powers of 1.66D and 3.33D to correct postoperative presbyopia. Two samples of the AT ELANA were studied: each lens had a nominal power of +20 D.
 |
Figure 1 AT ELANA 841P single-piece trifocal IOL (Carl Zeiss Meditec) with a C-loop haptic configuration and diffractive-refractive design. |
Metrology Setup
The IOLs’ optical characteristics were evaluated with the OptiSpheric IOL PRO2 (Trioptics GmbH, Wedel, Germany), a high-precision,11 fully automated optical test device capable of assessing IOLs irrespective of optical design. The evaluation adhered to the ISO 11979–2 standard for testing the optical performance of IOLs.12 The IOL PRO2 configuration includes a light source, reticle, collimator, eye model, microscope, and charge-coupled device (CCD) camera. During testing, a collimator illuminated a specific pattern, which was then captured by the IOL being tested and projected onto the CCD camera. This setup enabled the evaluation of the IOL’s optical quality and capabilities to extend the focus range. Three measurement conditions were used: Condition 1 being single-lens cornea with +0.27 µm of SA and polychromatic filter with spectral weighting consistent with the human eye’s spectral sensitivity; the +0.27-µm SA cornea and green monochromatic (546 nm) light were referred to as Condition 2; while Condition 3 was aberration-neutral cornea model (achromatic doublet) and monochromatic light.
Image Quality Metrics
The MTF is a widely accepted standard for testing IOL performance.12,13 A 50 lp/mm frequency was used as a quality criterion to determine the MTF at the far, intermediate, and near focus over a narrow focus range with the labeled power as a starting point. The through-focus (TF) MTF was assessed at 25, 50, and 100 lp/mm with a defocus range of +1.0 D to −3.5 D at the spectacle position (in 0.125D steps). Aperture sizes of 3 to 4.5 mm were used to study the IOLs’ pupil effects. The 1951 USAF resolution test chart was recorded at 3 mm.
The area under the MTF (MTFa) was calculated with VA simulations following the approach described by Alarcon et al.14 However, this model was developed from polychromatic MTFa data; hence, its application to predicting VA from monochromatic light testing needs to be interpreted with caution.
Simulating Photic Phenomena
The light distribution outside the center of the PSF was evaluated for visual effects.15 An image was captured through a 4.5-mm IOL aperture using a back-illuminated 0.1-mm pinhole. Given the differences in image saturation level between monochromatic and polychromatic light, the Condition-1 PSF maximum intensity was aligned with the integrated light intensity recorded under Conditions 2 and 3. The oversaturated condition was chosen to expose the light spread beyond the PSF center, which contains the light of intensity much lower than the PSF core.
Results
Best-Focus MTF Analysis
The average MTF curves of the AT ELANA samples at 3 and 4.5 mm and for the three conditions are compared in Figure 2. Each best-focus position (far, intermediate, and near) is presented and compared separately. In terms of optical quality at the far focus, Condition 1 (polychromatic) yielded lower MTF levels than both monochromatic comparisons. Despite close results, a slight enhancement was observed in the performance under Condition 3 compared to Condition 2. At 4.5 mm, both conditions featuring the aberrated corneal model were affected by the aperture increase. By contrast, Condition 3 demonstrated a high MTF performance. Figure 2 also shows a comparable MTF at intermediate despite the condition change, with only slight changes observed at 4.5 mm. Near-MTF was also close at 3 mm. However, at 4.5 mm, Condition 3 yielded higher optical quality than the other two.
