")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Once-Daily Abrocitinib for the Treatment of Moderate-to-Severe Atopic Dermatitis in Adults and Adolescents Aged 12 Years and Over: A Short Review of Current Clinical Perspectives
Authors Niculet E , Bobeica C , Stefanopol IA , Pelin AM , Nechifor A , Onisor C , Tatu AL
Received 13 January 2022
Accepted for publication 30 March 2022
Published 13 April 2022 Volume 2022:18 Pages 399—407
DOI https://doi.org/10.2147/TCRM.S338661
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Elena Niculet,1,2,* Carmen Bobeica,1 Ioana Anca Stefanopol,1,3 Ana Maria Pelin,4,* Alexandru Nechifor,2,5,* Cristian Onisor,1,* Alin Laurentiu Tatu2,4,5
1Department of Morphological and Functional Sciences, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, Galați, Romania; 2Multidisciplinary Integrated Center of Dermatological Interface Research MIC-DIR (Centrul Integrat Multidisciplinar de Cercetare de Interfata Dermatologica - CIM-CID), ‘Dunărea de Jos’ University, Galați, Romania; 3Department of Pediatrics, Clinical Emergency Hospital for Children “Sf. Ioan”, Galati, Romania; 4Department of Pharmaceutical Sciences, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, Galați, Romania; 5Dermatology Department, “Sf. Cuvioasa Parascheva” Clinical Hospital of Infectious Diseases, Galați, Romania
*These authors contributed equally to this work
Correspondence: Carmen Bobeica; Ioana Anca Stefanopol, Department of Morphological and Functional Sciences, Faculty of Medicine and Pharmacy, Dunărea de Jos University, Galați, 800008, Romania, Tel +40744368150 ; +40 744 222 488, Email [email protected]; [email protected]
Abstract: Atopic dermatitis (AD) is a chronic inflammatory skin disorder with high prevalence and a complex pathophysiology. This relapsing and remitting skin disorder has many negative consequences on the patient’s quality of life and that of his family. Until now, moderate-to-severe AD treatment was a symptomatic one, using skin emollients, topical corticosteroids, phototherapy, antihistamines and systemic drugs – immune suppressants and other systemic treatments (dupilumab). Starting from 2021, abrocitinib, a Janus kinase-1 inhibitor, was approved for the treatment of moderate-to-severe cases of AD in Europe, in adults. Multiple phase three studies (JADE MONO-1 [NCT03349060]; JADE MONO-2 [NCT03575871]; JADE TEEN [NCT03796676]; JADE COMPARE; GOODERHAM; JADE EXTEND) have yielded positive results in adults and adolescents suffering from this disease, with efficacy, a good tolerance, safe profile, and with generally mild side effects. The positive results were obtained even starting from the first stages of the oral drug administration. The low frequency of side effects and the advantage of having an orally administered medication makes abrocitinib an important additional tool for the treatment of moderate-to-severe forms of AD.
Keywords: abrocitinib, atopic dermatitis, adolescents, JADE, JADE-MONO
Introduction
Atopic dermatitis (AD) is a highly frequent chronic inflammatory skin disorder, affecting all skin types, and is clinically described as “eczema”, having a heterogeneous pathophysiology not yet understood due to its elevated complexity.1,2 The necessary diagnostic biomarkers for this world-wide disease have not yet been developed.3 The prevalence of AD can reach up to 3% to 10% of the adult population and even 25% of the pediatric population in countries, such as the United States of America (USA) or it can even manifest as a worldwide phenomenon.4 In Europe, AD has a particular prevalence, with higher numbers of patients affected in the north than south, and more in the urban areas than the rural ones, with the highest number of affected patients found in the pediatric population than the adult ones. More patients with higher level of education and socioeconomic status have this disease, with the highest number of affected children found in Denmark, while the highest numbers among the adult population can be found in Estonia.5 AD frequently develops during childhood, more than half of the patients (approximately 60%) developing it under 1 year of age, almost 90% of them up 5 years of age and 10% as adults.6
Factors which are considered to be involved in AD development are as follows: the patient’s genetic predispositions (such as filaggrin mutations which are involved in the skin’s barrier function, with pro-inflammatory properties, and/or interleukin-13 (IL-13) and ovo like transcriptional repressor 1 – OVOL1 gene mutations which in turn regulate the expression of filaggrin),1,4,7,8 disruption in the skin barrier, skin microbiota dysbiosis (Staphylococcus aureus colonization – AD relapses were found to be linked to with an increased colonization of Staphylococcus aureus, which reduces the skin’s bacterial diversity), dysregulation of the immune system (hay fever, asthma, allergies), disturbances in the skin’s innate immunity, environmental factors (such as exposure to elevated levels of ambient nitrogen dioxide – NO2 in the first year of life, climate), climate or the patient’s diet.1,4,7
The patients describe this eczematous, relapsing and remitting skin lesion as being intensely pruritic, suffering from multiple flares, having negative consequences on the patient’s quality of life and that of his family and other caretakers.4,9 AD is the type of disease that not only does it bring physical and economical costs but it also has substantial psychological and social impacts.10 Due to the nature of this disease, it is frequently associated with sleep disturbances, anxiety, depression, pain, work absenteeism and higher healthcare addressing.11,12
Although there is no serologic marker for diagnosing AD patients, the clinical signs and symptoms (dry skin, pruritus, excoriations, serous exudate, lichenification), associated with the patient’s personal and family history, and the exclusion of other inflammatory skin diseases, make the positive diagnosis of AD.5
The main objectives of the current work all stem from revealing the beneficial effects of JAK inhibitors on cases of moderate-to-severe AD. This article aims at describing the current treatment options for such cases, the JAK-inhibitor activity, the new abrocitinib medication and the results yielded from several clinical studies which included moderate-to-severe AD patients.
