")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Observation on China’s Strategies to Prevent the Resurgence of the COVID-19 Epidemic
Received 10 February 2021
Accepted for publication 27 April 2021
Published 18 May 2021 Volume 2021:14 Pages 2011—2019
DOI https://doi.org/10.2147/RMHP.S305413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Xiang Yu,1 Na Li,2,3 Yupeng Dong4
1School of Public Affairs, Fujian Jiangxia University, Fuzhou, Fujian Province, People’s Republic of China; 2School of Law, Ningbo University, Ningbo, Zhejiang Province, People’s Republic of China; 3School of the Belt and Road, Ningbo University, Ningbo, Zhejiang Province, People’s Republic of China; 4School of Media and Law, Ningbo Institute of Technology, Zhejiang University, Ningbo, Zhejiang Province, People’s Republic of China
Correspondence: Na Li
School of Law, Ningbo University, 818st Fenghua Road, Ningbo, 315211, People’s Republic of China
Email [email protected]
Abstract: After the first wave of the COVID-19 pandemic that began in early 2020 was brought under control, there have been some regional and small-scale cases of new infections in China. In order to prevent the resurgence of the epidemic, the Chinese government has continued the use of effective prevention and control measures in key epidemic areas. New prevention and control measures have also been developed based on the characteristics of the epidemic and the social habits of the Chinese people. The strategies applied in China include large-scale nucleic acid testing, travel health code management, and patient treatment based on a combination of Chinese and Western medicine. These measures can provide a reference point for the global public health system that is facing the pandemic. The article suggests that to prevent a pandemic, we must not only rely on vaccines and drugs, but also need to take actions and apply social measures to manage the risk of infectious diseases.
Keywords: risk management, COVID-19, virus test, health information, collaboration
Introduction
In January 2020, the novel coronavirus (COVID-19) spread nationwide in mainland China. After the Chinese government’s mobilization of infection control measures and medical effort, a state of zero new infections was achieved in China before summer 2020. This meant that the most dangerous phase of the epidemic had passed. However, COVID-19 did not go away in China. In the following weeks, new cases of infection were found in more than ten provinces, some provinces experienced clusters of cases, while some Chinese students studying abroad and business people returning from abroad also tested positive for the virus. From the summer to the winter of 2020, China put in place various measures to suppress the resurgence of the epidemic, and used this relatively safe time to restore the economy and develop vaccines. This article mainly discusses the role of nucleic acid testing, the travel health code, and drugs in reducing the number of new COVID-19 cases in China.
Methods and Materials
This study focuses on newly reported local COVID-19 monitoring and prevention measures in mainland China from June 2020. The data did not include cases in Hong Kong, Macau, Taiwan of China. Cases and patient data mainly came from official announcements and press conferences issued by the Chinese Central Government and provincial health commissions, statistical data from the China National Medical Products Administration, expert opinions from the China Centers for Disease Control and Prevention, public announcements issued by pharmaceutical companies and recent medical literatures. In the research design, we were thinking about whether some of the measures mentioned in the manuscript were effective and how long the effect can last. Our preliminary view was that the manuscript cannot give a relatively confident conclusion. It was more about providing perspectives or clues so that subsequent research can be targeted. Therefore, we had adopted a combination of focus research and comparative research methods. Focus research was to summarize and present the key factors of the event, such as the root and environment, goals and countermeasures, output and impact, etc., and process the information collected and stated facts in the manuscript into evidence in the research process. Comparative analysis was used to rank and compare different measures, ranking them in terms of time context and importance. Of course, this comparison was not on the same level, it was limited in terms of time, region, and medical technology, and because there were still more cognitive difficulties with the novel coronavirus, the purpose of our comparison was to try whether a certain solution is feasible, Instead of testing the following measures.
