Back to Journals » International Journal of General Medicine » Volume 19
Olfactory Decline in Elderly at High Altitudes: A Narrative Review
Received 6 January 2026
Accepted for publication 9 April 2026
Published 16 April 2026 Volume 2026:19 594165
DOI https://doi.org/10.2147/IJGM.S594165
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Xingjian Chen, Yufen Guo
Department of Otolaryngology, The Second Hospital & Clinical Medical School, Lanzhou University, Lanzhou, Gansu, 730030, People’s Republic of China
Correspondence: Yufen Guo, Department of Otolaryngology, The Second Hospital & Clinical Medical School, Lanzhou University, No. 82, Cuiyingmen, Chengguan District, Lanzhou, Gansu, 730030, People’s Republic of China, Email [email protected]
Abstract: Olfactory dysfunction is highly prevalent in the elderly population, severely affecting nutritional status, environmental safety perception, and quality of life, and is recognized as an early warning marker of neurodegenerative diseases. Compared with populations living at low altitudes, residents at high altitudes are chronically exposed to combined extreme environmental conditions including hypoxia, low temperature, and low humidity, which may lead to more complex and severe degenerative changes in the olfactory system. However, existing evidence remains fragmented, and a systematic synthesis is lacking. This narrative review aims to systematically integrate the epidemiological characteristics, pathophysiological mechanisms, diagnostic assessment tools, intervention strategies, and health risks associated with olfactory decline in elderly residents at high altitudes. Epidemiological evidence shows a significant negative correlation between altitude and olfactory function, and the effects of aging are substantially amplified under high-altitude conditions. The underlying mechanisms primarily involve chronic hypoxia interacting with aging and genetic susceptibility through damage to olfactory ensheathing cells, suppression of olfactory neurogenesis, and remodeling of synaptic plasticity in olfactory-related brain regions. Olfactory behavioral testing combined with functional magnetic resonance imaging and emerging biomarkers provides multidimensional tools for early diagnostic stratification. Although oxygen therapy, olfactory training, and environmental management have shown potential efficacy, evidence-based data specific to this population remain limited. The core value of this review lies in adopting an integrated perspective of “environment-aging” interactions to systematically elucidate the combined effects of high-altitude stress and age-related degenerative changes on the olfactory system, revealing the unique patterns and intervention targets for olfactory dysfunction in this vulnerable population. Future research urgently needs large-scale longitudinal cohort studies, establishment of altitude-specific normative olfactory assessment tools, and development of precision interventions targeting hypoxic injury to improve overall health outcomes in this population.
Keywords: high‑altitude, olfactory decline, elderly, hypoxia, review
Background
Olfaction is a crucial sensory function for detecting chemical signals, playing essential roles in food identification, environmental hazard perception, emotional regulation, and memory formation. With advancing age, the olfactory system undergoes degenerative changes, leading to a significant increase in the prevalence of olfactory dysfunction among older adults. Due to its insidious onset and slow progression, olfactory impairment has long been underappreciated. However, accumulating evidence suggests that olfactory decline not only affects nutritional intake, safety perception, and quality of life in the elderly but also serves as an early clinical marker for neurodegenerative diseases such as Alzheimer’s disease and Parkinson’s disease.1
Currently, research on olfactory decline in the elderly has predominantly focused on normoxic, low-altitude regions, whereas evidence regarding older populations residing in high-altitude environments (≥2500 m) remains limited. High-altitude regions are characterized by chronic hypoxia, hypobaria, low temperature, and low humidity,2 constituting a sustained composite environmental stress. Chronic hypoxia in this context refers to sustained hypobaric hypoxic exposure resulting from continuous residence at altitudes ≥2500 m for months to years, with clinical reference thresholds such as PaO2 <60 mmHg or arterial oxygen saturation <90% serving as indicators.3 Under such conditions, environmental factors—particularly chronic hypoxia—may interact with the aging process, further impairing neurogenesis, synaptic plasticity, and regenerative capacity of the olfactory system, thereby exacerbating olfactory dysfunction.
However, current knowledge regarding the interplay among high-altitude environments, aging, and olfactory dysfunction remains fragmented, lacking systematic synthesis and integration. Therefore, this review focuses on olfactory dysfunction in elderly residents at high altitudes, systematically summarizing epidemiological characteristics, underlying mechanisms, diagnostic approaches, intervention strategies, and associated health risks, with the aim of providing a theoretical basis and practical reference for early identification and precise management of this vulnerable population, as illustrated in Figure 1.
 |
Figure 1 Technical roadmap of the present review on olfactory decline in elderly residents at high altitudes. The figure outlines the research framework and analytical modules of this review. Module 1 (Environmental Exposure): elderly populations in high-altitude regions are chronically exposed to multiple factors including hypoxia, air pollution, high ultraviolet radiation, and low temperature. Module 2 (Pathophysiological Mechanisms): chronic hypoxia and aging affect olfactory neurons and the olfactory bulb, with alterations including decreased expression of olfactory marker protein (OMP) and ADCY3, as well as increased reactive oxygen species (ROS) generation. Module 3 (Clinical Consequences): olfactory decline may contribute to malnutrition and neurodegenerative diseases, thereby affecting the quality of life in the elderly. |
Epidemiological Characteristics of Olfactory Decline in Elderly Populations at High Altitude
Current Status of Epidemiological Investigations on Olfactory Decline in Elderly Populations at High Altitude
Although epidemiological studies specifically focusing on olfactory decline in the elderly population residing at high altitudes remain limited, independent research on the effects of high-altitude-related factors and aging provides important insights.
Multiple cross-sectional studies indicate a direct association between high-altitude exposure and decreased olfactory function. A controlled study conducted by Altundağ et al in Turkey recruited 41 healthy adult volunteers, excluding confounding factors such as chronic sinusitis or nasal polyps4. The study assessed participants’ odor threshold and identification abilities using the “Sniffin Sticks” test in both a high-altitude environment at 2200 meters and at sea level. The results showed a significant decline in olfactory function under high-altitude conditions, with the odor threshold decreasing from 10.3 ± 2.0 at sea level to 7.8 ± 2.2, and the odor identification score decreasing from 13.6 ± 1.5 to 12.4 ± 1.5, both differences being statistically significant (p < 0.001). Correlation analysis revealed a significant negative correlation between altitude and olfactory scores (threshold: r = 0.49; identification: r = 0.39). No significant association was found between changes in threshold and changes in identification ability, suggesting that high altitude may affect olfactory sensitivity and discrimination through different mechanisms. Furthermore, high-altitude exposure acutely impairs olfactory function by affecting nasal physiology and sensory conduction. A study by Cemal Cingi et al found2 that mountaineers experienced a 27.43% decrease in peak nasal inspiratory flow (p < 0.001) and an 8.94% decrease in peak nasal expiratory flow (p < 0.05), alongside significant declines in odor detection and identification abilities (p < 0.05).5
Regarding age-related effects, a U.S. population-based analysis using the NHANES database reported that olfactory dysfunction increases significantly with age based on both subjective self-report and objective odor identification testing.6 The risk ratio for olfactory decline in individuals over 80 years old is 9.288 (7.265–11.873) based on objective testing.6 Of note, discrepancies between self-reported and objective measures of olfactory function have been documented, highlighting the importance of specifying the measurement method when interpreting prevalence estimates.6 A population-based study reported that the prevalence of olfactory impairment in older adults is 24.5%, with rates increasing to 62.5% among those aged 80 to 97 years.7 Olfactory dysfunction is more pronounced in the context of disease. Dan et al found that selective odor discrimination loss is the initial change in olfactory behavior with aging, followed by declines in odor sensitivity and detection ability, while odor habituation typically persists for a longer duration. Compared to behavioral changes related to cognitive and motor functions, OD is considered one of the earliest biomarkers of aging and an independent risk factor for mortality.8,9 Additionally, a larger longitudinal cohort study involving 1556 elderly individuals assessed olfactory function using the San Diego Odor Identification Test over a follow-up period of 5 to 10 years. The 5-year incidence of olfactory impairment was 12.5%, with the incidence steadily increasing with age. Multivariate analysis identified several risk factors significantly associated with an increased likelihood of olfactory impairment: age (OR = 1.79 per 5-year increase [95% CI: 1.61–2.00]).10 These studies collectively suggest a potential association between aging and olfactory decline.
