Back to Journals » Risk Management and Healthcare Policy » Volume 16
On the Asymmetric Relationship Between Physician Mental Health Disorders on Quality of Healthcare Under the COVID-19 Pandemic in Taiwan: Quantile on Quantile Regression Analyses
Received 28 July 2023
Accepted for publication 19 October 2023
Published 6 November 2023 Volume 2023:16 Pages 2291—2307
DOI https://doi.org/10.2147/RMHP.S429516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kyriakos Souliotis
Wen-Yi Chen,1 Feng-Li Lin2
1Department of Senior Citizen Service Management, National Taichung University of Science and Technology, Taichung City, Taiwan; 2Department of Accounting, Chaoyang University of Technology, Taichung City, Taiwan
Correspondence: Feng-Li Lin, Department of Accounting, Chaoyang University of Technology, 168, Jifeng E. Road, Wufeng District, Taichung City, 41349, Taiwan, Tel +886 4 23323000 Ext 4580, Fax +886 4 23742359, Email [email protected]
Purpose: When examining the nexus of physician mental health disorders and healthcare quality from the empirical perspective, mental health disorders are frequently associated with cyclical patterns corresponding to cyclic seasonality, mood swings, emission of air pollution and business cycles, the potential asymmetric effects of physician mental health disorders on healthcare quality have not received adequate attention from researchers. Therefore, the purpose of this study is to explore the asymmetric relationship between physician mental health disorders and healthcare quality during the pandemic outbreak in Taiwan.
Methods: Daily data for care quality indicators and physician mental health disorders were collected from the National Insurance Research Database in Taiwan, and the quantile-on-quantile regression model was applied to proceed with our analyses.
Results: Our results indicated that the overall aggregate effects of each quantile of physician mental health disorders on the cumulative quantiles of healthcare quality are negative (positive) for the 14-day readmission rate (preventable hospitalization rate and non-urgent ED-visit rate). Positively (negatively) cumulative effects of each quantile of physician mental health disorders were detected in the middle (low and high) quantiles of the preventable hospitalization rate. The cumulative effects of each quantile of physician mental health disorders on the high (low and middle) quantiles of the 14-day readmission rate are negative (positive), but the cumulative effects on various quantiles of the non-urgent ED-visit rate exhibit the opposite pattern.
Conclusion: The observed variation in the relationship between physician mental health disorders and different quantiles of healthcare quality suggests the need for tailored strategic interventions based on distinct levels of healthcare quality when addressing the higher risk of physician mental health disorders during the pandemic outbreak conditions.
Keywords: physician mental disorders, readmission rate, preventable hospitalization, non-urgent emergency department visits, social distancing, quantile on quantile
Introduction
A higher risk of mental health disorders among physicians in their workplace has long been recognized in the healthcare literature.1–4 It is anticipated that symptoms of physician mental health disorders such as burnout, stress, anxiety, depression, and even suicide are likely to have worsened during the COVID-19 pandemic outbreak due to amplified workloads, increased exposure to infectious diseases, and the presence of various stressors in their working environments. In fact, there is a great deal of literature investigating the impact of the COVID-19 pandemic on physician mental health. For example, Peck and Porter conducted a comprehensive review investigating the effect of the COVID-19 pandemic on physician mental health based on the framework of the burnout cascade, addressing the influence of burnout on both an individual level and an organizational level.5 Their results revealed that the pandemic has significantly affected physician mental health, leading to increased levels of burnout, depression, anxiety, and post-traumatic stress disorder.5 In addition, Alkhamees et al applied the meta-analysis method to explore the epidemiology of burnout and associated risk factors among physicians during the COVID-19 pandemic outbreak. The findings generated from their meta-analysis showed that the prevalence of burnout among physicians during the COVID-19 pandemic ranged from 20.70% to 61.30%, with several risk factors contributing to burnout, and these factors include longer working hours, inadequate personal protective equipment, and fear of contracting COVID-19.6 Furthermore, many studies have examined the psychological effects of the COVID-19 pandemic on various groups of physicians, including anesthetists,7 family physicians,8 ophthalmologists,9 palliative care physicians,10 and both surgical and non-surgical physicians,11 among others.12
An essential concern to address is the impact of mental health disorders among physicians on healthcare quality. Previous studies on the relationship between physician mental health disorders and healthcare quality have generated ambiguous results. For example, Dewa et al conducted two comprehensive reviews that investigated the influence of mental health disorders, particularly the symptom of burnout, on healthcare quality provided by physicians and resident doctors. Their findings indicated that evidence supporting a negative relationship between physician burnout and healthcare quality is moderate.13,14 Following this line of research, Mangory et al also found insufficient evidence in support of the negative effect of physician burnout on healthcare quality.15 Nevertheless, recent meta-analysis studies conducted by various researchers have highlighted a significantly negative association between physician mental health disorders and healthcare quality.16–18 As with the above mentioned literature reviews focusing on the effect of physician mental health disorders on healthcare quality, recent empirical studies linking physician mental health disorders and healthcare quality have yielded diverse results. These studies have reported positive,19 negative,20–25 inconclusive26–28, or insignificant associations.29–33
When examining the nexus of mental health disorders and healthcare quality from the empirical perspective, mental health disorders are frequently associated with cyclical patterns corresponding to cyclic seasonality,34 mood swings,35 emission of air pollution36 and business cycles.37–39 The ambiguous association between physician mental health disorders and healthcare quality may stem from the fact that the cycles of mental health disorders would have asymmetric effects on healthcare quality. The effect on healthcare quality of a positive mental health shock among physicians may differ from the effect on healthcare quality of a negative mental health shock among physicians. Failure to account for the asymmetry of mental health disorder cycles in model specifications will lead to analyses showing an ambiguous relationship between physician mental health disorders and healthcare quality. The asymmetric effects of socioeconomic domains have been extensively studied in various fields of social sciences, such as suicide,40,41 fertility,42 crime,43,44 population health,45,46 and healthcare expenditure,47,48 among others.49 Nevertheless, the potential asymmetric effects of physician mental health disorders on healthcare quality have not received adequate attention from healthcare researchers.
In order to incorporate the asymmetric effects of mental health disorder cycles on healthcare quality, time series analyses were used in this study. Specifically, we utilized the quantile-on-quantile regression model (QQRM) proposed by Sim and Zhou50 to investigate the asymmetric relationship between physician mental health disorders and objective measures of care outcomes such as the unplanned readmission rate within 14 days after discharge, preventable hospitalization rate, and non-urgent emergency department-visit (ED-visit) rate during the COVID-19 pandemic outbreak in Taiwan. The significance of this study is twofold: First, although the significant prevalence of mental health disorders among physicians during the COVID-19 pandemic outbreak has been well-documented in the literature,5–12 there is little research on the asymmetric relationship between physician mental health disorders and objective measures of care outcomes during the COVID-19 pandemic outbreak. Second, Taiwan’s National Health Insurance (NHI) system provides comprehensive healthcare coverage to all residents, ensuring universal access to healthcare services, and it has responded effectively to the COVID-19 pandemic, successfully mitigating its adverse impacts and ensuring the continued provision of healthcare services.51 Nevertheless, previous studies have raised concerns regarding the quality of healthcare services within Taiwan’s NHI system, specifically highlighting issues related to shortages in nurse staffing and intense competition among clinics and hospitals.52,53 Consequently, investigation into the link between physician mental health disorders and healthcare quality is important, providing insights into the potential challenges faced by the healthcare system from the perspective of physician labor input and its impact on healthcare quality.
Materials and Methods
Data and Variables
The primary objective of this study is to examine the impact of physician mental health on healthcare quality within Taiwan’s NHI system during the COVID-19 pandemic outbreak. The study focuses on three dependent variables: inpatient care, outpatient care, and emergency care quality indicators. The indicator used in this study to measure inpatient care quality is the 14-day readmission rate, which calculates the number of unplanned readmissions within 14 days after discharge per 100,000 discharge cases. This indicator has been suggested by Taiwan’s National Health Insurance Administration as a measure of inpatient care quality under Taiwan’s NHI system.52 The outpatient care quality indicator used in this study is the PQI_90 composite, which is calculated in accordance with guideline’s provided by the US Agency for Healthcare Research and Quality (AHRQ) in 2020.54 The PQI_90 composite represents the number of hospital admissions per 100,000 population for outpatient care sensitive conditions (ACSCs). These ACSCs encompass a variety of health conditions such as diabetes short- and long-term complications, uncontrolled diabetes, lower-extremity amputation among patients with diabetes, chronic obstructive pulmonary disease, asthma, hypertension, heart failure, community-acquired pneumonia, and urinary tract infection. The purpose of measuring PQI_90 composite is to assess the potential impact of timely and appropriate outpatient care in preventing the need for hospitalization for these conditions.53,54 Therefore, the PQI_90 composite is used as a proxy for the preventable hospitalization rate. In addition, the emergency care quality indicator used in this study is the non-urgent ED-visit (emergency-department-visit) rate as measured by the prevalence of non-urgent visits to the emergency department (ED) in hospitals. The non-urgent ED-visit rate is calculated using the New York University algorithm proposed by Ballard et al.55 The algorithm helps identify non-urgent visits to the ED, allowing for the evaluation of emergency care quality and the appropriate utilization of emergency services.
