Back to Journals » International Medical Case Reports Journal » Volume 19
Ocular Decompression Retinopathy During Pars Plana Vitrectomy Without Pre-Existing Ocular Hypertension: A Case Report
Authors Brito ME ![]() , Romero JL, Rivas SA, Martínez IA, Fernández AE
, Romero JL, Rivas SA, Martínez IA, Fernández AE
Received 11 April 2026
Accepted for publication 6 July 2026
Published 13 July 2026 Volume 2026:19 615053
DOI https://doi.org/10.2147/IMCRJ.S615053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Giuseppe Giannaccare
Miguel E Brito,1,2 José L Romero,1,2 Samuel A Rivas,1,2 Irma A Martínez,1,2 Alfredo E Fernández1,2
1Instituto Docente de Especialidades Oftalmológicas (IDEO), Maracaibo, Zulia State, Venezuela; 2University of Zulia, Maracaibo, Zulia State, Venezuela
Correspondence: Miguel E Brito, Instituto Docente de Especialidades Oftalmológicas (IDEO), Calle 69A con Avenida 17, Edificio IDEO, Maracaibo, Estado Zulia, 4001, Venezuela, Tel +1 7866365127, Fax +58 2617628922, Email [email protected]
Purpose: To report a case of ocular decompression retinopathy that developed during pars plana vitrectomy in the absence of pre-existing ocular hypertension.
Case Presentation: An 84-year-old male patient was referred to our hospital following complicated phacoemulsification for cataract surgery involving a posterior capsular rupture. As a result, 25G+ pars plana vitrectomy was performed along with cortical remnant removal, iridodialysis repair, and intraocular lens (IOL) implantation. During surgery, ocular deformation occurred, accompanied by iris prolapse and acute hypotony due to abrupt intraocular pressure (IOP) fluctuations linked to infusion pressure changes during IOL implantation. Multiple intraretinal hemorrhages, including peripapillary hemorrhages and those over the posterior pole and equator, were observed. Optical coherence tomography performed on the following days confirmed the presence of hemorrhages identified during the intraoperative period at different retinal levels.
Conclusion: Ocular decompression retinopathy can occur after various ocular surgeries, especially those associated with intraoperative IOP changes. Intraocular pressure control maneuvers and maintenance of ocular tone are crucial for the success of any surgical procedure.
Keywords: ocular decompression retinopathy, vitrectomy, ocular hypertension, ocular complications, retina
Introduction
Ocular decompression retinopathy was first described by Fechtner et al in 1992.1 It is an uncommon but major complication associated with rapid intraocular pressure (IOP) changes during ocular surgeries, commonly seen in glaucoma surgeries such as trabeculectomies,2 valve implantation procedures, or following intraocular trauma.3
Vitrectomy, a common surgical procedure used to treat various ocular pathologies including vitreous hemorrhage and retinal detachment, may trigger this complication if the eye undergoes rapid decompression. Acute hypotony associated with intraoperative distortion of the eyeball increases shear stress on the blood capillaries, leading to rupture of the vascular wall and the development of hemorrhages at different levels. This explains its occurrence during pars plana vitrectomies in eyes without glaucoma or any other associated pathology.
Although this type of complication has been documented, it is essential to further investigate patients without preexisting ocular hypertension. In this report, we present a case of ocular decompression retinopathy during pars plana vitrectomy in a patient without preexisting ocular hypertension.
Case Presentation and Management
An 84-year-old male patient with no systemic history underwent cataract phacoemulsification complicated by a posterior capsular rupture. Preoperative visual acuity was hand motion (HM), and axial length measured 23.01 mm. Subsequently, under peribulbar anesthesia, 25G+ pars plana vitrectomy was performed to remove cortical remnants, repair iridodialysis, and implant an intraocular lens (IOL). Total surgery time was 52 minutes. Iridodialysis repair required approximately 15 minutes, while intraocular lens (IOL) implantation required approximately 5 minutes.
The IOP was initially maintained at 35 mmHg through proper positioning of the irrigation cannula. During lens implantation, the irrigation line was closed to allow anterior chamber maneuvers while maintaining ocular tone through correct cannula positioning. During these maneuvers and lens implantation, deformation of the globe and iris prolapse occurred, resulting in transient hypotony, which lasted approximately 55 seconds. After restoring infusion pressure, the globe regained its tone.