Results
Epidemic Trends in the China Mainland
The China mainland experienced a high-risk period of concentrated outbreaks of COVID-19 cases from January to March 2020.1 Starting from April 2020, China entered a low-infection phase, during which the most critical and difficult task was to stop the resurgence of the epidemic.2 During this period, there were small clusters of cases in Beijing, Xinjiang, Liaoning, Shandong, and Inner Mongolia Province in mainland China, and sporadic cases were also found in Shanghai, Tianjin, Anhui, Guangdong, and Sichuan Province. The areas with a high number of confirmed cases were as follows. (1) From June 11 to July 5, 2020, Beijing reported 335 confirmed cases and 31 asymptomatic infections. The main outbreak area was an agricultural wholesale market. (2) From July 16 to August 15, 2020, Xinjiang reported 826 confirmed cases and 127 asymptomatic infections. The cases were mainly in Urumqi and surrounding areas. From October 27 to November 5, 2020, 137 cases of asymptomatic infections were detected in factory workers and their surroundings in Kashgar, Xinjiang, and 78 confirmed cases. (3) From July 23 to August 5, 2020, Dalian reported 68 confirmed cases and 32 asymptomatic infections. The first infections were reported in employees of a seafood factory. (4) From October 12 to October 14, 2020, a total of 13 confirmed cases were reported in Qingdao. The initial infected individuals were also engaged in the processing and transportation of frozen seafood. (5) From November 25 to December 9, 2020, 26 new cases were detected in the Inner Mongolia Autonomous Region. The cases were mainly in Manzhouli, the busiest land port in the North of China.3 The transmission chain of the epidemic in these areas was relatively clear,4 the speed of diagnosis was relatively quick, and the Chinese health agencies took action relatively quickly to stop further transmission.5 (Figure 1)
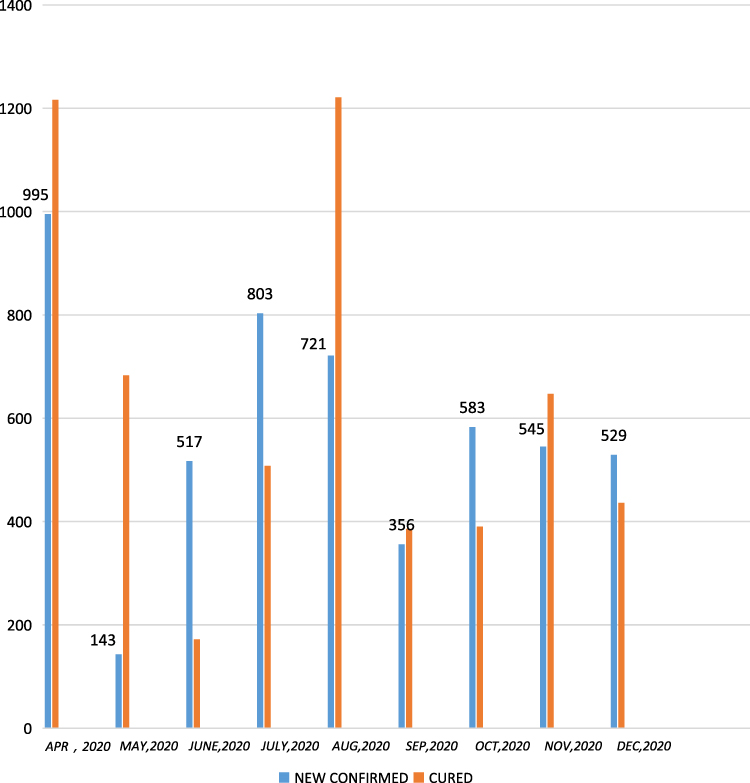 |
Figure 1 Trends of COVID-19 Infections in China Mainland from April 2020 to December 2020. |
From January 2021, with the arrival of the severe cold season, the number of confirmed infections in northern China increased significantly.6 A series of transmission incidents caused by one patient occurred in Jilin, Heilongjiang, and Liaoning Province in northeastern China, within which there were 522 confirmed cases in Heilongjiang Province and 425 cases in Jilin Province. There were also confirmed cases in Shijiazhuang City, Hebei Province in the area adjacent to the airport; the total number of infections increased to 866 cases. Compared with the cases in the previous few months, this wave of infection had more confirmed patients and faster spread.7 (Table 1) These places restarted community lockdown measures similar to those in Wuhan.
