")
Back to Journals » Clinical Ophthalmology » Volume 16
Ocular Manifestations of Buerger’s Disease – A Review of Current Knowledge
Authors Szydełko-Paśko U , Przeździecka-Dołyk J , Małecki R, Szuba A , Misiuk-Hojło M
Received 5 December 2021
Accepted for publication 28 January 2022
Published 18 March 2022 Volume 2022:16 Pages 851—860
DOI https://doi.org/10.2147/OPTH.S352608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Urszula Szydełko-Paśko,1 Joanna Przeździecka-Dołyk,1,2 Rafał Małecki,3 Andrzej Szuba,3 Marta Misiuk-Hojło1
1Department of Ophthalmology, Wroclaw Medical University, Wrocław, Poland; 2Department of Optics and Photonics, Wroclaw University of Science and Technology, Wrocław, Poland; 3Department of Angiology, Systemic Hypertension and Diabetology, Wroclaw Medical University, Wrocław, Poland
Correspondence: Urszula Szydełko-Paśko, Department of Ophthalmology, Wroclaw Medical University, Borowska 213, Wrocław, 50-556, Poland, Tel +48 71 736 43 00, Email [email protected]
Abstract: Buerger’s disease, also known as thromboangiitis obliterans, is a disorder of primarily small and medium arteries and veins of the arms and legs. We have failed to find a comprehensive review discussing a possible link between the disease and the eyes. The aim of this study is to review current knowledge on the topic of ocular manifestations in the course of Buerger’s disease. The Medline and Web of Science databases were searched without a time or language limit. We have managed to review 13 articles, describing the involvement of the eyes in thromboangiitis obliterans. It appears that patients suffering from Buerger’s disease may develop non-arteritic anterior ischemic optic neuropathy (NAION), occlusive retinal vasculitis and periphlebitis, papillophlebitis, central retinal artery occlusion (CRAO), branch retinal artery occlusion (BRAO), normal tension glaucoma (NTG), uveitis, chorioretinal atrophy, retinitis, papillitis, optic atrophy, changes typical for hypertensive retinopathy. Additionally the abnormalities in electroretinography might be present. The treatment options and the possible outcome depend on the type of ocular manifestations, so it seems impossible to propose a universal therapy. We would like to raise awareness of the possible ocular manifestations in the course of Buerger’s disease.
Keywords: Buerger’s disease, anterior ischemic optic neuropathy, central retinal artery occlusion, normal tension glaucoma, uveitis
Introduction
The involvement of the eye in the course of systemic diseases has been the topic of extensive research. In some disorders ocular manifestations have been found to be one of the first signs and symptoms. In others, however, they develop as complications secondary to the initial health problem. The connection between the eye and diseases such as diabetes mellitus, hypertension, sarcoidosis or multiple sclerosis has been studied for many years. In recent years some interesting links between rare diseases and ocular findings have been observed. Kreuzpointner et al described ophthalmological complications of Lemierre syndrome.1 The ocular involvement and the role of optical coherence tomography in Fabry disease was studied by Wiest et al.2 Multimodal imaging was shown by Böni et al to be effective in disclosing choroidal lesions in patients with disseminated Mycobacterium chimaera infection.3 Carneval et al demonstrated how useful optical coherence tomography angiography was in revealing ocular vascular changes in patients with systemic sclerosis.4 Even though extensive research has been conducted in the field of systemic diseases and their impact on the eye, we have failed to find a review discussing a possible link between Buerger’s disease and some ocular findings.
Buerger’s disease, also known as thromboangiitis obliterans, is a disease of primarily small and medium arteries and veins of the arms and legs.5 It was first reported by an Austrian physician Felix von Winiwarter in 1879, however, it was named after an Austrian American physician Leo Buerger, whose description of the pathological basis was very accurate (1908).6,7 The highest prevalence of the disease is in the Middle and Far East. It constitutes 45% to 63% of all patients with peripheral arterial disease in India as opposed to Western Europe, where it accounts for 0.5 to 5.6%.5 The annual incidence in the United States is equal to 12.6 per 100,000.8 The disease usually affects tobacco smoking men under 45 years of age. The ratio of men to women suffering from thromboangiitis obliterans equals 10:1 respectively.9 Smoking tobacco has been proven to be one of the main risk factors. However, it was discovered that the disease might also affect smokeless tobacco users (eg tobacco chewers).9 Another risk factor is chronic gum disease, although the reasons for it are still unknown.10 When left untreated, Buerger’s disease may lead to the development of gangrene because of insufficient blood supply. The most important form of prevention is quitting smoking.10
The symptoms of Buerger’s disease are caused by stenosis and occlusion of small blood vessels, which leads to ischemia typically of the upper and lower extremities.8 The patients suffer from intermittent claudication of the upper and lower extremities, rest pain, ulcers and gangrene, Raynaud’s phenomenon, change of skin colour, tingling and numbness of fingers and toes. Although the typical signs and symptoms connected with the extremities are well known, other manifestations of the disease seem understated. Fakour and Fazeli conducted a systematic review, in which they presented 78 case reports, 2 case series and 3 original papers concerning the involvement of the following organs in patients with thromboangiitis obliterans: the gastrointestinal tract, the heart, the central nervous system, the eye, the kidneys, the urogenital system, the mucocutaneous zones, the joints, the lymphohematopoietic system and the ear.11 In some patients the involvement of other organs had been noted long before the diagnosis of thromboangiitis obliterans whereas in others the first signs and symptoms later linked to Buerger’s disease began after the diagnosis. The results of Fakour and Fazeli’s study seem to be consistent with the findings of Leo Burger, who observed visceral arterial involvement in the patients with thromboangiitis obliterans he had examined.11 According to Fakour and Fazeli, neglecting a possible systemic character of the disease might be unfavourable for the patients. Olin et al also stated that some larger blood vessels (eg cerebral, coronary, pulmonary, mesenteric, renal) might be affected by the disease.12 Cabezas-Moya and Dragstedt described intestinal involvement of thromboangiitis obliterans in a patient, and Harten et al observed cerebral, splenic, pulmonary and myocardial signs of the disease.13,14
What also seems noteworthy is the involvement of the eye in other types of vasculitis. The prevalence of ocular symptoms is significant in granulomatosis with polyangiitis (50%), Behçet’s disease (60%-80) and giant cell arteritis (12%-70%).15–17 One third of patients with systemic lupus erythematosus develop ocular signs and symptoms, too.18 This made us raise the question whether thromboangiitis obliterans is localized vasculopathy or a systemic disorder like the diseases mentioned above.