As the surgery continued, multiple new-onset intraretinal hemorrhages were observed around the peripapillary area, posterior pole, and equator (Figure 1). There was no history of elevated IOP, either postoperatively or prior to surgery. No epinephrine was added to the infusion line or administered intracamerally. The patient was treated using topical steroids and cycloplegic agents.
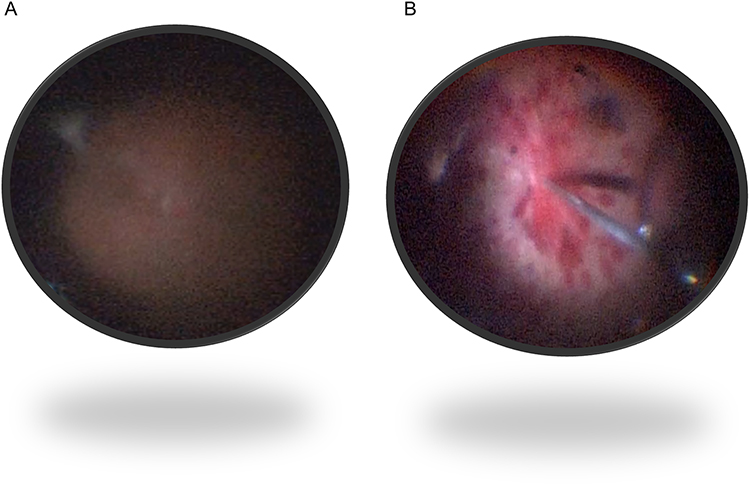 |
Figure 1 Intraoperative fundus images extracted from surgical video. (A) Posterior pole at the beginning of pars plana vitrectomy, showing absence of retinal hemorrhages. (B) Intraoperative appearance of diffuse retinal hemorrhages during surgery. |
In the following days, indirect ophthalmoscopy confirmed the presence of intraretinal hemorrhages initially observed intraoperatively (Figure 2). Spectral-domain optical coherence tomography (SD-OCT) (Spectralis, Heidelberg Engineering, Heidelberg, Germany) revealed hemorrhages in different retinal layers, predominantly within the inner layers, and localized neurosensory retinal detachments (Figures 3 and 4). Fluorescein angiography showed areas of hypofluorescence corresponding to hemorrhagic areas (Figure 5). One month later, gradual reabsorption of the hemorrhage and improvement in visual acuity were observed. Early postoperative visual acuity was counting fingers at 35 cm, improving to 20/100 at late postoperative follow-up.
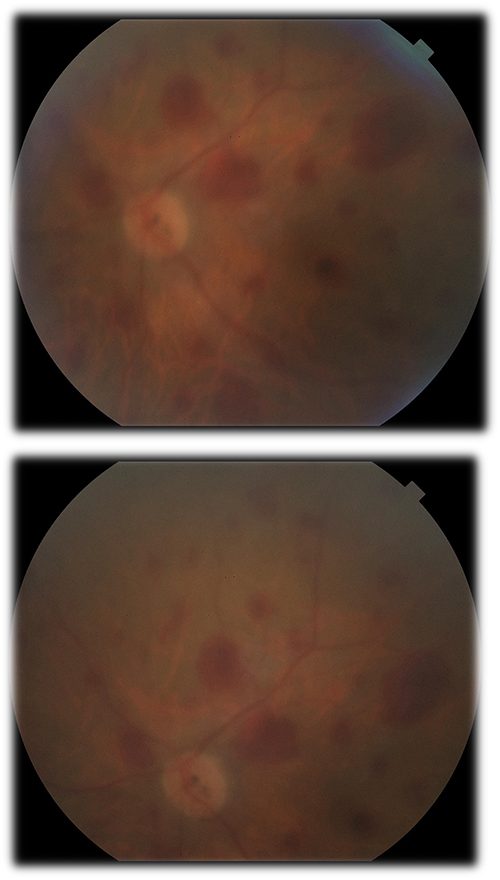 |
Figure 2 Color fundus photograph of the left eye with intraretinal hemorrhages in four quadrants. |
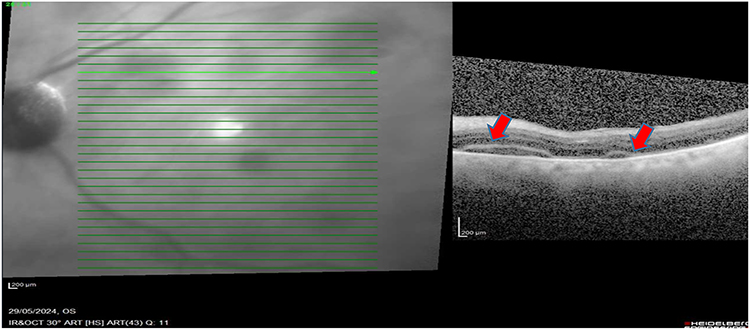 |
Figure 3 Optical coherence tomography (OCT) of the left eye showing two focal neurosensory retinal detachments with localized subretinal fluid (red arrows). |
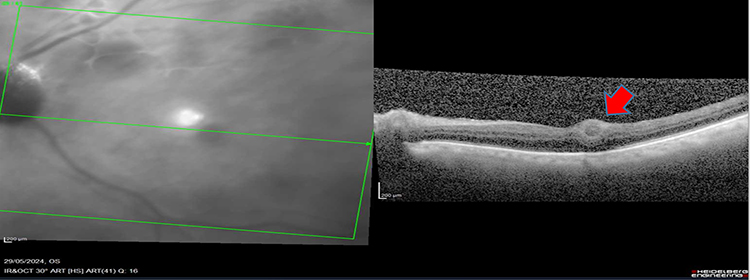 |
Figure 4 Spectral-domain optical coherence tomography (SD-OCT) of the left eye showing a focal intraretinal hemorrhage predominantly involving the inner retinal layers (red arrow). |
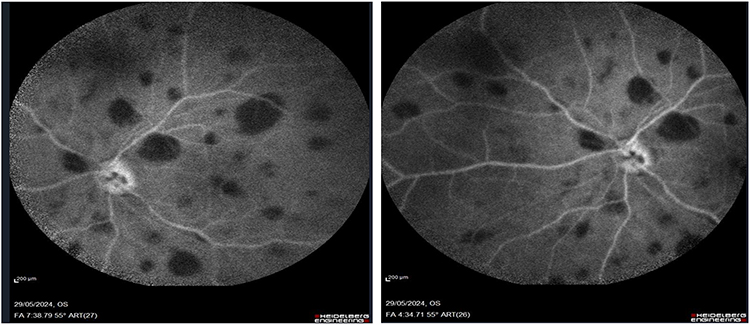 |
Figure 5 Fluorescein angiography of the left eye demonstrating multiple areas of hypofluorescence corresponding to intraretinal hemorrhages, consistent with blockage effect and without evident retinal vascular leakage. |
Discussion
This case suggests that ocular decompression retinopathy may occur, even in patients without prior ocular hypertension. While various cases of intraoperative decompression retinopathy have been reported in the literature, the primary associations have been with surgeries, such as phacoemulsification,4 silicone oil extraction,5 vitrectomies in eyes with a history of elevated IOP,5,6 decompressive paracentesis due to neovascular glaucoma,5,7 uveitic glaucoma,8 or open-angle glaucoma (after maximum medical therapy and selective laser trabeculoplasty),9 sclerotomies with mitomycin C,10 Nd:YAG laser iridotomies,11 orbital decompression surgeries,12 and goniotomies,13 most often associated with filtering surgeries,4,14–16 procedures under general anesthesia,17 and even exceptionally, in a non-surgical eye during acute angle-closure managed with rapid IOP reduction through medical treatment.18
