Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 16
One Rare Warfarin Resistance Case and Possible Mechanism Exploration
Received 6 February 2023
Accepted for publication 26 May 2023
Published 20 June 2023 Volume 2023:16 Pages 609—615
DOI https://doi.org/10.2147/PGPM.S404474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Li Zhao,1 Zhenguo Zhai,2 Pengmei Li1
1Pharmacy Department, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, China-Japan Friendship Hospital, Beijing, People’s Republic of China
Correspondence: Pengmei Li, Pharmacy Department, China-Japan Friendship Hospital, No. 2 Yinghua East Road, Beijing, People’s Republic of China, Tel +86-1084205661, Email [email protected]
Abstract: One 59-year-old female patient with deep venous thrombosis (DVT) and pulmonary embolism (PE) was treated with 6 mg warfarin once daily as an anticoagulant. Before taking warfarin, her international normalized ratio (INR) was 0.98. Two days after warfarin treatment, her INR did not change from baseline. Due to the high severity of the PE, the patient needed to reach her target range (INR goal = 2.5, range = 2~3) rapidly, so the dose of warfarin was increased from 6 mg daily to 27 mg daily. However, the patient’s INR did not improve with the dose escalation, still maintaining an INR of 0.97– 0.98. We drew a blood sample half an hour before administering 27 mg warfarin and detected single nucleotide polymorphism for the following genes, which were identified to be relevant with warfarin resistance: CYP2C9 rs1799853, rs1057910, VKORC1 rs9923231, rs61742245, rs7200749, rs55894764, CYP4F2 rs2108622, and GGCX rs2592551. The trough plasma concentration of warfarin was 196.2 ng/mL after 2 days of warfarin administration with 27 mg QD, which was much lower than the therapeutic drug concentration ranges of warfarin (500– 3,000 ng/mL). The genotype results demonstrate that the CYP4F2gene has rs2108622 mutation which can explain some aspect of warfarin resistance. Further investigations are necessary to fully characterize other pharmacogenomics or pharmacodynamics determinants of warfarin dose-response in Chinese.
Keywords: anticoagulation, warfarin resistance, CYP2C9, VKORC1, CYP4F2, GGCX, warfarin plasma concentration
Introduction
For more than 50 years, warfarin has been the sole agent administered to prevent or treat thromboembolic disorders orally. Despite the increased use of direct oral anticoagulants (DOACs), warfarin remains the main drug of choice for stroke prevention with mechanical heart valve replacement, antiphospholipid antibody syndrome, and end stage renal disease (ESRD).1–3
Because of the narrow therapeutic window, the application of warfarin carries out many potential risks including over- or under-anticoagulation. The inter-individual variation in dose requirements for warfarin was more than 20-fold.4 The large variation of warfarin attributes to clinical factors and DNA variants, which could impact the pharmacokinetic and/or pharmacodynamics of warfarin. Though there are many case reports about warfarin resistance in African-American and Caucasian populations, warfarin resistance is rarely documented in Chinese populations. In this report, we presented a rare warfarin resistance case in China and explored the possible mechanism in order to provide a clinical diagnosis and treatment pathway on warfarin resistance.
Case Report
A 59-year-old female (height: 161 cm, weight: 68 kg, and BMI: 26.56) was admitted into our hospital with deep venous thrombosis and pulmonary embolism. The CT pulmonary angiography (CTPA) result exhibited: the main pulmonary artery, upper lobar, middle lobar, and lower lobar arteries of the right lung, and lower lobar artery of the left lung all had thrombosis; the color ultrasound examination for deep veins of both lower limbs showed muscular venous thrombosis in the right side. Her D-Dimer was 1,090 ng/mL (0–400 ng/mL). Her medical history included bronchial asthma, chronic obstructive pulmonary disease (COPD), and hypertension. Before hospitalization, the patient was taking dabigatran 150 mg twice a day for anticoagulation. The patient had a low income and the cost of dabigatran was high for her (it costs RMB 19.8 yuan for one capsule of dabigatran, while it costs RMB 0.5 yuan for one tablet of warfarin), so she was eager to take warfarin instead of dabigatran. The baseline of her international normalized ratio (INR) was 0.98 before taking warfarin. Prior to using warfarin, our clinical pharmacists educated the patient about possible drug interactions for warfarin and a controlled diet. Considering the onset time of warfarin is slow, doctors prescribed subcutaneous enoxaparin 6,000 IU every 12 hours with warfarin 6 mg once daily. After 2 days, her INR did not change. In order to reach the target INR goal 2.5 (range 2~3) rapidly, her warfarin dose was increased from 6 mg/day on Day 1 to 27 mg/day on Day 9 (Figure 1 shows the changes in warfarin dose and INR). During the following 12 days, the INR did not achieve the therapeutic goal and remained at 0.97–1.00 despite the warfarin dosage being increased 4.5-fold (27 mg vs 6 mg). Due to the failure to reach target range, we prescribed enoxaparin 6,000 IU BID instead, and switched back to dabigatran 150 mg BID when discharged. After taking dabigatran for 4 months, the patient started to take aspirin instead of dabigatran. One year later, fresh thrombosis recurred in the branches of the patient’s pulmonary artery, and she was developed into chronic thromboembolic pulmonary hypertension (CTEPH) at last.
