Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Nutritional and Physical Prehabilitation in Elective Orthopedic Surgery: Rationale and Proposal for Implementation
Authors Briguglio M ![]() , Wainwright TW
, Wainwright TW ![]()
Received 30 September 2021
Accepted for publication 10 December 2021
Published 6 January 2022 Volume 2022:18 Pages 21—30
DOI https://doi.org/10.2147/TCRM.S341953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Matteo Briguglio,1 Thomas W Wainwright2,3
1IRCCS Orthopedic Institute Galeazzi, Scientific Direction, Milan, Italy; 2Orthopaedic Research Institute, Bournemouth University, Bournemouth, UK; 3Physiotherapy Department, University Hospitals Dorset NHS Foundation Trust, Bournemouth, UK
Correspondence: Matteo Briguglio
IRCCS Orthopedic Institute Galeazzi, Scientific Direction, Via Riccardo Galeazzi 4, Milan, 20161, Italy
Tel +39 02 66214978
Email [email protected]
Abstract: In the past, good food and exercise were not considered effective interventions to promote recovery in orthopedic surgery, and prolonged bed rest with not many calories has been deemed sufficient for the proper health restoration until the end of the nineteenth century. The advancement of scientific knowledge proved just the opposite, thus pushing health professionals to sustain the nutritional status and physical fitness of surgical patients. Nevertheless, the impoverishment of lifestyles and the lengthening of life expectancy have invariably contrasted the strength of constitution, giving rise to two of the most hazardous conditions for orthopedic patients: malnutrition and sarcopenia, often hiding nutrient deficits and poor body composition. These conditions are known to be negative prognostic factors in several areas of major surgery, including hip replacement, knee replacement, and spine surgery. Scoring systems to screen for malnutrition and physical inabilities exist, but disciplined management of the derived risks remains untested, potentially hindering the implementation of research findings into practice. A methodical approach of preoperative analysis, critical monitoring, and risk correction before surgery could lead to a substantial improvement of the prognosis while warranting the safety of patients and the efficiency of enhanced recovery after surgery pathways. The aim of this article is to discuss from a dietetic and exercise perspective the ideal nutritional and physical prehabilitation to lay the foundations for designing the appropriate integration of dietitians and physiotherapists in a preoperative enhanced recovery pathway. This methodical analysis could effectively calculate the patient’s risks, detect the best choices for resolving the risk, underline the ignored aspects of perioperative care, and represent a concrete means to integrate novel discoveries.
Keywords: hip replacement, knee replacement, malnutrition, sarcopenia, enhanced recovery after surgery, quality of health care
Introduction
The importance of maintaining a good nutritional status and physical ability for proper health restoration after orthopedic surgery has been broadly acknowledged. The inefficiency of the muscular system, nutrient deficits, the excess of body fat or being underweight are known to be a common burden for older patients undergoing orthopedic surgery,1,2 with poor nutritional and physical status both being associated with worse outcomes after hip,3,4 knee,5,6 and spine surgery.7,8 Hospitals have been consequently pushed to incorporate viable methods of preoperative nutritional and physical risk management in the field of elective surgery as several weeks may pass between the day of planning and the day of admission. Optimization plans for major orthopedic surgery exist9,10 together with the knowledge that fragile patients may have the most to gain from these multimodal approaches.11 However, it is a common belief that the rush to design these holistic approaches came at the expense of precision medicine interventions, with single disciplines of nutritional and physical supports not being appropriately planned, tested, or evidenced.12–14 Several scoring systems to identify malnutritional statuses or physical inabilities are in fact used, but how does this actually change practice? What corrective and monitoring path should the patient follow in order to reduce the nutrition-related and physical-related risks of postoperative complications? There is the need for a way of effectively controlling nutrition-related and physical-related hazards to look at whether planning a nutritional and physical prehabilitation will actually result in better outcomes. It is therefore necessary to refer to a methodical approach of risk observation and management that is schematic (essential but not limited), detailed (leaving nothing to chance), and inclusive (broad adaptable spectrum).15 The Hazard Analysis and Critical Control Points (HACCP) system could provide the framework to define an effective optimization protocol in preparation for surgery, accounting for all the variables involved. This safety control system was pioneered by the National Aeronautics and Space Administration of the United States for astronauts’ food during early space flights,16 and outlines all the set of procedures to follow to keep under control microbiological, chemical, or physical contaminations.17 The goal of this perspective article is not to propose nutritional or exercise recommendations. We aim to present how the HACCP-derived methodology of critical analysis and risk correction could be used to effectively manage preoperative nutritional and physical hazards, such as malnutrition and sarcopenia, in order to lead to a substantial improvement of the preoperative optimization while warranting patients’ safety and system efficiency.
The Methodology of Prehabilitation in Elective Orthopedic Surgery
The following seven principles of the HACCP system were adapted for the purpose of our article.
