")
Back to Journals » Clinical Ophthalmology » Volume 17
Ocular and Palpebral Manifestations of Facial Palsy: An Epidemiologic Descriptive Study
Authors Guerrero-de Ferran C , Valdez-García JE , Rivera-Alvarado IJ, González-García AE , Bastán-Fabián D , Rangel-Trejo M
Received 19 November 2022
Accepted for publication 27 January 2023
Published 1 April 2023 Volume 2023:17 Pages 1007—1011
DOI https://doi.org/10.2147/OPTH.S398190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Caroline Guerrero-de Ferran, Jorge E Valdez-García, I Jocelyn Rivera-Alvarado, Ángel E González-García, Daniel Bastán-Fabián, Melissa Rangel-Trejo
Tecnológico de Monterrey, School of Medicine and Health Sciences, Department of Ophthalmology, Monterrey, México
Correspondence: Caroline Guerrero-de Ferran, Tecnológico de Monterrey, School of Medicine and Health Sciences, Av. Ignacio Morones Prieto 3000. Colonia Los Doctores. CP 64710, Monterrey, Nuevo León, México, Tel +52 (81) 88 88 05 51, Email [email protected]
Purpose: We describe the ocular and periocular clinical features in patients with a facial palsy diagnosis of any etiology and to report the demographics, relevant medical history and treatment modalities in these patients.
Patients and Methods: Retrospective and descriptive observational study. A total of 60 patients with a facial palsy diagnosis in the last 5 years were recruited from an ophthalmological clinic in northeastern Mexico. Demographic data, such as age, sex, disease evolution and etiology, visual acuity, ocular symptoms and ocular and periocular clinical features were obtained. Personal history of previous ophthalmologic surgery, as well as ocular and systemic diseases, were also recorded. Finally, a comparative analysis was done to determine association between signs, symptoms and treatment modalities.
Results: A prevalence of 0.14% was reported, 56.7% of patients were female, and mean age of presentation was 55.63± 17.2 years. 76.7% of facial palsy was idiopathic in origin, followed by vascular disease in 8.30% and iatrogenic in 6.70%. 40% of patients had a history of arterial hypertension, 36.3% were diabetic, and 6.70% had cerebrovascular disease.
Conclusion: Early diagnosis of facial palsy is crucial in establishing an effective treatment plan and avoiding complications. The impact of this disease in patients’ quality of life cannot be overlooked, and steps should be taken to address the different impairments that this ailment entails.
Keywords: dry eye, ophthalmology, oculoplastics, facial palsy, epidemiology
Introduction
The facial nerve (CN VII) contains multiple fiber types, such as motor, sensory and parasympathetic fibers and their corresponding nuclei.1–4 Facial Palsy (FP) has a myriad of etiologies, from the use of forceps during complicated vaginal delivery to neoplastic lesions, but the most common culprit is Bell’s Palsy, which is thought to have its origin in a reactivation of viral replication by herpes simplex virus type-1 (HSV-1) in the nerve’s cranial ganglia.1,5,6 Other important etiologies include Ramsay-Hunt syndrome, Lyme’s disease, ear infections, iatrogenic, tumoral, congenital, granulomatous and traumatic conditions, and many more.3,6–9 Depending on the degree of nerve damage, the end result can range from a complete and persistent FP to a complete recovery in function.7 Its incidence can vary from 11 to 40 cases per 100,000 people annually.10
Diagnosis of this ailment is mainly clinical, with an acute onset, a duration of hours or days, and is generally accompanied by retroauricular pain. In peripheral FP, a total laxity of the hemiface is observed, with absent expression and a downward deviation of the ipsilateral mouth.1–5 The severity of FP is graded with the House-Brackmann clinical scale, although the Sunnybrook scale has gained more popularity internationally due to a more comprehensive scoring system.11 Inferior palpebral laxity and, ultimately, lagophthalmos can cause a variety of ocular surface damage, such as conjunctival irritation, corneal dryness and erosions, and even ulceration and/or perforation of the cornea.1–5 Bell’s phenomenon should be assessed to determine whether it is present or absent, since it represents a protective factor.2,6 It is also important to assess Meibomian gland dysfunction, since a growing body of evidence demonstrates structural alterations in these glands, which ultimately lead to tear film instability.12,13
Almost 90% of patients experience spontaneous recovery, albeit not a complete one. Around 70–80% of FP patients will experience a complete recovery, while the rest can present acute or chronic complications, such as persistent facial weakness, abnormal axonal branching, as well as synkinesis in muscles innervated by CN VII.5,8 Prompt treatment of this disease is crucial in avoiding complications, and it consists of medical, surgical, and rehabilitation modalities. It is of the utmost importance to protect the eyeball from continued exposure to environmental insults, such as air and pollutants, so ointments and protective eye shields should be prescribed. Medical treatment with corticosteroids, antivirals, analgesics and even botulinum toxin can be employed.3,5 Surgical treatment is usually reserved as a last resort and patients should be aware that it has varying degrees of success.1,9,14
Rehabilitation should be initiated as soon as possible, there are many different options, and an important rehabilitation modality is tailored facial muscles exercises. These exercises have moderate evidence of improving outcomes in patients with moderate and/or chronic FP and present virtually no adverse effects, so they should be considered.15 Techniques such as neuromuscular re-education, biofeedback, electrostimulation, and facial expression exercises are available, but they do not have a strong level of evidence.5,15,16 The term “facial disability” was coined to describe patient’s quality of life impairments, such as eating and speaking handicaps, as well as the emotional and social aspects that this ailment can entail.17,18
Materials and Methods
This study was registered on November 2th, 2021 under the registration number: P000602-MOPPAF-CI-CR002 and was approved by the local Ethics Committee. It was a retrospective and descriptive observational study. A total of 43,656 electronic records from two major third-level health institutions were surveyed, and 60 patients with a diagnosis of FP in the last 5 years were recruited. Patients were from the metropolitan area of Monterrey, Nuevo León in Mexico.