Materials and Methods
The current work is a narrative review type of article, using materials that are new and updated, such as articles from 2021, 2020, 2019, but not earlier than 2017. Database searches were done using Google Scholar and Web of Science, using keywords such as “abrocitinib”, “once daily abrocitinib”, “abrocitinib” and “adolescents” or “adults” combined: “abrocitinib moderate-to-severe atopic dermatitis”, generating the current work after disregarding duplicates in writing and after selection of the most representative and work-related articles (Figure 1, Tables 1 and 2).
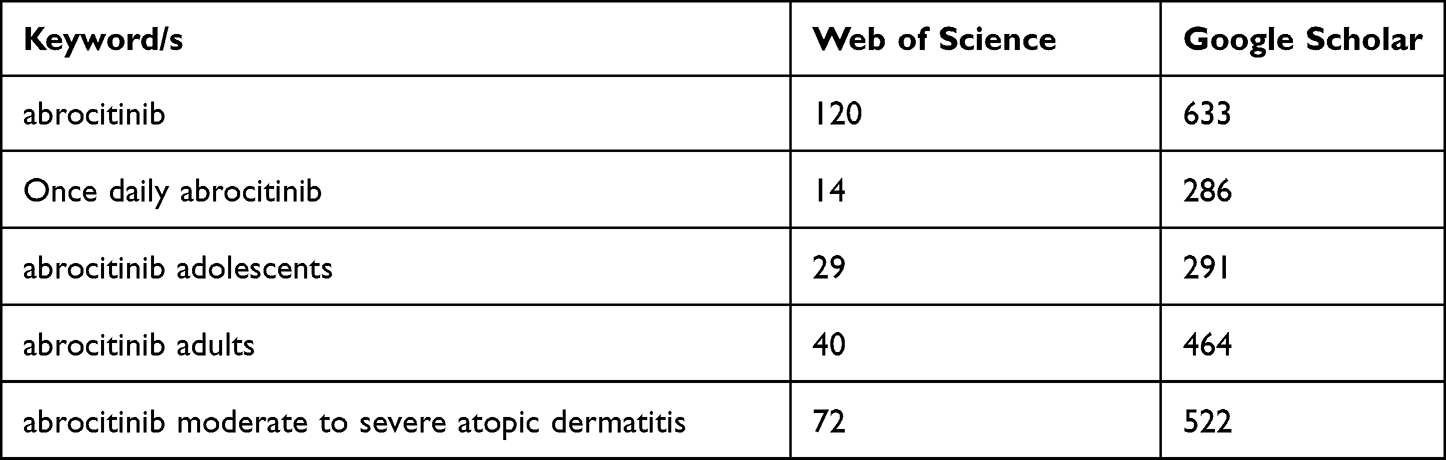 |
Table 1 Keywords/Key Phrases Used in Initial Database Search and Articles Found |
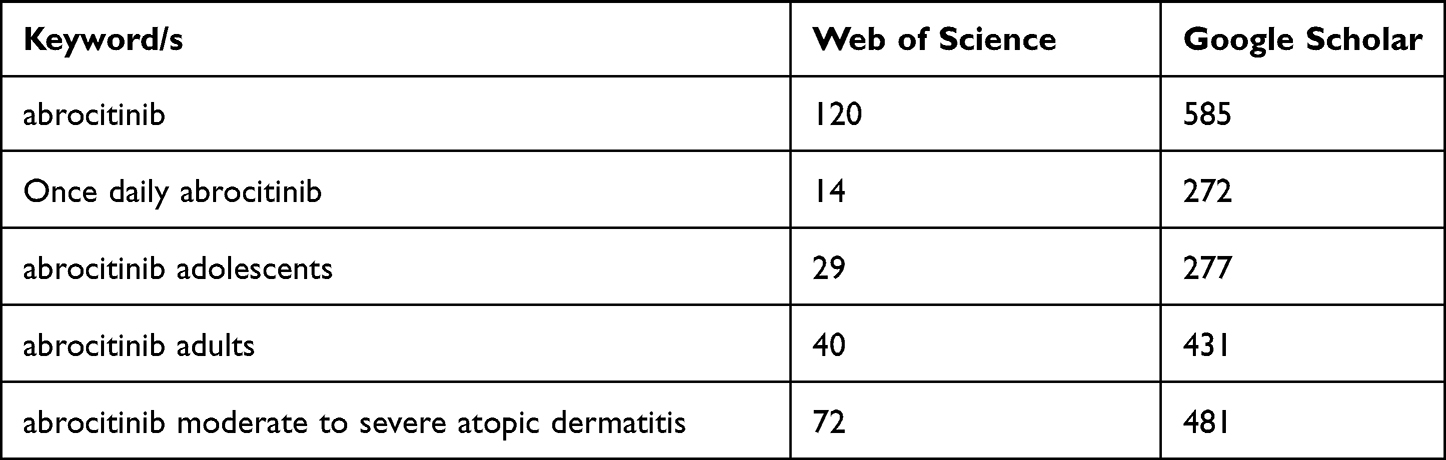 |
Table 2 Second Step of Database Search Which Included Articles Published Only Since 2017 |
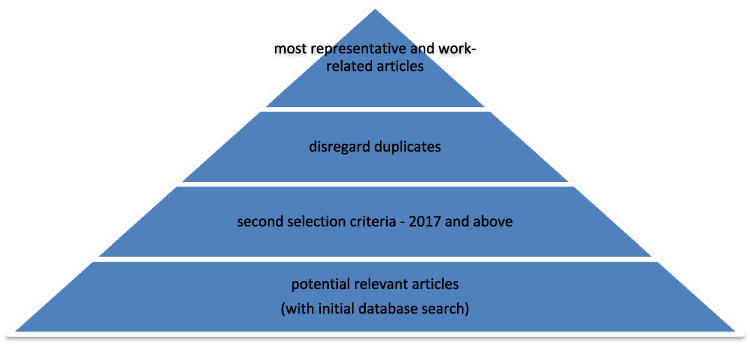 |
Figure 1 Prism flow diagram with article selection process steps. |
Results and Discussions
AD treatment benefitted from a classical (albeit insufficient) therapeutic approach: a symptomatic one, using emollients/moisturizers (which help avoid skin dryness), topical corticosteroids (to reduce skin erythema and edema), antihistamines (to reduce intense episodes of pruritus), phototherapy or systemic treatments such as immune suppressors or other systemic agents (such as dupilumab – a monoclonal antibody, as subcutaneous injections).4,9–11
Systemic treatment is currently used in those moderate-to-severe AD cases in which topical treatment has failed or has been highly used, immune suppressant agents having a rather modest disease response to many adverse events.11,13 Cyclosporine is an example of an immunosuppressive drug, which has been approved and is currently used in Europe for severe cases of AD, but with low tolerance rates and multiple adverse events; however, it has an efficacy rate of almost 95% with short-term treatments. Other immune suppressors which can be used are as follows: azathioprine (selective use; it is considered to be a second-line medication for adults, after cyclosporine, having the risk of bone marrow suppression), methotrexate (selective use, having similar efficacy to azathioprine; it is considered a second-line treatment in pediatric and adult cases of moderate-to severe AD, after cyclosporine), mycophenolate mofetil (it has low recommendation evidence levels; prolonged treatment presents the risk of herpes infection).12,14 Dupilumab, an anti–IL-4–receptor α mono-clonal antibody which is approved by both the Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for use in moderate-to-severe cases of AD in adolescents and adults, has the capacity to bind to the shared α-chain receptor of both IL-4 and IL-13, having a partial limiting effect on the inflammation driven by the Th2 activity.11–13 Thus being said, although many patients benefitted from it (with total response and/or no side effects), it might have limited use because not all patients respond to this treatment, they can present a partial response to it, they can develop tolerance or might not even want it due to its administering pathway (subcutaneous injections); it also determines injection site adverse reactions, neck and/or face erythema, conjunctivitis.11–13
AD treatment deals with the frequent skin flares, secondary infections and recurrence prevention; also, important are avoidance of the aggravating factors and gentle skin cleansing.8 Unfortunately, due to the nature of AD, especially in moderate-to-severe forms, treatment needs to be flexible, adapting the dosage and the nature of administered drugs, trying to obtain the best benefit-to-risk ratio.4,9
Recent medical research has yielded a new type of AD medication called Janus kinase-1 (JAK) inhibitors [part of the DMARDs (disease-modifying antirheumatic drugs) family, with the JAK-1, JAK-2, JAK-3 and tyrosine kinase-2 – TYK-2 molecules] which (from a pharmacological viewpoint) are small molecular (synthetic) compounds that inhibit the intracellular transduction of the signal derived from the cell’s cytokine receptors.4,6 Cytokines such as IL-1, 2, 4, 5, 13, 22, 31, stromal thymic lymphopoietin, interferon-γ are involved in AD’s pathologic process; JAK inhibitors exert their activity by cytokine receptor phosphorylation (an inhibiting action), which in turn modifies the immune response (by decreasing it).4,6,9,10 In its etiopathogenic complexity, AD derives from T helper 2 (Th2) immune reactions (important in developing the pruritus symptom, due to cytokines, such as IL-4, IL-13 and IL-31); chronic cases of AD, or those found in