Back to Journals » Vascular Health and Risk Management » Volume 19
Occupational Noise-Induced Pre-Hypertension and Determinant Factors Among Metal Manufacturing Workers in Gondar City Administration, Northwest Ethiopia
Authors Melese M, Adera A, Ambelu A, Gela YY ![]() , Diress M
, Diress M ![]()
Received 28 October 2022
Accepted for publication 11 January 2023
Published 15 January 2023 Volume 2023:19 Pages 21—30
DOI https://doi.org/10.2147/VHRM.S392876
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Mihret Melese, Ayechew Adera, Adugnaw Ambelu, Yibeltal Yismaw Gela, Mengistie Diress
Department of Human Physiology, School of Medicine, University of Gondar, Gondar, Ethiopia
Correspondence: Mengistie Diress, University of Gondar, P. O. Box 196, Gondar, Ethiopia, Email [email protected]
Introduction: Cardiovascular disorders are one of the commonly recognized occupational diseases in the developed world. Individuals chronically exposed to noise at workplaces had a higher risk of developing elevated arterial blood pressure. There are limited studies in Ethiopia regarding this topic and thus this study determined the prevalence and determinant factors of occupational noise-induced pre-hypertension among metal manufacturing workers in Gondar city administration, Northwest Ethiopia.
Methods: An institution-based cross-sectional study design was carried out. In this study, 300 study participants were recruited by census sampling method. A sound level meter was used to measure the working area noise level. A semi-structured pre-tested interviewer-administered questionnaire was used to collect sociodemographic and clinical data. Blood pressure was measured in a quiet room in the morning using a mercurial sphygmomanometer. Both bivariable and multi-variable binary logistic regressions were used to identify factors associated with noise-induced prehypertension. Adjusted odds ratio with 95% confidence interval was reported, and variables with p < 0.05 were considered as statistically associated factors with pre-hypertension.
Results: The prevalence of noise-induced pre-hypertension was 27.7% (95% CI: 22.7– 32.7). In multivariable logistic regression, working area noise level (AOR = 3.8, 95% CI: 6.8– 8.9), 45– 65 years’ age (AOR = 9.8, 95% CI: 5.4– 12.9), years of work experience ((6– 10 years (AOR = 2.8, 95% CI: 1.98– 5.90 and > 10 years (AOR = 4.8, 95% CI: 7.8– 9.75)), being a cigarette smoker (AOR = 3.6, 95% CI: 1.36– 9.77), and alcohol consumption (AOR = 2.4, 95% CI: 1.06– 1.04) were significantly associated with noise-induced prehypertension.
Conclusion: Workers in metal manufactures who were exposed to noise levels > 85 dB developed elevated blood pressure. The odds of having prehypertension were increased by years of work experience, advanced age, smoking, and alcohol consumption. Our findings recommended that the real-world preventive strategies should be taken to lower the risk of noise-induced pre-hypertension hastened by occupational noise exposure.
Keywords: noise, pre-hypertension, metal manufacturing workers, Ethiopia
Plain Language Summary
What is Already Known on This Topic?
Prolonged occupational noise exposure is associated with many health-related problems including elevated arterial blood pressure. Workers in metal processing factories are exposed to noise, which consecutively increases the risk noise-induced hypertension.
What This Study Adds?
This research demonstrated that employees working in a high sound level have developed pre-hypertension and it was associated with advanced age and longer work experience of workers. This study offers a strong association between noise exposure and elevated blood pressure among workers. This finding, which is specific on hypertension, will provide a significant information for workers and the employee to design and implement preventive strategies. Our study focused on a single health problem because the intervention mechanisms for every disorders are different. So, if the workers have been aware as high noise level causes elevated blood pressure, they would try to consider all possible primary and secondary prevention modalities.