Demographic data, such as age, sex, disease evolution, visual acuity, ocular symptoms, as well as ocular and periocular clinical features were obtained. Past medical history pertaining to systemic and/or ocular disease was also investigated. Also, history of ophthalmologic surgery was recorded.
Central tendency measurements were compared with the T-student method once they were adjusted for the homogeneity of the variance, Mann–Whitney test was used for non-parametric variables, and Odds Ratio analysis was performed. Data analysis was performed using IBM SPSS 26 and R Studio 4.1-1-1-383. Finally, a comparative analysis (Odds Ratio) was performed to determine whether an association between different signs, symptoms and treatment modalities could be found.
Results
An FP prevalence of 0.14% (CI 0.13–1.12) was calculated based on our sample size. Out of all 60 patients, 34 (56.7%) were female, mean age at presentation was 55.63 ± 17.2 years, and disease evolution time was 96.69 ± 135.4 months. Bell’s palsy was the most common etiology, with 46 (76.7%) patients presenting as such, followed by vascular disease in 5 (8.3%) patients and an iatrogenic origin in 4 (6.70%) patients. Also, 58 (96.7%) patients presented as unilateral FP. Synkinesis occurred in 18 patients (30%), while 42 experienced chronic flaccid FP.
The main disease associated with FP in this sample was Arterial Hypertension in 24 (40%) patients, followed by Diabetes Mellitus (DM) in 22 (36.30%) and past facial nerve surgery and cerebrovascular disease in 4 (6.70%). A summary of associated diseases can be consulted in Table 1. In terms of ocular and periocular disease association, the main entity was cataract in 12 (20%) patients, as well as glaucoma and diabetic retinopathy in 4 (6.70%), the rest of associated ocular/periocular diseases are summarized in Table 2.
 |
Table 1 Systemic Comorbidities in Our Population Sample |
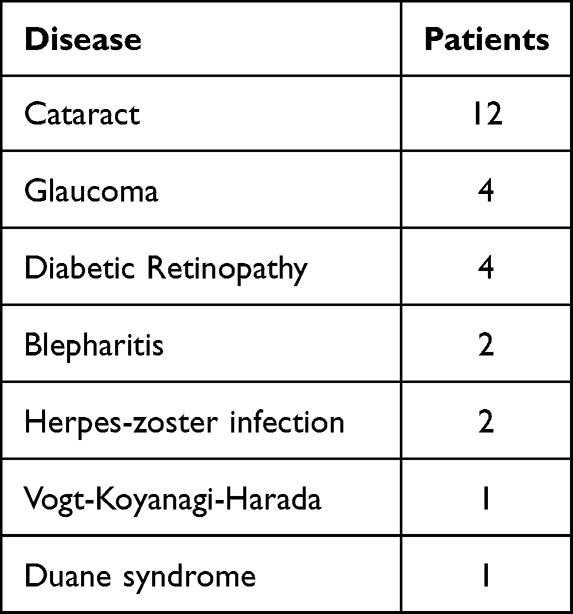 |
Table 2 Ocular Comorbidities in Our Population Sample |
Symptomatology associated with FP consisted of foreign body sensation in 33 (54.50%) patients, blurred vision in 30 (50%), facial asymmetry in 26 (43.90%), epiphora in 17 (28.30%) and ocular pain in 16 (26.30%). 85% of patients presented two or more symptoms. Ocular signs such as superficial punctate keratopathy presented in 41 (68.30%) patients, exposure keratopathy in 26 (43.30%), corneal pannus and corneal ulcer in 5 (8.80%), conjunctivitis in 2 (3.30%), and conjunctival chemosis and persistent epithelial defect in 1 patient each (1.80%).
