Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Nursing Practices and Risk Factors in Neonates with Respiratory Distress Syndrome Undergoing Surfactant Replacement Therapy: A Cross-Sectional Study in Saudi Arabia
Authors Elbilgahy AA ![]() , Jothirajan D, Alanazi LO, Alanazi FA, Alanazi MG, Alanazi AS
, Jothirajan D, Alanazi LO, Alanazi FA, Alanazi MG, Alanazi AS
Received 3 April 2025
Accepted for publication 17 July 2025
Published 8 August 2025 Volume 2025:18 Pages 4903—4918
DOI https://doi.org/10.2147/JMDH.S532177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr David C. Mohr
Amal Ahmed Elbilgahy,1,2 Deepa Jothirajan,1 Lujain Obaid Alanazi,3,4 Fai Abduallah Alanazi,3 Maryam Gharbi Alanazi,3,4 Atheer Saleh Alanazi3
1Maternal and Child Health Nursing Department, Faculty of Nursing, Northern Border University, Arar, Saudi Arabia; 2Pediatric Nursing Department, Faculty of Nursing, Mansoura University, Mansoura, Dakahlia, Egypt; 3Faculty of Nursing, Northern Border University, Arar, Saudi Arabia; 4Department of Operation Rooms (OR), Prince Abdulaziz bin Musaad Hospital, Ministry of Health, Arar, Saudi Arabia
Correspondence: Amal Ahmed Elbilgahy, Email [email protected]; [email protected]
Purpose: We examined nursing knowledge, care practices, and risk factors for respiratory distress syndrome (RDS) in newborns receiving surfactant therapy at a Saudi Arabian neonatal intensive care unit (NICU).
Methods: Our observational study included 53 NICU nurses and 381 newborns (28– 42 weeks gestation) with RDS. We assessed nurses’ knowledge through questionnaires, observed their care practices, and reviewed newborn medical records.
Results: Less than half of the nurses (47.2%) showed a strong understanding of RDS and surfactant therapy, with gaps in recognizing diagnostic methods (only 24.5% correct) and risk factors (60.4% incorrect). Most nurses (69.8%) provided competent care, especially those with more education (p < 0.001) or training (p = 0.002). Newborns averaged 35.9 weeks gestation with initial APGAR scores of 5.8. Key risks included premature birth (71.9%), cesarean delivery (63.8%), maternal diabetes (24.2%), and insufficient antenatal steroids (only 24.4% of mothers received full doses).
Conclusion: Our findings highlight opportunities to enhance nursing education about RDS, particularly in diagnosis and risk recognition. Implementing standardized care protocols for surfactant therapy and increasing antenatal steroid use could improve newborn outcomes. Preventing premature birth remains crucial for reducing RDS risk.
Plain Language Summary: This study focuses on the care of newborns with respiratory distress syndrome (RDS) who receive surfactant therapy. RDS is a serious condition that affects premature babies, making it hard for them to breathe. The researchers looked at how well neonatal nurses understood and practiced care for these infants. They found that while many nurses had good knowledge about RDS, there were still gaps in their understanding, particularly regarding the best practices for care. Common risk factors for RDS included premature birth, low birth weight, and maternal conditions like diabetes. The study emphasizes the need for continuous training for nurses to improve their skills and knowledge, which is essential for better outcomes for newborns with RDS. Overall, enhancing nursing practices can significantly impact the health and survival of these vulnerable infants.
Keywords: nursing care, premature, respiratory distress syndrome, surfactant replacement therapy
Introduction
Premature birth is a critical global health challenge and a leading cause of neonatal illness and death worldwide, affecting approximately 15 million infants annually. Preterm infants, with their immature organ systems, are particularly vulnerable to complications such as respiratory and feeding difficulties, growth impairments, thermoregulatory issues, and infections.1,2 Neonatal RDS, also known as hyaline membrane disease, primarily affects preterm infants and accounts for 30–40% of NICU admissions. Untreated RDS can lead to high morbidity and mortality, especially in infants born between 26 and 28 weeks.3 A substantial number of admissions to neonatal intensive care units (NICUs) for both preterm and term infants are attributed to RDS.4 The incidence of respiratory distress syndrome in infants born after 37 weeks of gestation in Taif, Saudi Arabia, is 0.15% (13 out of 8634).5
RDS typically appears immediately after birth, presenting with signs of respiratory distress such as tachypnea, grunting, nasal flaring, chest retractions, and cyanosis, with severity linked to prematurity. Extreme pre-term infants exhibit the most severe symptoms, and disease progression can lead to apnea, hypotonia, diminished breath sounds, and circulatory shock.6 Diagnosis involves clinical evaluation and testing, with characteristic chest X-ray findings showing a “ground-glass” pattern and alveolar atelectasis. Blood gas analysis indicates hypoxemia and acid-base imbalances, aiding in diagnosis and monitoring. Standardized scoring systems, particularly the Downes’ Score (for all neonates) and Silverman Anderson Score (for preterm infants), provide objective measures of respiratory distress severity. These tools guide clinical decision-making by enabling serial assessment of treatment response and disease course.7
Prenatal corticosteroid administration significantly decreases neonatal morbidity and mortality, particularly reducing risks of RDS, while decreasing the need for respiratory support and NICU admission. Current guidelines recommend a single course for women at imminent preterm delivery risk (24–34 weeks gestation), and consideration for preterm premature rupture of membranes before 32 weeks to mitigate RDS and mortality risks.8,9 Surfactants, a phospholipid secreted by alveolar cells, reduce surface tension in the lungs, promoting uniform alveolar expansion and preventing collapse. While adequate levels develop by 35 weeks’ gestation, preterm infants often experience deficiency-related respiratory distress. Surfactant replacement therapy (SRT) improves survival and reduces morbidity, with early rescue administration now preferred over prophylaxis. Current approaches favor minimally invasive techniques (eg, thin catheters) alongside non-invasive ventilation, though traditional intubation-surfactant-extubation remains common.10,11
Neonatal nurses play a crucial role in caring for newborns, especially those requiring surfactant replacement therapy (SRT) for RDS. Their responsibilities include managing ventilation whether through CPAP or mechanical ventilation and ensuring proper endotracheal tube placement. Close monitoring of oxygen levels, blood gases, and vital signs (eg, heart rate, SpO2, blood pressure) is essential for timely ventilator adjustments. Additionally, nurses must assess respiratory function, including air entry, breath sounds, chest expansion, and secretions, as well as track ventilator metrics like pressures, tidal volumes, and transcutaneous PCO2 (TcPCO2).12,13 Newborns with RDS require careful handling to maintain oxygenation and reduce metabolic strain. Excessive stimulation, such as crying, can worsen hypoxia, increase pulmonary pressure, and disrupt breathing. Proper temperature control is crucial to minimizing oxygen demand. While suctioning helps clear airway secretions, it must be performed cautiously to avoid complications like tracheal damage, bradycardia, or low oxygen levels. It should only be done, when necessary, guided by clinical signs such as abnormal breath sounds, oxygen desaturation, or infant distress.3 Neonatal nursing has become more complex, significantly impacting infant survival. Nurses must possess sharp observation skills, make accurate clinical decisions, and promptly recognize complications to ensure the best outcomes for critically ill newborns.
Optimal nursing care is critical for newborns with respiratory distress syndrome (RDS), particularly regarding surfactant replacement therapy (SRT) - a lifesaving intervention that remains underutilized in some clinical settings.14 While SRT significantly reduces RDS mortality, studies indicate persistent variations in nursing knowledge and practices across neonatal units, including inconsistent adherence to administration protocols, gaps in monitoring post-SRT complications, and limited training on emerging minimally invasive techniques.15 This study specifically examines these clinical practice gaps by evaluating current nursing competencies in SRT delivery and barriers to optimal surfactant administration as well as assessment of risk factors affecting RDS outcomes in Saudi NICUs. Ultimately, this research contributes to improving clinical outcomes for vulnerable neonates, reducing morbidity and mortality associated with RDS, and advancing evidence-based nursing practices in resource-limited settings. The study also lays a foundation for future research on tailored educational interventions and multidisciplinary care models.
Research Questions
- What is the level of nurses’ knowledge and practice about the quality of nursing care provided for neonates with RDS undergoing surfactant replacement therapy?
- What is the most common risk factor for respiratory distress syndrome among neonates?
Subjects and Methods
The current study utilized an observational cross-sectional exploratory research design, conducted in the Neonatal Intensive Care Unit (NICU) at Maternity & Children’s Hospital affiliated with the Ministry of Health in Arar, Saudi Arabia. Based on data from literature,16 to calculate the sample size with precision/absolute error of 5% and type 1 error of 5%, Sample size is calculated according to the following formula: n = Z1−α/22 × P(1−P) d2n = d2Z1−α/22 × P(1−P). Where, Z1-α/2 at 5% type 1 error (p < 0.05) is 1.96, P is the expected proportion in population based on previous studies and d is the absolute error or precision. Therefore, the sample size is n = (1.96)2 × 0.5 × 0.5(0.05)2 = 52.3 n = (0.05)2(1.96)2 × 0.5 × 0.5 = 52.3. Based on the predetermined sample size calculation, the study enrolled 53 neonatal nurses through convenience sampling from the target NICU setting. Inclusion criteria required participants to be: (1) actively registered nurses holding valid licensures, (2) possessing a minimum of six months’ clinical experience in neonatal intensive care, and (3) voluntarily consenting to participate in the research. The exclusion criteria systematically eliminated: (1) nurses declining participation and (2) those in internship or training positions.
