Back to Journals » International Journal of Women's Health » Volume 17
Nurse-Led Evidence-Based Practice to Promote Gastrointestinal Function Recovery in Women After Cesarean Delivery
Authors Lin L, Chen P, Wan T, Xie G, Wang P, Yan X, Li R, Chen W ![]() , Zhang W
, Zhang W
Received 4 July 2025
Accepted for publication 25 October 2025
Published 12 November 2025 Volume 2025:17 Pages 4399—4408
DOI https://doi.org/10.2147/IJWH.S551653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Lin Lin,1,* Peng Chen,1,* Ting Wan,1 Guixiang Xie,1 Peihong Wang,1 Xin Yan,2 Ruimin Li,3 Wei Chen,4 Wen Zhang1
1Department of Obstetrics and Gynecology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 2Department of Anesthesiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 3Department of Traditional Chinese Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 4Department of Pharmacy, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen Zhang, Email [email protected] Wei Chen, Email [email protected]
Objective: This study aims to help women recover their gastrointestinal function after a cesarean delivery. We will use a nurse-led, evidence-based approach and evaluate how well it works in a clinical setting.
Methods: Using the continuous quality improvement model, evidence was translated into clinical quality audit indicators to develop interventions. These interventions compared the implementation of evidence-based practices before (August - December 2023) and after (March - July 2024) enhancing medical staff’s knowledge. The aim was to improve the execution rate of indicators related to gastrointestinal function recovery. Key variables analyzed included perioperative fasting duration, pain (VAS), anxiety (GAD-7), time to first flatus, and incidences of thirst, hunger, nausea/vomiting, and abdominal distension.
Results: The study incorporated sixteen pieces of evidence and established eighteen review criteria. A comparative analysis conducted before and after the implementation of evidence-based practice revealed a significant increase in the evidence-based assessment score for healthcare professionals regarding the promotion of post-caesarean gastrointestinal function recovery, with scores rising from 57.84 ± 7.50 to 90.00 ± 7.07 points (P < 0.01). Additionally, the execution rate of all eighteen review criteria showed significant improvement (P < 0.05). The time to first anal exhaust was reduced from 32.19 ± 20.48 hours to 20.25 ± 8.14 hours (P < 0.01). Furthermore, the incidence of thirst decreased from 56.41% to 23.81% (χ2 = 35.97, P < 0.01), hunger from 48.72% to 16.67% (χ2 = 38.13, P < 0.01), nausea or vomiting from 35.90% to 11.90% (χ2 = 25.93, P < 0.01), and bloating from 27.56% to 14.29% (χ2 = 8.70, P = 0.003).
Conclusion: The implementation of nurse-led, multidisciplinary evidence-based practice effectively facilitates gastrointestinal recovery and improves postoperative comfort and satisfaction among women following elective caesarean section.
Keywords: elective cesarean delivery, gastrointestinal function, nursing, evidence - based practice
Corrigendum for this paper has been published.
Introduction
An elective cesarean delivery is a pre-planned surgical procedure performed prior to the onset of labor when both the pregnant woman and the fetus are in stable condition, and clinical indications for a cesarean delivery exist.1 Postoperative gastrointestinal dysfunction is a possible complication associated with cesarean deliveries. The global rate of cesarean deliveries is on an upward trajectory, anticipated to reach 29% by 2030.2 The incidence of postoperative abdominal distension is notably high, occurring in approximately 40% of cases, while the incidence of intestinal functional obstruction or dysfunction ranges from 26% to 31%.3 Common symptoms include nausea, vomiting, abdominal distension, abdominal pain, diarrhea, constipation, insomnia, and fever. These complications not only result in inadequate nutritional intake and reduced immunity in postpartum women, adversely affecting recovery and neonatal breastfeeding, but also extend hospital stays and escalate healthcare costs.
International research on the recovery of gastrointestinal function following cesarean deliveries predominantly focuses on the Enhanced Recovery After Surgery (ERAS) protocol. In 2021, the Society for Obstetric Anesthesia and Perinatology (SOAP) issued the “Consensus Statement and Recommendations on Enhanced Recovery After Cesarean (ERAC)”, which underscores the importance of early ambulation and the minimization of opioid use.4 This statement also endorses early postoperative gum chewing as a straightforward, cost-effective, and safe intervention to expedite gastrointestinal recovery, a practice that has gained widespread acceptance. The 2025 guidelines from the ERAS Society structure perioperative care for cesarean delivery into three distinct phases: preoperative preparation, intraoperative management, and postoperative recovery. A key recommendation to facilitate gastrointestinal recovery includes strategies like shortened preoperative fasting and the encouragement of early oral intake postoperatively.5–7 Furthermore, the Traditional Chinese and Integrated Medicine Branch of the China Maternal and Child Health Association released the “Clinical Practice Guidelines for Integrated Traditional Chinese and Western Medicine in Preventing and Treating Postoperative Gastrointestinal Dysfunction. (2023 Edition)”.8 These guidelines incorporate non-pharmacological therapies, including acupoint heat therapy, transcutaneous electrical acupoint stimulation (TEAS), and acupuncture. Despite the existence of numerous guidelines for enhanced recovery after cesarean delivery, conventional care demonstrates limited efficacy in ameliorating delayed gastrointestinal function recovery, thereby necessitating the investigation of multimodal intervention programs.
