Back to Journals » Lung Cancer: Targets and Therapy » Volume 15
NRG1 Fusions in NSCLC: Being eNRGy Conscious
Authors Gupta B, Gosa Barrett L, Liu SV ![]()
Received 18 February 2024
Accepted for publication 27 August 2024
Published 3 October 2024 Volume 2024:15 Pages 143—148
DOI https://doi.org/10.2147/LCTT.S464626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sai-Hong Ou
Brinda Gupta, Laura Gosa Barrett, Stephen V Liu
Lombardi Comprehensive Cancer Center, Georgetown University, Washington, DC, USA
Correspondence: Stephen V Liu, Georgetown University, Lombardi Comprehensive Cancer Center, 3800 Reservoir Road NW, Washington, DC, 20007, USA, Tel +1 202 444-2223, Fax +1 202 444-7889, Email [email protected]
Abstract: Fusions in neuregulin 1 (NRG1) are rare oncogenic drivers that occur across a number of tumor types, including non-small cell lung cancer (NSCLC). NRG1 has an EGF-like domain that serves as a ligand for HER3 receptors, inducing heterodimerization, usually with HER2, and subsequent activation of oncogenic downstream signaling pathways. Emerging evidence suggests that NSCLC harboring NRG1 fusions do not respond as well to standard therapeutic options including chemotherapy and immunotherapy, and prognosis is poor. Novel treatment approaches targeting the HER2/HER3 pathway are under investigation. Here, we discuss the biology and detection of NRG1 fusions in NSCLC and promising targeted treatment strategies for tumors harboring the mutation.
Keywords: NSCLC, NRG1, targeted therapy, HER2, HER3
Introduction
Gene fusions, or translocations, have emerged as key targetable oncogenic drivers in various tumor types. One study identified a total of 25,664 fusions in a set of 9642 tumors, suggesting that gene fusions drive the development of 16.5% of cancer cases and function as the sole driver in more than 1% of cancers.1 Treatment of non-small cell lung cancer (NSCLC) is particularly guided by the presence or absence of certain actional gene fusions. When pathogenic fusions in ALK, ROS1, or RET are present in advanced NSCLC, there are multiple highly effective and well-tolerated tyrosine kinase inhibitors approved by the US FDA as first-line therapy.2–8 The presence of these fusions predicts both benefit from these targeted therapies and relative lack of benefit from immunotherapy.9
NRG1 fusions represent a family of emerging and potentially actionable driver events. NRG1 fusions are relatively uncommon, occurring in only about 0.2% of solid tumors, and can be challenging to detect even when present.10 While data are limited for this rare subset of NSCLC, the emerging evidence suggests poor outcomes with standard chemotherapy and immunotherapy.11 Because of the underlying pathophysiology of NSCLC with NRG1 fusions, agents targeting the HER2/HER3 pathway have been explored and early experience shows promising activity. In this narrative review, we discuss the unique biology of NRG1 fusions and strategies in development to treat NSCLC harboring an NRG1 fusion.
Biology of NRG1
The NRG1 gene, located at chromosome 8p12, encodes for neuregulin-1, a protein that is essential to normal organ development and embryogenesis.12 Conversely, fusions that involve NRG1 result in the pathogenic production of oncoproteins which promote aberrant downstream signaling that results in cancer cell and tumor growth. NRG1 contains an epidermal growth factor (EGF)-like domain that binds and activates receptor-tyrosine kinases in the EGF receptor (ErbB) family, particularly HER3 and HER4. The fusion partner often contributes a transmembrane domain that tethers the EGF-like domain of NRG1 to the membrane, allowing it to bind to HER3 or HER4. The binding in turn results in the heterodimerization of HER2 and HER3 which leads to subsequent activation of the tumorigenic PI3K-AKT and MAPK signaling pathways.13
Incidence of NRG1 Fusions Across Tumors
The first NRG1 fusion (CD74-NRG1) was discovered in an invasive mucinous lung adenocarcinoma in 2014 through whole transcriptome sequencing.13 Since then, NRG1 fusions have been identified in a variety of tumor types at low frequencies. In the largest report to date, an analysis of 169,273 tumor samples subject to RNA-based next-generation sequencing (Caris Life Sciences) identified 261 tumors with an NRG1 fusion for an incidence of 0.154% across solid tumors.14 In this report, NSCLC accounted for the most cases (42.4%), though this in part reflects samples routinely sent for molecular testing. The remaining cases were comprised of breast cancer (11.9%), ovarian cancer (10.2%), pancreatic cancer (7.9%), colorectal cancer (6.8%), cancer of unknown primary (5.1%), cholangiocarcinoma (4.5%), prostate cancer (2.3%), bladder cancer (1.7%), and esophagogastric cancers (1.7%). Considering total cases tested, the incidence of NRG1 fusions in NSCLC was 0.232% (78 out of 33,648).