Asian patients, particularly have a Th17 and Th22 immune profiles.15,16 They are in essence a group of cytoplasmic tyrosine kinases, which aid in mediating the signaling pathways that are cytokine-activated and inhibit them.10 JAK-1 activity is not only associated with the development of AD but it also plays a role in the pathophysiology of other inflammatory/immunologic skin disorders, such as psoriasis, dermatomyositis, vitiligo, pruritus, lichen sclerosus, granuloma annulare, alopecia areata, sarcoidosis, lichen planus, morphea and, possibly, Multiple Autoimmune Syndrome (MAS).6,17–20 Statins are agents which have a new potential for being used in the treatment of alopecia areata by modulating the JAK/STAT pathway; they can also be used in combination with a JAK inhibitor, ensuring lower necessary doses of the latter for the same therapeutic effect, thus avoiding the possible complications or side effects when using higher dosages, as in the case of myeloproliferative neoplasms.21–23
Abrocitinib is part of the JAK-1 inhibitor class, currently being investigated for the use in cases of moderate-to-severe AD, which did not have a proper response to the use of topical treatment. Phase 3 studies have yielded beneficial responses in adolescents and adults who received abrocitinib once a day in doses of 200 mg or 100 mg, improving the eczema’s severity, area and pruritus. It has a general safe profile and can be used in combination with topical AD treatment, being effective and well tolerated in the adolescent and adult populations.9 Reports are encouraging for cases of moderate-to-severe AD that were treated with topical or oral JAK-1 inhibitors (anti-JAK1);10 abrocitinib use was found to have a lesser likelihood of stimulating an immunogenic response, in comparison to biologic treatment.11 Currently, the opportunity to use anti-JAK1 topically for AD (also known as atopic eczema) treatment is also investigated, targeting agents such as ruxolitinib and delgocitinib.6 The life-long AD course requires that anti-JAK1 be thoroughly investigated in order to discover their benefit-to-harm ratio so that they can be prescribed to patients with intermittent relapses.24
Once-daily, orally administered abrocitinib was reported by multiple studies to make possible the selective and reversible inhibition of JAK-1, highlighting its efficacy, good tolerance and positive results in adolescents and adults suffering from moderate-to-severe AD (such as: JADE MONO-1 [NCT03349060]; JADE MONO-2 [NCT03575871]; JADE TEEN [NCT03796676]; JADE COMPARE; GOODERHAM; JADE EXTEND – with not yet available results), in combination with topical therapy or not;13,15,24,25 it also has the advantage of not exerting effects on JAK2 (by not inhibiting it), significantly lowering the risk of developing anemia and neutropenia. Pruritus, a major AD symptom, improved after neuronal JAK1 pathway inhibition.13 Studies with combination therapy (anti-JAK1 and topical corticosteroids) had a higher level of difficulty of interpreting the results obtained, due to the additional dilemma of discerning which drug exerted the positive effects on AD lesions.24
Abrocitinib in Adolescents (>12 Years Old)
Adolescents suffering from AD have a higher probability to suffer from mental health problems and psychosocial ones, with sleep disturbances (troubles falling asleep, nighttime awakenings, and daytime drowsiness – as a consequence), anxiety, depression, interpersonal relationship problems, or even physical activity interferences.26
In adolescents (aged 12- to 17-year olds) suffering from moderate-to-severe AD, three phase three clinical studies (JADE TEEN [NCT03796676]; JADE MONO-1 [NCT03349060]; JADE MONO-2 [NCT03575871]) have found abrocitinib (administered as monotherapy or as combination therapy) to be effective in improving the clinical signs and symptoms, with amelioration in sleeping patterns and overall quality of life improvement.26–28 The patients were assigned to randomly to receive abrocitinib once a day in doses of either 100 mg or 200 mg, in combination with topical corticosteroids or as monotherapy, JADE TEEN, or, JADE MONO-1 and 2, respectively. All of the studies were conducted in 2017, 2018, 2019 and 2020, respectively. In JADE TEEN, the topical medication which was allowed to be used consisted of medium potency corticosteroids (on appropriate body areas), low potency corticosteroids (on thin-skin body areas, such as the face, neck, genital areas, intertriginous ones, or areas with skin atrophy) due to the known adverse effects of potent dermatologic corticosteroids; other types of medications were accepted for use, such as topical calcineurin inhibitors or phosphodiesterase inhibitors, in specially selected areas such as those with thinned skin suffering from active lesions, or in special cases where the topical corticosteroids were considered unsafe for patient use. JADE MONO −1/-2 also involved patients under 18 years of age (12 to 17, included), heavily burdened by the signs and symptoms of the moderate-to-severe AD, and were allowed topical emollients, but as permitted medication, not a required one.26,29
