")
Back to Journals » Clinical Ophthalmology » Volume 17
Novel Technique to Improve the Efficacy of Corneal Cross Linking in Cases of Post LASIK Ectasia
Authors Omar Yousif M, Elkitkat RS , Abdelsadek Alaarag N
Received 19 February 2023
Accepted for publication 4 April 2023
Published 11 April 2023 Volume 2023:17 Pages 1109—1120
DOI https://doi.org/10.2147/OPTH.S409256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohamed Omar Yousif,1,2 Rania Serag Elkitkat,1,3– 5 Noha Abdelsadek Alaarag1
1Ophthalmology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 2Maadi Eye Subspecialty Center, Cairo, Egypt; 3Watany Eye Hospital, Cairo, Egypt; 4Watany Research and Development Center, Cairo, Egypt; 5Ophthalmology Department, Faculty of Medicine, MTI University, Cairo, Egypt
Correspondence: Rania Serag Elkitkat, Future City, Shorouk, Cairo, Egypt, 11779, Tel +2012 21753904, Email [email protected]; [email protected]
Purpose: The aim of the present study was to validate the use of a novel technique that can improve the efficacy of corneal cross-linking (CXL) in cases with post LASIK ectasia.
Methods: This is a retrospective, comparative study that was conducted on patients who sought medical advice at Ain Shams University Hospitals and Maadi Eye Subspeciality Center, Cairo, Egypt. It included two groups of patients with post LASIK ectasia. Group 1 included patients who performed our proposed protocol (topo-guided PRK, followed by customized phototherapeutic keratectomy “PTK” to transmit the laser treatment to the corneal stroma, then CXL). For group 2, accelerated CXL was performed. Subjective refraction and relevant topographic/tomographic parameters (Sirius topographer) compared between the two groups. Recorded follow-ups included the 2 to 3-month follow-up visit and the last visit (mean ± SD of 17.2 months ± 10.2).
Results: Patients of group 1 (22 eyes of 22 patients) experienced significant improvements in most of the evaluated parameters at the 2- to 3-month follow-up visit and showed stability of the ectatic condition at the last follow-up visit, whereas patients of group 2 (10 eyes of 10 patients) showed stability of their ectatic condition at the 2- to 3-month follow-up visit, and one patient developed ectasia progression at the last follow-up visit.
Conclusion: The present study validates the use of our novel protocol in cases having post LASIK ectasia with proven efficacy, safety, and stability, providing regularization for the corneal surface while simultaneously avoiding the unnecessary loss of cross-linking effect within the LASIK flap that no longer shares in the corneal biomechanical strength.
Keywords: post LASIK ectasia, novel technique post LASIK ectasia, corneal cross-linking, strengthening cross-linking efficacy, post LASIK ectasia management
A Letter to the Editor has been published for this article.
Introduction
Post LASIK ectasia is one of the most disheartening complications that an ophthalmic surgeon can encounter.1 Its incidence has been estimated to range between 0.04% and 0.6%.2,3 Progressive corneal thinning and steepening with disturbed stromal biomechanical properties lead to progressive myopic shift, irregular astigmatism, and corneal aberrations, with consequent visual compromise.4 Proper management of such a dreadful condition has always been a major concern for refractive surgeons.5
Although recently approved by the US Food and Drug Administration, corneal cross-linking (CXL) has long been used as a safe and effective modality for addressing post LASIK ectasia.6–8 It can successfully strengthen the intrafibrillar and interfibrillar covalent bonds between the stromal collagen lamellae through the interaction of riboflavin and ultraviolet (UV) radiation.9
Combination of CXL and photorefractive keratectomy (PRK) in the same session has been introduced by Kanellopoulos et al10,11 and has been proven safe and effective in managing post LASIK ectasia.12 The original protocol involves performing a 50-um phototherapeutic keratectomy (PTK) at a 6.5-mm optical zone to remove the corneal epithelium, to be followed by a partial topography-guided PRK at a maximum depth of 50 um, application of mitomycin-C 0.02% for 20 seconds, and then finally higher fluence corneal CXL at 6 mW/cm2 for 30 minutes.10
Our team has recently published a modified, tissue saving protocol for combined PRK and CXL for keratoconus (KC) management, with proven efficacy, safety, and stability.13 The primary outcome of the present study was to evaluate the efficacy, safety, and stability of this novel protocol in cases with post LASIK ectasia, while the secondary outcome was to compare the results of such a novel technique to the conventional CXL protocol in post LASIK ectasia management.
