Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Opinion and Knowledge of Pulmonologists, Primary Care Physicians, and Nurses About Inhaled Therapy in COPD. Inhal-Epoc Survey
Authors De Miguel-Díez J ![]() , Giner Donaire J, Gómez Sáenz JT, Trigueros Carrero JA
, Giner Donaire J, Gómez Sáenz JT, Trigueros Carrero JA ![]() , Artigas Feliu R, Cruz Culebra N, Plaza V
, Artigas Feliu R, Cruz Culebra N, Plaza V ![]()
Received 28 November 2024
Accepted for publication 29 June 2025
Published 11 February 2026 Volume 2026:21 499279
DOI https://doi.org/10.2147/COPD.S499279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Javier De Miguel-Díez,1 Jordi Giner Donaire,2 José Tomas Gómez Sáenz,3 Juan Antonio Trigueros Carrero,4 Remei Artigas Feliu,5 Núria Cruz Culebra,5 Vicente Plaza6
1Pulmonology Service, Hospital General Universitario Gregorio Marañón, Universidad Complutense de Madrid, Instituto de Investigación Sanitaria Gregorio Marañón (IISGM), Madrid, Spain; 2Pulmonology and Allergology Service, Hospital de la Santa Creu I Sant Pau, Barcelona, Spain; 3Nájera Health Center, La Rioja, Spain; 4Buenavista Health Center, Toledo, Spain; 5Grupo Menarini España, Medical Department, Barcelona, Spain; 6Pulmonology and Allergology Service, Hospital de la Santa Creu I Sant Pau, Instituto de Investigación Biomédica Sant Pau (IIB Sant Pau), Departamento de Medicina, Universidad Autónoma de Barcelona, Barcelona, Spain
Correspondence: Javier De Miguel-Díez, Pulmonology Service, Hospital General Universitario Gregorio Marañón, Universidad Complutense de Madrid, Instituto de Investigación Sanitaria Gregorio Marañón (IiSGM), C/Dr. Esquerdo, 46, Madrid, 28007, Spain, Email [email protected]
Purpose: Despite the efforts made to improve inhalation technique by both patients and healthcare professionals, significant deficiencies were found in critical aspects of inhaler use and device selection. The aim of this study is to know the current opinion and knowledge of pulmonologists, primary care physicians, and nurses about inhaled therapy in chronic obstructive pulmonary disease (COPD).
Methods: Survey conducted between April-July 2023 by a committee of experts formed by 2 pulmonologists, 2 primary care physicians, and one nurse specialist in inhaled therapy. It consisted of 27 questions and was sent by e-mail to professionals throughout Spain with experience in the management of COPD with inhaled therapy.
Results: A total of 554 experts from all over Spain participated. Thirty-one percent and 43.5% of the respondents could not identify, respectively, which were the critical steps for correct inhalation of the pressurized metered-dose inhaler (pMDI) and the multidose dry powder inhaler (DPI). Conventional pMDIs were considered to be the devices that provide greater oropharyngeal deposition and less pulmonary deposition. The majority of respondents considered essential or important to take into account the patients’ opinion in selecting the inhaler, and preferred to review the inhalation technique rather than change the device. The main criteria for the choice of inhaler in COPD patients were their previous experience, preference, and severity. With a wide dispersion of results, Ellypta®, pMDI with chamber, Genuair®, Respimat®, and conventional pMDI were preferred in that order.
Conclusion: Knowledge about inhaled therapy in COPD remains insufficient. There is a significant and important lack of knowledge in key aspects of the use of inhaler devices, such as the critical steps for correct inhalation and the selection criteria for inhalation devices. It is necessary to continue promoting training programs for both patients and healthcare personnel in inhalers and inhalation techniques.
Keywords: COPD, DPI, inhalation device, inhaled therapy, pMDI
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive chronic respiratory condition that represents a significant public health burden worldwide. Effective management of COPD involves the use of inhaled therapies, which play a crucial role in controlling symptoms and improving patients’ quality of life. Despite the advantages of inhaled therapy over other routes of administration, such as faster onset of action, lower required doses, and fewer systemic adverse effects,1 it has the limitation to be administered properly for a minimal amount of the drug to reach the lower airways and exert its pharmacological action successfully. Incorrect use of the inhaler device would lead to increased reliever use, increased use of emergency medical services, and worsening of disease.2–7
Since the appearance of the first inhaler device 60 years ago (Medihaler-Epi®), today’s devices have evolved significantly, allowing treatment to be individualized for each patient. However, this evolution requires healthcare professionals to keep constantly up to date with the characteristics of the new inhaler devices, their limitations and drawbacks and, above all, the inhalation technique required for their operation. For this reason, most clinical practice guidelines consider training patients in the correct use of inhalation devices to be essential.8–12
Despite the involvement of medical societies and the pharmaceutical industry and the recommendations offered in all clinical practice guidelines to improve the use of inhaled therapy,13,14 numerous studies have shown that most patients do not adequately use inhalation devices15–22 or that the healthcare personnel involved in the treatment and supervision of these patients do not have sufficient knowledge or skills in their use.21,23–30 In this context, it is essential to assess the level of knowledge of health professionals responsible for COPD management, such as pulmonologists, primary care physicians, and nurses, regarding available inhaled therapies.
