Back to Journals » Clinical Ophthalmology » Volume 17
Opportunity Cost to Attending Surgeons of Intraoperative Training for Residents in Cataract Surgery
Authors Tsou BC, Smith K, Shah R, Woreta FA ![]() , Vedula SS, Sikder S
, Vedula SS, Sikder S ![]()
Received 2 June 2022
Accepted for publication 1 May 2023
Published 22 May 2023 Volume 2023:17 Pages 1433—1438
DOI https://doi.org/10.2147/OPTH.S374082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Brittany C Tsou,1 Kerry Smith,1 Rahul Shah,1 Fasika A Woreta,1 S Swaroop Vedula,2 Shameema Sikder1
1Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 2Malone Center for Engineering in Healthcare, Whiting School of Engineering, Johns Hopkins University, Baltimore, MD, USA
Correspondence: Shameema Sikder, Wilmer Eye Institute, Johns Hopkins University School of Medicine, 600 N Wolfe St, Baltimore, MD, 21218, USA, Tel +1-240-482-1108, Email [email protected]
Purpose: To estimate the opportunity cost to attending surgeons of teaching residents cataract surgery in the operating room.
Patients and methods: Operating room records at an academic teaching hospital from July 2016 to July 2020 were analyzed in this retrospective review of cases. Cases were identified using Current Procedural Terminology (CPT) codes 66982 and 66984 for cataract surgery. Outcomes measured include operative time and work relative value units (wRVUs). Cost analysis was performed using the generic 2021 Medicare Conversion Factor.
Results: Of 8813 cases, 2906 (33.0%) included resident involvement. For CPT 66982 cases, median (interquartile range (IQR)) operative time was 47 (22) minutes with resident involvement and 28 (18) minutes without (p< 0.001). For CPT 66984 cases, median (IQR) operative time was 34 (15) minutes with resident involvement and 20 (11) minutes without (p< 0.001). Median wRVUs was 78.5 (20.9) with resident involvement and 61.0 (14.4) without (p< 0.001) which converted to an opportunity cost (IQR) per case of $1393.72 ($1055.63). Among cases involving residents, median operative time was significantly higher during the first and second quarters (p< 0.001) and for every quarter when compared to cases performed by attendings only (p< 0.001).
Conclusion: Teaching cataract surgery in the operating room is associated with a considerable opportunity cost for attending surgeons.
Keywords: cataract surgery, resident involvement, opportunity cost, relative value units
Introduction
What does it cost attending surgeons to instruct residents during cataract surgery? Teaching residents in the operating room results in longer procedures. A study in one general surgery residency program found that resident operative times were longer than those of faculty alone for 46 out of 62 types of procedures.1 Other studies report similar findings for procedures in orthopedic surgery and plastic surgery.2,3 In ophthalmology, resident participation is associated with longer procedures in glaucoma, strabismus, and cataract surgery with a range of 3 to 20 additional minutes added per case.4–7 While teaching in the operating room is indispensable, longer procedures not only mean higher cost of care but also an opportunity cost (ie, time that the attending surgeon may have used for alternative activities).
The overall opportunity cost of teaching eye surgery in the operating room has not been quantified. Prior studies on cost of teaching cataract surgery estimated the cost of operating room use. However, estimating cost in terms of work relative value units (wRVUs) captures the time, skill, mental effort and judgment, and stress among attending surgeons.8 Thus, wRVUs represent the opportunity cost for attending surgeons. The wRVUs for each type of procedure performed are determined by the Centers for Medicare and Medicaid Services. Using wRVUs, the opportunity cost of teaching in the operating room was estimated to be $275 for plastic surgery residents and $440 for craniofacial fellows who were involved in cases with the longest operative times, and $159 for hand surgery residents.3,9 Our objective was to estimate the opportunity cost to attending surgeons of teaching residents cataract surgery in the operating room.
Methods
This study abides by the tenants of the Declaration of Helsinki, and ethical approval was obtained from the Johns Hopkins Institutional Review Board.
For this retrospective review of cases, our dataset included cataract surgery procedures performed at an academic teaching hospital between July 2016 and July 2020 with Current Procedural Terminology (CPT) codes 66892 and 66894. CPT code 66982 refers to complex extracapsular cataract removal compared to CPT code 66984. Patients who had cataract surgery combined with another procedure were excluded. Patient information collected included age, sex, race, and ethnicity. Variables collected from the cases included date of procedure, operative time, whether the case was performed by attending with resident or by attending only, and wRVUs. The beginning of the case was recorded at the time of initial incision, and the end of the case was recorded at the time the case was finished. The academic year was divided into four quarters to evaluate operative times throughout the year. Quarters 1–4 were defined as July–September, October–December, January–March, and April–June.