Altitude Distribution Characteristics of Populations with Olfactory Decline
The impact of varying altitudes on olfactory decline is increasingly drawing attention in the academic field. Emerging evidence suggests that changes in altitude can affect neural structures and gene expression related to olfactory function.11–13
In a study involving individuals with long-term exposure in different altitude environments, healthcare workers residing at high altitudes (eg., 4300 meters) scored significantly lower on multiple cognitive assessments compared to those at low altitudes (eg., 1700 meters). These assessments included the Montreal Cognitive Assessment (MoCA), Digit Span Test (DST), Verbal Fluency Test (VFT), Rey Auditory Verbal Learning Test (RAVLT), and Trail Making Test (TMT). Structural MRI data further revealed reductions in gray matter density, particularly in regions such as the left olfactory cortex, indicating that prolonged exposure to hypoxic environments may lead to widespread cognitive impairment and region-specific neurodegeneration potentially linked to olfactory dysfunction.14
Gender and Age Distribution Characteristics of Olfactory Decline Populations
Among elderly residents in high-altitude regions, the distribution of olfactory decline exhibits distinct age-related patterns, whereas evidence regarding gender differences remains less clear.15–17
Age is a primary determinant of olfactory dysfunction.18,19 Multiple studies consistently report that the incidence of olfactory decline increases with advancing age.19–21 For example, research on community-dwelling older adults shows that the risk of olfactory impairment significantly rises with every five-year increase in age.10
The role of gender is ambiguous. In a study examining older adults with obstructive lung disease (OLD) (including 98 OLD patients [mean age 71.2 years, 59.2% female] and 1,036 non-OLD individuals [mean age 69.5 years, 58.9% female]), decline in odor identification ability was associated with frailty in OLD patients. However, after adjusting for demographic variables, alcohol consumption, smoking, and comorbidities, this association was not observed in the non-OLD group. Longitudinal data from a nationally representative sample of older U.S. adults (aged 57–85 years) demonstrate that the rate of olfactory decline increases with age and is significantly greater in men than in women, with men making 0.17 additional errors per 5 years compared with women after adjusting for psychosocial and health factors (p = 0.005).22 To date, early studies have also noted that females outperform males in odor identification tasks, with males exhibiting olfactory decline from a younger age. Even after adjusting for psychosocial factors and underlying health conditions, results indicate a more rapid decline in olfactory function among males compared to females, at a rate of −0.15 percentage points (95% CI: −0.25, −0.04, p=0.007).22
Notably, no significant gender-based differences were detected in the relationship between olfactory decline and frailty.23
Similarly, a retrospective analysis of patients with olfactory dysfunction found no significant gender differences in the etiological distribution of olfactory decline. However, the proportion of idiopathic olfactory impairment was notably higher among older adults compared to younger cohorts.24
Overall, current evidence suggests that age is a consistent predictor of olfactory decline, whereas gender differences remain inconclusive. Research specifically targeting elderly residents in high-altitude environments is still limited, and further studies are needed to clarify potential sex-specific influences in this population.
Evidence from In vivo and In vitro Studies on the Impact of High Altitude on Olfaction in the Elderly Population
Effect of High‑Altitude Hypoxia on Olfactory Neurons
The hypoxic environment characteristic of high altitude exerts multifaceted and profound effects on olfactory neurons. Evidence suggests that hypoxia disrupts the metabolism and functional integrity of these neurons.25–27
At the animal level, mice subjected to chronic high‑altitude hypoxia (5,000 m, 12 weeks) displayed learning and memory impairments associated with hippocampal dysfunction, alongside reduced expression levels of synaptic proteins such as synaptophysin (SYP) and spinophilin (SPH) in the olfactory cortex. These findings indicate that neural and synaptic integrity in olfactory‑related brain regions may be compromised under chronic high‑altitude exposure, potentially contributing to olfactory decline.28 Furthermore, genetic studies of high‑altitude‑adapted animals (eg., yaks) have identified significant differences in the number and composition of olfactory receptor (OR) genes compared to low-altitude bovine species.29,30 These genetic adaptations may influence olfactory performance and further suggest that long-term altitude exposure can drive evolutionary changes in olfactory function.31
At the cellular level, in vitro studies on olfactory ensheathing cells (OECs) isolated from the olfactory bulbs of neonatal rats have demonstrated that hypoxia induces significant cellular damage.32 Since OECs play a critical role in axonal growth and myelination of olfactory neurons, their dysfunction may compromise neuronal survival and regenerative capacity. Interestingly, curcumin has been shown to enhance OECs viability under hypoxic conditions, suggesting its potential neuroprotective role in mitigating hypoxia-induced olfactory deficits.32
At the molecular level, hypoxia also alters gene expression patterns related to neurogenesis and neuronal function.33,34 In mouse models, chronic intermittent hypoxia (CIH) has been shown to downregulate the mRNA levels of olfactory marker protein (OMP), Olfr1507, ADCY3, and GNAL within the olfactory epithelium.35 Conversely, it upregulates transcripts associated with neurogenesis and neuronal stress responses, including NGFR, CNPase, NGFRAP1, NeuN, and MAP-2. These changes indicate CIH disrupts olfactory neurogenesis and cellular function through broad transcriptional reprogramming (Figure 2).36
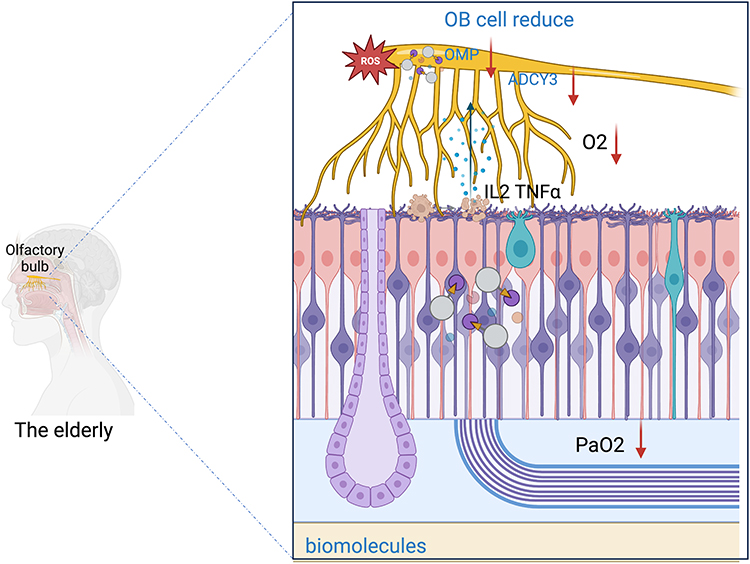 |
Figure 2 Schematic diagram of the mechanisms underlying high-altitude hypoxia-induced damage to the olfactory nervous system in the elderly. Long-term residence at altitudes ≥2500 m leads to chronic hypoxia (PaO2 ↓) combined with compounded environmental stressors including high ultraviolet radiation, air pollution, and low temperature. Hypoxia reduces the expression of olfactory marker protein (OMP) and ADCY3, while increasing reactive oxygen species (ROS) generation, resulting in damage and apoptosis of olfactory epithelial cells. Impairment of olfactory neurons further affects the number of fibers projecting to the olfactory bulb (OB) and synaptic stability, reducing neural circuit plasticity. Hypoxia activates the HIF pathway, but adaptive capacity declines with aging; concurrently, increased inflammatory markers and oxidative stress inhibit olfactory stem cell differentiation and survival of newly generated neurons. Blue arrows: pro‑inflammatory cytokine (IL‑2, TNF‑α) damage/interference to olfactory neurons. Red arrows: inhibition of signaling pathways (e.g., OMP, ADCY3); O2 ↓, PaO2 ↓: local hypoxic state. |
In addition, hypoxia may impair neurotransmitter signaling and synaptic plasticity in olfactory pathways, exacerbating dysfunction and accelerating decline.37 Nonetheless, the precise molecular and cellular mechanisms underlying these alterations remain incompletely understood and warrant further investigation.