Moreover, this study focuses on the explanatory variable of physician mental health, defined as the ratio of physician mental health disorders prevalence to general population mental health disorders prevalence. Several clinical diagnosis codes from the 2016 version of the International Classification of Diseases, 10th Revision (ICD-10), were used to identify mental health disorders. These codes include Z73.0 (burnout), F32.0 (mild depressive episode), F32.1 (moderate depressive episode), F32.2 (severe depressive episode without psychotic symptoms), F41.1 (generalized anxiety disorder), F42.0 (predominantly obsessional thoughts or ruminations), F43.0 (acute stress reaction), F43.1 (post-traumatic stress disorder), F43.2 (adjustment disorders), and F51.0 (nonorganic insomnia). The prevalence of mental health disorders is calculated as the proportion of total outpatient visits attributed to these symptoms of mental health disorders. Since the individual’s behavior in seeking care may have changed due to fear of COVID-19 infection during the pandemic outbreak,51 the social distance index (SDI), originated by Vokó and Pitter’s research,56 was used as a control variable to measure the magnitude of individual behavior change by comparing the time spent at various categories of places (such as retail and recreation, grocery and pharmacy, parks, transit stations, workplaces, and residential areas) to a baseline period before the pandemic. Given the promotion by Taiwan’s government of the voluntary stay-at-home policy during the COVID-19 pandemic outbreak, the positive or negative deviation from the baseline period of time spent at workplace areas and the other five places can reflect an individual’s social distancing behavior. Hence, the calculation of the Social Distance Index (SDI) involves two steps. First, the percentage deviation from the baseline period for time spent at residential areas (expected to be positive during the severe pandemic outbreak) is subtracted from the total percentage deviation from the baseline period for time spent at the other five places (anticipated to be negative during the severe pandemic outbreak). This subtraction results in a value that represents the deviation in social distancing behavior. Second, this obtained value is divided by six, yielding the SDI. Accordingly, a positive (or negative) value of the SDI indicates an increase (or a decrease) in social distancing behavior.
The data used to calculate the dependent and explanatory variables in this study were obtained from the National Insurance Research Database in Taiwan. This database administrated by the Health and Welfare Data Science Center provides valuable information for analyzing inpatient, outpatient and emergency care quality indicators. Additionally, the data used to compute the SDI were obtained from the Google COVID-19 Community Mobility Reports (https://www.google.com/covid19/mobility/), offering insights into individuals’ mobility patterns and social distancing behaviors during the COVID-19 pandemic outbreak. The data collection period for this study spans from February 15, 2020, to December 31, 2020, resulting in a total of 321 daily observations. The data collection process was approved by the Research Ethics Committee of Taichung Tzu Chi Hospital with the Certificate ID: REC111-23.
Quantile on Quantile Regression Model (QQRM)
As we discussed in the Introduction section, an asymmetric relationship between physician mental health disorders and healthcare quality is likely to exist. To better understand this nonlinear relationship, the QQRM, as developed by Sim and Zhou50 is used for our data analyses. It is important to address that the QQRM is a generalized specification of the conventional quantile regression model offering several advantages over the linear regression model. First, while the linear regression model can only estimate the effect of an explanatory variable (physician mental health disorders) on the conditional mean of the dependent variable (healthcare quality), the quantile regression model allows for more comprehensive analyses by decomposing this effect on the conditional mean into effects on the conditional quantiles. Second, the quantile regression model provides robust inference methods that are less sensitive to violations of the normal distributional assumption. Third, the QQRM extends the quantile regression model by estimating the effect of each specific quantile of the explanatory variable on various quantiles of the dependent variable. Fourth, the QQRM combines estimation procedures from quantile and local linear regression models, enabling its application to single equation models rather than being limited to system equation models.50 Thus, results generated by the QQRM are able to provide a comprehensive understanding of the evolving relationship between physician mental health disorders and healthcare quality. Specifically, the specification of the QQRM is displayed as follows:

where yt and xt represent healthcare quality and physician mental health disorders at time t, respectively. Since the linkage of yt and xt may be confounded by the individual’s behavior change in seeking care during the COVID-19 pandemic outbreak,51 the social distance index (zt) was included in (Equation 1) to control for this confounding effect. In addition, Sim and Zhou introduced an autoregressive term (yt-1) in (Equation 1) to account for potential auto-correlation in the error term.50 x(τ) denotes τ-quantile of physician mental health. The bracket on the right hand side of (Equation 1) represents θ-conditional quantile of healthcare quality.  is the error term conditional on the θ-conditional quantile of healthcare quality.
is the error term conditional on the θ-conditional quantile of healthcare quality.  , and
, and  are parameters. Unlike a standard conditional quantile regression model, our model specification of (Equation 1) captures an association between θ-quantile of healthcare quality and τ-quantile of physician mental health disorders given that
are parameters. Unlike a standard conditional quantile regression model, our model specification of (Equation 1) captures an association between θ-quantile of healthcare quality and τ-quantile of physician mental health disorders given that  and
and  are doubly indexed in θ and τ. Namely, the asymmetric relationship between healthcare quality and physician mental health disorders can be better understood in terms of the estimated effect of each quantile of x on various quantiles of y.
are doubly indexed in θ and τ. Namely, the asymmetric relationship between healthcare quality and physician mental health disorders can be better understood in terms of the estimated effect of each quantile of x on various quantiles of y.
Since the specification of the QQRM is the generalized form of the conventional quantile regression model, the sum of  over θ quantiles of yt indicates the overall effects of each quantile (τ) of physician mental health disorders on the cumulative quantiles of the healthcare quality indicator, encompassing the aggregated effects over θ quantiles of yt. In contrast, the sum of
over θ quantiles of yt indicates the overall effects of each quantile (τ) of physician mental health disorders on the cumulative quantiles of the healthcare quality indicator, encompassing the aggregated effects over θ quantiles of yt. In contrast, the sum of  over τ quantiles specifies the cumulative effects of each quantile of physician mental health disorders on the each quantile (θ) of the healthcare quality indicator, including the aggregated effects over τ quantiles of physician mental health disorders. The mean of the overall effects on the cumulative quantiles of healthcare quality is equivalent to the slope (ie,
over τ quantiles specifies the cumulative effects of each quantile of physician mental health disorders on the each quantile (θ) of the healthcare quality indicator, including the aggregated effects over τ quantiles of physician mental health disorders. The mean of the overall effects on the cumulative quantiles of healthcare quality is equivalent to the slope (ie,  ) of the conventional quantile regression model.50 The asymptotic properties of the non-parametric (kernel) regression methodology were utilized to generate the p values of the estimates
) of the conventional quantile regression model.50 The asymptotic properties of the non-parametric (kernel) regression methodology were utilized to generate the p values of the estimates  and
and  .50
.50
Results
Descriptive Statistics
Panel A of Table 1 presents descriptive statistics for all variables used in this study, covering the period from February 15th, 2020, to December 31st, 2020. As shown in Table 1, the mean (median) values of the 14-day readmission rate and preventable hospitalization rate were 28.746 (31.964) per 100,000 cases and 2.716 (2.801) per 100,000 population, respectively. The prevalence of non-urgent ED visits in hospitals ranged from 19.959% to 29.425%, with a mean (median) value of 23.309% (23.167%). The mean (median) ratio of the physician mental health disorders prevalence to the general population mental health disorders prevalence was 1.438 (1.133), indicating that the mean (median) prevalence of mental health disorders among physicians was 43.80% (13.30%) higher compared to the prevalence for the general population during the COVID-19 pandemic outbreak. The mean (median) value of the social distance index was 3.785 (3.167), suggesting an overall increase in social distancing behavior throughout the study period. It is important to note that JB-statistics (used to the test for the null hypothesis of the normality assumption) for all variables generated p values less than the 1% significance level, a result showing that the normality assumption used in the linear regression model is unlikely to be justified. Thus, the quantile regression model is more suitable for our data. In order to examine the aggregate effects of different quantiles of physician mental health on various quantiles of healthcare quality, standardized values of all variables were used to estimate the coefficients of the QQRM. Time plots of these variables could be found in Figure S1.
