Back to Journals » Clinical Ophthalmology » Volume 20
Ophthalmic Implications of Ehlers-Danlos Syndrome
Authors Zhang KR ![]() , Zhang X, Xu K, Kojima J
, Zhang X, Xu K, Kojima J ![]() , Anderson BD
, Anderson BD ![]() , Dunaief JL, Armenti ST
, Dunaief JL, Armenti ST
Received 21 February 2026
Accepted for publication 17 May 2026
Published 26 June 2026 Volume 2026:20 600529
DOI https://doi.org/10.2147/OPTH.S600529
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Kevin R Zhang, Xumeng Zhang, Kasey Xu, Joe Kojima, Brandon D Anderson, Joshua L Dunaief, Stephen T Armenti
Department of Ophthalmology, Scheie Eye Institute, University of Pennsylvania, Philadelphia, PA, USA
Correspondence: Stephen T Armenti, Department of Ophthalmology, Scheie Eye Institute, University of Pennsylvania, 51 N. 39 th Street, Philadelphia, PA, 19104, USA, Email [email protected]
Purpose: Ehlers-Danlos syndrome (EDS) is a group of inherited connective tissue disorders with systemic manifestations, but its ophthalmic implications are poorly characterized. Existing studies suggest an increased prevalence of many ophthalmic conditions as well as a higher rate of surgical complications, but a comprehensive understanding is lacking.
Methods: An anonymous survey was distributed online through social media and patient advocacy organizations. Participants reported genetic and ophthalmic diagnoses, year of diagnosis, refractive error, and ophthalmic surgical history. Analyses focused on individuals with hypermobile, vascular, and classical EDS.
Results: A total of 766 completed surveys were analyzed. Most respondents (83.3%) had hypermobile EDS. Dry eye, strabismus, amblyopia, blue sclera, and several other eye conditions were common and more prevalent compared to population estimates. Myopia was the most prevalent condition, with high myopia reported by approximately 40% of respondents, exceeding population estimates of 20– 30%. Several conditions, including glaucoma, posterior vitreous detachment, and retinal tear/detachment, presented at younger ages than expected. Ophthalmic surgeries were overall well tolerated, although persistent postoperative pain was frequently reported.
Conclusion: EDS may be associated with an increased risk and earlier onset of many ophthalmic conditions. Several of these conditions, including glaucoma and retinal tear/detachment, could lead to significant morbidity if not detected and managed early. Ophthalmic procedures are well tolerated, but persistent pain is common. Enhanced screening and tailored surgical management could improve quality of life in individuals with EDS.
Keywords: Ehlers-Danlos syndrome, epidemiology, surgical outcomes
Introduction
Ehlers-Danlos syndrome (EDS) is a set of 13 inherited connective tissue disorders characterized by stretchy skin, joint hypermobility, dysfunctional wound healing, and easy bruising.1 Twelve of the subtypes have known causative genetic mutations, but hypermobile EDS, the most common subtype, lacks a defined molecular cause and is diagnosed instead by clinical criteria.
Ophthalmic associations of EDS have been described as early as the 1950s, including by Peter Beighton,2 who developed the Beighton criteria that is currently crucial in the diagnosis of hypermobile EDS. Under a former classification of EDS devised in 1986 (the Berlin nosology), EDS type VI was specifically noted to have cardinal ocular involvement with microcornea, scleral perforation, and retinal detachment, and was called the ocular-scoliotic type of EDS.3 In subsequent revisions of EDS classification, EDS type VI was divided into kyphoscoliotic EDS and brittle cornea syndrome.1 While the current definition of kyphoscoliotic EDS (mutations in PLOD1 or FKBP14) still includes ocular manifestations such as blue sclera and refractive errors as minor diagnostic criteria, brittle cornea syndrome (mutation in ZNF469) has primary ophthalmic phenotypes, with major criteria including thin cornea, early onset keratoconus and keratoglobus, and blue sclera.1 Beyond these well-documented ophthalmic manifestations, many of the other EDS subtypes have been found to present in the eyes, but the ophthalmic manifestations of EDS are overall still poorly characterized despite the considerable visual and psychosocial morbidity they can cause.
Although case reports have described ophthalmic phenotypes of EDS, broader studies remain limited. Asanad et al comprehensively reviewed studies examining ocular findings across EDS subtypes, identifying associations ranging from common problems like myopia and ptosis to rarer conditions like blue sclera and retinal tears, although most studies were limited to case studies or small cohorts.4 Recently, Kim et al analyzed electronic health record (EHR) data from over 70,000 EDS patients and found that 40% of ocular diagnoses were more prevalent in EDS patients compared to the general population, including myopia, dry eye, and angioid streaks, while there were reduced odds of diabetic retinopathy and age-related macular degeneration.5 However, EHR-based analyses rely on accurate coding and lack EDS subtype stratification. Beyond these two studies, there are no other comprehensive evaluations of ophthalmic disease patterns in EDS.
Given the role of connective tissue integrity in wound healing, individuals with EDS have higher complication rates across multiple surgical disciplines.6,7 Ophthalmic surgical outcomes in EDS have been minimally studied. Louie et al conducted a survey-based study of 467 individuals with EDS, 112 of whom had an ophthalmic procedure.8 They reported high complication rates for a variety of procedures, suggesting that surgical procedures may require modification in this population.
To improve understanding of the ophthalmic implications of EDS, we conducted a large, survey-based study assessing ophthalmic diagnoses, age at diagnosis, and surgical outcomes in individuals with EDS. By leveraging patient-reported data, we aimed to characterize disease prevalence, identify patterns of early onset, and provide insight into surgical outcomes to inform clinical management and guide future research toward optimizing ophthalmic care for individuals with EDS.
