")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Online Survey to Investigate Asthma Medication Prescription and Adherence from the Perspective of Patients and Healthcare Practitioners in England
Received 16 June 2023
Accepted for publication 31 August 2023
Published 18 September 2023 Volume 2023:16 Pages 987—996
DOI https://doi.org/10.2147/JAA.S426227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Xiubin Zhang, Jennifer K Quint
National Heart and Lung Institute, Imperial College London, London, W12 0BZ, United Kingdom
Correspondence: Jennifer K Quint, National Heart and Lung Institute, Imperial College London, Level 9, Sir Michael Uren Hub, White City Campus, 86 Wood Lane, London, W12 0BZ, United Kingdom, Email [email protected]
Background: High short-acting β2-agonist (SABA) use and/or inhaled corticosteroid (ICS) underuse are common and are associated with poor asthma outcomes. This study explored patients’ and healthcare practitioners’ (HCPs’) perspectives to contextualize asthma treatment patterns observed in real-world studies.
Methods: Data were collected using online surveys from HCPs and people with asthma (≥ 18 years old with a confirmed asthma diagnosis of any severity) who had consented to research participation through the Clinical Practice Research Datalink. Data were analysed using descriptive statistics.
Results: In total, 76 HCPs and 63 patients were invited to take part. Of 48 valid HCP responders, 54.2% (n=26) reported scheduling an annual asthma treatment review with their patients and 83.3% of general practitioners (n=40) had prescribed repeated inhalers at the patient’s request. Of 47 valid patient responders, 57.4% (n=27) reported using their reliever (SABA) inhaler daily and 55.3% of patients (n=26) reported being prescribed a preventer inhaler. Of the total patient responders, 31.9% (n=15) reported that they never used their preventer inhaler. Consistent annual adherence with preventer inhalers was reported by 44.7% of all valid responders (n=21), while other patients admitted to using preventers intermittently.
Conclusion: SABA and ICS prescription patterns are driven by a combination of HCP and patient factors. Opportunities exist to improve asthma control and behaviours around inhaler use.
Keywords: asthma, adherence, healthcare professional, ICS, prescription, SABA
A Letter to the Editor has been published for this article.
Introduction
Asthma is a chronic inflammatory disease in which epithelial damage and bronchoconstriction result in increased mucus production, stimulating bouts of coughing, wheezing, and breathlessness.1,2 Treatment options involve the use of bronchodilators, usually short-acting beta-agonists (SABAs), colloquially termed “relievers”, in combination with inhaled corticosteroids (ICSs), colloquially termed “controllers” or “preventers”, to control and reduce the severity of symptoms, improve health outcomes, and reduce mortality. ICS therapy can also be used in combination with a long-acting bronchodilator as a reliever therapy.3,4
The prolonged high use of SABAs is recognized as a marker for poor symptom control and is associated with exacerbations and hospitalization.5 Results from a large cohort study investigating asthma therapy prescriptions concluded that the use of SABAs (defined as ≥12 inhalers over 12 months) increased from 8.6% to 10.5% in UK adults during a 6-year period (2007–2013). Over the same period, SABA use in France was relatively stable, ranging from 5.4% to 5.2%.6 A recent study of 1288 asthma patients indicated that only 20% are “well-controlled” according to the Global Initiative for Asthma (GINA) classification.7
The majority of existing patient databases only include data on the amount of prescribed or dispensed medication, but are unclear about how much patients actually use, why and when, as well as the prescribing behaviours of general practitioners (GPs). Therefore, understanding patients’ behavioural patterns and HCPs’ prescribing behaviours that result in low adherence to ICSs and relatively high SABA use will shape future practice. This requires recognition of the role played by prescribing practitioners in facilitating patient behaviours, ie their attitudes and approaches to prescribing. We aimed to explore the attitudes and behaviours of people with asthma and the prescribing behaviours of practitioners to help us to gain a better understanding of the reasons for and motivation behind SABA use, how this relates to ICS use, and ultimately, the impact on asthma-related healthcare resource utilization.
Methods
This was a cross-sectional online survey, exploring the perspectives of patients and healthcare practitioners (HCPs) to contextualize asthma treatment patterns.