Statistical analysis was performed using Stata version 13 (Statacorp, College Station, TX) and Microsoft Excel (Microsoft Corporation; Redmond, WA) with statistical significance set at p<0.05. Wilcoxon rank sum tests were used to compare medians between groups. Cost analysis was performed following prior methodology3 and using the generic 2021 Medicare Conversion Factor ($34.89/RVU) to convert RVU’s lost to opportunity cost.
Results
A total of 8808 patients were identified of which 3594 (40.8%) were male and 5208 (59.1%) were White or Caucasian (Table 1). The average age (±standard deviation) was 68.9 (±11.3) years.
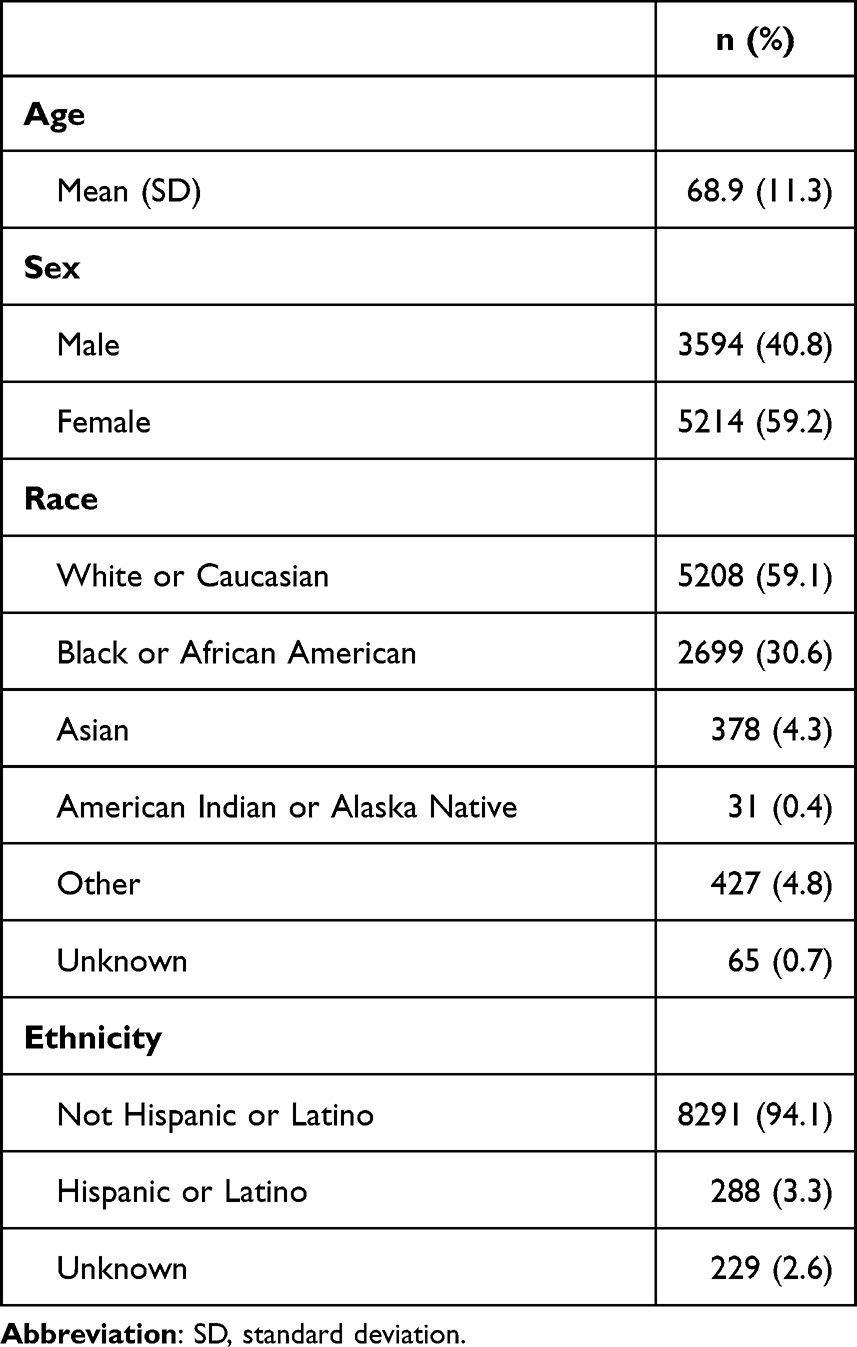 |
Table 1 Characteristics of Patients Who Underwent Cataract Surgery |
Of 8808 cataract surgery procedures, 2426 (27.5%) were logged as CPT 66892 and 6382 (72.5%) were logged as CPT 66894 (Table 2). Overall, 2906 (33.0%) cases included a resident surgeon.
