Back to Journals » Advances in Medical Education and Practice » Volume 11
Nursing and Midwifery Students’ Viewpoints of Clinical Learning Environment: A Cross-Sectional Study
Authors Sharifipour F ![]() , Heydarpour S, Salari N
, Heydarpour S, Salari N ![]()
Received 21 March 2020
Accepted for publication 17 June 2020
Published 30 June 2020 Volume 2020:11 Pages 447—454
DOI https://doi.org/10.2147/AMEP.S253782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Forozan Sharifipour,1 Sousan Heydarpour,2 Nader Salari3
1Department of Midwifery, Faculty of Nursing and Midwifery, Kermanshah University of Medical Sciences, Kermanshah, Iran; 2Department of Reproductive Health, Faculty of Nursing and Midwifery, Kermanshah University of Medical Sciences, Kermanshah, Iran; 3Department of Biostatistics, Faculty of Health, Kermanshah University of Medical Sciences, Kermanshah, Iran
Correspondence: Sousan Heydarpour
Department of Reproductive Health, Faculty of Nursing and Midwifery, Kermanshah University of Medical Sciences, Kermanshah, Iran
Email [email protected]
Objective: To determine the viewpoints of nursing and midwifery students regarding the clinical learning environment and to identify the relationship between these viewpoints with some demographic characteristics of students.
Methods: This cross-sectional study was carried out on nursing and midwifery students (n=119) in the educational hospitals affiliated to Kermanshah University of Medical Sciences from February to June 2017. The data-gathering tools were a demographics questionnaire and the standard undergraduate clinical education environment measure. This tool comprises two main scales of learning through experiencing and social participation, with four subscales of opportunities to learn in and through work and quality of supervision, preparedness for student entry, workplace interaction patterns and student inclusion, and equal treatment. The score ranged from 25 to 125 and the higher the score the higher the quality of the educational environment. The collected data were analyzed in “Statistical Package for the Social Sciences” (Version20).
Results: The nursing and midwifery students’ viewpoint of the clinical learning environment was suboptimal. There was a significant difference between the female and male students’ viewpoints of the clinical learning environment (p=0.007). There was no significant difference between students’ viewpoints of the clinical learning environment with marital status, employment, domicile, grade-point average, and number of days of internship. Nursing students had more positive viewpoints of the clinical learning environment than midwifery students (p=0.001).
Conclusion: The results showed that the clinical learning environment was suboptimal based on the nursing and midwifery students’ perspectives. Intervention to improve the clinical learning environment is recommended.
Keywords: internship, student, nursing, midwifery, clinical learning environment, viewpoints
Introduction
A critical stage in nursing and midwifery education is clinical learning, and it plays a notable role in creating professional capabilities in the learners.1 One of the effective factors in the quality and quantity of clinical education is the clinical learning environment. Students’ learning environment encompasses all the conditions and forces through which a learning and teaching mixture is influenced. The learning environment is a psychological combination, including cognitive, cultural, social, mental, emotional, educational, and motivational factors used by the instructors and students to work with each other. The learning environment functions as a factor in learning and teaching and it can play a role in favor or against learning situations for students.3 Achieving a satisfactory learning performance is not easy without a supportive environment.2
The learning environment impacts academic performance, motivation, and psychological well-being and is an important determinant of medical students’ behavior.4 The learning environment influences students’ readiness to practice as nurses, their satisfaction with nursing, and nursing retention.5 The clinical learning environment is known as one of the most effective fields for obtaining nursing skills and understanding scientific information.6 A negative learning environment leads to burn out and empathy reduction of medical students.7
The clinical learning method based on internship is one of the key approaches to fill the gap between theoretical and practical knowledge.8 Internship is part of a program of nursing and midwifery education designed to create appropriate opportunities to increase skills in the nursing and midwifery students.9 Internship and training courses play a key role in the development of fundamental skills and professional capabilities of nurses and midwives.10 “Internship” is part of the nursing and midwifery curriculum, and it is designed to create suitable opportunities for improving the skills of using nursing and midwifery knowledge in practice.11 This approach was first developed in the late 19th century in the USA to prepare medical students for the clinical environment after graduation, so that by passing the internship, students would achieve a sort of professional maturity.12 In Iran, nursing and midwifery education is part of higher education. It is a 4-year training, the last year of which is called the internship course. During this period, students work mainly independently and with ward staff, and school clinical teachers act as supervisors. The clinical supervisors and teachers at the local hospitals are school teachers and work for the nursing and midwifery school. The students’ performance in the clinics is assessed by university clinical teachers and ward staff at the end of the students' courses.