Bullet Points 1 – The Seven Principles of HACCP
I. Identify the hazards that must be prevented, eliminated, or reduced.
II. Identify the critical control points where an inspection is necessary.
III. Calculate the limits that distinguish acceptability from unacceptability.
IV. Define monitoring actions.
V. Plan interventions to correct the risk out of control.
VI. Prepare the documentation.
VII. Define surveillance procedures.
The Analysis of the Preoperative Hazards to Prevent, Eliminate, or Reduce
In orthopedic surgery, there are different nutrition-related and physical-related hazardous situations that can potentially cause a negative outcome after surgery. For the purpose of this article, we can categorise the hazardous nutrition-related aspects in dietary (eg, poor diet), biochemical (eg, deficits of blood nutrients), and anthropometric (eg, poor body composition). Similarly, the hazards associated with physical inability can be functional (eg, reduced muscle strength or imbalance) and anthropometric (eg, reduced lean mass). Although it is not the aim of this article to show original data from the literature, statistics in Table 1 summarize some of the most acknowledged hazardous conditions, the associated outcomes, and the nature of the relationship between the two factors (directly or indirectly proportional).
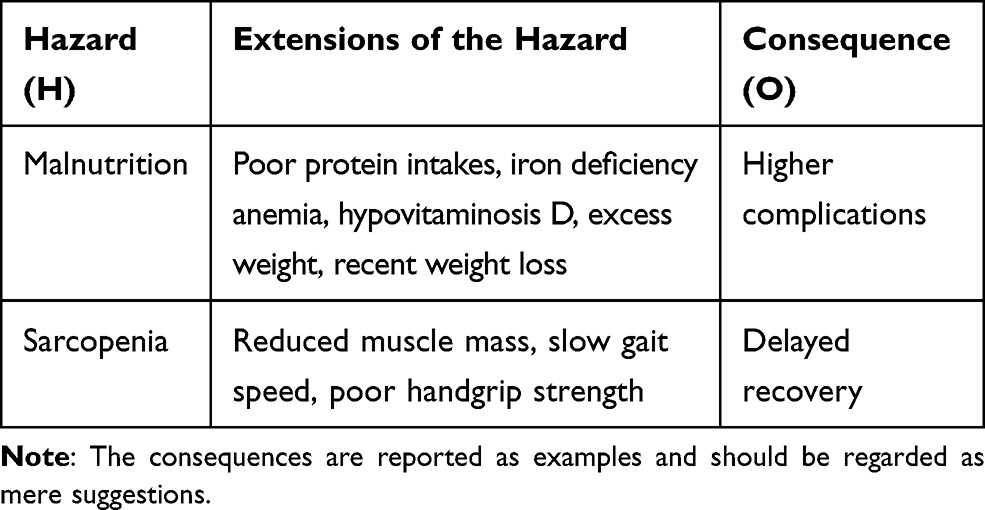 |
Table 1 Examples of Preoperative Nutritional and Physical Hazards, Their Extensions, and the Associated Consequences After Surgery That are Reasonable to Expect in Elective Orthopedic Surgery |
The analysis of these hazards to prevent, eliminate, or reduce should follow these sequential steps of risk identification and analysis:
Bullet Points 2 – Risk Analysis
- Identification of the Hazard (H), Consequences (O), and Severity (SO).
- Estimation of the association between the H and O.
- Estimation of the Probability of occurrence of the Hazard (PH).
- Estimation of the efficacy of corrective procedures (β) and efficiency of personnel (ε).
- Calculation of the risk (R).
The fulfilment of these sequential steps has the subsequent implication of determining if the nutritional and physical status would require precautionary or corrective measures in order to avoid negative postoperative consequences. Notably, the risk is distinguished from a hazard as the former refers to the probability. Importantly, the analysis should account for detailed demographic characteristics, environmental exposures, and consequences of these exposures. The risk analysis calculation (see Supplementary 1) culminates with the equation that identifies the preoperative nutritional and/or physical risk of patients undergoing elective orthopedic surgery.

R = risk.
SO = severity of consequences.
PH = probability of occurrence of the hazard.
β = beta factor from Greek “βελτίωση” (veltíosi, improvement), which depends on the efficacy of interventions.
ε = epsilon factor from Greek “εκπαίδευση” (ekpaídefsi, education), which depends on staff training.
∑(τ) = summation of each vulnerable condition called.
Tau factor from Greek “τρωτό” (trotó, vulnerability).
∑(φ) = summation of each burden called.
Phi factor from Greek “φoρТio” (fortío, burden).
∑(α) = summation of each root cause called.
Alpha factor from Greek “αγένεια” (agéneia, incivility).
This final equation accounts for conditions of vulnerability, environmental pressures18 that might expose the patient to increased risks for adverse outcomes, the efficacy of the corrective procedures (β), and efficiency of personnel (ε) that influences the proper execution of procedures.19 Further considerations about β and ε are discussed in the paragraphs concerning the surveillance procedures and the prerequisites, respectively. Considering that we cannot modify factors τ, φ, or α, the R can be reduced through 1) nutritional and physical prehabilitation interventions that optimize the strength of constitution of orthopedic patients (reduced PH), 2) the conduction of research initiatives that innovate protocol efficacy (increased β), 3) training programs that keep the staff updated on the correct executions of the operations (increased ε).
