Back to Journals » Journal of Pain Research » Volume 15
Off-Label Magnetic Resonance Imaging (MRI) in Patients with Persistent Pain with Spinal Cord Stimulators: A Case Series
Authors Ragukonis T ![]()
Received 25 January 2022
Accepted for publication 19 August 2022
Published 22 November 2022 Volume 2022:15 Pages 3625—3638
DOI https://doi.org/10.2147/JPR.S357416
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Dawood Sayed
Thomas Ragukonis
Bergen Pain Management, Paramus, NJ, USA
Correspondence: Thomas Ragukonis, Email [email protected]
Objective: Advances in spinal cord stimulator (SCS) technology and increasing prevalence of magnetic resonance imaging (MRI) diagnostic testing require empirical evidence describing the presence of MRI-related SCS adverse events related to off-label use of imaging. MRI safety recommendations vary based on the type of stimulator used with scant availability regarding adverse events associated with off-label MRI use. The aim of this case series is to describe the type and frequency of adverse events associated with off-label MRI use in patients with implanted SCSs.
Materials and Methods: Convenient samples of records of patients who had SCS and subsequently underwent MRI were included. Descriptive data including patient demographics, stimulator information, and frequency of adverse events were described.
Results: Sixty-nine individuals with implanted SCSs were included. The total number of scans was 78. Sixty-two percent of the sample was female. Over 92% of the MRI scans were considered off-label and the overall adverse event rate for off-label use was 9.72%. No serious adverse events were reported. Seven clinical adverse events were reported, all of which were related to the spinal cord stimulation and resolved.
Conclusion: This case series demonstrates that individuals implanted with SCSs experienced no serious adverse events associated with off-label MRI use. While these results represent a convenient sample, they provide important preliminary information about using MRI when medically necessary for patients with older spinal cord stimulator models. Specifically, these data demonstrate that the rate of observed adverse events related to MRI was low and suggest that the benefits of acquiring these images for pain management may outweigh the risks of not acquiring MRI for appropriate pain management.
Keywords: spinal cord stimulation, chronic pain, magnetic resonance imaging
Introduction
Spinal cord stimulators (SCS) are implantable devices used to manage intractable and persistent pain and involve low-voltage current intended to block nociceptive input.1 Spinal cord stimulators have been shown to be safe and effective for persistent pain conditions, including spinal pain and complex regional pain syndrome.2–6
Safety concerns exist for patients with implanted SCSs and the use of magnetic resonance imaging (MRI) due to the magnetic field interfering with the device and its functionality. For example, one concern is that the magnetic field may alter the position of the device and/or accelerate the device into the bore of the magnet, causing severe damage to patient tissue. Also, the radiofrequency current may lead to heating of SCS, resulting in thermal and/or electrical burns to the patient and potential device malfunction. Another concern is that the presence of the device may affect the quality of the image(s) depending on the location of the image relative to the device. If the goal of the MRI is to evaluate areas in which to potentially intervene, image quality is of obvious importance.7,8 Although individual studies have reported safety outcomes, no consensus guidelines exist on how to safely perform imaging of patients with various implanted SCS. Rather, manufacturers provide device-specific guidelines, but these guidelines vary on whether or not MRI is contraindicated, and which parts of the body are considered safe to image. For example, some devices have been developed to allow for full body scans while others allow only for head scans. In some devices, MRI may be an absolute contraindication and in others, safety has yet to be determined. De Andres et al9 described the frequency and type of adverse events associated with a single manufacturer and reported that in 31 patients with SCSs who underwent MRI, seven reported events ranging from feeling stimulation during the MRI and increased thermal sensations at the lead sites. Others have reported on SCS-related adverse events but not necessarily related to MRI.10
On-label versus off-label MRI in patients with SCSs is a related concern and one that has not been widely explored. Patients post-laminectomy syndrome or with failed back surgery syndrome (FBSS) are the most common historical indication for SCS therapy and are among those that may require repeat imaging.11,12 Prior to 2012, all spinal cord stimulation systems were not considered “on label” for MRI use. Spinal cord stimulator models, including Precision, Protégé, and Eon Mini systems, were excluded for MRI. In 2012, the Medtronic system gained MRI conditionality. As newer generation implantable pulse generators (IPGs) have gained MRI conditionality, some of these are specific only for head or extremities. Others require specifications inherent to the leads, such as normalized impedance values or placement within a particular anatomical region, T7-T12.