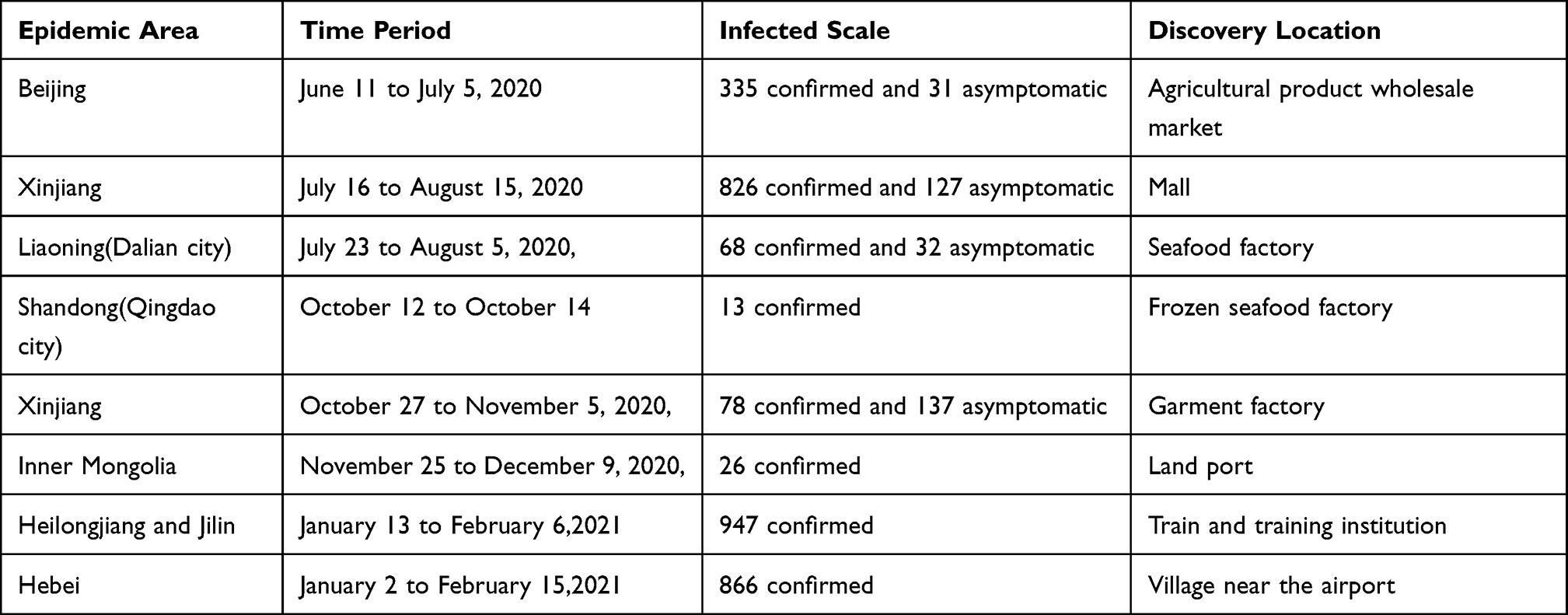 |
Table 1 Regional Clusters COVID-19 Cases in China Mainland Since June 2020 |
The Emergency Response Strategy Was to Implement Nucleic Acid Testing for All Residents
After a confirmed case was found, the guidelines developed by the Chinese Center for Disease Control and Prevention required analysis of the individual’s movements over the past 15 days, isolation and testing of their family members, colleagues, and close contacts, and disinfection of the environment.8 In these new outbreaks, some local governments in China believed that testing of close contacts was insufficient. Instead, they hoped to find all infected individuals and the only way to do this was to test everyone in the city.9 The first full-staff nucleic acid test was conducted in Wuhan. After successfully treating more than 50,000 patients, Wuhan decided to rule out the hidden coronavirus risk in the city. Starting on May 11, 2021, Wuhan completed the nucleic acid testing of nearly 10 million people over 10 days. Three hundred asymptomatic infections were found.10 Since then, Beijing has implemented large-scale centralized nucleic acid testing on more than 12 million people; 174 people tested positive.11 In October 2020, Qingdao conducted nucleic acid testing on 9 million citizens over 5 days, and no positive results were found.12 At the same time, the total number of people tested in Kashgar, Xinjiang reached 4.74 million, and 183 people tested positive.13 In Shijiazhuang City, the first round of nucleic acid testing for all residents was conducted from January 6 to January 8, 2021. A total of 10 million people were tested with 354 people testing positive. The second round of nucleic acid testing was completed on January 14, 2021, with 247 positive cases. From January 20 to 22, 2021, Shijiazhuang City conducted the third round of nucleic acid testing with a total of 30 positive samples being detected. A total of 631 positive samples were “screened” in the three rounds of full nucleic acid testing.14 Tonghua City in Jilin Province also conducted four rounds of full-staff nucleic acid tests.