 |
Figure 1 The trend of warfarin dose and INR. Abbreviation: INR, international normalized ratio. |
When taking warfarin, the patient was prescribed the following other medicines: budesonide and formoterol fumarate powder for inhalation, atorvastatin, minocycline, piperacillin sodium and sulbactam sodium, perindopril, lansoprazole, silybin meglumine, levofloxacin and nifedipine sustained release tablets. Among these drugs, some may increase the serum concentration or enhance the anticoagulant effect of warfarin, like lansoprazole, atorvastatin, and levofloxacin. None of them are CYP2C9 or CYP3A4 inducers. Furthermore, malabsorption disorders such as gastroenteritis, celiac disease, chronic pancreatitis, or short gut syndrome were also excluded.
In order to identify the hereditary and pharmacokinetics factors of warfarin resistance, we reviewed related literature about warfarin resistance. Gene polymorphisms in VKORC1, GGCX, and CYP4F2 were reported to be closely related to warfarin resistance. We used polymerase chain reaction to genotype the rs2592551 polymorphism in the GGCX gene, rs2108622 polymorphism in CYP4F2, rs9923231(−1639G>A), rs17878544, rs7200749, rs9934438(1173C>T), rs55894764(R12R) and the D36Y mutation in the VKORC1 gene, and rs1799853 and rs1057910 in the CYP2C9 gene (results of gene polymorphisms in our study are displayed in Table 1). The HPLC/MS/MS system was validated to detect the trough plasma concentration to analyze the internal exposure of warfarin in this patient. We sampled the trough concentration after 2 days of warfarin administration with 27 mg QD. The result of the plasma concentration of warfarin was 196.2 ng/mL, which was much less than the validity range of warfarin (500–3,000 ng/mL).
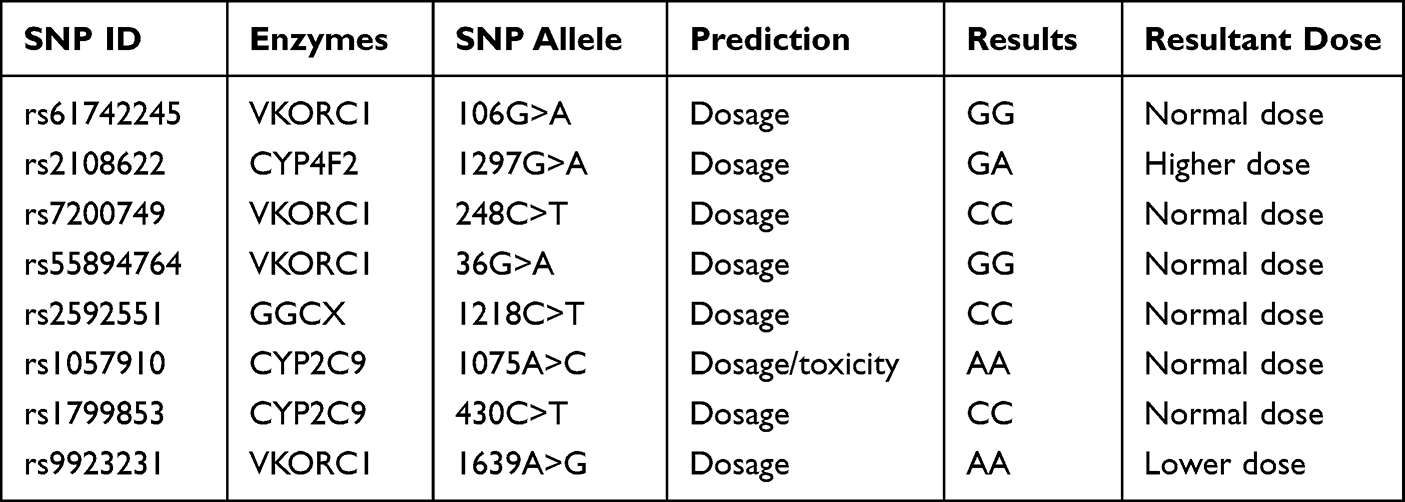 |
Table 1 The results of gene polymorphisms of the patient |
Discussion
Warfarin is the most widely prescribed oral anticoagulant in China despite the approval of several direct oral anticoagulants (DOACs). However, it has a narrow therapeutic index and wide dose variability. Diverse populations encounter higher adverse health risks compared to European patients. Asians have higher risks of warfarin-related intracranial hemorrhage outcomes than individuals with European ancestry.5 Average daily doses differ by race/ethnicity as the daily dose needed to reach a stable therapeutic INR is estimated at 5.1 mg in individuals of European ancestry, 5.7 mg in individuals of African ancestry, 4.4 mg in Latinos, 3.4 mg in individuals of Asian ancestry, and 4.5 mg in American Indian/ALASKA natives.6–8 Warfarin resistance is defined as the situation in which warfarin at a normal dose range cannot function properly in terms of increasing prothrombin time or raising INR into the target range.9 However, warfarin resistance is difficult to identify, since the normal warfarin doses required to reach and maintain INR in a target range in different patient populations have considerable fluctuation. Osinbowale et al’s10 study stated that patients who required