Survey Development
Prior to distribution of the surveys, a small number of GPs, patients registered with a lay patient advisory group, and asthma patients from the NHS England clinical service critically appraised and validated the survey questions during several online discussions. The feedback helped us to modify and revise the questions for understandability,8 and to estimate the time it would take for participants to complete the surveys (see Supplementary Materials).
Study Population and Eligibility Criteria
The study population included HCPs from research-active GP practices contributing to the Clinical Practice Research Datalink (CPRD) Aurum and GOLD primary care databases who had agreed to take part in additional studies, and adult patients with a current asthma diagnosis who were registered in those practices. CPRD is a real-world research service supporting retrospective and prospective public health and clinical studies.9,10 CPRD holds an anonymized GP records database containing continually updated primary care medical data. This database includes details on symptoms, diagnoses, tests, prescriptions, patient demographics, health behaviours, and referrals to secondary care.
Survey Data Collection
Both the GP and the patient survey data were collected from 3 October 2022 to 30 November 2022. The GP survey was created in an online platform (Qualtrics) and administered by the CPRD team via a customized link. The CPRD team disseminated the online survey instructions together with the study information pack to GP practices indicating interest in participation in research (“research-active” practices). The CPRD team provided the relevant links to 130 GP practices for accessing and completing the online survey. Completed survey data were anonymized and accessed by the research team for analysis.
For the patient survey, CPRD screened patients for possible participation based on the following eligibility criteria: patients with a current diagnosis of asthma, aged 18 years and over, and without a COPD diagnosis. After screening, patients who met the inclusion criteria were sent an invitation to take part in the study by the relevant GP practice. Participants who expressed an interest to participate were then sent the study information pack, the online survey link, and instructions on how to complete the survey. After the survey had concluded, the research team were able to access data from the online platform for analysis.
Data Analysis
Descriptive analysis was used to report the proportions of responses from the HCPs and the patients. SPSS 26 statistical software was used.
Results
GP Survey
A total of 76 GPs participated in the online survey. After eliminating invalid responses (surveys that contained missing data and where key questions had not been answered), there were 48 valid responders. All of the following percentages used 48 responders as the denominator. Overall, 47.1% (n=23) were female and 41.7% (n=20) male. Most respondents were in the age group 40–50 years (33.3%, n=16). Of the GPs, 27.1% (n=13) had been practising for 11–20 years and a similar number for 21–30 years. Half of the GPs reported seeing more than 10 patients with asthma in a month.
The survey results showed that 31.3% of GPs (n=15) prescribed SABAs differently in people also prescribed regular ICS compared with those on a single maintenance and reliever therapy (SMART) regime, while 29.2% (n=14) responded that they did not prescribe SABAs differently in people on regular ICS versus SMART; 39.6% (n=19) of answers to this question were missing. There were multiple reasons why GPs prescribed SABAs differently. Almost half of GPs (45.8%, n=22) said that they changed the prescription owing to poorly controlled symptomatic asthma; 54.2% (n=22) performed a treatment review for asthma patients as a scheduled annual review (Figure 1A and B), and 47.9% (n=23) reviewed the treatment in response to an increased quantity/frequency of SABA prescription and 45.8% owing to poorly controlled symptomatic asthma.