Also, a random sample of 381 neonates admitted to NICU fulfilling the following inclusion criteria: all neonates diagnosed with RDS from both genders are integrated in the study and the gestational age of the neonates is between 28–42 weeks. Neonates with transient tachypnea of the newborn were omitted from the study. The minimal sample size for the study was (381) according to the following equation: n = Z1−α/22 × P(1−P) d2n = d2Z1−α/22 × P(1−P). Where Z1-α/2= is the standard normal variate at 5% type 1 error (P < 0.05); it is 1.96. P = 54.7%; the expected proportion based on a previous study and (d) = the absolute error (0.05)
Instruments for Data Collection
Three instruments were employed for data collection. Tool 1: Nurses Knowledge About the Nursing Care Provided for Neonates with RDS & Undergoing Surfactant Replacement Therapy (SRT) Questionnaire. The questionnaire was developed by the researcher after reviewing related literature.17,18 It includes two parts: Part 1: demographic characteristics of the nurses studied and contains questions related to the nurses age, educational level, years of experience the NICU and previous attendance of training courses in NICU. Part 2: Knowledge regarding respiratory quality of nursing care provided for neonates with RDS & undergoing SRT. This part will include questions such as definition, signs, risk factors, prevention, management of SRD and the nurses’ knowledge of SRT such as definition, administration and nurse intervention. The study utilized a three-tiered classification system to evaluate nurses’ knowledge levels. Participants scoring 80% or higher were categorized as having good knowledge, demonstrating a comprehensive understanding of the subject matter. Those achieving scores between 75–79% were classified as possessing average knowledge, indicating partial but incomplete mastery. Scores below 75% were designated as inadequate knowledge, reflecting significant gaps in understanding.18
Tool II: Checklist to observe nurses practice regarding care of neonate with RDS. It consists of 17 steps and the nurses evaluate each step on a scale of “always”, “sometimes”, and “never.” The evaluation of nursing practice employed a standardized scoring system with defined competency thresholds. Nurses achieving a total score of ≥80% were classified as demonstrating competent practice, while those scoring below this benchmark were categorized as having incompetent practice.17,18
Tool III focuses on the prevalence and risk factors associated with respiratory distress syndrome in neonates. This tool was created by researchers following a review of relevant literature14 and consists of three sections. The first sections include questions about gender, gestational age, Apgar score, birth weight, height, length of stay in NICU. The second sections comprise questions about maternal risk factors for RDS like type of delivery, taking antenatal steroids and presence of chronic illness. The third part includes questions related to initiation of resuscitation at delivery room, administration of surfactants at delivery room and in NICU, doses of surfactant, use of ventilator support, neonatal feeding and neonatal outcome.
Validation and Reliability of Research Instruments
The research team implemented a rigorous validation process to ensure the robustness of the study instruments. Following development, the survey underwent comprehensive validation, including forward and backward translation to verify linguistic accuracy and conceptual equivalence. Five expert reviewers specializing in pediatric and neonatal nursing evaluated the tool’s content validity through a structured assessment process. These experts, selected based on their clinical expertise and research experience, received the instrument via Email and systematically evaluated it across three key domains: (1) item relevance to neonatal RDS care practices, (2) comprehensiveness in covering critical nursing knowledge domains, and (3) clarity of wording and instructions. The validation process incorporated multiple iterations of expert feedback, with revisions made to improve instrument quality until consensus was achieved.
The reliability of Tool I and Tool II was assessed using Cronbach’s alpha. Tool I, based on responses from all 53 nurses, showed excellent internal consistency (α = 0.901), with item analysis confirming that all questions had corrected item-total correlations above 0.30, ensuring none weakened overall reliability. Tool II demonstrated a similarly strong consistency (α = 0.893) across 17 items. For inter-rater reliability, two independent observers evaluated 20% of the nurses (n = 11), showing high agreement (Cohen’s κ = 0.81–0.89). This coefficient significantly exceeds the commonly accepted threshold of 0.70 for research instruments, indicating excellent consistency among survey items in measuring the targeted constructs. The combination of expert validation and statistical reliability testing ensured the tool’s appropriateness for assessing nursing knowledge and practices in the NICU setting.
Pilot Study
The pilot study was conducted on 5 nurses (10%) of the calculated study sample to test the clarity, validity and reliability of the tool 1 within our specific context. Since this pilot study was solely to validate the questionnaire’s applicability and did not involve any interventions, we included these participants in the total study sample. These nurses raised no concerns or issues regarding the questionnaire, which ensured that their responses remained unaffected by prior familiarity.
Ethics Approval and Consent to Participate
The study adhered to the principles outlined in the “Declaration of Helsinki.” Ethical agreement was granted from Northern Border University with the following number (HAP-09-A-043) with decision number (62/44/H) 12-7-2023. Furthermore, Ethical agreement was obtained from Institutional Review Board in Arar with the following number (H-09-A-051) with Log no: NIC-IRB-023-11-042. Administrative agreement attained by the head of department of NICU and hospital manager. Written informed consent was secured from the nurses prior to their participation in the study, following a clear explanation of the study’s purpose. Participants were informed that all data would be coded to ensure confidentiality.
Data Collection
The study employed a multi-method approach to data collection, utilizing three distinct instruments: (1) a structured questionnaire, (2) a standardized observation checklist, and (3) electronic medical record review. For efficient data capture of nurses’ knowledge (Tool I), the research team developed and administered a digital questionnaire through Google Forms, which was completed directly by participating in nursing staff. The remaining data collection tools (Tool II: observation checklist and Tool III: medical record abstraction) were implemented by the research team members themselves to ensure consistency in data recording and interpretation. Participant recruitment was conducted by disseminating an announcement through the head nurse and posting it in the NICU nurses’ WhatsApp group, which outlined the study’s objectives and included a link to the questionnaire.
Nurses were observed during their routine shifts using a structured checklist (Tool II) to evaluate their practices in caring for neonates with RDS. Observations occurred over two months, with each nurse assessed for approximately three hours per day, three times per week, covering morning, evening, and night shifts to capture variability in care delivery. To minimize bias, observers (trained research team members) were not involved in the nurses’ clinical duties and were blinded to the nurses’ demographic data (eg, experience level, training history) during assessments. Inter-rater reliability was ensured by training all observers on the checklist criteria prior to data collection, followed by joint observations to calibrate scoring. Discrepancies were resolved through consensus. The high internal consistency of Tool II (Cronbach’s α = 0.893) further supports the reliability of the observational data. To assess the prevalence and risk factors for respiratory distress syndrome among neonates (Tool III), data was extracted from electronic health records, following the acquisition of ethical and administrative approvals. The overall data collection period lasted six months, from November 20, 2023, to May 20, 2024. The random selection of neonates was operationalized through a systematic process to ensure unbiased representation. After obtaining ethical approvals, the researchers accessed the NICU’s electronic medical records and nursing Kardex, which listed all admitted neonates with various diagnoses. From this pool, neonates meeting the inclusion criteria (diagnosed with RDS, gestational age 28–42 weeks, both genders) were assigned unique identifiers based on their file numbers. Using these identifiers, neonates were randomly selected via a computerized randomization procedure to eliminate selection bias. This method ensured that every eligible neonate had an equal chance of inclusion, enhancing the generalizability of findings. This random selection process was employed for observational purposes only, and to ensure representative sampling of neonates with RDS and minimizing selection bias in our retrospective data collection with no interventions administered as part of study participation. The head nurse facilitated access to the electronic system to retrieve anonymized data, maintaining confidentiality, while adhering to the study’s cross-sectional design.
Statistical Analysis
All statistical analyses were performed using SPSS for Windows version 20.0 (SPSS, Chicago, IL). Continuous variables exhibited a normal distribution and were reported as mean ± standard deviation (SD). In contrast, categorical variables were presented as counts and percentages. To compare categorical data, the Chi-square test was employed, with Fisher’s exact test applied when appropriate. A p-value of less than 0.05 was established as the threshold for statistical significance.
Results
Nurse Demographics and Training Background (Table 1)
The study cohort comprised 53 neonatal nurses with distinct demographic characteristics as presented in Table 1 demographic characteristics of the nurses studied. The majority (58.5%) fell within the 25–30-year age range, with only 15.1% aged 30–35 years. Experience levels showed 62.3% had less than 5 years of NICU practice, while 26.4% possessed 5–10 years of experience. Educational attainment was notably high, with 83% holding bachelor’s degrees in nursing. Ethnically, the sample was diverse (41.5% Saudi, 45.3% Indian, 9.4% Philippine, 3.8% Egyptian), and 79.2% reported prior RDS-specific training.