Although the ERAS guidelines recommend specific evidence-based practices such as early feeding, mobilization, and multimodal analgesia, their clinical adoption remains suboptimal. A survey of 71 hospitals in Guangxi Province, China, revealed that only 25 (35.2%) had implemented an ERAS protocol for cesarean delivery.9 This study is conducted in the obstetrics ward of a tertiary first-class hospital in Wuhan, Hubei Province, China, where over 4000 cesarean deliveries are performed annually. Significant variations persist in perioperative nursing care for patients recovering from cesarean delivery, particularly in multidisciplinary collaboration among obstetrics, anesthesiology, and nutrition services. Inconsistent practices - such as adherence to preoperative fasting guidelines, the timing of postoperative ambulation, and the use of proactive measures to stimulate gastrointestinal recovery-highlight the absence of standardized, evidence-based protocols. This heterogeneity underscores the critical need for nurse-led initiatives to coordinate care and establish uniform intervention pathways across disciplines.
A retrospective audit conducted from June to December 2023 indicated that 38% of patients experienced delayed gastrointestinal recovery, defined as the first flatus occurring more than 24 hours post-surgery. This finding is concerning, as these measures are critical for promoting recovery and reducing complications. Research demonstrates that comprehensive nursing interventions that integrate both Western and Traditional Chinese Medicine practices can significantly enhance postoperative outcomes.10,11 Consequently, a working group has been established to develop standardized nursing protocols aimed at improving gastrointestinal function recovery following cesarean deliveries.
This study implemented a continuous quality improvement model, convening a task force to design a standardized nursing protocol. This model empowered nurses to lead systematic assessment, warning triggers, and multidisciplinary coordination. We then evaluated the framework’s effectiveness by comparing outcomes before and after implementation.
Methods
Literature Review and Review Indicators Confirmation
The evidence retrieval process was systematically executed in accordance with the “6S” evidence pyramid model. A comprehensive search strategy was formulated utilizing both controlled vocabulary (MeSH terms) and free-text keywords across the PubMed, Cochrane Library, and EMBASE databases. The search strategy integrated three conceptual domains using Boolean operators: (1) Population: (“cesarean delivery” OR “Obstetric Surgical Procedures”) AND “Elective Surgical Procedure”; (2) Intervention: (“Enhanced Recovery After Surgery” OR “Perioperative Care”) OR (“early feeding” OR “chewing gum”); (3) Outcome: (“Gastrointestinal Motility” OR “Intestinal Absorption” OR “Postoperative Ileus/prevention and control”). The search was restricted to clinical trials and systematic reviews published from 2013 to 2023. Ultimately, 12 articles were included, encompassing 7 guidelines and 5 expert consensuses.5–7,12–15, The evidence appraisal was conducted by one methodology expert and one clinical expert. Two evaluators independently assessed each article, and in instances of disagreement, a third researcher was consulted to arbitrate and make a final determination. Sixteen pieces of evidence for enhancing intestinal function recovery after elective cesarean deliveries were identified across pre-operation, intra-operation, and post-operation stages.16
The Evidence Evaluation Team used the FAME framework.17 Feasibility, Appropriateness, Clinical significance, and Effectiveness) to assess and incorporate 15 pieces of evidence, resulting in 18 review indicators (Table 1). For review indicators 1–3 and 11–17, a designated person administers the “Promoting Elective Cesarean Gastrointestinal Function Recovery Questionnaire” to postpartum mothers on the second day after surgery. This questionnaire assesses mothers’ adherence to guidelines for improving gastrointestinal function and the implementation of these guidelines by medical staff. Indicators 4–10 and 18 are gathered by reviewing medical records, including physician orders for analgesics, anti-nausea drugs, postoperative infusions, gastrointestinal motility drugs.