Given the limited information available regarding MRI conditionality in patients with SCS, the purpose of this case series is to describe the frequency and type of long-term adverse events associated with off-label MRI use in patients with SCSs.
Methods
This case series included a convenience sample of patient records from an outpatient interventional pain clinic. The records represent with a permanent SCS who subsequently underwent MRI. The frequency and type of long-term adverse events reported by patients were evaluated following MRI. This study involved a retrospective review of patient records and thus a waiver of informed consent was obtained and the study was approved by the Advarra Institutional Review Board; the data accessed complied with relevant data protection and privacy regulations. The primary outcomes of interest were the frequency and type of adverse events following MRI. Adverse events were coded as serious or clinical, SCS or MRI-related, and as mild, moderate, or severe. Demographic information, duration of clinical symptoms, manufacturer and model type of SCS, on- versus off- label MRI use, and adverse event frequency were described. All data were analyzed in Microsoft Excel.
Results
Sixty-nine patient records were included in this study and Table 1 includes demographic information about the sample. Of these 69 records, 7 included more than one MRI, thus the total scan count for this sample was 78. Forty-two (62%) were female and the average age of the sample was 60.5 years. The duration of pain symptoms ranged from 5 to 47 years, with an average of 12 years. The primary medical diagnoses included failed back surgery syndrome (FBSS), failed neck surgery syndrome (FNSS), and chronic regional pain syndrome. The primary rationale to opt for off-label MRI versus other imaging methods is that MRI in this sample was the best available option to visualize the spinal cord and nerves; MRI may show spinal abnormalities, injuries, and disease that may not be seen with other methods.
 |
Table 1 Demographic Information |
The duration from implant to MRI and duration from MRI to long-term follow-up are in Table 2. The time from permanent generator implant to MRI ranged from less than 1 month to 87 months (mean 19.4 months, standard deviation 17.7 months). The time from MRI to long-term follow-up ranged from 2 months to 17 months (mean 10.4 months, standard deviation 3.2 months). All patients underwent MRI in a 1.5 Tesla scanner (Siemens Medical Solutions USA, Inc, Malvern, PA).
 |
Table 2 MRI and Follow-Up Information |
The manufacturers and IPG models are listed in Table 3. Based on the IPG model, lead types, locations, and configurations, the overwhelming majority of patients in this sample (94.1%) underwent off-label MRI use. The frequency of adverse events for patients who underwent off-label MRI use was 10.9%. The most common reported as undesirable changes in stimulation (4/7), followed by persistent pain or numbness (2/7), and radicular chest wall or abdominal stimulation (1/7). All seven events were considered non-serious and all were resolved. For all adverse events, a representative from the company was called for troubleshooting and resolved with re-programming. If adequate stimulation could not be achieved, patients were sent for additional imaging to examine the leads and IPG under fluoroscopy. After testing the functionality of equipment, devices were re-programmed until optimal results were achieved.