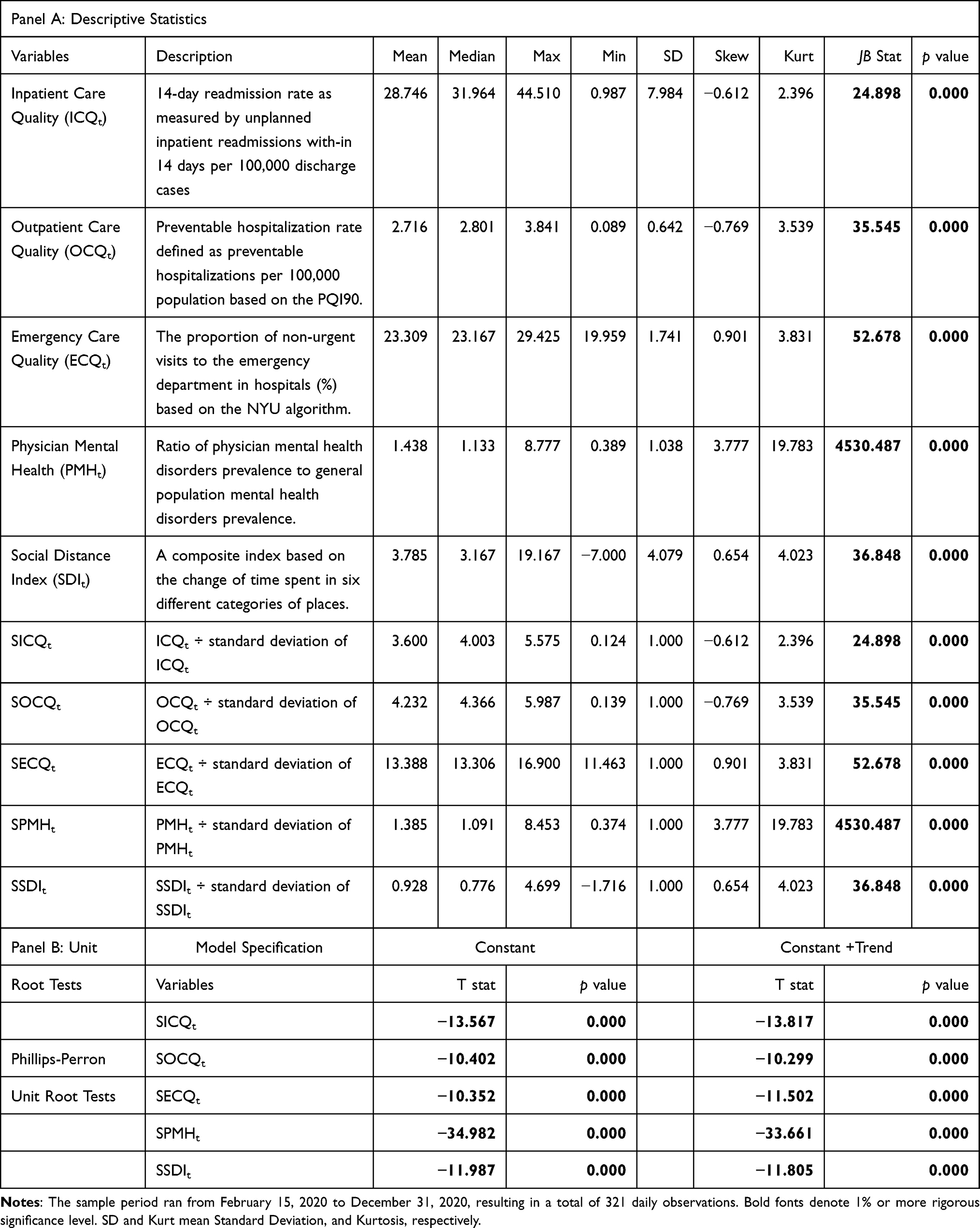 |
Table 1 Descriptive Statistics and Unit Root Tests |
Unit Root Tests
It is crucial to address that all variables used in this study are time series data, which may exhibit the presence of unit roots. The unit root property can result in a spurious relationship between two variables. In order to verify whether or not our data are stationary time series, the Phillips–Perron unit root test was used to test for the null hypothesis of unit root against stationary time series of these variables. This test provides a non-parametric correction to the t-test statistic which is robust with respect to unspecified autocorrelation and heteroscedasticity in the data generating process of the test equation.57 As shown in the Panel B of Table 1, the Phillips–Perron unit root tests with constant and with constant plus trend specifications generated p values less than the 1% significance level. These results indicated that all variables used in this study are stationary time series, which allowed us to proceed with estimating the QQRM using these variables in levels.
Results for the QQRMs
Presentations for QQRM Estimation
Table 2 displays the estimated results for the asymmetric relationship between physician mental health disorders and healthcare quality. Specifically, it presents the effects of the τ-quantile of physician mental health disorders (τ∈[0.1, 0.2, 0.3,…,0.9]) on the θ-quantile of healthcare quality (θ∈[0.1, 0.2, 0.3,…,0.9]). As shown in Panel A of Table 2, the estimated effects of each τ-quantile of physician mental health disorders (τ∈[0.1, 0.2,0.3,…,0.9]) on various quantiles of the 14-day readmission rate (θ∈[0.1, 0.2,0.3,…,0.9]) are statistically significant at the 10% level for most quantiles ranging from 10% to 90%. The relationship between physician mental health disorders and the 14-day readmission rate demonstrates negative, positive and non-significant effects of varying magnitudes. The same patterns are found in the estimated effects of each τ -quantile of physician mental health disorders (τ∈[0.1, 0.2, 0.3,…,0.9]) on various quantiles (θ∈[0.1, 0.2, 0.3,…,0.9]) of outpatient care quality (measured by the preventable hospitalization rate) and emergency care quality (measured by the non-urgent ED-visit rate), as indicate in Panel B and Panel C of Table 2, respectively. In order to facilitate a better understanding of the results, we demonstrate the area plots with the non-significant effects set as zero in Figures 1–3. In these figures, three distinct regions (low quantiles (≤30%), middle quantiles (40–60%), and high quantiles (>60%)) were segmented, allowing us to more easily discuss the asymmetric relationship between physician mental health disorders and healthcare quality.
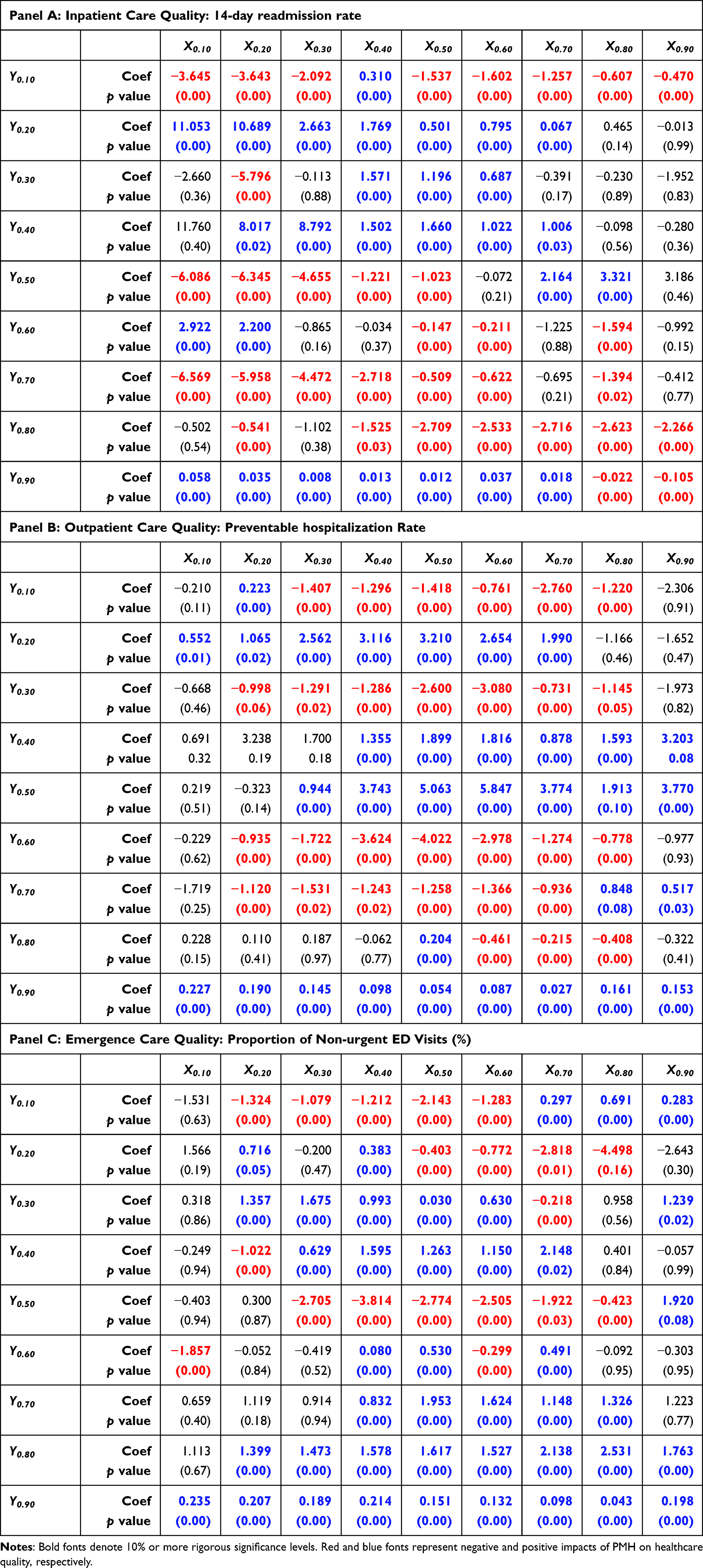 |
Table 2 Impact of Physician Mental Health on Healthcare Quality |
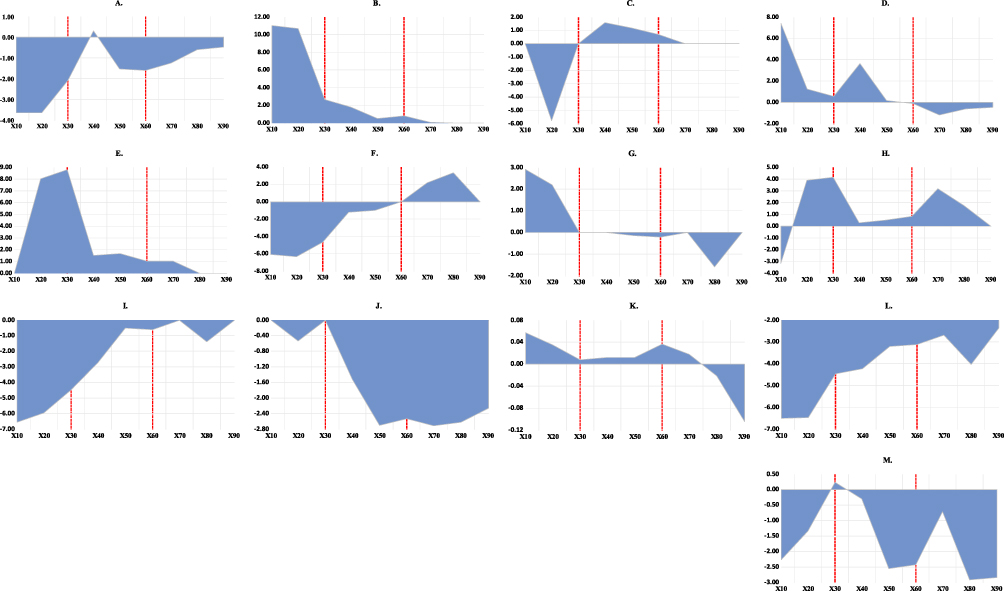 |
Figure 1 Impact of each quantile of physician mental health disorders (PMH) on various quantiles of inpatient care quality of (ICQ). Notes: Sub-figures (A–D) illustrate the effects of each quantile of PMH on the 0.1 (ICQ_0.1), 0.2 (ICQ_0.2), 0.3 (ICQ_0.3) quantile and the low quantiles of ICQ (ie, aggregate over low quantiles of ICQ), respectively; Sub-figures (E–H) illustrate the effects of each quantile of PMH on the 0.4 (ICQ_0.4), 0.5 (ICQ_0.5), 0.6 (ICQ_0.6) quantile and the middle quantiles of ICQ (ie, aggregate over middle quantiles of ICQ), respectively; Sub-figures (I–L) illustrate the effects of each quantile of PMH on the 0.7 (ICQ_0.7), 0.8 (ICQ_0.8), 0.9 (ICQ_0.9) quantile and the high quantiles of ICQ (ie, aggregate over high quantiles of ICQ), respectively; Sub-figure (M) depicts the cumulative impact of each PMH quantile across all quantiles of ICQ (ie, aggregate over all quantiles of ICQ). |
