Back to Journals » Clinical Ophthalmology » Volume 16
Ophthalmology Resident Ophthalmic Trauma Case Exposure: Trends Over Time and an ACGME Case Log Analysis
Authors Abousy M ![]() , Schilling A
, Schilling A ![]() , Qiu M
, Qiu M ![]() , Justin GA
, Justin GA ![]() , Rajaii F
, Rajaii F ![]() , Li X, Woreta FA
, Li X, Woreta FA ![]()
Received 28 January 2022
Accepted for publication 8 April 2022
Published 2 May 2022 Volume 2022:16 Pages 1365—1373
DOI https://doi.org/10.2147/OPTH.S359384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mya Abousy,1 Andy Schilling,1 Mary Qiu,2 Grant A Justin,3 Fatemeh Rajaii,1 Ximin Li,1 Fasika A Woreta1
1Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 2Department of Ophthalmology, University of Chicago Medicine, Chicago, IL, USA; 3Department of Ophthalmology, Walter Reed National Military Medical Center, Bethesda, MD, USA
Correspondence: Fasika A Woreta, Wilmer Eye Institute, Johns Hopkins University School of Medicine, 600 N. Wolfe Street, Baltimore, MD, 21287, USA, Email [email protected]
Purpose: To describe ophthalmology resident experience with ophthalmic trauma cases in the U.S.
Methods: We analyzed Accreditation Council for Graduate Medical Education (ACGME) case log data and de-identified case logs from US ophthalmology residency programs for residents graduating in 2018. Current Procedural Terminology (CPT) codes documented as “Globe Trauma” and trauma-related “Oculoplastic and Orbit” codes including lid lacerations and lateral canthotomies were analyzed.
Results: 38 residency programs provided case logs (response rate: 32.2%). Residents performed an average of 7.24± 4.37 open globe repairs, 8.66± 6.94 lid laceration repairs, 0.49± 1.4 orbital fracture repairs, 1.22± 1.81 lateral canthotomies, and 0.28± 0.69 anterior chamber washouts as primary surgeon. On average, the most logged “Globe Trauma” procedure was open globe repair as primary surgeon. The more common trauma-related “Oculoplastic and Orbit” procedure was lid laceration repair as primary surgeon. 42.8% of residents did not log any lateral canthotomy procedures. Medium programs performed significantly more canthotomies than large programs (F(2166) = 6.35, p = 0.002), and large programs performed significantly more orbital fracture repairs than small and medium programs (F(2166) = 4.45, p = 0.013).
Conclusion: Significant variation in globe trauma volume exists across programs. ACGME guidelines require a minimum of four globe trauma procedures for graduation, but procedures like anterior chamber paracentesis count towards this requirement. Open globe repairs, simple lid lacerations, and lateral canthotomies are basic skills every graduating resident should be competent in. Updating ACGME case log requirements for ophthalmic trauma and increasing opportunities for wet lab simulations may assist in ensuring graduating ophthalmology residents’ competency in performing these procedures.
Keywords: globe trauma, ACGME, education, residency, surgical education
Introduction
Preventable trauma to the eye is a significant public health issue, with approximately 2.0 to 2.4 million cases per year in the United States alone.1 Ocular trauma is the leading cause of monocular blindness worldwide.2,3 Ophthalmic trauma includes both open and closed globe intraocular injuries as well as adnexal injuries such as eyelid lacerations.1 A survey of practicing ophthalmologists regarding perceived importance of skills that should be obtained during residency training revealed that management of ophthalmic trauma was recognized as the second-most important skill following interpersonal and communication skills.4
Currently, the Accreditation Council for Graduate Medical Education (ACGME) specifies the minimum number of surgeries a resident must perform in order to graduate from a residency program in the US.5,6 Under the specific category of “globe trauma”, the minimum number of cases required by the ACGME is four procedures as primary surgeon. The ACGME divides ocular trauma cases into three broad categories: “corneal/corneoscleral laceration/globe rupture”, “intraocular foreign body” (IOFB), and “other globe trauma (eg, anterior chamber washout)”. Trends in resident exposure to other ophthalmic subspecialties over time including vitreoretinal surgery and glaucoma have been reported;7,8 however, trends in resident exposure to ophthalmic trauma procedures are yet to be reported.
The purpose of this study is thus twofold: (1) to evaluate national trends in US ophthalmology resident exposure to ophthalmic trauma according to publicly-available data from the ACGME and (2) to provide an in-depth analysis of resident exposure to ophthalmic trauma cases using case log data from residents graduating in 2018. The results of the study may inform curriculum redevelopment to reflect the importance and relevance of ophthalmic trauma in ophthalmologic training. Furthermore, this information may aid residency program directors in understanding which resident competencies need additional support or training opportunities.