From 360,000 Samples, 108 Positive Cases Were Confirmed15
In order to complete several million nucleic acid tests over a short period of time, the Chinese health department adopted three main methods to improve efficiency. The first method was to map a grid at the level of region and community to aid test notification and queuing. Samples were taken and collected locally, and then sent to the laboratory.16 The second method was a mixed test method. Usually the nasopharyngeal swab samples of ten subjects were mixed together and sent for testing.17 If all the samples were negative, it meant that the subjects were healthy. If suspicious markers were found in the tests, retests or separate tests for each subject would be carried out, which can greatly increase the test speed.18 The third method involved building temporary testing laboratories. A medical technology company from Shanghai had developed an on-board nucleic acid testing laboratory system, this kind of laboratory adopt the size of a standard container. The interior of the laboratory was divided into three independent sections: reagent preparation room, sample processing room and nucleic acid detection room. It can be transported by container trucks or placed on trains or freighters. Sometimes it also can be split into three independent experimental functional areas, and installs them in three commercial vehicles, and the testing can be carried out at any time.19 Another China Pharmaceutical Company invented an air cabin laboratory. An air cabin has an area of 4 square meters before being inflated, increasing to 70 square meters after inflation. The inflation process takes 50 minutes. The air cabin lab is equipped with an automated nucleic acid detector, which can automatically complete operations such as opening test kits, adding reagents, scanning codes, and entering information without manual assistance. A laboratory with 12 air cabins can process up to 1 million samples per day. In terms of safety, the air cabin is equipped with a fresh air system and high-efficiency filtration system to ensure cleanliness. The air cabin also uses one-way sample collection and a double-door locking mode to prevent virus leakage.20
The Routine Prevention Strategy Was to Implement a Travel Health Code
On January 20, 2020, the Chinese government officially classified COVID-19 as a statutory infectious disease and launched a Level 1 public health emergency response. Many air, train, and coach transportation services were suspended nationwide. During the pandemic, the number of business passengers in China decreased significantly. Due to health concerns and the closure of tourist attractions, the flow of tourist passengers in effect stopped.21 For the remaining few travelers, whether they used civil aviation, railway or road transportation, they had to accept body temperature testing and health surveys. During a journey, whenever people passed a city or a facility, their temperature had to be tested and they must fill in a declaration form.
From late March 2020, China’s epidemic began to lessen significantly, and the government and transportation companies began to consider restoring normal traffic in order to promote the economic recovery. They all realized that China had a large population and a variety of travel methods.22 It was unreliable and very time-consuming to rely on manual health checks. Some local governments submitted orders to IT companies to develop mobile phone applications. This was China’s “Travel Health Code”.(Figure 2)
 |
Figure 2 Sample of travel health code of China Mainland. |
The travel health code includes basic information on citizens, their health information and travel information. Scanning the health code at checkpoints allows information to be checked: Basic information includes name, age, ID number, home address, work, family information, owned vehicles and other transportation. Health information includes citizens’ recent body temperature record, medical treatment records in hospitals, and purchase records in pharmacies. Travel information is based on the user scanning travel health code, includes information on individuals’ travel trajectories, such as the malls they visited, restaurants they ate in, and the flights they have taken.23
The travel health code is divided into three colors: green, red, and yellow. Green indicates that the citizen and their cohabiting family members recently have had a normal body temperature, no hospital records of treatment of respiratory diseases, and have not visited areas with a COVID-19 high-risk level. Yellow indicates that the citizen has recently visited some risky areas or places with positive cases of COVID-19; has had a certain degree of contact history with people infected with COVID-19; or the citizen has recently experienced some respiratory-related diseases. Red is the highest alert level, indicating that the citizen comes from the epidemic-center area, or has experienced symptoms such as fever in the last 14 days. It can also indicate that a citizen and their family have been identified as close contacts of COVID-19 patients and needed to isolate and be observed. According to the color of the health code, the transportation department has the right to accept or reject passengers. Passengers whose travel health code is red or yellow are usually rejected, while passengers whose travel health code is green are allowed to travel.24
The local government supported the travel health code because the government provided all the citizen registration information managed by the police station, the hospital diagnosis and treatment information managed by the Health Commission, the citizen medical insurance information managed by the Medical Insurance Bureau, and the ticket purchase information and travel information of the transportation department. The developers of the travel health code programs designed the data structures, data element attributes, and data management requirements. The government also required each public service agency to upload information records to the database after scanning the travel health code to determine citizen’s travel trajectory map.25
Travel health codes were welcomed in some provinces, but codes in various regions were developed independently. There were problems with mutual recognition and information sharing. The Chinese State Council began to take two actions in response. The first was to require local governments to manage the travel health code: they could outsource data maintenance to private enterprise, but private enterprise was not allowed to develop the travel health code separately. In order to ensure that the content of the travel health code was accurate, the National Health Commission had successively consolidated the information of all confirmed and suspected patients with COVID-19, also the information of possible close contacts and the epidemic risk level of each administrative region, and information on entry personnel and fellow travelers. The data is provided to the travel health code systems of various local governments so that they can conduct investigations and comparisons when issuing travel health codes. The second was to require the Chinese National Standardization Commission to formulate a National Standard to unify the format, content, and application interface of travel health code collection information in various regions. The national standard of travel health code consists of reference model, data format and application interface. On the whole, the reference model is a framework standard, which focuses on the technical model of “ Travel Health Code” application system and mutual recognition between systems; the data format standardizes the personal health information data, focusing on the data “raw material” level; the application interface can be regarded as the operation instruction manual to realize the mutual recognition of system docking under the framework model. The ultimate aim was to achieve a “unified coding system, unified presentation mode, and unified data content”.