The Critical Control Points (CCPs)
The CCPs are the phases, between the operational steps, where an inspection is feasible and in which a loss of control of one of the hazards and their extensions in Table 1 could lead to an unacceptable health risk. The identification of the Critical Control Points (CCPs) requires a schematic and detailed approach, with the reasoning eventually analysing the existing operational phases of the preoperative flow. At the level of the CCPs, it is possible and necessary to prevent, eliminate, or reduce to an acceptable extent the risk of negative outcomes after surgery. The CCPs are identified through a decision tree (see Supplementary 2, adapted from a reference of interest)20 that analyses each phase of the process in sequence and discusses the questions on the basis of the hazards, the monitoring actions, and the interventions. As an example, we propose three CCPs to be integrated into the prehabilitation path of care. The CCP I is the “Assessment of the nutritional and physical status. This phase can be integrated into the usual pre-admission evaluation. At this stage, it is very likely to find a condition whose risk and severity is worth monitoring, like poor iron status, excessive body weight, reduced muscle mass, and poor balance. The CCP II is the “Control of the adherence to the program”. If the first control phase involved the prescription of corrective actions (dietary and exercise interventions), this second control phase would be useful for monitoring the adherence to interventional indications. Several hazardous malnutritional and sedentary factors stem from home environment, and long scheduling periods can worsen the R. Telephone contact could provide reinforcement measures/additive actions necessary to ensure patients’ confidence. The CCP III is the second “Assessment of the nutritional and physical status” before surgery. This point includes either a confirmation of surgery in case of risk control after the application of corrective protocols or a delay of surgery in case the risk still undermines the appropriate postoperative recovery.
The identification of critical control points is not to be underestimated. The definition of a CCP would involve the implementation of a monitoring system (principle IV of bullet points 1), which could encompass the use of different medical equipment and dedicated staff. If the patient was found to be at high risk, a dedicated room would be needed to ensure the proper interview with the dedicated healthcare professional. Moreover, the proper identification ensures the effective design and application of the corrective measures (principle V of bullet points 1). If a hazard has been identified at a stage where no control measure exists, the process would need an earlier or later phase to include the corrective intervention, which may be not always feasible.
Reference for Critical Ranges
At the level of CCPs, control measures must remain within acceptable ranges as far as it is concerned for patient safety. The critical intervals distinguish acceptability from unacceptability, demonstrating that a critical point is under/out of control. The measures of interest related to the hazards shown in Table 1 can be the conditions themselves (malnutrition and sarcopenia) or their extensions (eg, circulating blood parameters of nutrients or muscle strength). For instance, if the diagnostic tool for malnutrition (eg, MNA–SF)21 or sarcopenia (eg, U-Test)22 has been validated and/or tested on the population and setting of interest, then its performance is probably better than single extensional parameters. However, very often direct diagnostic tools do not indicate which factor to correct, the type of corrective action, or they are not specific to the orthopedic population (eg, the patient may be less performance not because there is sarcopenia but because of pain and crutches). More easily, the hazards are controlled by measuring and adjusting their related extensional parameters as the ones proposed in Table 1. Reference ranges can be inferred from different sources: national regulations, international guidelines, expert opinions, consensus, literature on a similar population and comparable setting, personal experience in the field, or results from surveillance. It is important to consider that the critical reference ranges, which demarcate the acceptable from the unacceptable, do not necessarily coincide with diagnostic values. They should indicate ranges beyond which there is an increased likelihood of being malnourished or sarcopenic. It is always advisable to translate the measure of interest into a quantitative variable to facilitate standardization between patients. For example, it is better to measure the concentration of circulating hemoglobin rather than asking the patient if he/she consumes iron-rich foods, or to measure gait speed rather than asking for his/her confidence in walking. Algorithm-derived judgments could effectively incorporate the nature of the condition (eg, low hemoglobin because of poor iron intake or disease-related?). Some examples of cut-off values can be waist circumference >80 cm (central obesity), <0.8/kg/day (protein intakes), <0.8 m/s (slowness), or <20 kg of handgrip strength (weakness). Monitoring techniques will then be able to provide rapid interpretations of the results, taking prompt corrective measures. The final goal is to set the boundaries at each CCP within which control measures must remain.
Monitoring of Critical Parameters
A strategic monitoring program at each critical point is a key element to identify a loss of control in a precise, accurate, and timely manner. The question to be asked is “Where and when is there more tendency to lose control of the extensional parameters of the hazards?”. Monitoring techniques must be identified for each parameter along with the relative frequency of checking. There are three general classes of monitoring techniques used to check whether a critical control point is within the reference limits. The physical techniques are relatively fast, with immediate results and direct associations with the physical ability, but the disadvantages are the need for equipment and the dependence on the skills and experience of the operator (medium accuracy). The biochemical parameters are precise, but there is the need for laboratory resources, the results are not always associated with the clinical feature (therefore not relevant), and there is the dependence on the sample processing (medium-high accuracy). The observation/interview techniques are fast, cheap, and accessible, but they are not easily correlated to the clinical feature and depend on the skills and experience of the operator (low accuracy). Whatever type of monitoring technique, it is important to record the results on specific forms, to be signed by the operator, and made available during surveillance procedures. Monitoring actions listed above are part of a planned sequence of activities.
Bullet Points 3 – Steps for Monitoring
- Define the monitoring procedures for each CCP.
- Indicate the monitoring technique to be used.
- Plan the “when” and the “how often”.
- Designate the dedicated executive staff.
- Anticipates the interpretation of the results.
- Start considering the corrective actions.