Materials and Methods
This is a retrospective, comparative clinical study that comprised the eyes of patients who were diagnosed as post LASIK ectasia. The included patients sought medical advice at the Ophthalmology Clinic of Ain Shams University Hospitals and Maadi Eye Subspeciality Center, Cairo, Egypt. All the enrolled participants previously performed LASIK procedure in the period between January 2009 and August 2018. The study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethical Committee of Ain Shams University (FMASU-R-190/2022). The Institutional Review Board (IRB) of Ain Shams University granted a waiver of informed consents from the participants owing to the retrospective nature of the study.
The electronic medical files of all the enrolled candidates were explored. The study comprised corneas with post LASIK ectasia and no previous treatment trials. The exclusion criteria included previous ocular surgeries other than LASIK, anterior segment pathologies other than corneal ectasia, posterior segment pathologies, and patients with poor healing (mainly long-standing steroid intake or collagen vascular diseases). Also, severe ectatic cases in which the corneal topography device failed to attain a good-quality image for topo-guided treatment were excluded from the study. For patients who performed the novel proposed protocol, flap thickness was always chosen to be >100 µm as measured by anterior segment Optical Coherence Tomography (AS-OCT) to have enough stromal bed to withstand the laser treatment without developing buttonholes or other flap-related complications.
The retrieved data from the medical files included age, sex, eye laterality, subjective refraction pre- and postoperatively (including uncorrected distance visual acuity [UDVA] and corrected distance visual acuity [CDVA] using Snellen acuity chart, treatment spherical equivalent (SE), and treatment cylinder), and topographic data from Sirius topographer (CSO Italia). Furthermore, any recorded postoperative complications, mainly delayed epithelial healing on slit-lamp examination or clinical signs of endothelial damage, were documented and analyzed.
All the patients were diagnosed as having post LASIK ectasia based on previously published clinical and topographic criteria, including myopic refractive error with or without progression of the manifest astigmatism, decreasing UDVA and/or CDVA, progressive inferior corneal steepening on topography, increasing posterior elevations, and/or decreasing inferior corneal thickness.12,14
Data concerning the laser treatment was retrieved from the surgical planning printout of Contoura topography-guided ablation software of WaveLight EX500 excimer laser system (Alcon, USA). It included the topography-guided treatment maximum depth, the thickness of the removed epithelium (the depth of PTK), and the thinnest residual stromal bed (all measured in micrometers).
Regarding the patients’ pre- and postoperative topographic data, it was obtained from Sirius topographer (CSO Italia) with software version Phoenix 3.2.1.60. The enrolled data included: keratometric power at the flattest corneal meridian (K1), keratometric power at the steepest corneal meridian (K2), topographic cylinder, mean Keratometry (K mean), maximum Keratometry (K max), corneal thinnest location, corneal asphericity (Q value), pupil diameter, inferior minus superior (I-S) keratometric difference at 2- and 4-mm diameters, and the root mean square (RMS) of coma aberration, spherical aberration, and higher order aberrations (HOAs).
For all the enrolled candidates, AS-OCT was performed to measure both the epithelial and flap thickness. Afterwards, topo-guided PRK was performed, followed by PTK to transmit the treatment to the corneal stroma at all the treated areas.
The technique involves performing topo-guided PRK on the corneal surface, followed by PTK to remove the remaining epithelial cells, to be followed by corneal collagen CXL.
Before describing the details of our presumably novel treatment protocol, we need to clarify the two set goals that we considered for performing the treatment protocol safely. Firstly, having at least 350 µm of residual stromal bed at the thinnest corneal location before initiating the CXL treatment. Secondly, keeping at least 50 µm of flap stroma after firing the topo-guided PRK and before removing the remaining epithelium by the subsequent PTK.
In order to guarantee the presence of at least 50 µm of flap stroma immediately after laser treatment, we used the following equation: residual flap stroma = Flap thickness – (PRK treatment maximum ablation depth + PTK ablation depth used to remove the remaining epithelium).