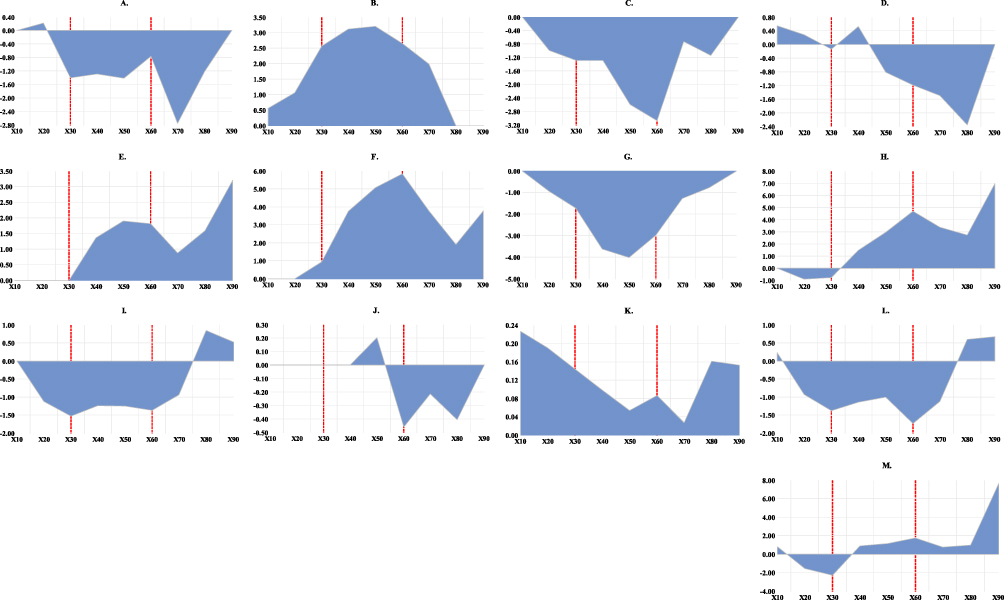 |
Figure 2 Impact of each quantile of physician mental health disorders (PMH) on various quantiles of outpatient care quality (OCQ). Notes: Sub-figures (A–D) illustrate the effects of each quantile of PMH on the 0.1 (OCQ_0.1), 0.2 (OCQ_0.2), 0.3 (OCQ_0.3) quantile and the low quantiles of OCQ (ie, aggregate over low quantiles of OCQ), respectively; Sub-figures (E–H) illustrate the effects of each quantile of PMH on the 0.4 (OCQ_0.4), 0.5 (OCQ_0.5), 0.6 (OCQ_0.6) quantile and the middle quantiles of OCQ (ie, aggregate over middle quantiles of OCQ), respectively; Sub-figures (I–L) illustrate the effects of each quantile of PMH on the 0.7 (OCQ_0.7), 0.8 (OCQ_0.8), 0.9 (OCQ_0.9) quantile and the high quantiles of OCQ (ie, aggregate over high quantiles of OCQ), respectively; Sub-figure (M) depicts the cumulative impact of each PMH quantile across all quantiles of OCQ (ie, aggregate over all quantiles of OCQ). |
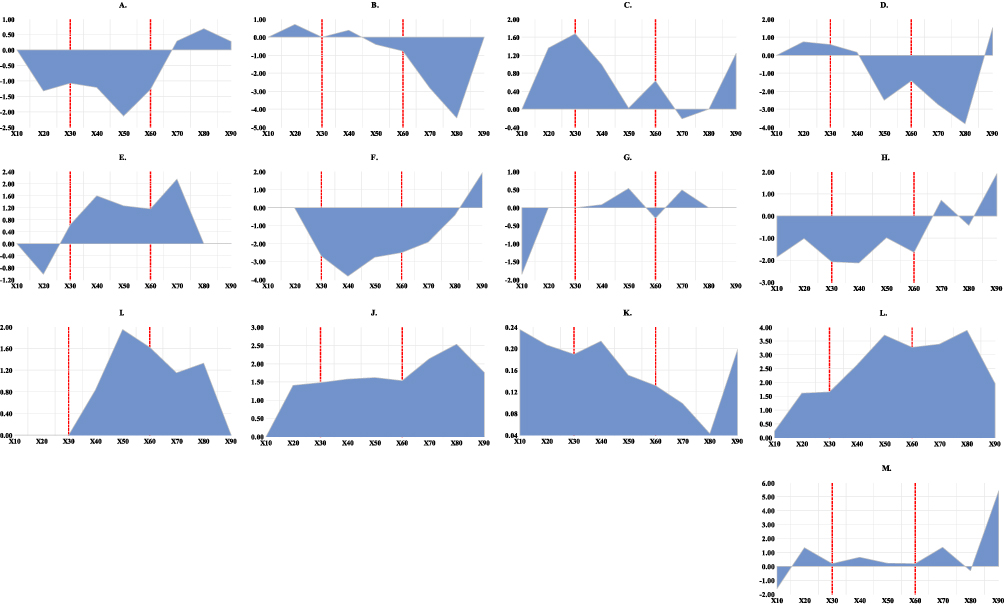 |
Figure 3 Impact of each quantile of physician mental health disorders (PMH) on various quantiles of emergency care quality (ECQ). Notes: Sub-figures (A–D) illustrate the effects of each quantile of PMH on the 0.1 (ECQ_0.1), 0.2 (ECQ_0.2), 0.3 (ECQ_0.3) quantile and the low quantiles of ECQ (ie, aggregate over low quantiles of ECQ), respectively; Sub-figures (E–H) illustrate the effects of each quantile of PMH on the 0.4 (ECQ_0.4), 0.5 (ECQ_0.5), 0.6 (ECQ_0.6) quantile and the middle quantiles of ECQ (ie, aggregate over middle quantiles of ECQ), respectively; Sub-figures (I–L) illustrate the effects of each quantile of PMH on the 0.7 (ECQ_0.7), 0.8 (ECQ_0.8), 0.9 (ECQ_0.9) quantile and the high quantiles of ECQ (ie, aggregate over high quantiles of ECQ), respectively; Sub-figure (M) depicts the cumulative impact of each PMH quantile across all quantiles of ECQ (ie, aggregate over all quantiles of ECQ). |
Effect of Physician Mental Health on Inpatient Care Quality
(Figure 1A–D) portray the effects of physician mental health disorders on low quantiles of the 14-day readmission rate. As indicated in (Figure 1A), the effects of physician mental health disorders on the 10% quantile of the 14-day readmission rate are negative across most quantiles of physician mental health disorders, except for the 40% quantile, where the relationship is positive. Nevertheless, (Figure 1B) demonstrates that physician mental health disorders are positively (non-significantly) associated with the 20% quantile of the 14-day readmission rate for the 70% and below quantiles (the 80% and above quantiles) of physician mental health disorders. As indicated in (Figure 1C), the relationship between physician mental health disorders and the 30% quantile of the 14-day readmission rate is positive for the 40% to 60% quantiles, negative for the 20% quantile, and non-significant for other quantiles of physician mental health disorders. These findings suggest that the aggregate effects of physician mental health disorders on low quantiles of the 14-day readmission rate are predominantly positive (negative) for the 50% and below quantiles (the 60% and above quantiles) of physician mental health disorders, as indicated in (Figure 1D).