Introduction
Cardiovascular disorders are one of the commonly recognized occupational diseases in the developed world. The World Health Organization estimates that about 250 million workers around the globe are exposed to potentially hazardous noise levels. Individuals chronically exposed to noise at workplaces had a higher risk of developing elevated arterial blood pressure.1,2
Smaller enterprises like metal processing factories play an important role in the economic growth of developing nations like Ethiopia.3 Metal workers are usually exposed to noise emanating from the manipulation of metals. Chronic exposure to this type of occupation is a risk factor for health abnormalities including hearing impairment4–6 and cardiovascular diseases like noise-induced hypertension.7–9 In the globe, there are numerous studies that demonstrate the association between occupational noise exposure and the development of cardiovascular and metabolic diseases.9–13 The mechanism of how noise causes cardiovascular disease is not well established. However, sustained autonomic and endocrine system activation induced by excessive and chronic noise is thought to be a factor contributing to the development of cardiovascular diseases, including hypertension.14–16
Environmental stressors produce unique cardiovascular risk factors such as hypertension, hyperglycemia, and hyperlipidemia.8,17,18 Exposure to manufacturings, road, railway, and recreational noises as a stressor can increase the risk of transient elevation of blood pressure, either by releasing stress hormones (such as adrenaline and cortisol) or by stimulating the sympathetic nervous system.18–23 If the noisy stress is chronic and repetitive, it may lead to pre-hypertension (systolic blood pressure=120–139 mmHg or diastolic blood pressure=80–89 mmHg) and hypertension (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg).24,25 Pre-hypertension tends to increase in severity over time and may progress to clinical hypertension in years and its prevalence increases as age increases.26
Different epidemiological studies in the world have explored the association between occupational noise exposure and elevated blood pressure. For every 5 dB(A) increase in occupational noise exposure, the incidence (relative risk) of hypertension was 1.14.27 Workers exposed to noise levels above 80 dB(A) have been reported to have a higher risk of hypertension.27,28 Prolonged exposure to noise levels ≥85 dBA increases the systolic and diastolic blood pressure levels.29 A study in Pakistan revealed that industrial areas are high noise sites (sound level ≥95 dBA) and the prevalence of prehypertension and hypertension was 23.6% and 24.4% among the employees respectively.11 Based on a study in Japan, the prevalence of hypertension among study participants working in the noise workplace was 16.9%.30 According to the study in China, the prevalence of hypertension among study participants exposed to occupational noise during their work period was 52.6%.31 Studies regarding the association between noise exposure and high BP in Sweden showed that the prevalence of prehypertension was 22% in boys and 8% in girls.32 An experimental study in Egypt indicated that occupational noise exposure is associated with the risk of prehypertension.33 Another study in south Korea confirmed a positive association between exposure to noise over 85 dB(A) with pre-hypertension and hypertension in male workers.34
Eventhough various literatures revealed the association of occupational noise and arterial blood pressure, very little is known about it in Africa, particularly in Ethiopia. Therefore, this study aimed to determine the prevalence and determinant factors of occupational noise-induced pre-hypertension among metal manufacturing workers in Gondar city administration, Northwest Ethiopia. Conducting this research will have a crucial role in filling the above gaps, and to design and implement strategies for the prevention and management of the problem in the study areas.
Methods and Materials
Study Setting, Design and Period
Cross-sectional study was conducted among metal manufacturing workers in Gondar City Administration, Northwest Ethiopia, from April 1 to May 30, 2021. Gondar is the capital city of the central Gondar zone in Amhara Regional State. It is one of the historical cities in the country and is located 750 km from Northwest of Addis Ababa. The city administration has 12 sub-cities with 12 urban and 10 rural kebeles. According to Gondar town industry development office information, there are 46 metal manufacturings in Gondar city administration.
Population and Eligibility Criteria
The source of population were all the metal factory workers in Gondar city. The study population were all metal factory workers who were present in the study area during the study period. All adult metal factory workers whose age ≥18 years and who have been working in the metal factory for at least 6 months were included in the study, whereas those who were known hypertensives and severely ill during data collection period were excluded.
Sample Size Determination and Sampling Technique
According to the thumb rule, our study population were not more than 500 and, therefore, sample size calculation was not applicable. Hence, Census sampling method was used to recruit the study participants for this study.
Variable of Study
Dependent Variables
- Noise-induced pre-hypertension (Yes/No).
Independent Variables
- Socio-demographic characteristics such as age, sex, occupation, educational level, income, work experience.
- Behavioral factors like alcohol, smoking, earphone utilization.
Operational Definition
Pre-Hypertension
Prehypertension was defined as the systolic blood pressure between the range of 121 and 139 mmHg or diastolic blood pressure between the range of 81 and 89 mmHg.35
Metal Factory/Manufacture
Institutions where metal welding, cutting, and reshaping were made to produce useful equipment.
Smoker
Metal factory workers who reported smoking at least for 6 months.36
High Noise Sound
Defined as the sound intensity level ≥85 dB.37
Alcohol Consumption
Participants who drank any alcohol at least 1 time per day for 1 year.38
Data Collection Tools and Procedures
Data were collected using pre-tested interviewer-administered semi-structured questionnaire adopted from previously published articles.9,11,12,29,30 The questionnaire was comprised of the socio-demographic characteristics, anthropometric measurement, and clinical factors collected by three professional nurses and two supervisors after providing 3 days of training.