The aim of this study was to review current knowledge on the topic of ocular manifestations in Buerger’s disease and raise awareness on the possible systemic character of the disease.
Materials and Methods
The search strategy consisted in searching the Medline and Web of Science databases without a time or language limit by entering the following key words or phrases: “Buerger’s disease”, “thromboangiitis obliterans” in conjunction with “ocular”, “ocular manifestations”, “eye” and “ophthalmology”. The last search was conducted on the 28th of May 2021. The inclusion criterion regarding Buerger’s disease we adopted was the diagnosis of the condition provided by the authors of the reviewed articles. The inclusion criterion for the ophthalmological involvement was any type of ocular manifestation with no restrictions. Buerger’s disease is known as a very rare disorder. Ophthalmological complications in its course are even rarer. We were keen on reviewing any type of article. The exclusion criterion was when there was no reference to the eye involvement in the course of Buerger’s disease. The references of the reviewed articles were also screened so as not to omit any eligible papers. The search was conducted independently by two authors (USzP and JPD). The total number of records identified from both databases equaled 142. After removing duplicates with the use of Zotero we considered 42 articles. After reading abstracts or full texts 29 articles were excluded from the study as not relevant to the topic. The final number of articles, on which our study is based equals 13. We reviewed 10 cases of ophthalmological manifestations of Buerger’s disease (each case was a separate publication) and 3 studies describing the involvement of the eye in Buerger’s disease in 43 patients (Homma et al. – 9 patients, Arslan et al. – 24 patients, Valdes et al. – 10 patients.19–21
The form of the presentation was mainly inspired by Fakour and Fazeli’s article entitled “Visceral bed involvement in thromboangiitis obliterans: a systemic review”.11 However, we decided to resign from some features included in the original work and replace them with what we believed to be more relevant to the topic. In the systematic review the tables included more categories connected to internal medicine, whereas we wanted our article to be mostly about the ophthalmological aspects. We decided not to write about the duration of Buerger’s disease and the smoking status. Instead, we wanted to describe in detail all the performed imaging tests and ophthalmological findings. We also included some information on the course of Buerger’s disease in each case.
Results
We present 9 articles in the form of a table summing up the findings (Table 1). The other 4 publications will be discussed in a narrative form. We would have liked to include all the information coming from our research in one table Yet, not from all the analyzed works could we obtain enough information to fill in the appropriate categories in the table For example for Copeto and Adamczyk or Homma et al only abstracts were available.19,22 Arslan et al’s. work or Valdes et al’s. paper, on the other hand, are not case reports.20,21 The structure of these studies is different, which means that they are incomparable to the case reports presented in the table To avoid numerous empty slots in the table, we decided to discuss all the incomplete data separately.