(Figure 1E–H) illustrate the effects of physician mental health disorders on middle quantiles of the 14-day readmission rate. (Figure 1E) demonstrates that, for the 20% to 70% quantiles, there are positive effects of physician mental health disorders on the 40% quantile of the 14-day readmission rate. Non-significant effects are observed for other quantiles. As indicated in (Figure 1F), the association between physician mental health disorders and the 50% quantile of the 14-day readmission rate is negative for the 50% and below quantiles, positive for the 70% to 80% quantiles, and non-significant for other quantiles of physician mental health. In addition, (Figure 1G) shows that the effects of physician mental health disorders on the 60% quantile of the 14-day readmission rate are positive for the 20% and below quantiles, negative for the 50%, 60%, and 80% quantiles, and non-significant for other quantiles of physician mental health disorders. These results suggest that the aggregate effects of physician mental health disorders on middle quantiles of the 14-day readmission rate are predominantly negative for the 10% quantile, positive for the 20% to 80% quantiles, and non-significant for 90% quantile of physician mental health disorders, as shown in (Figure 1H).
(Figure 1I–L) depict the effects of physician mental health disorders on high quantiles of the 14-day readmission rate. (Figure 1I) demonstrates that there are negative effects of physician mental health disorders on the 70% quantile of the 14-day readmission rate for most quantiles of physician mental health disorders, except for the 70% and 90% quantiles, where the relationship is non-significant. Similarly, (Figure 1J) indicates negative effects of physician mental health disorders on the 80% quantile of the 14-day readmission rate across most quantiles of physician mental health disorders, with non-significant effects observed at the 10% and 30% quantiles. As shown in (Figure 1K), the association between physician mental health disorders and the 90% quantile of the 14-day readmission rate is positive (negative) for the 70% and below quantiles (the 80% and above quantiles) of physician mental health disorders. These results indicate that the aggregate effects of physician mental health disorders on high quantiles of the 14-day readmission rate are predominantly negative across all quantiles of physician mental health disorders, as presented in (Figure 1L).
The overall effect of each quantile (τ=0.1, 0.2,….,0.9) of physician mental health disorders on the cumulative quantiles of the 14-day readmission rate is depicted in (Figure 1M). This figure shows the summed effects of each quantile of physician mental health disorders on the low, middle, and high quantiles of the 14-day readmission rate (ie, aggregating effects over all  from (Figure 1D, H, and L). In contrast, the cumulative effect of each quantile of physician mental health disorders on the low, middle, and high quantiles of the 14-day readmission rate can be identified by comparing the positive areas and negative areas from (Figure 1D, H, and L), respectively. Specifically, positively (negatively) cumulative effects of each quantile of physician mental health disorders on the low, middle, and high quantiles of the 14-day readmission rate are justified if the positive (negative) areas dominate the negative (positive) areas from (Figure 1D, H and L), respectively. As demonstrated in (Figure 1M), the overall effects of each quantile of physician mental health disorders on the cumulative quantiles of the 14-day readmission rate are predominantly negative across most quantiles of physician mental health disorders, except for the 30% quantile where a positive effect is found. Moreover, the cumulative effects of each quantile of physician mental health disorders on the low and middle (high) quantiles of the 14-day readmission rate are found to be positive (negative), as shown by the dominance of positive (negative) areas in comparison to negative (positive) areas in (Figure 1D, and H), respectively (Figure 1L).
from (Figure 1D, H, and L). In contrast, the cumulative effect of each quantile of physician mental health disorders on the low, middle, and high quantiles of the 14-day readmission rate can be identified by comparing the positive areas and negative areas from (Figure 1D, H, and L), respectively. Specifically, positively (negatively) cumulative effects of each quantile of physician mental health disorders on the low, middle, and high quantiles of the 14-day readmission rate are justified if the positive (negative) areas dominate the negative (positive) areas from (Figure 1D, H and L), respectively. As demonstrated in (Figure 1M), the overall effects of each quantile of physician mental health disorders on the cumulative quantiles of the 14-day readmission rate are predominantly negative across most quantiles of physician mental health disorders, except for the 30% quantile where a positive effect is found. Moreover, the cumulative effects of each quantile of physician mental health disorders on the low and middle (high) quantiles of the 14-day readmission rate are found to be positive (negative), as shown by the dominance of positive (negative) areas in comparison to negative (positive) areas in (Figure 1D, and H), respectively (Figure 1L).
Effect of Physician Mental Health on Outpatient Care Quality
(Figure 2A–D) present the effects of physician mental health disorders on low quantiles of the preventable hospitalization rate. As shown in (Figure 2A), the relationship between physician mental health disorders and the 10% quantile of the preventable hospitalization rate is positive for the 20% quantile, negative for the 30% to 80% quantiles, and non-significant for other quantiles of physician mental health disorders. (Figure 2B) demonstrates that the effects of physician mental health disorders on the 20% quantile of the preventable hospitalization rate are positive (non-significant) for the 70% and below (the 80% and above) quantiles of physician mental health disorders. Nonetheless, the relationship between physician mental health disorders and the 30% quantile of the preventable hospitalization rate is negative across most quantiles of physician mental health disorders, except for the 10% and 90% quantiles, where the relationship is non-significant (see (Figure 2C). These findings indicate that the aggregate effects of physician mental health disorders on low quantiles of the preventable hospitalization rate are predominantly positive for the 10%, 20%, and 40% quantiles, negative for the 30% and 50% to 80% quantiles and non-significant for the 90% quantile of physician mental health disorders, as shown in (Figure 2D).
(Figure 2E–H) illustrate the effects of physician mental health disorders on middle quantiles of the preventable hospitalization rate. As demonstrated in (Figure 2E), positive (non-significant) effects of physician mental health disorders on the 40% quantile of the preventable hospitalization rate are justified for the 40% and above quantiles (the 30% and below quantiles) of physician mental health disorders. Similarly, (Figure 2F) shows that physician mental health disorders are positively (non-significantly) associated with the 50% quantile of the preventable hospitalization rate for the 30% and above quantiles (the 20% and below quantiles) of physician mental health disorders. Nevertheless, (Figure 2G) portrays a negative association between physician mental health disorders and the 60% quantile of the preventable hospitalization rate across most quantiles of physician mental health disorders, except for the 10% and 90% quantiles, where the relationship is non-significant. These results suggest that the aggregate effects of physician mental health disorders on middle quantiles of the preventable hospitalization rate are predominantly positive for the 40% and above quantiles, negative for the 20% to 30% quantiles and non-significant for the 10% quantile of physician mental health disorders, as displayed in (Figure 2H).
(Figure 2I–L) describe the effects of physician mental health disorders on high quantiles of the preventable hospitalization rate. (Figure 2I) shows that the association between physician mental health disorders and the 70% quantile of the preventable hospitalization rate is non-significant for the 10% quantile, negative for the 20% to 70% quantiles, and positive for the 80% and above quantiles of physician mental health disorders. (Figure 2J) suggests that the relationship between physician mental health disorders and the 80% quantile of the preventable hospitalization rate is negative for the 60% to 80% quantiles, positive for the 50% quantile, and non-significant for other quantiles of physician mental health disorders. Nonetheless, (Figure 2K) shows an unambiguously positive association between physician mental health disorders and the 90% quantile of the preventable hospitalization rate across all quantiles of physician mental health disorders. These findings indicate that the aggregate effects of physician mental health disorders on high quantiles of the preventable hospitalization rate are predominantly negative for the 20% to 70% quantiles and positive for the 10%, 80% and above quantiles of physician mental health disorders, as illustrated in (Figure 2L). Moreover, as demonstrated in (Figure 2M), the overall effects of each quantile of physician mental health disorders on the cumulative quantiles of the preventable hospitalization rate are negative for the 20% and 30% quantiles of physician mental health disorders, while other quantiles exhibit positive effects. Furthermore, the cumulative effects of each quantile of physician mental health disorders on the low and high (middle) quantiles of the preventable hospitalization rate are found to be negative (positive), as shown by the dominance of the negative (positive) areas in comparison to the positive (negative) areas from (Figure 2D, and L), respectively (Figure 2H).
Effect of Physician Mental Health on Emergency Care Quality
(Figure 3A–D) demonstrate the effects of physician mental health disorders on low quantiles of the non-urgent ED-visit rate. As indicated in (Figure 3A), the effects of physician mental health disorders on the 10% quantile of the non-urgent ED-visit rate are non-significant, negative, and positive for the 10% quantile, the 20% to 60% quantiles, and the 70% and above quantiles of physician mental health disorders, respectively. (Figure 3B) suggests that the relationship between physician mental health disorders and the 20% quantile of the non-urgent ED-visit rate is non-significant for the 10%, 30%, and 90% quantiles, positive for the 20% and 40% quantiles, and negative for the 50% to 80% quantiles of physician mental health disorders. Nevertheless, (Figure 3C) shows that the relationship between physician mental health disorders and the 30% quantile of the non-urgent ED-visit rate is non-significant for the 10% and 80% quantiles, negative for the 70% quantile, and positive for other quantiles of physician mental health disorders. These findings suggest that the aggregate effects of physician mental health disorders on low quantiles of the non-urgent ED-visit rate are predominantly negative for the 50% to 80% quantiles, positive for the 20% to 40%, and 90% quantiles, and non-significant for the 10% quantile of physician mental health disorders, as demonstrated in (Figure 3D).
