Back to Journals » Clinical Ophthalmology » Volume 20
Opportunistic Glaucoma Detection in a Diabetic Eye Screening Program: Yield and Feasibility in a Caribbean Population
Authors Affoo AS, Mohammed Z, Sookhoo J, Lazarus LA, Bhola R
Received 14 March 2026
Accepted for publication 21 May 2026
Published 3 June 2026 Volume 2026:20 600638
DOI https://doi.org/10.2147/OPTH.S600638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Abigail Sara Affoo, Zahrid Mohammed, Jeanmarc Sookhoo, Lee Ann Lazarus, Ronnie Bhola
Department of Ophthalmology, Trinidad Eye Hospital, Tunapuna, Trinidad and Tobago
Correspondence: Abigail Sara Affoo, Email [email protected]
Purpose: Glaucoma is a leading cause of irreversible blindness worldwide and is highly prevalent in the Caribbean nations. It can remain asymptomatic until the late stages, underpinning the need for screening for early diagnosis. This study aimed to determine whether glaucoma screening should be performed in combination with population-based diabetic retinopathy screening in Trinidad and Tobago.
Methods: Diabetic retinopathy screening, including colour fundus photography, was conducted in communities across Trinidad and Tobago. Patients whose fundus photographs met the glaucoma suspect criteria (vertical cup-to-disc ratio (VCDR) ≥ 0.6, VCDR difference ≥ 0.2 between the eyes, disc haemorrhage, or suspected RNFL defect) were referred to the clinic for full evaluation and diagnosis.
Results: A total of 1754 adults with diabetes were screened, with 167 patients (9.5%) meeting the glaucoma suspect criteria. 45 patients (26.9% of those meeting the glaucoma suspect criteria) presented to the clinic and underwent a full evaluation. The extrapolated estimated prevalence of glaucoma in the diabetic population was 5.9% (minimum confirmed prevalence 1.6%) and the extrapolated estimated prevalence of undetected glaucoma 2.1%. The positive predictive value of fundus photography for detecting glaucoma was 62.2%.
Conclusion: Opportunistic glaucoma screening using fundus photography within an existing diabetic eye screening programme identified a clinically meaningful number of glaucoma cases in this Caribbean diabetic population.
Keywords: glaucoma screening, diabetic retinopathy screening, fundus photography, glaucoma prevalence, Caribbean population
Introduction
Glaucoma is an acquired, progressive optic neuropathy characterised by degeneration of retinal ganglion cells that results in visual compromise and eventual blindness.1 More than 60 million people have glaucoma worldwide with a projected increase to 111.8 million people by 2040.2 Glaucoma is therefore one of the leading causes of irreversible blindness worldwide with an estimated worldwide prevalence of 3.54% with even higher rates reported in the Caribbean population.3–5 Glaucoma is often undiagnosed in the early stages because of the lack of overt symptoms, with diagnosis often following severe vision loss. The National Eye Survey of Trinidad and Tobago attributed 31.7% of blindness to glaucoma.6
Targeted screening programmes for glaucoma have the potential to improve early detection and intervention to reduce the burden of visual impairment. However, the feasibility of population-based glaucoma screening programmes are underexplored in the Caribbean. Guidelines for glaucoma screening vary globally. The U.S. Preventive Services Task Force and UK National Screening Committee do not recommend universal population screening, whereas the American Academy of Ophthalmology supports screening from age 40 and ICO’s Sub-Saharan African Guidelines recommend screening adults over 35.7
Risk factors for primary open-angle glaucoma (POAG) include elevated intraocular pressure (IOP), older age, family history, African ancestry, and type 2 diabetes.8 Effective treatment such as laser therapy, medication and surgery has been found to reduce intraocular pressure, visual field loss and optic nerve changes, thereby reducing disease progression.9,10
The diagnosis of glaucoma involves a combination of tests that reveal degenerative changes in the optic disc and visual field defects with or without elevated IOP. Fundus photography can be used to assess an increased vertical cup-to-disc ratio (VCDR), VCDR asymmetry between eyes, disc haemorrhage, or suspected retinal nerve fibre layer defects. These features are associated with glaucoma and allow fundus photography to serve as a potential inexpensive screening tool. Fundus photographs are already being assessed in diabetic retinopathy screening conducted in Trinidad and Tobago, facilitating an opportunity to screen for glaucoma concomitantly. This study evaluated the yield of incorporating glaucoma detection into diabetic retinopathy screening using fundus photography in Trinidad and Tobago.