Environmental Noise Measurement Survey
The environmental noise (working area noise level) was measured in work stations using the sound level meter (model SL-5868I) with a measurement range between 25 and 130 dB. In this study, the sound level meter was calibrated before and after each use and workplace noise level measurements were taken on slow response. The device was placed at an approximate distance of at least 1 meter from the noise source. The data collector holds the device by facing the microphone towards the noise source and observes the measurement on the liquid crystal display. Working area noise level was measured according to the guideline of occupational safety and health management services.39 Noise level measurements were made at each selected working site on five different days with 8 hours interval. Keeping the microphone dry, avoiding serious vibrations during measurement, keeping conditions of temperature and humidity were properly considered during noise measurement. Lastly, the mean working area noise level of 8-hour time-weighted average on five different days was taken for each working area.40
Blood Pressure Measurements
The measurements of blood pressure were performed in a quiet room in the morning using a mercurial sphygmomanometer.41 The workers had to have a rest for at least 10 minutes before entering the room, and then were guided into the sitting position after about 5 minutes of rest to test the blood pressure of the brachial artery three times. The data were used in the mean of them to express individuals’ blood pressure in this study.42 Blood pressure was taken following a gap of more than 12 h after noise exposure. It was measured using a mercury sphygmomanometer with subjects in the sitting position after more than 15 minutes of rest. SBP and DBP were reported as the average of three repeat measurements with 30-s intervals.42
A trained nurse used a sphygmomanometer to measure subjects’ BP two times on the left arm in the morning before starting to work. Prehypertension was defined as having a systolic blood pressure between 121 and 139 mmHg or a diastolic blood pressure between 81 and 89 mmHg.25,43
Sociodemographic Characteristics
Body mass index calculation, weight (BW) in kilograms (Kg) and height in meters (m) were recorded for all participants during the first visit for sample collection. Height was measured without shoes, with eyes straight ahead and a right-angle triangle resting on the scalp and against the wall, to the nearest 0.5 cm. Without shoes, weight was measured to the nearest 100 grams. The body mass index (BMI) was calculated using the following equation; BMI = Body Mass Index (kg)/Height (m)2.44 A semi-structured pre-tested questionnaire was administered to the subjects after obtaining their consent to collect sociodemographic and clinical data. The questionnaire comprised details on socio-demographic variables, dietary habits, tobacco use, alcohol consumption, physical activity, family history of hypertension and stress levels. Anthropometric measurements and blood pressure were recorded.
Data Processing and Analysis Procedure
The Shapiro–Wilk test was first used to determine the normality of the continuous variables of resting SBP and DBP, which were relevant to the prevalence of prehypertension, as well as the independent variables of age, and working area noise levels, employment duration, and BMI. The Hosmer–Lemeshow test was done to assess model goodness-of-fit (p≥0.05).
Data was entered into and analyzed by IBM SPSS Statistics V.21. Descriptive variables were analyzed using frequencies, proportions, and means to describe the socio-demographic, behavioral, and physical characteristics. Bivariable logistic regression analysis was applied to identify factors associated with prehypertension. All variables with a p-value of 0.25 from bivariable logistic regression analysis were entered into a multivariable logistic regression model to control the possible effects of confounder/s and to identify statistically significant variables. The strength of association between dependent and associated factors was determined using an odds ratio (OR) with corresponding 95% confidence intervals (CI). The level of significance was computed at a p-value ≤0.05.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Institutional Review Board of the University of Gondar (457/04/20210). A permission letter was obtained from Gondar city administration office before data collection (255/04/202). After the study participants were adequately briefed about the study, written informed consent was taken from each study participant. All methods were performed in accordance with the relevant guidelines and regulations of the Declaration of Helsinki.45
Since the majority of the study participants were illiterate, the data collector read the consent form and explained about the purpose and procedure of the study. Then, the data collector marked as “Yes” on the written consent form when the study participants were volunteered to participate in the study and recorded their signature with “thumbprint” and this process was approved by the IRB of the University of Gondar. The participants’ names and other personal identifiers were not included to maintain confidentiality and privacy.