 |
Table 2 Characteristics of Cataract Surgery Procedures Stratified by Resident Involvement |
For cases logged as CPT 66982, the median (interquartile range) operative time was 47 (22) minutes with resident involvement and 28 (18) minutes without (p<0.001) (Table 3). For cases logged as CPT 66984, the median (interquartile range) operative time was 34 (15) minutes with resident involvement and 20 (11) minutes without (p<0.001).
 |
Table 3 Median Operative Time of Cataract Surgery Procedures Stratified by Resident Involvement |
In every quarter, the median operative time was significantly higher for cases with resident surgeon involvement compared to those with attending alone (p<0.001). For cases logged as CPT 66982: In quarter 1, the median (interquartile range) operative time was 53 (23) minutes with resident involvement and 28 (16) minutes without (p<0.001). In quarter 2, the median (interquartile range) operative time was 47 (22) minutes with resident involvement and 27 (18) minutes without (p<0.001). In quarter 3, the median (interquartile range) operative time was 44 (21) minutes with resident involvement and 29 (21) minutes without (p<0.001). In quarter 4, the median (interquartile range) operative time was 42 (21) minutes with resident involvement and 27 (18) minutes without (p<0.001). For cases logged as CPT 66984: In quarter 1, the median (interquartile range) operative time was 36 (17) minutes with resident involvement and 20 (13) minutes without (p<0.001). In quarter 2, the median (interquartile range) operative time was 37 (14) minutes with resident involvement and 19 (11) minutes without (p<0.001). In quarter 3, the median (interquartile range) operative time was 34 (14) minutes with resident involvement and 21 (10) minutes without (p<0.001). In quarter 4, the median (interquartile range) operative time was 32 (12) minutes with resident involvement and 20 (11) minutes without (p<0.001). Among cases involving residents, the median operative time was significantly higher during the first and second quarters (p<0.001). There was no significant difference in average operative times for attending cases over the year.
Overall, the median (interquartile range) wRVU’s was 78.5 (20.9) with resident involvement and 61.0 (14.4) without (p<0.001) which converted to an opportunity cost (interquartile range) per case of $1393.72 ($1055.63).
Discussion
In our study, cataract surgery cases with resident involvement had longer median operative times and higher median wRVU’s compared to cases performed by attendings alone. In addition, the median operative time was significantly higher for cases involving residents during the first and second quarters. Overall, the opportunity cost (interquartile range) to attendings was $1393.72 ($1055.63) per case.
In terms of operative times, our findings are similar to those of prior studies. Cases involving residents in our cohort had an overall median operative time of 39 minutes, comparable to the range of 42 to 49 minutes in a study at University of Washington10 and 46 minutes in a case series at the University of Colorado.6 Attending cases had an overall median operative time of 21 minutes which was slightly lower than 26 minutes from the University of Colorado case series6 and range of 27 to 32 minutes in the University of Washington study.10
However, the opportunity cost estimated using wRVU’s in our study was much higher than estimates from other studies. For instance, using an institution-specific non-supply cost of running the operating room of $8.30 per operating minute, another study found that resident participation at Penn State Hershey Eye Center added $105.40 to an average cataract surgery procedure.7 When applying the same non-supply cost of $8.30 per operating minute to our study instead of using wRVU’s, resident involvement would add $149.40 to an average cataract surgery procedure. This discrepancy is likely due to the different methodology used to estimate wRVUs. Some payors such as Medicare use a physician fee schedule to compensate physicians, and each fee depends on wRVU’s which account for the time, technical skill and effort, mental effort and judgment, and stress to provide a service. Thus, wRVU’s can more accurately reflect the opportunity cost to attending physicians although they do not necessarily increase in the same proportion as the amount of time spent on a patient.8
While the median operative time was significantly higher throughout the year for cases with resident involvement compared to those performed by attendings alone, cases involving residents had significantly longer median operative times during the first and second quarters compared to the third and fourth quarters. In fact, there was a trend of decreasing median operative times for cases involving residents throughout the academic year, whereas no such trend was observed for cases performed by attendings only, suggesting that the increased operative times in the first half of the academic year are likely due to inexperience of new residents. Similar findings were found in the study at Penn State Hershey Eye Center for monthly mean operative case duration.7 As residents gain more experience over time and enhance their surgical skills, they may operate more quickly, which can account for the decrease in mean operative times during the third and fourth quarters. In fact, prior studies have shown that median operative time significantly decreases between the 45th and 86th case11 and when comparing the first fifty surgeries with subsequent cases.12 However, another study suggests diminishing returns with no statistically significant decrease in operative time beyond 150th case.13