A Feasible Treatment Strategy for Confirmed Patients is the Combination of Chinese and Western Medicine
The causative pathogen of COVID-19 was a highly infectious enveloped positive-strand RNA virus.26 It binds to the host receptor through the S protein on its surface, thereby mediating membrane fusion and virus entry.27 The virus preferentially infects cells of the respiratory tract, and also enters the lungs, pharynx, heart, liver, brain, kidneys, and digestive system organs.28
The main protease or RNA of the coronavirus is dependent on the RNA polymerase nsp12.29 Therefore, scientists used these characteristics to find suitable drugs.30 On the one hand, the China Health Commission launched the “COVID-19 Diagnosis and Treatment Plan (Trial Seventh Edition)” and “COVID-19 Severe and Critical Case Diagnosis and Treatment Plan (Trial Second Edition)”, which recommended treatment with interferons, lopinavir, ritonavir, ribavirin, chloroquine phosphate, arbidol, etc. These antiviral drugs are already on the market. In addition to the above drugs, Chinese hospitals also used hormones, heparin, high-dose vitamin C and thymosin in clinical treatment, and added the traditional Chinese medicine “Qing fei pai du Decoction”.31 On the other hand, at the beginning of the outbreak, China, like other countries in the world, had great hope in the new polymerase drug remdesivir. Remdesivir is a nucleoside analog developed by Gilead, initially used in treatment against highly lethal infectious diseases such as Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV),Middle East Respiratory Syndrome Coronavirus (MERS-CoV), and Ebola virus.32
After the outbreak of COVID-19, remdesivir was first used in clinical treatment in the United States and France, and was also introduced into China.33 In February 2020, the Chinese National Medical Products Administration passed special approval to allow remdesivir to be used in two independent Phase III clinical trials in several hospitals in Wuhan, China. One was titled “Randomized controlled trials for severe COVID-19 patients”, and the other was “Randomized controlled trials for mild and moderate COVID-19 patients”.34 Gilead provided remdesivir injections in the clinical trials free of charge and provided support for the design and development of the study. The start time of the “Randomized controlled trials for severe COVID-19 patients” was February 6, 2020; it was expected to be used on 452 cases, and the completion date was May 1, 2020. The start time of the “Randomized controlled trials for mild and moderate COVID-19 patients” was February 5, 2020, it was expected to be used on 308 cases, and the completion date was April 7, 2020.35 However, from the end of March 2020, the number of people diagnosed with COVID-19 in China dropped to less than 100 per day, and the number of critically ill patients and deaths also decreased significantly. This had two effects: one was that the number of patients who could participate in clinical trials reduced, and the second was that the demand for COVID-19 special drugs decreased.36
According to disclosure from the Chinese Academy of Medical Sciences, the two remdesivir clinical trials mentioned above were forced to be terminated on April 15, 2020, 15–20 days sooner than the original planned trial time. The reason was that appropriate test samples could not be obtained. In the two trials, the experimental data for the critically ill patients were more-or-less collected completely, and the test results were publicly disclosed on April 29, 2020.Research showed that from February 6 to March 12, 2020, a total of 237 severe patients received medication. The 28-day mortality proportions within the experimental group and control group were 14% and 13%, respectively. The proportion of subjects experiencing side effects in the two groups were 66% and 64%, respectively; these figures were not statistically significant. For patients treated with remdesivir, the clinical improvement time and invasive mechanical ventilation time were shortened within 10 days of symptom onset, and the risk rate (HR) of clinical symptom improvement was 1.23. Clinical trials in China have concluded that the use of remdesivir has little to do with the improvement of clinical symptoms.37 These trials neither confirm that remdesivir is a special drug for COVID-19 nor that remdesivir is completely ineffective.
Discussion
The Strong Transmission Capacity of the Novel Coronavirus and the Reason for the Resurgence of the Epidemic in China
China paid a heavy price in the early stages of the pandemic. Therefore, when the epidemic was effectively under control in China, the Chinese government and people remained very cautious. For example, when resuming business, transportation, education, medical and other social activities, the government still required people to wear masks. Patients with cold, cough, and fever symptoms were required to take a nucleic acid test, and the aforementioned travel health code was mandatory.38 However, the coronavirus remained a threat in China. Based on the analysis of disease control experts, the main threats to newly confirmed patients were as follows. First, the vast majority of people paid attention to taking protective measures during the first wave of the epidemic so that they did not become infected by the virus.39 This also resulted in many people having no COVID-19 antibodies, meaning they had not produced an immune barrier against infection.40 Second, with the worldwide spread of COVID-19, the virus was detected in China in both immigrants and some imported cold chain foods, meaning the virus cross-spread through the two channels of “human-to-human” and “material-to-human”.41 Some people who are engaged in food processing and transportation, driving vehicles, catering and hotel services, as well as medical staff, will become infected if they display minor negligence in terms of protective measures.42 Third, in winter weather conditions, many places in China have adopted measures such as airtight doors and windows, heating, and so on, making COVID-19 easier to spread in a relatively closed environment.43 In this situation, although China adopted a series of high-strength prevention and control measures, it was still difficult to eliminate the virus completely.