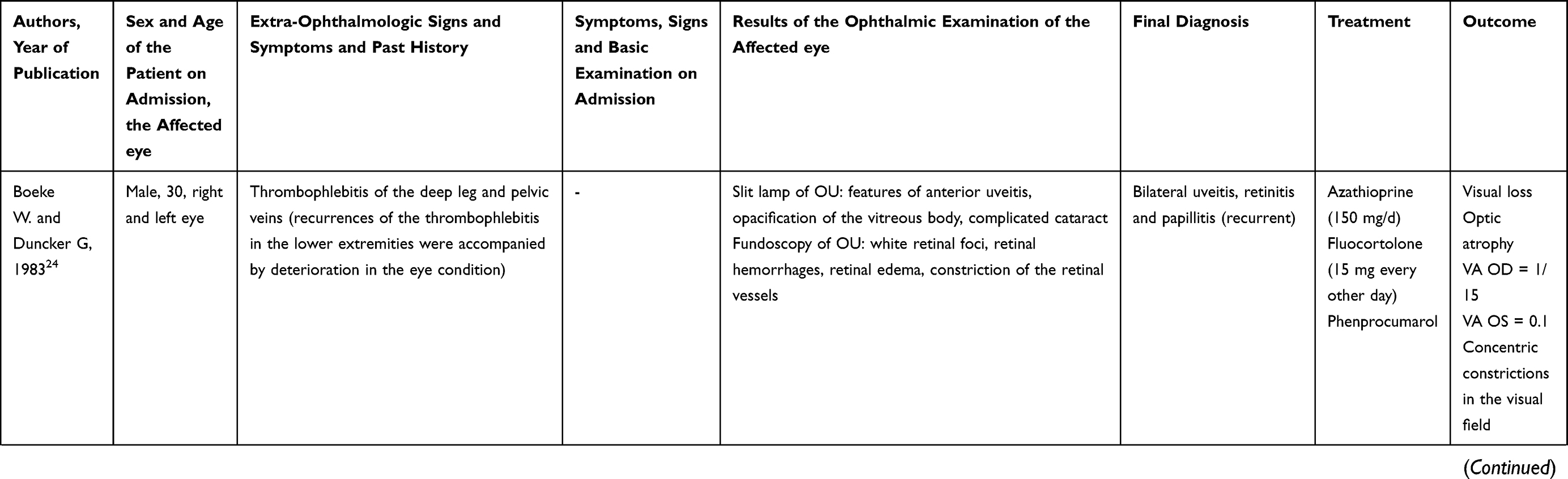 | 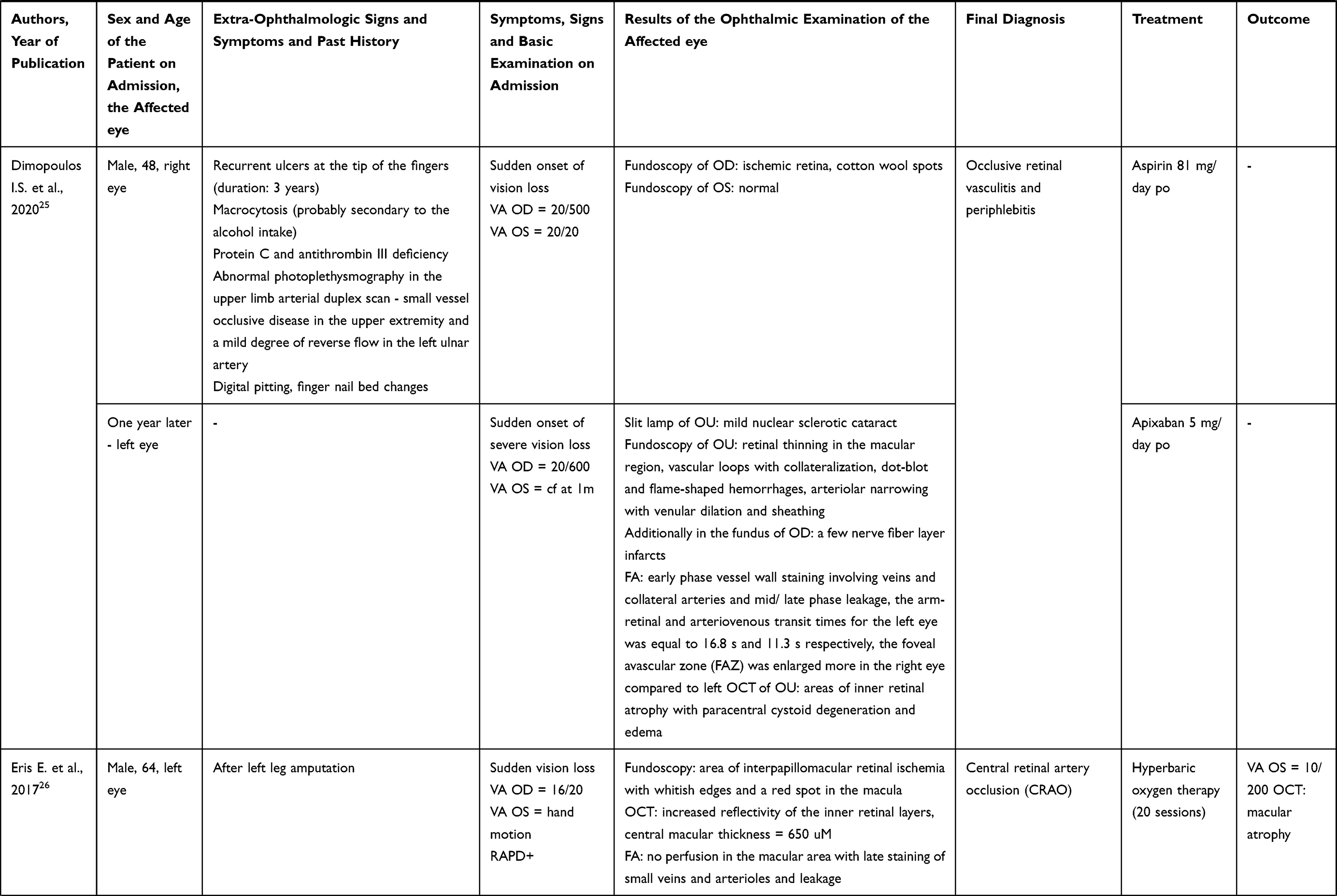 | 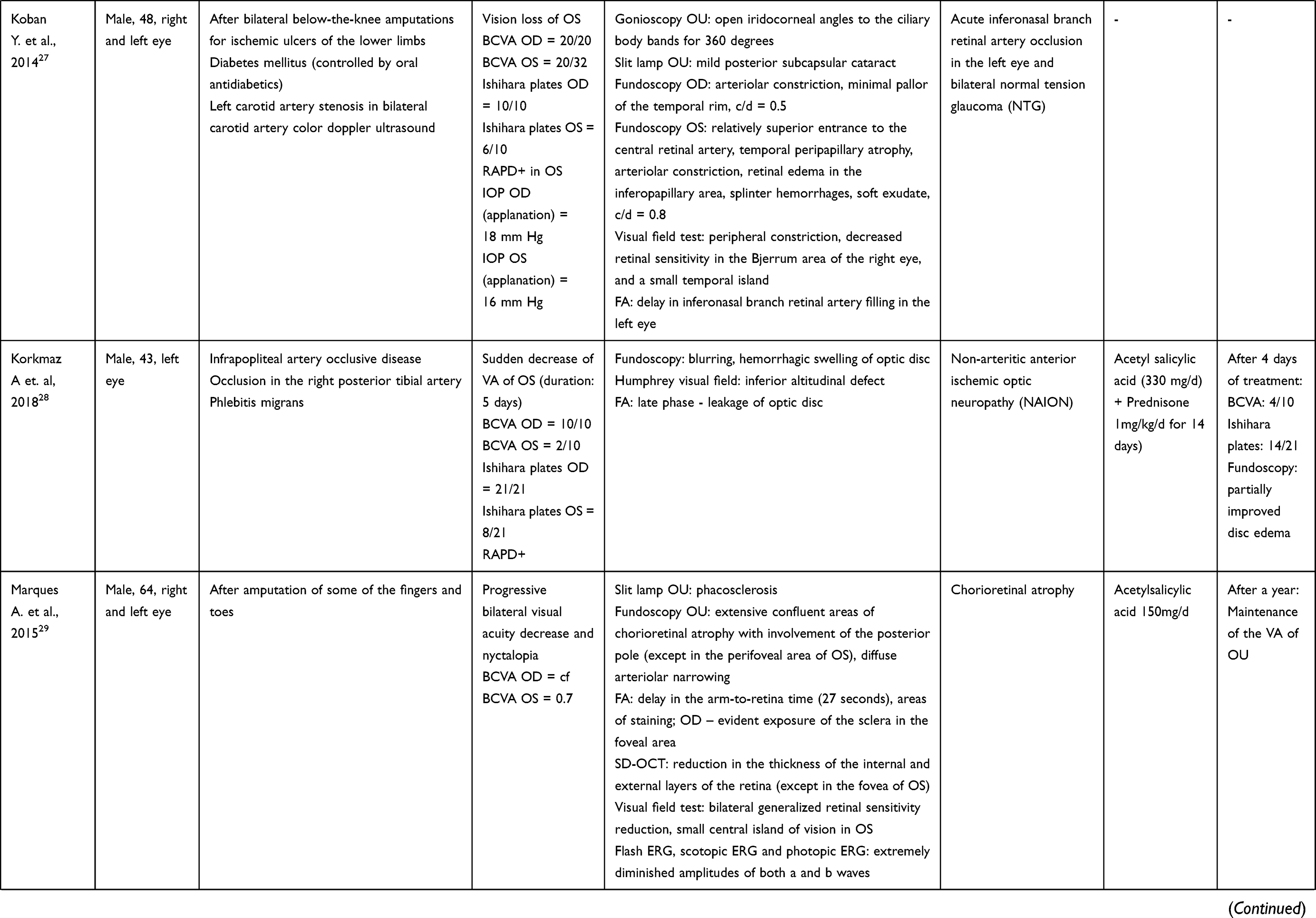 | 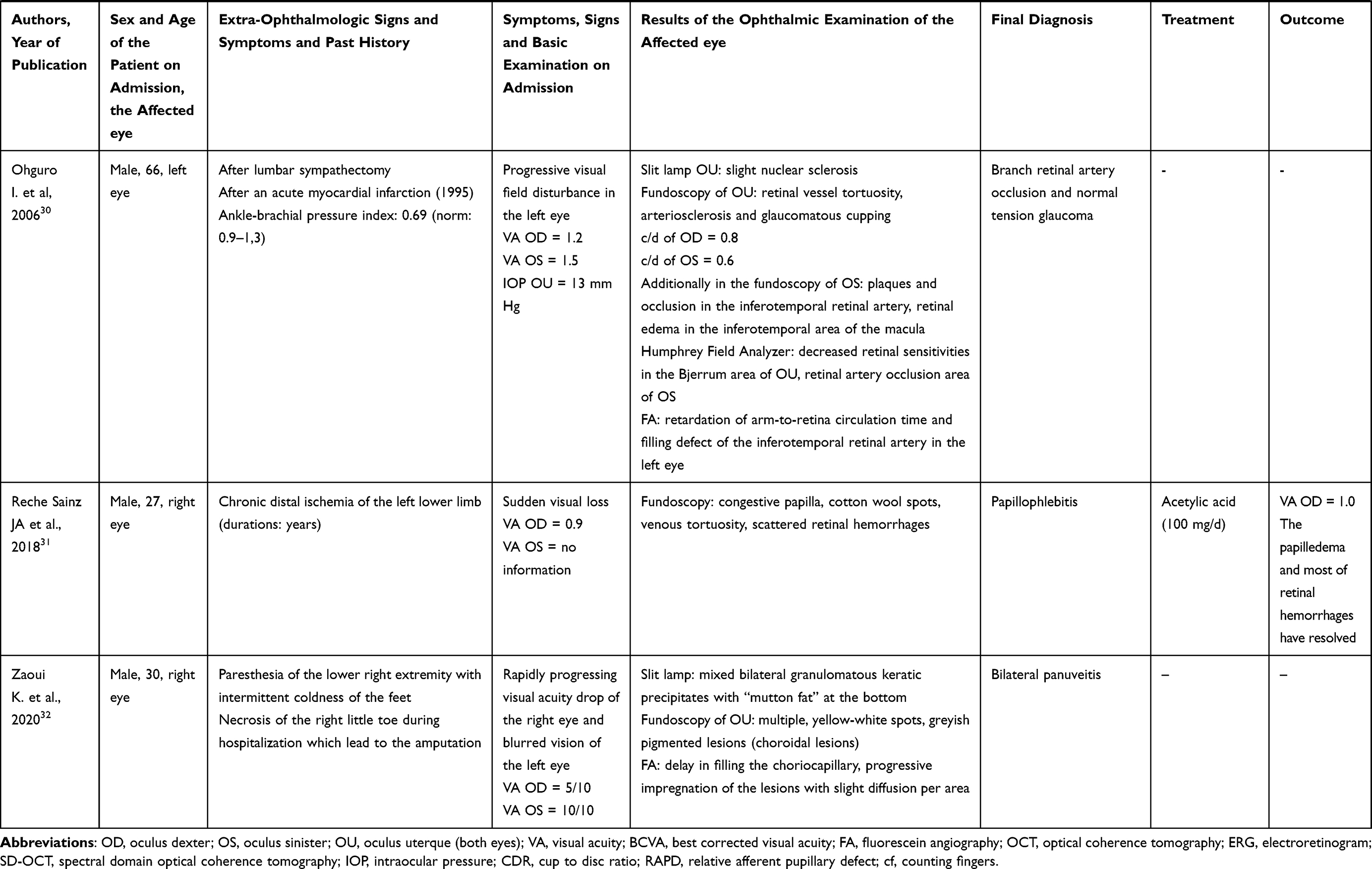 |
Table 1 Review of 9 Articles Concerning Ocular Manifestations of Buerger’s Disease |
As mentioned above, we have found 4 articles which we would like to discuss in a narrative form. Coppeto and Adamczyk reported anterior ischemic optic neuropathy in a 77-year-old patient suffering from Buerger’s disease.22 Arslan et al examined 26 men suffering from Buerger’s disease and compared them to 26 healthy men in a similar range of age.20 The only risk factors in both groups were male gender and smoking. The patients suffering from thromboangiitis obliterans were diagnosed based on the criteria proposed by Shinoaya.23 The extra-ophthalmological signs and symptoms of