In the preoperative managing of elective orthopedic surgery, an example of a monitoring procedure could be a blood test (biochemical monitoring) to assess the level of ferritin (extensional parameter of malnutrition) at the level of the CCP I in order the check if malnutrition is under control. After the identification of this parameter out of reference ranges, it would be much easier to intervene for restoring iron homeostasis through corrective protocols. Monitoring actions should be focused on parameters that are known to be critically associated with the clinical outcome in order to maximize the effectiveness of the risk analysis and corrective protocols.
Corrective Protocols
An effective control system requires that the hazardous nutrition-derived and physical-derived factors are treatable, implying that they can be prevented, eliminated, or reduced to acceptable levels. Considering the different ranges of risks, each resulting score should include corresponding corrective actions (see Table 2).
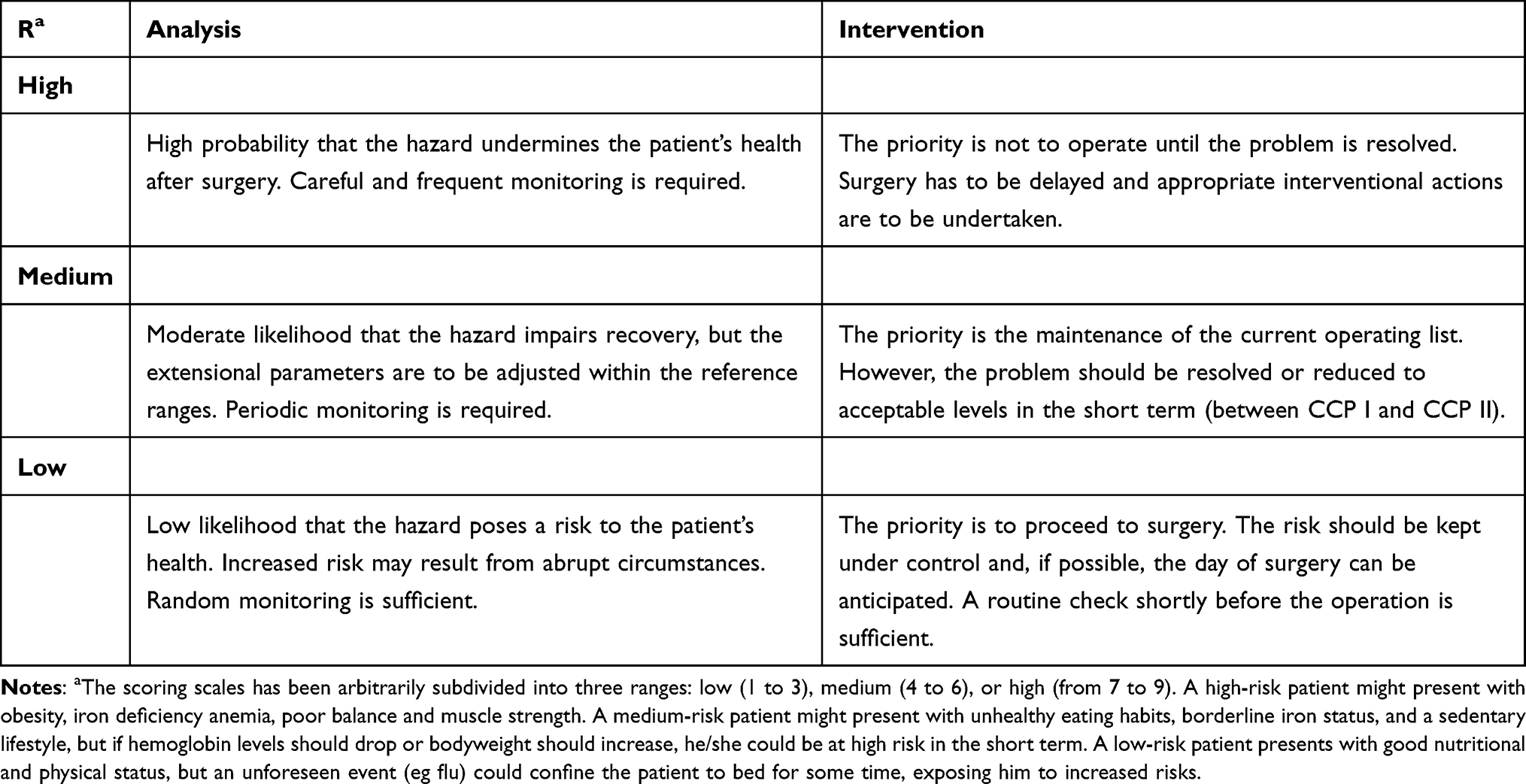 |
Table 2 Examples of Risk Scoring and Corresponding Corrective Actions That May Be Adopted at the CCPs in Elective Orthopedic Surgery |
Corrective actions comprise procedures that prevent the occurrence of problems, keep the process under control when there is a tendency to deviate from the limits, and that handle the risk once a deviation has occurred. Four types of corrective actions can therefore be planned: preventive protocols (targeted for the single patient at low risk or population medicine approach for consecutive patients),23 corrective protocols (for the patient at medium-high risk), reinforcements (strengthening adherence to indications), and repressive actions (for the patient when there is not enough time to correct the high risk). The programming of corrective measures must follow a pre-established sequence of actions to be applied without hesitation when the monitoring detects a deviation from the boundaries of acceptability.