Detection of NRG1 Fusions
NRG1 is encoded by a large gene that spans approximately 1.4 megabases, representing 1/2000th of the entire human genome. Only about 0.3% of the gene encodes for the protein, with the remaining gene consisting of large non-protein coding introns.15 Diagnostically, given its size and complex structure, NRG1 fusions have been difficult to detect by DNA-based sequencing alone. RNA-based next-generation sequencing has emerged as a more robust tool for detecting these relatively uncommon fusions.
In the global, retrospective eNRGy1 registry, the clear majority of NRG1 fusions (74%) were identified using RNA-based assays, whereas only 26% of patients were detected with DNA-based testing.11 Similarly, in an analysis of 2522 patients with lung adenocarcinoma, 5 patients were found to have a NRG1 fusion by RNA sequencing that was not detected by DNA-based sequencing.16 These findings emphasize the advantage of RNA-based analysis to detect NRG1 fusions.
There is considerable heterogeneity among NRG1 fusion partners within and across tumor types. In the above analysis of 261 unique tumors with an NRG1 fusion, there were 153 unique fusion partners.17 CD74 was the most common fusion partner (12.37%), followed by SLC3A2 (8.13%), ATP1B1 (4.59%), RBPMS (4.24%), and WRN (1.77%). It is worth noting that not all fusion events reported have been confirmed to be in-frame. Additionally, there are multiple breakpoints for each fusion, which contributes to the overall diversity of NRG1 fusions.
In most tumors harboring an NRG1 fusion, there are no other known oncogenic drivers, but in the eNRGy1 registry, 7 of 110 cases did have an alternate driver.11 Four cases had a co-mutation in KRAS; G12C (n=1), G12V (n=1), and G12D (n=2) were detected. The other three cases had an EGFR L858R mutation (n=2) or an EML4-ALK fusion (n=1, variant 3). PD-L1 status was known in 46% of the cases and most (70%) had no PD-L1 expression, 24% had low expression, and only 4% had PD-L1 expression in ≥50% of cells. Median tumor mutational burden was low in these NRG1 fusion-positive NSCLC cases at 0.9 mutations per megabase.11
Response to Standard Therapy
Although further analysis is needed, early reports indicate that NRG1 fusion-positive tumors tend to respond poorly to standard treatment options. As compared to other fusion-positive tumors such as those expressing ALK, ROS1, and RET fusions, data from 110 patients with NRG1 fusion-harboring NSCLC in the global eNRGy1 registry showed that patients did not respond well to platinum-based or taxane-based chemotherapy.11 The median OS for patients with stage IV NSCLC with an NRG1 fusion was 15.5 months. For patients who received platinum-doublet chemotherapy, the response rate was only 13% (n=2/15) with a median PFS of 5.8 months (95% CI, 2.2 to 9.8; range, 0.7–12.1 months). Similarly, 14% (n=1/7) of patients responded to taxane-based chemotherapy in the post-platinum doublet setting with 71% (n=5/7) achieving a best response of progressive disease. The median PFS in this set of patients was 4.0 months (95% CI, 0.8 to 5.3; range, 0.8–5.5 months).
Patients with NRG1 fusion positive NSCLC also had marginal benefit from immunotherapy.11 Three out of the five evaluable patients who received single-agent immunotherapy (60%) had progressive disease as best response and only one patient had a partial response. The median PFS with immunotherapy was 3.6 months (95% CI, 0.9 to undefined; range, 0.9–11.2 months). Results were similar for patients treated with chemoimmunotherapy with zero out of nine patients exhibiting a response and 56% (n=5/9) having progressive disease as their best response. Median PFS was 3.3 months (95% CI, 1.4 to 6.3; range, 1.4–15.2 months). Given these findings, there is a strong unmet need for novel treatments for tumors harboring an NRG1-fusion.