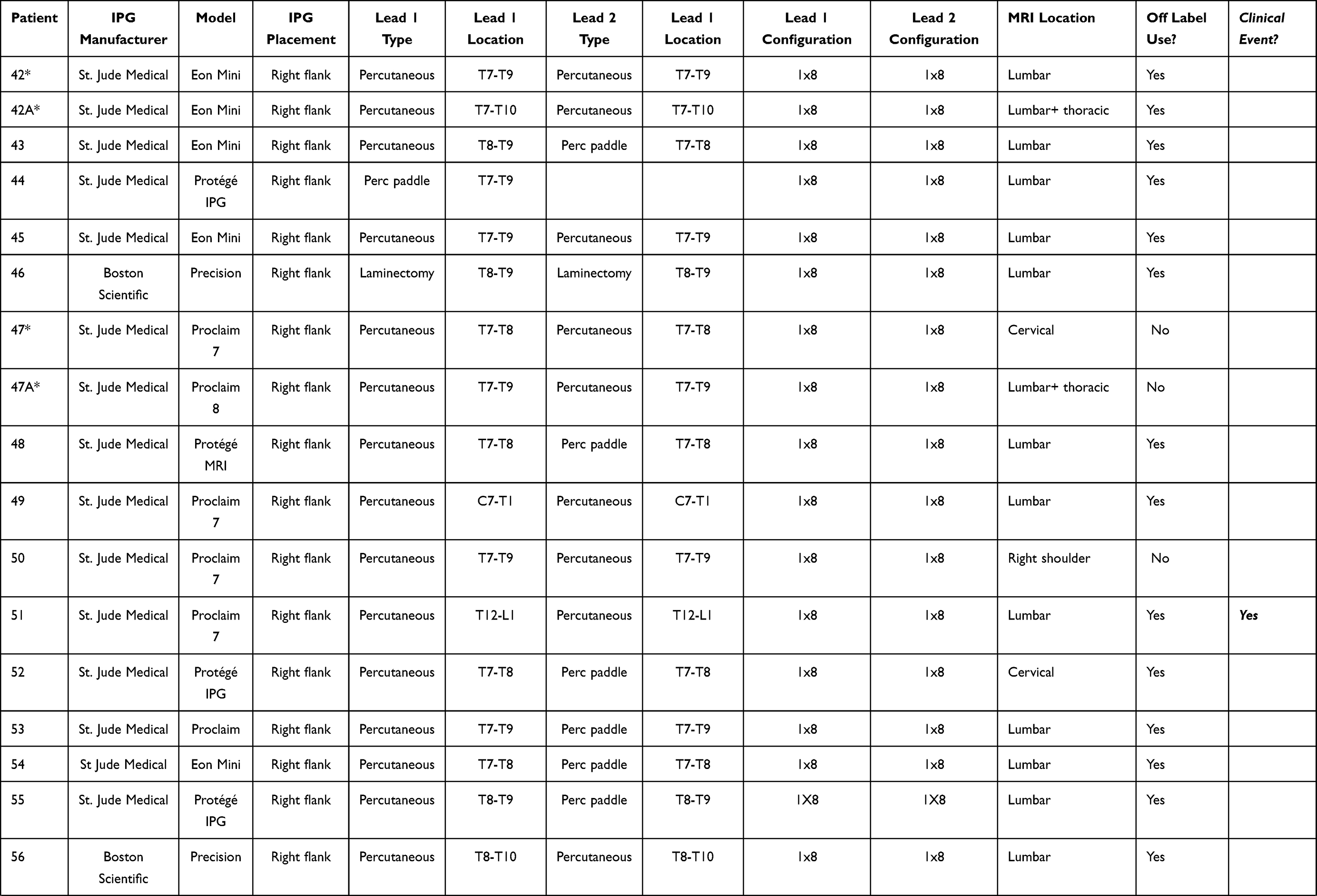 |
Table 3 Spinal Cord Stimulator Information |
Discussion
This case series indicates that off-label MRI use did not result in long-term serious adverse events. While these represent pilot data, this work is notable and relevant to clinical management of chronic pain for several reasons. These data add to existing work in this area regarding MRI safety in patients with SCS and have potentially important implications for both diagnostic radiology and interventional pain medicine. A recent case report from Dr Andres et al7 reported on the within-session adverse events associated with full-body MRI immediately following SCS implant. The patient in that case reported no serious or clinical events during the MRI. Second, the current case series expands on previous publications by examining off-label imaging and the frequency of long-term serious and clinical adverse events associated with this imaging. Previous recommendations for MRI in patients with SCS suggested that physicians should carefully select patients for MRI based on their potential to experience adverse events, including movement of the device, risk of thermal injury or burning, and alteration of the neurostimulation program.13 A small percentage of individuals from the current study experienced mild to moderate clinical events; however, all of the clinical events were related to the device rather than the MRI and the frequency rate of adverse events was similar to published trials of SCS long-term safety.14
Given the low rate of adverse events when MRI was used in an off-label manner, these results suggest that the benefits of obtaining MRI for the purposes of identifying structure(s) that may be contributing to a patient’s pain may outweigh the risks of not obtaining imaging in patients who have older SCS units. Future work may expand on the current study by exploring differences in adverse events in patients with on-label versus off-label MRI use. Although the vast majority of patients in the current study underwent off-label MRI, it is unclear if the frequency of adverse events may be different compared to individuals undergoing on-label MRI. These data would provide further information to aid clinical decision-making for diagnostic imaging in patients with persistent pain. Last, and as others have recommended,15,16 consensus guidelines for the use of MRI for patients with SCS should be developed and evaluated beyond individual manufacturer’s recommendations to provide in-depth information related to the safety parameters and utility of MRI in patients with chronic pain conditions.