Bullet Points 4 – Steps for Corrective Protocols
- Define the interventions for each CCP.
- Plan the protocols (preventive, corrective, reinforcement, or repressive).
- Plan the means and the time frame.
- Activate dedicated monitoring techniques according to the protocol.
- Designate the dedicated executive staff.
The decision to adopt a specific type of action mainly depends on the level of risk, when it is detected, and what is the efficacy of the means used in the corrective protocol. For instance, if a high risk of malnutrition is detected at the level of CCP I, which may be weeks before surgery, it is possible to intervene with nutritional prehabilitation that is able to correct the abnormality in time. If a high risk is detected during the CCP III, which may be close to surgery, it may be necessary to delay/suppress the orthopedic procedure. It should also be taken into account the time it takes for the parameter to fall within the reference limits and the possibility of interacting with the patient (in person or remotely). For example, the correction of circulating vitamin D can take as little as three weeks24 as well as the restoration of iron homeostasis23 or the overall physical function.25 Different control measures may be necessary to control a single hazard and, conversely, a distinct control measure can control multiple hazards. For instance, a balanced preoperative diet could correct vitamin deficiencies while integrating exercise interventions. The improvement of a parameter can be more rapid if the corrective protocol integrates the two dimensions (eg, exercise plus protein supplementation) and if it is tailored according to the patient’s propensities (eg, liking or disliking of vegetables, preference for cycling, single dish for dinner) and home environment (eg, lack of kitchen scale, physical activity in the living room or in the park, grocery shopping once every two weeks to the far supermarket). The experience of the prehabilitation team should provide the knowledge about the appropriate model for correcting the extensional parameters out of reference ranges. Research analyses are vital to confirm the efficacy of routine interventions or investigate novel approaches to complete the risk analysis (factor β). How to manage the compliance to the corrective programs? Additive monitoring techniques may be integrated into the usual path of care if, for instance, the assessment at the CCP I reveals a tendency to low adherence from prescribed therapies (see Figure 1 for the building of the preoperative flow, with the three corrective actions integrated into the final prehabilitation path of care).
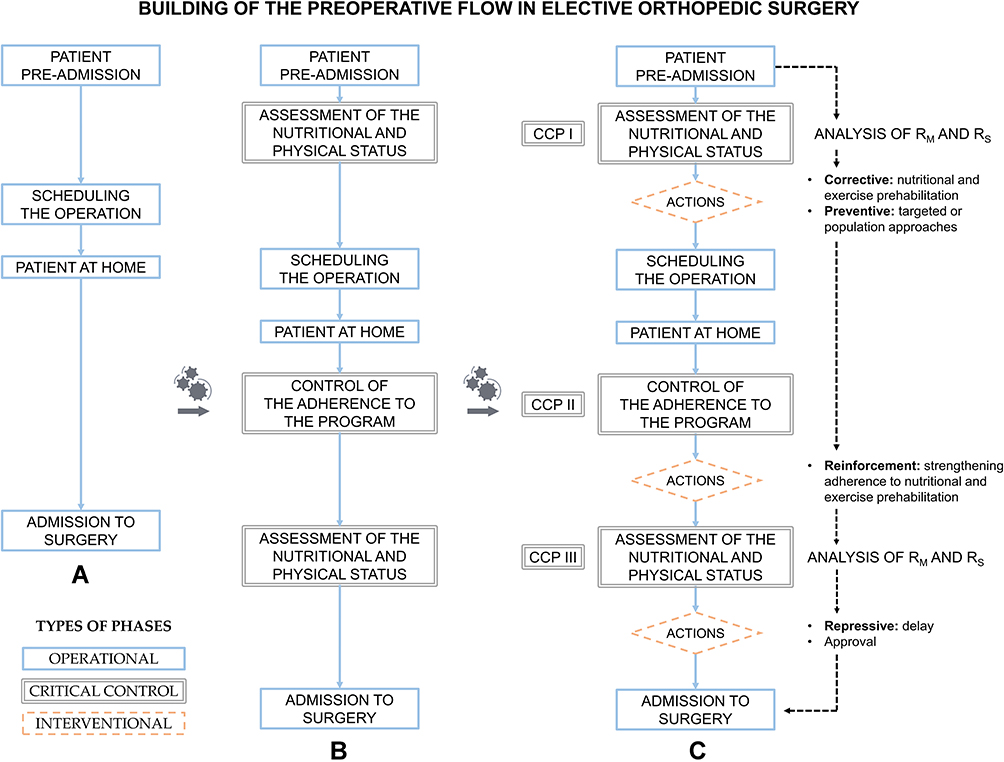 |
Figure 1 Building of the nutritional and physical prehabilitation in elective orthopedic surgery. (A) The preoperative flow of patients undergoing elective orthopedic surgery can be displayed through the operative steps (blue frames). (B) The addition of three critical control phases (CCPs, double gray frame) between the operative steps is useful in order to detect any risk to be prevented, eliminated, or reduced to an acceptable extent. (C) The final integration of the preoperative flow with different interventional procedures (red dotted frame) allows the efficient management of the patient’s nutritional and physical risks through preventive, corrective, reinforcements, or repressive actions. |
Documentation
Both the risk analysis and the control system should be documented, including all procedures (prescriptive documentation) and records from monitoring/interventions (consultative documentation). Appropriate documenting is required to reconstruct a patient’s history and to provide evidence of the process integrity in following the steps of bullet points 1, 2, 3, and 4. The minimum standards of documentation should describe, for example, the relevant pathological history, the vulnerable conditions, the burdens and root causes, the risk analysis findings, the critical parameters assessed, the clinical impression, the plan for preoperative care, the legible identity of the executive members of the staff, the patient progress (response and change in treatment), the revision of extensional parameters and risk analysis findings. The documents should be appropriately archived and made available in case of surveillance procedures. Clearly, the digitization of report forms and archiving systems is of fundamental utility to reduce operational times and speed up data extraction procedures.