Growing evidence has shown that there is a decline in the positive perception of clinical medical students towards the learning environment during medical training. The stability of findings across different educational settings suggests that this is a universal struggle.4,13,16 Additionally, the internship course is a new course introduced into the school of nursing and midwifery of Kermanshah. The students appear in the ward without a clinical instructor and receive a clinical education from the personnel. Regarding the importance of assessing new educational methods and the importance of clinical education, this study was conducted to determine the viewpoints of nursing and midwifery students about the clinical learning environment in educational hospitals affiliated to Kermanshah University of Medical Sciences, and to identify the relationship between students’ viewpoints with some demographic characteristics of students.
Methods
Design
This cross-sectional study was carried out from February to June 2017. After obtaining a letter of recommendation from the Research and Technology Department of the university, the authors visited the educational hospitals affiliated to Kermanshah University of Medical Sciences for sampling and filling out the questionnaire. Inclusion criteria were being an internship student and desire to participate. The exclusion criterion was a transition from other faculties. It is notable that the questionnaires were administered during the two or three last days of the internship course to the participants. The questionnaires were completed anonymously and were collected at the same time. There was no reward for participating in the study.
Settings
Study areas included educational hospitals affiliated to Kermanshah University of Medical Sciences, consisting of Motazedi (a maternity hospital), Imam Reza (the largest academic medical center in western Iran), Farabi (a neurology and psychiatry hospital), Dr. Mohammad Kermanshahi (a specialized center for children), and Imam Ali (a cardiovascular hospital) (n=130). These hospitals are located in Kermanshah, a large city in the west of Iran and the capital of Kermanshah province.
Participants
Participants consisted of all fourth-year undergraduate nursing and midwifery students (internship students) in the nursing and midwifery faculty related to Kermanshah University of Medical Sciences. One hundred and thirty students were invited to fill the questionnaire. Finally, 119 completed the questionnaire, and the response rate was 91.5% (n=119).
Data Collection Methods
The data-gathering tools included a two-section questionnaire. Section one was on demographics (eg, age, gender, domicile, major, hospital, ward, marital status, number of days of attending the ward, and grade-point average (GPA) of the three years before the internship). Section two of the questionnaire was a standard undergraduate clinical education environment measure (UCEEM). The measure was introduced in 2013 by Strand,17 in Sweden. The tool is comprised of two main scales of learning through experiencing and social participation; with four subscales of opportunities to learn in and through work and quality of supervision, preparedness for student entry, “workplace interaction patterns & student inclusion,” and equal treatment. The four subscales measure different aspects of clinical education from undergraduate students’ viewpoints based on a Likert scale. The tool is comprised of 25 statements designed based on a Likert five-point scale (1 = strongly disagree, 2 = disagree, 3 = no idea, 4 = agree, 5 = strongly agree). The minimum and maximum scores of the tool are 25 and 125, respectively, and the higher the score the higher the quality of educational environment.17 According to the standard deviation scores, the total score and the score of each subscale are categorized at three levels of optimal, moderate, and poor conventionally.18
Based on Salmani & Amirian,18 the total scores at the ranges 25–58, 56–89, and 90–125 are considered as poor, moderate, and optimal, respectively, in our study.
The first subscale (opportunities to learn in and through work and quality of supervision) is covered by 11 items and score range of 11 to 55 (scores in the ranges 11–25, 26–40, and 41–55 are considered as poor, moderate, and optimal, respectively, in our study). The second subscale “preparedness for student entry” is covered by six items with a score range from 6 to 30. (score ranges of 6–13, 14–21, and 22–30 represent poor, moderate, and optimal, respectively, in our study). The third subscale “workplace interaction patterns & student inclusion” is covered by six items with score range from 6 to 30 (score ranges of 6–13, 14–21, and 22–30 represent poor, moderate, and optimal, respectively, in our study). Finally, the fourth stage “equal treatment” is covered by two items with a score range of 2–10 (score range 2–4, 5–7, and 8–10 are considered as poor, moderate, and optimal, respectively, in our study).17 In Iran, the reliability and validity of this tool were examined by Abbasi et al in 2014, and the original four subscales of the tool were confirmed using exploratory factor analysis. Cronbach’s alpha coefficient of the translated measure was good (α=0/93).19
Statistical Analysis
Means, minimum and maximum values, and standard deviations were calculated using descriptive statistics. Results are presented as frequency counts and percentages. Data analysis was performed using Microsoft SPSS Version 20.0. Mann–Whitney and Kruskal–Wallis tests were used to determine the relationship between students’ viewpoints, about the clinical learning environment and demographic characteristics. A cut-off level for statistical significance using a p-value level of 0.05 was considered.