Results
Socio-Demographic Characteristics of Study Participants
A total of 300 metal factory workers participated in the study. The majority of study participants were males (94.4%) with a median age of 35 years (IQR=16). One-third of the study participants had more than 10 years of working experience (34%). More than half (52%) of the study participants were exposed to greater than 85 dB (A) of the working area noise level. One-third of the study participants were smokers (34.7%), and nearly 40% of metalwork shop workers drank alcohol (Table 1).
 |
Table 1 Socio-Demographic and Work-Related Characteristics of Study Participants Among Metal Workers at Gondar City, Northwest Ethiopia, 2021 (N=300) |
Prevalence of Noise-Induced Prehypertension Among Metal Factory Workers
The over all prevalence of noise-induced pre-hypertension among the study participants was 27.7% (95.5% CI: 22.7–32.7) (Figure 1).
 |
Figure 1 Prevalence of Noise-induced prehypertension among metal factory workers in Gondar city, Ethiopia, 2022. |
Factors Associated with Noise-Induced Prehypertension
Almost one-third of the study participants had noise-induced prehypertension (27.7% (p <0.001)). A binary logistic regression analysis model was executed to assess the association of hearing loss with its associated factors. In the bivariable logistic regression analysis, exposure to working area noise level, age, cigar smoking, ear protection equipment, and alcohol consumption were statistically associated with noise-induced prehypertension. Moreover, variables like exposure to working area noise level, age group 45–65 years, work experience of 6–10 years, work experience 10 years, being a smoker, and alcohol consumption were significantly associated with noise-induced prehypertension in multivariable logistic regression (p<0.5).
Participants in the study who were between the ages of 45 and 65 had a 9.8 times higher chance of developing prehypertension (AOR = 9.8, 95% CI, 5.4–12.9) than those who were between the ages of 18 and 29. Being a smoker had a 3.6 times higher chance of developing prehypertension as compared to non-smokers (AOR=3.6, 95% CI; 1.36–9.77). The likelihood of prehypertension among metal workshop workers who were drinking alcohol was 2.4 times higher than the counterparts (AOR=2.4.95% CI; 1.01–6.04). Metal workshop workers who were exposed to more than 85 dB were 3.8 times more likely to develop prehypertension as compared to those who were exposed to less than 85 dB (AOR=3.8, 95% CI: 2.8–5.9). When compared to the study subjects with working experience between 1 and 5 years, those with 6 to 10 years of experience were 2.8 times more likely to have prehypertension (AOR=2.8, 95% CI, 1.98–5.97), and study participants with >10 years of work experience had a 4.8 times higher risk of developing prehypertension than those with 1–5 years of work experience (AOR=4.8, 95% CI; 2.8–7.75) (Table 2).
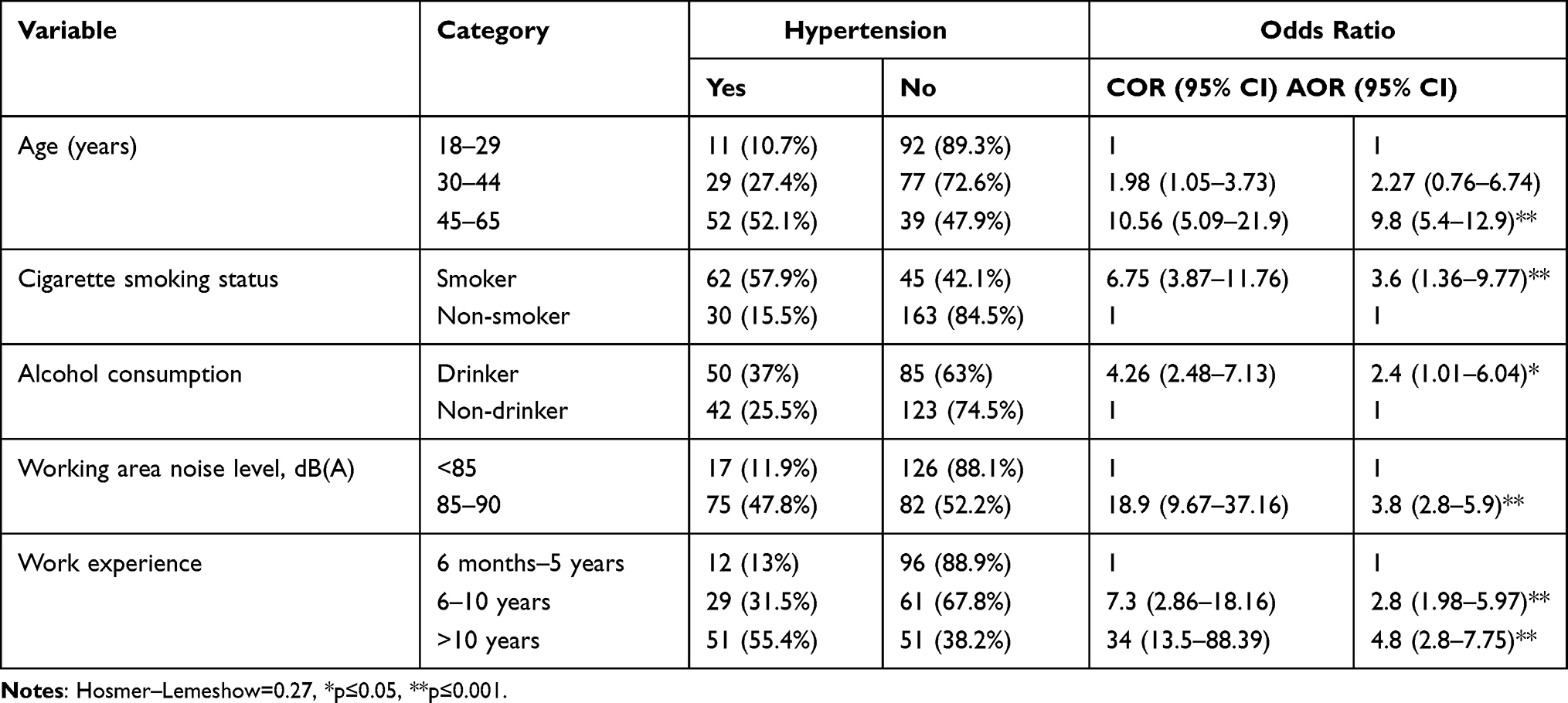 |
Table 2 Bivariable and Multivariable Logistic Regression Analysis of Noise-Induced Prehypertension Along with Explanatory Variables |
Discussion