Methods
This study analysed data collected from the Trinidad Eye Hospital (TEH) diabetic eye screening programme between January and December 2023.
The study participants consisted of individuals who attended free diabetic eye screening provided by the TEH at 31 locations throughout Trinidad and Tobago, including public libraries and community centres. Free eye screening was advertised using Trinidad Eye Hospital’s website, Facebook, and Instagram pages, as well as reports by local news media. The participants were required to book appointments for their desired screening dates and locations. All individuals included in the study were known to have type II diabetes mellitus and were at least 18 years old. The study was open to including non-institutionalised subjects of both sexes and subjects of all socioeconomic and ethnic backgrounds who were in Trinidad and Tobago at the time of screening. Participants who attended the screening but were unable to obtain satisfactory fundus photographs were excluded from the study.
As part of the Diabetic Eye Screening programme, participants’ age, sex, ethnicity, and location were recorded during screening. The participants underwent standard colour fundus photography using a digital non-mydriatic retinal camera (Canon CR-2 AF and Crystalvue NF-700). The photographs were assessed by a grading team composed of trained technicians (recipients of a Certificate of Higher Education in Diabetic Retinopathy Screening from the University of Gloucestershire) to identify glaucoma suspect criteria. The glaucoma suspect criteria comprised of a vertical cup-to-disc ratio ≥ 0.6, VCDR difference ≥ 0.2 between the eyes, disc haemorrhage, or suspected RNFL defect. These features are consistent with recognised structural features of glaucomatous optic neuropathy.11 Individuals who met the glaucoma suspect criteria were referred to an ophthalmology clinic at TEH for full assessment. Clinical assessment included a complete ophthalmic history, visual acuity assessment, tonometry, dilated slit lamp biomicroscope examination of the optic disc, Humphrey visual field 30–2 testing, pachymetry, ocular imaging using optical coherence tomography (OCT) of the optic nerve head/ganglion cell complex and anterior chamber angle (logMAR charts, Tonopen as well as Goldmann applanation tonometry and Topcon OCT). The diagnosis of glaucoma was determined by a consultant or resident ophthalmologist when one of the following criteria was met: visual field defect compatible with glaucoma, glaucomatous structural damage of the optic nerve head and/or retinal nerve fibre layer. Following the diagnosis of glaucoma, patients received treatment as necessary.
Data from the Diabetic Eye Screening programme were then analysed to calculate the prevalence of glaucoma among adults with diabetes who participated in the study. The positive predictive value was calculated by dividing the number of true positive cases by the sum of the true positive and false positive cases.
The tenets of the Declaration of Helsinki were adhered to. This study utilized anonymized data collected as part of a routine diabetic eye screening programme. Ethical approval was obtained from the Research Ethics Committee of the Ministry of Health, Trinidad and Tobago (Reference: He: 3/13/441 Vol. II dated 18 September 2025). All patients attending the screening service were informed that their anonymized clinical information might be used for research and quality improvement purposes. Patients were given the opportunity to decline participation through an opt-out option on the intake documentation. Participation in the screening process after receiving this information constituted implied informed consent for the use of anonymized data. No personally identifiable information was included in the dataset used for analysis.