Materials and Methods
National case log statistics for ophthalmology residents were extracted from publicly available ACGME records for the years of 2009–2018 to track trends in US ophthalmology resident experience with ophthalmic trauma over time.9 Average number of procedures per resident as primary surgeon, standard deviation, and number of residents were collected. ACGME statistics from 2009–2010 and 2017–2018 were compared to assess for temporal trends. This study was approved by the Institutional Review Board of the Johns Hopkins University, and study activities adhered to the guidelines of the Declaration of Helsinki.
To provide a more nuanced understanding of ophthalmic trauma case experience in residency, we contacted program directors of all 118 ophthalmology residency programs in the United States by e-mail and requested the deidentified case logs for residents graduating in the class of 2018. Programs were contacted up to two times after the initial email if no response was received. Program directors were given the option to not participate in the study. Incomplete case logs (ie, did not include procedures from all three years of residency or did not include procedures from all subspecialties) were excluded. The Current Procedural Terminology (CPT) codes of all resident case logs were tabulated along with the year the procedure was performed and whether the procedure was performed as primary surgeon or assistant. All procedures between July 2015 - June 2018 were recorded. For all responding programs, presence of a vitreoretinal and/or oculoplastic fellowship, program size, and program geographic region were documented based on information available on the program’s website.
All CPT codes listed as “Globe Trauma” were included in addition to trauma-related “Oculoplastic and Ophthalmic Surgery” codes. CPT codes were classified into 10 total categories (Table 1). The trauma-related procedures logged as oculoplastic and orbit surgeries include the following: eyelid lacerations, orbital fractures and implant procedures, canthotomy, and removal of eyelid foreign body. These procedures were included in the overall analysis of this study because they are often performed in patients that present with ophthalmic trauma. Lid lacerations, for example, can occur in conjunction with intraocular foreign bodies. Similarly, an orbital fracture may simultaneously involve injury to the eyelid and the globe. Lateral canthotomies are also essential procedures in ocular trauma, as rapid increases in intra-ocular pressure can often follow orbital trauma.10 While the majority of the analysis grouped procedures logged as “globe trauma” and trauma-related oculoplastic and orbit procedures together, we conducted a separate analysis to evaluate the correlation between these two procedure groups. Corneal/scleral lacerations were further divided into open and closed globe injuries based on whether full-thickness perforation was noted. Open globe injuries were divided into traditional repairs with suture versus with glue, as these are two separate skills that must be differentiated. CPT codes that were documented fewer than 0.2 times on average per resident as primary surgeon were grouped into the “other” category. Finally, all CPT codes labeled as cataract surgeries were additionally tabulated. This was done in order to validate the representativeness of our sample. We used an unpaired two-tailed t-test to compare the cataract surgery data between the residents in our study’s sample with that of the ACGME 2017–2018 case log reports of all US ophthalmology residents.
 |
Table 1 Categorization of Current Procedural Terminology (CPT) Codes from US Ophthalmology Residency Program Case Logs and their Descriptions |
Data were collected and analyzed using R version 4.0.2 (R Project, Vienna, Austria)11 for descriptive statistics, Student’s t-test, analysis of variance (ANOVA), and Tukey’s Honest Significant Difference (HSD) for post-hoc analysis. Results were considered significant at alpha < 0.05.
Results
ACGME national trends of ocular trauma cases can be found in Table 2, with graphical representations in Supplementary Tables 1-4. According to ACGME case log statistics, ocular trauma procedures accounted for 1.2% of all procedures logged by residents in 2017–2018.9 In this year, the average number of procedures logged as corneal/corneoscleral laceration/globe rupture was 7.9 ± 5 per resident, 0.4 ± 1 IOFB per resident, and 0.9 ± 1 procedures logged as “other globe trauma” per resident. The average number of total ocular trauma procedures was found to significantly decrease by 9% compared to those logged in 2009–2010 (average 10 ± 7 procedures per resident) (p = 0.0062). Similarly, procedures logged as “other globe trauma” performed by residents as primary surgeon in 2017–2018 was found to significantly decrease by 65.4% compared to those logged in 2009–2010 (2.6 ± 4) (p < 0.001). The average number of procedures logged as corneal/corneoscleral laceration/globe rupture in 2017–2018 was found to be significantly greater than those logged in 2009–2010 (2017–2018: 7.9 ± 5; 2009–2010: 7.2 ± 5) (p = 0.033), whereas the number of procedures logged as IOFB in 2017–2018 were not significantly different than the number logged in 2009–2010 (0.4 ± 1 for both years).