These studies gave patient-reported outcomes, such as: patient-oriented eczema measure (POEM), children’s dermatology life quality index (CDLQI), pruritus and symptoms assessment for atopic dermatitis (PSAAD), the night-time itch scale (NTIS) and SCORing Atopic Dermatitis (SCORAD) Visual Analog Scale (VAS) sleep loss. These self-reporting scales for pediatric patient use gave significant results when changes registered at least 6 points of improvement in the case of POEM and CDLI, which reflect the frequency of signs and symptoms reported a week prior, and, respectively, the effects that moderate-to-severe AD has on the quality of life of the patient also in the past week. PSAAD reports the patient’s symptoms in the last 24 hours, while NTIS reports the worst itching during the most recent sleep during the night and while SCORAD reports sleep loss during the last 3 nights prior to the evaluation.26,27,30
POEM revealed to register high levels of improvement (at least 6 points) in JADE TEEN, JADE MONO-1 and -2, the abrocitinib groups having better results than the placebo one, or the abrocitinib 200 mg groups yielding better improvement than the groups who received abrocitinib 100 mg, respectively. These results were found even from the beginning of week 2. The achieved score was clear/almost clear or mild, ranging from 0 to 7.26,27,30
The CDLQI reflects a better response to treatment when patients report higher scores, thus a higher impact in moderate-to-severe AD; all three studies revealed that abrocitinib had a “very large effect” on these patients, with the 200 mg dosage yielding better results.26,27
PSAAD includes 11 items to be reported and ranges from the least severe symptom – 0, to the most severe one – 10, with a significant clinical response being considered even a one-point difference. The best results were obtained with a 200 mg dose of abrocitinib in all clinical studies, decreasing in effectiveness with the use of the 100 mg dose, as compared to the placebo group.26
NTIS assesses the severity of the itchiness, ranging from 0 to 10, from “no itch” to “worst itch imaginable”. JADE TEEN and JADE MONO-2 revealed a minimum of 4 points improvement compared to the baseline, with better results being reported for abrocitinib at 200 mg/dose, even from week 2 of treatment. The JADE MONO-1 clinical trial did not report on NTIS.26
SCORAD VAS sleep loss scale ranges from none – 0 to worst – 10, all of the three JADE studies reporting lower values for both of the abrocitinib groups, in comparison to the placebo ones, even at week 2 of treatment. The patients reported reduced depression symptoms, decreased anxiety and fatigue.26,27
The reported findings from the first phase three trial, JADE TEEN, were confirmed by the adolescent subpopulation of the other 2 JADE trials (MONO – 1/-2). The promising results, which were reported at week 2, were maintained even at week 12 of these studies. JADE TEEN reported a high “placebo effect”, but it might most likely be due to a high adherence to topical therapeutics, as compared to the daily clinic experience; the pediatric population also has an immature function of the skin barrier, thus increasing the patients’ systemic exposure to topical drugs and increasing the positive results in the “placebo” group.26
Abrocitinib in Adults
JADE COMPARE, a phase 3 placebo-controlled trial, which included adults suffering from moderate-to-severe forms of AD and who received doses of 200 mg or 100 mg of oral abrocitinib daily, is one of the studies, which rendered abrocitinib useful for the systemic treatment of AD.28,31–33 The safety profile of this small molecule with selective anti-JAK1 properties, abrocitinib, was found to be similar to that reported by other studies, demonstrating a fast improvement in the patient’s signs and symptoms. This clinical study had a background in topical treatment (low or medium potency corticosteroids, calcineurin inhibitors, phosphodiesterase-4 inhibitors) that was applied to the active lesions, continuing for 7 days after they were under control. The efficacy of abrocitinib was compared continuously during the study with the results of dupilumab’s activity on AD lesions. Improvement was rapidly registered with both oral doses of abrocitinib (200 mg and 100 mg) as compared to the placebo patients, even as early as week 2 of treatment. Better results were found later during treatment, in between the 12th to 16th weeks of 200 mg abrocitinib, as compared to the 100 mg per dose patients or dupilumab patients.30–33