Occupational noise exposure has been shown to increase the risk of elevated blood pressure; however, the association between occupational noise exposure and hypertension is controversial. To the best of our knowledge, very little is known about the prevalence and associated factors of occupational noise-induced pre-hypertension among metal manufacturing workers in in the world including Ethiopia. Thus, this study (the first of its kind in Ethiopia) tried to offer insight on the prevalence of occupational noise-induced prehypertension and the possible associated factors among metal workers in Gondar city administration.
In this study, the overall prevalence of occupational noise-induced pre-hypertension among our study participants was 27.7% (95% CI: 22.7–32.7) which is in line with a study in Pakistan (23.6%).11 However, the prevalence of occupational noise-induced pre-hypertension in our study was higher than a study in Sweden (22% and 8%) and lower than a study in China (52.6%).31 The discrepancies might be due to the differences in sample size, study design, cut-off point for sound level and socio-economic reasons.
In our study, age, exposure to noise sound ≥85 dB, work experience, alcohol consumption and cigarette smoking were significantly associated with noise-induced pre-hypertension in multivariable logistic regression (p ≤ 0.5).
In the present study, age was significantly associated with prehypertension. Study participants with advanced age groups had higher chance of developing prehypertension than those who were in the lower age groups. This finding is supported by reports in South Korea,34 Japan,30 and Germany.46 The plausible justification could be as a result of increased arterial stiffness, increased sensitivities in salt intake, lack of enough exercise (sedentary lifestyle), and decreased or disturbed sleep with advanced age.
Our study demonstrated that those smoker study participants had a higher chance of developing prehypertension than non-smokers. This finding is in agreement with studies in China,31,47 Iran,48 and the USA.49 This might be due to the fact that smoking triggers the action of sympathetic nervous system which in turn causes vasoconstriction and increases the frequency heart pump finally leads to elevated blood pressure.
The likelihood of prehypertension among metal workshop workers who were drinking alcohol was found higher than the non-drinkers. This result is similar with studies in China31,47 and the USA.50,51 The possible association between alcohol consumption and prehypertension might be due to release of cortisol and activation of angiotensin II through the renin–angiotensin–aldosterone system by alcohol consumption. Excess alcohol consumption can also increase the total body fluid which would raise blood flow through blood vessels and results in high frictional force.
The odds of having noise-induced prehypertension among metal factory workers who exposed to ≥85 dB working area noise level was 3.8 times higher among participants who exposed to less than 85 dB working area noise level. Similar findings were observed in studies in China21,28,34 and the USA.52 This might be due to the general stress theory, posits that noise affects the autonomic nervous system and the endocrine system, which in turn affects the homeostasis of the human organism. The other possible reason might be also due to an increase in the level of chemical substances like cortisol, adrenaline and noradrenaline in response to the stress caused by noise which in turn could result in peripheral vasoconstriction, increased heart rate, and increased arterial blood pressure.