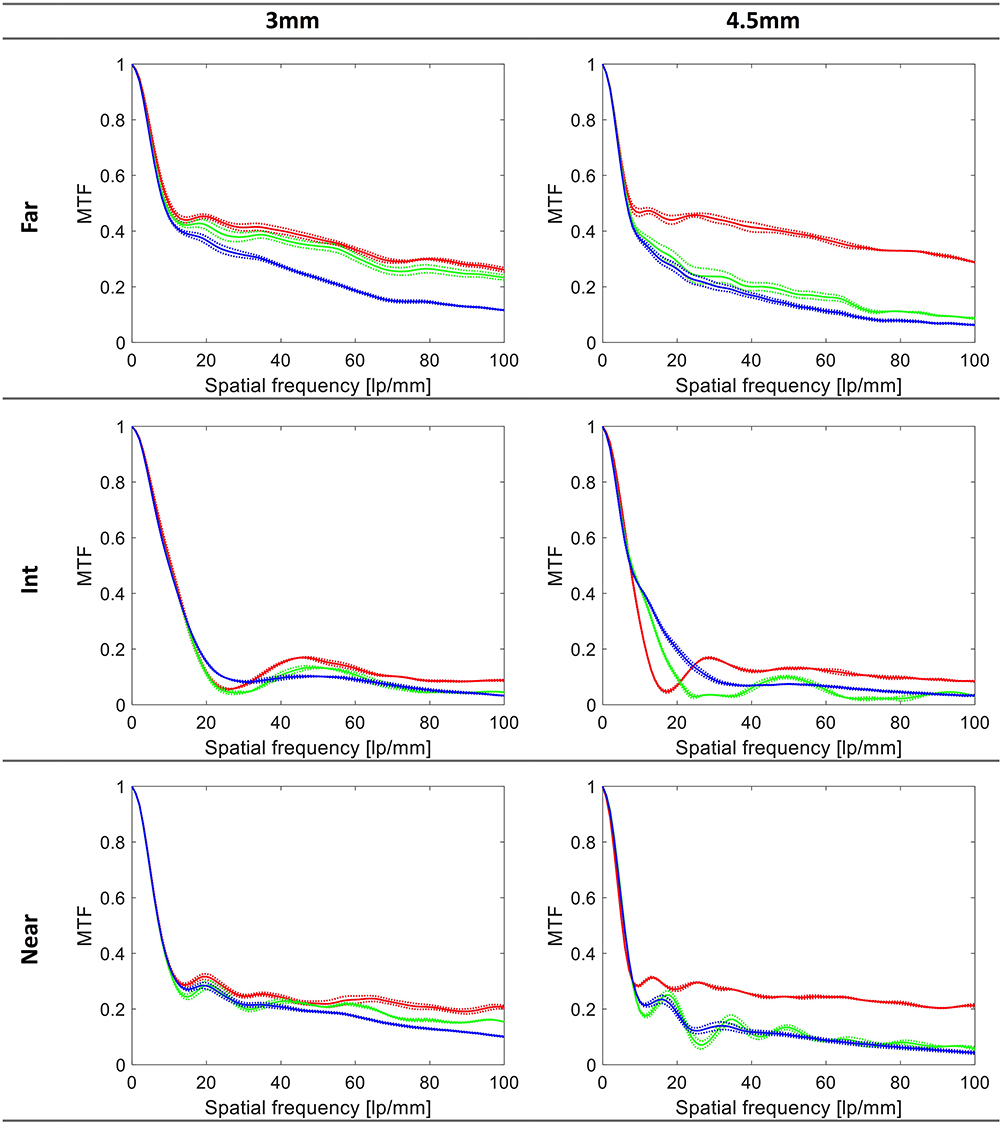 |
Figure 2 MTF levels at the best focus (far, intermediate, and near). The dotted lines show the values of each sample separately; the solid lines refer to their average. Blue lines represent Condition 1 (+0.27-µm SA cornea, polychromatic light), green represents Condition 2 (+0.27-µm SA cornea, monochromatic light), and red represents Condition 3 (SA-neutral cornea, monochromatic light). |
Through-Focus MTFs
The TF MTF of the tested samples measured at 25, 50, and 100 lp/mm and an extended defocus range are reported in Figure 3. The 25 lp/mm far-focus and secondary peak had a similar height among the three conditions. The V-shape of the curves was maintained across all configurations. At 50 lp/mm, the AT ELANA demonstrated its trifocal properties, though no clear separation between the far and intermediate peaks was seen under Condition 1. Minimal discrepancies in the location and height of the near focus were observed across the corneal models and light spectra. The impact of varying conditions on optical quality at 100 lp/mm was particularly seen in Condition 1, where the far-point quality exhibited decreased values. At 4.5 mm, the TF MTFs demonstrated a trifocal pattern for the AT ELANA at all spatial frequencies and configurations. Similar to the best-focus MTF analysis, the highest optical quality was observed in the SA-free model than in Conditions 1 and 2.