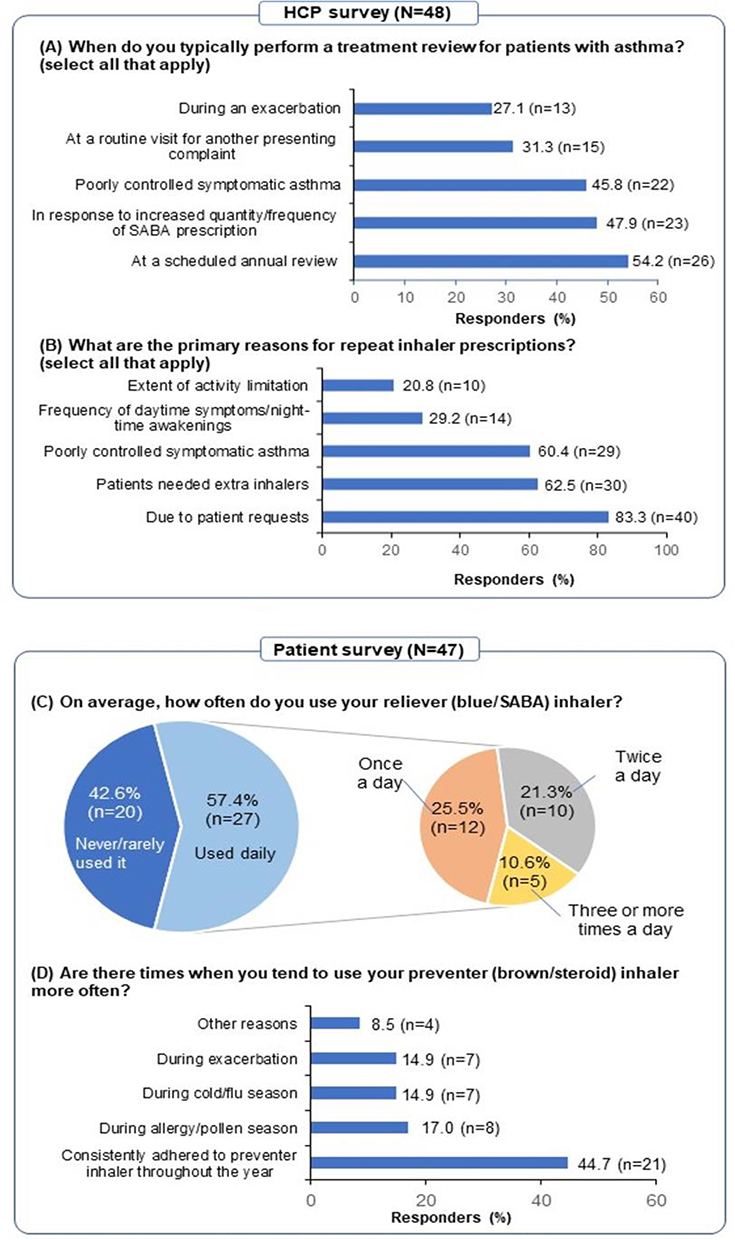 |
Figure 1 Responses received from healthcare practitioners (HCPs) and patients. (A and B) Responses received from HCPs. (C and D) Responses received from patients with asthma. |
In total, 83.3% of GPs (n=40) claimed that they prescribed repeated inhaler prescriptions (reliever and preventer) because of patients’ requests (Figure 1A and B). The reasons given for this varied from patients saying they needed extra inhalers (62.5%, n=30) to those having poorly controlled symptomatic asthma (60.4%, n=29). When asked to rank the reasons for prescribing specific inhalers, the majority of GPs said that the primary reason was patients’ requests/repeat prescriptions, although this varied by inhaler type: 60.4% (n=29) SABA inhaler, 60.4% (n=29) ICS therapy, and 45.8% (n=22) SMART (Table 1).
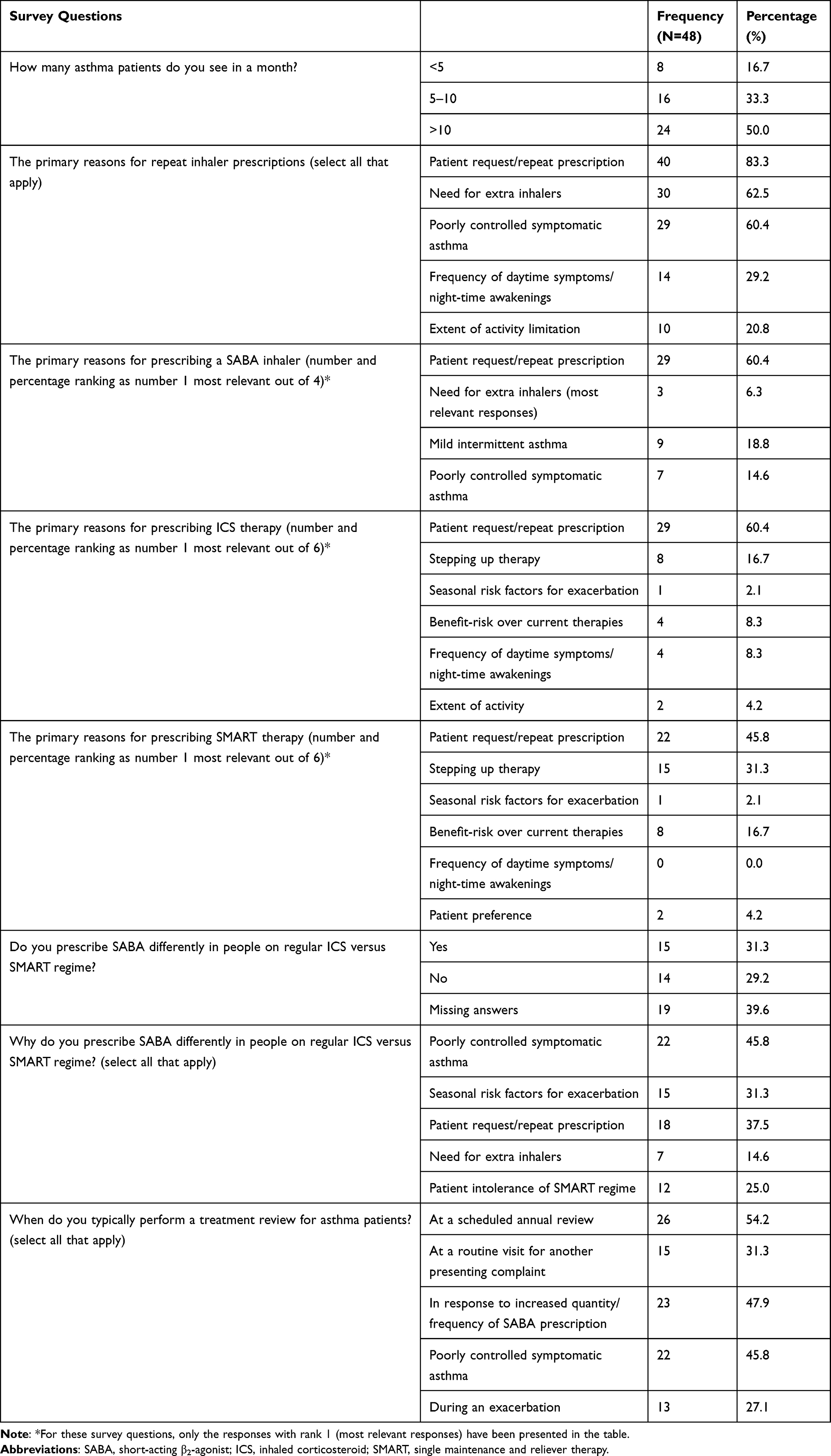 |
Table 1 Survey Responses from GPs |
Patient Survey
A total of 63 patients with asthma enrolled into the online survey. After eliminating invalid responses, there were 47 valid responders. All of the following percentages used 47 responders as the denominator. Of the 47 participants, 44.7% (n=21) said that they had been given an asthma treatment plan by their HCP, while 55.3% (n=26) said that they had not.
The survey found that 87.2% of participants (n=47) had been prescribed a reliever (blue/SABA) inhaler. Most patients (89.4%, n=42) said that they felt confident using their inhalers, whereas approximately 6% did not. Over half of the