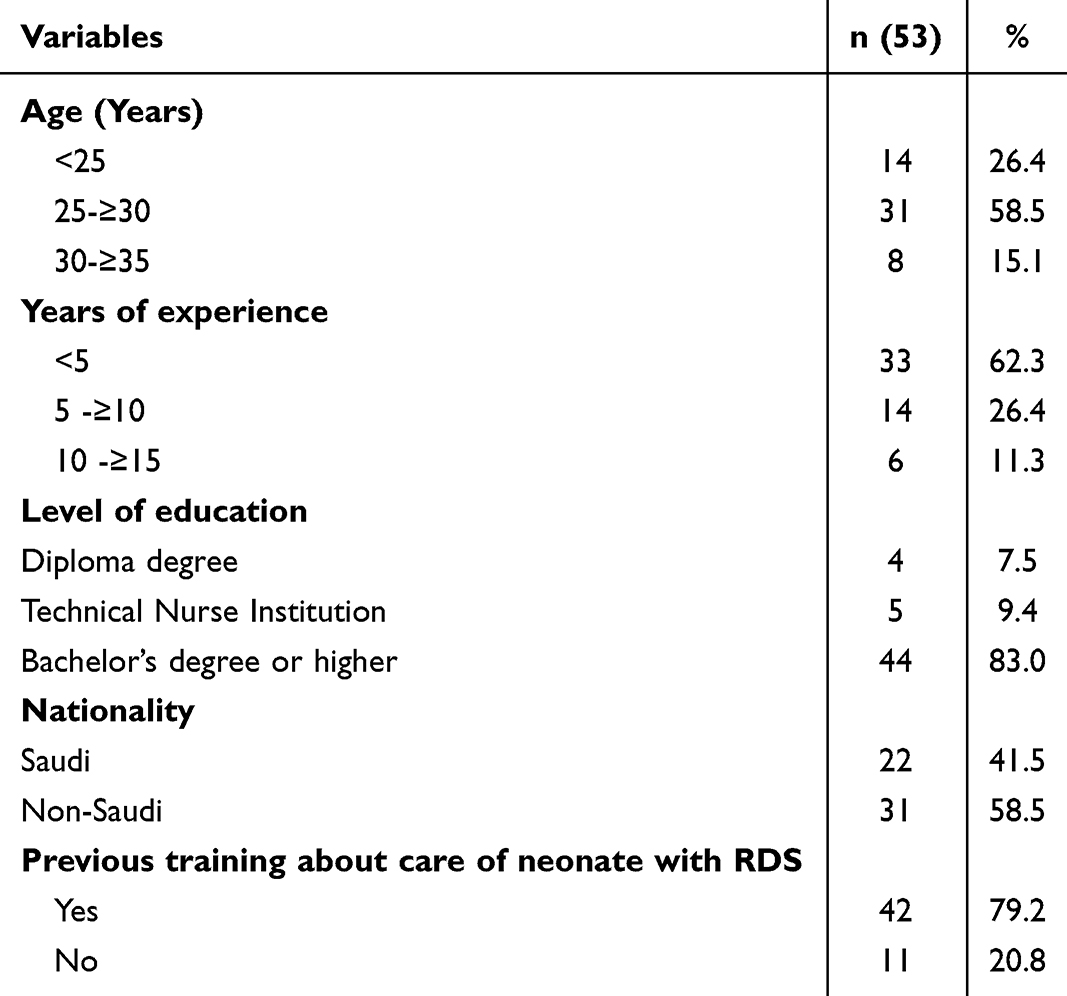 |
Table 1 Demographic Characteristics of the Studied Nurses |
Knowledge Assessment Outcomes (Table 2)
Evaluation of RDS knowledge revealed both strengths and gaps in nursing understanding. Concerning deficiencies were noted in fundamental areas: 69.8% could not correctly identify RDS assessment scales, 60.4% misunderstood key risk factors, and 69.8% were unaware of disease etiology. Diagnostic knowledge was particularly limited, with only 24.5% answering diagnosis-related questions correctly. However, therapeutic knowledge showed better performance regarding surfactant replacement protocols (77.4% correct), post-administration suction timing (69.8%), neonatal care after surfactant (64.2%), and administration routes (67.9% correctly identified endotracheal delivery).
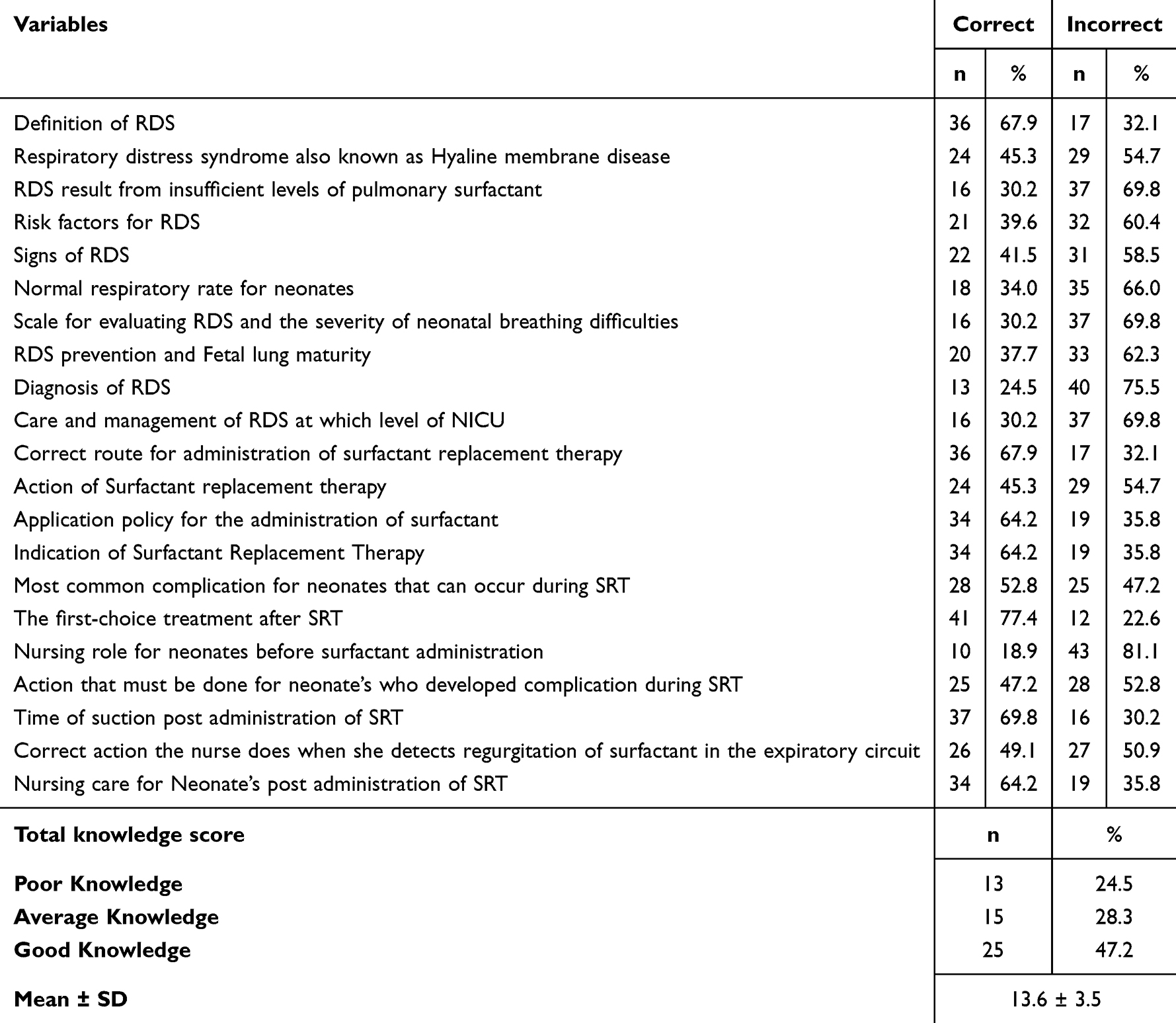 |
Table 2 Nurses’ Knowledge About Nursing Care Provided for Neonates with RDS Undergoing Surfactant Replacement Therapy |
Determinants of Clinical Knowledge (Table 3)
Educational attainment emerged as the strongest predictor of knowledge scores (p < 0.001), with bachelor’s-prepared nurses demonstrating significantly superior understanding compared to diploma holders. Clinical experience showed a weaker but still significant association (p = 0.001), as did participation in training programs (p = 0.002–0.031). These findings suggest that both formal education and practical experience contribute to RDS knowledge acquisition.