When compared to the study subjects with working experience between 1 and 5 years, those with 6 to 10 years of experience were 2.8 times more likely to have prehypertension (AOR=2.8, 95% CI, 1.98–5.97), and study participants with >10 years of work experience had a 4.8 times higher risk of developing prehypertension than those with 1–5 years of work experience (AOR=4.8, 95% CI; 2.8–7.75). This finding is consistent with studies in China,47,53 Italy54 and the USA.12 The mechanism that underlies this association might be because of the release of stress hormones (such as adrenaline and cortisol) or stimulation of the sympathetic nervous system by prolonged exposure to noise.
Limitation of the Study
Since our study was based on cross-sectional study design, we could not establish a cause-and-effect relationship or determine the direction of causality.
Conclusion
In conclusion, our study demonstrated that the risk of developing occupational noise-induced pre-hypertension is increased on the exposure of high sound level. The chance of having noise-induced prehypertension was also found to be increased by prolonged years of work experience, advanced age, smoking cigarettes, and alcohol consumption. These results suggest that practical actions should be taken to lower the risk of noise-induced pre-hypertension driven by occupational noise exposure. We recommend metal factory workers to practice on minimizing occupational noises and be aware of their blood pressure levels on a regular basis. We also recommended these workers to avoid or reduce alcohol consumption and cigarette smoking in their life.
Abbreviations
BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; OR, odds ratio; AOD, adjusted odds ratio; COD, crude odds ratio; CI, confidence interval; dB(A), decibel A.
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable requests.
Acknowledgments
The authors thank all study participants and data collectors for their contributions to the success of this study. The authors also thank the University of Gondar for providing ethical clearance.
Author Contributions
All authors made a significant contribution to the paperwork and were actively involved in the conceptualization, methods, execution, acquisition of data, analysis, and interpretation. They also took part in drafting, critically reviewed the manuscript, gave final approval the final manuscript, have agreed on the journal to which the manuscript has been submitted, and agreed to be responsible for all aspects of the work.
Disclosure
All authors declare that they have no competing interests.
References
1. Shrestha A, Shiqi M. Occupational noise exposure in relation to hypertension: a cross-sectional study in the steel factory. Occup Med Health Aff. 2017;5(266):2. doi:10.4172/2329-6879.1000266
2. Concha-Barrientos M, Steenland K, Prüss-üstün A, et al. Occupational Noise: Assessing the Burden of Disease from Work-Related Hearing Impairment at National and Local Levels. World Health Organization; 2004.
3. Federal M. Development agency (FMSEDA) 2005. MSE strategy; 2006.
4. Melese M, Adugna DG, Mulat B, Adera A. Hearing loss and its associated factors among metal workshop workers at Gondar city, Northwest Ethiopia. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.919239
5. Kirchner DB, Evenson E, Dobie RA, et al. Occupational noise-induced hearing loss: ACOEM task force on occupational hearing loss. J Occupat Environ Med. 2012;54(1):106–108. doi:10.1097/JOM.0b013e318242677d
6. Dobie RA. The burdens of age-related and occupational noise-induced hearing loss in the United States. Ear Hear. 2008;29(4):565–577. doi:10.1097/AUD.0b013e31817349ec
7. Dehghan H, Bastami MT, Mahaki B. Evaluating combined effect of noise and heat on blood pressure changes among males in climatic chamber. J Educ Health Promot. 2017;6. doi:10.4103/jehp.jehp_107_15
8. Münzel T, Gori T, Babisch W, Basner M. Cardiovascular effects of environmental noise exposure. Eur Heart J. 2014;35(13):829–836. doi:10.1093/eurheartj/ehu030
9. Kalantary S, Dehghani A, Yekaninejad MS, Omidi L, Rahimzadeh M. The effects of occupational noise on blood pressure and heart rate of workers in an automotive parts industry. ARYA Atheroscler. 2015;11(4):215.
10. Münzel T, Sørensen M, Gori T, et al. Environmental stressors and cardio-metabolic disease: part II–mechanistic insights. Eur Heart J. 2017;38(8):557–564. doi:10.1093/eurheartj/ehw294
11. Nawaz SK, Hasnain S. Noise induced hypertension and prehypertension in Pakistan. Bosnian J Basic Med Sci. 2010;10(3):239. doi:10.17305/bjbms.2010.2694
12. Lusk SL, Hagerty BM, Gillespie B, Caruso CC. Chronic effects of workplace noise on blood pressure and heart rate. Archiv Environ Health. 2002;57(4):273–281. doi:10.1080/00039890209601410
13. Teixeira LR, Azevedo TM, Bortkiewicz A, et al. WHO/ILO work-related burden of disease and injury: protocol for systematic reviews of exposure to occupational noise and of the effect of exposure to occupational noise on cardiovascular disease. Environ Int. 2019;125:567–578. doi:10.1016/j.envint.2018.09.040