A recent systematic review reported that 15% of decompression retinopathy cases developed on the day of surgery, with a mean time diagnosis of 1.5 ± 2.0 days postoperatively.3 Only one case occurred within minutes of performing a decompressive paracentesis;9 in other cases of anterior chamber decompression for neovascular glaucoma7 and uveitic glaucoma,8 detection occurred within 24 h following the procedure.
In scientific literature, only two cases of decompression retinopathy during 25G pars plana vitrectomy have been reported, both following cataract surgery and associated with elevated preoperative IOP.6,19 Therefore, most reported IOP cases are associated with glaucoma pathology; however, this is not the sole cause of its pathogenesis, making it essential to understand the dynamics of vascular rupture.
Surgical maneuvers during vitrectomy can significantly alter retinal hemodynamics. Mechanical and vascular theories have been proposed to explain these different presentations. Particular attention has been paid to the autoregulation and fragility of the retinal capillaries. Autoregulation accommodates fluctuations in systemic and intraocular signals; however, it is compromised in conditions such as diabetes mellitus, hypertension, and uncontrolled chronic diseases in which the internal system breaks down. In such cases, an acute reduction in IOP results in decreased arterial resistance and a consequent increase in blood flow, which can overwhelm the already fragile capillary bed and lead to capillary rupture.3
Another theory posits that anterior displacement due to sudden IOP drop may obstruct axoplasmic flow and cause disc edema and central retinal vein compression.3 Mechanically, any tubular structure can be exposed to two different forms of stress: inflation, which is related to increased intratubular pressure relative to external pressure, and elongation, which is associated with deformation. In both cases, this leads to the failure and extravasation of fluid, typically at the weakest points.20,21
Finite element analysis suggests that either a 30% increase in arteriolar capillary pressure or a complete reduction of IOP to zero increases shear stress by one- to two-fold on capillary blood vessels, equating to a 43-fold increase in wall tension and highlighting the potential for vascular rupture under mechanical distortion.