 |
Figure 3 Through-focus MTF curves measured at three spatial frequencies. The dotted lines show the values of each sample separately; the solid lines refer to their average. Blue lines represent Condition 1 (+0.27-µm SA cornea, polychromatic light), green represents Condition 2 (+0.27-µm SA cornea, monochromatic light), and red represents Condition 3 (SA-neutral cornea, monochromatic light). |
MTFa and VA Simulations
The left panel of Figure 4 illustrates the alterations in MTFa with defocus. This multi-frequency parameter demonstrated only slight changes between the monochromatic conditions (2 and 3), with the polychromatic one showing only reduced MTFa within ±0.50D. However, the differences between the conditions were unsubstantial for higher defocus, leaving the shape of defocus predominantly unaltered. The right panel of Figure 4 presents defocus curves derived from the MTFa. In Condition 1, the AT ELANA had a simulated VA of 0.20 logMAR or better throughout a range of +0.5 D to −3 D. At 0 D of defocus, the predicted VA was 0.00 logMAR. The AT ELANA’s simulated VA at −1.25 D was 0.1 logMAR with a near VA of 0.05 logMAR at −2.5D. After implementing Conditions 2 and 3, one observed a slight adjustment of VA values at distance, resulting in a mere 0.04 logMAR improvement.
 |
Figure 4 The area under the MTF curve and simulated visual acuity (VA) measured at the defocus range from +1 D to −3.5 D at the spectacle plane. The dotted lines show the values of each sample separately; the solid lines refer to their average. Blue lines represent Condition 1 (+0.27-µm SA cornea, polychromatic light), green represents Condition 2 (+0.27-µm SA cornea, monochromatic light), and red represents Condition 3 (SA-neutral cornea, monochromatic light). |
United States Air Force Test-Target Images
The resolution-test images presented in Figure 5 confirm the MTFa result. The image quality of the AT ELANA provided close performance under different conditions.
 |
Figure 5 USAF target images recorded at a defocus range of +1.0 D to −3.5 D at a 3-mm aperture. Condition 1 = +0.27-µm SA cornea and polychromatic light; Condition 2 = +0.27-µm SA cornea and monochromatic light; Condition 3 = SA-neutral cornea and monochromatic light. |
Simulating Photic Phenomena
The AT ELANA showed a comparable light spread across the three configurations, with multiple halo rings around the PSF center (Figure 6). In Condition 1, however, the PSF center demonstrated more energy spread than a confined central peak seen in Conditions 2 and 3. Besides, in polychromatic light, the shape and intensity of the halo rings were less pronounced than in the two monochromatic conditions.
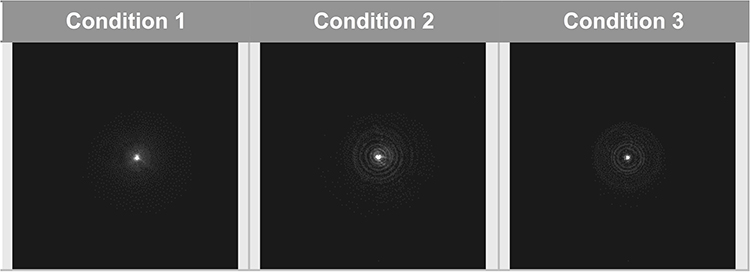 |
Figure 6 The visualization of the low-intensity light distribution produced by a 0.1-mm pinhole was recorded through a 4.5-mm pupil. Condition 1 = +0.27-µm SA cornea and polychromatic light; Condition 2 = +0.27-µm SA cornea and monochromatic light; Condition 3 = SA-neutral cornea and monochromatic light. |
Discussion
This preclinical study demonstrated experimentally that the AT ELANA IOL provides good optical quality across an extended range of distances. While, at the 3-mm aperture, the change in conditions had minimal effect on its performance, the aberration-neutral design adversely affected the simulated scotopic-eye optical quality under increased SA, but chromatic aberration effects were low.