Limitations
The current study included a convenience sample of patient records. Records were not included if follow-up data was not available (eg, the patient did not return to the clinic) or if demographic or other clinical information was not available in the patient record. The clinic from which these data were collected did not systematically assess (ie, at a specific time frame or manner) the presence of adverse events; thus, it is possible that the frequency of adverse events could be higher or lower based on the systematic evaluation of adverse events. Last, our follow-up time was relatively short at an average of 10.4 months. While we expect that adverse events associated with MRI would occur in the short-term (ie during the scan or shortly thereafter), it is possible that the MRI was associated with longer term effects that our follow-up period did not adequately capture.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971–979. doi:10.1126/science.150.3699.971
2. Deer TR, Krames E, Mekhail N, et al. The appropriate use of neurostimulation: new and evolving neurostimulation therapies and applicable treatment for chronic pain and selected disease states. Neuromodulation appropriateness consensus committee. Neuromodulation. 2014;17(6):599–615; discussion 615. doi:10.1111/ner.12204
3. Deer TR, Grider JS, Lamer TJ, et al. A systematic literature review of spine neurostimulation therapies for the treatment of pain. Pain Med. 2020;21(7):1421–1432.
4. Maheshwari A, Pope JE, Deer TR, Falowski S. Advanced methods of spinal stimulation in the treatment of chronic pain: pulse trains, waveforms, frequencies, targets, and feedback loops. Expert Rev Med Devices. 2019;16(2):95–106. doi:10.1080/17434440.2019.1567325
5. Hunter CW, Carlson J, Yang A, Deer T. Spinal cord stimulation for the treatment of failed neck surgery syndrome: outcome of a prospective case series. Neuromodulation. 2018;21(5):495–503. doi:10.1111/ner.12769
6. Lad SP, Babu R, Bagley JH, et al. Utilization of spinal cord stimulation in patients with failed back surgery syndrome. Spine. 2014;39(12):E719–727. doi:10.1097/BRS.0000000000000320
7. De Andres J, Martinez-Sanjuan V, Fabregat-Cid G, Asensio-Samper JM, Sanchis-Lopez N, Villanueva-Perez V. MRI-compatible spinal cord stimulator device and related changes in patient safety and imaging artifacts. Pain Med. 2014;15(10):1815–1819. doi:10.1111/pme.12522
8. Manfield J, Bartlett R, Safety PN. Utility of spinal magnetic resonance imaging in patients with high-frequency spinal cord stimulators: a prospective single-centre study. Stereotact Funct Neurosurg. 2019;97(4):272–277. doi:10.1159/000503730
9. De Andres J, Valia JC, Cerda-Olmedo G, et al. Magnetic resonance imaging in patients with spinal neurostimulation systems. Anesthesiology. 2007;106(4):779–786. doi:10.1097/01.anes.0000264776.17533.06
10. Kapural L, Gupta M, Paicius R, et al. Treatment of chronic abdominal pain with 10-kHz spinal cord stimulation: safety and efficacy results from a 12-month prospective, multicenter, feasibility study. Clin Transl Gastroenterol. 2020;11(2):e00133. doi:10.14309/ctg.0000000000000133
11. Amirdelfan K, Webster L, Poree L, Sukul V, McRoberts P. Treatment options for failed back surgery syndrome patients with refractory chronic pain: an evidence based approach. Spine. 2017;42(Suppl 14):S41–S52. doi:10.1097/BRS.0000000000002217
12. Sitzman BT, Provenzano DA. Best practices in spinal cord stimulation. Spine. 2017;42(Suppl 14):S67–S71. doi:10.1097/BRS.0000000000002220
13. Liem LA, van Dongen VC. Magnetic resonance imaging and spinal cord stimulation systems. Pain. 1997;70(1):95–97. doi:10.1016/S0304-3959(96)03298-8
14. Mekhail N, Levy RM, Deer TR, et al. Long-term safety and efficacy of closed-loop spinal cord stimulation to treat chronic back and leg pain (Evoke): a double-blind, randomised, controlled trial. Lancet Neurol. 2020;19(2):123–134. doi:10.1016/S1474-4422(19)30414-4
15. Ghaly RF, Tverdohleb T, Candido KD, Knezevic NN. Do we need to establish guidelines for patients with neuromodulation implantable devices, including spinal cord stimulators undergoing nonspinal surgeries? Surg Neurol Int. 2016;7:18. doi:10.4103/2152-7806.176373
16. Harned ME, Gish B, Zuelzer A, Grider JS. Anesthetic considerations and perioperative management of spinal cord stimulators: literature review and initial recommendations. Pain Physician. 2017;20(4):319–329. doi:10.36076/ppj.2017.329
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.