more than 105 mg of warfarin per week (15 mg/day) should be considered as warfarin-resistant, while another paper regarded warfarin dose requirements greater than 70 mg/week as warfarin resistance.11 Yuan et al12 defined warfarin resistance as an effective dose greater than 60 mg/week in Taiwaneses patients. In general, warfarin resistance is more common in African-Americans,13 followed by Caucasians.14,15 Reported instances of warfarin resistance in Asian populations are relatively rare.12,16 In our case, this is the first patient we met whose warfarin dose was 27 mg per day while her INR was still 1.0. The reasons for warfarin resistance include five possible contributing causes: poor patient compliance, increased clearance, decreased absorption of warfarin, drug interactions, and hereditary.
The patient maintained consistency with vitamin-K-containing foods in her diets and took all warfarin as instructed during hospitalization. The possibility of poor compliance of the patient was excluded. The patient did not have emesis, diarrhea, or malabsorption syndrome, which may cause reduced absorption of warfarin. Several reports have presented that lowering serum lipids, primarily triglycerides, increases the sensitivity to warfarin,17 most likely on account of a decreased pool of vitamin K. In our case, the patient’s total cholesterol was 5.57 mmol/L (reference range <5.20 mmol/L), low density lipoprotein was 3.87 mmol/L (reference range <3.4 mmol/L), and TG was 1.68 mmol/L (reference range <1.7 mmol/L). Hyperlipidemia may be one reason for the warfarin resistance of this patient.
Concomitant drugs of the patient included lansoprazole, perindopril, levofloxacin, and extended release nifedipine. The US Food and Drug Administration has suggested that proton pump inhibitors (PPIs) including lansoprazole may increase INR when used concomitantly with warfarin because it is competitively metabolized by cytochrome P450 2C19 (CYP2C19).18 Quinolone antibacterials including nalidixic acid, such as ciprofloxacin,19,20 gatifloxacin,21,22 and levofloxacin,23 could increase the activity of warfarin. Common drugs that may decrease INR are azathioprine, bosentan, carbamazepine, mercaptopurine, ribavirin, rifampin, etc. All the concomitant medicines of this patient have no known negative impacts on warfarin pharmacokinetic concentration and resultant INR change.
Over 35 CYP2C9 alleles have been described to influence warfarin metabolism. The CYP2C9*2(rs1799853) and *3(rs1057910) alleles are the most extensively studied mutations. The single nucleotide polymorphisms in CYP2C9*2(rs1799853), and *3(rs1057910) can lead to significant reductions in enzyme activity.24 Individuals with the CYP2C9*2 and *3 variants are more likely to need lower doses of warfarin, take a longer time to reach target INR upon starting warfarin therapy, and have an increased risk of bleeding complications. The patient’s result was CYP2C9 *1/*1, indicating that the enzyme activity of CYP2C9 was normal and the target INR could be reached soon.