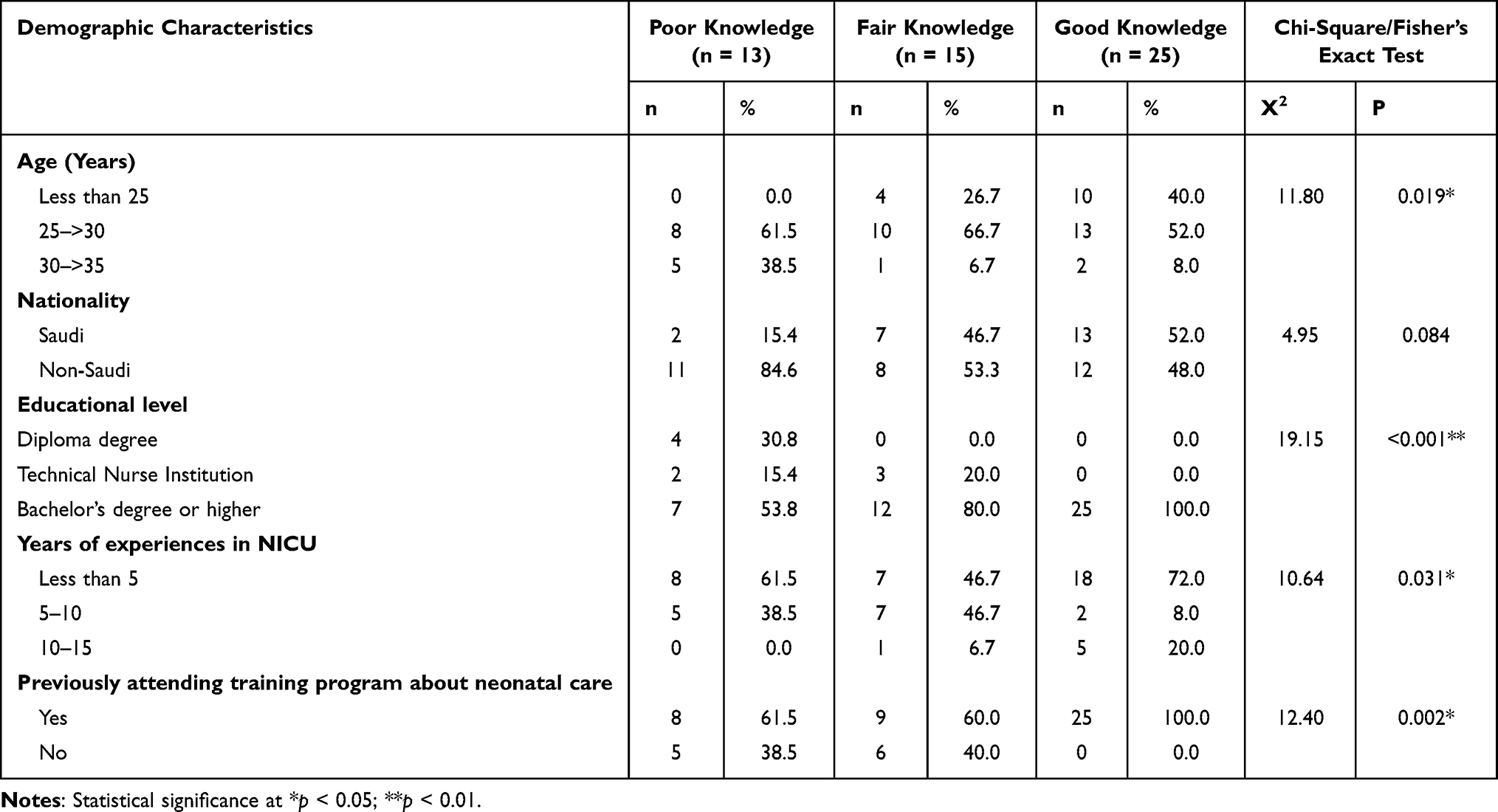 |
Table 3 Relationship Between Demographic Characteristics of Nurses and Total Knowledge Level |
Relationship Between Demographic Characteristics and Nurses Practice Level (Table 4)
The findings demonstrate a strong correlation between educational level and practice level (p < 0.001). Nurses with a bachelor’s degree or higher qualification have a higher percentage of competent practice compared to those with a diploma or technical nurse institution degree. Additionally, there is a significant relationship between years of experience and practice level (p = 0.041). Nurses with less than 5 years of experience have a higher proportion of incompetent practice compared to those with 5–10 or 10–15 years of experience.
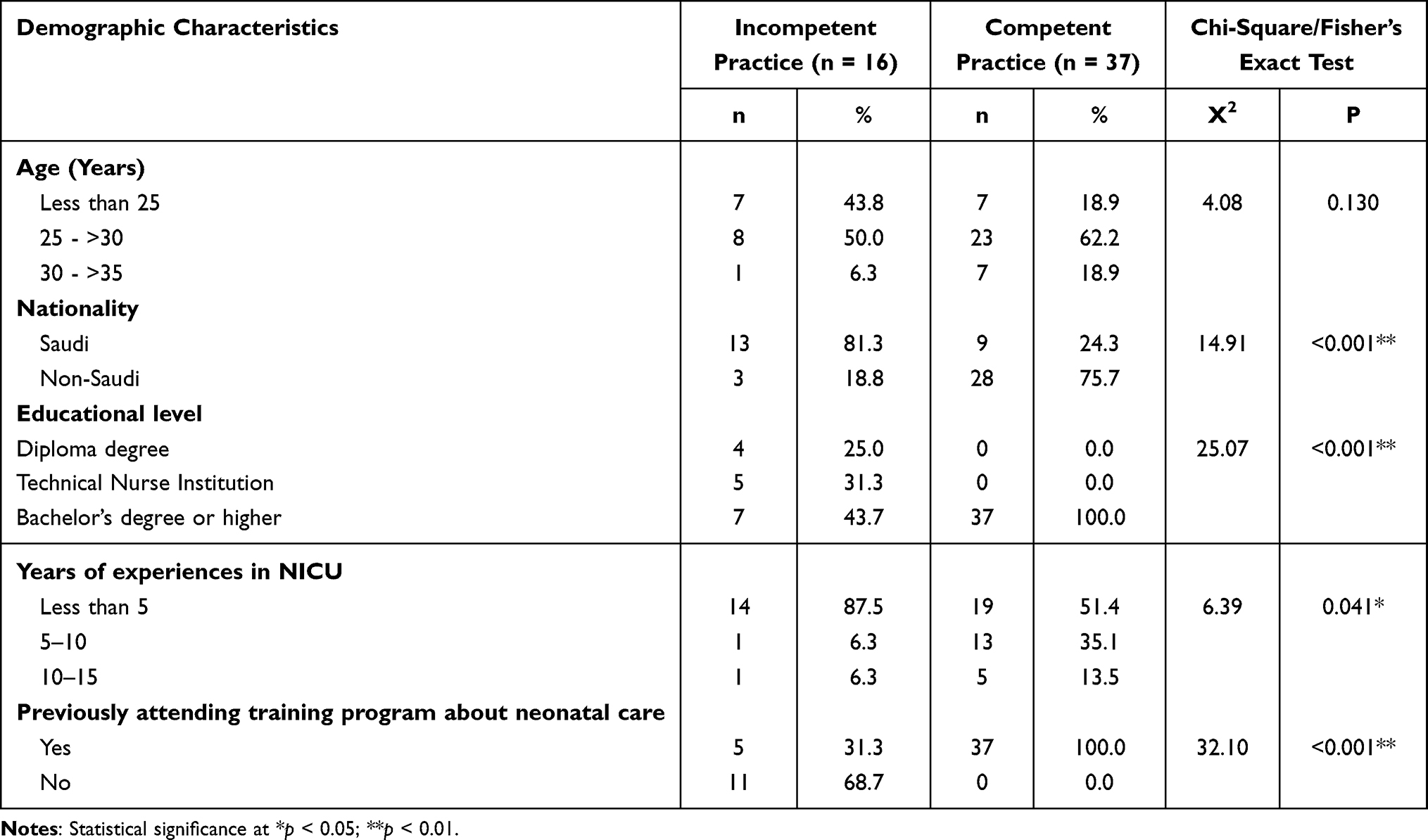 |
Table 4 Relationship Between Demographic Characteristics of Nurses and Total Practice Level |
Relationship Between Total Nurses’ Knowledge and Total Practice Level (Table 5)
Table 5 reveals a statistically significant relationship (p < 0.001) between nurses’ knowledge levels and their competency in managing neonates with respiratory distress syndrome (RDS) receiving surfactant replacement therapy (SRT). Specifically, all nurses (100%) with poor knowledge were found to have incompetent clinical practice, while none (0%) of those with good knowledge fell into that category. In contrast, every nurse (100%) with good knowledge demonstrated competent practice. The chi-square test (X² = 41.61) supports a robust association between knowledge and practice, emphasizing that greater knowledge is strongly linked to higher clinical performance.