This study aims to address the imperative need for a thorough understanding of the degree of knowledge that these health care professionals in Spain have about inhaled therapies used in the treatment of COPD. The information gathered through this research will not only contribute to improving the care and treatment of COPD patients, but will also provide valuable insights for the design of educational and training programs to strengthen the training of health professionals in this field.
Methods
Spanish descriptive survey conducted by a committee of experts formed by 2 pulmonologists, 2 primary care physicians, and one nurse specialist in inhaled therapy. It consisted of 27 questions and was sent by e-mail to professionals throughout Spain with experience in the management of COPD with inhaled therapy. The survey was carried out between April and July 2023. In agreement with the clinical research ethics committee of the Hospital Universitario Gregorio Marañón (Madrid, Spain), the study did not require its approval because it did not involve patients, but rather health professionals who accepted the conditions of the survey by participating in it.
The first 5 questions gathered information about the respondents’ age, sex, medical specialty, geographical location, and number of COPD patients attended (Table 1). Subsequent questions were developed using a multiple choice format and concerned the following topics: technical knowledge of inhalers (Table 2), patient preferences and satisfaction (Table 3), and specific aspects of inhalers in COPD (Table 4). Final results of the questionnaire were shown as percentages with respect to the total number of respondents.
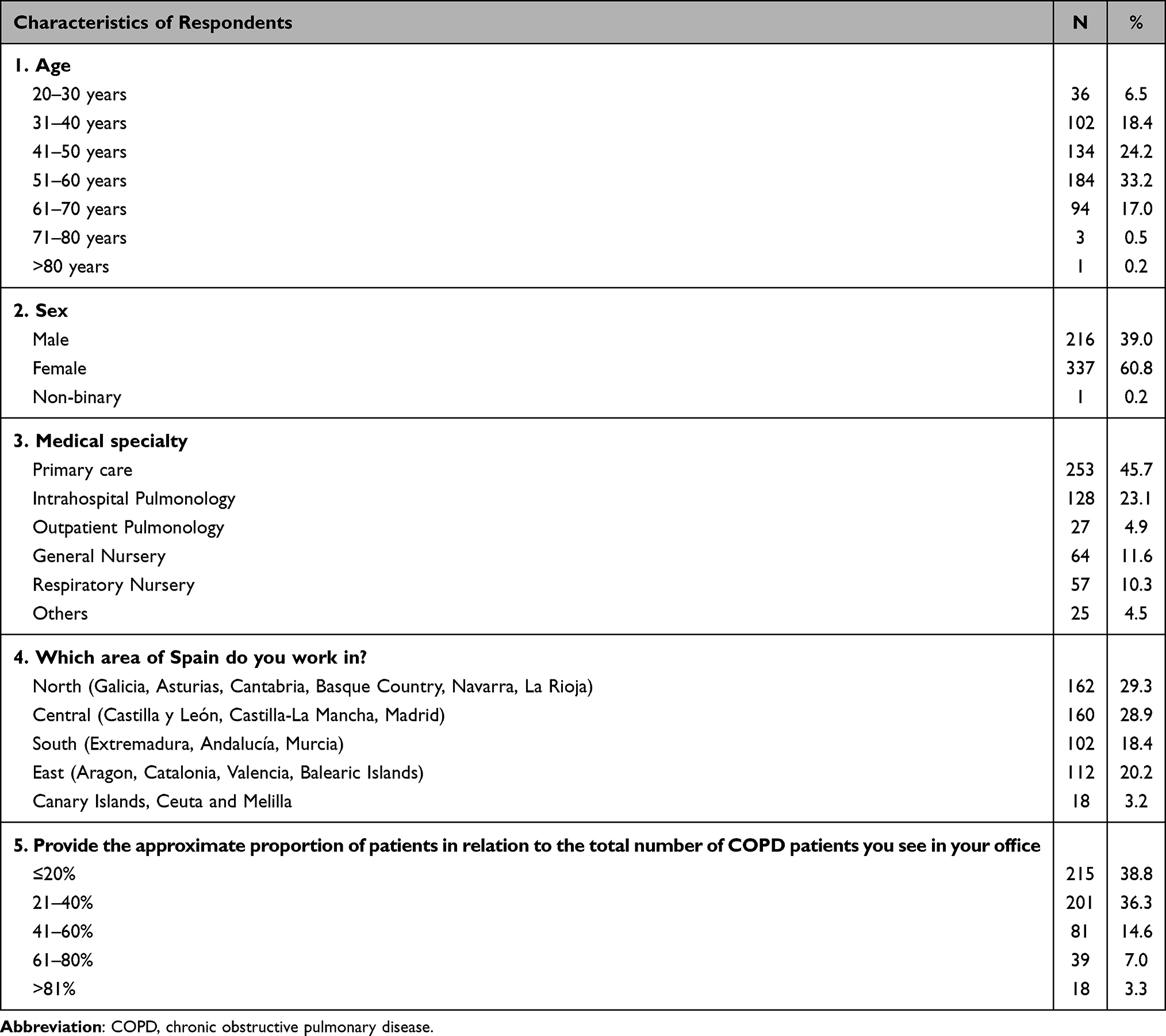 |
Table 1 Characteristics of Respondents (N = 554) |
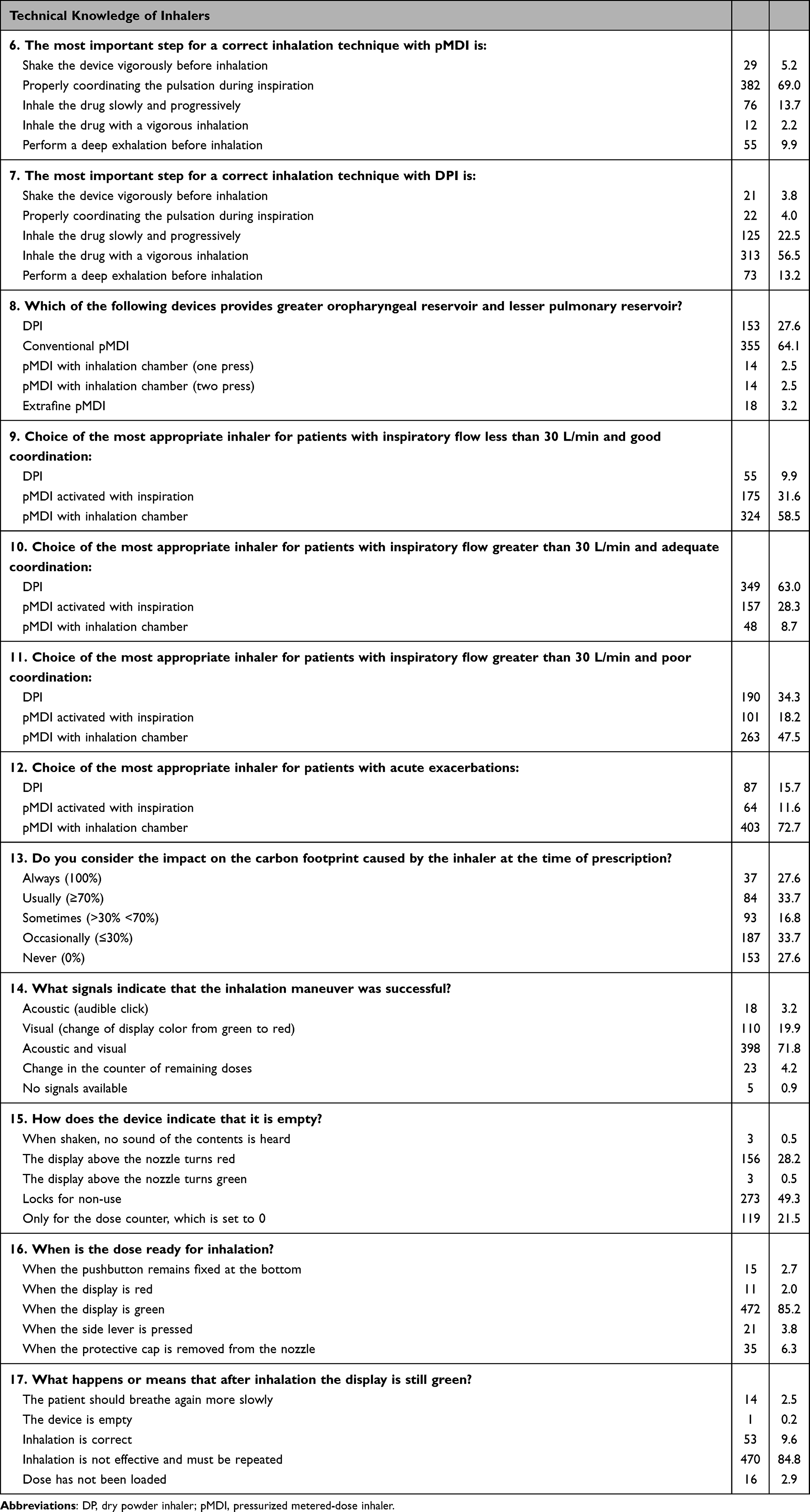 |
Table 2 Technical Knowledge of Inhalers (N = 554) |
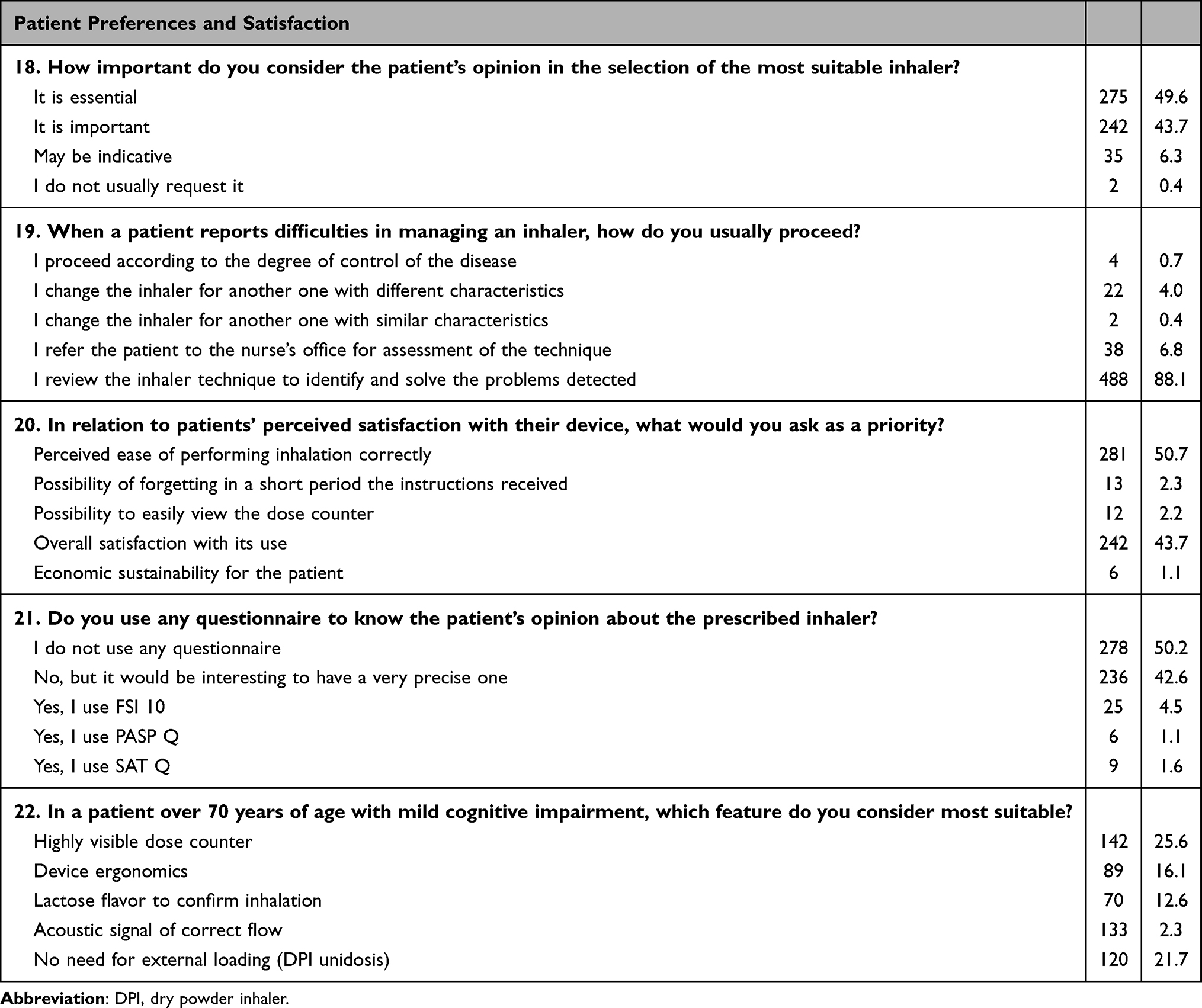 |
Table 3 Patient Preferences and Satisfaction (N = 554) |
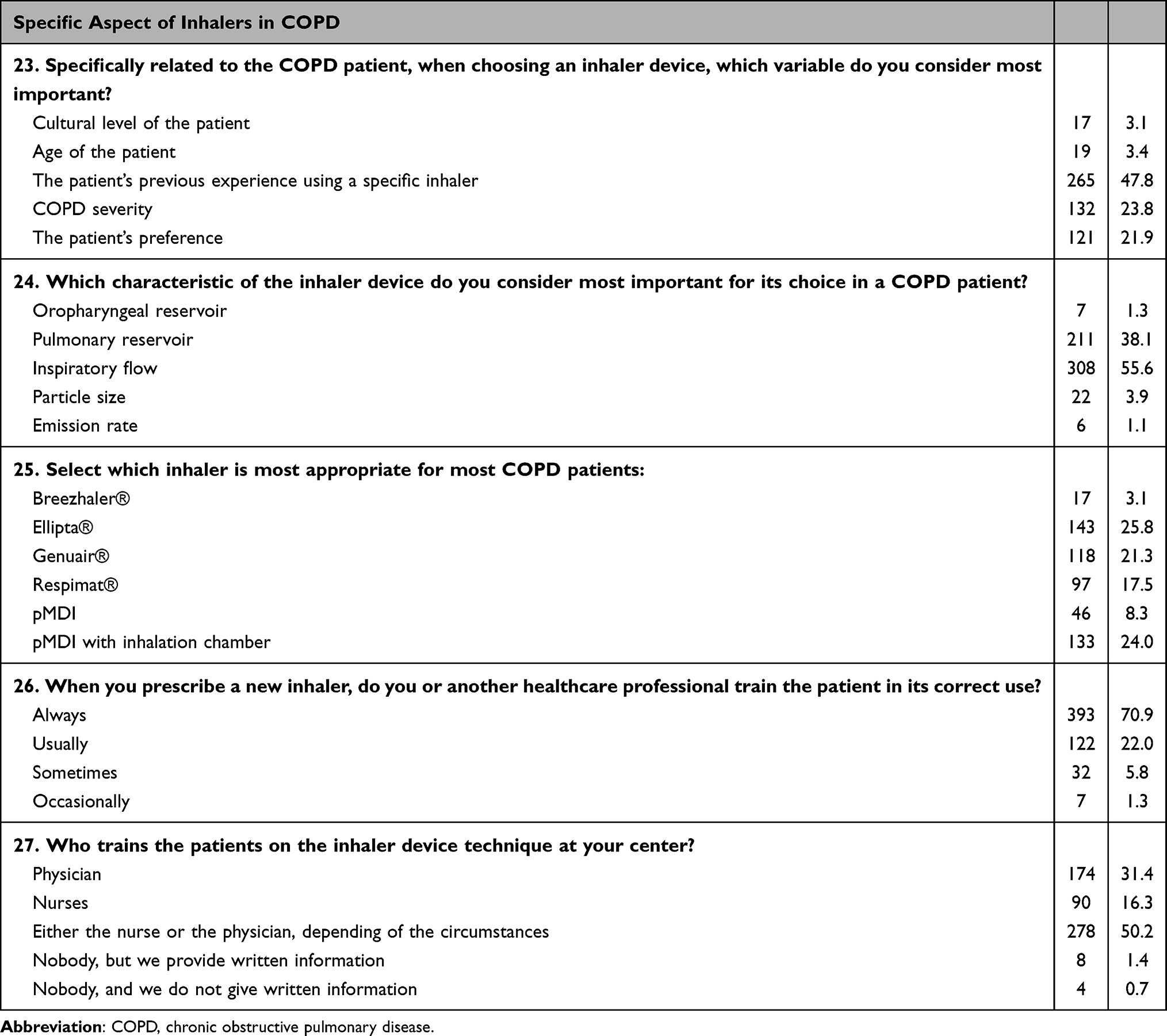 |
Table 4 Specific Aspect of Inhalers in COPD (N = 554) |
Results
A total of 554 experts from all over Spain completed the questionnaire. Most respondents were female (60.8%) and were between 51 and 60 years old (33.2%). Regarding medical specialty, 45.7% were Primary Care physicians, 23.1% intrahospital pulmonologists, 11.6% general nurses, 10.3% respiratory nurses, and 4.9% were outpatients pulmonologists. Respondents came from the following areas of Spain: 29.3% were from the north, 28.9% from the central area, 20.2% from the eastern regions, 18.4% from the south, and 3.2% were from the Canary Islands and Ceuta y Melilla cities (Table 1).