Which Was More Effective: Medical or Non-Medical Strategies?
COVID-19 was sweeping through the world at a very fast rate, and no country could avoid the threat. Every country very much hopes to control the epidemic as soon as possible, and even hope to end the epidemic. Therefore, they have adopted various measures, China is no exception. We analyzed some of the measures that were seemed to prevent the epidemic from rebounding. We try to be as clear as possible that the effects of which measures can be fully confirmed? Which measures should take time to observe the effect? Which measures are currently difficult to confirm? In terms of reducing the chaos and loss of life inflicted by the virus, the conventional method was to rely on medicine.44 On the one hand, the medical community scaled up the comparison and research of broader-spectrum antiviral drugs, and developed faster and more accurate nucleic acid detection methods.45 On the other hand, many people placed hope in the development and marketing of vaccines. China made remarkable progress in the production and testing capabilities of nucleic acid testing reagents, and played an important role in quickly detecting infected patients and preventing the spread of the epidemic.46 The Chinese government has also recently decided to provide free vaccines to residents. However, the medical community has not found a specific drug to combat this coronavirus, and effective treatment methods are still being explored. Besides, China has a large population and cannot rely on large-scale and repeated nucleic acid tests to diagnose cases. If vaccination is to be implemented, it will take a long time and a huge amount of money. The effect of antibodies in the body and the duration of the antibodies is still unknown, and the ability of vaccines to resist virus mutations also needs to be studied.47 In order to safeguard life and health, the government has no further options left to explore. It can only rely on unconventional and non-medical methods to change people’s lives and social interactions. Such as travel of residents in the epidemic area remains restricted and they are not allowed to gather, some commercial and educational activities will be suspended, some close contacts will be quarantined for observation, and life in areas free of the epidemic will also be affected until government officials and disease control experts agree that the risk has been minimized. These measures were very different from previous medical measures when other infectious diseases broke out. It was made by the Chinese government under the urgent situation of the epidemic. At the time of choice, it was not clear evidence whether these measures will produce effects. The choice can only be made based on “fast”, “full coverage”, and “operability” as the criteria. However, the implementation of non-medical measures requires both the strong will of the government and the cooperation of residents.48 In order to implement such prevention and control measures, China urgently amended the “Law on the Prevention and Control of Infectious Diseases”, which enhanced the legal consequences of non-compliance with the government’s order for epidemic prevention. However, how long such non-medical measures should last, how to reduce management costs and reduce the inconvenience to life, and other issues need more extensive discussion.49
Conclusion
The COVID-19 pandemic would most likely not end in the short term, it is not just a disease but represents a challenge to the public health system and public life around the world. In this manuscript, we used China as an example to discuss what we can do in response to wave after wave of threats. While implementing medical treatment, China had also adopted many non-medical measures, and it was obvious that these non-medical measures were mainly applied to healthy people. We believed these non-medical measures cannot directly cure the patient, but they can protect the people from the virus and indirectly save lives, while this effect needed to be confirmed by more scientific evidence. However, the novel coronavirus would not leave us enough time to wait for the result of this proof. Every person must realize that both medical and non-medical methods can play a role in their respective fields of expertise, when medicine and science cannot clearly help us mitigate the risk, we must learn to change the way of life, such as communication, travel and home life. In the crisis, residents, communities, and the government should unite as much as possible, especially the majority of residents should place more concern on public affairs, understand and cooperate with the health authorities in this extraordinary period, and temporarily put aside some personal interests. Moreover, the government should use its authority and resources to protect the public need for hygiene.
Acknowledgments
This research was supported by the Fujian Province Social Science Fund, China (Grant No. FJ2018B034) and KC Wong Magna Fund in Ningbo University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cheng ZJ, Shan J. 2019 Novel coronavirus: where we are and what we know. Infection. 2020;48:155–163. doi:10.1007/s15010-020-01401-y
2. Jones DS. History in a crisis — lessons for Covid-19. N Engl J Med. 2020;382:1681–1683. doi:10.1056/NEJMp2004361
3. National Health Commission of the People's Republic of China. Daily epidemic notification. Available from: http://www.nhc.gov.cn/xcs/yqtb/list_gzbd.shtml.