Materials and Methods
Study Design
This was a cross-sectional, online, survey-based study. The study was approved by the University of Pennsylvania Institutional Review Board as exempt research (IRB Protocol #856383). All methods were conducted in accordance with the Declaration of Helsinki and the Health Insurance Portability and Accountability Act (HIPAA). Individuals aged 13 or older provided consent electronically; parents or guardians provided assent for children aged 6–12 years. No individuals younger than 6 years were included.
All data were collected anonymously. Participants could exit the survey at any time and were given a return code to continue their responses. Questions dealt with demographics, connective tissue diagnosis (Marfan syndrome, Ehlers-Danlos syndrome, or none of those two), smoking history, ophthalmic diagnoses and year of diagnosis, refractive error, and ophthalmic surgical history. Participants also had the option to upload retinal imaging.
Source Population
The survey was distributed through EDS and Marfan syndrome focused Facebook groups and nonprofit organizations, including the Ehlers-Danlos Society, EDS Canada Foundation, Ehlers-Danlos Australia, and the Marfan Foundation. Responses were collected from July 10, 2024, through October 6, 2025.
Data Analysis
Only completed surveys from individuals reporting EDS were analyzed. To reduce misclassification, participants chose diagnoses from a list of radio buttons instead of typing free-text responses. To mitigate recall bias, age at diagnosis was calculated using reported birth year and diagnosis year.
Because respondents could have undergone a wide range of ophthalmic procedures, information on surgical history was collected as free text. Responses were manually reviewed to accommodate variable terminology. Participants reporting multiple ophthalmic procedures were excluded from analyses for satisfaction, ongoing pain, and willingness to repeat the surgery due to ambiguity regarding procedure-specific outcomes.
All analyses were performed using R.
Results
A total of 766 completed survey responses were received from individuals reporting a diagnosis of Ehlers-Danlos syndrome. Most respondents were White and female (Supplemental Table 1). The majority (638; 83.3%) of respondents had hypermobile EDS. All EDS subtypes except for dermatosparaxis, musculocontractural, and periodontal EDS were represented (Figure 1A). Analyses of ophthalmic conditions focused on hypermobile, vascular, and classical EDS, the three most common subtypes globally,9 with median ages being 39, 38, and 39 years, respectively (Figure 1B).
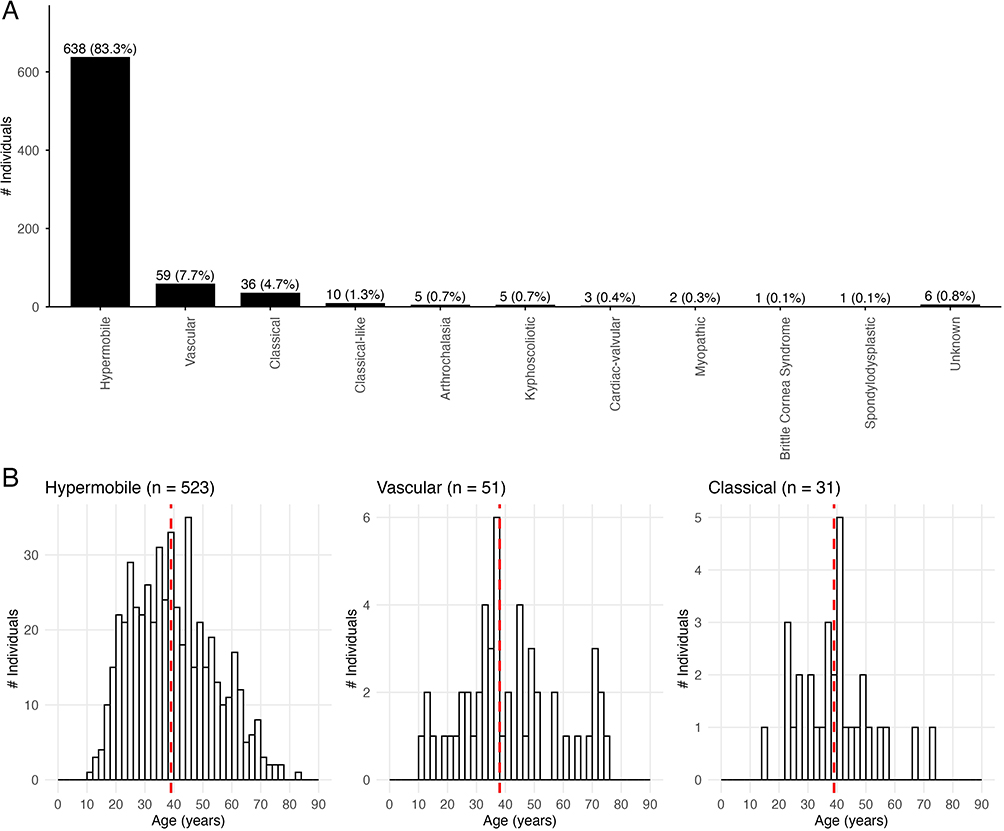 |
Figure 1 EDS subtypes and ages of survey respondents. (A). EDS subtypes reported by survey respondents. Subtypes with no respondents are not represented. (B). Age distribution for the three major EDS subtypes examined in this study. The red line represents the median age. |
Figure 2 illustrates the prevalence of ophthalmic conditions, ordered by prevalence in all 766 survey respondents. Myopia was the most common diagnosis, reported by 63% of respondents with hypermobile EDS. Other common conditions included dry eye, hyperopia, and double vision. Blue sclera, an uncommon condition typically associated with osteogenesis imperfecta, was prevalent in all three major EDS subtypes. Conversely, angioid streaks, historically associated with EDS, were rare, though this may be underestimated given the self-reported nature of the survey. Keratoconus and retinal tears were more prevalent in classical EDS. Ophthalmic conditions reported by respondents with less common EDS subtypes are detailed in Supplemental Table 2.