Emerging Targeted Therapy
While there are challenges in conducting prospective clinical trials for rare genomic subsets, there are several clinical trials that include patients with NRG1 fusion-positive tumors. Early results are encouraging, but many of these studies are ongoing (Table 1).
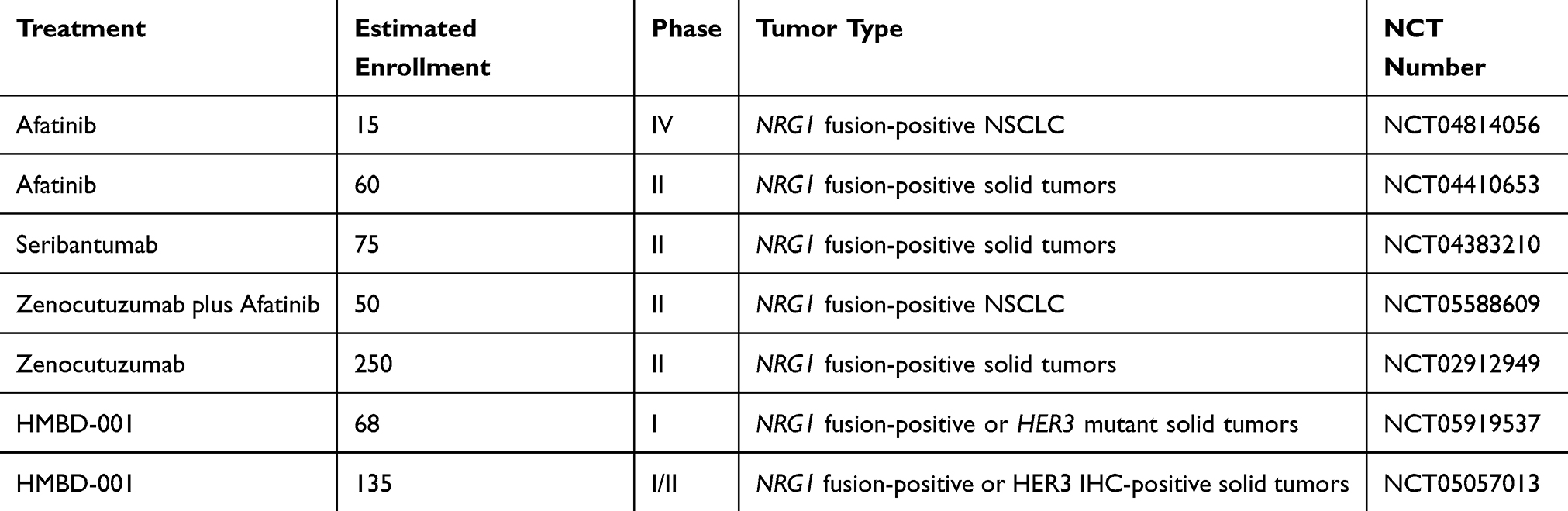 |
Table 1 Select Trials Including Patients with NRG1-Fusion Positive Cancers |
Afatinib
Given that NRG1 fusions rely on the ErbB family of receptors to activate downstream oncogenic pathways, afatinib, a pan-ERBb inhibitor, is an appealing therapeutic option. There is early in vitro and in vivo data suggesting that targeting HER4 and EGFR in addition to HER2 and HER3 alone leads to enhanced antitumor activity.18 Case reports of patients with NRG1 fusion-positive cancers treated with afatinib have also shown promising results. In one series, 12 of 19 patients achieved a response, including a durable response lasting for 24 months.19 Out of the patients in that series with NSCLC, 62% (n=8/13) achieved a PR with a duration of response between 6.5 and 27 months; another 15% (n=2/13) had stable disease. Another case report described a patient with NPTN-NRG1 fusion who achieved a PR with afatinib lasting 14 months.