patients (57.4%, n=27) used their reliever inhaler frequently (25.5% of patients once a day, 21.3% twice a day, and 10.6% three or more times a day), whereas 42.6% of patients (n=20) never or rarely used it (Figure 1C). Furthermore, 59.6% of patients (n=28) were more likely to use the reliever during the cold/flu season, 42.6% during the allergy/pollen season, and 38.3% (n=18) before exercise or other known triggers. Only 19.1% (n=9) used the SABA inhaler the same amount throughout the year.
When responding to the question “What types of inhalers have you been prescribed?”, of SABA, ICS, and SMART, 55.3% of respondents (n=26) reported that they had been prescribed a preventer (brown/steroid) inhaler (Table 2). But on the question “Are there times when you tend to use your preventer inhaler more often?”, 17% of respondents (n=8) used it once a day and 31.9% twice a day, while only about 4% used it three or more times a day. Furthermore, 44.7% (n=21) adhered to their preventer inhaler the same amount throughout the year, while the rest of the participants used it depending upon certain circumstances, such as 17% (n=8) using it during the allergy/pollen season and 14.9% (n=7) during the cold/flu season (Figure 1D). As a result of the online survey being self-reported, there exist inconsistencies in the responses to these two questions; these may also have occurred because in the first question, the responses considered only SABA, but in the second question, they accounted for both SABA and SMART.