Results
A total of 1754 individuals participated in the TEH diabetic screening programme between January and December 2023. Figure 1 depicts the geographical areas represented in the sample population. A total of 167 individuals (9.5% of patients screened) met the glaucoma suspect criteria and were referred to the clinic. Of the patients meeting the suspect criteria, 45 (26.9%) presented to the clinic for full evaluation, 39 (23.4%) presented to the clinic but did not complete the full evaluation, and 83 (49.7%) did not present to the clinic. Table 1 shows the age and ethnicity of the 167 patients who met the glaucoma suspect criteria and those with glaucoma. Table 2 shows the demographic characteristics of those meeting the glaucoma suspect criteria stratified by clinic attendance status. There was no significant difference between the group that met the glaucoma suspect criteria but did not attend clinic, the group that attended clinic but did not complete the full evaluation and the group that received the full evaluation in terms of age, sex or ethnic composition. 14 patients with glaucoma (50%) were of Indo-Caribbean ethnicity and 13 patients with glaucoma (46%) were of Afro-Caribbean ethnicity. Table 3 shows the classification of participants with confirmed glaucoma or a glaucoma-related diagnosis.
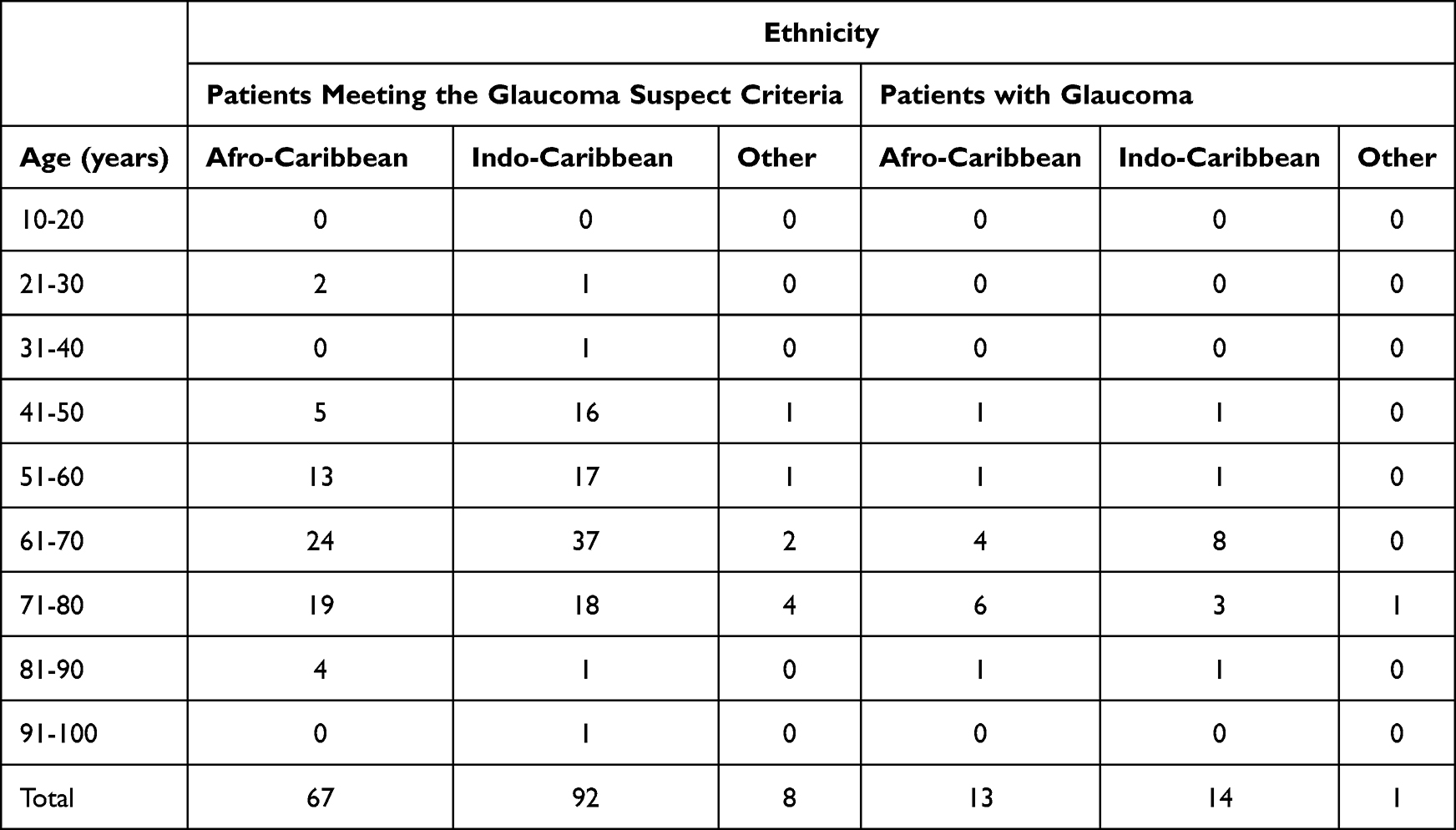 |
Table 1 Age and Ethnicity of the Patients Meeting the Glaucoma Suspect Criteria and Patients with Glaucoma |
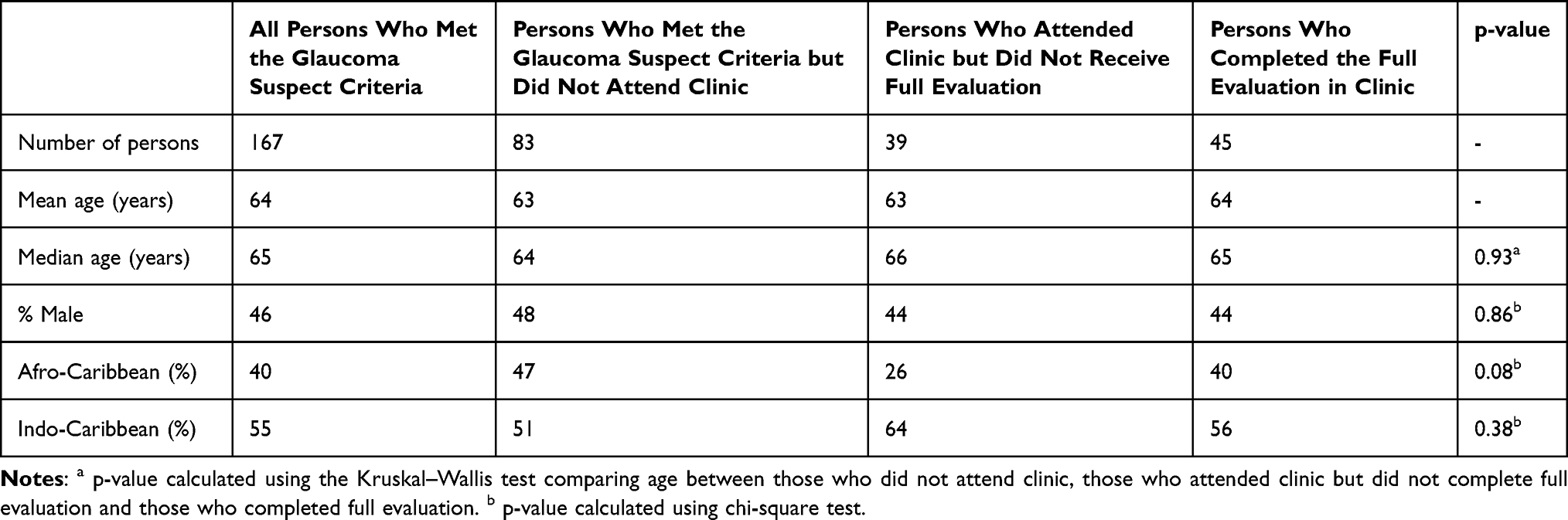 |
Table 2 Demographic Characteristics of Persons Meeting the Glaucoma Suspect Criteria |
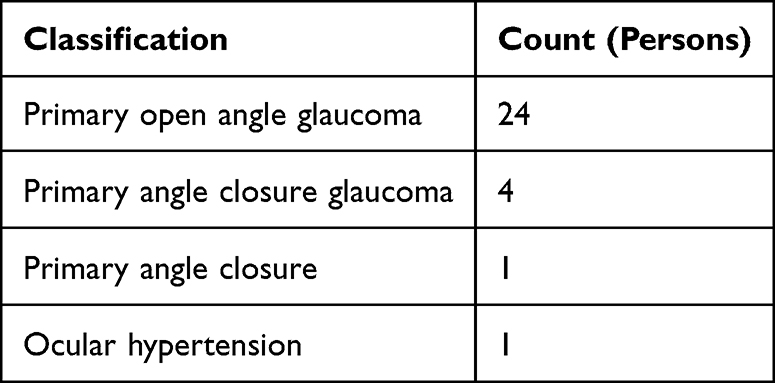 |
Table 3 Classification of Participants with Confirmed Glaucoma or Glaucoma-Related Diagnosis |
 |
Figure 1 Picture showing the geographical areas represented in the sample population. |
28 of the 45 patients who received full evaluation had glaucoma, representing true-positive cases. The 17 patients who screened positive by meeting the suspect criteria but who were not found to have glaucoma on full evaluation represented false-positive cases. Therefore, the positive predictive value of fundus photography for detecting glaucoma in this study was 62.2%.