14. Babisch W. Stress hormones in the research on cardiovascular effects of noise. Noise Health. 2003;5(18):1.
15. Van Kempen EE, Kruize H, Boshuizen HC, Ameling CB, Staatsen BA, de Hollander AE. The association between noise exposure and blood pressure and ischemic heart disease: a meta-analysis. Environ Health Perspect. 2002;110(3):307–317. doi:10.1289/ehp.02110307
16. Münzel T, Sørensen M, Daiber A. Transportation noise pollution and cardiovascular disease. Nat Rev Cardiol. 2021;18(9):619–636. doi:10.1038/s41569-021-00532-5
17. Guo X, Zhang X, Guo L, et al. Association between pre-hypertension and cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. Curr Hypertens Rep. 2013;15(6):703–716. doi:10.1007/s11906-013-0403-y
18. Babisch W. The noise/stress concept, risk assessment and research needs. Noise Health. 2002;4(16):1.
19. Basner M, Babisch W, Davis A, et al. Auditory and non-auditory effects of noise on health. Lancet. 2014;383(9925):1325–1332. doi:10.1016/S0140-6736(13)61613-X
20. Petri D, Licitra G, Vigotti MA, Fredianelli L. Effects of exposure to road, railway, airport and recreational noise on blood pressure and hypertension. Int J Environ Res Public Health. 2021;18(17):9145. doi:10.3390/ijerph18179145
21. Ismaila SO, Odusote A. Noise exposure as a factor in the increase of blood pressure of workers in a sack manufacturing industry. Beni-Suef Univ J Basic Appl Sci. 2014;3(2):116–121. doi:10.1016/j.bjbas.2014.05.004
22. Attarchi M, Golabadi M, Labbafinejad Y, Mohammadi S. Combined effects of exposure to occupational noise and mixed organic solvents on blood pressure in car manufacturing company workers. Am J Ind Med. 2013;56(2):243–251. doi:10.1002/ajim.22086
23. Babisch W. Traffic noise and cardiovascular disease: epidemiological review and synthesis. Noise Health. 2000;2(8):9.
24. Ising H, Kruppa B. Health effects caused by noise: evidence in the literature from the past 25 years. Noise Health. 2004;6(22):5.
25. Chobanian AV, Bakris GL, Black HR. National High blood pressure education program committee: seventh report of the joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42:1206–1252. doi:10.1161/01.HYP.0000107251.49515.c2
26. Vasan RS, Larson MG, Leip EP, Kannel WB, Levy D. Assessment of frequency of progression to hypertension in non-hypertensive participants in the Framingham Heart Study: a cohort study. Lancet. 2001;358(9294):1682–1686. doi:10.1016/S0140-6736(01)06710-1
27. Skogstad M, Johannessen H, Tynes T, Mehlum I, Nordby K-C K-C, Lie A. Systematic review of the cardiovascular effects of occupational noise. Occup Med. 2016;66(1):10–16. doi:10.1093/occmed/kqv148
28. Chang T-Y, Jain R-M, Wang C-S, Chan -C-C. Effects of occupational noise exposure on blood pressure. J Occupat Environ Med. 2003;45(12):1289–1296. doi:10.1097/01.jom.0000100003.59731.3d
29. Chang T-Y, Hwang B-F, Liu C-S, et al. Occupational noise exposure and incident hypertension in men: a prospective cohort study. Am J Epidemiol. 2013;177(8):818–825. doi:10.1093/aje/kws300
30. Inoue M, Laskar M, Harada N. Cross-sectional study on occupational noise and hypertension in the workplace. Arch Environ Occup Health. 2005;60(2):106–110. doi:10.3200/AEOH.60.2.106-110
31. Wang D, Zhou M, Li W, et al. Occupational noise exposure and hypertension: the Dongfeng-Tongji cohort study. J Am Soc Hyperten. 2018;12(2):71–9. e5. doi:10.1016/j.jash.2017.11.001
32. Wallas AE, Eriksson C, Bonamy A-KE, et al. Traffic noise and other determinants of blood pressure in adolescence. Int J Hyg Environ Health. 2019;222(5):824–830. doi:10.1016/j.ijheh.2019.04.012
33. Said MA, El-Gohary OA. Effect of noise stress on cardiovascular system in adult male albino rat: implication of stress hormones, endothelial dysfunction and oxidative stress. Gen Physiol Biophys. 2016;35(3):371–377. doi:10.4149/gpb_2016003
34. Kim MG, Ahn Y-S, Jin Z. The relationship between occupational noise exposure and hypertension using nearest age-matching method in South Korea male workers. Cogent Engine. 2021;8(1):1909798. doi:10.1080/23311916.2021.1909798
35. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. hypertension. 2003;42(6):1206–1252.