some patients included: segmental occlusions in extremities, foot wounds (12), rest pain and hyperemia (14), wounds on the fingers (3), positive Allen’s test (6). Nineteen patients had undergone unilateral lumbar sympathectomy, 2 patients had bilateral lumbar sympathectomy performed and in 4 cases finger amputation was carried out. All patients were treated with acetylsalicylic acid (150 mg). In the experimental group only 2 patients had no pathology in the fundus of their eyes. The other patients presented with optic atrophy (2 patients) and atherosclerotic hypertensive retinopathy (10 patients - grade I, 12 patients - grade II). In the control group only 4 patients were diagnosed with grade I retinopathy and the results of the other patients were unremarkable.20 Homma et al observed severe narrowing of the bulbar conjunctival arteries in patients with thromboangiitis obliterans.19 Valdes et al performed electroretinography in 10 patients previously diagnosed with Buerger’s disease on the basis of clinical, angiographical and anatomopathological criteria.21 They observed changes in the latency, amplitude and number of oscillatory potentials as well as changes in the a and b waves in the electroretinogram (eg elongated latency of OP, absence of subcomplex b, decreased amplitude of OP, decreased number of OP).21
The number of patients with ocular manifestations of Buerger’s disease described in the reviewed articles equaled 44. We did not take into account the study published by Homma et al, as the exact number of patients with ocular involvement had not been given. The percentage of different types of ophthalmological involvement is given in Table 2.