Ethical Approval
This study was approved by the Ethical Committee of the Kermanshah University of Medical Sciences (KUMS.REC.1396.245). In addition, although the authors are educators at the faculty, they did not play any role in the teaching of clinical sections and student training classes. The participants were briefed at first about the objectives, and expressed their written informed consent to participate. Participation was voluntary.
Results
The mean age of students was 24 years (20–48) and 45 students (37.8%) were nursing students. Thirty-five students (29.4%) were married, 19 students (16%) were men, and 11 students (9.2%) were employed. All the midwifery students were women and in total, 62.2% (n=74) of the participants were women. In terms of domicile, 42% (n=50) lived in dormitories and 49.6% (n=59) of the students were at Motazedi Hospital for their internship course. The mean GPA of the past three years of the students was 16.64 (out of 20), and the students spent 10.94 days at hospitals on average (Table 1).
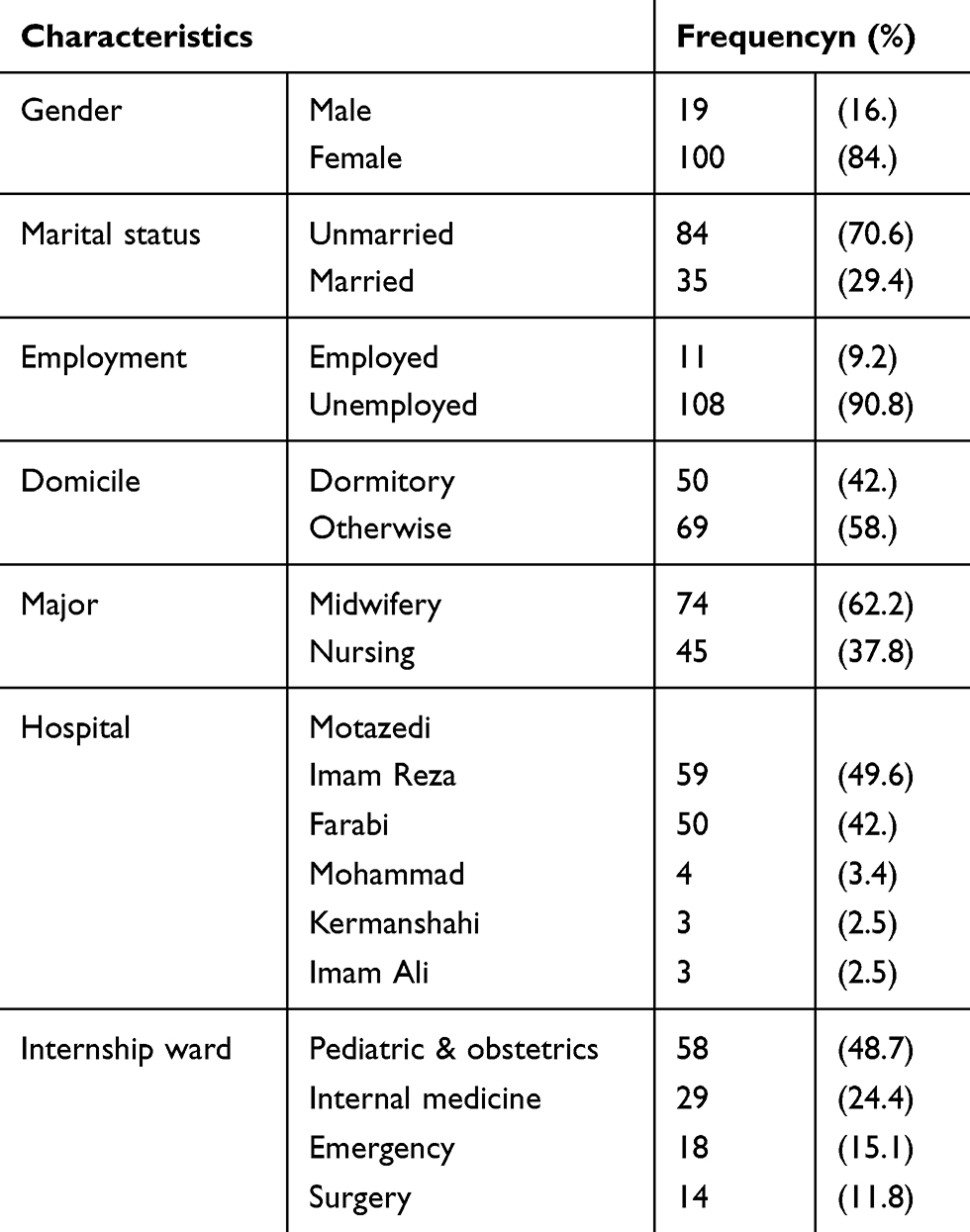 |