VKORC1−1639G>A (rs9923231) genotypes (AA, AG, and GG) have been linked with warfarin dose requirement. The AA (most sensitive, low dose) genotype is predominant in Asians, whereas the GG (least sensitive, high dose) genotype is the most common one in African-Americans. For the AA, AG, and GG genotypes, the average predictive warfarin maintenance doses were 3, 5, and 6 mg/day, respectively.8 In our case, the patient was AA genotype, which made it unlikely this gene loci caused the insensitivity of warfarin.
The VKORC1 Asp36Tyr (rs61742245) SNP was first described as a warfarin resistance SNP in 2007.25 After that, numerical studies demonstrated that rs61742245 was strongly associated with high warfarin dose requirements (>70 mg/week), and it has been identified as one of the few markers for warfarin resistance.26,27 Compared with non-carriers, the carriers of one rs61742245 variant require a double maintenance dose to reach a therapeutic dose.28 This new mutation was relatively common in Jewish ethnic groups of Ethiopian descent (in whom the prevalence is 5%) and Ashkenazi descent (prevalence 4%), but its prevalence in other populations was rarely studied. The genotype of VKORC1 rs61742245 for the patient in our case was Wt/Wt, which rules out the attribution of rs61742245 variants. We also tested two other genotypes of VKORC1 in rs7200749 and rs55894746, which were reported to correlate with higher warfarin dose requirements in a South African black population.29,30 Our results shows that both genes of this patient are normal too.
Furthermore, we examined the genotypes of GGCX rs2592551 and CYP4F2 rs2108622. GGCX is one of the enzymes affecting the metabolism of warfarin.31–37 In the atrial fibrillation population in Xinjiang, the Xiayizha Kamali study concluded that patients with CT and TT genotypes in GGCX gene rs259251 loci required significantly higher warfarin doses than those with the CC genotype.38 The patient’s results revealed that GGCX rs2592551 was not a mutation, which indicates that GGCX rs2592551 was not working in the warfarin resistance of the patient. CYP4F2 rs2108622 was reported to affect VK1 oxidation activity. CYP4F2 CC exhibited the highest VK1 oxidation activity, while CYP4F2 TT exhibited a 75% reduction and the CT pool displayed an intermediate activity.39 CYP4F2 rs2108622 T carriers were likely to have higher hepatic levels of VK1 and thus require a higher warfarin dose.39 The outcomes of the individual meta-analysis for CYP4F2 genotype showed that warfarin doses in patients with genotype CT and TT were significantly higher by 10% and 21%, respectively, compared to individuals with the homozygous CYP4F2 genotype CC. CYP4F2 rs2108622 of the patient was heterozygote, which may play some role but not the most important role in the warfarin resistance of this patient.
All known gene mutations could account for around 42% of warfarin dose variance. Among them, SNPs in VKORC1 −1639 G>A are the most important, which can explicate up to ~30%, while two SNPs in CYP2C9 *2 and *3 could interpret about 10% of warfarin dose variance. The rs2108622 in CYP4F2 only elucidated approximately 1.5−7% of warfarin dosing variability.40–43 A considerable percentage of patients with warfarin resistance cannot be explained by known gene variation, which may be related to genetic mutations in VKORC1 and/or CYP2C9, drug interaction, or food and/or herbs.44
Potential mechanisms of pharmacodynamics warfarin resistance include increased affinity of vitamin K1, prolongation of normal clotting factor activity, production of clotting factors which is not dependent on vitamin K, and decreased VKOR sensitivity to warfarin. In humans, they result in high dose requirement to achieve a therapeutic effect in the setting of normal warfarin pharmacokinetics, normal warfarin concentration, and normal half-lives of blood clotting proteins.
Studies in humans suggest that a therapeutic total plasma warfarin level lies between 500–3,000 ng/mL.10 Our findings indicated that the patient has a plasma warfarin concentration of 196.2 ng/mL, which was much lower than the therapeutic range of warfarin. The patient was diagnosed as warfarin resistant, because her plasma warfarin concentration was shown to be lower than normal range, and the INR did not arrive at 2–3, even though the total dose of warfarin was increased to 159 mg in 10 days (15.9 mg/day on average), which was much higher than the normal population.