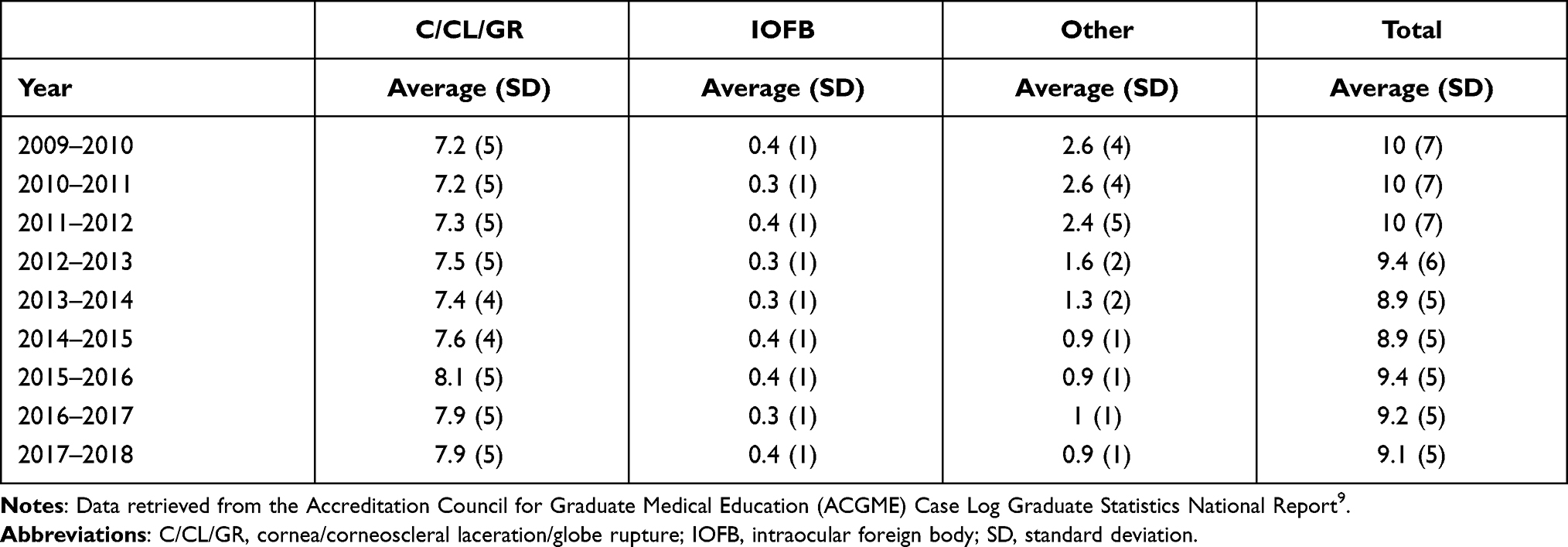 |
Table 2 Accreditation Council for Graduate Medical Education (ACGME) Surgeon Averages of All Globe Trauma Categories from 2009–2018 |
Out of 488 US ophthalmology residents graduating in 2018, a total of 166 (34%) provided case logs. These residents represented 38 (32.2%) of 118 ophthalmology residency programs. The majority of responding programs had between four to five residents (44.7% of programs), were located in the South (39.5%), and had a vitreoretinal surgery fellowship (78.9%). Half of the programs did not have an oculoplastic surgery fellowship (50%). The average number of residents per program was 4.81 ± 1.46, with a median of 4 (interquartile range 4–6). Specific program characteristics can be found in Table 3. No significant difference was found between ACGME primary surgeon cataract volume (198.1 ± 67) with that of our sample’s (206 ± 64), serving as a measure of representativeness of our sample compared to national case log statistics (p = 0.14).