Impairment of Olfactory Function by Pollutants in High-Altitude Environments
Research specifically addressing the impairment of pollutants on olfactory function in high-altitude environments remains limited. Nonetheless, existing evidence suggests that pollutants common to such regions-including industrial emissions, airborne dust particles, and storm-related particulate matter-may adversely affect the olfactory system.38,39
Indirect studies indicate that environmental pollutants can enter the human body via the respiratory tract, alter the nasal microenvironment and olfactory epithelium, and consequently impair olfactory performance.40,41 Epidemiological observations have shown that in areas with severe air pollution, the prevalence of both respiratory diseases and olfactory dysfunction is elevated, implying a detrimental role of pollutants in olfactory health.42
Dust storms, which are frequent in certain high-altitude regions, represent another potential risk factor.43 Particulate matter carried in dust can adsorb toxic compounds and directly irritate the olfactory mucosa.44 In addition, dust exposure can trigger inflammatory responses that disrupt the structural and functional integrity of olfactory receptor neurons.45,46 These mechanisms collectively contribute to olfactory impairment.
Despite these insights, specific mechanisms and related studies on olfactory impairment caused by particular pollutants in high-altitude regions remain scarce. Further targeted research is needed to clarify the relationship between environmental pollutants in high-altitude areas and olfactory decline.
The Impact of High‑Altitude Related Disorders on Olfactory Function
High-altitude illness refers to a series of pathological conditions caused by rapid ascent or prolonged residence in a hypoxic environment.47 Emerging evidence suggests a possible association between olfactory decline and high-altitude illness,48 though the underlying mechanisms remain incompletely understood.
Acute Mountain Sickness (AMS) is among the most common conditions in high-altitude regions.49 Studies have reported that individuals with AMS may exhibit impaired olfactory function, manifested as elevated odor thresholds and reduced odor discrimination and identification abilities.50,51 While the specific mechanisms remain unclear, these changes may be related to systemic hypoxia, neuroinflammation, and neurological dysfunction associated with AMS.52,53
In contrast, chronic high-altitude illnesses-such as Chronic Mountain Sickness (CMS)-resulting from long-term exposure to high-altitude environments, may indirectly affect the olfactory system.54 CMS is often characterized by hematological abnormalities, including polycythemia and increased blood viscosity, which can impair cerebral blood flow.54 Reduced perfusion of olfactory centers in the brain may compromise neuronal function and contribute to olfactory decline.55
Despite these observations, research directly linking olfactory impairment with high-altitude illnesses is still limited and largely preliminary. More clinical and experimental studies are required to elucidate the intrinsic relationship between a high-altitude illness and olfactory dysfunction, as well as to uncover the molecular and physiological mechanisms involved.
Potential Interactive Mechanisms of Olfactory System Dysfunction in the Context of High Altitude and Aging
Combined Effects of Environmental Factors at High Altitude
The high-altitude environment is characterized by hypoxia, low temperature, reduced humidity, and enhanced ultraviolet radiation, all of which can adversely affect the olfactory system.56 Among these factors, hypoxia has been identified as a primary contributor to olfactory dysfunction.57
Clinical evidence suggests that hypoxia associated with Obstructive Sleep Apnea Syndrome (OSAS) may impair olfactory performance.58,59 A cross-sectional study involving 69 snoring patients (divided into mild [Apnea-Hypopnea Index (AHI) <15] and moderate-to-severe [AHI ≥15] groups), significant differences were observed in body mass index, mean oxygen saturation (SaO2), minimum SaO2, mean snoring duration, and olfactory function tests (using the Korean version of the Sniffin’ Sticks test I and II). AHI values significantly correlated with odor threshold scores, whereas mean SaO2 correlated with odor discrimination scores. These findings suggest that hypoxia and reduced nasal airflow may jointly contribute to olfactory impairment.60 Furthermore, high-altitude hypoxia may impair the development and function of olfactory neurons.51 Olfactory ensheathing cells (OECs) exhibit enhanced migratory capacity in response to brain-derived neurotrophic factor (BDNF) via TRPC channel activation, thereby promoting axonal regeneration and neuronal support in the olfactory system.61 However, hypoxic conditions impair OECs and affect their function. High-altitude hypoxia may disrupt olfactory function by damaging OECs.32
Beyond hypoxia, low temperatures may reduce enzymatic activity in the olfactory mucosa and slow the diffusion rate of odorant molecules;62 low humidity predisposes the nasal mucosa to dryness and ciliary dyskinesia, affecting the effective adsorption and transport of odorant molecules;63 intense ultraviolet radiation may indirectly damage olfactory epithelial cells by inducing oxidative stress.64 These factors often coexist in high-altitude environments, potentially producing additive or synergistic effects that collectively exacerbate the functional load on the olfactory system.
Mechanisms of Aging Effects on the Olfactory System
Olfactory function gradually declines with age, a process associated with various physiological and molecular changes.18,20,65
From a neurological perspective, studies have demonstrated a close link between type 2 diabetes (T2D) and olfactory dysfunction. In aged T2D rat models, the piriform cortex exhibits pathological alterations, including changes in NeuN-positive neurons and Calbindin-D28k-positive interneurons. These changes are accompanied by elevated cellular stress, as evidenced by c-Jun N-terminal kinase (JNK) phosphorylation, although no apoptosis is observed.66
From a genetic perspective, interindividual differences in olfactory sensitivity may be related to polymorphisms in genes associated with odorant-binding proteins (OBPs).67–69 A study of OBPIIa gene polymorphism (rs2590498) in 69 subjects found that individuals with the AA genotype had significantly higher odor threshold scores compared to those with GG or heterozygous genotypes. The AA genotype and A allele were associated with normal olfactory function, whereas the GG genotype and G allele were linked to hyposmia. These findings suggest that OBPIIa gene polymorphism may contribute to age-related differences in olfactory performance.70 Additionally, age-related changes in the olfactory epithelium also lead to functional decline. During aging, horizontal basal cells (HBCs), crucial for olfactory neuron regeneration, become activated. This is often accompanied by dysfunction in retinoic acid metabolism, resulting in diminished olfactory neuron regenerative capacity and increased respiratory epithelial metaplasia, both of which impair olfactory function.71
Interactive Effects of Genetic Variants Related to High-Altitude Adaptation and Olfactory Aging
Genetic factors play a crucial role in both olfactory decline and physiological adaptation to high-altitude environments, particularly for elderly residents of plateau regions.71–74
A notable example is the olfactory receptor gene Olfr78, which has been identified as functionally significant in both olfaction and hypoxia sensing.75 Olfr78 is highly and selectively expressed in oxygen-sensitive glomus cells of the carotid body. Studies on Olfr78-deficient mice show that these animals fail to increase ventilation in response to hypoxia, although their response to hypercapnia remains intact. This indicates that Olfr78 not only functions in olfactory perception but also acts as a lactate-sensitive hypoxia sensor, modulating the respiratory response to hypoxic conditions.76
Comparative genetic studies on yaks, which have evolutionarily adapted to high-altitude habitats, further highlight the role of genetic variation in olfactory function.77,78 Yaks possess a significantly lower number of olfactory receptor (OR) genes compared to low-altitude cattle species and lack receptors associated with compounds such as β-ionone and isovaleric acid (IVA). This may reflect an evolutionary adaptation to the reduced plant diversity in alpine environments and the underdeveloped sweat glands of yaks, both of which diminish the need for a highly diversified olfactory repertoire.31
In humans, genetic variants associated with high-altitude adaptation—such as those involved in oxygen transport, erythropoiesis, and vascular regulation—also influence the development and function of the nervous system, including olfactory pathways.73,79 While direct links between these variants and olfactory function remain underexplored, emerging evidence suggests that genetic adaptations to high altitude may indirectly affect sensory performance in the elderly population.72 Further research is needed to clarify these mechanisms and their implications for age-related olfactory decline.