Periocular clinical features refer to palpebral and adnexal alterations, such as lagophthalmos in 25 (41.70%) patients, ptosis in 18 (30%), blepharospasm in 16 (26.70%), hemifacial spasm in 12 (20%), palpebral laxity in 10 (17.50%), and ectropion and brow ptosis in 8 (13.30%).
The different treatment modalities used in these patients can be grouped into medical or surgical management. It is important to mention that many patients underwent both types of treatment, and some even had one or more treatments in the same category. A complete summary of treatments can be viewed in Table 3.
 |
Table 3 Treatment Modalities Used in Our Patients |
Patients presenting with comorbidities had an increased risk of needing surgical treatment (63.64%, OR 5.64 [1.79–17.74], P = 0.0051). A strong association between having a comorbidity and epiphora (59.09%, OR 12.28 [3.21–46.89], P < 0.001). The main periocular features that had an impact in future morbidity were palpebral laxity (45.5%, P < 0.001), abnormal regeneration (54.5%, P < 0.001), and ectropion (31.82%, P = 0.0027). Finally, patients with morbidity secondary to FP were more likely to require treatment with lubricant eye gel (45.45% OR 3.69 [1.14–11.93], P < 0.0376) or lateral canthopexy (40.9%, P < 0.001).
Discussion
The results reported in our study reflect those described by Tavares-Brito et al, where 920 patients with FP were evaluated and the predominant sex was female, most cases were unilateral, and the most frequent etiology was Bell’s palsy.18,19 The prevalence calculated in our sample was very similar to that reported by Chang et al, being 0.12%.20
Our analysis yielded a strong association between the presence of a previously diagnosed comorbidity and the eventual need of a surgical treatment. Even though most patients were female, there was no correlation between sex and the development of comorbidities, and this was also reflected with age, whereas increasing age did not correlate with an increased risk of comorbidity. It would have been interesting to determine whether the severity of FP was correlated with this outcome, but a limitation of this study was its retrospective nature, and not all patients were graded with the House-Brackmann scale.
There was a strong association between epiphora and comorbidities pertaining to the ocular surface. Other clinical features that had an important impact on whether a morbidity could develop, or a surgical treatment would be eventually needed, were palpebral laxity, aberrant regeneration and paralytic ectropion. Some studies have estimated that aberrant regeneration can present in up to 9% of cases, while 30% of cases suffered from this outcome in our study, which reflects more recent evidence.20–22 It is important to note that 56.7% of the patients in our study underwent medical treatment with 2 or more options.
Conclusion
FP is an important cause of ocular morbidity and not many studies report epidemiologic data on Hispanic patients. The importance of this statement is that diseases must be analyzed with different perspectives, since different factors such as culture, politics and economics have an impact on their diagnosis and treatment. The scenario in lower-income countries is dire and, in many instances, diagnosis is delayed. This also impacts the outcome of treatment of many ailments, and early detection is crucial in FP, since prompt treatment can make a great difference in a patient’s quality of life.21
One limitation of this study, as previously mentioned, was its retrospective nature. Since clinical research in our country is not common practice, clinical records are not always filled out with research purposes in mind. This ultimately translates to missing pieces of information, which affect data precision. Nonetheless, valuable epidemiologic data could be reported in this study, as well as information on important clinical features and treatment modalities.
In summary, physicians should be aware that early diagnosis of FP can have a powerful impact in outlining an efficient treatment plan and avoiding morbidity. The toll that FP takes on patients’ quality of life is a major issue that should not be overlooked, and one must be ready to treat, or refer if the need arises, this ailment to improve patient care.
Abbreviations
FP, facial palsy; CN VII, cranial nerve VII; HSV-1, herpes simplex virus 1; DM, diabetes mellitus; OR, odds ratio.
Ethics Declaration
The present study was approved by the Monterrey Institute of Technology and Higher Education Ethics in Research Committee (Comité de Ética en Investigación de la Escuela de Medicina del Instituto Tecnológico y de Estudios Superiores de Monterrey) and the Monterrey Institute of Technology and Higher Education Research Committee (Comité de Investigación del Instituto Tecnológico y de Estudios Superiores de Monterrey) under the registration number: P000602-MOPPAF-CI-CR002. All patients agreed to participate in this study and informed consent was obtained. This study follows the principles of the Helsinki Declaration.