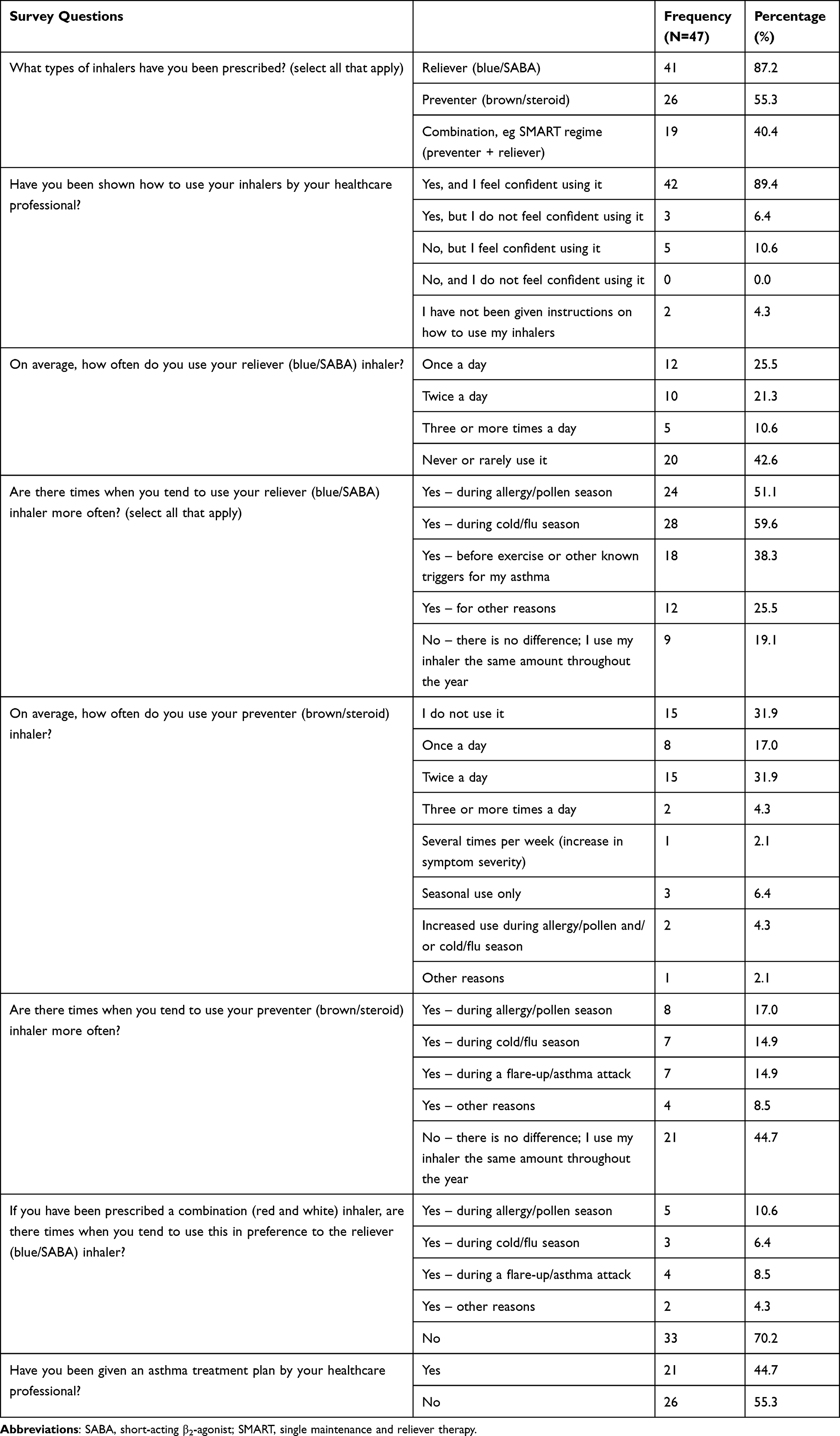 |
Table 2 Survey Responses from Patients |
Overall, 40.4% of respondents (n=19) claimed that they had been prescribed a SMART regime (preventer + reliever). However, for the question “If you have been prescribed a combination (red and white) inhaler, are there times when you tend to use this in preference to the reliever (blue/SABA) inhaler?”, of 47 responses, 70% (n=33) did not prefer to use SMART, and only 10.6% (n=5) preferred to use SMART during the allergy/pollen season rather than use SABA (Table 2).