Regarding the technical knowledge of the inhalers (Table 2), only 69% and 56.5% of the respondents could identify, respectively, which were the critical steps for correct inhalation of the pressurized cartridge (pMDI) and the multidose dry powder inhaler (DPI). Conventional pMDIs were considered by 64.1% of respondents to be the devices that provide greater oropharyngeal deposition and less pulmonary deposition; 58.5% considered pMDI with chamber the most appropriate for patients with inspiratory flow < 30 L/min and good coordination; 63% considered DPI the most appropriate for patients with inspiratory flow > 30 L/min and adequate coordination; 47.5% and 34.3% considered pMDI with chamber and DPI respectively the most appropriate devices for patients with inspiratory flow > 30 L/min and poor coordination; and 72.7% considered pMDI with chamber the most appropriate for acute exacerbations. About Genuair®, most participants knew when the device was ready and if inhalation has been ineffective, but showed imprecision about the empty device indication.
About patient preferences and satisfaction (Table 3), the majority of respondents considered essential (49.6%) or important (43.7%) to take into account the patients’ opinion in selecting the inhaler. To know the satisfaction of the patient with the inhaler, 50.7% of respondents ask as priority about the perceived ease of performing inhalation correctly and 43.7% about overall satisfaction with its use. However, 50.2% do not use any questionnaire to know patient’s opinion about the inhaler, but 42.6% would be interested in having a precise questionnaire about that. When a patient reports difficulties in managing an inhaler, 88.1% prefer to review the inhalation technique rather than change the device.
Finally, the main criteria for the choice of inhaler in the COPD patient were previous experience (47.8%), patient severity (23.8%), and patient preferences (21.9%). In these patients, 55.6% considered inspiratory flow and 38.1% pulmonary reservoir as the most important characteristics for the inhaler device. With a wide dispersion of results, Ellypta® (25.8%), pMDI with inhalation chamber (24%), Genuair® (21.3%), Respimat® (17.5%), and pMDI (8.3%) were the inhaler devices selected for COPD patients. Near 71% of respondents always train the patient in the correct use of a new prescribed inhaler device, and 50.2% answered that either the nurse or the physician are the healthcare professional who train the patient depending the circumstances (Table 4).
Discussion
The present study shows that the knowledge on inhaled therapy currently used in COPD treatment remains poor in Spain. Moreover, importance of this study lies in its ability to identify possible gaps in knowledge, thus allowing the development of specific strategies to improve the competence of health professionals in the management of inhaled therapy in patients with COPD. With the information obtained, it will be possible to implement educational and awareness interventions that lead to a more effective and personalized management of the disease, improving in turn the clinical outcomes and quality of life of patients affected by this chronic lung disease.
Despite the good answers of most of the respondents, there is a significant and important lack of knowledge in key aspects on the use of inhaler devices: 31% and 43.5% of the respondents could not identify, respectively, which were the critical steps for correct inhalation of pMDI and DPI. Even there was no broad agreement on the selection criteria for inhalation devices. This lack of knowledge among healthcare professionals involved in the treatment of COPD has important implications for patient education on the use of inhalers and, therefore, for adherence to treatment and disease control outcomes.
Most of the studies performed to evaluate the inhalation therapy highlight that the majority of patients do not adequately use inhalation devices and the healthcare personnel involved in their treatment and monitoring do not have sufficient knowledge or skills in the use of these devices.13–30 A meta-analysis evaluated patients’ inhaler technique skills over the past 40 years (from 1975 to 2014).22 It described that the use of inhalers (MDI or DPI) in patients with asthma or COPD had not improved in all that time. The inhalation technique was correct in only 31% of patients, acceptable in 41%, and poor in 31%.22 In another meta-analysis with the same methodology, studies assessing the inhaler technique proficiency of health care professional in using pMDI and DPI inhalers over the past 40 years were evaluated.30 As in the case of patients, healthcare professionals demonstrated an inadequate knowledge of the proper use of inhalers. The inhaler technique was considered correct in 15.5% of cases, decreasing over time from 20.5% from the early period (defined as 1975–1995) to 10.8% (95% CI, 7.3–14.8) during the late period (1996–2014).30
Of these studies, it is worth mentioning one conducted more than 10 years ago in the same environment and by practically the same team as the current study, which makes it possible to compare its results with ours.29 The results of that study are very similar to the current study, which means that in more than 10 years the use of inhalation devices has not improved. However, it is interesting to highlight some of them. Regarding the technical knowledge of inhalers, it seems that that the knowledge of pMDI has decreased (from 72.3% to 69%) and that of DPI has improved (from 46.1% to 56.5%). Concerning the factors considered when prescribing the inhalation device, the previous study gave priority to the patient’s experience (38.8%), the disease to be treated (25.7%), and the patient’s preferences (12.3%). In the current study, the importance of the patient’s experience (47.8%) and, especially, the patient’s preferences (21.9%) has increased. Ten years ago, only 27.7% of healthcare professionals “always” assessed the inhalation technique of patients, whereas now 70.9% do so. Finally, previously, patient training on the use of inhalers was carried out by the physician (34.6%), nursing (22.4%) or either (38.8%). Currently, 50.2% of respondents considered that training is done by either the nurse or the physician depending on the circumstances. Very few thought that only the nurse (16.3%) or the physician (31.4%) would do it.