To better illustrate the proposed biomechanical sequence underlying ocular decompression retinopathy, a conceptual pathophysiological cascade is shown in Figure 6.
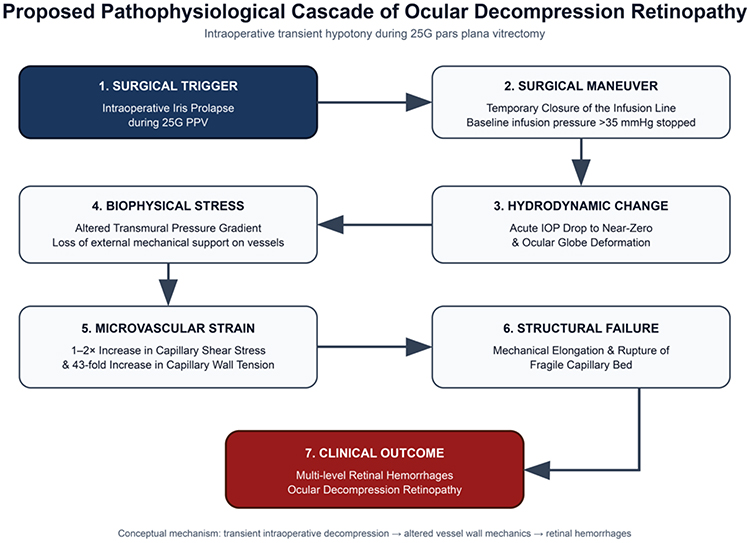 |
Figure 6 Proposed pathophysiological cascade of ocular decompression retinopathy during pars plana vitrectomy, illustrating the potential biomechanical sequence linking abrupt intraoperative hypotony and globe deformation to increased capillary stress and intraretinal hemorrhage. |
In the intraoperative period in the present case, infusion pressures greater than 35 mmHg were maintained through an irrigation cannula from the start of surgery to preserve adequate ocular tone. However, iris prolapse occurred during iris repair and IOL implantation, necessitating the closure of the irrigation line for immediate repositioning. This resulted in ocular deformation and hypotony, which were quickly corrected by restoring infusion pressure to the aforementioned levels.
It is important to emphasize that changes in infusion pressure causing ocular globe deformation and associated hypotony represent key mechanical factors in the development of retinopathy. These mechanical changes may occur independently or in association with different intraocular pathologies, such as glaucoma, increasing the predisposition to capillary dysregulation, as described in two other reported cases of decompression retinopathy.17
Saricaoglu et al17 reported a noteworthy finding in a case of congenital glaucoma, in which retinal hemorrhages were found in one eye with high postoperative IOP, while no such hemorrhages were found in the other eye, which was hypotonic following glaucoma surgery. This observation suggests that hemorrhage is likely caused by intraoperative or perioperative hypotony, with postoperative hypotony playing a less important role in the pathogenesis. In the second case, there was no predisposition to defective vascular autoregulation, such as that associated with long-standing glaucoma, indicating that retinal hemorrhage may have resulted from a Valsalva maneuver during extubation under general anesthesia. The Valsalva maneuver impedes venous return by increasing the intrathoracic pressure, which in turn increases retinal blood flow. In this patient, hypotony may have further amplified the effect of the Valsalva maneuver on the retinal circulation.17
Additionally, general anesthesia is considered a predisposing factor for decompression retinopathy, likely by amplifying the effects of hypotony in combination with the Valsalva phenomenon. This should not be confused with Valsalva retinopathy, which typically presents as premacular preretinal hemorrhage.17
Medryzcka et al18 confirmed this difference through multimodal imaging and reported an exceptional case in which decompression retinopathy developed in one eye without prior surgical procedures and solely following rapid IOP reduction in a case of acute angle-closure achieved through medical treatment. This was detected using fundus photography, OCT, OCT angiography, and fluorescein angiography.18
OCT allows the assessment of retinal thickness and morphology of decompression retinopathy. It enables the evaluation and evolution of hemorrhages at various retinal levels as well as the integrity of the outer retina and retinal pigment epithelium. In many cases, decreased visual acuity is associated with macular hemorrhage. Similarly, OCT aids in the differential diagnosis of central retinal vein occlusion given the absence of macular edema and lack of venous dilatation observed on fluorescein angiography, particularly in young, asymptomatic patients without prior vascular filling abnormalities.18,22,23
Mukkamala et al found macular edema in 5% of decompression retinopathy cases and associated it with decreased visual acuity when hemorrhage was not detected in the foveal area. In the reported case evaluated using SD-OCT, cystoid macular edema was not observed.