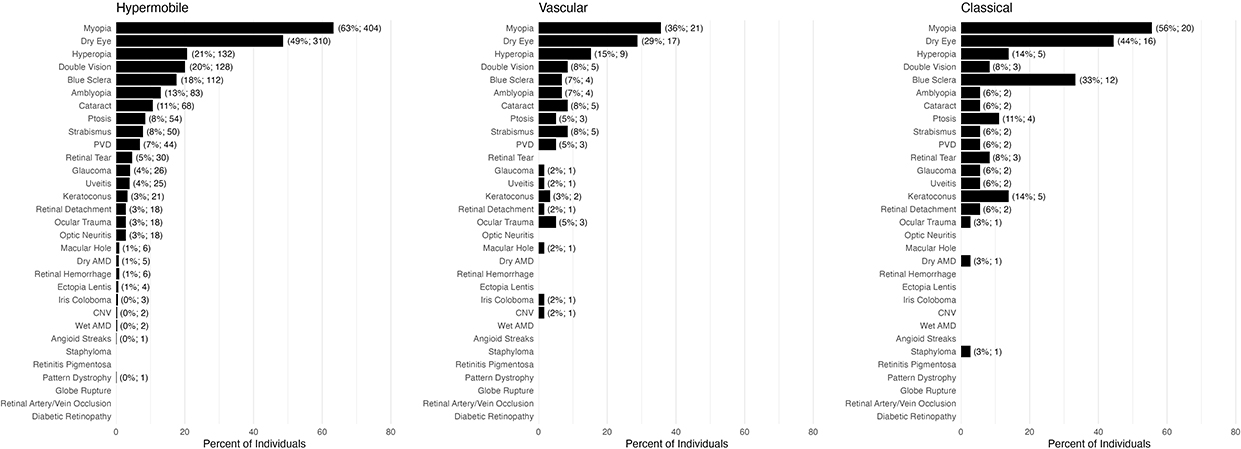 |
Figure 2 Prevalence of ophthalmic conditions reported by survey respondents. Conditions are arranged by order of prevalence in all subtypes combined. Numbers in parentheses represent percent and total number of respondents with the condition. |
To examine whether EDS may lead to earlier onset of ophthalmic disease, survey respondents were asked to input their birth year and the year of diagnosis for each ophthalmic condition, from which age at diagnosis was calculated. Figure 3 illustrates the age at diagnosis for all ophthalmic conditions in individuals with hypermobile EDS for which there were at least 10 responses. Data for ophthalmic conditions in individuals with hypermobile EDS with fewer than 10 respondents is shown in Supplemental Figure 1 and was not analyzed given the low number of responses. Supplemental Figures 2 and 3 show ages at diagnosis in individuals with vascular and classical EDS, respectively.
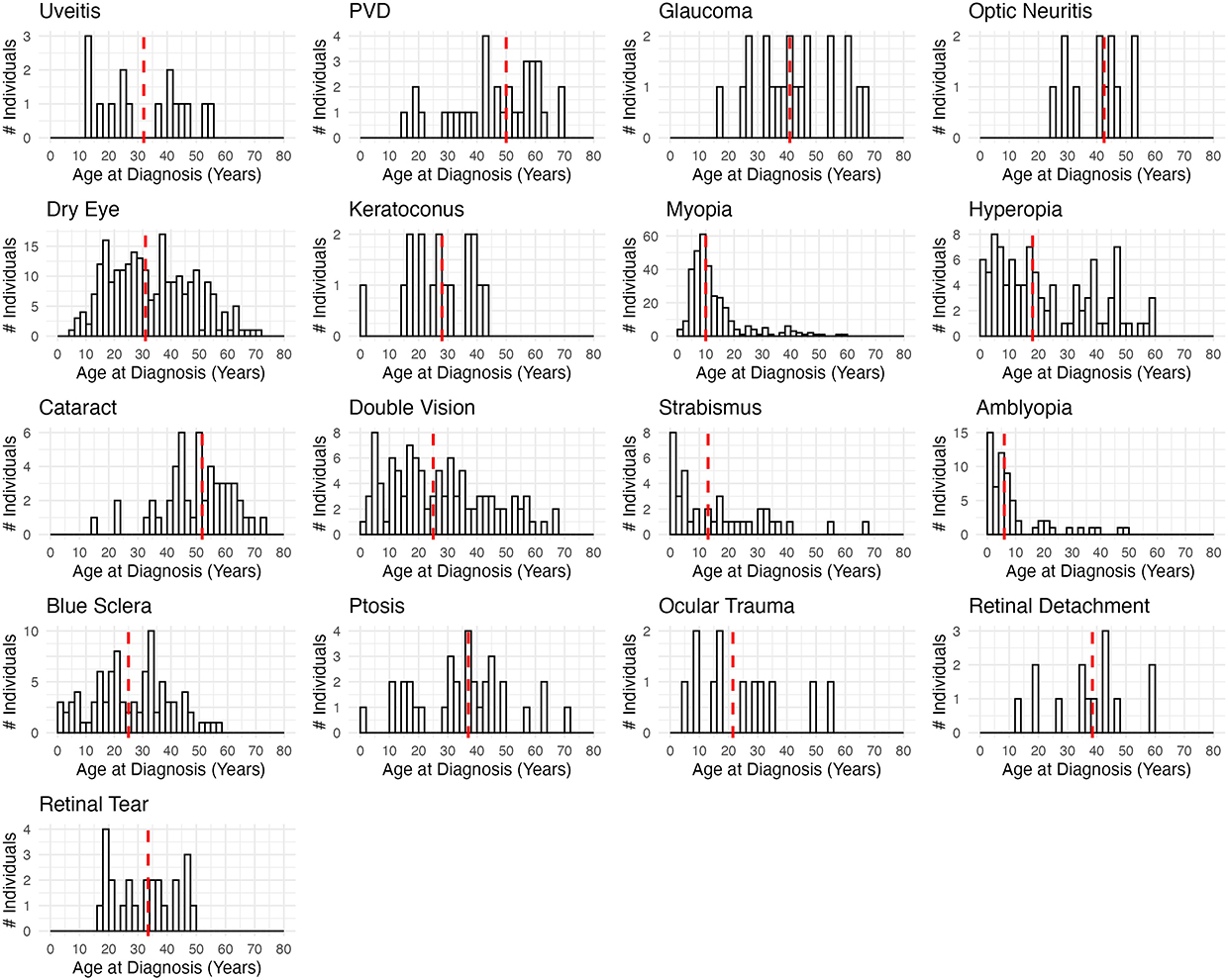 |
Figure 3 Age of onset of ophthalmic conditions in individuals with hypermobile EDS. The red line represents the median age. |
Given the high prevalence of refractive errors in individuals with EDS, and to assess whether EDS may be associated with stronger glasses prescriptions, survey respondents were asked about their prescriptions. Respondents must have checked the binary myopia or hyperopia options on the survey for their prescription