The main limitation of our study is related to the method used. The data are based solely on the results of a survey on self-perceived knowledge and may not reflect respondents’ behavior in actual clinical practice.
Conclusions
Despite the efforts made to improve inhalation technique by both patients and healthcare professionals, these efforts do not seem to have been sufficient. However, despite the lack of knowledge about the correct use of inhalation devices, there is a greater awareness of their importance. Now more than before, any healthcare staff member, depending on the circumstances, always teaches patients the correct inhalation technique. In any case, it is necessary to continue promoting training programs for both patients and healthcare personnel in inhalers and inhalation techniques.
Ethics Approval and Informed Consent
In agreement with the clinical research ethics committee of the Hospital Universitario Gregorio Marañón (Madrid, Spain), the study did not require its approval because it did not involve patients, but rather health professionals who accepted the conditions of the survey by participating in it. This ethics committee has provided the authors with a certificate accrediting this decision.
Acknowledgments
The authors would like to thank LUZAN 5 and Fernando Sánchez Barbero for editorial assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by Menarini (Spain).
Disclosure
JMD has received grants and honoraria from AstraZeneca, Bial, Boehringer-Ingelheim, Chiesi, FAES, Gebro, GSK, Janssen, Menarini, Novartis, Roche, Teva, Pfizer, and Zambón. JGD collaborated in studies with Chiesi, Menarini, and Orion. JTGS in the last three years has received honoraria for speaking at sponsored meetings from AstraZeneca, Boehringer-Ingelheim, Chiesi, GSK, and Menarini. JATC in the last three years has received honoraria for teaching activities sponsored by AstraZeneca, Bial, Chiesi, GSK, Menarini, Pfizer, TEVA, and Zentiva. RAF is a member of Menarini LMSA’s medical department. NCC is a member of Menarini LMSA’s medical department. VP in the last three years has received honoraria for speaking at sponsored meetings from AstraZeneca, Boehringer-Ingelheim, Chiesi, Gebro, GSK, Luminova-Medwell, and Sanofi; help assistance to meeting travel from AstraZeneca and Chiesi; and act as a consultant for AstraZeneca, Chiesi, GSK, and Menarini. The authors report no other conflicts of interest in this work.
References
1. Pritchard J, Sharma R. Introduction: inhaled drug delivery. J Aerosol Med. 2002;14(1):S1–9. doi:10.1089/08942680150506277
2. McFadden Jr ER. Improper patient techniques with metered dose inhalers: clinical consequences and solutions to misuse. J Allergy Clin Immunol. 1995;96(2):278–283. doi:10.1016/S0091-6749(95)70206-7
3. Lotvall J. Inhalation therapy of the future - How will it change the way we treat asthma? J Aerosol Med. 2001;14(Suppl 1):S45–50. doi:10.1089/08942680150506330
4. Lindgren S, Bake B, Larsson S. Clinical consequences of inadequate inhalation technique in asthma therapy. Eur J Respir Dis. 1987;70(2):93–98.
5. Giraud V, Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002;19(2):246–251. doi:10.1183/09031936.02.00218402
6. Barnes PJ. Achieving asthma control. Curr Med Res Opin. 2005;21(Suppl 4):S5–9. doi:10.1185/030079905X61730
7. Molimard M, Raherison C, Lignot S, et al. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2017;49(2):1601794. doi:10.1183/13993003.01794-2016
8. Laube BL, Janssens HM, de Jongh FH, et al. What the pulmonary specialist should know about the new inhalation therapies. Eur Respir J. 2011;37(6):1308–1331. doi:10.1183/09031936.00166410
9. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Available from: https://goldcopd.org.