There are two approaches to treat warfarin resistant patients: increasing warfarin doses with monitoring until the prothrombin time and INR are in target, or switching to another anticoagulant drug. In the former approach, the warfarin dose can be safely increased to more than 100 mg daily as long as patients are monitored regularly and other medications are otherwise stable.10 Alternatively, other anticoagulant drugs may be substituted for warfarin and are currently available in China. These include subcutaneous heparins and the subcutaneous factor Xa inhibitor fondaparinux, dabigatran, rivaroxaban, and apixaban. Because warfarin did not exert any effect on the patient by increasing the warfarin dose, the anticoagulant drug dabigatran was prescribed to replace warfarin following the patient’s will.
Conclusion
Up to date, this was the first report about warfarin resistance reporting warfarin dose exceeding 20 mg per day in Chinese patients. There was no impaired absorption disease, no drug–drug interaction increasing the metabolism and clearance of warfarin, yet the trough warfarin concentration was only 196.2 ng/mL, which was much lower than the therapeutic range of warfarin. For the gene mutation perspective, we investigated 8 mainly SNP affecting warfarin dosage. Only the CYP4F2 rs2108622 gene was heterozygote, which may play a role but not the most important role in the high dosage of the patient. We speculated that the main reason for warfarin resistance in this patient was poor absorption and/or rapid metabolism/elimination pathway. Further investigation is required to fully characterize the pharmacogenomics and pharmacodynamics genotype determinants of warfarin dose-response.
Declaration of Institution Approval
This study was approved to publish the case details by our hospital.
Acknowledgments
Written informed consent to publish this case report was obtained from the patient and her family member. The reason why we let the patient and her family member sign the informed consent is the dose of warfarin was very high and exceeded many times more than the traditional dosage. That dosage would greatly increase the bleeding risk. In order to ensure the patient takes the drug and adheres to it, we obtained the consent of the patient and her family member who was in charge of taking care of the patient in hospital.
We thank our colleagues Xiaoxue Wang and Wangjun Qin at the Department of Pharmacy, China-Japan Friendship Hospital, Beijing, China. We also thank Professor Zhenguo Zhai from the Department of Respiratory and Critical Care Medicine, Center for Respiratory Diseases, China-Japan Friendship Hospital, China for their continuous help support.
Funding
This study was supported by the National Key Research and Development Program of China (Grant No. 2020YFC2005504) and Capital’s Funds for Health Improvement and Research (Gant No. CFH-2020-1-2031).
Disclosure
The authors declare no conflict of interest.
References
1. Pengo V, Denas G, Zoppellaro G, et al. Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome. Blood. 2018;132(13):1365–1371. doi:10.1182/blood-2018-04-848333
2. John WE, Stuart JC, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med. 2013;396(13):1206–1220. doi:10.1056/NEJMoa1300615
3. Ageno W, Gallus AS, Wittkowsky A, et al. Oral anticoagulant therapy—antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2):e44–e88. doi:10.1378/chest.11-2292
4. Voora D, McLeod HL, Eey C, Gage BF. The pharmacogenetics of coumarin therapy. Pharmacogenomics. 2005;6(5):503–513. doi:10.2217/14622416.6.5.503
5. Shen AY, Yao JF, Brar SS, Jorgensen MB, Chen W. Racial/ethnic differences in the risk of intracranial hemorrhage among patients with atrial fibrillation. J Am Coll Cardiol. 2007;50(4):309–315. doi:10.1016/j.jacc.2007.01.098
6. Dang MT, Hambleton J, Kayser SR. The influence of ethnicity on warfarin dosage requirement. Ann Pharmacother. 2005;39(6):1008–1012. doi:10.1345/aph.1E566