A systematic review done by Le et al revealed that three phase three clinical studies (Bieber et al, Simpson et al, Silverberg et al) have also evaluated adults with moderate-to-severe forms of AD. These studies used the following criteria for evaluation: the Eczema Area and Severity Index (EASI) score (with a baseline of at least 16), the Investigator’s Global Assessment score (IGA, baseline = at least 3), the Body Surface Area (BSA, baseline = at least 10% of body surface affected) and the peak pruritus numeric rating scale (PP-NRS, baseline = at least 4). After 16 weeks of treating the patients (12 weeks and, respectively, 12 weeks), this study revealed similar results. Most adults (71%, 63% and, respectively, 61% of them) from these randomized, phase three trials, who were treated with abrocitinib 200 mg per dose, had the best results, obtaining an Eczema Area and Severity Index (EASI)-75 score, meaning a 75 reduction from baseline in the EASI score. At a decreasing frequency, EASI-75 was also found in most patients treated with abrocitinib 100 mg per dose and, respectively, those treated with dupilumab. An IGA score of 0 or 1 (meaning, clear to almost clear) with an improvement of ≥2 grades from baseline and a PP-RNS improvement of at least 4 points from baseline were necessary in order for the drug to be considered as clinical effective, and the results found concerning these items reflected those of the EASI score, meaning that abrocitinib in 200 mg doses registered the best results, with decreasing efficacy for abrocitinib 100 mg per dose and, respectively, dupilumab.8,13,27,30,34,35 These changes were also registered in a phase IIb trial, which included adult patients suffering from moderate-to-severe forms of AD, and also reporting better results for the 200 mg per dose oral abrocitinib, for all patient-reported outcomes.30,33,35
The most significant and frequent patient-reported symptom of AD is pruritus; abrocitinib studies (including a Phase 2b one) reflected important improvement, alleviating this daily manifestation, along with other symptoms (dryness, bleeding, redness, and so on), possibly through the inhibition of a common cytokine. The studies taken into account have differences concerning their design, the degree of baseline severity, the population characteristics and the duration of treatment, and their direct comparison is truly limited, but the overall patient improvement is highlighted by all.8,13,34,36
An integrated safety analysis study done by Simpson et al found that abrocitinib has a long-term safe profile, being tolerated by moderate-to-severe AD patients that are selected for this type of treatment (both adults and adolescents); the most frequent dose-related and drug-related reported side effects (Table 3) were mild, non-lethal ones, more frequently located at the respiratory and/or gastrointestinal level, such as: headaches, dizziness, nasopharyngitis, symptoms of upper respiratory tract infection, epigastric pain, nausea, vomiting, creatine phosphokinase increase (CK increase without rhabdomyolysis), folliculitis and acne, all with mild or moderate intensity;8,37,38 herpes zoster infection was found occurring with a higher frequency in patients receiving 200 mg of abrocitinib in daily oral doses. These adverse effects were self-limited and treatment rarely required interruption or even permanent discontinuation. Severe adverse events were also reported, which were considered treatment-related: eczema herpeticum, herpangina and pneumonia (in 100 mg abrocitinib receiving patients), acute pancreatitis, chronic inflammatory bowel disease; in 200 mg abrocitinib receiving patients lowered platelet counts were registered, some patients even suffering from thrombocytopenia.8,9,13,37
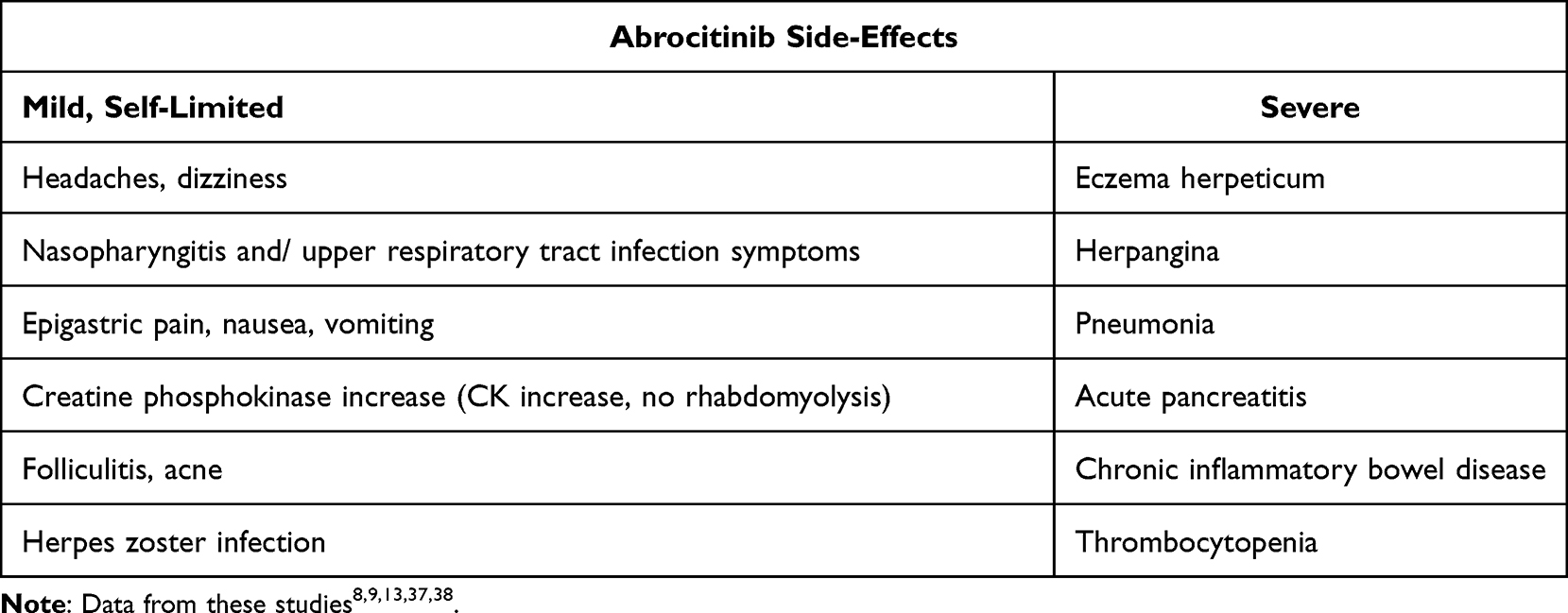 |
Table 3 Abrocitinib Side Effects |
In the studies already mentioned in this review, anti-JAK1 agents (such as: abrocitinib, upadacitinib) have shown to have better results than dupilumab, but with higher rates of adverse events, these result being in accordance with results published prior in the specialty literature. An important setback is that some studies have not separated the results according to the adult and the adolescent population; those studies which have published their results according to the patient population have found similar results between the two.24