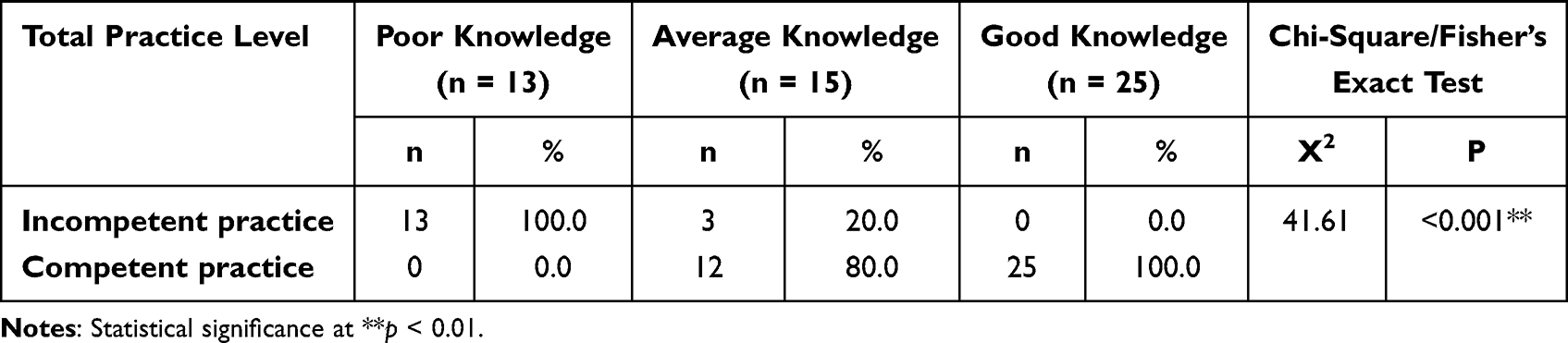 |
Table 5 Relationship Between Total Nurses Knowledge and Practice Score Regarding Care of Neonates with RDS Undergoing SRT |
Knowledge Proficiency Distribution (Figure 1)
The nurse cohort displayed a tri-modal knowledge distribution: 47.2% exhibited good understanding of RDS management, while 28.3% showed average competency and 24.5% demonstrated poor knowledge levels regarding both disease prevention and surfactant therapy protocols.
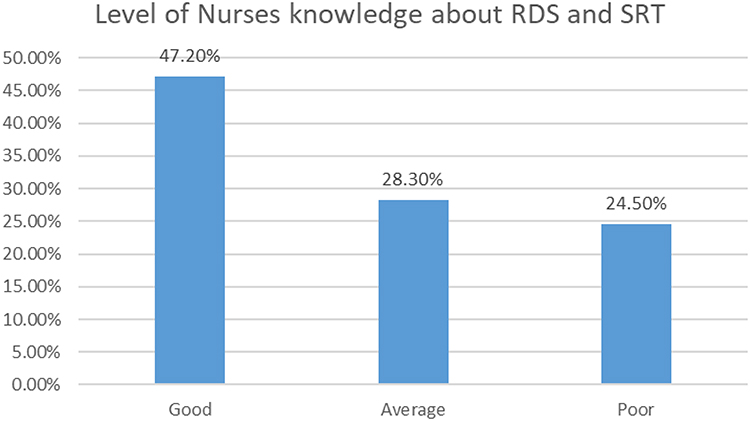 |
Figure 1 Level of nurses’ knowledge about RDS and Surfactant Replacement Therapy (SRT). Data are presented as percentages (%) of nurses with good, average, or poor knowledge levels. |
Practice Competence Distribution (Figure 2)
Figure 2 illustrates the overall level of nursing practice concerning the care of neonates with respiratory distress syndrome (RDS) and those receiving surfactant replacement therapy (SRT). About one-third (30.2%) of the nurses surveyed displayed incompetent practice, whereas 69.8% showed competent practice.
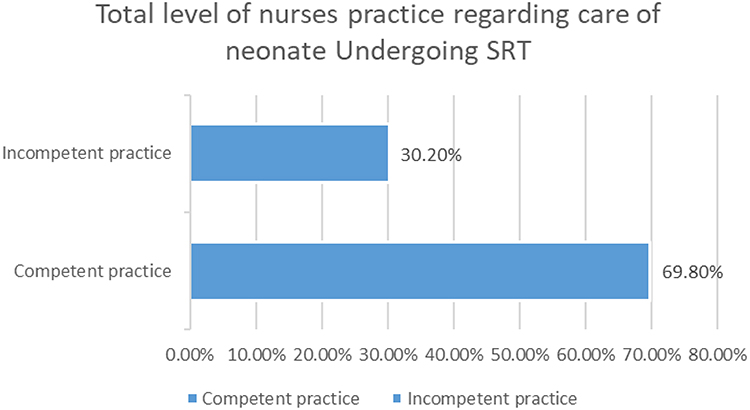 |
Figure 2 Total level of nurses’ practice competency in caring for neonates undergoing Surfactant Replacement Therapy (SRT). Data are presented as percentages (%) of nurses demonstrating competent vs incompetent practice. |
Neonatal Population Characteristics (Table 6)
The 381 neonates studied presented with typical RDS demographics: 59.1% male, mean gestational age 35.9 ± 3.01 weeks, and 48% weighing <2.5kg. Clinical indicators showed expected progression, with Apgar scores improving from 5.8 ± 1.8 at 1 minute to 8.3 ± 1.03 by 10 minutes. Only 22.8% required surfactant therapy, all receiving 1–2 doses.
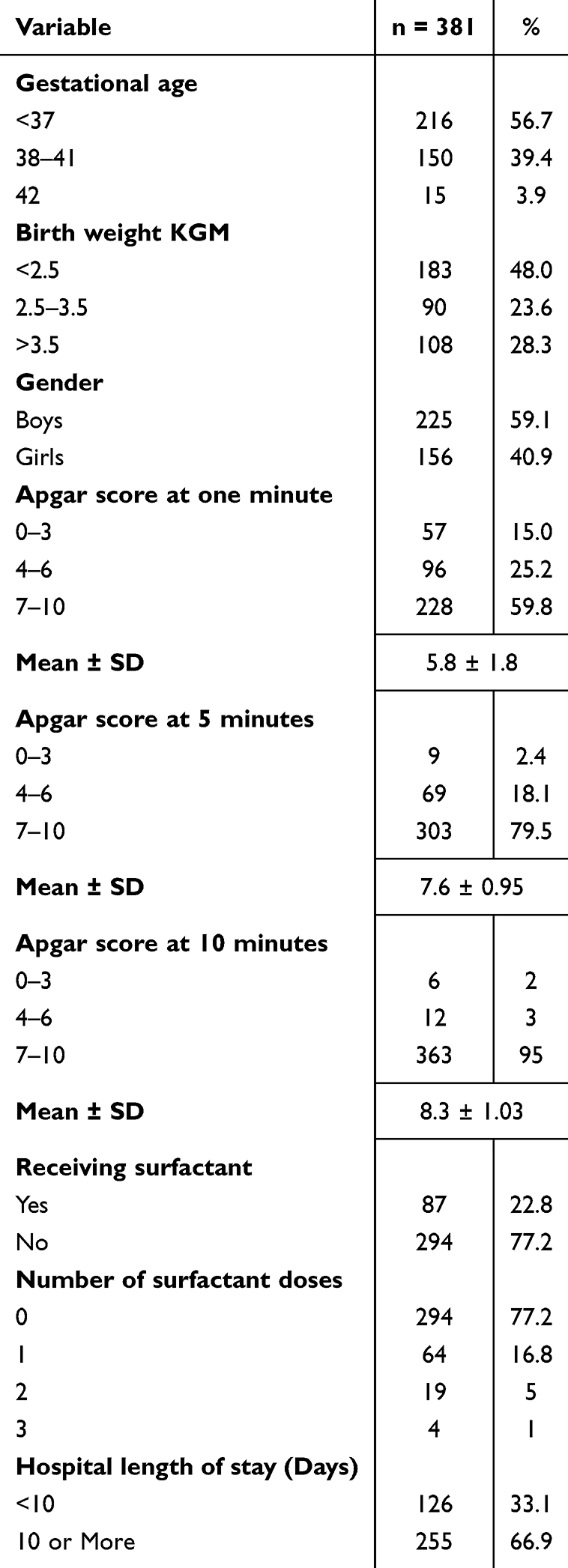 |
Table 6 Demographic and Health Characteristics of the Studied Neonates |
Maternal Risk Factor Profile (Table 7)
Mothers of RDS neonates were predominantly young (52.8% aged 20–30 years, mean 31.25 ± 6.22) and frequently delivered by cesarean section (63.8%). Comorbidities included diabetes (24.2%) and premature rupture of membranes (18.9%). Notably, only 24.4% received complete antenatal steroid courses despite known benefits for lung maturation.