As 62.2% of those receiving full evaluation had glaucoma and 9.5% of the screened patients met the suspect criteria, the extrapolated estimated prevalence of glaucoma in the entire diabetic population was calculated to be 5.9%. Additionally, the minimum confirmed prevalence of glaucoma in the screened diabetic population is 1.6%.
Of the 28 patients with glaucoma, 10 (36%) were newly diagnosed and started initial treatment, while 18 (64%) were already receiving treatment. These 10 newly diagnosed patients represented an extrapolated estimated prevalence of undetected glaucoma of 2.1% and a minimum confirmed prevalence of 0.6%.
19 patients (68%) with glaucoma had no family history of glaucoma.
Of the 167 patients who met the glaucoma suspect criteria, 11 (6.6%) also had diabetic retinopathy changes on fundus photography, and 21 (12.6%) screened positive for cataract.
Discussion
By utilising a diabetic retinopathy screening programme, we were able to gain new insights into the potential of fundus photography for glaucoma screening.
The extrapolated estimated prevalence of glaucoma in the diabetic population of Trinidad and Tobago was 5.9% which is nearly twice the global prevalence of 3.54% in the 40–80 years age group reported by Tham et al.2 It is, however, consistent with the findings of other Caribbean nations, as studies have reported the prevalence of open-angle glaucoma among the Afro-Caribbean population to be 8.8% in St. Lucia and 7% in Barbados.3–5 This is significant because it emphasises a greater burden of disease in the Caribbean population. Screening among this population is therefore more likely to yield benefits as a significant percentage of the population is affected by glaucoma in comparison to countries with a large Caucasian ethnic makeup, such as the United States where prevalence is estimated at 2.56% in those 40 years and older.12
Trinidad and Tobago has a multiethnic population and a diabetes prevalence of approximately 12.4%. In our study, there was near equivalence between Indo-Caribbean and Afro-Caribbean individuals among those who were found to have glaucoma. African ancestry has been reported to have a higher prevalence of glaucoma; however, limited data are available on the prevalence of glaucoma in the Indo-Caribbean population. Reported glaucoma prevalence from Asia and India is approximately 3–4%.2,13 In view of Trinidad and Tobago having near equivalent Indo-Caribbean and Afro-Caribbean populations, 35% and 34% of the general population respectively, it was expected that the Afro-Caribbean population would have comprised the majority of cases of glaucoma, given the population’s known predisposition to the disease. In this study, there were many individuals of Indo-Caribbean descent (92) compared to the number of persons of Afro-Caribbean descent (67) in the Glaucoma Suspect group which is a possible explanation for the apparent high prevalence of glaucoma in the Indo-Caribbean population. The Indo-Trinidadian ethnic group has a higher percentage of diabetes than the Afro-Trinidadian population resulting in the diabetic population screened being skewed toward this ethnic group.14
Cost is a major barrier to glaucoma screening given the low global prevalence of the disease. However, targeted screening may be more justifiable in higher-risk groups, such as the Caribbean and diabetic populations. Nevertheless, the long-term financial burden of blindness on individuals, families and the healthcare system cannot be ignored especially because irreversible blindness due to glaucoma is preventable. Aspberg et al investigated the effect of population screening on low vision and blindness from POAG and showed that low vision or blindness in the screened population was reduced by half.15 Fundus photography is an inexpensive method of screening especially when patients already receive fundus photographs as part of their diabetic screening. Glaucoma detected through screening rather than by symptomatic presentation is likely to be less severe, and studies have reported an association between higher costs and advancing severity of glaucoma.16 Although screening of the whole population may not be economically feasible, a national policy incorporating combined diabetic retinopathy and glaucoma screening has the potential to reduce visual impairment and the economic burden it carries.