In the present case, localized subretinal fluid with focal neurosensory retinal detachments were observed on SD-OCT. Although a direct causal relationship between ocular decompression retinopathy and subretinal fluid accumulation cannot be definitively established, acute intraoperative hypotony may represent a plausible contributing mechanism. Abrupt reduction in intraocular pressure may alter choroidal hydrostatic dynamics and disrupt normal fluid homeostasis, favoring transient fluid accumulation beneath the neurosensory retina during periods of ocular hypotony. This mechanism may plausibly explain the localized subretinal fluid observed in our patient.24
These findings support the mechanical theory as a trigger for decompression retinopathy in cases where hypotony and ocular deformation act as causal agents. The resulting alterations in shear stress are believed to generate hemorrhage at all retinal levels, thereby affecting visual recovery. Despite their typical self-limiting course and spontaneous resolution, these hemorrhages can affect visual recovery. This finding highlights the importance of maintaining a stable IOP during surgery to prevent associated complications. This report suggests that transient intraoperative hypotony alone may trigger ocular decompression retinopathy during pars plana vitrectomy, even in eyes without pre-existing ocular hypertension, emphasizing the critical role of maintaining stable intraocular pressure throughout vitreoretinal surgery.
Conclusion
Ocular decompression retinopathy is a potential complication of surgery involving significant IOP fluctuations, particularly those requiring intraoperative maneuvers that induce ocular deformation or hypotony. These mechanical changes lead to capillary rupture owing to the increased intratubular tension. Although decompression retinopathy is typically self-limiting, with spontaneous resolution of retinal hemorrhages and gradual visual improvement, its occurrence underscores the importance of maintaining a stable IOP throughout surgical procedures. Effective control of IOP and preservation of ocular tone are critical for minimizing the risks and ensuring successful surgical outcomes.
Consent for Publication
Institutional approval was not required for publication of this case report. Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal upon request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fechtner RD, Minckler D, Weinreb RN, Frangei G, Jampol LM. Complications of glaucoma surgery. Ocular decompression retinopathy. Arch Ophthalmol. 1992;110:965–7.
2. Yalvac IS, Kocaoglan H, Eksioglu U, Duman S. Decompression retinopathy after Ahmed glaucoma valve implantation in a patient with congenital aniridia and pseudophakia. J Cataract Refract Surg. 2004;30:1582–1585.
3. Agarwal L, Pradhan D, Agrawal N, Joshi I, Kumari A, Kushwaha A. Intraoperative ocular decompression retinopathy during 23 gauge transconjunctival vitrectomy: a case report. Int Med Case Rep J. 2019;12:389–392. doi:10.2147/IMCRJ.S236499
4. Chen YL, Yang XN, Liu YL, Li WT, Huo LJ. Ocular decompression retinopathy after phacoemulsification in a patient with primary acute angle-closure glaucoma undergoing chemotherapy. Int J Ophthalmol. 2024;17(2):397–400. doi:10.18240/ijo.2024.02.25
5. Arévalo JF, Mendoza AJ, Fernández CF, et al. Decompression retinopathy after intraocular surgery. Arch Soc Esp Oftalmol. 2007;82(10):629–634. doi:10.4321/s0365-66912007001000007
6. Rezende FA, Regis LGT, Kickinger M, Alcântara S. Decompression retinopathy after 25-gauge transconjunctival sutureless vitrectomy: report of 2 cases. Arch Ophthalmol. 2007;125(5):699–700. doi:10.1001/archopht.125.5.699