In the eNRGy1 registry, of the 20 patients with NRG1 fusion-positive NSCLC treated with afatinib, 25% (n=5/20) achieved a partial response.11 Fusion partners were reported in four of these five patients: CD74 (n=2), SLC3A2 (n=1), and SDC4 (n=1). An additional 15% (n=3/20) of patients had stable disease. Unfortunately, the majority of patients (60%, n=12/20) experienced progressive disease as best response. The median PFS with afatinib was 2.8 months (95% CI, 1.9 to 4.3; range, 0.3–25.3 months). There was no significant difference in survival between patients who received afatinib and those who did not.
A more recent retrospective review of 110 patients with NRG1 fusion-positive cancers included 72 patients treated with afatinib, 29 of whom (40.9%) had NSCLC.20 Afatinib was typically given as second-line or later treatment and 69.4% of patients had an Eastern Cooperative Oncology Group performance status of 2–4. In the afatinib cohort, the response rate was 37.5% with a median PFS of 5.5 months and a median survival of 7.2 months. In the 29 patients with NSCLC, the RR with afatinib was 48.3% with a median duration of response of 6.8 months. Prospective data for afatinib in NSCLC with an NRG1 fusion is lacking but data may emerge from the Drug Rediscovery Protocol trial in the Netherlands (DRUP, NCT02925234) or the multi-cohort Targeted Agent and Profiling Utilization Registration trial in the United States (TAPUR, NCT02693535).
Seribantumab
Seribantumab is a fully human anti-HER3 IgG2 monoclonal antibody that can inhibit NRG1-mediated HER3 activation, HER2/HER3 dimerization, and downstream signaling. In preclinical studies, seribantumab was able to effectively inhibit NRG1-stimulated growth.21 In the global, multicenter Phase II CRESTONE trial, patients with solid tumors harboring an NRG1 fusion were treated with intravenous seribantumab 3 g once weekly. Cohort 1 included 11 patients with NSCLC who had not had prior HER-directed therapy and in this cohort and were evaluable for response. The RR for seribantumab in this subset was 36% (n=4/11) and median duration of response has not yet been reached (range 1.4 to 11.5 months). The most common treatment-related adverse events were diarrhea (40% all grade, 3% ≥ grade 3), fatigue (29% all grade, 0% ≥ grade 3), and rash (26% all grade, 0% ≥ grade 3). Seribantumab was granted Fast Track Designation by the US Food and Drug Administration; however, further clinical development has been paused.
Zenocutuzumab
Zenocutuzumab (MCLA-128) is a bispecific antibody that targets HER2 and HER3 and is another potential treatment option for patients with solid tumors harboring NRG1 fusions. By targeting both HER2 and HER3, zenocutuzumab prevents NRG1 binding to HER3 and disrupts the subsequent HER2 and HER3 heterodimerization and downstream activation of the PI3K-AKT and MAPK pathways. In vitro, zenocutuzumab inhibited growth of NRG1 fusion-positive cell lines and xenograft models.22
Zenocutuzumab is being explored in the prospective, phase II eNRGy trial (NCT02912949).23 Preliminary results from 75 patients with NSCLC with an NRG1 fusion show a response rate of 37.2% and a clinical benefit rate of 61.5%.24 The median time to response was 1.8 months and the median duration of response was 14.9 months. Treatment-related adverse events included diarrhea (17% all grade, 2% grade 3–4), infusion reactions (12% all grade, 0% grade 3–4), and fatigue (10% all grade, 0% grades 3–4). There were no treatment discontinuations due to treatment related adverse events. Zenocutuzumab was granted Fast Track Designation by the US Food and Drug Administration.
NRG1 Fusions Mediating Resistance
Interestingly, targeting NRG1 and its downstream signaling pathways may be a potential strategy to overcome resistance to targeted therapy. A RALGAPA1-NRG1 fusion was detected in a patient with stage IV NSCLC with an ALK fusion that had progressed on ALK targeted therapy with crizotinib and alectinib.25 Further study revealed that the NRG1 fusion was present prior to initiation of crizotinib therapy, suggesting that concurrent NRG1 fusions may contribute to inherent development of resistance to ALK targeted therapy. In preclinical studies, this resistance was overcome by targeting the HER pathway with afatinib.