The MTF values of various trifocal IOLs have been examined and reported in previous investigations. Carson et al, employing a 3 mm aperture for the PanOptix lens (Alcon, Fort Worth, TX, USA), provided MTF values at 50 lp/mm as 0.402 for the far, 0.153 for intermediate, and 0.181 for near focal points.16 Correspondingly, the AT LISA tri exhibited values of 0.388, 0.118, and 0.199, while the FineVision (BVI, Liège, Belgium) demonstrated 0.361, 0.096, and 0.165 for the far, intermediate, and near ranges with equivalent pupil size.16 In comparison to our present study, under the same optical configuration, characterized by monochromatic light and a model cornea matched with AT ELANA’s asphericity (Figure 2 - Condition 3), it exhibits close values at the far and near foci (MTF = 0.369 and MTF = 0.214, respectively). While differences can be observed in the intermediate range, as the AT ELANA displayed a lower 50 lp/mm MTF value of 0.136 compared to PanOptix, it was higher, though, than the AT LISA tri and the FineVision.16 Our recent in vitro study comparing three presbyopia-correcting IOLs, ie, AT LISA tri, PanOptix, and Synergy (Johnson & Johnson Vision, Santa Ana, CA, USA), in a polychromatic light setting indicates that the AT LISA tri and the Synergy may provide a slightly higher optical quality due to reduced chromatic aberration.17 A further analysis involving five recently introduced trifocal IOLs provides extensive comparative data obtained under the current investigation’s Conditions 1 and 3. In Condition 1, Synergy’s far MTF at 50 lp/mm was 0.29, 0.28 for the Triumf (BVI, Liège, Belgium), and 0.26 for the AT LISA tri, which are higher than the recorded 0.23 in the AT ELANA. It was, however, better than MTF = 0.20 observed in the PanOptix, and MTF = 0.19 in the Trinova Pro C (VSY, Istanbul, Turkey). In Condition 3, the reported values of all trifocals except one were close to MTF = 0.33 at distance, but for the Synergy it was 0.29 - indicating a 0.07 difference in favor of the AT ELANA. However, more study is needed to directly compare the AT ELANA with other contemporary trifocals, to determine its efficacy and highlight similarities and differences to the competing technologies.
Since the AT ELANA is currently beginning the clinical trial phase, no peer-reviewed publications are available to assess its performance. However, the range of vision provided by the AT ELANA appears comparable to that of the AT LISA tri, which has been extensively studied in clinical research. Furthermore, the existence of similarities between two lenses, sharing close design characteristics but differing in the water content of their material, has also been observed in other IOLs.18 In a recent paper, Torky et al compared the performance of the AT LISA tri against another trifocal and an EDoF model.19 The binocular defocus curve of their AT LISA tri patients showed a logMAR VA of 0.07 at −1D, 0.15 at −2D, and 0.13 at −3D. In another comparative study published in the same year, Zhu et al found 0.09, 0.15, and 0.13 logMAR in their AT LISA tri patients at −1D, −2D, and −3D, respectively.20 Those values are nearly identical to the ones reported by Torky et al,19 showing a good agreement between the VA of the two cohorts. Our simulated polychromatic VA assessment for the AT ELANA yielded logMAR values of 0.09, 0.10, and 0.11 at defocus levels of −1D, −2D, and −3D, respectively. While comparable results to the AT LISA tri were observed for −1D and −3D, a half-a-line improvement in VA was noticeable at −2D. Although a close alignment of the simulated and clinical defocus curves has been demonstrated,14,17,21 the optical bench analysis only approximates the in vivo performance, corresponding to the average eye rather than an individual patient. Therefore, these simulated VA values must be confirmed once clinical trial results become available.
Trifocal IOLs may reduce visual quality due to photic phenomena, eg, glare, halo, and starburst, which impact patients’ postoperative satisfaction.15 The halo effect in trifocal lenses primarily arises from the combined influence of blurred images tied to the intermediate and near add powers.22 Further influencing these halo differences are dissimilarities in lens material, variations in corneal spherical aberration correction, and distinct methods used by each trifocal design to distribute light across the three focal points in response to changes in pupil size.23 Photic phenomena are commonly associated with multifocal optics – as many as 90% of trifocal-IOL patients report these symptoms.24 Most of these patients, however, can generally tolerate the symptoms, which may result from careful patient selection and comprehensive information on the potential for postoperative dysphotopsia after surgery. It is important to note that the mitigation of these effects typically occurs over time, and this is attributed to neuroadaptation.25 A study by Asena revealed minimal disparities between the PanOptix and AT LISA tri IOLs regarding the frequency, intensity, or perceptual disturbance of diverse visual symptoms like halos and glare.26 Similarly, Vargas et al’s investigation revealed no statistically significant differentiation between the AT LISA tri and a bifocal IOL.24 Furthermore, Law et al documented a progressive decline in recognition of halos as time elapsed, decreasing from 80% one month post the AT LISA tri implantation to 40% at the six-month mark.27 This suggests that neuroadaptation considerably influences the perception of photic phenomena. The AT ELANA appears to have a close profile to the AT LISA tri; hence,17 a comparable satisfaction level could be expected. Still, this assumption requires clinical verification, as besides the intensity difference due to the designs of the IOLs, the perception of such effects vary among individuals.28
Conclusion
In conclusion, based on our laboratory simulation, the AT ELANA showed good optical performance, an extended range of focus spanning from far through intermediate to near distances, and robust performance under various spectral and SA conditions. Although more research is needed to characterize the photic-phenomena profile, our laboratory results and design similarities with the AT LISA tri indicate that it may be equivalent to the established trifocal IOLs.