Given the high opportunity cost of teaching cataract surgery in the operating room, it is necessary to develop other ways that residents can gain practice with the procedure outside of the operating room. For instance, virtual reality simulation training has been shown to decrease operative times in learners. Third-year residents learning phacoemulsification who underwent mandatory virtual cataract surgery simulator surgical training in their second year of residency before starting intraocular surgeries had significantly decreased operative times compared to non-simulator trained peers.14 In addition, virtual reality simulation training has been shown to decrease the errors that learners make while performing cataract surgery. Residents who were trained to perform scleral tunnel construction using a simulation-based curriculum performed fewer errors in their first twenty attempts at tunnel construction compared to those trained with a conventional institution-specific curriculum.15 Prior research shows resident surgeons take longer to learn and perform a subset of steps in cataract surgery.16 Targeted training to competence with different steps in the procedure, either through simulation or feedback could lead to development of novel and optimized training curricula.
In addition, other ways to compensate and motivate educators are needed. The development of an academic RVU system has previously been described in radiology to assess productivity in various academic activities including teaching.17 When educational value units were integrated with incentives in an academic emergency medicine department, there were significant increases in faculty educational contributions.18 The educational value unit has also been used as a metric to distribute university funds to support faculty efforts in education.19 In a busy academic environment where faculty have clinical and research responsibilities in addition to teaching responsibilities, it is important to continue promoting education. In fact, there are other aspects of opportunity cost for the attending surgeon, including time that could have been used to conduct research and emotional trauma from dealing with possible resident complications.
Finally, there were fewer cases in 2020 due to the impact of COVID-19 on surgical volume. Within ophthalmology, an international survey found that the vast majority of residents reported a >75% decrease of surgical activity during the pandemic.20 Decreased surgical volume has also been reported in numerous other surgical sub-specialties due to COVID-19.21
Our dataset was retrospectively captured, which may have introduced coding or data entry errors. We did not analyze the level of training of the resident surgeon and the extent of their involvement in each procedure, ie, what steps the resident surgeon performed. The analysis did not consider other opportunity costs, such as managing complications of residents’ surgeries. Our study was limited to data at a single eye institution, which may limit generalizability. There were fewer cases in 2020 due to the impact of COVID-19 on surgical volume. Both attending cases with and without resident involved decreased that year, limiting the number of cases for our analysis.
Conclusion
Teaching cataract surgery in the operating room is associated with a considerable opportunity cost for attending surgeons. Our findings emphasize the need for novel approaches to resident training to optimize costs and provide a metric to evaluate their effectiveness. Future studies may also estimate the opportunity cost to attending surgeons of teaching residents other types of ophthalmic surgery in the operating room.
Acknowledgments
We would like to acknowledge Jing Tian from the Wilmer Biostatistics Core for her assistance with statistical analyses.
Funding
This study was supported by grant P30EY01765 (Wilmer Biostatistics Core Grant) from the National Eye Institute, Bethesda, Maryland. Drs. Sikder and Vedula are supported by the National Eye Institute of the National Institutes of Health under award number 1R01EY033065. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bridges M, Diamond DL. The financial impact of teaching surgical residents in the operating room. Am J Surg. 1999;177:28–32. doi:10.1016/S0002-9610(98)00289-X
2. Farnworth LR, Lemay DE, Wooldridge T, et al. A comparison of operative times in arthroscopic ACL reconstruction between orthopaedic faculty and residents: the financial impact of orthopaedic surgical training in the operating room. Iowa Orthop J. 2001;21:31–35.