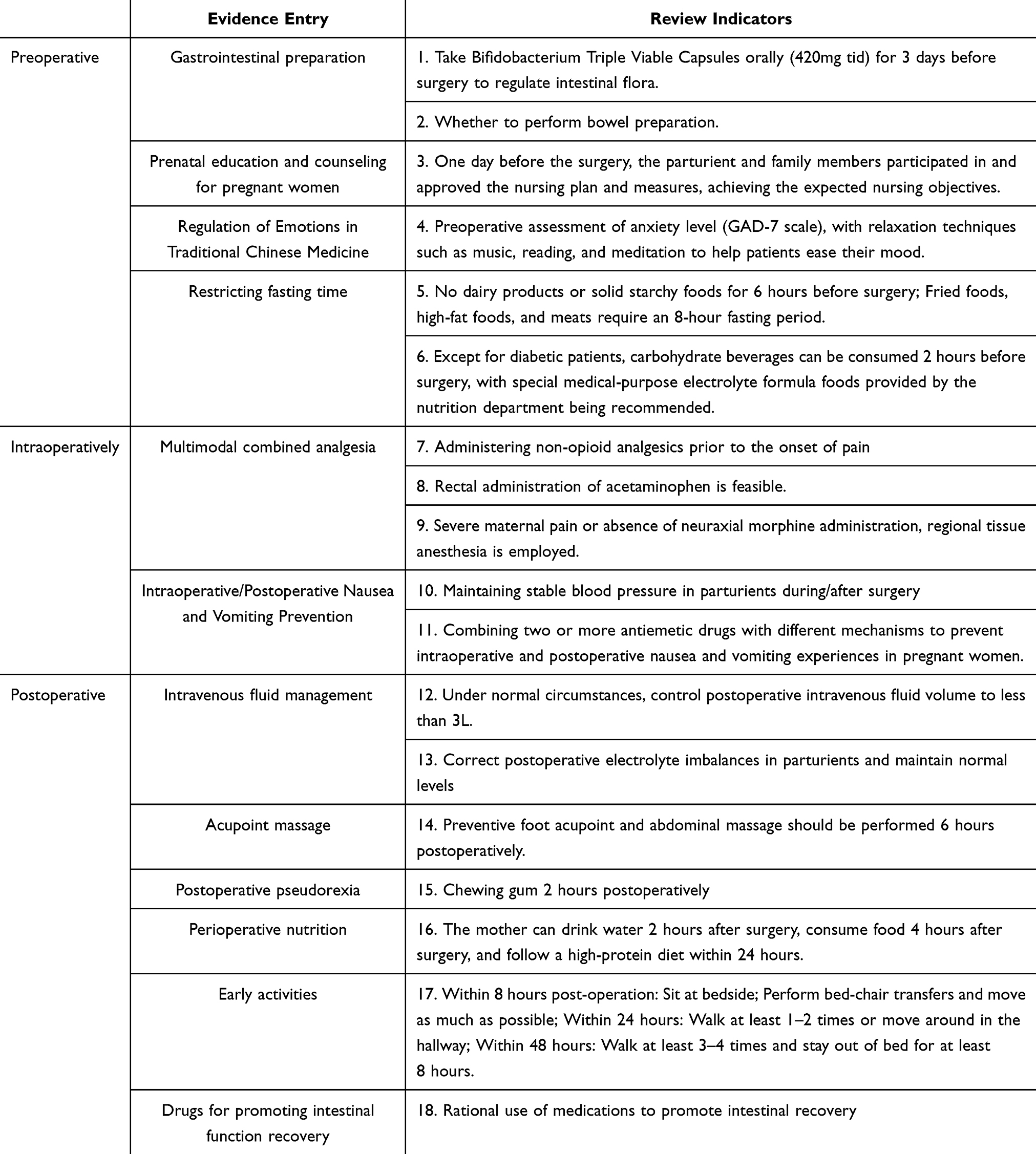 |
Table 1 Evidence on Promoting Gastrointestinal Function Recovery After Elective Cesarean Section and Review Indicators |
After reviewing the indicators, we identified key barriers to delayed gastrointestinal recovery: 1) Lack of timely communication across departments; 2) Medical staff’s insufficient evidence-based knowledge, leading to extended fasting times; 3) Inadequate health education systems with non-standardized content and missing informed consent; 4) Poor post-cesarean pain management, hindering early mobility; 5) Prolonged use of analgesic pumps and delayed catheter removal, limiting early activity. We will implement targeted interventions based on these findings.
Implementation of Evidence-Based Practice
Research Subject
The primary research subjects are pregnant women undergoing elective cesarean deliveries, with medical staff as secondary subjects. Inclusion criteria for the women are age 18 or older, elective cesarean, no gastrointestinal or psychiatric disorders, and normal communication. Exclusion criteria include emergency surgery post-admission, severe post-surgery complications, or ICU transfer. Medical staff includes nurses, obstetricians, anesthesiologists, nutritionists, and traditional Chinese medicine doctors, excluding those off duty during the survey.
Interference Measures Confirmation and Implementation Methods
Based on an analysis of the factors impeding the recovery of gastrointestinal function following cesarean deliveries, we have developed targeted intervention strategies. A nurse-led, evidence-based taskforce was established, consisting of obstetricians, anesthesiologists, dietitians, pharmacists, and rehabilitation therapists. The roles within the taskforce were delineated as follows: Obstetric nurses were responsible for coordinating perioperative care and implementing gastrointestinal monitoring protocols, including the timing of first flatus and defecation, as well as the incidence of nausea and vomiting. Anesthesiologists administered multimodal analgesia, utilizing a spinal-epidural combination, and provided prophylaxis for postoperative nausea and vomiting (PONV). Dietitians developed phased nutritional plans, offering lactose-free alternatives for patients with lactose intolerance. Rehabilitation specialists guided acupoint massage, focusing on Zusanli (ST36) and Hegu (LI4), and advised on activity progression. Theoretical training was delivered through hybrid modules that covered ERAS guidelines, traditional Chinese medicine (TCM) interventions, and conflict resolution strategies. Skill validation involved TCM specialists demonstrating standardized acupressure techniques, while scenario simulations were used to assess protocol adherence in the presence of complications.