4. Chinese National Health Commission. Diagnosis and treatment of COVID-19 pneumonia. Available from: http://www.nhc.gov.cn/yzygj/s7653p/202001/4294563ed35b43209b31739bd0785e67.shtml.
5. Chinese Center For Disease Prevention And Control. Epidemic update and risk assessment of COVID-19. Available from: http://www.chinacdc.cn/jkzt/crb/zl/szkb_11803/.
6. Horton R. Offline: the second wave. Lancet. 2020;395(10242):1960. doi:10.1016/S0140-6736(20)31451-3
7. Lee EC, Wada NI, Grabowski MK, et al. The engines of SARSCoV-2 spread. Science. 2020;370(6515):406–407. doi:10.1126/science.abd8755
8. Wang L, Shi Y, Xiao T, et al. Chinese expert consensus on the perinatal and neonatal management for the prevention and control of the 2019 novel coronavirus infection. Ann Transl Med. 2020;8(3):47. doi:10.21037/atm.2020.02.20
9. She J, Jiang J, Ye L, et al. 2019 novel coronavirus of pneumonia in Wuhan, China: emerging attack and management strategies. Clin Transl Med. 2020;9(1):19. doi:10.1186/s40169-020-00271-z
10. Chinese State Council Information Office. Wuhan launches nucleic acid testing for all residents. Available from: http://www.scio.gov.cn/xwfbh/xwbfbh/wqfbh/42311/43043/index.htm.
11. Xinhua News Agency. Build a strong line of defense to protect the city and protect life-Beijing launches large-scale nucleic acid testing. Available from: http://www.gov.cn/xinwen/2020-06/25/content_5521835.htm.
12. Qingdao Daily. How to complete the nucleic acid test for all residents in Qingdao with a population of tens of millions in 5 days. Available from: http://www.dailyqd.com/3g/html/2020-10/17/content_293423.htm.
13. Xinjiang Daily. Complete nucleic acid testing for all residents in Kashgar. Available from: http://news.ts.cn/system/2020/10/28/036481078.shtml.
14. Renmin Net. Go straight to the scene: Shijiazhuang, Hebei Province, started nucleic acid testing for all employees in the early morning of the 6th. Available from: http://health.people.com.cn/n1/2021/0106/c14739-31991097.html.
15. Jilin Daily. Tonghua launches four rounds of nucleic acid testing for all residents. Available from: http://www.dajilin.com/quanlifangkongxinguanfeiyanyiqing/2021-01-30/211103.html.
16. Wu Z, Mc Googan JM. Characteristics and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
17. Hope MD, Raptis CA, Henry TS. Chest computed tomography for detection of coronavirus disease 2019 (COVID-19): don´t rush the science. Ann Intern Med. 2020;173:147–148. doi:10.7326/M20-1382
18. Yokota I, Shane PY, Okada K, et al. Mass screening of asymptomatic persons for SARS-CoV-2 using saliva. Clin Infect Dis. 2020:ciaa1388. doi:10.1093/cid/ciaa1388
19. Xinhua News. Shanghai mobile nucleic acid testing laboratory was officially delivered. Available from: http://m.xinhuanet.com/sh/2020-08/08/c_139274452.htm.
20. Xinhua News. Beijing’s first air cabin “Huoyan” nucleic acid testing laboratory officially opened. Available from: http://www.bj.xinhuanet.com/2020-06/24/c_1126157683.htm.
21. Yu X, Li N. Understanding the beginning of a pandemic: China’s response to the emergence of COVID-19. J Infect Public Heal. 2021;14:347–352. doi:10.1016/j.jiph.2020.12.024
22. Bedford J, Enria D, Giesecke J, et al. Living with the COVID-19 pandemic: act now with the tools we have. Lancet. 2020;396(10259):1314–1316. doi:10.1016/S0140-6736(20)32117-6
23. Guangming Daily. Health code: let the resume work and labor press the shortcut key. Available from: http://www.gov.cn/xinwen/2020-03/22/content_5494086.htm.
24. China government website. National standard of personal health information code was issued. Available from: http://www.gov.cn/xinwen/2020-05/02/content_5508190.htm.
25. Renmin Daily. In most areas of the country, health code has been able to achieve “one code access”. Available from: http://health.people.com.cn/n1/2020/0405/c14739-31662189.html.
26. Cohen MS, Corey L. Combination prevention for COVID-19. Science. 2020;368:551. doi:10.1126/science.abc5798
27. World Health Organization. Transmission of SARS-CoV-2: implications for infection prevention precautions. Available from: http://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions.on.3.August.2020.