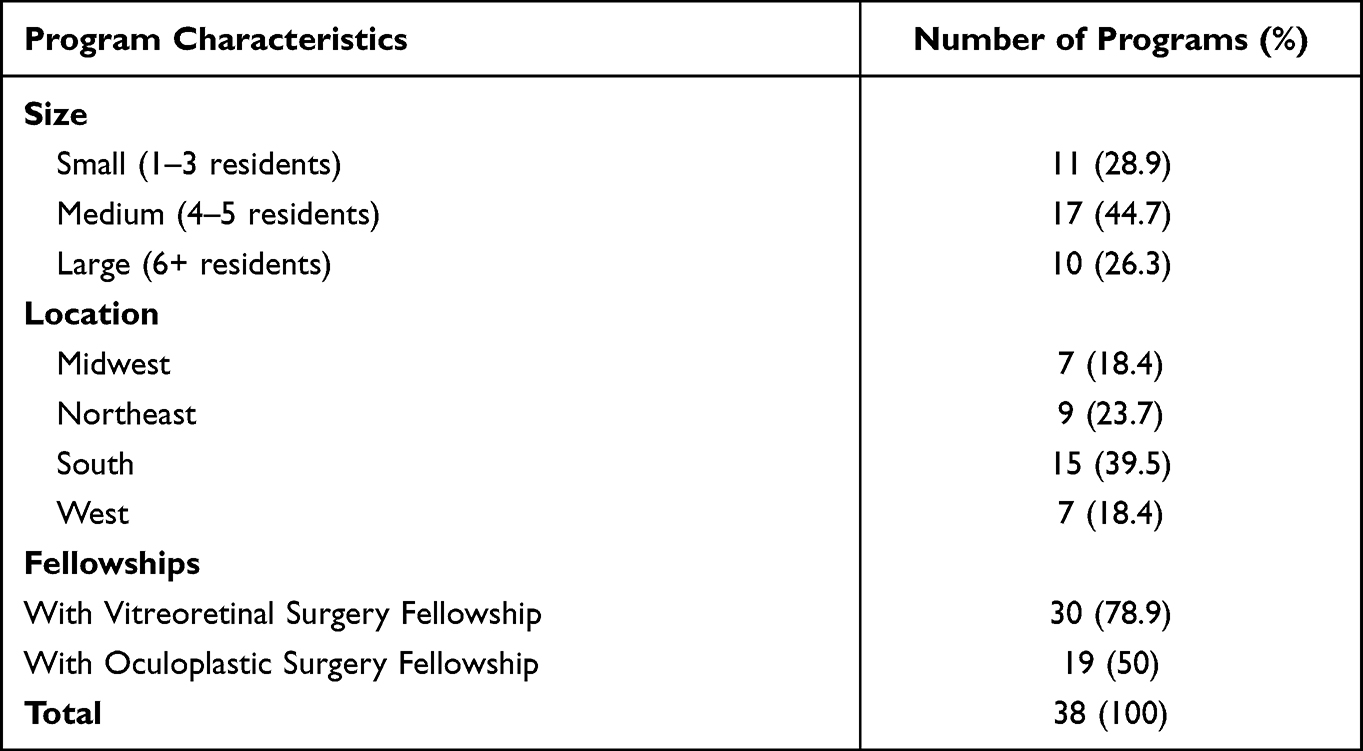 |
Table 3 Characteristics of 38 US Ophthalmology Residency Programs That Provided Case Logs for Residents Graduating in 2018 |
The average, standard deviation, minimum and maximum number of ophthalmic trauma procedures performed as primary surgeon are listed in Table 4. Residents performed an average of 9.0 ± 5.0 (minimum: 0; maximum: 29; median: 8) procedures that qualified for the ocular trauma case log requirement, and an average of 19.7 ± 11 (minimum: 6; maximum: 78; median: 18) procedures that included trauma-related oculoplastic and orbit procedures. 6 (3.6%) residents did not meet the requirement of four ocular trauma procedures, and 16 (9.6%) residents performed the bare minimum of four procedures. The most frequently logged procedures per resident (irrespective of role) were lid lacerations 9.9 ± 7.5, open globe repairs (8.1 ± 4.5), and orbital fractures (1.8 ± 3.1). The most common procedure logged as primary surgeon was lid laceration repair (8.7 ± 6.9) while the most logged procedure as assistant was orbital fracture repair (1.3 ±2.2). The least logged procedures (irrespective of role) were eyelid foreign body (0.16 ± 0.48), repair of iris (0.11 ± 0.41), and injection (0.06 ± 0.24). Presence of vitreoretinal surgery fellowship programs had no significant impact on the average number of IOFB procedures per resident (with fellowship: 0.31 ± 0.67 per resident; without fellowship: 0.41 ± 0.57, p = 0.37). Similarly, oculoplastic and orbit surgery fellowship programs did not have a significant impact on the average number of lid lacerations (with fellowship: 8.2 ± 6.3; without fellowship: 9.2 ± 7.6, p = 0.36) or orbital fractures (with fellowship: 0.66 ± 1.8; without fellowship: 0.31 ± 0.83, p = 0.10).
 |
Table 4 Summary of Number of Procedures Completed by Residents as Primary Surgeon Based on 2018 Case Logs Provided by 38 US Ophthalmology Residency Programs |
Table 5 lists the average number of each procedure type performed based on program size. The most commonly performed procedure across all programs, regardless of size, was lid laceration repair. The most commonly performed procedure in all programs except for those located in the West was also lid laceration repair, with open globe repair being more common in the West. Program size was found to significantly impact the average number of canthotomies and orbital fracture repairs performed by residents, with medium programs performing significantly more canthotomies than large programs (F(2166) = 6.35, p = 0.002), and large programs performing significantly more orbital fracture repairs than small and medium programs (F(2166) = 4.45, p = 0.013). Program location was not found to impact the average number of ophthalmic trauma procedures. The volume of procedures logged as ophthalmic trauma was strongly correlated with the volume of trauma-related oculoplastic and orbit procedures (r = 0.9, p < 0.001).