Acknowledgments
We thank Donald J. Munro for his contribution to the review of the manuscript.
Funding
Supported by a research grant from Carl Zeiss Meditec, Berlin, Germany. The David J Apple Laboratory receives support from the Klaus Tschira Foundation, Heidelberg, Germany.
Disclosure
G Auffarth reports grants, lecture fees, and nonfinancial support from Alcon, Hoya, Kowa, and SIFI; grants and lecture fees from Santen and Johnson & Johnson; and grants from Carl Zeiss Meditec, BVI, PhysIOL, and Acufocus outside the submitted work. R Khoramnia reports grants, lecture fees, and nonfinancial support from Carl Zeiss Meditec, Johnson & Johnson Vision Care, Inc., Hoya, Rayner, 1stQ, Teleon, Kowa, and Alcon Laboratories, Inc.; grants and lecture fees from BVI; personal fees, non-financial support from Heidelberg Engineering; and lecture fees from Santen, Acufocus, Ophtec, and Bausch & Lomb outside the submitted work. G Łabuz and W Yan have nothing to disclose.
References
1. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;12(12):CD003169. doi:10.1002/14651858.CD003169.pub4
2. Alio JL, Plaza-Puche AB, Fernandez-Buenaga R, Pikkel J, Maldonado M. Multifocal intraocular lenses: an overview. Surv Ophthalmol. 2017;62(5):611–634. doi:10.1016/j.survophthal.2017.03.005
3. Ang R. Long-term trifocal toric intraocular lens outcomes in Asian eyes after cataract surgery. J Cataract Refract Surg. 2023;49(8):832–839. doi:10.1097/j.jcrs.0000000000001195
4. Lubiński W, Podborączyńska-Jodko K, Kirkiewicz M, Mularczyk M, Post M. Comparison of visual outcomes after implantation of AtLisa tri 839 MP and Symfony intraocular lenses. Int Ophthalmol. 2020;40(10):2553–2562. doi:10.1007/s10792-020-01435-z
5. Niazi S, Gatzioufas Z, Dhubhghaill SN, et al. Association of Patient Satisfaction with Cataract Grading in Five Types of Multifocal IOLs. Adv Ther. 2023. doi:10.1007/s12325-023-02698-5
6. Breyer DRH, Beckers L, Ax T, Kaymak H, Klabe K, Kretz FTA. Aktuelle Übersicht: multifokale Linsen und Extended-Depth-of-Focus-Intraokularlinsen [Current Review: multifocal Intraocular Lenses and Extended Depth of Focus Intraocular Lenses]. KlinMonbl Augenheilkd. 2020;237(8):943–957. doi:10.1055/a-1111-9380
7. Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended Depth of Focus Versus Trifocal for Intraocular Lens Implantation: an Updated Systematic Review and Meta-Analysis. Am J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
8. A RET. Long Term Clinical Outcomes of Hydrophilic and Hydrophobic Versions of a Trifocal IOL with the Same Optical Design. Clin Ophthalmol. 2023;17:623–632. doi:10.2147/OPTH.S403351
9. Borkenstein AF, Borkenstein EM. Clinical Performance of New Enhanced Monofocal Intraocular Lenses: comparison of Hydrophobic C-loop and Hydrophilic Plate-Haptic Platform. Adv Ther. 2023;40(10):4561–4573. doi:10.1007/s12325-023-02635-6
10. Janardhanan R, Garg P, Ranjan Srivastava M, Kumari R. Intra Ocular Lens Technology - A Review of Journey from Its Inception. Ophthalmol Res Int J. 2020;11(3):1–9.
11. Łabuz G, Papadatou E, Khoramnia R, Auffarth GU. Longitudinal Chromatic Aberration and Polychromatic Image Quality Metrics of Intraocular Lenses. J Refract Surg. 2018;34(12):832–838. doi:10.3928/1081597X-20181108-01
12. English D. ISO-11979-2. Ophthalmic implants — intraocular lenses — part 2: optical properties and test methods. Int Organization Standardization. 2014.