36. Friedman JI, Wallenstein S, Moshier E, et al. The effects of hypertension and body mass index on cognition in schizophrenia. Am J Psychiatry. 2010;167(10):1232–1239. doi:10.1176/appi.ajp.2010.09091328
37. John W, Sakwari G, Mamuya SH. Noise exposure and self-reported hearing impairment among gas-fired electric plant workers in Tanzania. Ann Global Health. 2018;84(3):523. doi:10.29024/aogh.2305
38. Dawes P, Cruickshanks KJ, Moore DR, et al. Cigarette smoking, passive smoking, alcohol consumption, and hearing loss. J Assoc Res Otolaryngol. 2014;15(4):663–674. doi:10.1007/s10162-014-0461-0
39. World Health Organization. Environmental Noise Guidelines for the European Region: World Health Organization. Regional Office for Europe; 2018.
40. Zaw AK, Myat AM, Thandar M, et al. Assessment of noise exposure and hearing loss among workers in textile mill (Thamine), Myanmar: a cross-sectional study. Saf Health Work. 2020;11(2):199–206. doi:10.1016/j.shaw.2020.04.002
41. Van Kempen E, Babisch W. The quantitative relationship between road traffic noise and hypertension: a meta-analysis. J Hypertens. 2012;30(6):1075–1086. doi:10.1097/HJH.0b013e328352ac54
42. Pickering TG. Do we really need a new definition of hypertension? J Clin Hyperten. 2005;7(12):702. doi:10.1111/j.1524-6175.2005.04149.x
43. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289(19):2560–2571. doi:10.1001/jama.289.19.2560
44. Hwang L. A nested case control study on multiple risk factors for acute fatal cerebrovascular accident and coronary heart disease. Chin J Fam Med. 1997;7:121–130.
45. Association GAotWM. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Coll Dent. 2014;81(3):14–18.
46. Bolm-Audorff U, Hegewald J, Pretzsch A, Freiberg A, Nienhaus A, Seidler A. Occupational noise and hypertension risk: a systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(17):6281. doi:10.3390/ijerph17176281
47. Chen S, Ni Y, Zhang L, et al. Noise exposure in occupational setting associated with elevated blood pressure in China. BMC Public Health. 2017;17(1):1–7. doi:10.1186/s12889-017-4050-0
48. Attarchi M, Dehghan F, Safakhah F, Nojomi M, Mohammadi S. Effect of exposure to occupational noise and shift working on blood pressure in rubber manufacturing company workers. Ind Health. 2012;50(3):205–213. doi:10.2486/indhealth.MS1321
49. Rezk-Hanna M, Doering L, Robbins W, Sarna L, Elashoff RM, Victor RG. Acute effect of hookah smoking on arterial stiffness and wave reflections in adults aged 18 to 34 years of age. Am J Cardiol. 2018;122(5):905–909. doi:10.1016/j.amjcard.2018.05.033
50. Husain K, Ansari RA, Ferder L. Alcohol-induced hypertension: mechanism and prevention. World J Cardiol. 2014;6(5):245. doi:10.4330/wjc.v6.i5.245
51. Okojie OM, Javed F, Chiwome L. Hypertension and alcohol: a mechanistic approach. Cureus. 2020;12(8):e10086.
52. D’Souza J, Weuve J, Brook RD, Evans DA, Kaufman JD, Adar SD. Long-Term exposures to urban noise and blood pressure levels and control among older adults. Hypertension. 2021;78(6):1801–1808. doi:10.1161/HYPERTENSIONAHA.121.17708
53. Kuang D, Yu YY, Tu C, Zago AS. Bilateral high-frequency hearing loss is associated with elevated blood pressure and increased hypertension risk in occupational noise exposed workers. PLoS One. 2019;14(9):e0222135. doi:10.1371/journal.pone.0222135
54. Tomei F, De Sio S, Tomao E, et al. Occupational exposure to noise and hypertension in pilots. Int J Environ Health Res. 2005;15(2):99–106. doi:10.1080/09603120500061534
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.