Table 1 Characteristics of Participating Students (n=119) |
The total score for students’ perceptions was 79.92 ± 15.48 that generally tend to be sub-optimal. Table 2 shows the maximum score of total UCEEM and its four subscales, mean and standard deviation, of all domains. The highest score was found in the subscales of opportunities to learn in and through work and quality of supervision (mean: 33.88, standard deviation: 7.61) and the lowest in the subscales of equal treatment (mean: 7.5, standard deviation: 2.06) (Table 2).
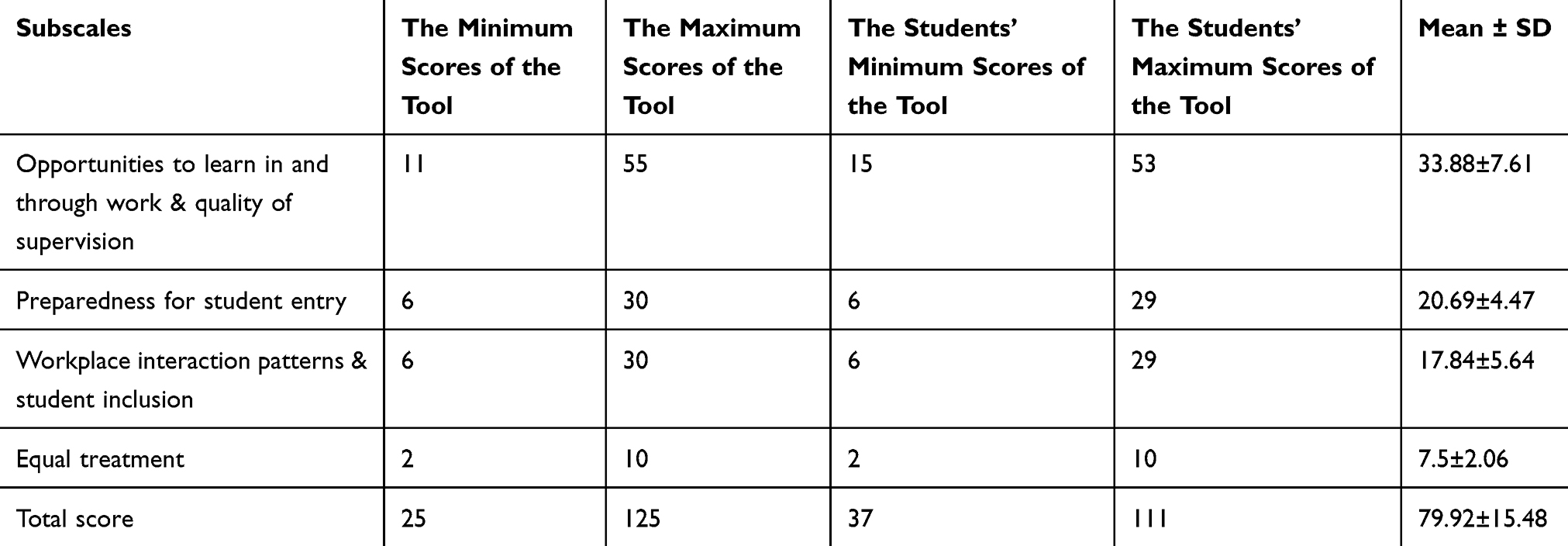 |
Table 2 The Viewpoints of Nursing and Midwifery Students About Clinical Learning Environment |
The relationship between students’ viewpoints of CLE and some of their characteristics was determined. Kruskal–Wallis test revealed a significant difference between students’ viewpoints of CLE with their internship wards (p=0.001) so that students in the pediatric and obstetrics wards had the most negative views, and they had the most positive views in the surgery ward.