Discussion
This study found numerous challenges to consistent adherence to controller medication for patients with asthma. It investigated SABA and ICS prescription patterns, showing how asthma control is driven by a combination of HCP and patient factors. At the individual level, patients’ behaviours with regard to medication adherence play an important role in their illness control; we found that only slightly more than half of the patients adhered to their preventer medication and that less than half of the participants were using their preventer inhaler throughout the year. This may be appropriate if asthma is seasonal. Meanwhile, more than half the patients used the inhaler only during allergy or cold seasons, or during periods of asthma exacerbation. The study also identified that HCPs’ prescribing behaviours play a role in adherence to asthma medication, such as GPs prescribing the inhaler prescriptions to meet the patients’ requirements rather than following a clinical guideline. This may be because the majority of prescriptions prescribed are requests for repeat prescriptions rather than the initial treatment. This suggests that further research is needed to identify the most effective approaches to promote medication prescription by HCPs and to educate patients about the importance of medication adherence in asthma control.
Previous studies have found that some patients are non-compliant with medication use when they are symptom free and only adhere to medication during symptomatic episodes.11 A study from five European countries also found that when symptoms worsen, most patients increase SABA use, instead of evaluating the appropriateness of stepping up the maintenance medication.12 Numerous studies indicate that adherence to the use of preventer medication by patients with asthma is poor worldwide,13,14 and has been associated with an increased socio-economic burden.15 There is also a tendency for patients to misjudge their condition and overestimate their management and symptom control.11
The findings of our study also show that almost half of the HCPs did not schedule asthma treatment follow-up with their patients. Consequently, the lack of monitoring of asthma control will subsequently affect patients’ medication adherence. Follow-up schedules have been proven to be effective by many studies, as these are one of the key components of asthma treatment and disease control.16–18
Our study also found that eight out of 10 HCPs have prescribed repeated inhaler prescriptions because of a request by the patient. Previous studies have found that prescribing behaviours are associated with several factors, including inadequate HCP training on asthma management,19 the increased cost of maintenance therapy, the generalized definition of the disease, and the doctor–patient relationship.20 Alerts on computerized support systems for repeat prescriptions can also influence GPs’ prescribing behaviours.21 Furthermore, different guidelines and treatment approaches for asthma management may lead to the overuse of SABA and underuse of controllers.22–24
Poor adherence is a major problem in asthma control, and results in increased hospitalization, mortality, and healthcare use and costs. One study identified that different determinants explained different reasons for non-adherence.25 Therefore, identifying determinants of non-adherence can help HCPs to develop targeted interventions to reduce non-adherence. A number of trials designed to change patients’ health behaviour showed that interventions such as sending a reminder message to the patient have the potential to improve disease monitoring and management.26 Studies have also shown how developing a personalized self-management care plan for patients involving mobile technology interventions13 and, where feasible, annual reviews on inhaler use and technique is important for symptom management and control.15,27,28 However, despite extensive research on poor adherence and interventions, an ideal solution remains elusive and demands further research. For example, studies on understanding HCPs’ and patients’ perceptions and behaviours and the possible barriers to asthma treatment, including psychological dependence, are important.
Study Limitations
Using an online survey method to explore patients’ and HCPs’ views and experiences around their diagnosis and medication use has provided valuable insights into the motivation behind preferred inhaler use, and the potential challenges relating to medication non-adherence and prescribing practices. However, several important limitations of the study need to be addressed. Firstly, since the online survey was self-reported, responses may be inconsistent; this potentially leads to over- or under-reporting of SABA use and may cause misclassification of outcomes. Secondly, online data collection may help in reducing costs but tends to have high non-response rates. Our small sample size gave results which may not be sufficiently powered to detect differences between the groups. There are some potential reasons for the small sample size. Firstly, the online survey was self-selected, which may have caused the low response rate and the low completion rate. The second reason may be due to the fact that the surveys were distributed via CPRD; for patient data protection, our research team could not make any contact with or send a reminder to the potential respondents; in addition, we did not use any conjunction methods, such as web or emails, for survey collection, so the study only yielded a small sample size. The timing of the study may also have affected response rates, as the study was delayed for years because of COVID-19 and was distributed at a time when GP practices were still recovering their services. Thirdly, selection bias due to recruiting prescreened patient participants may have the potential to skew the results and reduce the generalizability of the study. To limit the chance of selection bias, the online survey was based on randomly selecting respondents from the population of interest; furthermore, the respondents’ characteristics could not be observed or known, which reduced the selection bias. Finally, we could not calculate the proportions of patients on SMART who used daily SABAs, as we do not have these data. This would be worth exploring in future studies.