Acknowledgments
The authors would like to thank all patients included in this study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Seneviratne SO, Patel BC. Facial nerve anatomy and clinical applications. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554569/.
2. Spencer CR, Irving RM. Causes and management of facial nerve palsy. Br J Hosp Med. 2016;77(12):686–691. doi:10.12968/hmed.2016.77.12.686
3. Lee V, Currie Z, Collin JRO. Ophthalmic management of facial nerve palsy. Eye. 2004;18(12):1225–1234. doi:10.1038/sj.eye.6701383
4. De Seta D, Mancini P, Minni A, et al. Bell’s palsy: symptoms preceding and accompanying the facial paresis. Sci World J. 2014;2014:54.
5. Agostini F, Mangone M, Santilli V, et al. Idiopathic facial palsy: umbrella review of systematic reviews and meta-analyses. J Biol Regul Homeost AGENTS. 2020;34(4):1245–1255.
6. Mavrikakis I. Facial nerve palsy: anatomy, etiology, evaluation, and management. Orbit. 2008;27(6):466–474. doi:10.1080/01676830802352543
7. Jowett N, General A. Approach to Facial Palsy. Otolaryngol Clin North Am. 2018;51(6):1019–1031. doi:10.1016/j.otc.2018.07.002
8. Gilchrist JM. Seventh cranial neuropathy. Semin Neurol. 2009;29(1):5–13. doi:10.1055/s-0028-1124018
9. Hohman MH, Hadlock TA. Etiology, diagnosis, and management of facial palsy: 2000 patients at a facial nerve center. Laryngoscope. 2014;124:7. doi:10.1002/lary.24542
10. Melvin TAN, Limb CJ. Overview of facial paralysis: current concepts. Facial Plast Surg. 2008;24(2):155–163. doi:10.1055/s-2008-1075830
11. Kanerva M, Jonsson L, Berg T, et al. Sunnybrook and House-Brackmann systems in 5397 facial gradings. Head Neck Surg. 2011;144(4):570–574. doi:10.1177/0194599810397497
12. Shah CT, Blount AL, Nguyen EV, Hassan AS. Cranial nerve seven palsy and its influence on meibomian gland function. Ophthal Plast Reconstr Surg. 2012;28(3):166–168. doi:10.1097/IOP.0b013e31823f2f82
13. Ekin A. The role of meibomian gland dysfunction on the development of dry eye disease in patients with facial nerve palsy. Arq Bras Oftalmol. 2021;1–8.
14. Custer PL. Ophthalmic management of facial nerve palsy patients. Semin Plast Surg. 2004;18(1):31–38.
15. Teixeira LJ, Valbuza JS, Prado GF. Physical therapy for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Sys Rev. 2011;(12):CD006283. doi:10.1002/14652858.CD006283.pub3
16. Khan AJ, Szczepura A, Palmer S, et al. Physical therapy for facial nerve paralysis (Bell’s palsy): an updated and extended systematic review of the evidence for facial exercise therapy. Clin Rehabil. 2022;36(11):1424–1449. doi:10.1177/02692155221110727
17. Kahn JB, Gliklich RE, Boyev KP, Stewart MG, Metson RB, McKenna MJ. Validation of a patient-graded instrument for facial nerve paralysis: the FaCE Scale. Laryngoscope. 2001;111(3):387–398. doi:10.1097/00005537-200103000-00005
18. Fonseca KM, Mourão AM, Motta AR, Vicente LCC. Scales of degree of facial paralysis: analysis of agreement. Braz J Otorhinolaryngol. 2015;81(3):288–293. doi:10.1016/j.bjorl.2014.04.005
19. Tavares-Brito J, van Veen MM, Dusseldorp JR, Bahmad F, Hadlock TA. Facial Palsy-Specific Quality of Life in 920 Patients: correlation with Clinician-Graded Severity and Predicting Factors. Laryngoscope. 2019;129(1):100–104. doi:10.1002/lary.27481
20. Chang YS, Choi JE, Kim SW, Baek SY, Cho YS. Prevalence and associated factors of facial palsy and lifestyle characteristics: data from the Korean National Health and Nutrition Examination Survey 2010-2012. BMJ Open. 2016;6(11):1–7. doi:10.1136/bmjopen-2016-012628
21. Yamamoto E, Nishimura H, Hirono Y. Occurrence of sequelae in bell’s palsy. Acta Otolaryngol. 1987;104(S446):93–96. doi:10.3109/00016488709121848
22. Guntinas-Lichius O, Prengel J, Cohen O, et al. Pathogenesis, diagnosis and therapy of facial synkinesis: a systematic review and clinical practice recommendations by the international head and neck scientific group. Front Neurol. 2022;13:1019554. doi:10.3389/fneur.2022.1019554
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.