Surveillance Procedures
Monitoring aims to observe the status of the parameter while surveillance aims at verifying the effect of the control measures, confirming or not that the path is supporting the patient’s health. Surveillance procedures comprise different modalities, like periodic reviews of the entire prehabilitation flow, an inspection of each CCP to confirm safety, or verification of the correct execution of all the planned actions. The frequency of surveillance should be based on the complexity of the preoperative flow and on the likelihood that estimated risks may occur.
Bullet Points 5 – Key Elements for Defining Surveillance
- Designation of the surveillance team.
- Random analysis at critical points.
- Audit of prescriptive and consultative documents.
- Validation of critical limits and monitoring techniques.
- Confirmation that hazards are kept under control.
- Investigations on the proper application of corrective procedures.
- Research initiatives to validate current/new corrective protocols (to increase β factor).
The last point is of extreme importance. One of the main goals of prehabilitation is the constant endowment of “the best possible nutritional and exercise management”. The increase of the β factor in the equation of risk analysis would reduce the R, and therefore research studies should be persistently conducted in parallel to clinical practice. Once a new and more effective protocol is discovered, the entire preoperative flow must be modified, incorporating changes of documentation to ensure updated information. Concerning the role assignment, the surveillance team should comprise members different from the executive and monitoring staff. Conversely, other individuals can perform multiple executive and monitoring tasks, but all relevant information should be available to all team members.
The Seven Prerequisites of Prehabilitation
The health of orthopedic patients cannot solely derive from the support actions established through the HACCP-derived nutritional and physical prehabilitation. 1) Environment preventive measures are an important rudiment and should routinely interest the workplace and personnel, such as hygiene procedures and calibration/maintenance of equipment. 2) Training programs, such as information campaigns or focused courses, should keep staff informed of the most recent advancements because untrained hospital personnel could nullify operational, monitoring, of corrective procedures (the greater the ε factor in the equation of risk analysis the lower the R). 3) The team of specialists of the prehabilitation program should preferably involve different healthcare professionals, in order to bring together the whole spectrum of knowledge to lay the groundwork for a reliable, precise/accurate, and effective program. 4) The experts in charge of research initiatives should have knowledge about the Good Clinical Practices (GCP) inherent in human research in order to conduct and report high-level clinical trials. 5) Quality improvement resources should be used to provide pictorial displays of the phases and the decision-making procedures, with any upgrading resulting in a modification of the original flowchart or algorithm in order to advance the visual exactness. 6) The hospital food system should comply with various standards (HACCP principles), including quality raw materials to guarantee hospitalized patients the best possible nutrition. 7) Any dietary supplement of interest should follow the appropriate management procedures, with the involvement of the hospital pharmacy playing an essential role.
Conclusion
In the current panorama, the main indications for orthopedic surgery include end-stage degenerations like coxarthrosis, gonarthrosis, and vertebral deformities that are typical of multi-frail individuals.26,27 The increasing demand for these orthopedic procedures contrasts with the complex phenotypes of old orthopedic patients progressively malnourished and sarcopenic,2,28 giving rise to complex pathological spectra like sarcopenic obesity.29 Examinations into modifiable risk factors acknowledged preoperative malnutritional status and physical inability as critical factors for patient’s distress.30 Collectively, these two conditions reduce the strength of constitution necessary to cope with the physiological stressors of orthopedic surgery (see Supplementary 3 for the typical nutrition-related and physical-related factors affecting patients undergoing elective orthopedic surgery). Multidisciplinary approaches like the ERAS or the HEPAS (Healthy Eating, Physical Activity, and Sleep hygiene)2,31 appear to be very useful in the most fragile individuals. However, they lack of systematic assessments, methodology of interventions, and suggestions on the management of monitoring procedures. This lack of methodology could hide important aspects of preoperative care and hinder the implementation of research findings into practice. In this context, the use of the flexible principles of the HACCP system may allow the adoption of an essential, detailed, and inclusive method for process analysis, critical monitoring, and lifestyle-derived risk correction before elective procedures. An effective nutritional and physical prehabilitation could enhance the physiological reserves and the overall resilience of old orthopedic patients (see Figure 2). If the seven prerequisites are met (hygiene practices, training, multidisciplinarity, research integrity, visualization, food safety, and supplement management), the design of the orthopedic prehabilitation is certainly enabled, with the equation of risk analysis efficiently considering both patient-related (τ, φ, and α) and process (β and ε) factors. The management of malnutrition and physical inabilities is not sufficient to improve the clinical outcome of orthopedic patients, but it is reasonable to say that it is a necessary requirement for the effectiveness of the entire path of care.