Diagnostic Techniques for Olfactory Dysfunction in Elderly Residents at High Altitudes
Application of Olfactory Function Testing
Olfactory function testing serves as a critical tool for assessing olfactory decline in elderly populations residing at high altitudes. Standardized olfactory tests commonly used in the general population remain applicable in these environments.80 For example, the Sniffin’ Sticks test, a widely utilized clinical assessment, evaluates three key domains of olfactory performance: threshold, discrimination, and odor identification.81 Studies involving elderly high-altitude residents have confirmed its effectiveness in determining olfactory functional status.82
In addition to conventional methods, simplified screening approaches are being developed to facilitate easier screening of olfactory decline in elderly populations, particularly in resource-limited or high-altitude settings.83,84 One such tool is the 4-item Concise Olfactory Screening Test for the Elderly (4-CAST), which predicts olfactory dysfunction by incorporating variables such as age, type II diabetes status, overall olfactory visual analog scale (VAS) score, and safety-impact VAS score related to olfaction.85 In the development cohort, the 4-CAST model demonstrated strong predictive validity, with an area under the curve (AUC) of 0.805 (p < 0.001) for identifying individuals in the lowest 25th percentile of the Sniffin’ Sticks test. Validation results showed similar level of accuracy, correctly classifying 83.8% of participants. These findings highlight the potential clinical utility of 4-CAST as a rapid and reliable screening tool for olfactory decline among elderly high-altitude residents.85
Imaging Diagnosis
Imaging techniques provide valuable objective evidence for diagnosing olfactory decline in elderly residents of high-altitude regions.86 Structural magnetic resonance imaging (MRI) enables the assessment of morphological and volumetric changes in brain regions associated with olfaction.87 Studies in older adults with dementia but without cognitive impairment have demonstrated that impaired olfactory function is correlated with reduced volume in the hippocampus, entorhinal cortex, fusiform gyrus, and middle temporal cortex. These findings suggest that structural degeneration in these regions may be linked to olfactory dysfunction.88 In high-altitude environments, chronic hypoxia may accelerate degeneration in these regions. Thus, MRI examinations may assist in the early detection of structural alterations with olfactory decline-related brain.
Functional MRI (fMRI) provides complementary insights by detecting brain activity in response to olfactory stimuli.89 In patients with olfactory dysfunction, fMRI has revealed alteration activation patterns within primary olfactory cortices and the hippocampus, with changes correlating to behavioral measures. Among elderly high-altitude residents, fMRI offers the potential to uncover functional abnormalities in olfactory-related networks, thereby providing more precise diagnostic and prognostic information.90
However, high-altitude conditions pose imaging challenges. Environmental factors such as hypobaric hypoxia and technical limitations in MRI equipment performance may affect both image quality and diagnostic accuracy. Therefore, further methodological optimization and development of altitude-adapted imaging protocols are required to enhance the reliability of MRI-based diagnostics in these settings.
Research on Biomarkers
The identification of biomarkers for olfactory decline holds significance for the early diagnosis and timely intervention of olfactory impairment in elderly populations residing at high altitudes. Insights from studies on neurodegenerative and metabolic diseases suggest potential candidates that may also be relevant in this context.
In Alzheimer’s disease (AD), both structural and functional alterations in the primary olfactory cortex (POC) have been proposed as biomarkers of olfactory decline and disease progression.91 In one study including 27 cognitively normal (CN), 21 mild cognitive impairment (MCI), and 15 AD subjects, revealed significant atrophy of the POC and hippocampus was observed in MCI and AD groups, correlating with behavioral olfactory measures. Importantly, reductions in olfactory activation volume within the POC and hippocampus were more pronounced in the MCI patients than the degree of tissue atrophy, resembling the pattern observed in the AD. These findings suggest that olfactory functional magnetic resonance imaging (fMRI) may provide an earlier and more sensitive biomarker of neurodegeneration compared to structural imaging alone in AD and MCI patients.92
Beyond neuroimaging, genetic and protein biomarkers have also attracted attention. In studies of patients with type 2 diabetes mellitus (T2DM), a panel of biomarkers-including plasma β-amyloid (Aβ), platelet glycogen synthase kinase-3β (GSK-3β), apolipoprotein E (ApoE) genotype, and olfactory function measures-proved effective in diagnosing MCI. Among these, decline in olfactory function emerged as a key predictive indicator, highlighting the potential utility of combining olfactory testing with molecular biomarkers for early detection of cognitive decline in metabolic disorders.93 For elderly populations at high altitudes, chronic hypoxia may modulate these biomarkers through pathways involving inflammatory responses, oxidative stress, and hypoxia-inducible factors (HIFs). Although direct evidence in high-altitude cohorts remains limited, these candidate biomarkers are potentially feasible to measure and warrant investigation in future studies targeting olfactory decline in this population.
Further research into these established biomarkers, along with the discovery of novel molecular and imaging biomarkers specific to high-altitude elderly populations, are essential. Such efforts will enhance the precision and timeliness of diagnosing olfactory decline and may ultimately contribute to improved strategies for prevention and intervention.
Several limitations of current diagnostic approaches should be acknowledged. First, most olfactory tests, imaging modalities, and biomarkers have been validated primarily in low-altitude populations, and their applicability to elderly residents at high altitudes remains to be established. Second, the feasibility of advanced imaging techniques such as fMRI in high-altitude settings may be affected by equipment stability and the lack of altitude-specific protocols. Third, although biomarkers associated with hypoxic stress have been identified, their specificity for olfactory decline requires further validation in high-altitude cohorts.
Treatment Strategies for Olfactory Dysfunction in Elderly High-Altitude Residents
Intervention Measures for Olfactory Decline in High-Altitude Environments
Targeted interventions are essential for addressing olfactory decline associated with high-altitude environments. One major strategy involves mitigating hypoxia stress. The use of oxygen delivery devices to improve systemic oxygenation in elderly high-altitude residents has been shown to alleviate hypoxia-induced neuronal damage, thereby improving olfactory function. In some medical institutions located in high-altitude regions, oxygen therapy is routinely offered to elderly patients.94 Clinical observations indicate that certain individuals experience partial improvements in olfactory performance following oxygen supplementation, although outcomes vary depending on individual physiological and health factors.95
Another commonly employed intervention is nasal irrigation, aimed at reducing the harmful effects of dust, pollutants, and other irritants frequently encountered in high-altitude settings.96,97 Regular irrigation can help cleanse the nasal cavity, minimize direct stimulation of the olfactory epithelium by harmful substances, and alleviate inflammatory responses, thus contributing to the maintenance of olfactory function.97 Evidence from clinical studies suggests that irrigation with saline or specialized solutions can improve the nasal microenvironment and provide symptomatic relief for some patients experiencing olfactory decline.97
Beyond direct clinical interventions, environmental management plays a critical preventive role. Strategies such as reducing pollutant emissions, strengthening dust control, and improving overall air quality in high-altitude regions are vital for protecting nasal and olfactory health. By combining individual-level interventions with population-level environmental measures, a more comprehensive approach to the prevention and treatment of olfactory decline in elderly high-altitude residents can be achieved.
Application of Pharmacotherapy in Elderly High-Altitude Residents
Pharmacotherapy may provide therapeutic benefits in managing olfactory decline among elderly residents living at high altitudes. Several pharmacological approaches have shown potential in supporting neuronal survival and mitigating hypoxia-related damage.98,99
Brain-derived neurotrophic factor (BDNF) plays a crucial in neural development, plasticity, and functional maintenance.100 It is theorized that BDNF could promote the survival and regeneration of olfactory neurons, thereby counteracting hypoxia-induced decline.101 While large-scale clinical studies investigating BDNF specifically for olfactory impairment in elderly high-altitude populations are currently lacking, evidence from basic research and studies on other neurological conditions suggests positive effects on neural repair and regeneration, indicating its potential therapeutic value in this context.100
In addition, antioxidant therapies may counteract the oxidative stress associated with chronic hypoxia in high-altitude environments. Curcumin, for instance, has demonstrated the ability to protect olfactory ensheathing cells (OECs) under hypoxic conditions and to mitigate oxidative damage in olfactory neurons.32 Results from in vitro experiments and small-scale human studies indicate that curcumin possesses both antioxidant and neuroprotective effects, although its specific efficacy in elderly high-altitude residents remains to be confirmed through larger clinical trials.32
Pharmacotherapy in this population faces significant challenges, including altered drug metabolism, potential side effects, and variability in treatment response. Future research is needed to determine the most appropriate pharmacological agents, optimize dosage regimens, and evaluate long-term safety and efficacy for elderly high-altitude residents experiencing olfactory decline.