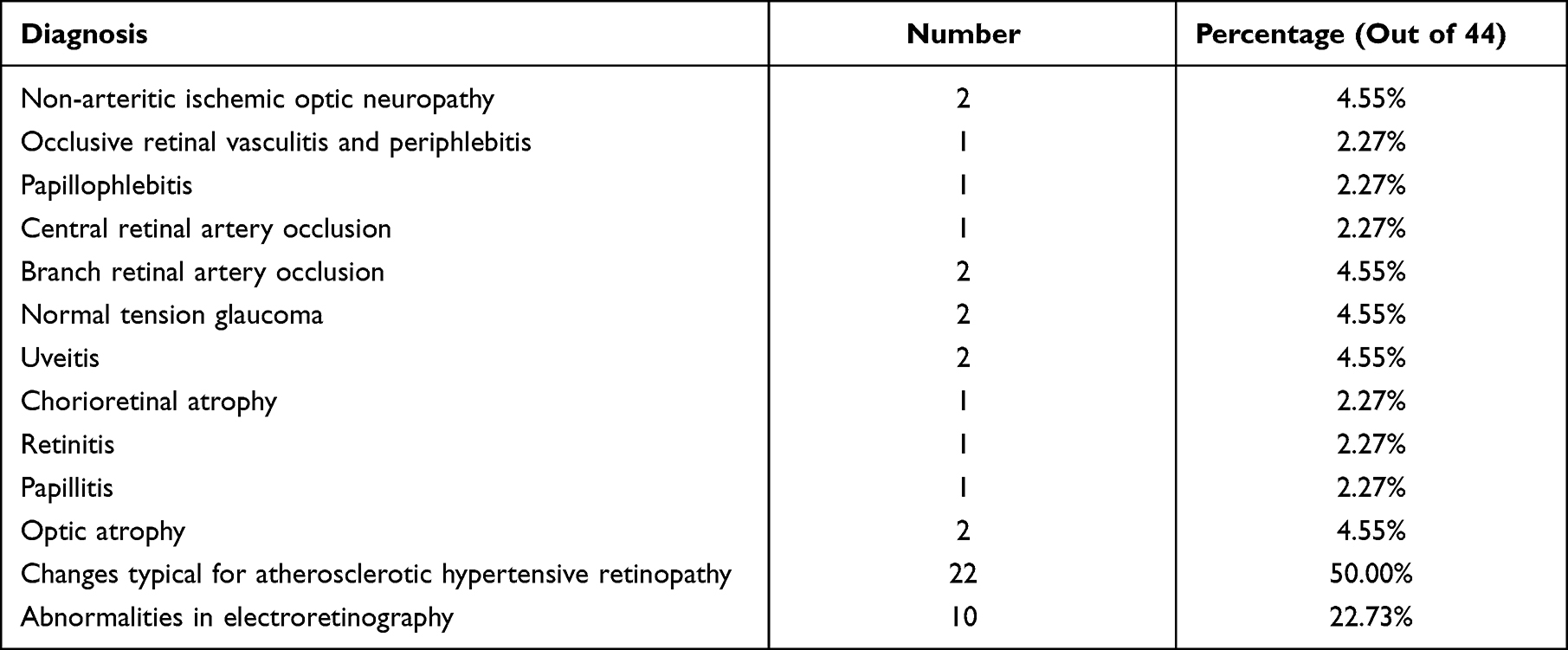 |
Table 2 The Percentage of Different Types of Ophthalmological Involvement in Patients with Buerger’s Disease |
Discussion
The first reports concerning ocular manifestations of Buerger’s disease date back to the 1930s and 1940s. The following presentations were described: narrowing and obliteration of a vascular lumen in the vessels of the retina, iris and ciliary body in retinal periphlebitis, iritis, iridocyclitis, complicated cataract, phthisis bulbi, choroiditis, vitreous opacities, choroid atrophy, white colouring of the retinal artery, white sheath on the retinal arteries, embolism of the central retinal arteries, hemorrhages in the retina and the vitreous body, retinitis proliferans, retinal atrophy, optic atrophy and Eale’s disease.33 Except for the case report published in the 1980s, the topic was not further researched until the next millennium. We managed to review 13 articles describing the involvement of the eyes in the course of thromboangiitis obliterans. We presented 10 isolated cases and 3 studies (conducted by Homma et al, Arslan et al, Valdes et al and Homma et al) showing ophthalmological changes in more than one patient. There seems to be no more studies on a larger group.
The criteria for the diagnosis of Buerger’s disease differ depending on the author. Ollin et al have included the following aspects in the diagnosis: “an age of less than 45 years and current (or recent) history of tobacco use; the presence of distal-extremity ischemia (indicated by claudication, pain at rest, ischemic ulcers, or gangrene) documented by noninvasive vascular testing; exclusion of autoimmune diseases, hypercoagulable states, and diabetes mellitus by laboratory tests; exclusion of a proximal source of emboli by echocardiography and arteriography; and consistent arteriographic findings in the clinically involved and noninvolved limbs“.12 The slightly different criteria were proposed by Papa et al, Mills and Porter or Shionoya.23,34,35 The reviewed articles were written from the ophthalmological perspective and in many cases the patients had been diagnosed with Buerger’s disease prior to the eye problems. That is why the information on the exact criteria on the basis of which Buerger’s disease was actually diagnosed is frequently missing.
What needs to be emphasized is that diagnosing thromboangiitis obliterans is based mainly on excluding some other systemic diseases (eg autoimmune diseases). In almost each reviewed article the process of diagnosing was explained in details. Laboratory tests, imaging tests (eg color duplex ultrasound, extremities angiography, photoplethysmographic waveform analysis) and clinical presentation were taken into account. This also explains how the ophthalmological manifestations were attributed to Buerger’s disease, as patients suffering from thromboangiitis obliterans are usually thoroughly examined in search for any other comorbidity. That is why the chance of some other disorder causing the involvement of the eye in Buerger’s disease is low.