A recent study has found that abrocitinib use was generally safe for use and well tolerated, but in patients suffering from moderate and severe renal function impairment, the drug’s active moiety was higher, proving the need for lowering by half the dosage of abrocitinib in such high-risk patients.39
In all of these studies, abrocitinib in doses of 100 mg (combined with topical corticosteroids) resulted in having the safest profile in what concerns adverse effects (including severe ones), upper tract infections and withdrawal syndrome, even slightly better than using abrocitinib 200 mg in association with topical corticosteroids.9,24 Also, studies which evaluated the patients’ quality of life reported major progress, with improved work and an improved productivity (for patients in the work field), changes which were statistically significant for abrocitinib as compared to the placebo groups, even with or without topical corticosteroids.24,27 The Committee for Medicinal Products for Human Use of the European Medicines Agency supports the marketing authorization for abrocitinib in treating AD, a statement issued in October. Recently, in December 2021, abrocitinib was approved in Europe for the treatment of moderate-to-severe AD in the adult population (candidates for systemic treatment) in dosages of 100 mg and 200 mg per day; also, a dosage of 50 mg a day was approved for those suffering from moderate-to-severe renal impairment and for patients treated with P450 cytochrome inhibitors. The European Commission has approved the use of this systemic drug on the basis of the four phase three clinical trials which were taken into consideration in this review – JADE MONO-1 and MONO-2, JADE COMPARE and JADE REGIMEN, and also on an ongoing extension study named JADE EXTEND.40
Concerning the USA, abrocitinib is currently being reviewed by the FDA, all the while being approved in 2021 for AD treatment in Japan, the United Kingdom and Korea. Other countries, such as Australia, are also considering abrocitinib for AD treatment, and are reviewing the regulatory applications.41
Conclusion
Research done by comparing the efficacy and safety profile of various therapeutic agents (especially, but not only) on AD lesions, will prove useful for physicians in having treatment options, and consequently treatment will be adapted to the patient’s profile. Caution needs to be paid due to the fact that AD is a life-long disease which requires long-term treatment and research is limited in this matter. Given the existing evidence, the most satisfying results were found in moderate-to-severe AD patients treated with high doses of abrocitinib for short time periods, gaining rapid symptom control and having a general safe profile. The overall positive effects were obtained even from the first stages of oral drug administration. The low frequency of adverse effects and the convenience of having an oral administered drug makes abrocitinib an important additional tool for the treatment of moderate-to-severe forms of AD, besides agents such as dupilumab; thus being said, the data presented stemmed only from clinical trials and the true nature of abrocitinib use will reveal itself only by using it in the real world, with more studies on a higher number of patients, a trait which other systemic treatments such as dupilumab rejoices in.8,15,24
Abbreviations
AD, atopic dermatitis; USA, the United States of America; IL-13, interleukin-13; OVOL1 gene, ovo-like transcriptional repressor 1 gene; NO2, nitrogen dioxide; FDA, the Food and Drug Administration; EMA, the European Medicines Agency; JAK-1, Janus kinase-1 (JAK); DMARDs, disease-modifying antirheumatic drugs; TYK-2, tyrosine kinase-2 molecules; Th2, T helper 2; MAS, Multiple Autoimmune Syndrome; JAK/STAT pathway, the Janus kinase-signal transducer and activator of transcription pathway; anti-JAK1, Janus kinase-1 inhibitors; POEM, patient-oriented eczema measure; CDLQI, children’s dermatology life quality index; PSAAD, pruritus and symptoms assessment for atopic dermatitis; NTIS, the night-time itch scale (NTIS); SCORAD, SCORing Atopic Dermatitis; VAS, Visual Analog Scale; EASI, the Eczema Area and Severity Index; IGA, the Investigator’s Global Assessment score; BSA, the Body Surface Area; PP-NRS, the peak pruritus numeric rating scale; CK, creatine phosphokinase.
Data Sharing Statement
The information will be granted access to under reasonable request.