Since all patients in this study found to have glaucoma were aged over 40 years, age-targeted screening may improve cost-effectiveness by focussing on the older, higher-risk group. Interestingly, the majority of the patients with glaucoma in this study had no family history of glaucoma (68%). Therefore, we recommend screening individuals, regardless of their family history.
In this study, we identified previously undetected glaucoma cases that could be treated. Our findings of more than a third of glaucoma patients in this study being undiagnosed compared to worldwide, where at least half of all glaucoma cases are undetected with higher rates of undetected glaucoma in Africa and Asia.17
Only 6.6% of those meeting the glaucoma suspect criteria were found to have diabetic retinopathy features on fundus photography and would have been referred to the clinic, regardless of screening for glaucoma. The vast majority of individuals meeting the screening criteria for glaucoma were referred to the clinic solely for the assessment of glaucoma and would not have received assessment, timely diagnosis and treatment without glaucoma screening.
Fundus photography was moderately accurate in detecting glaucoma in 62.2% of those who screened positive for the disease. In our study, fundus photographs were determined to meet the glaucoma suspect criteria by a grading team. Although each member of the grading team had received training in grading the photos, this subjective assessment was subject to inter-observer variability. AI-assisted fundus photograph grading has shown promising diagnostic performance for glaucoma, with reported sensitivities of 77–97% and accuracies over 80%. Its use has the potential to improve sensitivity, efficiency and reduce reliance on labour-intensive manual grading.18–22
Previous studies have investigated the incorporation of glaucoma screening into the established diabetic retinopathy screening programmes. In the London borough of Brent, Ong et al found the positive predictive value of their diabetic retinopathy screening programme in detecting glaucoma to be 78.8%.23 Tan et al investigated Singapore’s diabetic retinopathy programme and found the sensitivity of a VCDR ≥0.65 on fundus photography in detecting glaucoma to be 70.5%. An enlarged VCDR in combination with other glaucomatous features on fundus photographs increased the sensitivity to 81.8% and yielded a positive predictive value of 14.1% in their study.24 Our study adds to the current literature as it provides data from the Caribbean, in which published reports of concomitant glaucoma and diabetic retinopathy screening by fundus imaging are scarce. The positive predictive value of 62.2% in our study is comparable to that reported in previous studies.
Strengths of this study include its broad geographical distribution, its extensive age range (22–91 years), its fair sample size and representation of the two main ethnic groups locally, supporting its representation of the diabetic population of Trinidad and Tobago.
This study provides a valuable addition to the current knowledge on the prevalence of glaucoma in the diabetic population of Trinidad and Tobago and supports the feasibility of concomitant glaucoma and diabetic retinopathy screening through fundus photography in this population. However, this study had several limitations. The main limitation of the study is that of the persons screened who met the suspect criteria, only 26.9% received full evaluation. The calculated prevalence of glaucoma is therefore an estimate based on data in which there was incomplete follow-up. A possible reason for the poor completion rate in this study is that the patients were required to pay for the visual field and OCT imaging. Another limitation was that only participants who met the glaucoma suspect criteria were referred to the clinic. It was not within the scope of this study to fully evaluate persons who did not meet the suspect criteria; therefore, there is an unknown number of true cases of glaucoma that may have been missed by the grading team so specificity, sensitivity and the negative predictive value were not able to be calculated. Additional limitations include the retrospective design of the study as well as a potential selection bias due to participation in the diabetic eye screening programme being voluntary and therefore individuals who attended the screening may not be fully representative of the wider Caribbean diabetic population. Furthermore, because only persons with diabetes were included in this study, the results may not reflect the prevalence or detection yield of glaucoma in the general population.