13. Bass M, DeCusatis C, Enoch J. Handbook of Optics, Volume II: Design, Fabrication and Testing, Sources and Detectors, Radiometry and Photometry. McGraw-Hill, Inc; 2009.
14. Alarcon A, Canovas C, Rosen R, et al. Preclinical metrics to predict through-focus visual acuity for pseudophakic patients. Biomed Opt Express. 2016;7(5):1877–1888. doi:10.1364/BOE.7.001877
15. Alba-Bueno F, Garzon N, Vega F, Poyales F, Millan MS. Patient-Perceived and Laboratory-Measured Halos Associated with Diffractive Bifocal and Trifocal Intraocular Lenses. Curr Eye Res. 2018;43(1):35–42. doi:10.1080/02713683.2017.1379541
16. Carson D, Xu Z, Alexander E, Choi M, Zhao Z, Hong X. Optical bench performance of 3 trifocal intraocular lenses. J Cataract Refract Surg. 2016;42(9):1361–1367. doi:10.1016/j.jcrs.2016.06.036
17. Yan W, Łabuz G, Khoramnia R, Auffarth GU. Trifocal Intraocular Lens Selection: predicting Visual Function From Optical Quality Measurements. J Refract Surg. 2023;39(2):111–118. doi:10.3928/1081597X-20221207-02
18. Khoramnia R, Kretz F, Gerl M, Breyer D, Auffarth GU. Long-term Clinical Outcomes After Bilateral Implantation of Two Trifocal Diffractive IOLs. J Refract Surg. 2023;39(12):798–807. doi:10.3928/1081597X-20231006-01
19. Torky MA, Nokrashy AE, Metwally H, Abdelhameed AG. Visual performance following implantation of presbyopia correcting intraocular lenses. Eye. 2022;1–9.
20. Zhu M, Fan W, Zhang G. Visual outcomes and subjective experience with three intraocular lenses based presbyopia correcting strategies in cataract patients. Sci Rep. 2022;12(1):19625. doi:10.1038/s41598-022-23694-9
21. Łabuz G, Yan W, Baur ID, Khoramnia R, Auffarth GU. Comparison of Five Presbyopia-Correcting Intraocular Lenses: optical-Bench Assessment with Visual-Quality Simulation. J Clin Med. 2023;12(7):2523. doi:10.3390/jcm12072523
22. Łabuz G, van den Berg TJTP, Auffarth GU, Khoramnia R. Light scattering from a diffractive-refractive intraocular lens: a goniometer-based approach for individual zone assessment. Biomed Opt Express. 2022;13(12):6724–6732. doi:10.1364/BOE.474778
23. Vega F, Alba-Bueno F, Millán MS, Varón C, Gil MA, Buil JA. Halo and Through-Focus Performance of Four Diffractive Multifocal Intraocular Lenses. Invest Ophthalmol Vis Sci. 2015;56(6):3967–3975. doi:10.1167/iovs.15-16600
24. Vargas V, Alio JL, Oliveira RF, Renna A, Yebana P. Long-term objective and subjective outcomes following bilateral implantation of diffractive bifocal or trifocal intraocular lenses. Eur J Ophthalmol. 2021;31(3):1014–1020. doi:10.1177/1120672120926870
25. Piñero DP, Maldonado-López MJ, Molina-Martin A, et al. Randomised placebo-controlled clinical trial evaluating the impact of a new visual rehabilitation program on neuroadaptation in patients implanted with trifocal intraocular lenses. Int Ophthalmol. 2023;43(11):4035–4053. doi:10.1007/s10792-023-02809-9
26. Sezgin Asena B. Visual and refractive outcomes, spectacle Independence, and visual disturbances after cataract or refractive lens exchange surgery: comparison of 2 trifocal intraocular lenses. J Cataract Refract Surg. 2019;45(11):1539–1546. doi:10.1016/j.jcrs.2019.06.005
27. Law EM, Aggarwal RK, Kasaby H. Clinical Outcomes with a New Trifocal Intraocular Lens. Eur J Ophthalmol. 2013;24(4):501–508. doi:10.5301/ejo.5000407
28. Rampat R, Gatinel D. Multifocal and Extended Depth-of-Focus Intraocular Lenses in 2020. Ophthalmology. 2021;128(11):e164–e185. doi:10.1016/j.ophtha.2020.09.026
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.