Structured patient education encompasses several stages. Pre-operatively, within 24 hours prior to surgery, patients receive individualized counseling focused on activity milestones, which include a timeline from bedside activities to ambulation, as well as dietary progression from clear fluids to solid food intake criteria. In the immediate postoperative period, from 0 to 6 hours, bedside demonstrations and verbal instructions are provided to guide patients through the timeline for postnatal recovery, including steps such as turning over, sitting up, getting out of bed, passing gas, and defecating. Patients are also shown the proper method for drinking water, emphasizing small, slow sips. From 6 to 24 hours post-operation, patients are encouraged to scan a QR code to access instructional videos and synchronize their activities with the duty nurse. Visual aids, such as the dietary pyramid diagram, are utilized to indicate the types of food permissible at each postoperative stage. Additionally, portable acupoint positioning cards are used to identify acupoints like Zusanli and Hegu, providing guidance on acupoint and abdominal massage techniques. Discharge planning includes the use of symptom surveillance checklists, advising patients to seek medical attention if symptoms such as bloating exceed a score of 6 on the Visual Analog Scale (VAS).
Early Mobilization Protocol: To standardize the pain assessment process, a visual analog scale (VAS) is employed to establish a dynamic assessment system. Assessment intervals include routine evaluations at 6, 12, and 24 hours post-operation, as well as immediate reassessments prior to any positional changes or ambulation. Postoperative analgesic medications should be administered based on the pain level to maintain VAS scores at or below 3 points. Acetaminophen can be used as a foundational analgesic, administered either intravenously or orally. If potent neuraxial morphine analgesia is not utilized, consideration should be given to local anesthetic wound infiltration or the implementation of regional nerve blocks, such as a transversus abdominis plane block or a quadratus lumborum block, to enhance analgesic efficacy. The protocol also includes standardized procedures for early removal of the urinary catheter, scheduled 12 hours post-operation (between 08:00 and 10:00), to prevent disruptions to maternal sleep and reduce the risk of falls. The Structured Early Mobilization Protocol for Post-Cesarean Recovery is divided into three phases. Phase I (0–8 hours postoperative) involves positioning the patient in a Semi-Fowler position (30–45° elevation) without enforcing a supine posture. Bed-based activities include axial turning maneuvers every 2 hours, ankle pump exercises (10 repetitions per hour), and bed-to-chair transfers with assistive devices. Phase II (8–24 hours postoperative) includes an ambulation protocol with assisted hallway walking sessions, at least twice daily, covering a minimum of 50 meters per session. Phase III (24–48 hours postoperative) sets activity targets with a goal of ≥8 hours of out-of-bed time per day, monitored using wearable accelerometers. Independent ambulation ≥3 sessions/day (6-Minute Walk Test distance ≥100m).
Indicator Evaluation
A self-developed questionnaire was used to evaluate healthcare professionals’ knowledge, attitudes, and compliance with evidence-based practices for enhancing bowel function recovery after elective cesarean deliveries. The questionnaire includes 20 questions, each worth 5 points, totaling 100 points. A higher score indicates better knowledge.
To assess the compliance rate with indicators for promoting gastrointestinal function recovery in mother’s post-elective cesarean delivery, behaviors or phenomena meeting the criteria are recorded as “Y”, those not meeting the criteria as “N”, and those not applicable as “NA”. The compliance rate is calculated as: Compliance Rate = (Number of Y responses) / (Number of Y + N responses) × 100%.
In this study, we conducted a comparative analysis of preoperative and postoperative fasting and water deprivation durations among maternal patients, both prior to and following the implementation of evidence-based practices. We evaluated maternal experiences by measuring pain using the Visual Analogue Scale (VAS) and psychological well-being using the Generalized Anxiety Disorder 7-item (GAD-7) scale. A statistical analysis was performed to assess daily maternal gastrointestinal recovery, focusing on parameters such as time to first anal exhaust, as well as the incidence of thirst, hunger, nausea or vomiting, and bloating.
Results
Clinical Characteristics of Elective Cesarean Delivery Patients
The study cohort comprised 156 pregnant women before the adoption of evidence-based practices, with a mean age of 31.72±4.16 years, a mean gestational age of 38.55±1.19 weeks, and a mean operation duration of 1.37±0.28 hours. Following the implementation of evidence-based practices, 168 pregnant women were included, with a mean age of 31.69±3.42 years, a mean gestational age of 38.08±1.46 weeks, and a mean operation duration of 1.38±0.29 hours. Statistical analysis revealed no significant differences in maternal age, gestational age, or operation time before and after the implementation of evidence-based practices (P>0.05).