Olfactory Training and Rehabilitation Methods
Olfactory training has emerged as a promising non-pharmacological intervention for olfactory decline and may hold particular value for elderly residents in high-altitude environments. Multiple studies have demonstrated its effectiveness in improving olfactory function.102,103 A systematic review and meta-analysis involving 639 patients reported statistically significant improvements in threshold, discrimination, and identification (TDI) scores (mean difference [MD] 3.77; 95% confidence interval [CI], 2.28–5.26), as well as in odor discrimination (MD 1.92; 95% CI, 1.13–2.71) and odor identification (MD 1.61; 95% CI, 0.55–2.68). No significant improvement was observed in odor threshold (MD −0.01; 95% CI, −0.42–0.39), indicating that olfactory training olfactory training primarily enhances discrimination and identification rather than sensitivity.104
Further evidence comes from research on COVID-19-related olfactory dysfunction. In a prospective study, 57 COVID-19 patients underwent standardized olfactory training, and those who adhered to the regimen showed greater mid-term improvement in psychophysical olfactory scores compared to non-adherent individuals. These findings support broader applicability of olfactory training across etiologies, including in populations vulnerable to hypoxia-induced olfactory decline such as elderly high-altitude residents.105
In addition, emerging multimodal rehabilitation approaches-such as combining olfactory training with visual or cognitive stimuli-may further enhance treatment outcomes. However, optimal training protocols, duration, and integration with adjunctive therapies remain areas requiring further clinical investigation.
The evidence supporting current therapeutic strategies in elderly high-altitude populations remains limited. Most interventions have been evaluated in small-scale studies with heterogeneous outcome measures and short follow-up durations. Moreover, the pharmacokinetic and pharmacodynamic profiles of pharmacological agents may be altered by chronic hypoxia and age-related changes in hepatic and renal function, yet systematic studies in this population are lacking. Olfactory training, while non-invasive, requires standardized protocols tailored to this specific population. Future randomized controlled trials with adequate statistical power are needed to establish evidence-based guidelines.
Health Risks and Future Perspectives of Olfactory Decline in Elderly Residents at High Altitudes
Impact of Olfactory Decline on the Quality of Life of Elderly Residents at High Altitudes
Olfactory decline exerts wide-ranging adverse effects on the quality of life of elderly individuals living in high-altitude areas.
Firstly, olfactory function is closely related to dietary experience and nutrition.106 A diminished sense of smell reduces the ability to perceive food odors, which can negatively affect appetite, food preference, and overall dietary intake and nutritional intake.
Secondly, olfactory impairment affects social interactions and psychological well-being. The sense of smell contributes to recognizing familiar scents, perceiving interpersonal cues such as body odor, and maintaining social connectedness. Loss of this ability may lead to discomfort, self-consciousness, and avoidance of social activities. This can foster social isolation, loneliness, and adverse mental health outcomes in elderly populations.
Finally, olfactory dysfunction poses safety risks by reducing the ability to detect hazardous environmental odors, such as smoke from fires, or gas leaks. This diminished hazard perception may significantly increase vulnerability in elderly high-altitude residents, further compromising quality of life and safety.
Relationship Between Olfactory Decline and Malnutrition in Elderly Residents at High Altitudes
A bidirectional relationship likely exists between olfactory decline and malnutrition among elderly residents in high-altitude regions.
On one hand, olfactory impairment reduces the perception of food odors, which can diminish appetite and decrease overall food intake.107 This effect is particularly pronounced for nutrient-rich foods with subtle aromas, leading to an increased risk of malnutrition.108 Studies have shown that individuals with olfactory dysfunction are more prone to protein-energy malnutrition and may also exhibit inadequate intake of essential vitamins and minerals.109,110
On the other hand, malnutrition itself may exacerbate olfactory dysfunction.111 Deficiencies in nutrients critical for olfactory function, such as vitamin A and zinc, can impair neuronal metabolism and compromise the structural and functional integrity of olfactory neurons, thereby worsening olfactory performance.111
Food diversity, and dietary habits already contribute to unbalanced nutrient intake among elderly residents.112,113 Olfactory decline may further aggravate these issues, creating a vicious cycle in which impaired olfaction and malnutrition perpetuate one another.
Therefore, comprehensive interventions that address both olfactory function and nutritional status are crucial for improving the overall well-being of elderly high-altitude populations.
Conclusions and Future Directions
Olfactory decline in elderly residents at high altitudes significantly affects quality of life, nutritional status, social participation, and safety awareness. Although existing studies provide preliminary evidence for early identification, diagnosis, and intervention, many unknowns remain regarding the pathological mechanisms, epidemiological characteristics, and comprehensive intervention strategies for olfactory decline in this population under high-altitude conditions.
Future research should strengthen longitudinal cohort and large-scale multicenter investigations to systematically evaluate the long-term effects of high-altitude exposure, aging processes, and genetic adaptability on olfactory function, and to establish reliable risk prediction models. At the same time, integrated diagnostic tools combining structural and functional imaging with molecular and protein biomarkers should be developed to enable early detection and disease monitoring. Regarding intervention strategies, the pharmacokinetic and pharmacodynamic profiles of elderly high-altitude populations warrant careful consideration. Polypharmacy, age-related decline in hepatic and renal function, and the hypoxic environment may alter drug absorption, distribution, metabolism, and elimination, directly affecting treatment efficacy and safety. Therefore, tailored strategies should be developed for pharmacological interventions and clinical management. Moreover, multimodal comprehensive interventions remain key to improving olfactory health in elderly high-altitude residents, including medical management, nutritional support, psychological intervention, environmental optimization, and olfactory training. Notably, incorporating health education into the intervention framework can enhance residents’ awareness and self-management capacity regarding olfactory function, nutritional status, environmental exposure risks, and daily safety, thereby improving the sustainability and overall effectiveness of interventions. Personalized strategies based on individual genetic background, altitude exposure level, and health status will help maximize efficacy and minimize risks.
By integrating basic research, epidemiological investigations, and multidisciplinary intervention strategies, future research and practice are expected to provide more scientific, effective, and sustainable olfactory health management solutions for elderly residents in high-altitude regions, thereby improving their quality of life and overall health, and providing an evidence base for public health policy development.
Ethics Statement
As this is a narrative review based on published literature, ethical approval and informed consent are not applicable.