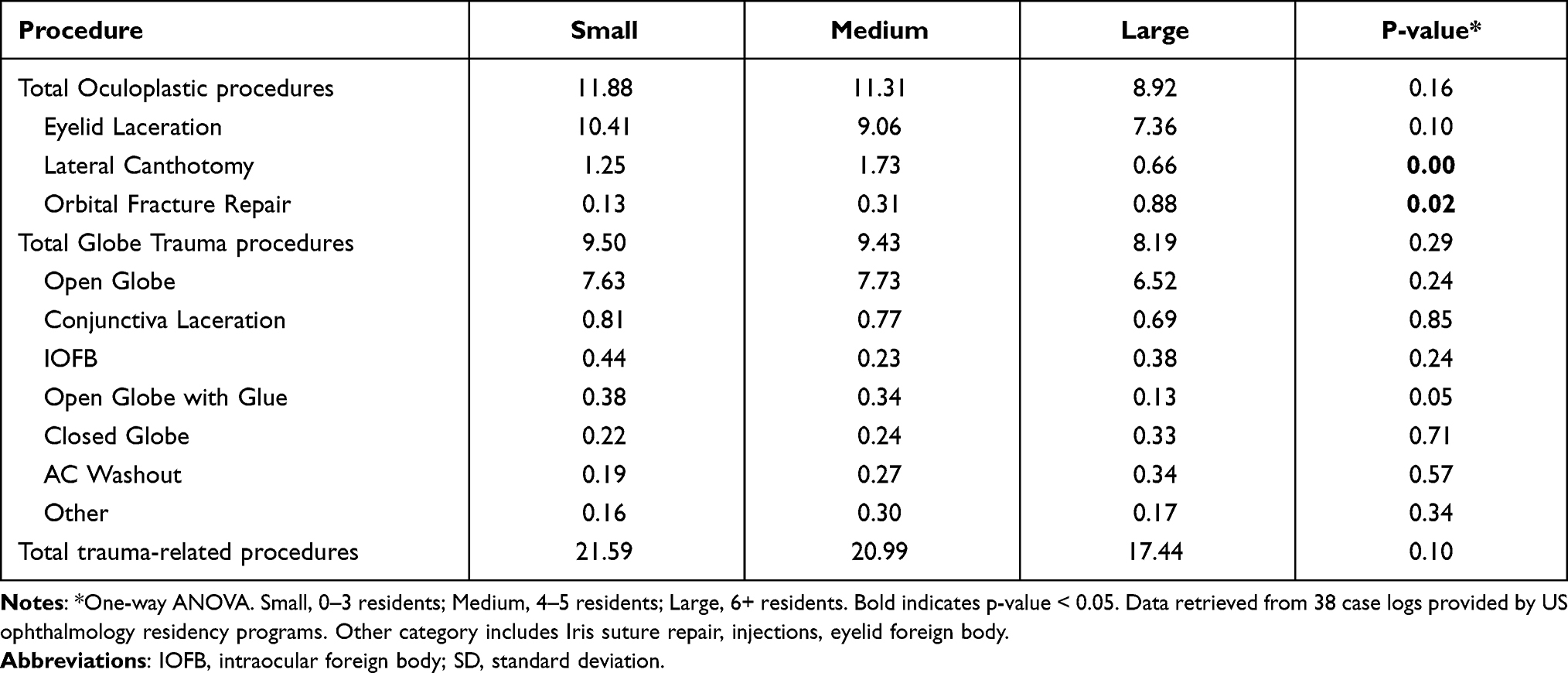 |
Table 5 Average Number of All Procedures as Primary Surgeon Based on Program Size |
Discussion
Three key findings are highlighted by the results of this study: (1) average ocular trauma cases per resident decreased between 2009–2018, (2) canthotomy and orbital fracture repair volume was dependent on program size, and (3) 6 residents graduated ophthalmology residency in 2018 without completing the required number of ocular trauma cases, and 16 performed only the minimum.
Our analysis of ACGME ocular trauma case log statistics between 2009–2018 demonstrated that there was an overall 9% decrease in average ocular trauma cases per resident. Prior studies of ophthalmic trauma epidemiology reflect this decreasing trend, though the magnitude of decrease varies.1,12,13 A cohort study evaluating pediatric ophthalmic trauma cases between 2006 and 2014 found a 26.1% decline in ophthalmic injuries among all the injury mechanisms recorded.12 Similarly, Iftikhar et al. analyzed ophthalmic trauma incidence between 2001 and 2014 and revealed that there was a 23.1% decrease in primary ophthalmic trauma during this time frame, where primary ophthalmic trauma was defined as the reason for admission to the hospital and the first diagnosis listed in the patient’s admission record. Orbital fracture was reported as the most common diagnosis in patients with primary ophthalmic trauma, while contusion of eye and adnexa was the most common in patients with secondary ophthalmic trauma.1 Ophthalmic trauma was considered secondary when it was not the principal diagnosis listed in the patient’s admission. Another study of ophthalmic trauma epidemiology by Morris et al. revealed a fourfold decrease in ophthalmic trauma cases between 1992 and 2009.13
The ACGME “other globe trauma” category similarly demonstrated a decrease in average cases between 2009 and 2018. Given the lack of detail regarding what procedures are included in this category, it is difficult to evaluate which procedures contributed to this decline. The ambiguity created by categories like “other globe trauma” must be recognized as a major limitation of using ACGME case log requirements as a way to measure resident surgical competency progress.