Conclusions
We found that SABA and ICS prescription patterns are driven by a combination of HCP and patient factors. The findings indicate room for improvement in asthma control and SABA prescription practices, and suggest that there are opportunities for better targeted education for both patients and HCPs, leading to effective healthcare resource utilization and improved asthma control.
Ethical Approval
The data handling and storage complies with the General Data Protection Regulation (GDPR) guidelines. The Independent Scientific Advisory Committee (ISAC) granted approval for the study on 28 May 2020 (protocol number 20_085) to access anonymized primary care data through CPRD. HRA and Health and Care Research Wales (HCRW) approval was given for the study on 22 November 2021 (REC reference: 21/PR/1438). The study was conducted according to the guidelines of the Declaration of Helsinki. Informed consent was obtained from all patients participating in the study.
Acknowledgments
The authors wish to acknowledge the contributions of Rupa Sisoda, Anne-Marie Russell, and Adrian Rabe for their work on the study protocol, and Claudia Cabrera for developing the SABINA framework (particularly the quantitative CPRD study), which set the groundwork for this study. We thank Mina Khezrian and her AstraZeneca colleagues for reviewing the paper prior to submission.
Funding
The study was funded by AstraZeneca.
Disclosure
Professor Jennifer K Quint reports grants from AstraZeneca, during the conduct of the study; and grants and/or personal fees from AZ, Chiesi, GSK, and MRC, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Kaufman G. Asthma: pathophysiology, diagnosis and management. Nurs Standard. 2011;26(5):48. doi:10.7748/ns.26.5.48.s55
2. National Institute for Health and Care Excellence (NICE). Asthma: what is it?; 2021. Available from: https://cks.nice.org.uk/topics/asthma/background-information/definition/.
3. GINA. Global initiative for asthma, pocket guide for asthma management and prevention. Available from: https://ginasthma.org/pocket-guide-for-asthma-management-and-prevention.
4. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma (GINA) strategy 2021–executive summary and rationale for key changes. J Allergy Clin Immunol. 2021;2021:1.
5. Nwaru BI, Ekström M, Hasvold P, Wiklund F, Telg G, Janson C. Overuse of short-acting β 2 -agonists in asthma is associated with increased risk of exacerbation and mortality: a nationwide cohort study of the global SABINA programme. Eur Respir J. 2020;55(4):1901872. doi:10.1183/13993003.01872-2019
6. Belhassen M, Nibber A, Van Ganse E, et al. Inappropriate asthma therapy—a tale of two countries: a parallel population-based cohort study. PJ Prim Care Respir Med. 2016;26(1):1–5. doi:10.1038/npjpcrm.2016.76
7. Fuhlbrigge A, Marvel J, Electricwala B, et al. Physician–patient concordance in the assessment of asthma control. J Allergy Clin Immunol. 2021;9(8):3080–3088.