Assessment Results of Medical Staff
The evaluation of evidence-based knowledge among healthcare professionals concerning the facilitation of bowel function recovery in patients following elective cesarean deliveries was conducted. The study comprised 44 healthcare professionals, with 28 participants from the obstetrics and gynecology department and 16 from other departments. Two assessments were administered: one prior to and one following the implementation of evidence-based practice. The questionnaire content for investigating gastrointestinal function recovery after elective cesarean delivery among medical staff can be found in Table S1. Initially, the mean assessment score for healthcare professionals on promoting bowel function recovery in post-elective cesarean delivery patients was 57.84±7.50 points. Following the implementation of evidence-based practice, the mean score increased to 90.00±7.07 points, with the difference being statistically significant (t=−20.15, P<0.01).
Implementation Rate of Review Criteria
This project initially included a total of 18 review indicators. During the baseline assessment, only 2 indicators achieved an execution rate of 100.00%, while 3 indicators had an execution rate of 0. The remaining 13 indicators exhibited execution rates ranging from 2.56% to 95.51%. Following the application of evidence-based interventions, 8 indicators reached an execution rate of 100.00%, with no indicators maintaining an execution rate of 0. The execution rates for the remaining indicators improved to a range of 47.02% to 91.67%, as illustrated in Figure 1.
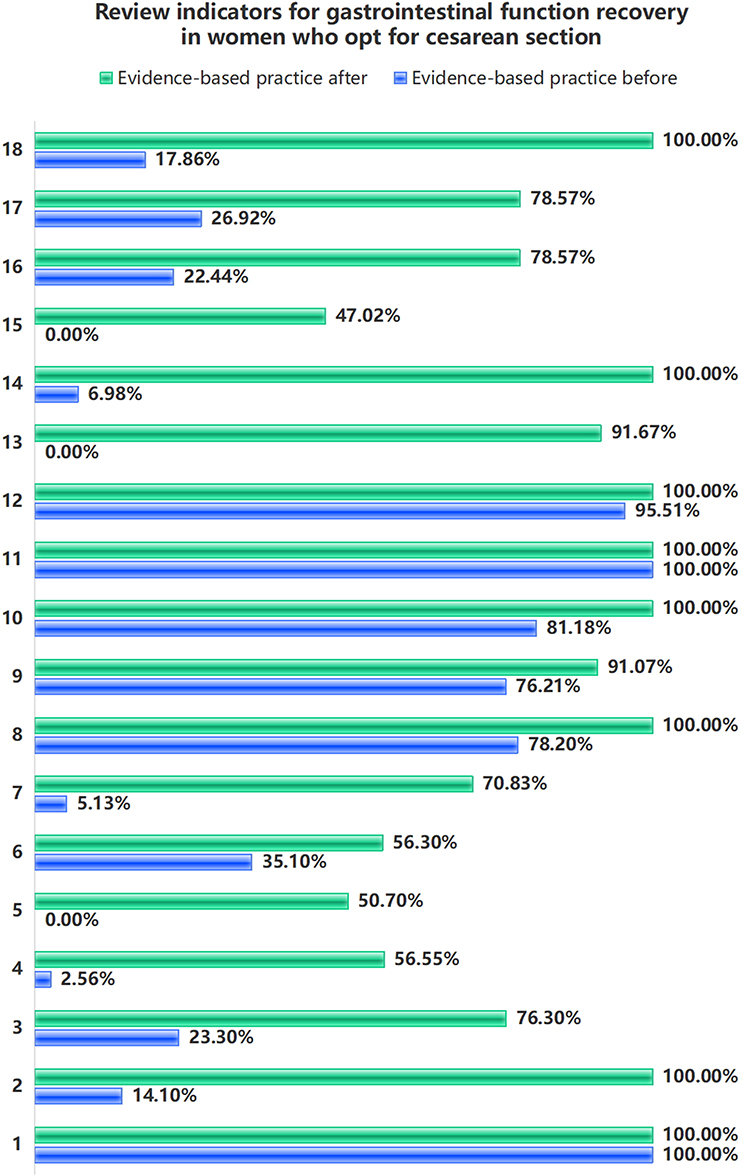 |
Figure 1 Review indicators for gastrointestinal function recovery in women who opt for cesarean section. |
Comparison of Maternal Outcome Indicators Pre- and Post-Clinical Practice
The implementation of evidence-based practice resulted in a significant reduction in the duration of preoperative and postoperative fasting and water deprivation (P < 0.01). Additionally, there was a decrease in both VAS scores from 5.05±1.00 to 3.20±0.67 (P < 0.01) and GAD-7 scores from 2.94±0.88 to 1.07±1.04 (P = 0.023). The time to first anal exhaust was also significantly shortened from 32.19±20.48h to 20.25±8.14h (P < 0.01). Furthermore, the incidence of thirst decreased from 56.41% to 23.81% (χ2 = 35.97, P < 0.01), hunger incidence reduced from 48.72% to 16.67% (χ2 = 38.13, P < 0.01), nausea or vomiting incidence declined from 35.90% to 11.90% (χ2 = 25.93, P < 0.01), and bloating incidence decreased from 27.56% to 14.29% (χ2 = 8.70, P = 0.003), as detailed in Table 2. Due to the lack of strict controls, these promising findings require further validation through more rigorous randomized controlled trials in the future.