Decreases in ocular trauma are thought to be due to improved advocacy and safety measures taken over the past several years. The introduction of laws regulating the disclosure of potential hazards in products may partially explain this decrease in the pediatric population.12 Warning labels on products and child-proof packaging are additional measures that have been taken.12 Technologic advancements in imaging and changes in clinical practice for ocular trauma over time are further factors that could account for the decrease in ocular trauma cases.1 A possible explanation for the discordance in rates of ocular trauma case decrease per ACGME statistics is due to the discrepancies in defining cases as ocular trauma cases versus oculoplastic and orbit cases. Orbital fractures and lid lacerations, both frequently found in ophthalmic trauma diagnoses, are logged as oculoplastic and orbit procedures rather than “globe trauma”. These diagnoses, along with eyelid foreign body and canthotomy, were included in our in-depth analysis of ophthalmic trauma case logs for residents graduating in 2018. However, the ACGME views these cases (orbital fractures, lid lacerations, eyelid foreign body, and canthotomy) as separate from ocular trauma cases, which may explain the smaller decrease in ocular case volume over time in our study as compared with the literature.
Among our sample of US ophthalmology residents, the most performed ophthalmic trauma procedures on average as primary surgeon or assistant included lid laceration repairs, open globe repairs, and orbital fractures. “Other” procedures (eyelid foreign body, repair of iris, and injection), open globe repair with glue, and closed globe were least performed. Canthotomy and anterior chamber washouts were also infrequently logged in comparison to other procedures. Ocular trauma injuries, particularly blunt trauma, can lead to compartment syndrome of the orbit. Lateral canthotomy and cantholysis (LCC) is a rapid and simple procedure that can save a patient’s vision if performed correctly.14 However, 42.8% of residents did not perform a single LCC during their time in residency. Given every ophthalmology resident should be competent in performing this early on in residency, this may suggest the importance of simulation. Increasing opportunities for wet lab simulations may improve resident confidence in approaching ophthalmic trauma.15,16 The COVID-19 pandemic has had a considerable effect on resident surgical education given the decrease in surgical procedure volume and limits to the number of individuals in the operating room.17,18 Wet lab simulations, therefore, played an increasingly important role in resident surgical education during this time in order to compensate for the lost operating room time.18 Zafar et al. demonstrated that residents who participated in both supervised and unsupervised informal lab practice reported feeling more competent and prepared for surgical cases.15 Pantanelli et al. found that the implementation of a cataract surgery simulation course was correlated with a roughly 62% decrease in intraoperative posterior capsule tear incidence.19 Similarly, another study assessed differences in cataract surgery complication rates between residents that trained with the Eyesi simulator and residents who did not. Residents who participated in wet lab simulations had significantly lower rates of complications. Improvement in surgical skills after wet lab simulation is not limited to cataract surgery; Zhao et al. created a wet lab simulator for eyelid laceration repair and found that residents felt increased confidence in their laceration repair skills following simulator use.20 These studies all suggest that implementing surgical simulations into residency training curriculums may increase resident confidence in performing procedures that they otherwise would not be able to practice enough given the limited case exposure.
With regards to the relationship between program characteristics and case volume, program size was found to impact orbital fracture and canthotomy case volume. Large programs were found to perform significantly more orbital fracture repairs than both small- and medium-sized programs. Larger programs may have greater case volumes and a larger referral base, providing residents with more opportunities to encounter ophthalmic trauma. Medium programs were found to perform significantly more canthotomies than large programs. While larger programs may receive a more diverse array of cases, the cases must be distributed amongst a greater number of residents. Overall case load may not necessarily be in perfect correlation with program size, meaning that while larger programs may have more cases than medium programs, the difference may not be directly proportional to the difference in resident number. Furthermore, lateral cantholysis is not as common a procedure as orbital fracture or eyelid laceration repair, so there may be fewer cases regardless of program size to distribute among residents. These differences in case volume based on program size reflect the high variability in ophthalmic trauma exposure that may not be explained by one specific program characteristic. This calls attention to the need for a standardized approach to increasing ophthalmic trauma exposure and education in residency to ensure that all residents, regardless of their program, graduate with sufficient skills to manage these cases.