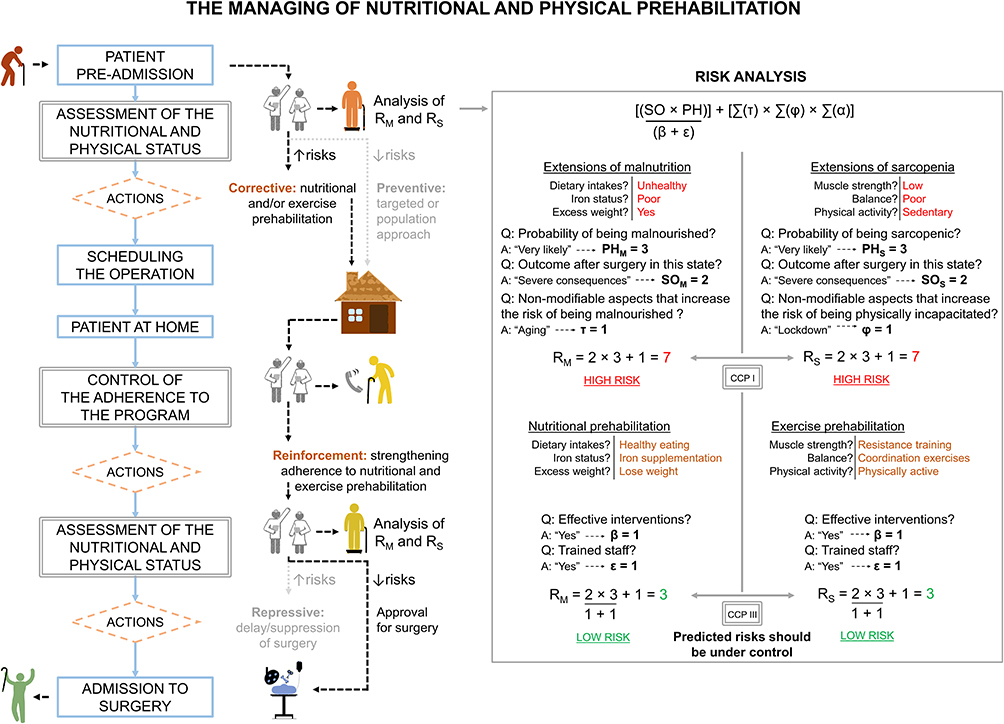 |
Figure 2 The application of the hazard analysis and critical control point (HACCP) system in elective orthopedic surgery, with a focus on nutrition-related and physical-related factors. |
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ji HM, Han J, Jin DS, Suh H, Chung YS, Won YY. Sarcopenia and sarcopenic obesity in patients undergoing orthopedic surgery. Clin Orthop Surg. 2016;8(2):194–202. doi:10.4055/cios.2016.8.2.194
2. Briguglio M. The burdens of orthopedic patients and the value of the HEPAS approach (Healthy Eating, Physical Activity, and Sleep hygiene). Front Med. 2021;8. doi:10.3389/fmed.2021.650947
3. Eminovic S, Vincze G, Eglseer D, et al. Malnutrition as predictor of poor outcome after total hip arthroplasty. Int Orthop. 2021;45(1):51–56. doi:10.1007/s00264-020-04892-4
4. Ueoka K, Kabata T, Kajino Y, et al. The prevalence and impact of sarcopenia in females undergoing total hip arthroplasty: a prospective study. Mod Rheumatol. 2021:1–6. doi:10.1080/14397595.2021.1899603
5. Black CS, Goltz DE, Ryan SP, et al. The role of malnutrition in ninety-day outcomes after total joint arthroplasty. J Arthroplasty. 2019;34(11):2594–2600. doi:10.1016/j.arth.2019.05.060
6. Ardeljan AD, Polisetty TS, Palmer J, Vakharia RM, Roche MW. Comparative analysis on the effects of sarcopenia following primary total knee arthroplasty: a retrospective matched-control analysis. J Knee Surg. 2020. doi:10.1055/s-0040-1713355
7. Tsantes AG, Papadopoulos DV, Lytras T, et al. Association of malnutrition with surgical site infection following spinal surgery: systematic review and meta-analysis. J Hosp Infect. 2020;104(1):111–119. doi:10.1016/j.jhin.2019.09.015
8. Flexman AM, Street J, Charest-Morin R. The impact of frailty and sarcopenia on patient outcomes after complex spine surgery. Curr Opin Anaesthesiol. 2019;32(5):609–615. doi:10.1097/ACO.0000000000000759
9. Wainwright TW, Gill M, McDonald DA, et al. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS((R))) society recommendations. Acta Orthop. 2020;91(1):3–19. doi:10.1080/17453674.2019.1683790
10. Debono B, Wainwright TW, Wang MY, et al. Consensus statement for perioperative care in lumbar spinal fusion: Enhanced Recovery After Surgery (ERAS(R)) society recommendations. Spine J. 2021;21(5):729–752. doi:10.1016/j.spinee.2021.01.001
11. Starks I, Wainwright TW, Lewis J, Lloyd J, Middleton RG. Older patients have the most to gain from orthopaedic enhanced recovery programmes. Age Ageing. 2014;43(5):642–648. doi:10.1093/ageing/afu014
12. Vasta S, Papalia R, Torre G, et al. The influence of preoperative physical activity on postoperative outcomes of knee and hip arthroplasty surgery in the elderly: a systematic review. J Clin Med. 2020;9(4):4. doi:10.3390/jcm9040969
13. Burgess LC, Phillips SM, Wainwright TW. What is the role of nutritional supplements in support of total hip replacement and total knee replacement surgeries? A systematic review. Nutrients. 2018;10(7):820. doi:10.3390/nu10070820
14. Godziuk K, Prado CM, Beaupre L, Jones CA, Werle JR, Forhan M. A critical review of weight loss recommendations before total knee arthroplasty. Joint Bone Spine. 2021;88(2):105114. doi:10.1016/j.jbspin.2020.105114
15. Wainwright TW. The quality improvement challenge-how nurses and allied health professionals can solve the knowing-doing gap in Enhanced Recovery after Surgery (ERAS). Medicina. 2020;56(12):652. doi:10.3390/medicina56120652
16. Briguglio M. Nutritional Orthopedics and space nutrition as two sides of the same coin: a scoping review. Nutrients. 2021;13(2):483. doi:10.3390/nu13020483
17. NATIONS FAAOOTU. The Hazard Analysis and Critical Control Point (HACCP) system. In: Food Quality and Safety Systems - a Training Manual on Food Hygiene and the Hazard Analysis and Critical Control Point (HACCP) System. Rome: Publishing Management Group, FAO Information Division; 1998.