to be analyzed. Data from both eyes were combined (Figure 4). Myopia was defined as having a prescription ≤−0.5 diopters, and high myopia was defined as having a prescription ≤−5 diopters.10 Hyperopia was defined as having a prescription >0.5 diopters.11 Further analysis showed that 193/478 (40.4%), 11/27 (40.7%), and 8/22 (36.4%) of eyes in individuals with hypermobile, vascular, and classical EDS qualified as being highly myopic.
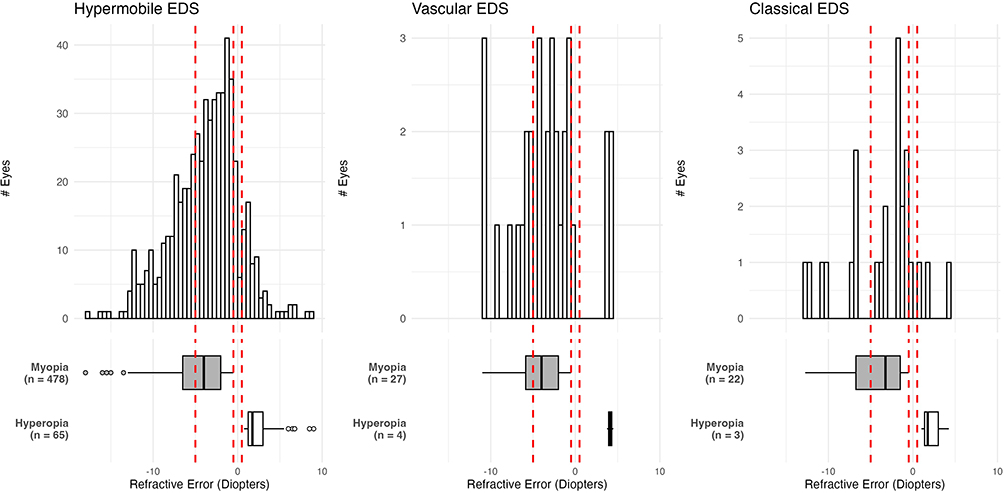 |
Figure 4 Refractive error for individuals reporting a diagnosis of myopia or hyperopia. From left to right, the red lines represent diopter cutoffs for high myopia (≤−5 diopters), myopia (≤−0.5 diopters), and hyperopia (>0.5 diopters). |
Previous studies have suggested that EDS is associated with higher rates of surgical complications. Survey participants indicated any previous ophthalmic procedures through free text, reporting also their satisfaction with the procedure, presence of ongoing pain, and willingness to undergo the procedure again if necessary. Given the diversity of answers, responses were manually analyzed. The most common procedures were blepharoplasty, cataract surgery, corneal crosslinking, laser photocoagulation, LASIK, and strabismus surgery. Satisfaction was generally high (Figure 5A), although persistent postoperative pain was common (Figure 5B). Most respondents indicated willingness to undergo surgery again if needed (Figure 5C).