The residents in our sample performed an average of 19.7 trauma-related procedures. Of these procedures, an average of 9 procedures counted towards the ocular trauma case log requirement. However, 3.6% of residents did not meet the requirement, and 9.6% of residents met only the minimum of four procedures. While resident graduation is contingent on program directors’ evaluation of surgical competency, the fact that there are ophthalmology residents graduating without experience in crucial procedures raises great concern regarding physician preparedness in managing ocular trauma. For example, under current ACGME requirements, a resident may be able to graduate after fulfilling the ocular trauma case requirement with four AC washouts and no open globe repairs. Furthermore, according to ACGME case logs, ocular trauma cases accounted for only 1.2% of all recorded procedures by all residents graduating in 2017–2018. A survey in 2019 of United Kingdom ophthalmology residents revealed that 78% of trainees felt very low confidence in their abilities to perform ocular trauma procedures.21 In this same survey, residents reported that attending formal educational courses did not change their own perceived confidence in performing these procedures,21 emphasizing the necessity to increase resident exposure to these cases. This scarcity of ophthalmic trauma exposure is likely consistent across US ophthalmology residency programs, evidenced by the fact that program size and location were not found to impact the average number of procedures performed per resident per program for the majority of ophthalmic trauma procedures.
To address the limited ophthalmic trauma exposure in residency, reevaluation of the minimum number of ophthalmic trauma cases is required. With approximately 30–40% of monocular blindness caused by ocular trauma,2 it is essential each graduating resident is competent in critical procedures like open globe repair, hyphema washout and lateral canthotomies. Oculoplastic and orbit procedures have subcategories with their own required number of cases, including eyelid lacerations (3), chalazion excision (3), and ptosis/blepharoplasty (3). More specific classifications on ocular trauma may be beneficial. In particular, a requirement for a minimum number of open globe repairs may better prepare residents to handle one of the most devastating ocular conditions. Distinguishing open globe repairs from other less common ocular trauma procedures such as AC washout will further ensure that graduating residents first develop a strong foundational skillset for frequently encountered situations.
Another approach to this issue of limited ophthalmic trauma exposure in residency is to assess residents on surgical competency in addition to required case volume completion. Prior literature is conflicting regarding whether increased surgical volume correlates with improved surgical skill level,22,23 therefore it is difficult to conclude that increasing case log requirements will result in increased resident competency in these procedures. Furthermore, ACGME notes that achievement of procedure requirements does not necessarily imply competency in a skill, and that residents should continue to practice these skills far beyond case log requirements.6 However, increasing case log requirements while simultaneously using case logs as a guide for program directors to review individual residents’ surgical competencies may aid in addressing any skill- or competency-related issues residents may encounter.22
The limitations of this study warrant discussion. The small sample size limits the generalizability of our results to all residency programs. However, given the comparable cataract volume data, which is often used as a marker of residency program case volume, we believe our sample was similar to the national statistics. Secondly, residents may have made entry errors when logging their surgical procedures, thus altering case log accuracy. Finally, there is no guarantee that residents continued to log cases after reaching minimum volume requirements. Therefore, reported case logs may be an underrepresentation of true resident case exposure.
Conclusion
This analysis of US ophthalmology residency ocular trauma exposure between 2009–2018 and cross-sectional review of case logs of residents graduating in 2018 highlights the variability that exists not only in overall case volume exposure over time, but also the variability with specific procedure exposure among residents based on program size. Furthermore, the low number of required cases for globe trauma emphasizes the need to increase educational efforts towards this subspecialty.
Acknowledgments
The authors would like to thank the Wilmer Eye Institute for its support.
Disclosure
This work was supported by the NIH grant P30EY001765: Wilmer Biostats Core. Dr Fatemeh Rajaii is a consultant and shareholder for Horizon Therapeutics outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Iftikhar M, Latif A, Farid UZ, Usmani B, Canner JK, Shah SMA. Changes in the Incidence of Eye Trauma Hospitalizations in the United States From 2001 Through 2014. JAMA Ophthalmol. 2019;137(1):48. doi:10.1001/jamaophthalmol.2018.4685
2. Aghadoost D. Ocular Trauma: an Overview. Arch Trauma Res. 2014;3(2):432. doi:10.5812/atr.21639
3. Jmj R. Leading causes of blindness worldwide. Bull Soc Belge Ophtalmol. 2002;283:19–25.
4. Michels KS, Hansel MTEB, Choi MD, Andreas P, Lauer K. A Survey of Desired Skills to Acquire in Ophthalmology Training: a Descriptive Statistical Analysis. Ophthalmic Surgery Lasers Imaging Retina. 2007;38(2):107.