3. Sasor SE, Flores RL, Wooden WA, Tholpady S. The cost of intraoperative plastic surgery education. J Surg Educ. 2013;70:655–659. doi:10.1016/j.jsurg.2013.04.008
4. Thangamathesvaran L, Crane E, Modi K, Khouri AS. Outcomes of resident-versus attending-performed tube shunt surgeries in a United States residency program. J Curr Glaucoma Pract. 2018;12:53–58. doi:10.5005/jp-journals-10028-1245
5. Winter TW, Olson RJ, Larson SA, Oetting TA, Longmuir SQ. Resident and fellow participation in strabismus surgery: effect of level of training and number of assistants on operative time and cost. Ophthalmology. 2014;121:797–801. doi:10.1016/j.ophtha.2013.10.004
6. Taravella MJ, Davidson R, Erlanger M, Guiton G, Gregory D. Time and cost of teaching cataract surgery. J Cataract Refract Surg. 2014;40:212–216. doi:10.1016/j.jcrs.2013.07.045
7. Hosler MR, Scott IU, Kunselman AR, Wolford KR, Oltra EZ, Murray WB. Impact of resident participation in cataract surgery on operative time and cost. Ophthalmology. 2012;119:95–98. doi:10.1016/j.ophtha.2011.06.026
8. Satiani B. Use, misuse, and underuse of work relative value units in a vascular surgery practice. J Vasc Surg. 2012;56:267–272. doi:10.1016/j.jvs.2012.03.013
9. Zhu WY, Beletsky A, Kordahi A, et al. The cost to attending surgeons of resident involvement in academic hand surgery. Ann Plast Surg. 2019;82:S285–S288. doi:10.1097/SAP.0000000000001873
10. Gupta D, Taravati P. Effect of surgical case order on cataract surgery complication rates and procedure time. J Cataract Refract Surg. 2015;41:594–597. doi:10.1016/j.jcrs.2014.06.032
11. Wiggins MN, Warner DB. Resident physician operative times during cataract surgery. Ophthalmic Surg Lasers Imaging. 2010;41:518–522. doi:10.3928/15428877-20100726-07
12. Umali MIN, Castillo TR. Operative time and complication rates of resident phacoemulsification surgeries in a national university hospital: a five-year review. Clin Ophthalmol. 2020;14:4065–4072. doi:10.2147/OPTH.S283754
13. Liebman DL, McKay KM, Haviland MJ, Moustafa GA, Borkar DS, Kloek CE. Quantifying the educational benefit of additional cataract surgery cases in ophthalmology residency. J Cataract Refract Surg. 2020;46:1495–1500. doi:10.1097/j.jcrs.0000000000000298
14. Lopez-Beauchamp C, Singh GA, Shin SY, Magone MT. Surgical simulator training reduces operative times in resident surgeons learning phacoemulsification cataract surgery. Am J Ophthalmol Case Rep. 2020;17:100576. doi:10.1016/j.ajoc.2019.100576
15. Nair AG, Ahiwalay C, Bacchav AE, et al. Effectiveness of simulation-based training for manual small incision cataract surgery among novice surgeons: a randomized controlled trial. Sci Rep. 2021;11:10945. doi:10.1038/s41598-021-90410-4
16. Rali A, Grosel T, Fontus J, et al. Assessing the phacoemulsification learning curve using duration of each step. J Cataract Refract Surg. 2022;48:44–50. doi:10.1097/j.jcrs.0000000000000703
17. Mezrich R, Nagy PG. The academic RVU: a system for measuring academic productivity. J Am Coll Radiol. 2007;4:471–478. doi:10.1016/j.jacr.2007.02.009
18. House J, Santen SA, Carney M, Nypaver M, Fischer JP, Hopson LR. Implementation of an Education Value Unit (EVU) system to recognize faculty contributions. West J Emerg Med. 2015;16:952–956. doi:10.5811/westjem.2015.8.26136
19. Stites S, Vansaghi L, Pingleton S, Cox G, Paolo A. Aligning compensation with education: design and implementation of the Educational Value Unit (EVU) system in an academic internal medicine department. Acad Med. 2005;80:1100–1106. doi:10.1097/00001888-200512000-00006
20. Ferrara M, Romano V, Steel DH, et al. Reshaping ophthalmology training after COVID-19 pandemic. Eye (Lond). 2020;34:2089–2097. doi:10.1038/s41433-020-1061-3
21. Wise CE, Bereknyei Merrell S, Sasnal M, et al. COVID-19 impact on surgical resident education and coping. J Surg Res. 2021;264:534–543. doi:10.1016/j.jss.2021.01.017
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.