7. Tsai YE, Hsu CR. Ocular decompression retinopathy after anterior chamber paracentesis for neovascular glaucoma. Medicina. 2021;57(10):1038. doi:10.3390/medicina57101038
8. Rao SK, Greenberg PB, Macintyre RB, Ducharme JF. Ocular decompression retinopathy after anterior chamber paracentesis for uveitic glaucoma. Retina. 2009;29(2):280–281. doi:10.1097/IAE.0b013e318185ea54
9. Prince J, Fleischman D. Immediate manifestation of ocular decompression retinopathy following anterior chamber paracentesis. Case Rep Ophthalmol. 2019;10(2):287–291. doi:10.1159/000501846
10. Salinas L, Chaudhary A, Mansouri K. Optical coherence tomography angiography description of ocular decompression retinopathy after deep sclerectomy in traumatic glaucoma. J Glaucoma. 2018;27(3):297–301. doi:10.1097/IJG.0000000000000870
11. Waheeb SA, Birt CM, Dixon WS. Decompression retinopathy following YAG laser iridotomy. Can J Ophthalmol. 2001;36(5):278–280. doi:10.1016/s0008-4182(01)80035-1
12. Ben Simon GJ, Goldberg RA, McCann JD. Bilateral decompression retinopathy after orbital decompression surgery. Br J Ophthalmol. 2004;88:1605–1606. doi:10.1136/bjo.2004.049767
13. Burstein ES, Netland PA. Decompression retinopathy after goniotomy in a child. J Glaucoma. 2017;26(8):747–748. doi:10.1097/IJG.0000000000000681
14. Mukkamala SK, Patel A, Dorairaj S, et al. Ocular decompression retinopathy: a review. Surv Ophthalmol. 2013;58(6):505–512. doi:10.1016/j.survophthal.2012.11.001
15. Bansal A, Ramanathan US. Ocular decompression retinopathy after trabeculectomy with mitomycin-C for angle recession glaucoma. Indian J Ophthalmol. 2009;57(2):153–154. doi:10.4103/0301-4738.45510
16. Singh KS, Bhattacharyya M, Wali K, Rana K, Jain D. Ocular decompression retinopathy: a case series. Nepal J Ophthalmol. 2017;9(18):194–198. doi:10.3126/nepjoph.v9i2.19269
17. Saricaoglu MS, Kalayci D, Guven D, Karakurt A, Hasiripi H. Decompression retinopathy and possible risk factors. Acta Ophthalmol. 2009;87(1):94–95. doi:10.1111/j.1600-0420.2007.01083.x
18. Mędrzycka J, Szabelska P, Rerych M, Różycki R, Gołębiewska J. Multimodal imaging techniques in monitoring a patient with ocular decompression retinopathy. Diagnostics. 2023;13(12):1992. doi:10.3390/diagnostics13121992
19. Gupta R, Browning AC, Amoaku WM. Multiple retinal haemorrhages (decompression retinopathy) following paracentesis for macular branch artery occlusion. Eye. 2005;19(5):592–593. doi:10.1038/sj.eye.6701530
20. Williamson T. Vitreoretinal Surgery.
21. Doğramacı M, Dikkaya F, Şentürk F, Aras C. Experimental laboratory modeling of choroidal vasculature: a study of the dynamics of intraoperative choroidal hemorrhage during pars plana vitrectomy. Turk J Ophthalmol. 2021;51(5):294–300. doi:10.4274/tjo.galenos.2020.64927
22. Ferro Desideri L, Anguita R. Decompression retinopathy. J Fr Ophtalmol. 2023;46(9):1127–1128. doi:10.1016/j.jfo.2023.05.004
23. Singlas M, Coppens C, Jany B, Tran THC. Rétinopathie de décompression post-iridotomie périphérique: à propos d’un cas. J Fr Ophtalmol. 2023;46(4):e108–e110. doi:10.1016/j.jfo.2022.10.013
24. Besirli CG, Johnson MW. Uveal effusion syndrome and hypotony maculopathy. In: Ryan SJ, Schachat AP, Sadda SR, Hinton DR, Wilkinson CP, Wiedemann P. editors. Retina. Vol. 2,
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Surgical Outcomes for Uncomplicated Primary Retinal Detachment Repair
Heydinger S, Ufret-Vincenty R, Robertson ZM, He YG, Wang AL
Clinical Ophthalmology 2023, 17:907-915
Published Date: 17 March 2023
Ocular Hypertension Following Open Globe Injury in Patients Undergoing Pars Plana Vitrectomy
Karimaghaei S, Al-Hindi H, Chauhan MZ, Elhusseiny AM, Sanvicente CT, Uwaydat SH
Clinical Ophthalmology 2025, 19:1339-1344
Published Date: 19 April 2025