We understand the necessity of providing strict inclusion criteria for Buerger’s disease, uniform for all articles and based on the acknowledged classifications. Yet, we could not follow such rigorous methodology because of all articles reviewed in our analysis only two referred to a specific classification of criteria for diagnosing Buerger’s disease (Dimopoulos et al and Arslan et al.). In the remaining works the diagnosis was taken for granted as the starting point for further investigation of ocular problems. Some researchers stated that other causes, risk factors or systemic diseases had been excluded (Eris et al, Korkmaz et al, Re-Sainz et al, Zaoui et al, Marques et al.). Ohguro et al mentioned the patient’s past medical history. We assumed that the diagnoses of Buerger’s disease in the reviewed papers were accurate.
It appears that patients suffering from Buerger’s disease may develop non-arteritic anterior ischemic optic neuropathy (NAION), occlusive retinal vasculitis and periphlebitis, papillophlebitis, central retinal artery occlusion (CRAO), branch retinal artery occlusion (BRAO), normal tension glaucoma (NTG), uveitis, chorioretinal atrophy, retinitis, papillitis, optic atrophy, changes typical for hypertensive retinopathy. Additionally, the abnormalities in electroretinography might be present. In the presented cases the occlusion of retinal vessels was the most common ocular manifestation of thromboangiitis obliterans (3 cases: 1 patient with central retinal artery occlusion and 2 patients with branch retinal artery occlusion), followed by normal tension glaucoma (2 cases) and uveitis (2 cases). The first condition mentioned above could be explained by vasospasm and thrombotic occlusion in the course of Buerger’s disease.26,30 Vasospasm may also be responsible for the development of normal tension glaucoma and non-arteritic anterior ischemic optic neuropathy, as it may lead to disturbances in the blood flow within the optic nerve head.27,28,30 There are studies suggesting an autoimmune background in thromboangiitis obliterans, which might be connected with the development of uveitis (also an autoimmune disease) in two cases.32,36,37
The types of tests which may be useful when examining patients suffering from Buerger’s disease mainly depend on the symptoms. However, in many cases fluorescein angiography was conducted and delivered important information. The treatment options and the possible outcome also depend on the type of ocular manifestations, so it seems impossible to propose a universal therapy.
To our knowledge, there seems to be no publication which would discuss all the articles we have managed to find. The most comprehensive review published by Fakour and Fazeli summed up 5 positions.11 The limitation of our review might be that we did not restrict the time span within which the publications for the analysis were to be found. Only 5 articles were published in the past 5 years. Finally, our inclusion criterion regarding the diagnosis of Buerger’s disease in the reviewed works was not based on any specific classification.
Conclusion
Although the number of publications we have found might not be impressive (13), we need to remember that Buerger’s disease is rare and the ocular manifestations in its course are extremely rare. Furthermore, there seems to be no specific features that would make it possible to predict which patient with Buerger’s disease is likely to develop ophthalmological complications. The patients described in the review articles did not differ from a typical patient suffering from thromboangiitis obliterans. That is why all patients with this disorder should be treated with caution as potentially at risk for eye problems. Introducing routine eye examination for all patients with Buerger’s disease might be helpful. Some of the ocular manifestations of the disorder could be detected during a basic ophthalmic examination comprised of visual acuity and intraocular pressure tests as well as a slight lamp examination. Having analyzed the findings we suspect that Buerger’s disease may not be localized vasculopathy but a systemic disease and - like other vasculitis – it may affect various organs and systems. We hope our review may help to raise awareness of possible ocular manifestations in the course of Buerger’s disease and encourage physicians taking care of patient with thromboangiitis obliterans to perform ophthalmological examinations.
Funding
The study was supported by Wroclaw Medical University, Wrocław, Poland.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kreuzpointner R, Valerio L, Corsi G, et al. Ophthalmic complications of lemierre syndrome. Acta Ophthalmol. 2021;100:e314.
2. Wiest MRJ, Toro MD, Nowak A, et al. Globotrioasylsphingosine Levels and Optical Coherence Tomography Angiography in Fabry Disease Patients. J Clin Med. 2021;10(5):1093.
3. Böni C, Al-Sheikh M, Hasse B, et al. Multimodal imaging of choroidal lesions in disseminated mycobacterium chimaera infection after cardiothoracic surgery. Retina. 2019;39(3):452–464.
4. Carnevali A, Giannaccare G, Gatti V, et al. Retinal microcirculation abnormalities in patients with systemic sclerosis: an explorative optical coherence tomography angiography study. Rheumatology. 2021;3:957.
5. Rivera-Chavarría IJ, Brenes-Gutiérrez JD. Thromboangiitis obliterans (Buerger’s disease). Ann Med Surg. 2016;7:79–82.
6. von Winiwarter F. Über eine eigentümliche Form von Endarteriitis und Endophlebitis mit Gangrän des Fusses. Arch Klin Chir. 1879;23:202–226.
7. Buerger L. Thromboangiitis Obliterans. Indian Med Gazette. 1953;88:395–396.
8. Piazza G, Creager MA. Thromboangiitis obliterans. Circulation. 2010;121(16):1858–1861.
9. National Organization for Rare Disorders. Buerger’s Disease. Available from: https://rarediseases.org/rare-diseases/buergers-disease/.
10. Mayo Clinic. Buerger’s disease. Available from: https://www.mayoclinic.org/diseases-conditions/buergers-disease/symptoms-causes/syc-20350658.
11. Fakour F, Fazeli B. Visceral bed involvement in thromboangiitis obliterans: a systematic review. Vasc Health Risk Manag. 2019;15:317–353.