In addition, there was a significant difference between the average score of opportunities to learn in and through work and quality of supervision and workplace interaction patterns and student inclusion subscales in terms of internship ward (p=0.001). However, there was no significant difference between the average score of preparedness for student entry and equal treatment subscales in terms of the internship ward (p≥0.05).
The results of the Mann–Whitney test showed that there was a significant difference between the female and male students’ viewpoints of CLE (p=0.007). In general, boys were more positive than girls. There was no significant difference between students’ viewpoints of the clinical learning environment with marital status, employment, domicile, GPA, and the number of days of internship (p>0.05). However, nursing students had a more positive viewpoint of CLE than midwifery students (p=0.001). (Table 3).
 |
Table 3 The Relationship Between Nursing and Midwifery Students’ Viewpoints About Clinical Learning Environment with Demographic Characteristics |
Discussion
Results showed that nursing and midwifery students’ viewpoint regarding clinical learning environment was suboptimal and the students rated the learning environment more positively than negatively and the total and subscale scores of the undergraduate clinical education environment measure (UCEEM) suggest that the students were relatively satisfied with the learning environment. Few studies have been conducted in Iran about evaluating the clinical learning environment of nursing and midwifery students. Consistent with our results, Abbasi et al found that nursing and midwifery students assess the CLE as suboptimal.20 Other studies in Iran reported that nursing students were not satisfied with their CLE.21,22 Moreover, in Kuwait, Karim et al found that undergraduate medical student’s viewpoint of CLE was suboptimal.23 In Hong Kong, Chan & IP found that nursing students’ viewpoints of their CLE were not ideal, and they were not satisfied with it.24 However, nursing students had a more positive view of their CLE in studies conducted in England and Australia.25,26 In addition, Robert D. Perry et al stated that students perceived their CLE positively.27 The study of Ezeala et al showed that the students rated the learning environment more positively and the total and subscale scores of the Dundee Ready Education Environment Measure (DREEM) suggest that the students were satisfied with the learning environment.28 Safari-Moradabadi et al found that 23 female dental students had a very positive attitude to the learning environment.29 This difference can be due to the tools used, the sample size, a different clinical environment, and students’ majors. Moreover, the discrepancy in human resources and educational technologies between developed and developing countries can account for this difference.30
The findings of the present study showed that the subscale of “opportunities to learn in and through work & quality of supervision” had the highest scores, which is consistent with the Strand study.17 Khorasani et al stated that quality of supervision is the most effective factor in clinical education.31 When clinical instructors’ performance is not matched with students’ expectations, the motivation of the instructor to teach, and the students to learn are affected.32 Various studies have introduced different roles for clinical instructors, showing that some students have taken them as spiritual guides.33 Other roles like that of a supporter, guide, motivator, facilitator, and advisor have been mentioned for clinical instructors.34 With regard to surveying the quality of instruction, a study at Tabriz University of Medical Sciences showed that the relationship between the instructor and students was the main barrier in clinical education.35 Another survey showed that the type of interaction between students and instructors might create a sense of support or lack of support.18 Taking into account and assessing the performance of clinical instructors has a notable effect on students’ learning, as nursing and midwifery students find instructors as a reliable source for learning.30 However, Abbasi et al reported that the scores of “opportunities to learn in and through work and quality of supervision” and “preparedness for student entry” subscales were the same,20 which is inconsistent with our study and that of Strand.17 Another study reported that the students evaluated “opportunities to learn in and through work & quality of supervision” as moderate and noted that lack of learning opportunity through the clinical environment was one of the barriers to the empowerment of students.18 Although the main domain of the educational environment is different between studies, it seems that creating learning opportunities at clinical LE is a necessity.