Conclusion
NRG1 fusions are emerging as a relatively rare but clinically important genomic alteration in a variety of cancers. NRG1 fusions have been identified in several cancer types, including NSCLC and pancreatic cancers. These fusions result in the constitutive activation of HER signaling, which can drive tumor growth, invasion, and metastasis. The identification of NRG1 fusions has significant implications for cancer prognosis and treatment. Retrospective studies show that outcomes with standard treatment including chemotherapy and immunotherapy are poor and there is a pressing need for novel therapeutic strategies. The development of NRG1-directed therapies may provide a promising new treatment option for patients with NRG1 fusion-positive cancers. However, more research is needed to fully understand the biology and clinical implications of NRG1 fusions in cancer.
Funding
There is no funding to report for this work.
Disclosure
BG and LGB report no conflicts of interest in this work. SVL reports consulting and advisory fees from AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Catalyst, Daiichi Sankyo, Eisai, Elevation Oncology, Genentech/Roche, Gilead, Guardant Health, Janssen, Jazz Pharmaceuticals, Merck, Merus, Mirati, Novartis, Regeneron, Revolution Medicines, Sanofi, Takeda, and Turning Point Therapeutics; research funding (to institution) from AbbVie, Alkermes, AstraZeneca, Elevation Oncology, Ellipses, Genentech, Gilead, Merck, Merus, Nuvalent, OSE Immunotherapeutics, Puma, Pfizer, RAPT, and Turning Point Therapeutics; and serving on a data safety monitoring board for Candel Therapeutics.
References
1. Gao Q, Liang WW, Foltz SM, et al. Driver fusions and their implications in the development and treatment of human cancers. Cell Rep. 2018;23(1):227–238e3. doi:10.1016/j.celrep.2018.03.050
2. Camidge DR, Dziadziuszko R, Peters S, et al. Updated efficacy and safety data and impact of the EML4-ALK fusion variant on the efficacy of alectinib in untreated ALK-positive advanced non-small cell lung cancer in the global phase III Alex study. J Thoracic Oncol: off Publication Int Assoc Study Lung Cancer. 2019;14(7):1233–1243. doi:10.1016/j.jtho.2019.03.007
3. Camidge DR, Kim HR, Ahn MJ, et al. Brigatinib versus crizotinib in ALK-positive non-small-cell lung cancer. New Engl J Med. 2018;379(21):2027–2039. doi:10.1056/NEJMoa1810171
4. Solomon BJ, Bauer TM, Mok TSK, et al. Efficacy and safety of first-line lorlatinib versus crizotinib in patients with advanced, ALK-positive non-small-cell lung cancer: updated analysis of data from the Phase 3, randomised, open-label CROWN study. Lancet Respir Med. 2023;11(4):354–366. doi:10.1016/S2213-2600(22)00437-4
5. Drilon A, Chiu CH, Fan Y, et al. Long-term efficacy and safety of entrectinib in ROS1 fusion-positive NSCLC. JTO Clin Res Rep. 2022;3(6):100332. doi:10.1016/j.jtocrr.2022.100332
6. Ou SI, Bang YJ, Camidge DR, et al. Efficacy and safety of crizotinib in patients with advanced ROS1 -rearranged non-small cell lung cancer (NSCLC). J Clin Oncol: off J Am Soc Clin Oncol. 2013;31(15_suppl):8032. doi:10.1200/jco.2013.31.15_suppl.8032
7. Zhou C, Solomon B, Perol M. Selpercatinib or chemotherapy in RET fusion-positive NSCLC. reply. New Engl J Med. 2024;390(4):381–382. doi:10.1056/NEJMc2314327
8. Gainor JF, Curigliano G, Kim DW, et al. Pralsetinib for RET fusion-positive non-small-cell lung cancer (ARROW): a multi-cohort, open-label, Phase 1/2 study. Lancet Oncol. 2021;22(7):959–969. doi:10.1016/S1470-2045(21)00247-3
9. Mazieres J, Drilon A, Lusque A, et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann Oncol. 2019;30(8):1321–1328. doi:10.1093/annonc/mdz167