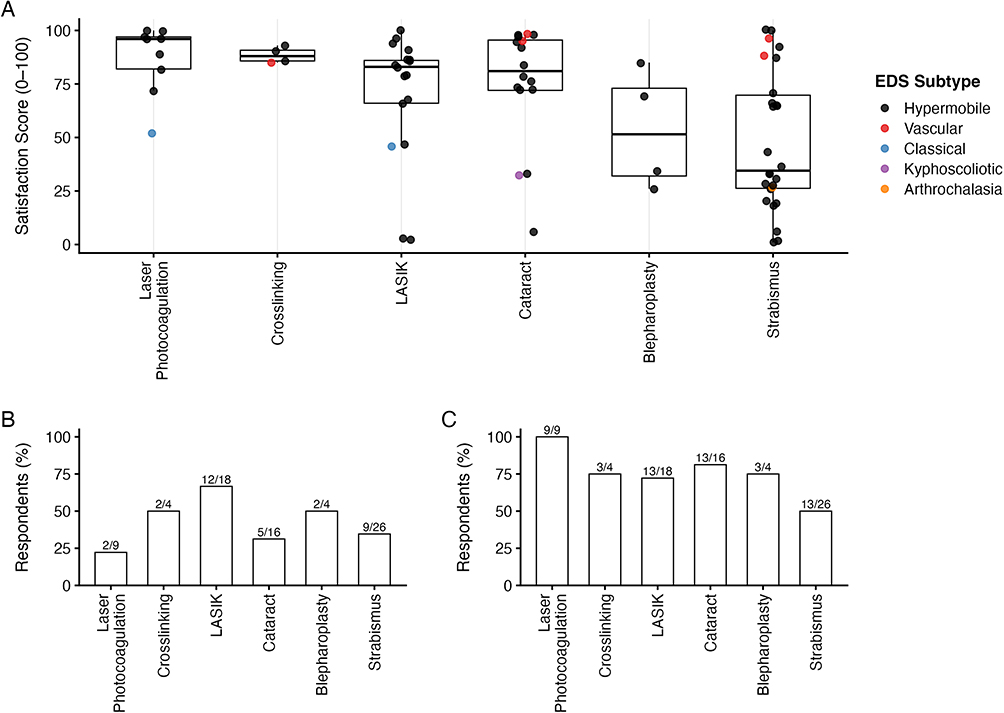 |
Figure 5 Surgical outcomes for the six most common ophthalmic procedures. (A) Satisfaction scores for each procedure, with individual data points colored by EDS subtype. (B). Fraction and percent of respondents reporting ongoing pain after their procedure. (C) Fraction and percent of respondents indicating that they would be willing to get the procedure again if necessary. |
Survey respondents indicated any surgical complications through free text, which was also manually analyzed. Of the 26 respondents who underwent strabismus surgery only, 13 (50%) reported that their strabismus/diplopia was either not fully corrected, overcorrected, or returned after a short period of time. Other complications included loss of stereopsis, scarring, and pain. Blepharoplasty was reported by only four individuals, but satisfaction scores ranged widely, and complications included double vision and relapse of ptosis with scarring. Corneal crosslinking was also only reported by four individuals, and while half reported ongoing pain and one reported that they were unwilling to get the procedure again, there were no complications noted. Cataract surgery was well tolerated, and few respondents noted complications, although 2/16 respondents said they began experiencing dry eyes after the surgery and one respondent said their sight overall worsened. Laser photocoagulation was also well-tolerated, although one individual reported conjunctival hemorrhaging and another indicated ongoing visual disturbances almost a year after the procedure; in the latter situation, it is unclear whether the underlying retinal tear or the procedure caused these visual changes. LASIK was the last procedure reported by at least four participants and was also relatively well tolerated, although 6/18 respondents reported dry eyes after the procedure, one reported photophobia, and another indicated difficulty with night vision with glare.
Discussion
This survey-based study characterizes ophthalmic disease patterns and surgical outcomes in individuals with EDS. Limited awareness of these manifestations may delay diagnosis and management, contributing to morbidity in a medically complex patient population that frequently experiences diagnostic uncertainty and dismissal by clinicians.12,13
Prevalence and Age of Onset
Our study population was 94.4% female and 91.0% White, with most individuals having hypermobile EDS. Although highly skewed at first glance, this strong female predominance mirrors previous studies.14,15 The reasons for the racial skew are less apparent, and both socioeconomic and access-related factors may be responsible for the potential overrepresentation of White individuals in our study.16
Several conditions appeared at younger ages in respondents with hypermobile EDS (Figure 3). Glaucoma was reported by 4% of individuals with hypermobile EDS, with a median onset of 41 years. In contrast, population prevalence is only 0.08–0.2% under age 40 but rises to 7.75% over age 80.17 Kim et al likewise found higher glaucoma prevalence in younger (≤60 years) but not older age groups.5 Although the US Preventive Services Task Force (USPSTF) recommends against routine population screening, our results suggest that individuals with hypermobile EDS may represent a unique population for which early screening may be warranted.
Posterior vitreous detachment (PVD), retinal detachment, and retinal tear also presented at younger ages. Median ages of onset were 50, 38.5, and 33.5 years, respectively, compared to mean ages of 67.8, 59.5, and 58.4 years in a large general-population study.18 Earlier onset of retinal tear and detachment in individuals with EDS is consistent with previous studies.5,8 EDS may predispose to premature vitreoretinal degeneration, underscoring the need for vigilance when evaluating patients with concerning visual symptoms, even if they are young.
Many ophthalmic conditions were more prevalent in our EDS population compared to the general population. Dry eye was reported by 49% of individuals with hypermobile EDS, 29% with vascular EDS, and 44% with classical EDS. These are substantially higher than general population estimates of 6.8% to 8.1%.19,20 This high prevalence, also observed by Gharbiya et al21 and Kim et al,5 was accompanied by earlier onset. Whereas dry eye typically develops after age 50,19 the median ages of onset were 31, 38.5, and 41 years for hypermobile, vascular, and classical EDS, respectively. Early adoption of artificial tears or warm compresses could be beneficial.
Strabismus and amblyopia were also more common in EDS. Strabismus was reported by 8% of respondents with hypermobile and vascular EDS, and 6% with classical EDS. This is higher than population estimates of 2–4%.22–24 Amblyopia, with a global prevalence of 1–2%,25,26 was reported by 13%, 7%, and 6% of individuals with hypermobile, vascular, and classical EDS, respectively. High amblyopia prevalence may be secondary to the higher rates of strabismus and refractive errors observed in EDS. However, in hypermobile EDS, the median age of onset for amblyopia (6 years) preceded that for strabismus (13 years), suggesting other factors may contribute. These findings support early ophthalmic screening in children with EDS or a relevant family history.