18. Schroder-Butterfill E, Marianti R. A framework for understanding old-age vulnerabilities. Ageing Soc. 2006;26(1):9–35. doi:10.1017/S0144686X05004423
19. Gesme DH, Towle EL, Wiseman M. Essentials of staff development and why you should care. J Oncol Pract. 2010;6(2):104–106. doi:10.1200/JOP.091089
20. Hazard Analysis and Critical Control Point system. The national advisory committee on microbiological criteria for foods. Int J Food Microbiol. 1992;16(1):1–23.
21. Cereda E, Pedrolli C, Klersy C, et al. Nutritional status in older persons according to healthcare setting: a systematic review and meta-analysis of prevalence data using MNA((R)). Clin Nutr. 2016;35(6):1282–1290. doi:10.1016/j.clnu.2016.03.008
22. Kamitani T, Wakita T, Wada O, Mizuno K, Kurita N. U-TEST, a simple decision support tool for the diagnosis of sarcopenia in orthopaedic patients: the Screening for People Suffering Sarcopenia in Orthopedic cohort of Kobe study (SPSS-OK). Br J Nutr. 2021;126(9):1323–1330.
23. Briguglio M, Hrelia S, Malaguti M, et al. Oral supplementation with sucrosomial ferric pyrophosphate plus L-ascorbic acid to ameliorate the martial status: a randomized controlled trial. Nutrients. 2020;12(2):386. doi:10.3390/nu12020386
24. Briguglio M, Gianturco L, Stella D, et al. Correction of hypovitaminosis D improved global longitudinal strain earlier than left ventricular ejection fraction in cardiovascular older adults after orthopaedic surgery. J Geriatr Cardiol. 2018;15(8):519–522. doi:10.11909/j.issn.1671-5411.2018.08.005
25. Whittle J, Wischmeyer PE, Grocott MPW, Miller TE. Surgical prehabilitation: nutrition and exercise. Anesthesiol Clin. 2018;36(4):567–580. doi:10.1016/j.anclin.2018.07.013
26. Seidlitz C, Kip M. Introduction to the indications and procedures. In: Bleß HH, Kip M, editors. White Paper on Joint Replacement: Status of Hip and Knee Arthroplasty Care in Germany. Berlin (Germany): Springer; 2018.
27. Martin BI, Lurie JD, Tosteson AN, et al. Indications for spine surgery: validation of an administrative coding algorithm to classify degenerative diagnoses. Spine. 2014;39(9):769–779. doi:10.1097/BRS.0000000000000275
28. Briguglio M, Giorgino R, Dell’Osso B, et al. Consequences for the elderly after COVID-19 isolation: FEaR (Frail Elderly amid Restrictions). Front Psychol. 2020;11:565052. doi:10.3389/fpsyg.2020.565052
29. Moreno-Franco B, Perez-Tasigchana RF, Lopez-Garcia E, et al. Socioeconomic determinants of sarcopenic obesity and frail obesity in community-dwelling older adults: the Seniors-ENRICA Study. Sci Rep. 2018;8(1):10760. doi:10.1038/s41598-018-28982-x
30. Briguglio M, Gianola S, Aguirre M-FI, et al. Nutritional support for enhanced recovery programs in orthopedics: future perspectives for implementing clinical practice. Nutr Clin Metab. 2019;33(3):190–198. doi:10.1016/j.nupar.2019.04.002
31. Briguglio M, Lombardi G, Sansoni V, Perego S, Colonna VDG, Stella D, Colombo C, Bonadies M, De Blasio G, Banfi G, Turiel M. Vitamin D, cardio-inflammation, and endothelial dysfunction in older adults after orthopedic surgery: Results from an open-label trial to ameliorate cardiac function. Nutrition Clinique et Métabolisme. 2020; Volume 34; Issue 4; 313-318. doi:10.1016/j.nupar.2020.06.003.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.