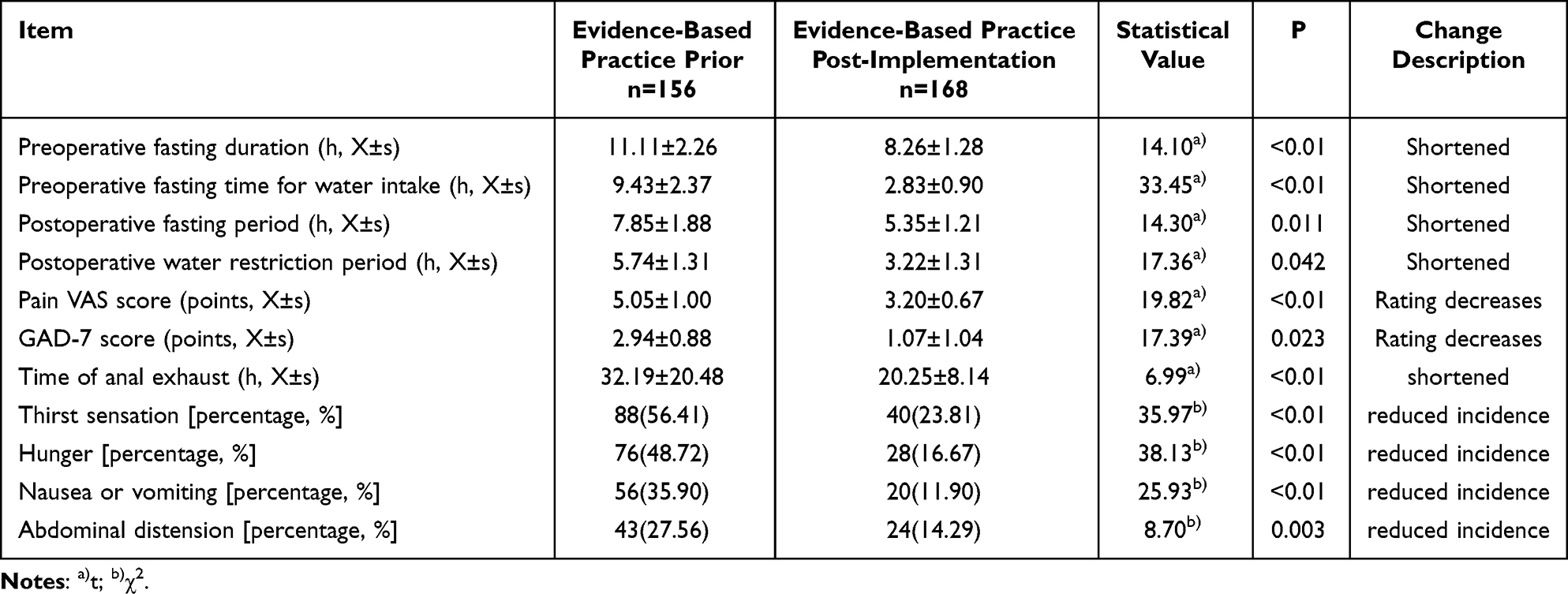 |
Table 2 Comparison of Evaluation Indicators Before and After Evidence-Based Practice |
Discussion
This study utilized the PDCA cycle and evidence-based practices18 to establish and implement a nurse-led, multidisciplinary collaborative evidence-based practice program for Broussonetia papyrifera, which significantly improved gastrointestinal function recovery in elective cesarean section patients. Baseline assessments were conducted before training, with immediate evaluations afterward using patient cases and clinical scenarios as key teaching tools.19 The success of this program lies in its systematic approach to addressing the core barriers in the translation from “knowing” to “doing”.
The establishment of a closed-loop, sustainable knowledge transformation system was central to the success of this initiative. Whereas standalone training often yields only transient effects, the integrated “training-implementation-monitoring-optimization” framework, coupled with the PDCA cycle, ensured the continuity and stability of practice change. Immediate post-training evaluations using clinical cases effectively bridged theoretical knowledge and clinical practice. Concurrently, the institutionalization of monthly compliance analyses and multidisciplinary reviews established a robust mechanism for continuous quality control and feedback, which proved crucial for embedding new nursing practices into routine workflows. These findings underscore that sustainable change depends not only on initial education but, more critically, on a system capable of ongoing monitoring, feedback, and iterative optimization.
The implementation of evidence-based care, aimed at enhancing patient safety and supporting clinical decision-making, effectively addressed common post-cesarean discomforts like hunger, thirst, and bloating.20,21 This study highlights the importance of personalized and humanized medical care in clinical decision-making, aiming to improve maternal satisfaction and treatment outcomes.22 A bundled intervention—incorporating reduced perioperative fasting, early mobilization guided by digital tools, pain and fluid management, and TCM massage was introduced. This strategy significantly reduced the time to anal exhaust (from 32.19±20.48 to 20.25±8.14 hours, P < 0.05) and improved maternal comfort by alleviating pain, anxiety, and GI symptoms. Complementing this, a shared decision-making model empowered mothers in their post-operative care. While perioperative fasting and fluid restriction management needs enhancement, future nursing decision support systems may bolster clinical decisions.23 These findings demonstrate that a comprehensive, multi-faceted approach is more effective than single measures for facilitating postoperative recovery.