In terms of preparedness for student entry, “readiness to accept students,” the students found the readiness at a moderate level in hospitals. This finding is consistent with other studies.20,35 In another study, students reported that the facilities available at the clinical learning environment for educational purposes were not at a desirable level despite their importance.36
In our study, “workplace interaction patterns & student inclusion” was not optimal; which is consistent with Abbasi et al.20 It is notable that students in both studies gave the same score to this subscale. The positive environment of the ward and teamwork are effective in the learning performance of students.37,38 Lili Jedhal et al reported that the sense of belongingness, welcoming students when they enter the ward for the first time, teamwork, and student-centered supervision were prerequisites of efficient learning and care to the patient.39
Students gave the lowest scores to the “equal treatment” subscale of the UCEEM. This finding is consistent with other studies.17,20
In our study, the relationship between students’ viewpoints regarding the clinical learning environment with some demographic characteristics of students was determined. The results showed a significant difference in the perspective of nursing and midwifery students, and nursing students had a more positive perception compared with midwifery students. This finding is consistent with Salimi et al, who reported that there was a significant difference between nursing and midwifery students in terms of learning environment viewpoints so that the nursing students had a more positive view than the midwifery students.40
The facts that all midwifery students were girls, that there was a discrepancy in the clinical environment of nursing and midwifery students, and also that the educational approach of the clinical instructors was different in the clinical learning environment may explain the difference in the views of nursing and midwifery students. Robert et al (2017) reported that obstetrics and gynecology wards obtained the lowest scores in terms of the clinical education environment.41 Consistent with Abbasi et al, there was no significant difference in students’ viewpoints based on marital status.20
There was a significant relationship between the students’ viewpoints on the internship ward and the days of attendance in the wards. Abbasi et al reported that the number of days of attending in wards and type of hospital were not significantly related to the student’s viewpoints.20 This can be due to prior experience among the students with internship and similarities or differences in hospitals. There was a significant difference in students’ viewpoints towards the clinical learning environment based on gender. The male students’ viewpoints towards CLE were more positive compared with the female students. Karim et al found that a better learning environment is provided for male students than female students at medical schools of Kuwait and Saudi Arabia, while the opposite was provided by Dundee University23 It seems that the context in which students learn is affected by culture.
There was no significant difference between students’ viewpoints with employment, domicile, GPA of the past three years, and mean days of internship. Abbasi et al reported that there was no significant difference in the clinical learning environment in terms of GPA of the past three years, and average days of internship.20 This may be due to previous students’ experiences before entering the internship plan and the same nature of the hospitals.
Limitations
The study limit was the impossibility to more deeply discuss the quantitative results due to the lack of data related to the personal experience of students. In this regard, a multi-method approach is recommended rather than just a qualitative one. In the study, only the viewpoint of nursing and midwifery students of Kermanshah nursing and midwifery faculty was assessed. So, we suggest that in future studies, the viewpoint of nursing and midwifery instructors regarding the quality of CLE is assessed.
Conclusion
We found that nursing and midwifery students’ viewpoint of the clinical learning environment was suboptimal. It is suggested that clinical education is provided by experienced instructors with good communication skills. In addition, providing facilities and equipment in wards and hospitals, promoting a positive atmosphere and teamwork, improving interaction skills in nursing and midwifery students, and improving learning opportunities in the clinical education environment is recommended.
Acknowledgment
This research is registered under the research plan No.96234 in Kermanshah University of Medical Sciences. The authors wish to express their gratitude to the Department of Research of the university for the financial support of the work. The authors also thank the students in the School of Nursing and Midwifery for participation in the study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data, and also they took part in drafting the article and revising it critically for important intellectual content. In addition, they gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflict of interests.
References
1. Delaram M, Reisi Z, Alidusti M. Strengths and weaknesses of clinical education from the viewpoints of nursing and midwifery students in Shahrekord University of Medical Sciences, Shahrekord, Iran. Qom Univ Med Sci J. 2012;6(2):76–81.
2. Cook J. The role of the virtual learning environments in UK medical education. J Theoretical Appl Phys. 623:1–10.
3. Sand-Jecklin KE Student Evaluation of Clinical Education Environment (SECEE): instrument development and validation. Thesis Ph.D. Morgantown: School of Nursing, West Virginia University 1998: 25–30.