5. Arnold A. Developing the Educational Milestones for Ophthalmology. J Grad Med Educ. 2014;6(1 Suppl 1):144–145. doi:10.4300/JGME-06-01s1-37
6. ACGME. Institutional Requirements. Available from: https://www.acgme.org/Portals/0/PFAssets/InstitutionalRequirements/000InstitutionalRequirements2018.pdf?ver=2018-02-19-132236-600.
7. Shah VA, Reddy AK, Bonham AJ, Sabates NR, Lee AG. Resident surgical practice patterns for vitreoretinal surgery in ophthalmic training programs in the United States. Ophthalmology. 2009;116(4):783–789. doi:10.1016/j.ophtha.2008.11.010
8. Qiu M, Woreta FA, Boland MV. Microinvasive Glaucoma Surgery in US Ophthalmology Residency: surgical Case Log Cross-sectional Analysis and Proposal for New Glaucoma Procedure Classification. J Glaucoma. 2021;30(7):621–628. doi:10.1097/IJG.0000000000001846
9. ACGME - Accreditation Data System (ADS). Available from: https://apps.acgme.org/ads/Public/Reports/Report/25.
10. Sotomayor TM, Bailey MP, Dorton SL. Using Simulation to Address a Training Gap in Battlefield Ocular Trauma: a Lateral Canthotomy and Cantholysis (LCC) Prototype Training System. Mil Med. 2019;184(Suppl 1):335–341. doi:10.1093/milmed/usy285
11. Core Team R (2020). — European Environment Agency. Available from: https://www.eea.europa.eu/data-and-maps/indicators/oxygen-consuming-substances-in-rivers/r-development-core-team-2006.
12. Matsa E, Shi J, Wheeler KK, McCarthy T, McGregor ML, Leonard JC. Trends in US Emergency Department Visits for Pediatric Acute Ocular Injury. JAMA Ophthalmol. 2018;136(8):895–903. doi:10.1001/jamaophthalmol.2018.2062
13. Morris DS, Willis S, Minassian D, Foot B, Desai P, MacEwen CJ. The incidence of serious eye injury in Scotland: a prospective study. Eye. 2014;28(1):34–40. doi:10.1038/eye.2013.213
14. Amer E, El-Rahman Abbas A. Ocular Compartment Syndrome and Lateral Canthotomy Procedure. J Emerg Med. 2019;56(3):294–297. doi:10.1016/j.jemermed.2018.12.019
15. Zafar S, Chen X, Woreta F, Sikder S. Self-perceived preparedness and competence among ophthalmology residents for open globe repair. Clin Ophthalmol Auckl NZ. 2019;13:1273–1278. doi:10.2147/OPTH.S211144
16. Almaliotis D, Athanasopoulos GP, Almpanidou S, Papadopoulou EP, Karampatakis V. The contribution of wet labs in the education of ophthalmologists. Ann Med Surg. 2021;72:103034. doi:10.1016/j.amsu.2021.103034
17. Devaraj A, Satheesh AN, Panicker GJ, Kaliyaperumal S. Wetlab training during COVID-19 era; an ophthalmology resident’s perspective. Indian J Ophthalmol. 2021;69(1):158–159. doi:10.4103/ijo.IJO_3496_20
18. Hussain R, Singh B, Shah N, Jain S. Impact of COVID-19 on ophthalmic specialist training in the United Kingdom—the trainees’ perspective. Eye. 2020;2:1–4. doi:10.1038/s41433-020-1034-6
19. Pantanelli SM, Papachristou G, Callahan C, Chen M, Khalifa Y. Wet Lab-Based Cataract Surgery Training Curriculum for the PGY 2/PGY 3 Ophthalmology Resident. J Teach Learn Resour. 2018;14:10782. doi:10.15766/mep_2374-8265.10782
20. Zhao J, Ahmad M, Gower EW, Fu R, Woreta FA, Merbs SL. Evaluation and implementation of a mannequin-based surgical simulator for margin-involving eyelid laceration repair - a pilot study. BMC Med Educ. 2021;21(1):170. doi:10.1186/s12909-021-02600-3
21. Shirodkar A, Yeo DC, Shuttleworth MG. Trainee confidence managing ocular trauma. Eye. 2019;33(4):691–692. doi:10.1038/s41433-018-0328-4
22. Stride HP, George BC, Williams RG, et al. Relationship of procedural numbers with meaningful procedural autonomy in general surgery residents. Surgery. 2018;163(3):488–494. doi:10.1016/j.surg.2017.10.011
23. Randleman JB, Wolfe JD, Woodward M, Lynn MJ, Cherwek DH, Srivastava SK. The resident surgeon phacoemulsification learning curve. Arch Ophthalmol Chic. 2007;125(9):1215–1219. doi:10.1001/archopht.125.9.1215
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.