10. Jonna S, Feldman R, Ou SH, et al. Characterization of NRG1 gene fusion events in solid tumors. J Clin Oncol: off J Am Soc Clin Oncol. 2020;38(15_suppl):3113. doi:10.1200/JCO.2020.38.15_suppl.3113
11. Drilon A, Duruisseaux M, Han JY, et al. Clinicopathologic features and response to therapy of nrg1 fusion–driven lung cancers: the enrgy1 global multicenter registry. J Clin Oncol: off J Am Soc Clin Oncol. 2021;39(25):2791–2802. doi:10.1200/JCO.20.03307
12. Liu SV. NRG1 fusions: biology to therapy. Lung Cancer. 2021;158:25–28. doi:10.1016/j.lungcan.2021.05.011
13. Fernandez-Cuesta L, Plenker D, Osada H, et al. CD74-NRG1 fusions in lung adenocarcinoma. Cancer Discovery. 2014;4(4):415–422. doi:10.1158/2159-8290.CD-13-0633
14. Gupta B, Wu S, Ou SH, et al. NRG1 fusions in solid tumors. J Clin Oncol: off J Am Soc Clin Oncol. 2023;41(suppl_16):3132. doi:10.1200/JCO.2023.41.16_suppl.3132
15. Falls DL. Neuregulins: functions, forms, and signaling strategies. Exp Cell Res. 2003;284(1):14–30. doi:10.1016/s0014-4827(02)00102-7
16. Benayed R, Offin M, Mullaney K, et al. High yield of RNA Sequencing For Targetable Kinase Fusions In Lung Adenocarcinomas With No Mitogenic Driver Alteration Detected by DNA sequencing and low tumor mutation burden. Clin Cancer Res: off J Am Assoc Cancer Res. 2019;25(15):4712–4722. doi:10.1158/1078-0432.CCR-19-0225
17. Antonia S, Goldberg SB, Balmanoukian A, et al. Safety and antitumour activity of durvalumab plus tremelimumab in non-small cell lung cancer: a multicentre, phase 1b study. The Lancet Oncology Mar. 2016;17(3):299–308. doi:10.1016/S1470-2045(15)00544-6
18. Udagawa H, Nilsson M, Robichaux J, et al. HER4 and EGFR activate cell signaling in NRG1 fusion-driven cancers: implications for HER2-HER3-specific versus pan-HER targeting strategies. J Thorac Oncol. 2024;19(1):106–118. doi:10.1016/j.jtho.2023.08.034
19. Cadranel J, Liu SV, Duruisseaux M, et al. Therapeutic potential of afatinib in nrg1 fusion-driven solid tumors: a case series. Oncologist. 2021;26(1):7–16. doi:10.1634/theoncologist.2020-0379
20. Liu SV, Frohn C, Minasi L, et al. Real-world outcomes associated with Afatinib use in patients with solid tumors harboring NRG1 gene fusions. Lung Cancer. 2024;188:107469. doi:10.1016/j.lungcan.2024.107469
21. Odintsov I, Lui AJW, Sisso WJ, et al. The Anti-HER3 MAB seribantumab effectively inhibits growth of patient-derived and isogenic cell line and xenograft models with oncogenic NRG1 fusions. Clin Cancer Res: off J Am Assoc Cancer Res. 2021;27(11):3154–3166. doi:10.1158/1078-0432.CCR-20-3605
22. Schram AM, Odintsov I, Espinosa-Cotton M, et al. Zenocutuzumab, a HER2xHER3 bispecific antibody, is effective therapy for tumors driven by NRG1 gene rearrangements. Cancer Discovery. 2022;12(5):1233–1247. doi:10.1158/2159-8290.CD-21-1119
23. Kim DW, Schram AM, Hollebecque A, et al. The phase I/II eNRGy trial: zenocutuzumab in patients with cancers harboring NRG1 gene fusions. Future Oncol. 2024;20(16):1057–1067. doi:10.2217/fon-2023-0824
24. Schram AM, Goto K, Kim D, et al. Durable efficacy of zenocutuzumab, a HER2 x HER3 bispecific antibody, in advanced NRG1 fusion-positive (NRG1+) non-small cell lung cancer (NSCLC). Ann Oncol. 2023;34(suppl_2):S755–S851. doi:10.1016/annonc/annonc1331
25. McCoach CE, Le AT, Gowan K, et al. Resistance mechanisms to targeted therapies in ROS1(+) and ALK(+) non-small cell lung cancer. Clin Cancer Res: off J Am Assoc Cancer Res. 2018;24(14):3334–3347. doi:10.1158/1078-0432.CCR-17-2452
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.