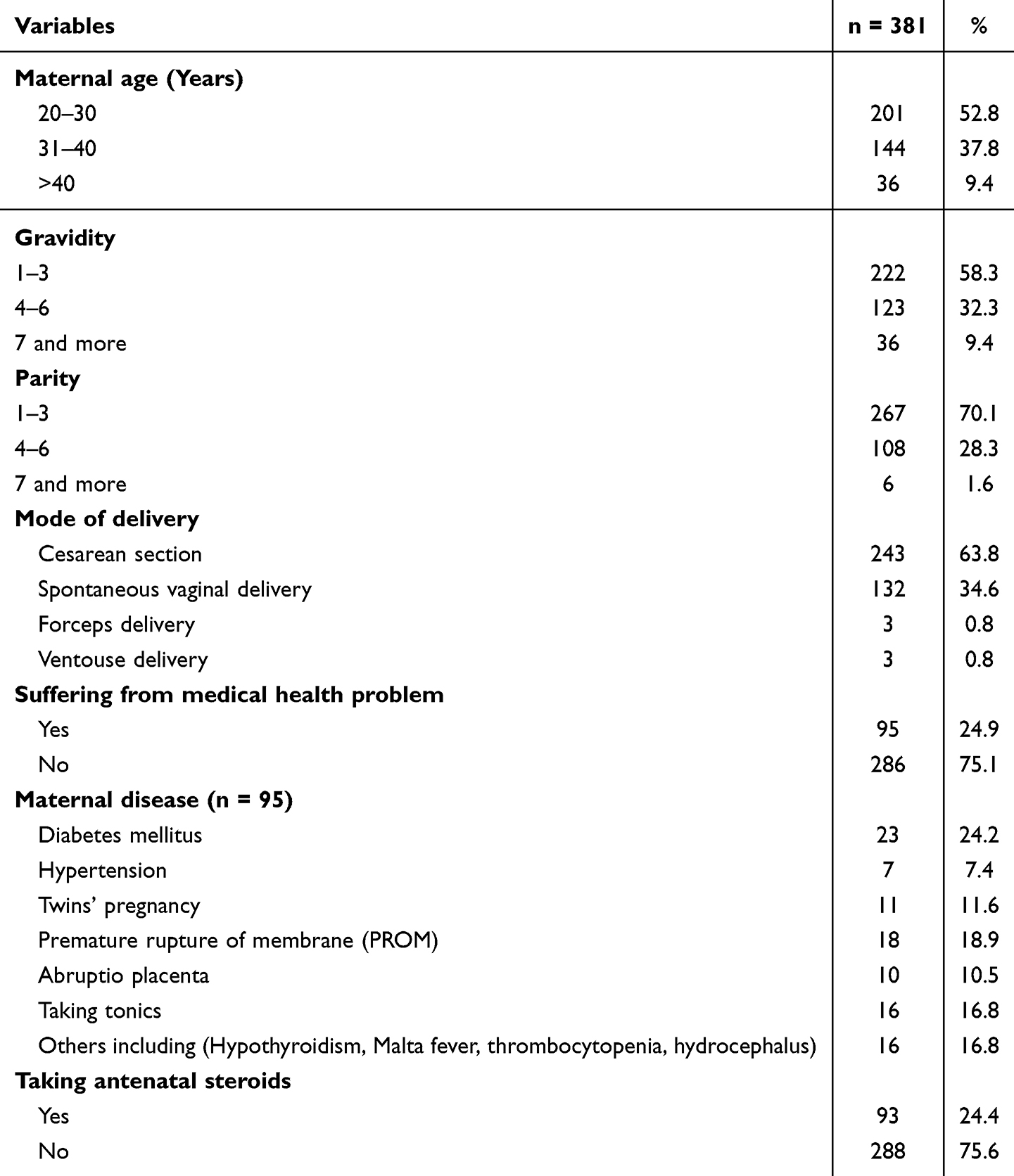 |
Table 7 Maternal Risk Factors for Neonates with Respiratory Distress Syndrome |
Respiratory Support Requirements (Table 8)
Oxygen support needs evolved across care settings: 76.6% required nasal cannula in the delivery room, while 19.8% needed bag-mask ventilation and 13.5% required intubation. Surfactant administration was rare at delivery (3.4%). NICU care primarily involved nasal cannula (56.3%) or CPAP (37.8%), indicating most cases were managed with non-invasive support.
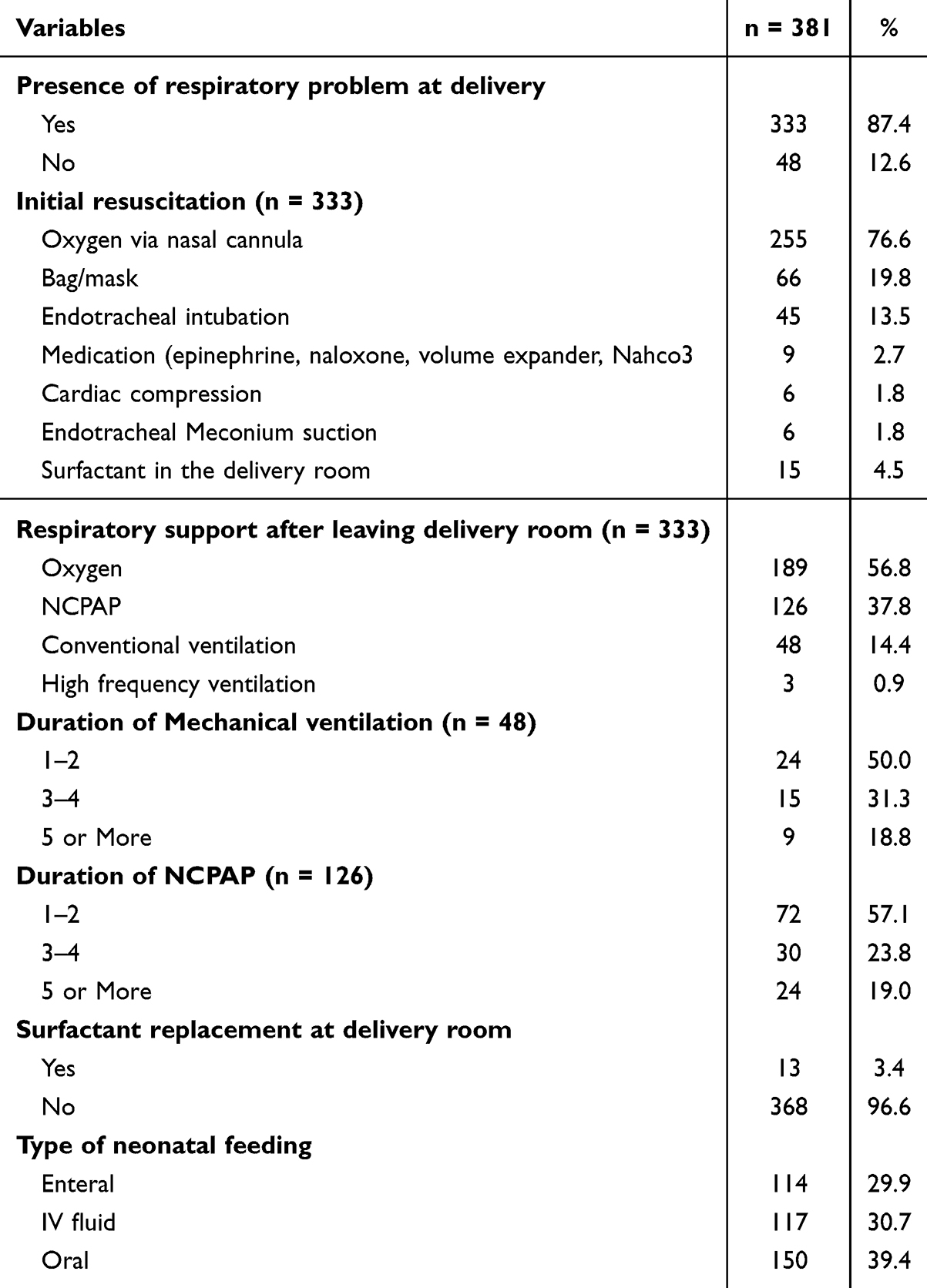 |
Table 8 Oxygenation Status of the Neonates After Delivery and in Neonatal Intensive Care Unit (NICU) |
Discussion
The current study provides new insights into nursing practices and risk factors for RDS in neonates undergoing surfactant replacement therapy, building upon existing knowledge while revealing important clinical implications. While prior studies19–21 have established that RDS severity correlates with birth weight and gestational age, our findings specifically demonstrate that in our cohort of 381 neonates, those with lower Apgar scores (mean 5.8 ± 1.8 at 1 minute) and birth weights (<2.5kg in 48% of cases) had more severe presentations, requiring earlier intervention. Notably, only 22.8% of neonates received surfactant therapy despite 37.8% requiring CPAP support, suggesting potential gaps in treatment protocols that differ from the higher intervention rates reported in previous studies. Unlike earlier work that focused primarily on physiological factors, our study uniquely identifies specific nursing practice patterns with 69.8% demonstrating competent care but concerning knowledge gaps in RDS recognition (only 24.5% correctly identified diagnostic criteria). These findings complement existing literature by quantifying how nursing factors interact with known clinical predictors during the critical 48–72-hour window post-birth.