8. Patrick DL, Burke LB, Gwaltney CJ, et al. Content validity-establishing and reporting the evidence in newly developed patient-reported outcomes (PRO) instruments for medical product evaluation: ISPOR PRO good research practices task force report: part 2—assessing respondent understanding. Value Health. 2011;14(8):978–988. doi:10.1016/j.jval.2011.06.013
9. Herrett E, Gallagher AM, Bhaskaran K, et al. Data resource profile: clinical practice research datalink (CPRD). Int J Epidemiol. 2015;44(3):827–836. doi:10.1093/ije/dyv098
10. Wolf A, Dedman D, Campbell J, et al. Data resource profile: clinical practice research Datalink (CPRD) aurum. Int J Epidemiol. 2019;48(6):1740–1740g. doi:10.1093/ije/dyz034
11. Partridge MR, van der Molen T, Myrseth S-E, Busse WW. Attitudes and actions of asthma patients on regular maintenance therapy: the INSPIRE study. BMC Pulm Med. 2006;6(1):1–9. doi:10.1186/1471-2466-6-13
12. Looijmans-van den Akker I, Werkhoven A, Verheij T. Over-prescription of short-acting beta agonists in the treatment of asthma. Fam Pract. 2021;5:612–616. doi:10.1093/fampra/cmab013
13. Miller L, Schüz B, Walters J, Walters EH. Mobile technology interventions for asthma self-management: systematic review and meta-analysis. JMIR mHealth uHealth. 2017;5(5):e57. doi:10.2196/mhealth.7168
14. Horne R. Compliance, adherence, and concordance: implications for asthma treatment. Chest. 2006;130(1):65S–72S. doi:10.1378/chest.130.1_suppl.65S
15. Bårnes CB, Ulrik CS. Asthma and adherence to inhaled corticosteroids: current status and future perspectives. Respir Care. 2015;60(3):455–468. doi:10.4187/respcare.03200
16. Park HJ, Byun MK, Kim HJ, et al. Regular follow-up visits reduce the risk for asthma exacerbation requiring admission in Korean adults with asthma. Allergy Asthma Clin Immunol. 2018;14:1–7. doi:10.1186/s13223-018-0250-0
17. Gallucci M, Carbonara P, Pacilli AMG, Di Palmo E, Ricci G, Nava S. Use of symptoms scores, spirometry, and other pulmonary function testing for asthma monitoring. Front Pediatr. 2019;7:54. doi:10.3389/fped.2019.00054
18. Roche N, Morel H, Martel P, Godard P. Clinical practice guidelines: medical follow-up of patients with asthma—adults and adolescents. Respir Med. 2005;99(7):793–815. doi:10.1016/j.rmed.2005.03.011
19. Román-Rodríguez M, Ibarrola-Ruiz L, Mora F, et al. Motivational interviewing for adherence: post-training attitudes and perceptions of physicians who treat asthma patients. Patient Prefer Adherence. 2017;Volume 11:811–820. doi:10.2147/PPA.S127645
20. Tan N, Tay I, Ngoh A, Tan M. Factors influencing family physicians’ drug prescribing behaviour in asthma management in primary care. Singapore Med J. 2009;50(3):312.
21. Matui P, Wyatt JC, Pinnock H, Sheikh A, McLean S. Computer decision support systems for asthma: a systematic review. PJ Prim Care Respir Med. 2014;24(1):1–10. doi:10.1038/npjpcrm.2014.5
22. Martin MJ, Harrison TW. Is it time to move away from short-acting beta-agonists in asthma management? Eur Respir J. 2019;53:1802223. doi:10.1183/13993003.02223-2018
23. O’Byrne PM, Jenkins C, Bateman ED. The paradoxes of asthma management: time for a new approach? Eur Respir J. 2017;50(3). doi:10.1183/13993003.01103-2017
24. Papi A, Blasi F, Canonica GW, Morandi L, Richeldi L, Rossi A. Treatment strategies for asthma: reshaping the concept of asthma management. Allergy Asthma Clin Immunol. 2020;16(1):1–11. doi:10.1186/s13223-020-00472-8
25. Unni E, Farris KB. Determinants of different types of medication non-adherence in cholesterol lowering and asthma maintenance medications: a theoretical approach. Patient Educ Couns. 2011;83(3):382–390. doi:10.1016/j.pec.2011.02.017
26. Patel M, Perrin K, Pritchard A, et al. Accuracy of patient self‐report as a measure of inhaled asthma medication use. Respirology. 2013;18(3):546–552. doi:10.1111/resp.12059
27. Ring N, Jepson R, Hoskins G, et al. Understanding what helps or hinders asthma action plan use: a systematic review and synthesis of the qualitative literature. Patient Educ Couns. 2011;85(2):e131–e143. doi:10.1016/j.pec.2011.01.025
28. Levy ML, Hardwell A, McKnight E, Holmes J. Asthma patients’ inability to use a pressurised metered-dose inhaler (pMDI) correctly correlates with poor asthma control as defined by the global initiative for asthma (GINA) strategy: a retrospective analysis. Prim Care Respir J. 2013;22(4):406–411. doi:10.4104/pcrj.2013.00084
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.