28. Vardhana SA, Wolchok JD. The many faces of the anti-COVID immune response. J Exp Med. 2020;217:e20200678. doi:10.1084/jem.20200678
29. Bailey AL, Diamond MS. A crisp(r) new perspective on SARS-CoV-2 biology. Cell. 2021;184(1):15–17. doi:10.1016/j.cell.2020.12.003
30. Daniloski Z, Jordan TX, Wessels HH, et al. Identification of required host factors for SARS-CoV-2 infection in human cells. Cell. 2021;184(1):92–105.e16. doi:10.1016/j.cell.2020.10.030
31. Chinese Preventive Medicine Association. An update on the epidemiological characteristics of novel coronavirus pneumonia (COVID-19). Zhong Hua Liu Xing Bing Xue Za Zhi. 2020;41(2):139–144. doi:10.3760/cma.j.issn.0254-6450.2020.02.002
32. Sarpatwari A, Kaltenboeck A, Kesselheim AS, et al. Missed opportunities on emergency remdesivir use. JAMA. 2020;324(4):331–332. doi:10.1001/jama.2020.11932
33. Clark A, Jit M, Warren-Gash C, et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modelling study. Lancet Glob Health. 2020;8:e1003–e1017. doi:10.1016/S2214-109X(20)30264-3
34. Oran DP, Topol EJ. Prevalence of asymptomatic SARS-CoV-2 infection: a narrative review. Ann Intern Med. 2020;173:362–367. doi:10.7326/M20-3012
35. Yu X, Li N, Li YY. Were it business opportunities or hidden risks: observations on clinical trials and marketing authorizations of Gilead Science’s remdesivir in China. Die Pharmazie. 2020;75:407–410. doi:10.1691/ph.2020.0549
36. Daniloski Z, Jordan TX, Wessels HH, et al. Identification of required host factors for SARS-CoV-2 infection in human cells. Cell. 2020;184(1):92–105.e16. doi:10.1016/j.cell.2020.10.030
37. Wang Y, Zhang D, Du G, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2020;395:1569–1578. doi:10.1016/S0140-6736(20)31022-9
38. Subbarao K, Mahanty S. Respiratory virus infections: understanding COVID-19. Immunity. 2020;52(6):905–909. doi:10.1016/j.immuni.2020.05.004
39. Rubin EJ, Baden LR, Morrissey S. A new monoclonal antibody for COVID-19. N Engl J Med. 2020;383:e117. doi:10.1056/NEJMe2032410
40. Long QX, Tang XJ, Shi QL, et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat Med. 2020;26:1200–1204. doi:10.1038/s41591-020-0965-6
41. Quer G, Radin JM, Gadaleta M, et al. Wearable sensor data and self-reported symptoms for COVID-19 detection. Nat Med. 2020;10:1–5. doi:10.1038/s41591-020-1123-x
42. Wang S, Qiu Z, Hou Y, et al. Axl is a candidate receptor for sars-cov-2 that promotes infection of pulmonary and bronchial epithelial cells. Cell Res. 2021;31(2):1–15. doi:10.1038/s41422-020-00460-y
43. Mallapaty S. Why COVID outbreaks look set to worsen this winter. Nature. 2020;586(7831):653. doi:10.1038/d41586-020-02972-4
44. Mc Aloon C, Collins Á, Hunt K, et al. Incubation period of COVID-19: a rapid systematic review and meta-analysis of observational research. BMJ Open. 2020;10:e039652. doi:10.1136/bmjopen-2020-039652
45. Furukawa NW, Brooks JT, Sobel J. Evidence supporting transmission of severe acute respiratory syndrome coronavirus 2 while presymptomatic or asymptomatic. Emerg Infect Dis. 2020;26. doi:10.3201/eid2607.201595
46. Schwartz JL. Evaluating and deploying COVID-19 vaccines—the importance of transparency, scientific integrity, and public trust. N Engl J Med. 2020;383:1703–1705. doi:10.1056/NEJMp2026393
47. Hodgson SH, Mansatta K, Mallett G, et al. What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect Dis. 2020;21(2):e26–e35. doi:10.1016/S1473-3099(20)30773-8
48. Doshi P. Will COVID-19 vaccines save lives? Current trials aren’t designed to tell us. BMJ. 2020;371:m4037. doi:10.1136/bmj.m4037
49. Bell BP, Romero JR, Lee GM. Scientific and ethical principles underlying recommendations from the advisory committee on immunization practices for COVID-19 vaccination implementation. JAMA. 2020;324(20):2025–2026. doi:10.1001/jama.2020.20847
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.