Blue sclera, which is classically associated with osteogenesis imperfecta but is also a feature of over 60 other genetic syndromes, arises from collagen-related scleral thinning and uveal show.27 Though rare, with a <1% prevalence, it has been described in several EDS subtypes and is a minor criterion for kyphoscoliotic EDS.4 Notably, 18% of respondents with hypermobile EDS, 7% with vascular EDS, and 33% with classical EDS reported blue sclera. This unexpectedly high rate suggests broader connective tissue involvement, but overreporting is also possible given the visible and self-diagnosable nature of blue sclera.
Classical EDS had a strikingly high prevalence of keratoconus (14%), compared to only 3% in hypermobile and vascular EDS. Because this condition is presumably less familiar to patients, reporting bias is likely minimal. The low global prevalence of keratoconus (0.12% to 4.79%)28 makes the rate in classical EDS particularly notable. The causative COL5A1 and COL5A2 mutations of classical EDS are known to produce abnormal corneal curvature and thinning,29 and evidence has directly linked COL5A1 variants to keratoconus.30 Given the high prevalence of keratoconus, patients with EDS and frequent eyeglass prescription changes may warrant thorough corneal evaluation.
Myopia was the most prevalent condition overall, reported by 63% of individuals with hypermobile EDS, 36% with vascular EDS, and 56% with classical EDS. Global estimates of myopia prevalence generally range between 20% and 30%.10,31 Among individuals who reported their prescriptions, high myopia (≤−5.00 diopters) occurred in about 40% of cases in all three EDS subtypes (Figure 4), much higher than the global estimate of 12%.10 These elevated myopia prevalences align with previous reports,4,5 potentially reflecting abnormal scleral or corneal extracellular matrix32 leading to axial elongation and corneal refractive aberration. Conversely, hyperopia was less frequent among those with EDS (21% in hypermobile EDS, 15% in vascular EDS, and 14% in classical EDS) compared to the global average of about 30%,11 suggesting the same tendency towards axial elongation rather than shortening. Given the retinal risks associated with high myopia, proactive counseling and close monitoring may be beneficial and prevent significant morbidity.
Understanding the mechanism underlying these ophthalmic associations in EDS could facilitate the development of targeted therapies. While connective tissue laxity and extracellular matrix abnormalities likely contribute to many findings, and has previously been documented for myopia and dry eye,5 this explanation alone may be incomplete. EDS is associated with systemic features that could influence ophthalmic physiology. For example, autonomic dysfunction and increased sympathetic activity, both described in EDS,33 may contribute to dry eye alongside abnormalities in the lacrimal gland extracellular matrix21 and corneal collagen.5 Additionally, variants in KLK15 and other kallikrein genes have recently been associated with hypermobile EDS.34 Although their ocular roles in EDS have not yet been investigated, kallikreins are expressed in multiple ocular tissues and may regulate retinal blood flow and aqueous humor dynamics.35 More broadly, EDS has been linked to variants in hundreds of genes spanning diverse biological pathways, including platelet adhesion, ion transport, and immune regulation, suggesting that multiple mechanisms likely contribute to the spectrum of ophthalmic manifestations.36
Surgical Outcomes
Surgical outcome analysis focused on general characteristics such as satisfaction, ongoing pain, and willingness to repeat the procedure, given the wide range of procedures reported. Satisfaction was generally high (Figure 5A), though persistent pain was common (Figure 5B). Most ophthalmic procedures were well tolerated, but our results suggest that the possibility for persistent pain should be mentioned during risk-benefit discussions prior to procedures.
Strabismus surgery stood out for lower satisfaction. This is consistent with Louie et al, who reported a 58.8% complication rate.8 Many of our respondents noted postoperative relapse. While overall surgical success for strabismus ranges from 50% to 80%,37–39 our findings suggest slightly worse outcomes in EDS, warranting further study to optimize techniques and reduce recurrence.
In contrast, LASIK outcomes were unexpectedly favorable, with over 70% of respondents saying they would undergo the procedure again. Although the FDA lists EDS as a contraindication due to theoretical increased complication risks, prior reports40 and our data indicate that outcomes are often favorable. There were few complications aside from dry eye, which is a known complication.41 No one reported postoperative corneal ectasia, perhaps the most serious complication of LASIK,42 although one individual noted severe night glare. LASIK may thus be feasible in select, carefully screened patients.
Strengths and Limitations
Distributing the survey through social media and nonprofit foundations enabled collection of a large sample size for this rare connective tissue disorder and included individuals who might be underrepresented in clinic-based studies due to mobility limitations. While database and EHR studies offer huge sample sizes, they rely on provider coding accuracy and often lack EDS subtype information,5 timing of diagnoses, or patient-reported outcomes. In contrast, by capturing user-reported outcomes, our survey was able to measure subjective outcomes such as surgical satisfaction and pain, which are seldom available in EHR analyses yet are critical measures of surgical success.
As an anonymous, self-reported survey, this study has several limitations. Anonymity prevented verification of demographics, diagnoses, and procedures, and may have allowed duplicate responses. Inclusion of only completed surveys may have biased results toward more symptomatic or motivated individuals. Although radio-button formats minimized misclassification, self-diagnosis and recall bias remained possible, especially for visible or familiar conditions such as blue sclera. We attempted to reduce recall bias by requesting the year rather than age of diagnosis. Selection bias may also have occurred through recruitment in patient advocacy groups. Due to the design of the survey, data from individuals reporting multiple types of ophthalmic procedures could not be analyzed, possibly underestimating true complication rates by dropping data from more medically complex patients.