Conclusion
Opportunistic glaucoma detection within a diabetic eye screening programme in Trinidad and Tobago was able to identify a clinically meaningful number of previously undetected cases of glaucoma. The extrapolated estimated prevalence of glaucoma in the diabetic population of Trinidad and Tobago was 5.9% in our study (minimum confirmed prevalence 1.6%). These findings suggest that adding glaucoma suspect assessment to existing diabetic retinopathy screening using fundus photography can be a useful strategy in tackling the burden of preventable visual impairment due to glaucoma.
The authors of this study recommend that established diabetic retinopathy screening programmes in the Caribbean incorporate glaucoma suspect criteria into their referral protocols. Opportunistic case-finding should target patients over 40 years old regardless of family history. When integrated into an existing diabetic retinopathy screening service which utilises fundus photography, opportunistic glaucoma detection is feasible. This study, however, does not support universal population-level glaucoma screening at this stage as further studies with a formal cost-effectiveness modelling would be required.
Abbreviations
VCDR, vertical cup-to-disc ratio; IOP, intraocular pressure; TEH, Trinidad Eye Hospital; RNFL, retinal nerve fibre layer; POAG, primary open-angle glaucoma; OCT, optical coherence tomography; AI, artificial intelligence.
Ethical Approval
The tenets of the Declaration of Helsinki were adhered to. This study utilized anonymized data collected as part of a routine diabetic eye screening programme. Ethical approval was obtained from the Research Ethics Committee of the Ministry of Health, Trinidad and Tobago (Reference: He: 3/13/441 Vol. II dated 18 September 2025). All patients attending the screening service were informed that their anonymized clinical information might be used for research and quality improvement purposes. Patients were given the opportunity to decline participation through an opt-out option on the intake documentation. Participation in the screening process after receiving this information constituted implied informed consent for the use of anonymized data. No personally identifiable information was included in the dataset used for analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors report no competing interests in this work.
References
1. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901–8. doi:10.1001/jama.2014.3192
2. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
3. Mason RP, Kosoko O, Wilson MR, et al. National survey of the prevalence and risk factors of glaucoma in St. Lucia, West Indies. Part I. Prevalence Findings. Ophthalmology. 1989;96(9):1363–1368. doi:10.1016/S0161-6420(89)32708-4
4. Leske MC, Wu SY, Nemesure B, Hennis A; Barbados Eye Studies Group. Causes of visual loss and their risk factors: an incidence summary from the Barbados Eye Studies. Rev Panam Salud Publica. 2010;27(4):259–267. doi:10.1590/S1020-49892010000400004
5. Leske MC, Connell AM, Schachat AP, Hyman L. The Barbados Eye Study: prevalence of open-angle glaucoma. Arch Ophthalmol. 1994;112(6):821–829. doi:10.1001/archopht.1994.01090180121046
6. Braithwaite T, Verlander NQ, Peto T, et al. National Eye Survey of Trinidad and Tobago (NESTT): prevalence, causes, and risk factors for presenting vision impairment in adults over 40 years. Br J Ophthalmol. 2020;104:74–80. doi:10.1136/bjophthalmol-2018-313428
7. Gunzenhauser R, Coleman AL. Glaucoma screening guidelines worldwide. J Glaucoma. 2024;33(Suppl 1):S9–S12. doi:10.1097/IJG.0000000000002362