Funding
This research has received funding by the Gansu province natural science foundation (NO.: 23JRRA1635).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Doty RL. Olfactory dysfunction in neurodegenerative diseases: is there a common pathological substrate? Lancet Neurol. 2017;16(6):478–15. doi:10.1016/S1474-4422(17)30123-0
2. Grocott M, Montgomery H, Vercueil A. High-altitude physiology and pathophysiology: implications and relevance for intensive care medicine. Crit Care. 2007;11(1):203. doi:10.1186/cc5142
3. West JB. High-altitude medicine. Am J Respir Crit Care Med. 2012;186(12):1229–1237. doi:10.1164/rccm.201207-1323CI
4. Altundağ A, Salihoglu M, Çayönü M, Cingi C, Tekeli H, Hummel T. The effect of high altitude on olfactory functions. Eur Arch Otorhinolaryngol. 2014;271(3):615–618. doi:10.1007/s00405-013-2823-3
5. Cingi C, Selcuk A, Oghan F, Firat Y, Guvey A. The physiological impact of high altitude on nasal and lower airway parameters. Eur Arch Otorhinolaryngol. 2011;268(6):841–844. doi:10.1007/s00405-010-1468-8
6. Noel J, Habib AR, Thamboo A, Patel ZM. Variables associated with olfactory disorders in adults: a U.S. population-based analysis. World J Otorhinolaryngol Head Neck Surg. 2017;3(1):9–16. doi:10.1016/j.wjorl.2017.02.005
7. Murphy C, Schubert CR, Cruickshanks KJ, Klein BE, Klein R, Nondahl DM. Prevalence of olfactory impairment in older adults. JAMA. 2002;288(18):2307–2312. doi:10.1001/jama.288.18.2307
8. Dan X, Yang B, McDevitt RA, et al. Loss of smelling is an early marker of aging and is associated with inflammation and DNA damage in C57BL/6J mice. Aging Cell. 2023;22(4):e13793. doi:10.1111/acel.13793
9. Pinto JM, Wroblewski KE, Kern DW, Schumm LP, McClintock MK. Olfactory dysfunction predicts 5-year mortality in older adults. PLoS One. 2014;9(10):e107541. doi:10.1371/journal.pone.0107541
10. Schubert CR, Cruickshanks KJ, Klein BE, Klein R, Nondahl DM. Olfactory impairment in older adults: five-year incidence and risk factors. Laryngoscope. 2011;121(4):873–878. doi:10.1002/lary.21416
11. Aboouf MA, Thiersch M, Soliz J, Gassmann M, Schneider Gasser EM. The brain at high altitude: from molecular signaling to cognitive performance. Int J Mol Sci. 2023;24(12):10179. doi:10.3390/ijms241210179
12. Xie JY, Zhang Y, Shen W, et al. Tracking neural activity patterns during rapid high-altitude transitions. Neuroimage. 2025;311:121197. doi:10.1016/j.neuroimage.2025.121197
13. Graham AM, Saputra E, Kirilenko B, et al. Convergent reduction of olfactory genes and olfactory bulb size in mammalian species at altitude. Curr Biol. 2025;35(13):3269–3277.e4. doi:10.1016/j.cub.2025.05.061
14. Zhang YQ, Zhang WJ, Liu JH, Ji WZ. Effects of chronic hypoxic environment on cognitive function and neuroimaging measures in a high-altitude population. Front Aging Neurosci. 2022;14:788322. doi:10.3389/fnagi.2022.788322
15. Wu Y, Jin Y, Deng L, et al. Long-Term high-altitude exposure, accelerated aging, and multidimensional aging-related changes. JAMA Network Open. 2025;8(5):e259960. doi:10.1001/jamanetworkopen.2025.9960
16. Mallet RT, Burtscher J, Richalet JP, Millet GP, Burtscher M. Impact of high altitude on cardiovascular health: current perspectives. Vasc Health Risk Manag. 2021;17:317–335. doi:10.2147/VHRM.S29412112
17. Levine BD, Zuckerman JH, deFilippi CR. Effect of high-altitude exposure in the elderly: the tenth mountain division study. Circulation. 1997;96(4):1224–1232. doi:10.1161/01.cir.96.4.122413
18. Kondo K, Kikuta S, Ueha R, Suzukawa K, Yamasoba T. Age-Related olfactory dysfunction: epidemiology, pathophysiology, and clinical management. Front Aging Neurosci. 2020;12:208. doi:10.3389/fnagi.2020.00208
19. Ruane R, Lampert O, Larsson M, Vetrano DL, Laukka EJ, Ekström I. Olfactory deficits and mortality in older adults. JAMA Otolaryngol Head Neck Surg. 2025;151(6):558–566. doi:10.1001/jamaoto.2025.0174
20. Papazian EJ, Pinto JM. Olfactory loss and aging: connections with health and well-being. Chem Senses. 2021;46:bjab045. doi:10.1093/chemse/bjab045
21. Pan Y, Chen H, Yuan Y, et al. Dysfunction in olfactory identification and physical function decline in older adults. JAMA Otolaryngol Head Neck Surg. 2026. doi:10.1001/jamaoto.2026.0072
22. Pinto JM, Wroblewski KE, Kern DW, Schumm LP, McClintock MK. The rate of age-related olfactory decline among the general population of older U.S. J Gerontol A Biol Sci Med Sci. 2015;70(11):1435–1441. doi:10.1093/gerona/glv072
23. Wang E, Wroblewski KE, McClintock MK, Pinto JM, Witt LJ. Olfactory decline develops in parallel with frailty in older US adults with obstructive lung diseases. Int Forum Allergy Rhinol. 2024;14(4):819–827. doi:10.1002/alr.23273
24. Okumura S, Saito T, Okazaki K, Fushimi K, Tsuzuki K. Clinical features of olfactory dysfunction in elderly patients. Auris Nasus Larynx. 2023;50(2):241–246. doi:10.1016/j.anl.2022.06.001
25. Wheaton WW, Chandel NS. Hypoxia. 2. Hypoxia regulates cellular metabolism. Am J Physiol Cell Physiol. 2011;300(3):C385–C393. doi:10.1152/ajpcell.00485.2010
26. Lee P, Chandel NS, Simon MC. Cellular adaptation to hypoxia through hypoxia inducible factors and beyond. Nat Rev Mol Cell Biol. 2020;21(5):268–283. doi:10.1038/s41580-020-0227-y
27. Fiskum V, Sandvig A, Sandvig I. Silencing of activity during hypoxia improves functional outcomes in motor neuron networks in vitro. Front Integr Neurosci. 2021;15:792863. doi:10.3389/fnint.2021.792863
28. Sharma R, Cramer NP, Perry B, et al. Chronic exposure to high altitude: synaptic, astroglial and memory changes. Sci Rep. 2019;9(1):16406. doi:10.1038/s41598-019-52563-1
29. Ge Q, Guo Y, Zheng W, Cai Y, Qi X, Zhao S. A comparative analysis of differentially expressed mRNAs, miRNAs and circRNAs provides insights into the key genes involved in the high-altitude adaptation of yaks. BMC Genomics. 2021;22(1):744. doi:10.1186/s12864-021-08044-9
30. Qiu Q, Zhang G, Ma T, et al. The yak genome and adaptation to life at high altitude. Nat Genet. 2012;44(8):946–949. doi:10.1038/ng.234326
31. Zhou C, Liu Y, Zheng X, et al. Characterization of olfactory receptor repertoires provides insights into the high-altitude adaptation of the yak based on the chromosome-level genome. Int J Biol Macromol. 2022;209(Pt A):220–230. doi:10.1016/j.ijbiomac.2022.03.194
32. Bonfanti R, Musumeci T, Russo C, Pellitteri R. The protective effect of curcumin in olfactory ensheathing cells exposed to hypoxia. Eur J Pharmacol. 2017;796:62–68. doi:10.1016/j.ejphar.2016.11.038
33. Nakayama K, Kataoka N. Regulation of gene expression under hypoxic conditions. Int J Mol Sci. 2019;20(13):3278. doi:10.3390/ijms20133278
34. Cui C, Jiang X, Wang Y, et al. Cerebral hypoxia-induced molecular alterations and their impact on the physiology of neurons and dendritic spines: a comprehensive review. Cell Mol Neurobiol. 2024;44(1):58. doi:10.1007/s10571-024-01491-4
35. Kim BY, Park JY, Bae JH. The effects of the levels of hypoxia in the olfactory nervous system in mouse model. Am J Rhinol Allergy. 2023;37(5):575–585. doi:10.1177/19458924231184332
36. Kim BY, Lee SH, Kim IK, Park JY, Bae JH. Chronic intermittent hypoxia impacts the olfactory nervous system in an age-dependent manner: pilot study. Eur Arch Otorhinolaryngol. 2023;280(1):241–248. doi:10.1007/s00405-022-07529-x
37. Mukandala G, Tynan R, Lanigan S, O’Connor JJ. The effects of hypoxia and inflammation on synaptic signaling in the CNS. Brain Sci. 2016;6(1):6. doi:10.3390/brainsci601000633
38. Yu W, Ye T, Chen Z, et al. Global analysis reveals region-specific air pollution exposure inequalities. One Earth. 2024;7:2063–2071.