7. Fohner AE, Robinson R, Yracheta J, et al. Variation in genes controlling warfarin disposition and response in American Indian and Alaska Native people: CYP2C9, VKORC1, CYP4F2, CYP4F11, GGCX. Pharmacogenet Genomics. 2015;25(7):343–353. doi:10.1097/FPC.0000000000000143
8. Limdi NA, Wadelius M, Cavallari L, et al. Warfarin pharmacogenetics: a single VKORC1 polymorphism is predictive of dose across 3 racial groups. Blood. 2010;115(18):3827–3834. doi:10.1182/blood-2009-12-255992
9. Lefrere JJ, Horellou MH, Conard J, Samama M. Proposed classification of resistance to oral anticoagulant therapy. J Clin Pathol. 1987;40(2):242. doi:10.1136/jcp.40.2.242-c
10. Osinbowale O, Al Malki M, Schade A, Bartholomew JR. An algorithm for managing warfarin resistance. Cleve Clin J Med. 2009;76(12):724–730. doi:10.3949/ccjm.76a.09062
11. Loebstein R, Dvoskin I, Halkin H, et al. A coding VKORC1 Asp36Tyr polymorphism predisposes to warfarin resistance. Blood. 2007;109(6):2477–2480. doi:10.1182/blood-2006-08-038984
12. Yuan HY, Chen JJ, Lee MT, et al. A novel functional VKORC1 promoter polymorphism is associated with inter-individual and inter- ethnic differences in warfarin sensitivity. Hum Mol Genet. 2005;14(13):1745–1751. doi:10.1093/hmg/ddi180
13. Aklillu E, Leong C, Loebstein R, Halkin H, Gak E. VKORC1 Asp36Tyr warfarin resistance marker is common in Ethiopian individuals. Blood. 2008;111(7):3903–3904. doi:10.1182/blood-2008-01-135863
14. Sabol BJ, Basa RR, Wilkins CE. Malabsorption-associated warfarin resistance. Am J Health Syst Pharm. 2009;66(17):1548–1553. doi:10.2146/ajhp080477
15. Bodin L, Perdu J, Diry M, et al. Multiple genetic alterations in vitamin K epoxide reductase complex subunit 1 gene (VKORC1) can explain the high dose requirement during oral anticoagulation in humans. J Thromb Haemost. 2008;6(8):1436–1439. doi:10.1111/j.1538-7836
16. Haiying WANG, Zhicheng JIN, Congjian LI, et al. A case report of warfarin resistance in a patient with pulmonary embolism and literature review. Chin J Cardiol. 2004;32(11):1039–1040.
17. Nikkila EA, Pelkonen R. Serum lipid-reducing agents and anticoagulant requirement. Lancet. 1963;1(7276):332. doi:10.1016/S0140-6736(63)92283-9
18. Hata M, Shiono M, Akiyama K1, et al. Incidence of drug interaction when using proton pump inhibitor and warfarin according to cytochrome P450 2C19 (CYP2C19) genotype in Japanese. Thorac Cardiovasc Surg. 2015;63(1):45–50. doi:10.1055/s-0034-1383814
19. Mott FE, Murphy S, Hunt V. Ciprofloxacin and warfarin. Ann Intern Med. 1989;111(6):542–543. doi:10.7326/0003-4819-111-6-542_2
20. Kamada AK. Possible interaction between ciprofloxacin and warfarin. DICP Ann Pharmacother. 1990;24(1):27–28. doi:10.1177/106002809002400106
21. Health Canada. Fluoroquinolones and warfarin: suspected interaction. Can Adverse React News. 2004;14(3):1–2. doi:10.2165/00128415-200410100-00003
22. Chock AWY, Stading JA. Indeterminable international normalized ratio with concurrent use of warfarin and gatifloxacin. Am J Health Syst Pharm. 2006;63(16):1539–1542. doi:10.2146/ajhp060021
23. Jones CB, Fugate SE. Levofloxacin and warfarin interaction. Ann Pharmacother. 2002;36(10):1554–1557. doi:10.1345/aph.1C074
24. Ieiri I, Tainaka H, Morita T, et al. Catalytic activity of three variants (Ile, Leu, and Thr) at amino acid residue 359 in human CYP2C9 gene and simultaneous detection using single-strand conformation polymorphism analysis. Ther Drug Monit. 2000;22(3):237–244. doi:10.1097/00007691-200006000-00001
25. D’Ambrosio RL, D’Andrea G, Cafolla A, et al. A new vitamin K epoxide reductase complex subunit-1 (VKORC1) mutation in a patient with decreased stability of CYP2C9 enzyme. J Thromb Haemost. 2007;5(1):191–193. doi:10.1111/j.1538-7836.2006.02261.x
26. Rettie AE, Tai G. The pharmacogenomics of warfarin: closing in on personalized medicine. Molec Interve. 2006;6(4):223–227. doi:10.1124/mi.6.4.8