8. Mahabadi N, Zeppieri M, Tripathy K. Open-angle glaucoma. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2024.
9. Boland MV, Ervin AM, Friedman DS, et al. Comparative effectiveness of treatments for open-angle glaucoma: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2013;158:271–279. doi:10.7326/0003-4819-158-4-201302190-00008
10. Mangione CM, Barry MJ, Nicholson WK; US Preventive Services Task Force. Screening for primary open-angle glaucoma: US Preventive Services Task Force recommendation statement. JAMA. 2022;327(20):1992–1997. doi:10.1001/jama.2022.7013
11. Gedde SJ, Vinod K, Wright MM, et al. Primary open-angle glaucoma preferred practice pattern®. Ophthalmology. 2021;128(1):P71–P150. doi:10.1016/j.ophtha.2020.10.022
12. Ehrlich JR, Burke-Conte Z, Wittenborn JS, et al. Prevalence of glaucoma among US adults in 2022. JAMA Ophthalmol. 2024;142(11):1046–1053. doi:10.1001/jamaophthalmol.2024.3884
13. Palimkar A, Khandekar R, Venkataraman V. Prevalence and distribution of glaucoma in central India (Glaucoma Survey 2001). Indian J Ophthalmol. 2008;56(1):57–62. doi:10.4103/0301-4738.37597
14. Nayak BS, Sobrian A, Latiff K, et al. The association of age, gender, ethnicity, family history, obesity, and hypertension with type 2 diabetes mellitus in Trinidad. Diabetes Metab Syndr. 2014;8(2):91–95. doi:10.1016/j.dsx.2014.04.018
15. Aspberg J, Heijl A, Bengtsson B. Screening for open-angle glaucoma and its effect on blindness. Am J Ophthalmol. 2021;228:106–116. doi:10.1016/j.ajo.2021.03.030
16. Real J, Lafuente M, Palma S, Tártara L. Direct costs of glaucoma: relationship between cost and severity of the disease. Chronic Illn. 2018;16(4):266–274. doi:10.1177/1742395318803660
17. Soh Z, Yu M, Betzler B, et al. The global extent of undetected glaucoma in adults: a systematic review and meta-analysis. Ophthalmology. 2021;128:1393–1404. doi:10.1016/j.ophtha.2021.04.009
18. Sidhu Z, Mansoori T. Artificial intelligence in glaucoma detection using color fundus photographs. Indian J Ophthalmol. 2024;72(3):408–411. doi:10.4103/IJO.IJO_613_23
19. Zapata MA, Royo-Fibla D, Font O, et al. Artificial intelligence to identify retinal fundus images, quality validation, laterality evaluation, macular degeneration, and suspected glaucoma. Clin Ophthalmol. 2020;14:419–429. doi:10.2147/OPTH.S235751
20. Rao DP, Shroff S, Savoy FM, et al. Evaluation of an offline, artificial intelligence system for referable glaucoma screening using a smartphone-based fundus camera: a prospective study. Eye. 2024;38:1104–1111. doi:10.1038/s41433-023-02826-z
21. Coan LJ, Williams BM, Adithya VK, et al. Automatic detection of glaucoma via fundus imaging and artificial intelligence: a review. Surv Ophthalmol. 2023;68(1):17–41. doi:10.1016/j.survophthal.2022.08.005
22. Boverhof BJ, Corro Ramos I, Vermeer KA, et al. The cost-effectiveness of an artificial intelligence-based population-wide screening program for primary open-angle glaucoma in the Netherlands. Value Health. 2025;28(9):1317–1326. doi:10.1016/j.jval.2025.06.006
23. Ong HS, Levin S, Vafidis G. Glaucoma detection using optic disc images from the English National Screening Programme for diabetic retinopathy. J Glaucoma. 2013;22(6):496–500. doi:10.1097/IJG.0b013e3182447d58
24. Tan R, Teo KYC, Husain R, et al. Evaluating the outcome of screening for glaucoma using colour fundus photography-based referral criteria in a teleophthalmology screening programme for diabetic retinopathy. Br J Ophthalmol. 2024;108:933–939. doi:10.1136/bjo-2023-323339
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.