Concerning the demographic characteristics of the nurses examined, it was observed that over half of them were aged between 25 and 30 years. This finding aligns with the study conducted by Elsayed et al,16 they reported in their study that more than half of the study nurses were in the age group from 20–30 years. This suggests that the nursing staff caring for neonates with RDS is relatively young and likely reflects the general demographic trends in the nursing profession. Furthermore, most nurses replied that they are receiving training programs about the care of neonate with RDS. Similarly, Aziz, and Mansi22 reported that most nurses participated in the training courses about the care of high-risk neonate in NICU.23 On the contrary, Elsayed et al,16 reported that most of the nurses in the study had not attended any training programs. This disparity draws attention to the possible differences in nursing populations’ or health-care environments’ access to and involvement in professional development opportunities. Prioritizing the provision of current and pertinent training programs for all nurses who care for neonates with RDS is important because it can have a direct effect on the standard of care given to these critically ill infants and ultimately affect their outcomes.
As for the nurses’ knowledge of nursing care for newborns undergoing surfactant replacement therapy, a quarter of nurses had poor knowledge, while approximately half of nurses had good level of knowledge. Most of the nurses knew information about the action of SRT and the correct procedure that the nurse takes when she discovers the reflux of surfactant in the expiratory circuit, and they gave correct answers about nursing care after giving surfactant replacement therapy to newborns and the most common complications in newborns that can occur during surfactant replacement therapy, as well as the procedure that should be done for newborns who developed complications during surfactant replacement therapy. This result indicates that the nurses are well-equipped to provide high-quality care for newborns receiving SRT. These results were contrary to the study of Loutfy et al,23 that showed that three-quarters of nurses had incomplete and incorrect answers regarding their knowledge of nursing care for newborns undergoing surfactant replacement therapy. The research explains this difference because in Loutfy et al23 study it was (83.3%) of the nurses did not receive training in care and management with RDS. Also, there were no training programs that emphasized RDS as a critical neonatal disease, but in the current study most nurses received training on care and management with RDS at which level of NICU. Also, the nurses were of different nationalities and may have different nationalities with different educational backgrounds affecting their knowledge. Another study conducted by Elsayed et al16 revealed that approximately two thirds of studied nurses had unsatisfactory knowledge regarding RDS in both hospitals at AL-Noor Specialist Hospital and Heraa General Hospital.
Regarding nurses’ practices about nursing care of neonates with RDS on a CPAP machine, we found that most nurses always monitor vital signs and oxygen saturation and of course this is due to the increased use of oxygen therapy and pulse oximetry for preferred infants with RDS. These results were in line with those of Elsayed et al,16 who investigated the establishment of fundamental nursing care protocols in neonatal intensive care units and discovered that all nurses performed well when it came to providing oxygen therapy or pulse oximetry care. The present study showed that nurses mostly maintain the body temperature in the normal range, change the child’s position every 3 hours or more frequently, apply antibiotic ointment to the nostrils if there is a sign of infection, and change the CPAP machine and CPAP tube every 7 days when it is used for more than one week, they remove excess water from the CPAP tube.
The current study indicates that over two-thirds of the nurses caring for neonates undergoing SRT demonstrated competent practices. This aligns with findings from Elsayed et al,16 who noted that most nurses performed competently, with only a small fraction exhibiting inadequate performance. Both studies were conducted in Saudi Arabia, suggesting that the nurses are well-trained and capable of delivering high-quality care to neonates. Conversely, Loutfy et al24 reported insufficient performance levels among nurses in NICU settings. Additionally, Mohamed et al13 found that nursing practice scores varied, showing both satisfactory and unsatisfactory results. These discrepancies can be attributed to differences in hospital environments, training programs, supervision, and assessment methods across various studies.
The present study reveals a statistically significant relationship between nurses’ educational backgrounds and their levels of knowledge and practice. Nurses with bachelor’s degrees demonstrated better knowledge and were more likely to be classified as competent practitioners compared to their diploma or technical counterparts. Higher education is linked to improved knowledge and essential practical skills. Additionally, the study found that nurses with less than five years of NICU experience had good knowledge levels, while those with 5–10 and 10–15 years of experience showed a higher likelihood of having competent practice. This suggests that newer graduates may possess more up-to-date training and knowledge, despite having less experience. In contrast, Elsayed et al16 reported that nurses with diplomas performed better than those with bachelor’s degrees, which may stem from differences in the sample characteristics of the studies.
Identifying risk factors for neonates with RDS is crucial for developing preventive measures and early treatment strategies. The current study found that over two-thirds of mothers had cesarean sections, with a significant percentage also experiencing diabetes mellitus, multiple gestations, the use of tonics, and premature rupture of membranes (PROM). Alfarwati et al and Condò et al,5,25 similarly reported an association between cesarean sections and RDS, identifying elective cesarean delivery as a primary risk factor for respiratory distress in term infants. Infants born via cesarean section often have a greater residual lung fluid volume, reduced functional residual capacity, and consequently produce less surfactant in the alveolar space. In contrast, vaginal delivery compresses the infant’s chest, aiding in the expulsion of fetal lung fluid and promoting surfactant release due to adrenergic stimulation during labor.26 Despite the high rate of cesarean deliveries in our study, only 25% of mothers received antenatal corticosteroids (ACS). While a single course of ACS is well-established in improving fetal lung maturation and reducing severe RDS in preterm births,8 the low utilization observed here may be attributed to the retrospective nature of the study. Many cesarean deliveries were likely emergency procedures, leaving insufficient time for ACS administration, a factor not captured in the collected data. Additionally, potential barriers such as late hospital admission, lack of prenatal care, or clinical urgency may have contributed to the underuse of ACS despite its proven benefits. Further prospective studies should evaluate the reasons behind low ACS administration to optimize its timely use in at-risk pregnancies.
The current study revealed that more than 50% of newborns with RDS were male, aligning with previous findings by Baseer et al and Niesłuchowska-Hoxha et al27,28 It is widely recognized that lung growth and development begin before birth, with female fetuses typically exhibiting more advanced lung maturation. Fetal oral movements, which emerge between weeks 16 and 26 of gestation and indicate breathing activity, play a vital role in lung development.29 Furthermore, sex hormones significantly influence lung maturation. Testosterone, released by fetal testes, tends to suppress surfactant production, slowing its increase. On the other hand, placental estrogens enhance both surfactant synthesis and alveologenesis in neonates and during puberty.30
Additionally, the current study found that most neonates (71.9%) with RDS were born prematurely, with a mean gestational age of 35.9 ± 3.01 weeks, confirming prematurity as the most critical risk factor. An Indian study reported that the incidence of RDS decreases sharply with advancing gestational age, ranging from 86% at 24 weeks to less than 1% at 39 weeks, highlighting that RDS should be expected in infants of diabetic mothers (IDMs) and preterm deliveries.31 In our study, neonates with RDS had a lower mean birth weight (2501.04 ± 1062.6 grams) and reduced Apgar scores at both one and five minutes, further supporting the association between low birth weight and RDS. These findings align with Condò et al,25 who identified low birth weight in term infants as a significant risk factor for RDS.
The current study found that 22.8% of neonates received surfactant replacement therapy (SRT), primarily administered using the Intubate-Surfactant-Extubate (INSURE) technique, with most infants requiring only a single dose. While this proportion may appear low compared to some reported rates, it likely reflects several factors, including the heterogeneity of respiratory distress syndrome (RDS) severity in the study population, the early and effective use of non-invasive respiratory support (eg, CPAP) that may have reduced the need for SRT, and variations in institutional protocols regarding surfactant administration. Early recognition of respiratory distress and prompt intervention remain critical for improving outcomes, and the observed rate suggests that a significant proportion of neonates may have been managed successfully without surfactants. However, retrospective data limited our ability to assess specific eligibility criteria (eg, FiO2 thresholds) for SRT in each case, which could further explain the variation. Future prospective studies should evaluate optimal SRT timing in similar settings and clarify the best thresholds for surfactant administration in this population, particularly in resource-limited contexts where clinical judgment plays a key role in decision-making.
Regarding respiratory support, most neonates initially required assistance via nasal cannula at delivery, while approximately one-third needed bag-mask ventilation or mechanical ventilation. During NICU admission, the majority received respiratory support through nasal cannula or CPAP, suggesting that non-invasive strategies were frequently employed. These findings highlight the importance of tailored respiratory management based on disease severity and clinical response.