Acknowledgments
The authors wish to acknowledge that the present study was academically supported by the ‘Dunarea de Jos’ University of Galati, Romania, through the research center – Multidisciplinary Integrated Center of Dermatological Interface Research MIC-DIR (Centrul Integrat Multidisciplinar de Cercetare de Interfata Dermatologica – CIM-CID).
Author Contributions
EN, AMP, CO and ALT were involved in the conception of the study and had major contribution in the writing and revising of the manuscript. CB and IAS contributed to the acquisition, analysis and interpretation of the data. All authors have substantially revised and critically reviewed this article. All authors have agreed on the journal to which the article will be submitted and agreed to take responsibility and be accountable for the contents of the article. All authors reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
Funding
The article publishing charge was paid by the “Dunarea de Jos” University of Galati, Romania.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Crowley EL, Nezamololama N, Papp K, Gooderham MJ. Abrocitinib for the treatment of atopic dermatitis. Expert Rev Clin Immunol. 2020;16(10):955–962. doi:10.1080/1744666X.2021.1828068
2. Zhang L, Wang L, Jiang X. The efficacy of Janus kinase inhibitors in patients with atopic dermatitis: a systematic review and network meta-analysis. Dermatol Ther. 2021;34(5):e15098. doi:10.1111/dth.15098
3. Simpson EL, Bieber T, Thyssen JP, Valdez H, Rojo R. Abrocitinib for atopic dermatitis - Authors’ reply. Lancet. 2021;397(10270):196. doi:10.1016/S0140-6736(21)00037-4
4. Fadlalmola HA, Albadrani MS, Elhusein AM, Mohamedsalih WE, Swamy VDS, Mamanao DM. Effectiveness and safety of abrocitinib in patients with moderate-to-severe atopic dermatitis: a systematic review and meta-analysis of randomized clinical trials. Dermatol Res Pract. 2021;2021:8382761. doi:10.1155/2021/8382761
5. Kowalska-Olędzka E, Czarnecka M, Baran A. Epidemiology of atopic dermatitis in Europe. J Drug Assess. 2019;8(1):126–128. doi:10.1080/21556660.2019.1619570
6. Nezamololama N, Fieldhouse K, Metzger K, Gooderham M. Emerging systemic JAK inhibitors in the treatment of atopic dermatitis: a review of abrocitinib, baricitinib, and upadacitinib. Drugs Context. 2020;9:1–7. doi:10.7573/dic.2020-8-5
7. Nezamololama N, Crowley EL, Gooderham MJ, Papp K. Abrocitinib: a potential treatment for moderate-to-severe atopic dermatitis. Expert Opin Investig Drugs. 2020;29(9):911–917. doi:10.1080/13543784.2020.1804854
8. Le M, Berman-Rosa M, Ghazawi FM, et al. Systematic review on the efficacy and safety of oral janus kinase inhibitors for the treatment of atopic dermatitis. Front Med. 2021;8:682547. doi:10.3389/fmed.2021.682547
9. Blauvelt A, Silverberg JI, Lynde CW, et al. Abrocitinib induction, randomized withdrawal, and retreatment in patients with moderate-to-severe atopic dermatitis: results from the JAK1 Atopic Dermatitis Efficacy and Safety (JADE) REGIMEN phase 3 trial. JAAD. 2022;86(1):104–112. doi:10.1016/j.jaad.2021.05.075
10. Gooderham MJ, Forman SB, Bissonnette R, et al. Efficacy and safety of oral janus kinase 1 inhibitor abrocitinib for patients with atopic dermatitis: a Phase 2 randomized clinical trial. JAMA Dermatol. 2019;155(12):1371–1379. doi:10.1001/jamadermatol.2019.2855
11. Bieber T, Simpson EL, Silverberg JI, et al. Abrocitinib versus placebo or dupilumab for atopic dermatitis. N Engl J Med. 2021;384:1101–1112. doi:10.1056/NEJMoa2019380
12. Simpson EL, Sinclair R, Forman S, et al. Efficacy and safety of abrocitinib in adults and adolescents with moderate-to-severe atopic dermatitis (JADE MONO-1): a multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet. 2020;396(10246):255–266. doi:10.1016/S0140-6736(20)30732-7
13. Silverberg JI, Simpson EL, Thyssen JP, et al. Efficacy and safety of abrocitinib in patients with moderate-to-severe atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2020;156(8):863–873. doi:10.1001/jamadermatol.2020.1406
14. Lee JH, Kim JE, Park GH, et al. Consensus update for systemic treatment of atopic dermatitis. Ann Dermatol. 2021;33(6):497–514. doi:10.5021/ad.2021.33.6.497
15. Nakashima C, Yanagihara S, Otsuka A. Innovation in the treatment of atopic dermatitis: emerging topical and oral Janus kinase inhibitors. Allergol Int. 2021;71(1):40–46. doi:10.1016/j.alit.2021.10.004
16. Weidinger S, Schreiber S. Abrocitinib for atopic dermatitis: a step forward. Lancet. 2020;396(10246):215–217. doi:10.1016/S0140-6736(20)31284-8
17. Petronelli M, Petrou I. FDA warns about some JAK inhibitors. Dermatol Times. 2021;42(9):44–45.
18. Tatu AL, Ionescu MA. Multiple autoimmune syndrome type III- thyroiditis, vitiligo and alopecia areata. Acta Endo. 2017;13(1):124–125. doi:10.4183/aeb.2017.124
19. Brănișteanu DE, Pintilie A, Dimitriu A, et al. Clinical, laboratory and therapeutic profile of lichen planus. Med Surg J. 2017;121(1):25–32.
20. Tatu AL, Nwabudike LC The treatment options of male genital lichen sclerosus et atrophicus. Short title for a running head: treatments of genital lichen sclerosus.