Because sample sizes for individual EDS subtypes and age groups were limited, we did not stratify prevalence estimates by age. This restricts direct comparison with literature focused on specific age ranges. The small number of respondents with vascular or classical EDS further precluded our ability to perform age of onset analyses. Given a mean respondent age of 40.8 years, our data may also overestimate conditions that develop early (eg. myopia, hyperopia, strabismus, amblyopia, and blue sclera) and underestimate age-related diseases (eg. cataract, PVD, retinal detachment, and retinal tear). The young age of our cohort may be an artifact of using social media to distribute the survey. Nevertheless, integrating prevalence with age-at-diagnosis distributions (Figure 3 and Supplemental Figures 1–3) provides a useful overview of how ophthalmic disease differs in EDS.
Conclusion
Individuals with EDS experienced higher prevalence and earlier onset of several ophthalmic conditions, including glaucoma, posterior vitreous detachment, and retinal tears/detachment, which may appropriately increase clinical suspicion for these highly morbid conditions. Most ophthalmic procedures were well tolerated, although persistent pain was common. These findings support a role for comprehensive ophthalmologic evaluation following EDS diagnosis. Future studies should use verifiable clinical methods to clarify associations and determine the pathophysiologic basis for these ophthalmic associations.
Funding
This research was supported by an unrestricted grant to the University of Pennsylvania from Research to Prevent Blindness.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Malfait F, Francomano C, Byers P, et al. The 2017 international classification of the Ehlers–Danlos syndromes. Am J Med Genetics Part C. 2017;175(1):8–11. doi:10.1002/ajmg.c.31552
2. Beighton P. Serious ophthalmological complications in the Ehlers-Danlos syndrome. Br J Ophthalmol. 1970;54(4):263–268. doi:10.1136/bjo.54.4.263
3. Beighton P, de Paepe A, Danks D, et al. International nosology of heritable disorders of connective tissue, Berlin, 1986. Am J Med Genet. 1988;29(3):581–594. doi:10.1002/ajmg.1320290316
4. Asanad S, Bayomi M, Brown D, et al. Ehlers-Danlos syndromes and their manifestations in the visual system. Front Med. 2022;9:996458. doi:10.3389/fmed.2022.996458
5. Kim SB, Shaia JK, Kaelber DC, Singh RP, Talcott KE. Ocular manifestations in Ehlers-Danlos syndrome. Eye. 2025;39(10):1990–1997. doi:10.1038/s41433-025-03787-1
6. Yonko EA, LoTurco HM, Carter EM, Raggio CL. Orthopedic considerations and surgical outcomes in Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2021;187(4):458–465. doi:10.1002/ajmg.c.31958
7. Burcharth J, Rosenberg J. Gastrointestinal surgery and related complications in patients with Ehlers-Danlos syndrome: a systematic review. Digestive Surg. 2012;29(4):349–357. doi:10.1159/000343738
8. Louie A, Meyerle C, Francomano C, et al. Survey of Ehlers‒Danlos Patients’ ophthalmic surgery experiences. Mol Genet Genomic Med. 2020;8(4):e1155. doi:10.1002/mgg3.1155
9. Malfait F, De Paepe A. The Ehlers-Danlos Syndrome. In: Halper J, editor. Progress in Heritable Soft Connective Tissue Diseases. Dordrecht: Springer Netherlands; 2014:129–143. doi:10.1007/978-94-007-7893-1_9
10. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
11. Hashemi H, Fotouhi A, Yekta A, Pakzad R, Ostadimoghaddam H, Khabazkhoob M. Global and regional estimates of prevalence of refractive errors: systematic review and meta-analysis. J Curr Ophthalmol. 2017;30(1):3–22. doi:10.1016/j.joco.2017.08.009
12. Locke JD, Eastman JT. Navigating the psychosocial landscape of Ehlers–Danlos syndrome: an autobiographic case study. Discov Ment Health. 2025;5(1):123. doi:10.1007/s44192-025-00268-5
13. Wagner W, Doyle TA, Francomano CA, Knight DRT, Halverson CME. Patient interest in the development of a center for Ehlers-Danlos syndrome/hypermobility spectrum disorder in the Chicagoland region. Orphanet J Rare Dis. 2024;19(1):122. doi:10.1186/s13023-024-03109-w
14. Petrucci T, Barclay SJ, Gensemer C, et al. Phenotypic clusters and multimorbidity in hypermobile Ehlers-Danlos syndrome. Mayo Clin Proc. 2024;8(3):253–262. doi:10.1016/j.mayocpiqo.2024.04.001
15. Castori M, Camerota F, Celletti C, et al. Natural history and manifestations of the hypermobility type Ehlers-Danlos syndrome: a pilot study on 21 patients. Am J Med Genet A. 2010;152A(3):556–564. doi:10.1002/ajmg.a.33231
16. Glayzer JE, Bray BC, Kobak WH, Steffen AD, Schlaeger JM. Lack of diversity in research on females with ehlers-danlos syndromes: recruitment protocol for a quantitative online survey. JMIR Res Protoc. 2024;13:e53646. doi:10.2196/53646
17. Ehrlich JR, Burke-Conte Z, Wittenborn JS, et al. Prevalence of glaucoma among US adults in 2022. JAMA Ophthalmol. 2024;142(11):1046–1053. doi:10.1001/jamaophthalmol.2024.3884
18. Saraf SS, Lacy M, Hunt MS, Lee CS, Lee AY, Chee YE. Demographics and seasonality of retinal detachment, retinal breaks, and posterior vitreous detachment from the intelligent research in sight registry. Ophthalmol Sci. 2022;2(2):100145. doi:10.1016/j.xops.2022.100145