Rapid postoperative recovery depends on effective measures and multidisciplinary cooperation. Nurses are essential in patient care, improving communication, education, and psychological support. To promote evidence-based nursing, nurse leaders must lead interventions and encourage EBP discussions within organizations.24 Recent research highlights that clear vision, strong communication, and leadership skills, including ongoing nurse education, are vital for maintaining commitment to EBP in clinical settings.25 Among the 18 nursing interventions, nurses independently led 10 items and coordinated with other healthcare professionals to complete the remaining 6. This underscores the pivotal role of nurses as both “catalysts” and “coordinators” in evidence-based practice. Through a digital platform enabling daily monitoring and weekly feedback, nurses ensured the consistent implementation of the interventions. Furthermore, the introduced shared decision-making model empowered parturients to make autonomous choices regarding aspects such as catheter removal and ambulation, thereby enhancing the patient-centered nature of the care protocol and improving both maternal compliance and satisfaction. Thus, establishing clear leadership roles for nurses and fostering effective communication and coordination mechanisms are essential to the successful implementation of evidence-based practice within multidisciplinary teams. Although preoperative assessments and health education require additional time from nurses, this investment is offset in two ways: standardized protocols reduce the hidden time costs associated with complications from prolonged fasting, and decreased patient discomfort significantly lowers the postoperative care burden. Therefore, by optimizing nursing efficiency and potentially shortening hospital stays, this practice not only improves care quality but also demonstrates positive economic value, showing promising implications for broader adoption.
While this study contributes to evidence-based practices for gastrointestinal recovery after cesarean delivery, several limitations must be acknowledged. The primary limitations concern the study design and its associated risk of bias. The non-randomized, pre-post design over two time periods, while pragmatic, precludes strong causal inferences and is susceptible to confounding from factors like seasonal variations. Furthermore, the lack of multivariable adjustment in our statistical analysis means we could not control for potential confounding variables, which complements the inherent limitations of the design. Additionally, the absence of blinding for participants and staff may have introduced performance and detection bias. The generalizability of our findings is limited by the single-center setting and a sample from a specific demographic. Key physiological indicators, such as intestinal flora, were not tracked, and the brief study duration may not capture long-term outcomes. Future research should utilize multicenter, randomized designs with blinding, longer follow-up, and broader biomarker assessment to validate and extend these findings.
Conclusion
This nurse-led study uses evidence-based practices to improve gastrointestinal recovery in mothers undergoing elective cesarean deliveries by fostering multidisciplinary collaboration. It enhances evidence-based care and teamwork among healthcare professionals, offering personalized and efficient nursing services to support perioperative recovery.
Data Sharing Statement
The project received approval from the Assistant Nursing Director of the clinical nursing unit. To ensure confidentiality during data collection, no patient-identifying information was recorded. Specifically, the project team did not collect patients’ names, identification numbers, or diagnoses during the audit. Access to the collected data was restricted exclusively to the project team members.
Ethics Approval and Consent to Participate
This study has been approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (Approval No. [2023]0493).
Acknowledgments
Despite this study include Traditional Chinese Medicine (TCM), the design, analysis, and reporting of this research were conducted with a commitment to scientific objectivity, and all findings were based on predefined outcome measures.
Funding
There is no funding to report.
Disclosure
All authors declare no competing interests in this work.
References
1. Sun JJ, Wang H, Tang LL, Jiang H, Liu XS. Effect of intraoperative dexmedetomidine on recovery of gastrointestinal function after caesarean section undergoing spinal and epidural anesthesia: a randomized, double blind, placebo-controlled clinical trial. Eur J Obstet Gynecol Reprod Biol. 2024;297:30–35. doi:10.1016/j.ejogrb.2024.03.038
2. Betran AP, Ye J, Moller AB, Souza JP, Zhang J. Trends and projections of caesarean section rates: global and regional estimates. BMJ Glob Health. 2021;6(6):e005671. doi:10.1136/bmjgh-2021-005671
3. Rabiepoor S, Yas A, Navaei J, Khalkhali HR. Does coffee affect the bowel function after caesarean section? Eur J Obstet Gynecol Reprod Biol. 2018;220:96–99. doi:10.1016/j.ejogrb.2017.07.028