10. Global Initiative for Asthma (GINA). Available from: https://ginasthma.org.
11. Guía Española para el Manejo del Asma (GEMA). Available from: https://www.gemasma.com.
12. Plaza Moral V, Alobid I, Álvarez Rodríguez C, et al. GEMA 5.3. Spanish Guideline on the Management of Asthma. Open Respir Arch. 2023;5(4):100277. doi:10.1016/j.opresp.2023.100277
13. Dolovich MB, Ahrens RC, Hess DR, et al. Device selection and outcomes of aerosol therapy: evidence-based guidelines: american College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127(1):335–371. doi:10.1378/chest.127.1.335
14. Plaza V, Casan P, de Diego A, et al. Recommendations for the use of inhaled drugs. Arch Bronconeumol. 1996;32(Suppl 1):8–9.
15. De Blaquiere P, Christensen DB, Carter WB, Martin TR. Use and misuse of metered-dose inhalers by patients with chronic lung disease. A controlled, randomized trial of two instruction methods. Am Rev Respir Dis. 1989;140(4):910–916. doi:10.1164/ajrccm/140.4.910
16. Thompson J, Irvine T, Grathwohl K, Roth B. Misuse of metered-dose inhalers in hospitalized patients. Chest. 1994;105(3):715–717. doi:10.1378/chest.105.3.715
17. Goodman DE, Israel E, Rosenberg M, Johnston R, Weiss ST, Drazen JM. The influence of age, diagnosis, and gender on proper use of metered-dose inhalers. Am J Respir Crit Care Med. 1994;150(5 Pt 1):1256–1261. doi:10.1164/ajrccm.150.5.7952549
18. van der Palen J, Klein JJ, Kerkhoff AH, van Herwaarden CL. Evaluation of the effectiveness of four different inhalers in patients with chronic obstructive pulmonary disease. Thorax. 1995;50(11):1183–1187. doi:10.1136/thx.50.11.1183
19. van Beerendonk I, Mesters I, Mudde AN, Tan TD. Assessment of the inhalation technique in outpatients with asthma or chronic obstructive pulmonary disease using a metered-dose inhaler or dry powder device. J Asthma. 1998;35(3):273–279. doi:10.3109/02770909809068218
20. Molimard M, Raherison C, Lignot S, Depont F, Abouelfath A, Moore N. Assessment of handling of inhaler devices in real life: an observational study in 3811 patients in primary care. J Aerosol Med. 2003;16(3):249–254. doi:10.1089/089426803769017613
21. Plaza V, Sanchis J. Medical personnel and patient skill in the use of metered dose inhalers: a multicentric study. CESEA Group. Respiration. 1998;65(3):195–198. doi:10.1159/000029259
22. Sanchis J, Gich I, Pedersen S. Aerosol Drug Management Improvement Team (ADMIT). Systematic review of errors in inhaler use: has patient technique improved over time? Chest. 2016;150(2):394–406. doi:10.1016/j.chest.2016.03.041
23. Kelling JS, Strohl KP, Smith RL, Altose MD. Physician knowledge in the use of canister nebulizers. Chest. 1983;83(4):612–614. doi:10.1378/chest.83.4.612
24. Hanania NA, Wittman R, Kesten S, Chapman KR. Medical personnel’s knowledge of and ability to use inhaling devices. Metered-dose inhalers, spacing chambers, and breath-actuated dry powder inhalers. Chest. 1994;105(1):111–116. doi:10.1378/chest.105.1.111
25. Self TH, Arnold LB, Czosnowski LM, Swanson JM, Swanson H. Inadequate skill of healthcare professionals in using asthma inhalation devices. J Asthma. 2007;44(8):593–598. doi:10.1080/02770900701554334
26. Kim SH, Kwak HJ, Kim TB, et al. Inappropriate techniques used by internal medicine residents with three kinds of inhalers (a metered dose inhaler, Diskus, and Turbuhaler): changes after a single teaching session. J Asthma. 2009;46(9):944–950. doi:10.3109/02770900903229701
27. Felez MA, González Clemente JM, Cardona Q, Montserrat JM, Picado C. Skill in the handling of aerosols by health care personnel. Rev Clin Esp. 1991;188(4):185–187.
28. Plaza V, Giner J, Gómez J, Casan P, Sanchis J. Health workers’ knowledge and skills regarding the use of the Turbuhaler inhaler. Arch Bronconeumol. 1997;33(3):113–117. doi:10.1016/S0300-2896(15)30638-4
29. Plaza V, Sanchis J, Roura P, et al. Physicians’ knowledge of inhaler devices and inhalation techniques remains poor in Spain. J Aerosol Med Pulm Drug Deliv. 2012;25(1):16–22. doi:10.1089/jamp.2011.0895
30. Plaza V, Giner J, Rodrigo GJ, Dolovich MB, Sanchis J. Errors in the use of inhalers by health care professionals: a systematic review. J Allergy Clin Immunol Pract. 2018;6(3):987–995. doi:10.1016/j.jaip.2017.12.032
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.