(Figure 3E–H) illustrate the effects of physician mental health disorders on middle quantiles of the non-urgent ED-visit rate. (Figure 3E) shows that the association between physician mental health disorders and the 40% quantile of the non-urgent ED-visit rate is negative for the 20% quantile, positive for the 30% to 70% quantiles, and non-significant for other quantiles of physician mental health disorders. As indicated in (Figure 3F), the effects of physician mental health disorders on the 50% quantile of the non-urgent ED-visit rate are non-significant, negative, and positive for the 20% and below quantiles, the 30% to 80% quantiles, and the 90% quantile of physician mental health disorders, respectively. (Figure 3G) shows that the effects of physician mental health disorders on the 60% quantile of the non-urgent ED-visit rate are negative for the 10% and 60% quantiles, positive for the 40%, 50%, and 70% quantiles, and non-significant for other quantiles of physician mental health disorders. These results indicate that the aggregate effects of physician mental health disorders on middle quantiles of the non-urgent ED-visit rate are predominantly positive for the 70% and 90% quintiles of physician mental health disorders, while other quantiles exhibit predominantly negative effects, as demonstrated in (Figure 3H).
(Figure 3I–L) display the effects of physician mental health disorders on high quantiles of the non-urgent ED-visit rate. As indicated in (Figure 3I), the relationship between physician mental health disorders and the 70% quantile of the non-urgent ED-visit rate is positive for the 40% to 80% quantiles of physician mental health disorders, while the relationship is non-significant for other quantiles. (Figure 3J) presents the positive effects of physician mental health disorders on the 80% quantile of the non-urgent ED-visit rate across all quantiles except for the 10% quantile where the relationship is non-significant. Similarly, (Figure 3K) shows unambiguously positive impacts of physician mental health disorders on the 80% quantile of the non-urgent ED-visit rate across all quantiles of physician mental health disorders. These findings indicate that the aggregate effects of physician mental health disorders on high quantiles of the non-urgent ED-visit rate is predominantly positive across all quantiles of physician mental health disorders, as illustrated in (Figure 3L). Furthermore, as demonstrated in (Figure 3M), the overall effect of each quantile of physician mental health disorders on the cumulative quantiles of the non-urgent ED-visit rate are negative for the 10% and 80% quantiles of physician mental health disorders while other quantiles exhibit positive effects. Finally, the cumulative effects of each quantile of physician mental health disorders on the low and middle (high) quantiles of the non-urgent ED-visit rate are found to be negative (positive), as indicated by the dominance of the negative (positive) areas in comparison to the positive (negative) areas in (Figure 3D and H), respectively (Figure 3L).
Discussion
Evidence from Table 2 and Figures 1–3 allows us to discuss two types of asymmetric relationships between physician mental health disorders and healthcare quality, these being the overall effects of each quantile of physician mental health disorders on the cumulative quantiles of healthcare quality, and the cumulative effects of each quantile of physician mental health disorders on various quantiles of healthcare quality. Based on our empirical results, several policy implications can be drawn from these effects and stated as follows:
First, it is crucial to recognize that the impact of physician mental health disorders on healthcare quality can be ambiguous when considering both the theoretical and empirical perspectives. The empirical viewpoint is supported by studies that have observed cyclical patterns of mental health disorders.34–39 On the other hand, the theoretical viewpoint is based on the conventional production theory, which explains the connection between physician mental health and healthcare quality as an input-output relationship. In this framework, healthcare quality is considered to be the output of an aggregate health production function, while physician mental health serves as the labor input. Insight into the effect of physician mental health disorders on healthcare quality can be gained by considering the unobserved quantity input and quality of input propositions as motivated by the recent research conducted by Casalino et al.19 The unobserved quantity input proposition hypothesizes that a higher prevalence of mental health disorders among physicians may indicate their dedication and effort to provide quality care. In other words, physicians who prioritize patient well-being may experience elevated levels of stress and burnout, potentially leading to mental health disorders. This proposition, nevertheless, implies that these physicians are still capable of delivering good quality care despite their mental health challenges.3,19 In contrast, the quality of input proposition postulates that mental health disorders would undermine the professional competence of physicians, affecting their ability to provide quality care. This proposition highlights that the resilience and adaptability of physicians may not be sufficient to maintain their performance standards when confronted with mental health challenges.19,58
Second, both the overall and cumulative effects of each quantile of physician mental health disorders depicted in Figures 1–3 suggest ambiguous effects of physician mental health disorders on healthcare quality. These findings are consistent with previous studies that have also reported an ambiguous relationship between physician mental health disorders and healthcare quality.19–28 Moreover, the overall effects of each quantile of physician mental health disorders on the cumulative quantiles of healthcare quality can be further aggregated into the overall aggregate effects of each quantile of physician mental health disorders, and these effects can be identified by comparing the positive and negative areas depicted in (Figures 1M, 2M and 3M). As indicated in these figures, the overall aggregate effects are found to be negative (positive) for the cumulative quantiles of the 14-day readmission rate (preventable hospitalization rate and non-urgent ED-visit rate), providing evidence in favor of the unobserved quantity input proposition (the quality of input proposition) for the inpatient (outpatient and ED) sectors of Taiwan’s NHI system. It is worth noting that physician mental health disorders do not directly cause an increase in non-urgent ED utilization. Nevertheless, physician mental health disorders can serve as an indicator of the trustworthiness and stability of the healthcare system. When individuals perceive a lack of accessibility and stability in the healthcare system due to an increase in physician mental health disorders, it may contribute to an increase in non-urgent ED utilization. This phenomenon was particularly observed during the COVID-19 pandemic, when retired healthcare professionals were called back to the healthcare system to ensure the stability of physician labor inputs and healthcare services.
Similar to healthcare systems in other countries, Taiwan’s NHI system has also encountered challenges such as a shortage of healthcare personnel and increased work pressure and psychological burden during the pandemic. In order to prevent the collapse of the healthcare system, strict administrative orders have been implemented to restrict healthcare utilization in inpatient sectors, resulting in an increase in the non-urgent ED-visit rate. Therefore, when healthcare administrators detect an increased risk of physician mental health disorders, they should implement relevant intervention strategies to maintain healthcare quality in the outpatient and ED sectors under Taiwan’s NHI system. These strategies may include enhancing the effectiveness of physician support systems, improving the working environment for physicians, introducing various incentives to motivate physicians, and most importantly, reestablishing public confidence in the accessibility of healthcare services during outbreak conditions.
Third, while the unobserved quantity input proposition (the quality of input proposition) is supported for the inpatient (outpatient and ED) sectors of Taiwan’s NHI system, the acceptance of either the unobserved quantity input proposition or the quality of input proposition varies across different quantiles of healthcare quality. Specifically, the unobserved quantity input (quality of input) proposition holds true based on the negatively (positively) cumulative effects of each quantile of physician mental health disorders on the high (low and middle) quantiles of the 14-day readmission rate for the inpatient sector. Consequently, when facing with low inpatient care quality (corresponding to high quantiles of the 14-day readmission rate in (Figure 1L), increasing work pressure to improve the delivery of healthcare services may somewhat elevate the risk of physician mental health disorders, but it may also enhance inpatient care quality. Conversely, when facing with middle and high inpatient care quality (corresponding to middle and low quantiles of the 14-day readmission rate in in (Figure 1H and D), respectively), when there is a higher risk of physician mental health disorders, healthcare administrators must actively intervene to address physician mental health disorders and reduce the risk in order to maintain high-quality inpatient care.
It is important to note that the same active intervention strategies should be implemented by healthcare administrators for the outpatient sector when faced with middle outpatient care quality, since we found that the quality input proposition holds true based on the positively cumulative effects of each quantile of physician mental health disorders on the middle quantiles of the preventable hospitalization rate, as illustrated in (Figure 2H). Contrarily, the unobserved quantity input proposition holds true based on the negatively cumulative effects of each quantile of physician mental health disorders on the low and high quantiles of the preventable hospitalization rate, as indicated in (Figure 2D and L), respectively. Additionally, we observed that the unobserved quantity input (quality input) proposition is supported for the negatively (positively) cumulative effects of each quantile of physician mental health disorders on the low and middle (high) quantiles of the non-urgent ED-visit rate in the ED sector, as indicated in (Figure 3D, H and L). Therefore, healthcare administrators should prioritize establishing public confidence in the accessibility of healthcare services during the pandemic outbreak conditions, particularly in the context of low-quality emergency care, as indicated by the high quantiles of the non-urgent ED-visit rate shown in (Figure 3L).
This study makes contributions beyond those of the existing literature on the relationship between physician mental health and healthcare quality in three respects: First, although cyclical patterns of mental health disorders have attracted lots of attention in the healthcare research,34–39 the literature has not explored the asymmetric effects of physician mental health disorders on healthcare quality stemming from these cyclical patterns. In this study, we employed the QQRM proposed by Sim and Zhou50 for the first time, allowing for the incorporation of results similar to the positive,19 negative,20–25 inconclusive26–28 or insignificant effects of physician mental health disorders on healthcare quality found in previous studies.29–33 Second, the QQRM provides advantages over linear regression in terms of its reduced sensitivity to the normality assumption in statistical inference. In addition, we have utilized the unobserved quantity input and quality of input propositions, drawing upon the research conducted by Casalino et al,19 to interpret the ambiguous effects of physician mental health disorders on healthcare quality obtained from the QQRM. These propositions have provided valuable insights into the complex relationship between physician mental health and the healthcare quality. Third, in contrast to previous research that relied on self-reported or survey data on mental health disorders and patient outcomes to establish the relationships between physician mental health disorders and healthcare quality, our study utilized clinical diagnosis data for specific symptoms of mental health disorders (such as burnout, depressive episodes without psychotic symptoms, anxiety disorder, predominantly obsessional thoughts or ruminations, acute stress reaction, post-traumatic stress disorder, adjustment disorders, and nonorganic insomnia) and objective patient-care outcomes (such as the 14-day readmission rate, preventable hospitalization rate, and non-urgent ED-visit rate) obtained from the National Insurance Research Database in Taiwan to investigate the linkage between physician mental health disorders and healthcare quality. The data collection process used in this study not only has a higher likelihood of generating fewer measurement errors compared to survey methods employed in previous studies, but it also enhances the robustness and validity of our findings regarding the relationship between physician mental health disorders and healthcare quality.