4. Roslan NS, Mohammad JA-M, Ismail M-A-A, Ahmad A, Yusoff MSB. Rethinking education environment: the clinical education environment framework. Educ Med J. 2018;10(3):31–46. doi:10.21315/eimj2018.10.3.4
5. Flott EA, Linden L. The clinical learning environment in nursing education: a concept analysis. J Adv Nurs. 2015;72(3):501e13.
6. Thorell-Ekstrand I, Bjorvell H. Nursing students’ experience of care planning activities in clinical education. Nurse Educ Today. 1995;15(3):196–203. doi:10.1016/S0260-6917(95)80106-5
7. Brazeau CMLR, Schroeder R, Rovi S, Boyd L. Relationships between medical student burnout, empathy, and professionalism climate. Acad Med. 2010;85(10 SUPPL.):33–36. doi:10.1097/ACM.0b013e3181ed4c47
8. Wallace J. Nursing student work-study internship program: an academic partnership. J Nurs Educ. 2016;55(6):357–359. doi:10.3928/01484834-20160516-11
9. Miles S, Leinster S. Medical student’s viewpoints of their educational environment: expected versus actual viewpoints. Med Educ. 2007;41:265–272.
10. Shabani H. Maharathayeamoozeshivaparvareshi (Raveshhavafonoonetadris).
11. Lockwood-Rayermann S. Preceptor leadership style and the nursing practicum. J Prof Nurs. 2003;19(1):32–37. doi:10.1053/jpnu.2003.7
12. Wentz DK, Ford CV. A brief history of the internship. JAMA. 1984;252(24):3390–4.12. doi:10.1001/jama.1984.03350240036035
13. Dunham L, Dekhtyar M, Gruener G, et al. Medical student viewpoints of the learning environment in medical school change as students transition to clinical training in undergraduate medical school. Teach Learn Med. 2017;29(4):383–391. doi:10.1080/10401334.2017.1297712
14. Yusoff MSB, Jaa’far R, Arzuman H, Arifn WN, Mat PMN. Viewpoints of medical students regarding educational climate at different phases of medical training in a Malaysian medical school. J Med Educ. 2013;5(3):30–41. doi:10.5959/eimj.v5i3.146
15. McKee A, Markless S. Using action learning sets to support students managing transition into the clinical learning environment in a UK medical school. Action Learn. 2017;14(3):275–285. doi:10.1080/14767333.2017.1360933
16. Seabrook M. Clinical students’ initial reports of the educational climate in a single medical school. Med Educ. 2004;38:659–669. doi:10.1111/j.1365-2929.2004.01823.x
17. Strand P. Development and psychometric evaluation of the Undergraduate Clinical Education Environment Measure (UCEEM). Med Teach. 2013;35:1014–1026. doi:10.3109/0142159X.2013.835389
18. Salmani S, Amirian H. Comparison between nursing students and trainers viewpoints about clinical educator environment in Islamic Azad university of Yazd. Strides Devel Med Educ. 2006;1(3):11–18.
19. Abbasi Z, Ahmadi S, Esmaeilpourzanjani S, Peyman P. A psychometric properties of the undergraduate clinical educational environment measure UCEEM in Iranian nursing and midwifery students. Eur Proc Educ Soc Sci. 2015;3:38–41.
20. Abbasi Z, Ahmadi S, Esmaeilpour-zanjani S, Payman A, Far -mahini -frahani M. Nursing and Midwifery Students viewpoints of clinical learning environment of Tehran Medical Sciences branch of Islamic Azad University using undergraduate clinical education environment measure. Med J Azad Univ. 2016;1(26):61–65.
21. Zaighami R, Faseleh M, Jahanmiri S, Ghodsbin F. Nursing student’s viewpoints about the problems of clinical teaching. J Qazvin Univ Med Sci. 2004;30.
22. Shahbazi L, Salimi T. Attitudes of nursing and midwifery students on clinical status; 8(2): 97-103. J Shahid Sadoughi Univ Med Sci Health Serv. 2000;8(2):97–103.