39. Aguilera R, Corringham T, Gershunov A, Benmarhnia T. Wildfire smoke impacts respiratory health more than fine particles from other sources: observational evidence from Southern California. Nat Commun. 2021;12(1):1493. doi:10.1038/s41467-021-21708-0
40. Shetty SS, D D, H S, et al. Environmental pollutants and their effects on human health. Heliyon. 2023;9(9):e19496. doi:10.1016/j.heliyon.2023.e19496
41. Wallbanks S, Griffiths B, Thomas M, Price OJ, Sylvester KP. Impact of environmental air pollution on respiratory health and function. Physiol Rep. 2024;12(16):e70006. doi:10.14814/phy2.7000637
42. Alyami MM, Balharith FH, Ravi SK, Reddy RS. Urban air pollution and chronic respiratory diseases in adults: insights from a cross-sectional study. Front Public Health. 2025;13:1507882. doi:10.3389/fpubh.2025.1507882
43. Lian L, Huang J, Chen S, Du S, Zhang L, Yang J. A comprehensive review of dust events: characteristics, climate feedbacks, and public health risks. Curr Poll Rep. 2025;11(18). doi:10.1007/s40726-025-00347-9
44. Thangavel P, Park D, Lee YC. Recent insights into particulate matter (PM2.5)-Mediated toxicity in humans: an overview. Int J Environ Res Public Health. 2022;19(12):7511. doi:10.3390/ijerph19127511
45. Imamura F, Hasegawa-Ishii S. Environmental toxicants-induced immune responses in the olfactory mucosa. Front Immunol. 2016;7:475. doi:10.3389/fimmu.2016.0047541
46. Wellford SA, Moseman EA. Olfactory immunology: the missing piece in airway and CNS defence. Nat Rev Immunol. 2024;24(6):381–398. doi:10.1038/s41577-023-00972-942
47. Taylor AT. High-altitude illnesses: physiology, risk factors, prevention, and treatment. Rambam Maimonides Med J. 2011;2(1):e0022. doi:10.5041/RMMJ.1002243
48. Mazzatenta A, Bondi D, Di Giulio C, Verratti V. Olfactory response to altitude hypoxia: a pilot study during a himalayan trek. Adv Exp Med Biol. 2022;1375:55–61. doi:10.1007/5584_2021_67944
49. Gatterer H, Villafuerte FC, Ulrich S, Bhandari SS, Keyes LE, Burtscher M. Altitude illnesses. Nat Rev Dis Primers. 2024;10(1):43. doi:10.1038/s41572-024-00526-w45
50. Chen YN, Kostka JK. Beyond anosmia: olfactory dysfunction as a common denominator in neurodegenerative and neurodevelopmental disorders. Front Neurosci. 2024;18:1502779. doi:10.3389/fnins.2024.150277946
51. Liu DT, Besser G, Lang M, et al. Odor mixtures in identification testing using sniffin’ sticks: the ssomix test. Sci Rep. 2020;10(1):8155. doi:10.1038/s41598-020-65028-747
52. Jia NN, Yao MF, Zhu CX, et al. Chronic intermittent hypoxia-induced neural injury: pathophysiology, neurodegenerative implications, and therapeutic insights. CNS Neurosci Ther. 2025;31(4):e70384. doi:10.1111/cns.7038448
53. Chand Dakal T, Choudhary K, Tiwari I, Yadav V, Kumar Maurya P, Kumar Sharma N. Unraveling the triad: hypoxia, oxidative stress and inflammation in neurodegenerative disorders. Neuroscience. 2024;552:126–141. doi:10.1016/j.neuroscience.2024.06.02149
54. Hancco I, Bailly S, Baillieul S, et al. Excessive erythrocytosis and chronic mountain sickness in dwellers of the highest city in the world. Front Physiol. 2020;11:773. doi:10.3389/fphys.2020.00773
55. Bothwell AR, Resnick SM, Ferrucci L, Tian Q. Associations of olfactory function with brain structural and functional outcomes. A systematic review. Ageing Res Rev. 2023;92:102095. doi:10.1016/j.arr.2023.102095
56. West JB. Physiological effects of chronic hypoxia. N Engl J Med. 2017;376(20):1965–1971. doi:10.1056/NEJMra161200852
57. Nisar A, Khan S, Li W, et al. Hypoxia and aging: molecular mechanisms, diseases, and therapeutic targets. MedComm. 2024;5(11):e786. doi:10.1002/mco2.78653
58. Zhang Q, Zhang G, Ba P, Wu T, Wang G. Advances in the study of mechanisms underlying olfactory dysfunction in obstructive sleep apnea:a narrative review. Sleep Biol Rhythms. 2025;23(3):263–274. doi:10.1007/s41105-025-00582-z54
59. Maniaci A, Lentini M, Bianco MR, et al. Exploring the relationship between obstructive sleep apnea and olfactory function. Life. 2025;15(4):675. doi:10.3390/life1504067555
60. Shin DH, Ahn SH, Yang Y, et al. The effect of sleep disordered breathing on olfactory functions: analysis by apnea-hypopnea index. Clin Exp Otorhinolaryngol. 2017;10(1):71–76. doi:10.21053/ceo.2015.0143856
61. Wang Y, Teng HL, Gao Y, Zhang F, Ding YQ, Huang ZH. Brain-derived neurotrophic factor promotes the migration of olfactory ensheathing cells through TRPC channels. Glia. 2016;64(12):2154–2165. doi:10.1002/glia.2304957
62. Olsson P, Bende M. Influence of environmental temperature on human nasal mucosa. Ann Otol Rhinol Laryngol. 1985;94(2 Pt 1):153–155. doi:10.1177/00034894850940021158
63. Klos B, Wolf S, Ohla K, et al. Effects of one year of extreme isolation in Antarctica on olfactory and gustatory functions. Sci Rep. 2025;15(1):32369. doi:10.1038/s41598-025-16900-x59
64. Kang W, Son B, Park S, Choi D, Park T. UV-Irradiation- and inflammation-induced skin barrier dysfunction is associated with the expression of olfactory receptor genes in human keratinocytes. Int J Mol Sci. 2021;22(6):2799. doi:10.3390/ijms2206279960
65. Doty RL, Kamath V. The influences of age on olfaction: a review. Front Psychol. 2014;5:20. doi:10.3389/fpsyg.2014.00020
66. Lietzau G, Nyström T, Östenson CG, Darsalia V, Patrone C. Type 2 diabetes-induced neuronal pathology in the piriform cortex of the rat is reversed by the GLP-1 receptor agonist exendin-4. Oncotarget. 2016;7(5):5865–5876. doi:10.18632/oncotarget.682362
67. Trimmer C, Keller A, Murphy NR, et al. Genetic variation across the human olfactory receptor repertoire alters odor perception. Proc Natl Acad Sci U S A. 2019;116(19):9475–9480. doi:10.1073/pnas.180410611563
68. Wang P, Lyman RF, Shabalina SA, Mackay TF, Anholt RR. Association of polymorphisms in odorant-binding protein genes with variation in olfactory response to benzaldehyde in Drosophila. Genetics. 2007;177(3):1655–1665. doi:10.1534/genetics.107.079731
69. Jimenez RC, Casajuana-Martin N, García-Recio A, et al. The mutational landscape of human olfactory G protein-coupled receptors. BMC Biol. 2021;19(1):21. doi:10.1186/s12915-021-00962-0
70. Sollai G, Melis M, Magri S, et al. Association between the rs2590498 polymorphism of Odorant Binding Protein (OBPIIa) gene and olfactory performance in healthy subjects. Behav Brain Res. 2019;372:112030. doi:10.1016/j.bbr.2019.11203066
71. Håglin S, Berghard A, Bohm S. Increased retinoic acid catabolism in olfactory sensory neurons activates dormant tissue-specific stem cells and accelerates age-related metaplasia. J Neurosci. 2020;40(21):4116–4129. doi:10.1523/JNEUROSCI.2468-19.202067
72. Julian CG, Moore LG. Human genetic adaptation to high altitude: evidence from the andes. Genes. 2019;10(2):150. doi:10.3390/genes1002015068
73. Sharma V, Varshney R, Sethy NK. Human adaptation to high altitude: a review of convergence between genomic and proteomic signatures. Hum Genomics. 2022;16(1):21. doi:10.1186/s40246-022-00395-y69
74. Storz JF. High-Altitude adaptation: mechanistic insights from integrated genomics and physiology. Mol Biol Evol. 2021;38(7):2677–2691. doi:10.1093/molbev/msab06470
75. Peng YJ, Nanduri J, Wang N, et al. Hypoxia sensing requires H2S-dependent persulfidation of olfactory receptor 78. Sci Adv. 2023;9(27):eadf3026. doi:10.1126/sciadv.adf302671
76. Chang AJ, Ortega FE, Riegler J, Madison DV, Krasnow MA. Oxygen regulation of breathing through an olfactory receptor activated by lactate. Nature. 2015;527(7577):240–244. doi:10.1038/nature1572172
77. Naz S, Chatha AMM, Ullah Q, et al. Genomic adaptation, environmental challenges, and sustainable yak husbandry in high-altitude pastoral systems. Vet Sci. 2025;12(8):714. doi:10.3390/vetsci1208071473