This study, nevertheless, is subject to several limitations. First, although the clinical diagnosis codes utilized in this study to calculate the prevalence of mental health disorders were based on previous research,4 it is important to acknowledge that the prevalence of mental health disorders may vary depending on the inclusion of specific clinical diagnosis codes. To mitigate potential biases stemming from the inclusion of clinical diagnosis codes, our analyses utilize a relative measure of mental health disorders, namely the ratio of physician mental health disorders prevalence to general population mental health disorders prevalence. Second, this study falls under the category of ecological time series analysis. In order to avoid the ecological fallacy,59 our empirical results cannot be interpreted as directly capturing individual patients’ decision-making regarding healthcare utilization (eg, inpatient, outpatient, and emergency care) or their individual social distancing behaviors in response to changes in physician mental health disorders during the COVID-19 pandemic outbreak. We recommend that future studies collect individual-level data to explore the interplay between changes in physician mental health, patients’ healthcare-seeking decisions, and individuals’ social distancing behaviors during the COVID-19 pandemic outbreak within Taiwan’s NHI system.
Conclusion
Although there is a substantive body of literature investigating the impact of physician mental health disorders on healthcare quality, the asymmetric relationship between these two variables remains unexamined in the field of healthcare services. In order to unravel this asymmetric relationship, we applied the QQRM proposed by Sim and Zhou50 to investigate the asymmetric effect of physician mental health disorders on healthcare quality during the COVID-19 pandemic outbreak in Taiwan for the first time. Daily data for inpatient, outpatient, and emergency care quality indicators (represented by the 14-day readmission rate, preventable hospitalization rate, and overall non-urgent ED-visit rate, respectively) and physician mental health disorders were collected from the National Insurance Research Database in Taiwan. Additionally, the Google COVID-19 Community Mobility Report provided daily data on the time spent in various categories of places (including retail and recreation, grocery and pharmacy, parks, transit stations, workplaces, and residential areas) compared to a baseline period before the pandemic. These data were used to calculate the social distance index, which served as a control variable to measure the extent of individual behavior change during the COVID-19 pandemic outbreak. The sample period spanned from February 15, 2020, to December 31, 2020, resulting in a total of 321 daily observations.
Our results revealed that the overall aggregate effects of each quantile of physician mental health disorders on the cumulative quantiles of healthcare quality are negative (positive) for the 14-day readmission rate (preventable hospitalization rate, and non-urgent ED-visit rate). Moreover, we observed that the cumulative effects of each quantile of physician mental health disorders on the high quantiles of the 14-day readmission rate are negative, while they are positive for the low and middle quantiles. In contrast, the cumulative effects of each quantile of physician mental health disorders on various quantiles of the non-urgent ED-visit rate exhibit the opposite pattern as that seen for the 14-day readmission rate. Furthermore, the positively (negatively) cumulative effects of each quantile of physician mental health disorders are detected in the middle (low and high) quantiles of the preventable hospitalization rate.
The underlying message drawn from the variation in the relationship between physician mental health disorders and different quantiles of healthcare quality delivery suggests that the impact of physician mental health disorders on healthcare quality is not straightforward within the inpatient, outpatient, and ED care sectors of Taiwan’s NHI system. This complexity remains, despite the average prevalence of mental health disorders among physicians was 43.80% higher than that among the general population during the COVID-19 pandemic outbreak. Therefore, strategic interventions, including the promotion of physician support systems, enhancements to working environments, provision of incentives to motivate physicians, and efforts to rebuild public confidence in healthcare service accessibility, should be carefully tailored based on the observed level of care quality when facing a higher risk of physician mental health disorders during pandemic outbreak conditions.
Ethics
The secondary data were extracted from the National Insurance Research Database administrated by the Health and Welfare Data Science Center in Taiwan, and data collection process was approved by the Research Ethics Committee of Taichung Tzu Chi Hospital with the Certificate ID: REC111-23.
Acknowledgments
The authors would like to thank the editor of the journal and the two anonymous referees for their insightful comments and suggestions that allowed us to improve the quality of this study. A special gratitude goes to Tr. W.W. Liu for her unwavering support throughout the study period. The final proof-reading of the study by Lisa Brutcher (at Washington State University, USA) is deeply acknowledged. All errors are ours.
Funding
This research has been supported by the National Science and Technology Council in Taiwan for the research project entitled “The detection of the overloaded capacity phenomenon under Taiwan’s healthcare system through healthcare workers’ burnout: evidence from the COVID 19 pandemic outbreak and its connection with quality of healthcare” with Grant No. 111-2410-H-025-009.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ryan E, Hore K, Power J, Jackson T. The relationship between physician burnout and depression, anxiety, suicidality and substance abuse: a mixed methods systematic review. Front Public Health. 2023;11:1133484. doi:10.3389/fpubh.2023.1133484
2. Adam AR, Golu FT. Prevalence of depression among physicians: a comprehensive meta-analysis. Roman Med J. 2021;68(3):327–337. doi:10.37897/RMJ.2021.3.1
3. Harvey SB, Epstein RM, Glozier N, et al. Mental illness and suicide among physicians. Lancet. 2021;398(10303):920–930. doi:10.1016/S0140-6736(21)01596-8
4. Petrie K, Crawford J, Baker STE, et al. Interventions to reduce symptoms of common mental disorders and suicidal ideation in physicians: a systematic review and meta-analysis. Lancet Psychiat. 2019;6(3):225–234. doi:10.1016/S2215-0366(18)30509-1
5. Peck JA, Porter TH. Pandemics and the impact on physician mental health: a systematic review. Med Care Res Rev. 2022;79(6):772–788. doi:10.1177/10775587221091772
6. Alkhamees AA, Aljohani MS, Kalani S, et al. Physician’s burnout during the Covid-19 pandemic: a systematic review and meta-analysis. Int J Environ Res Public Health. 2023;20(5):4598. doi:10.3390/ijerph20054598
7. Magnavita N, Soave PM, Ricciardi W, Antonelli M. Occupational stress and mental health among anesthetists during the Covid-19 pandemic. Int J Environ Res Public Health. 2020;17(21):8245. doi:10.3390/ijerph17218245
8. Taş BG, Özceylan G, Öztürk GZ, Toprak D. Evaluation of job strain of family physicians in Covid-19 pandemic period- an example from Turkey. J Community Health. 2021;46(4):777–785. doi:10.1007/s10900-020-00950-5
9. Almater AI, Tobaigy MF, Younis AS, Alaqeel MK, Abouammoh MA. Effect of 2019 Coronavirus pandemic on ophthalmologists practicing in Saudi Arabia: a psychological health assessment. Middle East Afr J Ophthalmol. 2020;27(2):79–85. doi:10.4103/meajo.MEAJO_220_20
10. Varani S, Ostan R, Franchini L, et al. Caring advanced cancer patients at home during Covid-19 outbreak: burnout and psychological morbidity among palliative care professionals in Italy. J Pain Sympt Manage. 2021;61(2):e4–e12. doi:10.1016/j.jpainsymman.2020.11.026
11. Elbay RY, Kurtulmuş A, Arpacıoğlu S, Karadere E. Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Res. 2020;290:113130. doi:10.1016/j.psychres.2020.113130
12. Li W, Frank E, Zhao Z, et al. Mental health of young physicians in China during the novel Coronavirus disease 2019 outbreak. JAMA Network Open. 2020;3(6):e2010705. doi:10.1001/jamanetworkopen.2020.10705
13. Dewa CS, Loong D, Bonato S, Trojanowski L. The relationship between physician burnout and quality of healthcare in terms of safety and acceptability: a systematic review. BMJ Open. 2017;7(6):e015141. doi:10.1136/bmjopen-2016-015141
14. Dewa CS, Loong D, Bonato S, Trojanowski L, Rea M. The relationship between resident burnout and safety-related and acceptability-related quality of healthcare: a systematic literature review. BMC Med Educ. 2017;7(1):195. doi:10.1186/s12909-017-1040-y