21. Cervantes J, Jimenez JJ, DelCanto GM, Tosti A. Treatment of alopecia areata with simvastatin/ezetimibe. J Investig Dermatol Symp Proc. 2018;19(1):S25–S31. doi:10.1016/j.jisp.2017.10.013
22. Nwabudike LC, Elisei AM, Buzia OD, Miulescu M, Tatu AL. Statins. A review on structural perspectives, adverse reactions and relations with non-melanoma skin cancer. Rev Chim. 2018;69(9):2557–2562. doi:10.37358/RC.18.9.6575
23. Griner LN, McGraw KL, Johnson JO, List AF, Reuther GW. A mechanistic rationale for the use of statins to enhance JAK inhibitor therapy in MPNs. Blood. 2011;118(21):2816. doi:10.1182/blood.V118.21.2816.2816
24. Pereyra-Rodriguez JJ, Alcantara-Luna S, Domínguez-Cruz J, et al. Short-term effectiveness and safety of biologics and small molecule drugs for moderate to severe atopic dermatitis: a systematic review and network meta-analysis. Life. 2021;11(9):927. doi:10.3390/life11090927
25. Eichenfield LF, Flohr C, Sidbury R, et al. Efficacy and safety of abrocitinib in combination with topical therapy in adolescents with moderate-to-severe atopic dermatitis: the JADE TEEN randomized clinical trial. JAMA Dermatol. 2021;157(10):1165–1173. doi:10.1001/jamadermatol.2021.2830
26. Cork MJ, McMichael A, Teng J, et al. Impact of oral abrocitinib on signs, symptoms and quality of life among adolescents with moderate-to-severe atopic dermatitis: an analysis of patient-reported outcomes. J Eur Acad Dermatol Venereol. 2021;36(3):422–433.
27. Silverberg JI, Thyssen JP, Simpson EL, et al. Impact of oral abrocitinib monotherapy on patient-reported symptoms and quality of life in adolescents and adults with moderate-to-severe atopic dermatitis: a pooled analysis of patient-reported outcomes. Am J Clin Dermatol. 2021;22(4):541–554. doi:10.1007/s40257-021-00604-9
28. Traidl S, Freimooser S, Werfel T. Janus kinase inhibitors for the therapy of atopic dermatitis. Allergol Select. 2021;5:293–304. doi:10.5414/ALX02272E
29. Niculet E, Bobeica C, Tatu AL. Glucocorticoid-induced skin atrophy: the old and the new. Clin Cosmet Investig Dermatol. 2020;13:1041–1050. doi:10.2147/CCID.S224211
30. Ferreira S, Guttman-Yassky E, Torres T. Selective JAK1 inhibitors for the treatment of atopic dermatitis: focus on upadacitinib and abrocitinib. Am J Clin Dermatol. 2020;21(6):783–798. doi:10.1007/s40257-020-00548-6
31. Thyssen JP, Yosipovitch G, Paul C, et al. Patient-reported outcomes from the JADE COMPARE randomized phase 3 study of abrocitinib in adults with moderate-to-severe atopic dermatitis. J Eur Acad Dermatol Venereol. 2021;36(3):434–443.
32. Bieber T, Simpson EL, Silverberg JI, et al. Comparing abrocitinib and dupilumab in the treatment of atopic dermatitis: a plain language summary. Immunotherapy. 2021;14(1):5–14. doi:10.2217/imt-2021-0224
33. Napolitano M, Fabbrocini G, Ruggiero A, Marino V, Nocerino M, Patruno C. The efficacy and safety of abrocitinib as a treatment option for atopic dermatitis: a short report of the clinical data. Drug Des Devel Ther. 2021;15:1135–1147. doi:10.2147/DDDT.S240866
34. Kim BS, Silverberg JI, Ständer S, et al. Rapid Improvement of itch associated with atopic dermatitis with abrocitinib is partially independent of overall disease improvement: results from pooled Phase 2b and 3 monotherapy studies. Dermatitis. 2021;32(1S):S39–S44. doi:10.1097/DER.0000000000000770
35. Soto E, Banfield C, Gupta P, Peterson MC. Kinetic-pharmacodynamic model of platelet time course in patients with moderate-to-severe atopic dermatitis treated with oral janus kinase 1 inhibitor abrocitinib. CPT Pharmacometrics Syst Pharmacol. 2020;9(10):553–560. doi:10.1002/psp4.12548
36. Simpson EL, Wollenberg A, Bissonnette R, et al. Patient-reported symptoms and disease impacts in adults with moderate-to-severe atopic dermatitis: results from a Phase 2b study with abrocitinib. Dermatitis. 2021;32(1S):S53–S61. doi:10.1097/DER.0000000000000725
37. Simpson EL, Silverberg JI, Nosbaum A, et al. Integrated safety analysis of abrocitinib for the treatment of moderate-to-severe atopic dermatitis from the Phase II and Phase III clinical trial program. Am J Clin Dermatol. 2021;22:693–707. doi:10.1007/s40257-021-00618-3
38. Li C, Sun X, Zhao K, et al. Efficacy and safety of janus kinase inhibitors for the treatment of atopic dermatitis: a systematic review and meta-analysis. Dermatology;2021:1–11. doi:10.1159/000518541
39. Wang EQ, Le V, Winton JA, et al. Effects of renal impairment on the pharmacokinetics of abrocitinib and its metabolites. J Clin Pharmacol. 2021;61(10):1311–1323. doi:10.1002/jcph.1858
40. Medscape Dermatology [homepage on the Internet]. Abrocitinib approved for atopic dermatitis in Europe; 2021. Available from: https://www.medscape.com/viewarticle/964706?uac=90986EY&faf=1&sso=true&impID=3871959&src=wnl_newsalrt_211213_MSCPEDIT.
41. Deeks ED, Duggan S. Abrocitinib: first approval. Drugs. 2021;81(18):2149–2157. doi:10.1007/s40265-021-01638-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.