78. Mahar K, Gurao A, Kumar A, et al. Genomic insights into high-altitude adaptation and evolutionary dynamics of Indian yaks in the Trans-Himalayan region. Conserv Gene. 2025;26:49–62. doi:10.1007/s10592-024-01650-6
79. Shi J, Jia Z, Sun J, et al. Structural variants involved in high-altitude adaptation detected using single-molecule long-read sequencing. Nat Commun. 2023;14(1):8282. doi:10.1038/s41467-023-44034-z76
80. Kern DW, Schumm LP, Wroblewski KE, Pinto JM, Hummel T, McClintock MK. Olfactory thresholds of the U.S. Population of home-dwelling older adults: development and validation of a short, reliable measure. PLoS One. 2015;10(3):e0118589. doi:10.1371/journal.pone.011858977
81. Hummel T, Sekinger B, Wolf SR, Pauli E, Kobal G. ‘Sniffin’ sticks’: olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory threshold. Chem Senses. 1997;22(1):39–52. doi:10.1093/chemse/22.1.3978
82. Wang C, Zhang L, Liu Z, et al. Effects of long-term very high-altitude exposure on cardiopulmonary function of healthy adults in plain areas. Sci Rep. 2025;15(1):24826. doi:10.1038/s41598-025-07474-9
83. Robb KA. The integrated screening action model (I-SAM): a theory-based approach to inform intervention development. Prev Med Rep. 2021;23:101427. doi:10.1016/j.pmedr.2021.101427
84. Marchis EH, Aceves BA, Brown EM, Loomba V, Molina MF, Gottlieb LM. Assessing implementation of social screening within US health care settings: a systematic scoping review. J Am Board Fam Med. 2023;36(4):626–649. doi:10.3122/jabfm.2022.220401R182
85. Soler ZM, Gregoski MJ, Kohli P, LaPointe KA, Schlosser RJ. Development and validation of the four-item concise aging adults smell test to screen for olfactory dysfunction in older adults. Int Forum Allergy Rhinol. 2025;15(3):250–257. doi:10.1002/alr.23476
86. Whitcroft KL, Hummel T. Clinical diagnosis and current management strategies for olfactory dysfunction: a review. JAMA Otolaryngol Head Neck Surg. 2019;145(9):846–853. doi:10.1001/jamaoto.2019.172884
87. Tae WS, Ham BJ, Pyun SB, Kim BJ. Current clinical applications of structural MRI in neurological disorders. J Clin Neurol. 2025;21(4):277–293. doi:10.3988/jcn.2025.018585
88. Dintica CS, Marseglia A, Rizzuto D, et al. Impaired olfaction is associated with cognitive decline and neurodegeneration in the brain. Neurology. 2019;92(7):e700–e709. doi:10.1212/WNL.0000000000006919
89. Finn ES, Poldrack RA, Shine JM. Functional neuroimaging as a catalyst for integrated neuroscience. Nature. 2023;623(7986):263–273. doi:10.1038/s41586-023-06670-9
90. Zhang H, Ji D, Yin J, et al. Olfactory fMRI activation pattern across different concentrations changes in Alzheimer’s disease. Front Neurosci. 2019;13:786. doi:10.3389/fnins.2019.00786
91. Ávila-Villanueva M, Marcos Dolado A, Gómez-Ramírez J, Fernández-Blázquez M. Brain structural and functional changes in cognitive impairment due to Alzheimer’s disease. Front Psychol. 2022;13:886619. doi:10.3389/fpsyg.2022.88661989
92. Vasavada MM, Wang J, Eslinger PJ, et al. Olfactory cortex degeneration in Alzheimer’s disease and mild cognitive impairment. J Alzheimers Dis. 2015;45(3):947–958. doi:10.3233/JAD-14194790
93. Liu Y, Zhang S, He B, et al. Periphery biomarkers for objective diagnosis of cognitive decline in type 2 diabetes patients. Front Cell Dev Biol. 2021;9:752753. doi:10.3389/fcell.2021.75275391
94. Viruez-Soto A, Arias S, Casas-Mamani R, et al. Oxygen therapy limiting peripheral oxygen saturation to 89-93% is associated with a better survival prognosis for critically ill COVID-19 patients at high altitudes. Respir Physiol Neurobiol. 2022;299:103868. doi:10.1016/j.resp.2022.10386892
95. Mehta V, Vasu TS, Phillips B, Chung F. Obstructive sleep apnea and oxygen therapy: a systematic review of the literature and meta-analysis. J Clin Sleep Med. 2013;9(3):271–279. doi:10.5664/jcsm.250093
96. Pecoraro L, Di Muri E, Lezzi G, et al. Nasal irrigations: a 360-Degree view in clinical practice. Medicina. 2025;61(8):1402. doi:10.3390/medicina6108140294
97. Bastier PL, Lechot A, Bordenave L, Durand M, de Gabory L. Nasal irrigation: from empiricism to evidence-based medicine. A review. Eur Ann Otorhinolaryngol Head Neck Dis. 2015;132(5):281–285. doi:10.1016/j.anorl.2015.08.00195
98. Pekdemir B, Raposo A, Saraiva A, et al. Mechanisms and potential benefits of neuroprotective agents in neurological health. Nutrients. 2024;16(24):4368. doi:10.3390/nu1624436896
99. Jalouli M, Rahman MA, Biswas P, et al. Targeting natural antioxidant polyphenols to protect neuroinflammation and neurodegenerative diseases: a comprehensive review. Front Pharmacol. 2025;16:1492517. doi:10.3389/fphar.2025.149251797
100. Bathina S, Das UN. Brain-derived neurotrophic factor and its clinical implications. Arch Med Sci. 2015;11(6):1164–1178. doi:10.5114/aoms.2015.5634298
101. Pisani A, Paciello F, Del Vecchio V, et al. The role of BDNF as a biomarker in cognitive and sensory neurodegeneration. J Pers Med. 2023;13(4):652. doi:10.3390/jpm13040652
102. Vance DE, Del Bene VA, Kamath V, et al. Does olfactory training improve brain function and cognition? A systematic review. Neuropsychol Rev. 2024;34(1):155–191. doi:10.1007/s11065-022-09573-0
103. Delgado-Lima AH, Bouhaben J, Delgado-Losada ML. The efficacy of olfactory training in improving olfactory function: a meta-analysis. Eur Arch Otorhinolaryngol. 2024;281(10):5267–5284. doi:10.1007/s00405-024-08733-7101
104. Pekala K, Chandra RK, Turner JH. Efficacy of olfactory training in patients with olfactory loss: a systematic review and meta-analysis. Int Forum Allergy Rhinol. 2016;6(3):299–307. doi:10.1002/alr.21669102
105. Lechien JR, Vaira LA, Saussez S. Effectiveness of olfactory training in COVID-19 patients with olfactory dysfunction: a prospective study. Eur Arch Otorhinolaryngol. 2023;280(3):1255–1263. doi:10.1007/s00405-022-07665-4103
106. Boesveldt S, Parma V. The importance of the olfactory system in human well-being, through nutrition and social behavior. Cell Tissue Res. 2021;383(1):559–567. doi:10.1007/s00441-020-03367-7104
107. Fjaeldstad AW, Smith B. The effects of olfactory loss and parosmia on food and cooking habits, sensory awareness, and quality of Life-A possible avenue for regaining enjoyment of food. Foods. 2022;11(12):1686. doi:10.3390/foods11121686107
108. Troesch B, Biesalski HK, Bos R, et al. Increased intake of foods with high nutrient density can help to break the intergenerational cycle of malnutrition and obesity. Nutrients. 2015;7(7):6016–6037. doi:10.3390/nu7075266108
109. Van Regemorter V, Hummel T, Rosenzweig F, Mouraux A, Rombaux P, Huart C. Mechanisms linking olfactory impairment and risk of mortality. Front Neurosci. 2020;14:140. doi:10.3389/fnins.2020.00140109
110. Yuan ZQ, Peng XC, Liu L, Yang FY, Qian F. Olfactory receptors and human diseases. Cell Tissue Res. 2025;401(1):1–14. doi:10.1007/s00441-025-03971-5110
111. Schäfer L, Schriever VA, Croy I. Human olfactory dysfunction: causes and consequences. Cell Tissue Res. 2021;383(1):569–579. doi:10.1007/s00441-020-03381-9111
112. Wang Y, Lü Y, Lü D, Yin L, Wang X. Climate change and its ecological risks are spatially heterogeneous in high-altitude region: the case of Qinghai-Tibet plateau. CATENA. 2024;243:108140.
113. Zhang KL, Leng YN, Hao RR, et al. Adaptation of high-altitude plants to harsh environments: application of phenotypic-variation-related methods and multi-omics techniques. Int J Mol Sci. 2024;25(23):12666. doi:10.3390/ijms252312666
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.