15. Mangory KY, Ali LY, Rø K, Tyssen R. Effect of burnout among physicians on observed adverse patient outcomes: a literature review. BMC Health Serv Res. 2021;21(1):369. doi:10.1186/s12913-021-06371-x
16. Al-Ghunaim TA, Johnson J, Biyani CS, Alshahrani KM, Dunning A, O’Connor DB. Surgeon burnout, impact on patient safety and professionalism: a systematic review and meta-analysis. The American Journal of Surgery. 2022;224(1):228–238. doi:10.1016/j.amjsurg.2021.12.027
17. Hodkinson A, Zhou A, Johnson J, et al. Associations of physician burnout with career engagement and quality of patient care: systematic review and meta-analysis. BMJ. 2022;378:e070442. doi:10.1136/bmj-2022-070442
18. Pereira-Lima K, Mata DA, Loureiro SR, Crippa JA, Bolsoni LM, Sen S. Association between physician depressive symptoms and medical errors: a systematic review and meta-analysis. JAMA Network Open. 2019;2(11):e1916097. doi:10.1001/jamanetworkopen.2019.16097
19. Casalino LP, Li J, Peterson LE, et al. Relationship between physician burnout and the quality and cost of care for medicare beneficiaries is complex. Health Aff. 2022;41(4):549–556. doi:10.1377/hlthaff.2021.00440
20. Hewitt DB, Ellis RJ, Chung JW, et al. Association of surgical resident wellness with medical errors and patient outcomes. Ann Surg. 2021;274(2):396–402. doi:10.1097/SLA.0000000000003909
21. Hall LH, Johnson J, Watt I, O’Connor DB. Association of GP wellbeing and burnout with patient safety in UK primary care: a cross-sectional survey. Br J Gener Pract. 2019;69(684):e507–e514. doi:10.3399/bjgp19X702713
22. Tawfik DS, Profit J, Morgenthaler TI, et al. Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clinic Proceed. 2018;93(11):1571–1580. doi:10.1016/j.mayocp.2018.05.014
23. Sulaiman CFC, Henn P, Smith S, O’Tuathaigh CMP. Burnout syndrome among non-consultant hospital doctors in Ireland: relationship with self-reported patient care. Intern J Qual Health Care. 2017;29(5):679–684. doi:10.1093/intqhc/mzx087
24. Loerbroks A, Glaser J, Vu-Eickmann P, Angerer P. Physician burnout, work engagement and the quality of patient care. Occupat Med. 2017;67(5):356–362. doi:10.1093/occmed/kqx051
25. Wen J, Cheng Y, Hu X, Yuan P, Hao T, Shi Y. Workload, burnout, and medical mistakes among physicians in China: a cross-sectional study. Biosci Trends. 2016;10(1):27–33. doi:10.5582/bst.2015.01175
26. Owoc J, Mańczak M, Tombarkiewicz M, Olszewski R. Burnout, well‑being, and self‑reported medical errors among physicians. Polish Archiv Inter Med. 2021;131(7–8):626–632. doi:10.20452/pamw.16033
27. Menon NK, Shanafelt TD, Sinsky CA, et al. Association of physician burnout with suicidal ideation and medical errors. JAMA Network Open. 2020;3(12):e2028780. doi:10.1001/jamanetworkopen.2020.28780
28. Garrouste-Orgeas M, Perrin M, Soufir L, et al. The Iatroref study: medical errors are associated with symptoms of depression in ICU staff but not burnout or safety culture. Intensive Care Med. 2015;41(2):273–284. doi:10.1007/s00134-014-3601-4
29. Guillou P, Pelaccia T, Bacqué MF, Lorenzo M. Does burnout affect clinical reasoning? an observational study among residents in general practice. BMC Med Educ. 2021;21(1):35. doi:10.1186/s12909-020-02457-y
30. Brunsberg KA, Landrigan CP, Garcia BM, et al. Association of pediatric resident physician depression and burnout with harmful medical errors on inpatient services. Acad Med. 2019;94(8):1150–1156. doi:10.1097/ACM.0000000000002778
31. Sun BZ, Chaitoff A, Hu B, Neuendorf K, Manne M, Rothberg MB. Empathy, burnout, and antibiotic prescribing for acute respiratory infections: a cross-sectional primary care study in the US. Br J Gener Pract. 2017;67(661):e565–e571. doi:10.3399/bjgp17X691901
32. Kwah J, Weintraub J, Fallar R, Ripp J. (2016) The effect of burnout on medical errors and professionalism in first-year internal medicine residents. J Grad Med Educ. 2016;8(4):597–600. doi:10.4300/JGME-D-15-00457.1
33. Rabatin J, Williams E, Manwell LB, Schwartz MD, Brown RL, Linzer M. Predictors and outcomes of burnout in primary care physicians. J Prim Care Community Health. 2016;7(1):41–43. doi:10.1177/2150131915607799
34. Zhang H, Khan A, Chen Q, Larsson H, Rzhetsky A, Munafò M. Do psychiatric diseases follow annual cyclic seasonality? PLoS Biol. 2021;19(7):e3001347. doi:10.1371/journal.pbio.3001347
35. Chakrabarti S, Singh N. Psychotic symptoms in bipolar disorder and their impact on the illness: a systematic review. World J Psych. 2022;12(9):1204–1232. doi:10.5498/wjp.v12.i9.1204
36. Jiang W, Chen Y. Air pollution, foreign direct investment, and mental health: evidence from China. Front Public Health. 2022;10:858672. doi:10.3389/fpubh.2022.858672
37. Chen AY, Sturm R. Depressive symptoms among US adults during the Great recession and economic recovery. J Ment Health Policy Econom. 2022;25(1):3–10.
38. Chen WY, Chang T, Lin YH. Investigating the persistence of suicide in the United States: evidence from the quantile unit root test. Soc Indic Res. 2018;135(2):813–833. doi:10.1007/s11205-016-1492-1
39. Chang T, Cai Y, Chen WY. Are suicide rate fluctuations transitory or permanent? panel KSS unit root test with a Fourier function through the sequential panel selection method. Roman J Econ Forecast. 2017;20(3):5–17.
40. Lin YH, Chen WY. Does unemployment have asymmetric effects on suicide rates? evidence from the United States: 1928–2013. Econ Res Ekonomska Istraživan. 2018;31(1):1404–1417. doi:10.1080/1331677X.2018.1484788
41. Chang T, Chen WY. Revisiting the relationship between suicide and unemployment: evidence from linear and nonlinear cointegration. Econ Syst. 2017;41(2):266–278. doi:10.1016/j.ecosys.2016.06.004
42. Chen WY, Lin YH. On the relationship between business cycle and fertility rate in Taiwan: evidence from the nonlinear cointegration methodology. Roman J Econ Forecast. 2018;21(1):140–156.
43. Mishra A, Mishra V, Parasnis J. The asymmetric role of crime in women’s and men’s labour force participation: evidence from India. J Econ Behav Organ. 2021;188:933–961. doi:10.1016/j.jebo.2021.06.015
44. Cook S, Watson D, Parker L. (2014) New evidence on the importance of gender and asymmetry in the crime–unemployment relationship. Appl Econ. 2014;46(2):119–126. doi:10.1080/00036846.2013.835481
45. Liu YH, Chang WS, Chen WY. Health progress and economic growth in the United States: the Mixed Frequency VAR analyses. Qual Quant. 2019;53(4):1895–1911. doi:10.1007/s11135-019-00847-z
46. Chen W-Y. Health progress and economic growth in the USA: the continuous wavelet analysis. Empir Econ. 2016;50(3):831–855. doi:10.1007/s00181-015-0955-6
47. Pu X, Zeng M, Luo Y. The effect of business cycles on health expenditure: a story of income inequality in China. Front Public Health. 2021;9:653480. doi:10.3389/fpubh.2021.653480
48. Chen WY, Wen MJ, Lin YH, Liang YW. On the relationship between healthcare expenditure and longevity: evidence from continuous wavelet analyses. Qual Quant. 2016;50(3):1041–1057. doi:10.1007/s11135-015-0189-x
49. Ogburn WF, Thomas DS. The influence of the business cycle on certain social conditions. J Am Stat Assoc. 1922;18(139):324–340. doi:10.1080/01621459.1922.10502475
50. Sim N, Zhou H. (2015) Oil prices, US stock return, and the dependence between their quantiles. J Bank Finance. 2015;55:1–8. doi:10.1016/j.jbankfin.2015.01.013
51. Lai CC, Lee PI, Hsueh PR. How Taiwan has responded to COVID-19 and how COVID-19 has affected Taiwan, 2020–2022. J Microbiol Immunol Infec. 2023;56(3):433–441. doi:10.1016/j.jmii.2023.04.001
52. Chen WY. On the relationship among nurse staffing, inpatient care quality and hospital competition under the global budget payment scheme in Taiwan’s National health insurance system: mixed frequency VAR analyses. Systems. 2022;10(5):187. doi:10.3390/systems10050187
53. Chen WY. The effect of interdependences of referral behaviors on the quality of ambulatory care: evidence from Taiwan. Risk Manag Healthc Policy. 2021;14:4709–4721. doi:10.2147/RMHP.S338387
54. AHRQ. Prevention quality indicators technical specifications updates-version v2020 (ICD 10-CM/PCS). Maryland: Agency for Healthcare Research and Quality; 2020. Available from: https://www.qualityindicators.ahrq.gov/Modules/PQI_TechSpec_ICD10_v2020.aspx.
55. Ballard DW, Price M, Fung V, et al. Validation of an algorithm for categorizing the severity of hospital emergency department visits. Med Care. 2010;48(1):58–63. doi:10.1097/MLR.0b013e3181bd49ad
56. Vokó Z, Pitter JG. The effect of social distance measures on COVID-19 epidemics in Europe: an interrupted time series analysis. Geroscience. 2020;42(4):1075–1082. doi:10.1007/s11357-020-00205-0
57. Phillips PCB, Perron P. Testing for a Unit Root in time series regression. Biometrika. 1988;75:335–346. doi:10.1093/biomet/75.2.335
58. Balme E, Gerada C, Page L. Doctors need to be supported, not trained in resilience. BMJ. 2015;351:h4709. doi:10.1136/bmj.h4709
59. Robinson WS. Ecological Correlations and the Behavior of Individuals. Am Sociol Rev. 1950;15(3):351–357. doi:10.2307/2087176
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.