27. Rost S, Fregin A, Ivaskevicius V, et al. Mutations in the VKORC1 cause warfarin resistance and multiple coagulation factor deficiency type 2. Nature. 2004;427(6974):537–541. doi:10.1038/nature02214
28. Kurnik D, Qasim H, Sominsky S, et al. Effect of the VKORC1 D36Y variant on warfarin dose requirement and pharmacogenetic dose prediction. Thromb Haemost. 2012;108(4):781–788. doi:10.1160/TH12-03-0151
29. Mitchell C, Gregersen N, Krause A. Novel CYP2C9 and VKORC1 gene variants associated with warfarin dosage variability in the South African black population. Pharmacogenomics. 2011;12(7):953–963. doi:10.2217/pgs.11.36
30. Isabel Anton A, Cerezo-Manchado JJ, Padilla J, et al. Novel associations of VKORC1 variants with higher acenocoumarol requirements. PLoS One. 2013;8(5):e644469. doi:10.1371/journal.pone.0064469
31. Kimura R, Miyashita K, Kokubo Y, et al. Genotypes of vitamin K epoxide reductase, gamma-glutamyl carboxylase, and cytochrome P450 2C9 as determinants of daily warfarin dose in Japanese patients. Thromb Res. 2007;120(7):181–186. doi:10.1016/j.thromres.2006.09.007
32. Stromich JJ, Weber AK, Mirzaei YR, et al. New adjuvants to enhance anticoagulant activity of warfarin. Bioorg Med Chem Lett. 2010;20(5):1928–1932. doi:10.1016/j.bmcl.2010.01.123
33. Vanakker OM, De Coen K, Costrop L, et al. Functional polymorphism in gamma-glutamylcarboxylase is a risk factor for severe neonatal hemorrhage. J Pediatr. 2011;159(2):347–349. doi:10.1016/j.jpeds.2011.04.044
34. Wadelius M, Chen LY, Downes K, et al. Common VKORC1 and GGCX polymorphisms associated with warfarin dose. Pharmacogenomics J. 2005;5(4):262–270. doi:10.1038/sj.tpj.6500313
35. Rieder MJ, Reiner AP, Rettie AE. Gamma-glutamyl carboxylase (GGCX) tagSNPs have limited utility for predicting warfarin maintenance dose. J Thromb Haemost. 2007;5(11):2227–2234. doi:10.1111/j.1538-7836.2007.02744.x
36. Weston BW, Monahan PE. Familial deficiency of vitamin K-dependent clotting factors. Haemophilia. 2008;14(6):1209–1213. doi:10.1111/j.1365-2516.2008.01853.x
37. Schelleman H, Brensinger CM, Chen J, et al. New genetic variant that might improve warfarin dose prediction in African Americans. Br J Clin Pharmacol. 2010;70(3):393–399. doi:10.1111/j.1365-2125.2010.03709.x
38. XiayizhaKamali M, Yang Y-C, Yang Y-C, et al. Association of GGCX gene polymorphism with warfarin dose in atrial fibrillation population in Xinjiang. Lipids Health Dis. 2013;12:149–154. doi:10.1186/1476-511X-12-149
39. McDonald MG, Rieder MJ, Nakano M, Hsia CH, Rettie AE. Cyp4F2 is a vitamin K1 oxidase: an explanation for altered warfarin dose in carriers of the V433m variant. Mol Pharmacol. 2009;75(6):1337–1346. doi:10.1124/mol.109.054833
40. Caldwell MD, Awad T, Johnson JA, et al. CYP4F2 genetic variant alters required warfarin dose. Blood. 2008;111(8):4106–4112. doi:10.1182/blood-2007-11-122010
41. Sagrieya H, Berube C, Wen A, et al. Extending and evaluating a warfarin dosing algorithm that includes CYP4F2 and pooled rare variants of CYP2C9. Pharmacogenet Genomics. 2010;20(7):407–413. doi:10.1097/FPC.0b013e328338bac2
42. Borgiani P, Ciccacci C, Forte V, et al. CYP4F2 genetic variant (rs2108622) significantly contributes to warfarin dosing variability in the Italian population. Pharmacogenomics. 2009;10(2):261–266. doi:10.2217/14622416.10.2.261
43. Takeuchi F, McGinnis R, Bourgeois S, et al. A genome-wide association study confirms VKORC1, CYP2C9, and CYP4F2 as principal genetic determinants of warfarin dose. PLoS Genet. 2009;5(3):e1000433. doi:10.1371/journal.pgen.1000433
44. Klein TE, Altman RB, Eriksson N, et al; International Warfarin Pharmacogenetics Consortium. Estimation of the warfarin dose with clinical and pharmacogenetic data. N Engl J Med. 2009;360(8):753–764. doi:10.1056/NEJMoa0809329
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.