Strength, Limitations and Future Work
The current study has some limitations; First, the retrospective nature of the study limited our ability to gather additional information on other variables that could be examined for their association with the incidence of respiratory distress syndrome. Also, the researcher was not able to link the risk factor with the outcome of the neonate as we collected the data from electronic systems and the data for deceased infants was not available. Furthermore, the small sample size precluded the use of logistic regression analysis to ascertain the specific odds associated with various risk factors.
Conclusion and Recommendation
This study revealed that most nurses demonstrated moderate knowledge levels, with identifiable gaps in understanding and clinical practices related to neonatal RDS and surfactant replacement therapy (SRT). Key risk factors for RDS in term neonates included low birth weight, prematurity, cesarean delivery, maternal diabetes, and low Apgar scores, highlighting the need for targeted education and standardized protocols to enhance nursing care, particularly for neonates on CPAP. To address these gaps, we recommend (1) implementing structured in-service training programs with competency assessments to improve RDS prevention, SRT administration, and CPAP management; (2) developing evidence-based clinical guidelines tailored to local contexts to standardize care across institutions; (3) ensuring resource accessibility through updated digital and print materials, such as mobile-friendly guides and quick-reference pamphlets, for point-of-care support; and (4) investigating systemic contributors to knowledge gaps, including disparities in professional development and the impact of multinational workforce diversity on practice variability. Future research should further explore barriers to guideline adherence and assess the effectiveness of these interventions in improving neonatal outcomes.
Data Sharing Statement
All the data generated was included in this article.
Acknowledgment
The authors gratefully acknowledge the approval and the support of this research study by the grant No (NURA-2023-12-2013) from the Deanship of Scientific Research at Northern Border University, Arar, Saudi Arabia.
Disclosure
The researchers declare that there is no conflict of interest.
References
1. Walani SR. Global burden of preterm birth. Int J Gynaecol Obstet. 2020;150(1):31–33. doi:10.1002/ijgo.13195
2. Samir EA, Mahmoued FS, Bayoumi MH. Effect of evidence-based guidelines on nurses’ performance regarding care of high-risk neonates undergoing surfactant replacement therapy. Benha J Appl Sci. 2023;8(4):23–32.
3. Wang Y. The advance treatment on neonatal respiratory distress syndrome. J Pediatr Neonatal Care. 2017;6(5):78–98. doi:10.15406/jpnc.2017.06.00262
4. Kunswa MA, Mohamed HR. Effect of instructional guidelines on nurses’ performance regarding care of high-risk neonates undergoing extubation of mechanical ventilator. Egypt J Health Care. 2021;12(2):1739–1756. doi:10.21608/ejhc.2021.234298
5. Alfarwati TW, Alamri AA, Alshahrani MA, Al-Wassia H. Incidence, risk factors and outcome of respiratory distress syndrome in term infants at academic centre, Jeddah, Saudi Arabia. Med Arch. 2019;73(3):183–186. doi:10.5455/medarh.2019.73.183-186
6. Rezaei M, Abassi B, Najib K, et al. Surfactant therapy in neonates with respiratory distress syndrome: minimally invasive surfactant therapy (MIST) or intubation-surfactant administration-extubation (INSURE). JAMA Pediatr. 2023;177(5):512–519. doi:10.1001/jamapediatrics.2023.0123
7. Shashidhar A, Rao PNS, Jose J. Downes score vs Silverman Anderson score for assessment of respiratory distress in preterm newborns. Pediatr Oncall J. 2016;13(3):66–68. doi:10.7199/ped.oncall.2016.42
8. Roberts D, Brown J, Medley N, Dalziel SR. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2017;3(3):CD004454. doi:10.1002/14651858.CD004454.pub3
9. Sahaf F, Zakariya NA. The effect of antenatal betamethasone on prevention of neonatal respiratory distress syndrome before elective cesarean section at term. J Clin Neonatol. 2021;10(4):220–226. doi:10.5005/jp-journals-10009-1767
10. Ng EH, Shah V. Guidelines for surfactant replacement therapy in neonates. Paediatr Child Health. 2021;26(1):35–41. doi:10.1093/pch/pxaa116
11. Gharehbaghi M, Moghaddam YJ, Radfar R. Comparing the efficacy of surfactant administration by laryngeal mask airway and endotracheal intubation in neonatal respiratory distress syndrome. Crescent J Med Biol Sci. 2018;5(3):222–227.
12. Reynolds P, Bustani P, Darby C, et al. Less-invasive surfactant administration for neonatal respiratory distress syndrome: a consensus guideline. Neonatology. 2021;118(5):586–592. doi:10.1159/000518396
13. Mohamed BM, El Dakhakhny AM, Bassam SEA, El Sayed LM. Assessment of nursing care provided to premature neonates at neonatal intensive care unit at Zagazig University Children Hospital. Zagazig Nurs J. 2019;7(2):1–14.
14. World Health Organization. Maternal, newborn, child and adolescent health: what is quality of care and why is it important? 2017. https://www.who.int/maternal_child_adolescent/topics/quality-of-care.
15. Ibrahim Abd El-Galil N, Mohamed Adly R, Elsayed AbdelHady H, et al. Effect of staff development program on nurses’ performance regarding quality standards of neonatal care. Egypt J Health Care. 2019;10(4):261–284. doi:10.21608/ejhc.2019.65535
16. Elsayed LA, El-Nagger NS, Aly SM. Nursing care provided for neonates with respiratory distress syndrome in the neonatal intensive care units at Makkah Al-Mukarramah in Saudi Arabia. Life Sci J. 2013;10(1):3403–3412.
17. Alfadil MA. Assessment of Nurse’s Knowledge and Practice Regarding Care of Neonate With Respiratory Distress Syndrome in Soba University Hospital [dissertation]. Mariam Mohamed Elnageeb; 2018.
18. Refat NH, Zak NA, Sayed EH, Ahmed MK. Impact of an educational program on improving nurses’ knowledge and practice concerning caring for neonates with respiratory distress syndrome. Assiut Sci Nurs J. 2020;8(22):145–152. doi:10.21608/asnj.2020.38850.1032
19. World Health Organization. WHO recommendations for care of the preterm or low-birth-weight infant. World Health Organization; 2022. https://www.who.int/publications/i/item/9789240058262.
20. Yadav S, Lee B, Kamity R. Neonatal respiratory distress syndrome. In StatPearls. StatPearls Publishing; 2020. https://www.ncbi.nlm.nih.gov/books/NBK560779/.
21. Alharbi MF, Marzouk SA, Alrashidi N, et al. Effectiveness of nurses’ training about mechanical ventilation weaning on neonatal outcomes. BMC Nurs. 2025;24(1):654. doi:10.1186/s12912-025-03257-9
22. Aziz AR, Mansi QH. Assessment quality of nursing care provided to neonates with respiratory distress syndrome at intensive care unit in Al-Nasiriyah city hospitals. Kufa J Nurs Sci. 2017;7(2).
23. Qari SA, Alsufyani AA, Muathin SH, El Margoushy NM. Prevalence of respiratory distress syndrome in neonates. Egypt J Hosp Med. 2018;70(2):257–264. doi:10.12816/0043086
24. Loutfy A, Mohamed AR, Abed Ella NH. Quality of nursing care provided for preterm infants suffering from respiratory distress syndrome. Port Said Sci J Nurs. 2014;1(2):281–295. doi:10.21608/pssjn.2014.35072
25. Condò V, Cipriani S, Colnaghi M, et al. Neonatal respiratory distress syndrome: are risk factors the same in preterm and term infants? J Matern Fetal Neonatal Med. 2017;30(11):1267–1272. doi:10.1080/14767058.2016.1210597
26. Abou-Faddan HH, Abdelaziz N. Respiratory distress and its outcome among neonates admitted to neonatal intensive care unit of Assiut University Children Hospital, Egypt. Egypt J Community Med. 2018;36(2).
27. Baseer KAA, Mohamed M, Abd-Elmawgood EA. Risk factors of respiratory diseases among neonates in neonatal intensive care unit of Qena University Hospital, Egypt. Ann Glob Health. 2020;86(1). doi:10.5334/aogh.2739
28. Niesłuchowska-Hoxha A, Cnota W, Czuba B, et al. A retrospective study on the risk of respiratory distress syndrome in singleton pregnancies with preterm premature rupture of membranes between 24+0 and 36+6 weeks, using regression analysis for various factors. Biomed Res Int. 2018;2018:1–6. doi:10.1155/2018/7162478
29. Laube M, Thome UH. Why it matters - sex differences in fetal lung development. Biomolecules. 2022;12(3):437. doi:10.3390/biom12030437
30. Seaborn T, Simard M, Provost PR, Piedboeuf B, Tremblay Y. Sex hormone metabolism in lung development and maturation. Trends Endocrinol Metab. 2010;21(12):729–738. doi:10.1016/j.tem.2010.09.001
31. Kumar TR, Suresh PM, Prasath SA. Prevalence of antenatal steroids coverage in preterm labor and its influence on neonatal respiratory morbidity and mortality in Kanyakumari district. Int J Sci Study. 2017;5(1):197–199.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.