12. Olin JW. Thromboangiitis obliterans (Buerger’s disease). N Engl J Med. 2000;343(12):864–869.
13. Cebezas-Moya R, Dragstedt LRII. An extreme example of Buerger’s disease. Arch Surg. 1970;101:632–634.
14. Harten P, Muller-Huelsbeck S, Regensburger D, Loeffler H. Multiple organ manifestations in thromboangiitis obliterans (Buerger’s disease): a case report. Angiology. 1996;47:419–425.
15. Tarabishy AB, Schulte M, Papaliodis GN, Hoffman GS. Wegener’s granulomatosis: clinical manifestations, differential diagnosis, and management of ocular and systemic disease. Surv Ophthalmol. 2010;55(5):429–444.
16. Deuter CM, Kötter I, Wallace GR, Murray PI, Stübiger N, Zierhut M. Behçet’s disease: ocular effects and treatment. Prog Retin Eye Res. 2008;27(1):111–136.
17. Vodopivec I, Rizzo JF. Ophthalmic manifestations of giant cell arteritis. Rheumatology. 2018;57:63–72.
18. Palejwala NV, Walia HS, Yeh S. Ocular manifestations of systemic lupus erythematosus: a review of the literature. Autoimmune Dis. 2012.
19. Homma S, Tsushima N, Minamiyama M, Hayashi T, Matsuo H. Microvascular blood is distributed more to venules than to arterioles in patients with Buerger’s disease. Observation of bulbar conjunctiva by intravital microscope system. Int Angiol. 2000;19(2):135–141.
20. Arslan C, Altan H, Tanrıverdi S, Demirbaş M, Topçu K, Bozkurt AK. Investigation of eye involvement in Buerger’s disease. Turk J Thorac Cardiovasc Surg. 2009;17:179–181.
21. Valdes AR, Freixa RS, Cossio OH, Bizet LMO, Hernandez JS. Alteraciones electroretinograficas de la tromboangeitis obliterante (Enfermedad de Buerger). Angiologia. 1988;88:166–169.
22. Coppeto JR, Adamczyk D. Anterior ischemic optic neuropathy in Buerger’s disease. Ann Ophthalmol. 1988;20(9):332–334.
23. Shinoya S. Diagnostic criteria of Buerger’s disease. Int J Cardiol. 1998;66(Suppl 1):S243–S247.
24. Böke W, Duncker G. Beidseitig rezidivierende Uveitis, Retinitis und Papillitis. Komplikation einer Thromboangiitis obliterans? Klin Mbl Augenheik. 1983;3:294–297.
25. Dimopoulos IS, Dollin M, Gottlieb CC. Occlusive retinal vasculitis and periphlebitis in Buerger’s disease: a case report. J Ophthalmic Inflamm Infect. 2020;10(1):29.
26. Eris E, Sucu ME, Perente I, Alkın Z, Ozkaya A, Tarakcioglu HN. Retinal Artery Occlusion Secondary to Buerger’s Disease (Thromboangiitis Obliterans). Case Rep Ophthalmol Med. 2017;2017:3637207.
27. Koban Y, Bilgin G, Cagatay H, et al. ‘The association of normal tension glaucoma with Buerger’s disease: a case report. BMC Ophthalmol. 2014;14:130.
28. Korkmaz A, Karti O, Top karti D, Yüksel B, Zengin MO, Kusbeci T. Could Buerger’s disease cause nonarteritic anterior ischemic optic neuropathy?: a rare case report. Neurol Sci. 2018;39(7):1309–1312.
29. Marques AS, Portelinha J, Almeida A, Guedes M. Chorioretinal atrophy in a patient with Buerger’s disease. Ophtalmologia. 2015;38:139–143.
30. Ohguro I, Ohguro H, Ohta T, Nakazawa M. A case of normal tension glaucoma associated with Buerger’s disease. Tohoku J Exp Med. 2006;209(1):49–52.
31. Reche-Sainz JA, Gutiérrez-Montero O. Papillophlebitis in a young male patient with Buerger’s disease. Papiloflebitis en varón joven con enfermedad de Buerger. Arch Soc Esp Oftalmol. 2018;93(7):354–356.
32. Zaoui K, Messaoudi R, Salaheddine B. Unusual Association of Uveitis and Buerger’s Disease. J Ophthalmol Clin Res. 2020;4(1):876.
33. Puttanna ST. Thromboangeitis associated with retinal vasculitis. J All India Ophthalmol Soc. 1966;14(5):209–213.
34. Papa MZ, Rabi I, Adar R. A point scoring system for the clinical diagnosis of Buerger’s disease. Eur J Vasc Endovasc Surg. 1996;11(3):335–339.
35. Mills JL, Porter JM. Buerger’s disease: a review and update. Semin Vasc Surg. 1993;6(1):14–23.
36. Papa M, Bass A, Adar R, et al. Autoimmune mechanisms in thromboangiitis obliterans (Buerger’s disease): the role of tobacco antigen and the major histocompatibility complex. Surgery. 1992;111(5):527–531.
37. Lee T, Seo JW, Sumpio BE, Kim SJ. Immunobiologic analysis of arterial tissue in Buerger’s disease. Eur J Vasc Endovasc Surg. 2003;25(5):451–457.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.