19. Farrand KF, Fridman M, Stillman IÖ, Schaumberg DA. Prevalence of diagnosed dry eye disease in the United States among adults aged 18 years and older. Am J Ophthalmol. 2017;182:90–98. doi:10.1016/j.ajo.2017.06.033
20. McCann P, Abraham AG, Mukhopadhyay A, et al. Prevalence and incidence of dry eye and meibomian gland dysfunction in the United States: a systematic review and meta-analysis. JAMA Ophthalmol. 2022;140(12):1181–1192. doi:10.1001/jamaophthalmol.2022.4394
21. Gharbiya M, Moramarco A, Castori M, et al. Ocular features in joint hypermobility syndrome/ehlers-danlos syndrome hypermobility type: a clinical and in vivo confocal microscopy study. Am J Ophthalmol. 2012;154(3):593–600.e1. doi:10.1016/j.ajo.2012.03.023
22. Fieß A, Elflein HM, Urschitz MS, et al. Prevalence of strabismus and its impact on vision-related quality of life: results from the german population-based gutenberg health study. Ophthalmology. 2020;127(8):1113–1122. doi:10.1016/j.ophtha.2020.02.026
23. Hashemi H, Pakzad R, Heydarian S, et al. Global and regional prevalence of strabismus: a comprehensive systematic review and meta-analysis. Strabismus. 2019;27(2):54–65. doi:10.1080/09273972.2019.1604773
24. Zhang XJ, Lau YH, Wang YM, et al. Prevalence of strabismus and its risk factors among school aged children: the Hong Kong Children Eye Study. Sci Rep. 2021;11(1):13820. doi:10.1038/s41598-021-93131-w
25. Fu Z, Hong H, Su Z, Lou B, Pan CW, Liu H. Global prevalence of amblyopia and disease burden projections through 2040: a systematic review and meta-analysis. Br J Ophthalmol. 2020;104(8):1164–1170. doi:10.1136/bjophthalmol-2019-314759
26. Hu B, Liu Z, Zhao J, et al. The global prevalence of amblyopia in children: a systematic review and meta-analysis. Front Pediatr. 2022;10:819998. doi:10.3389/fped.2022.819998
27. Brooks JK. A review of syndromes associated with blue sclera, with inclusion of malformations of the head and neck. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018;126(3):252–263. doi:10.1016/j.oooo.2018.05.012
28. Gomes JAP, Rodrigues PF, Lamazales LL. Keratoconus epidemiology: a review. Saudi J Ophthalmol. 2022;36(1):3–6. doi:10.4103/sjopt.sjopt_204_21
29. Segev F, Héon E, Cole WG, et al. Structural abnormalities of the cornea and lid resulting from collagen V mutations. Invest Ophthalmol Vis Sci. 2006;47(2):565–573. doi:10.1167/iovs.05-0771
30. Fransen E, Valgaeren H, Janssens K, et al. Resequencing of candidate genes for Keratoconus reveals a role for Ehlers–Danlos Syndrome genes. Eur J Hum Genet. 2021;29(12):1745–1755. doi:10.1038/s41431-021-00849-2
31. Liang J, Pu Y, Chen J, et al. Global prevalence, trend and projection of myopia in children and adolescents from 1990 to 2050: a comprehensive systematic review and meta-analysis. Br J Ophthalmol. 2025;109(3):362–371. doi:10.1136/bjo-2024-325427
32. Chiarelli N, Ritelli M, Zoppi N, Colombi M. Cellular and molecular mechanisms in the pathogenesis of classical, vascular, and hypermobile Ehlers‒Danlos syndromes. Genes. 2019;10(8):609. doi:10.3390/genes10080609
33. Gazit Y, Nahir AM, Grahame R, Jacob G. Dysautonomia in the joint hypermobility syndrome. Am J Med. 2003;115(1):33–40. doi:10.1016/s0002-9343(03)00235-3
34. Gensemer C, Beck T, Guo L, et al. Variants in the kallikrein gene family and hypermobile Ehlers-Danlos syndrome. Res Sq. 2024:
35. Webb JG. The kallikrein/kinin system in ocular function. J Ocul Pharmacol Ther. 2011;27(6):539–543. doi:10.1089/jop.2011.0187
36. Wilson GN. A Gene network implicated in the joint-muscle pain, brain fog, chronic fatigue, and bowel irregularity of Ehlers-Danlos and “Long” COVID19 syndromes. 2023. doi:10.1101/2023.03.24.23287706
37. Kampanartsanyakorn S, Surachatkumtonekul T, Dulayajinda D, Jumroendararasmee M, Tongsae S. The outcomes of horizontal strabismus surgery and influencing factors of the surgical success. J Med Assoc Thai. 2005;88:S94–99.
38. Kumari N, Amitava AK, Ashraf M, Grover S, Khan A, Sonwani P. Prognostic preoperative factors for successful outcome of surgery in horizontal strabismus. Oman J Ophthalmol. 2017;10(2):76–80. doi:10.4103/ojo.OJO_133_2016
39. Abbasoglu OE, Sener EC, Sanac AS. Factors influencing the successful outcome and response in strabismus surgery. Eye. 1996;10(Pt 3):315–320. doi:10.1038/eye.1996.66
40. Gauthier AC, Bower KS, Singman EL. Outcomes and complications in patients with hypermobile Ehlers-Danlos syndrome who have undergone laser in situ keratomileusis surgery. Cornea. 2023;42(3):284–291. doi:10.1097/ICO.0000000000003028
41. Melki SA, Azar DT. LASIK complications: etiology, management, and prevention. Survey Ophthalmol. 2001;46(2):95–116. doi:10.1016/S0039-6257(01)00254-5
42. Binder PS, Lindstrom RL, Stulting RD, et al. Keratoconus and corneal ectasia after LASIK. J Cataract Refract Surg. 2005;31(11):2035–2038. doi:10.1016/j.jcrs.2005.12.002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.