23. Karim J, Al-halabi B, Marwan Y, Sadeq H, Dawas A, Al-Abdulrazzaq D. The educational environment of the undergraduate medical curriculum at Kuwait University. Advan Med Educ Pract. 2015;6:297–303. doi:10.2147/AMEP.S81729
24. Chan DS, WY IP. Perception of hospital learning environment: a survey of Hong Kong nursing students. Nurse Educ Today. 2007;27(7):677–684. doi:10.1016/j.nedt.2006.09.015
25. Midgley K. Pre-registration student nurses perception of the hospital-learning environment during clinical placements. Nurse Educ Today. 2006;26(4):338–345. doi:10.1016/j.nedt.2005.10.015
26. Dunn SV, Hansford B. Undergraduate nursing students’ viewpoints of their clinical learning environment. J Adv Nurs. 1997;25(6):1299–1306. doi:10.1046/j.1365-2648.1997.19970251299.x
27. Robert D, Perry A, Madeline M, et al. Pilot study: nursing students’ viewpoints of the environment in two different clinical models. Int J Nurs Sci. 2016;3:2 8 5 e2 9 0.
28. Ezeala Christian C, Moleki MM, Shula H, Goma Fastone M. Issues in the learning context of undergraduate physiotherapy programme at a premier medical school in Zambia. J Med Educ Summer. 2017;16(3):188–195.
29. Safari-Moradabadi A, Kasmaei P, Khalfe Nilsaz M, et al. Evaluation of the learning environment based on the dundee ready education environment measure model from the perspective of primary school students in Roudsar City. J Res Med Dental Sci. 2018;6(1):140–145. doi:10.24896/jrmds.20186122
30. Rahmani A, Zamanzadeh V, Abdullah-zadeh F, Lotfi M, Bani S, Hassanpour S. Clinical learning environment in viewpoint of nursing students in Tabriz University of Medical Sciences. Iran J Nurs Midwifery Res. Summer; 2011;16(3):253–256.
31. KhorasaniGh A, Mahmoudi M, Vahidshahi C, Shahbaznezhad L, GhaffariChraty M. BarrasyekeifiateamoozeshedarmangahiazdidgaheasatidvadaneshjooyanedaneshkadeyepezeshkyedaneshgaheoloompezeshkyeMazandaran 1385. J Mazandaran Univ Med Sci. 2007;58(17):87–100.
32. Azizi F. Medical Education. Tehran: Ministry of Health and Medical Education; 2003.
33. Guzman A, Pablo LA, Prieto RJ, Purificacion VN, Que JJ, Quia P. Understanding the persona of clinical instructors: the use of students’ doodles in nursing research. Nurse Educ Today. 2008;28(1):48–54. doi:10.1016/j.nedt.2007.02.012
34. Poor Man SG, Webb CA, Mastorovich ML. Students’ stories: how faculty help and hinder students at risk. Nurse Educ. 2002;27(3):126–131. doi:10.1097/00006223-200205000-00010
35. Meimandi K, Alavi M, Abedi HA. The comparison of student’s and teacher’s viewpoint about clinical education for evaluating of quality education in Beheshti University of medical sciences. Iran J Med Educ. 2008;7:325–334.
36. Hadizadeh F, Firoozi M, Shamaeyan Razavi N. Nursing and midwifery students perspective on clinical education in Gonabad University of Medical Sciences. Iran J Med Educ. 2005;5(1):70–78.
37. Tiwari A, Lam D, Yuen K, Chan R, Fung T, Chan S. Student learning in clinical nursing education: viewpoints of the relationship between assessment and learning. Nurse Educ Today. 2005;25(4):299–308. doi:10.1016/j.nedt.2005.01.013
38. Sand-Jecklin KE Student evaluation of clinical education environment (SECEE): instrument development and validation [Dissertation]. Morgantown: School of Nursing, West Virginia University 2007.
39. Liljedahl M, Boman LE, Fält CP, Laksov KB. What students really learn: contrasting medical and nursing students’ experiences of the clinical learning environment. Advan Health Sci Educ. 2015;20(3):765–779. doi:10.1007/s10459-014-9564-y
40. Salimi T, Khodayarian M, Rajabioun H, et al. A survey on viewpoints of nursing and midwifery students and their clinical instructors at Faculty of Nursing and Midwifery of ShahidSadoughiUniversity of Medical Sciences towards clinical education during 2009-2011. J Med Educ Devel. 2012;7:67–78.
41. Roberts R, Cleland J, Strand P, Johnston P. Medical students’ views of clinical environments. Clin Teach. 2017. doi:10.1111/tct.12691.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.