4. Bollag L, Lim G, Sultan P, et al. Society for obstetric anesthesia and perinatology: consensus statement and recommendations for enhanced recovery after cesarean. Anesth Analg. 2021;132(5):1362–1377. doi:10.1213/ANE.0000000000005257
5. Wilson RD, Monks DT, Sharawi N, et al. Guidelines for antenatal and preoperative care in cesarean delivery: enhanced recovery after surgery society recommendations (part 1)-2025 update. Am J Obstet Gynecol. 2025. doi:10.1016/j.ajog.2025.01.014
6. Caughey AB, Sultan P, Monks DT, et al. Guidelines for intraoperative care in cesarean delivery: enhanced recovery after surgery society recommendations (part 2)-2025 update. Am J Obstet Gynecol. 2025. doi:10.1016/j.ajog.2025.02.040
7. Sultan P, Monks DT, Sharawi N, et al. Guidelines for postoperative care in cesarean delivery: enhanced recovery after surgery society recommendations (part 3)-2025 update. Am J Obstet Gynecol. 2025. doi:10.1016/j.ajog.2025.01.038
8. Xue J, Xu Z, Hou H, et al. Clinical practice guideline for prevention and treatment of postoperative gastrointestinal disorder with integrated traditional Chinese and Western medicine (2023 edition). Chinese J of Evidence-Based Med. 2024;24(6):15. doi:10.7507/1672-2531.202312185
9. Zhou Y, Yang L, Ling J, Wei X, Zhou Z, Qin P. Application status of rapid rehabilitation after cesarean section and investigation on knowledge, practice and behavior states of nursing personnel in the department of obstetrics. Guangxi Medical Journa. 2024;2024(5):7. doi:10.11675/j.issn.0253-4304.2024.05.25
10. Liu XY, Chen XB, Wen YL, Guo XP, Zhou XB. Effect of psychological nursing intervention combined with acupressure on postoperative recovery of women after cesarean section. World J Clin Cases. 2024;12(21):4527–4535. doi:10.12998/wjcc.v12.i21.4527
11. Zhang Y, Wang X, Yang H. Effect of traditional Chinese medicine nursing on postoperative patients with gastric cancer and its impact on quality of life. Am J Transl Res. 2021;13(5):5589–5595.
12. Nelson G, Bakkum-Gamez J, Kalogera E, et al. Guidelines for perioperative care in gynecologic/oncology: enhanced Recovery After Surgery (ERAS) society recommendations-2019 update. Int J Gynecological Cancer. 2019;29(4):651–668. doi:10.1136/ijgc-2019-000356
13. Xue J, Xu Z, Wang Q, et al. Clinical practice guidelines for prevention and treatment of postoperative gastrointestinal disorder with integrated traditional Chinese And Western medicine (2023). J Evid Based Med. 2024;17(1):207–223. doi:10.1111/jebm.12587
14. Huang J, Cao C, Nelson G, Wilson RD. A review of enhanced recovery after surgery principles used for scheduled caesarean delivery. J Obstet Gynaecology Canada. 2019;41(12):1775–1788. doi:10.1016/j.jogc.2018.05.043
15. Hedrick TL, McEvoy MD, Mythen MMG, et al. Perioperative quality initiative (POQI) 2 Workgroup. American society for enhanced recovery and perioperative quality initiative joint consensus statement on postoperative gastrointestinal dysfunction within an enhanced recovery pathway for elective colorectal surgery. anesth Analg. 2018;126(6):1896–1907. doi:10.1213/ANE.0000000000002742
16. Pearson A, Wiechula R, Court A, Lockwood C. The JBI model of evidence-based healthcare. Int J Evid Based Healthc. 2005;3(8):207–215. doi:10.1111/j.1479-6988.2005.00026.x
17. Weaver SJ, Lyons R, DiazGranados D, et al. The anatomy of health care team training and the state of practice: a critical review. Acad Med. 2010;85(11):1746–1760. doi:10.1097/ACM.0b013e3181f2e907
18. Mackey A, Bassendowski S. The history of evidence-based practice in nursing education and practice. J Prof Nurs. 2017;33(1):51–55. doi:10.1016/j.profnurs.2016.05.009
19. Lehane E, Leahy-Warren P, O’Riordan C, et al. Evidence-based practice education for healthcare professions: an expert view. BMJ Evidence Based Med. 2019;24(3):103–108. doi:10.1136/bmjebm-2018-111019
20. Beyea SC, Slattery MJ. Historical perspectives on evidence-based nursing. Nurs Sci Q. 2013;26(2):152–155. doi:10.1177/0894318413477140
21. Hedrick TL, McEvoy MD, Mythen MMG, et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on postoperative gastrointestinal dysfunction within an enhanced recovery pathway for elective colorectal surgery. Anesthesia Analg. 2018;126(6):1896–1907. doi:10.1213/ane.0000000000002742
22. Truglio-Londrigan M, Slyer JT. Shared decision-making for nursing practice: an integrative review. Open Nurs J. 2018;12:1–14. doi:10.2174/1874434601812010001
23. Noorbakhsh-Sabet N, Zand R, Zhang Y, Abedi V. Artificial intelligence transforms the future of health care. Am J Med. 2019;132(7):795–801. doi:10.1016/j.amjmed.2019.01.017
24. Bianchi M, Bagnasco A, Bressan V, et al. A review of the role of nurse leadership in promoting and sustaining evidence-based practice. J Nurs Manag. 2018;26(8):918–932. doi:10.1111/jonm.12638
25. Fleiszer AR, Semenic SE, Ritchie JA, Richer MC, Denis JL. Nursing unit leaders’ influence on the long-term sustainability of evidence-based practice improvements. J Nurs Manag. 2016;24(3):309–318. doi:10.1111/jonm.12320
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.