Our novel treatment protocol was well achieved by studying the topo-guided PRK profile on the laser treatment screen, then the refraction to be corrected and the treatment optical zone were manipulated by the surgeon to achieve a maximal ablation depth that will not go deeper than a point which is 50 µm from the flap interface. Afterwards, by studying the color codes on the laser treatment screen, the minimal ablation thickness could be well detected, so the remaining epithelium at these points of minimal ablation could be calculated and hence the needed PTK ablation depth could be adjusted for complete epithelial removal homogenously (this usually ranges from 0 to 50 µm). All the calculations considered having at least 350 µm of residual stroma before initiating the CXL treatment on the corneal stroma.15 Figure 1 shows the laser treatment screen with the various parameters upon which the treatment protocol was based.
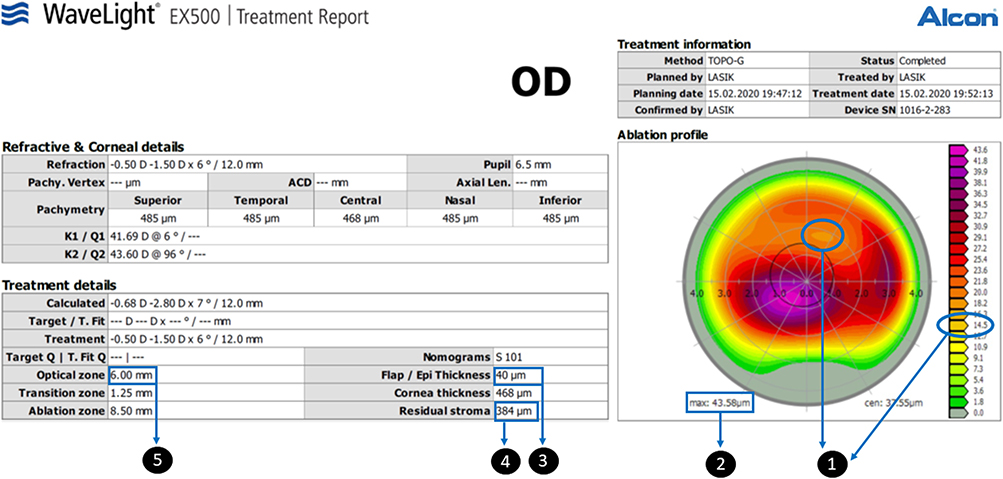 |
Figure 1 The surgical planning printout of Contoura topography-guided ablation software of WaveLight EX500 excimer laser system (Alcon, USA) showing how to use the treatment screen data to calculate the treatment parameters and set a treatment plan: Minimum ablation depth (it is determined by correlating the ablation profile color-coded map with the color scale, where its value here is 14.5 µm). Maximum ablation depth. Phototherapeutic keratectomy depth needed for epithelial removal is then calculated (here it was set to be 40 to reach the 50 µm needed for complete epithelial removal over the area of minimum ablation). Residual stroma (it should not go below 360 µm as a lower limit). Treatment optical zone (here it was set to 6 mm to cover the scotopic pupil diameter). The maximum stromal ablation depth here is 33 µm. |
There were certain rules that we abided by to determine the patient’s refraction that will be corrected together with the topo-guided treatment, as follows:
When the axes of both the refractive and topographic cylinders coincided, we used the lower dioptric power of the two axes.
When the two axes did not coincide, we did not add the cylindrical correction to the treatment profile, instead we added the SE of the cylinder to the spherical correction.
If we had to compromise either the spherical or the cylindrical correction so as not to get a deeper ablation depth and remove more corneal tissue, we decreased or even omitted the spherical correction.
If the topo-guided treatment alone would reach the maximum stromal ablation depth limits, we omitted the refraction from the treatment profile, using only the topo-guided treatment with “zero” refractive correction.
Any postoperative residual or induced myopic shift was corrected with either glasses or Implantable Collamer Lens “ICL” implantation accordingly. This induced myopic shift is likely to happen on using topo-guided treatment alone with “zero” refractive correction, and also in cases where an eccentric cone with irregular cornea was converted to a more central but regular one.
Following the laser treatment, mitomycin-C 0.02% was applied for 20 seconds, then CXL was performed for all the corneas, starting by corneal surface irrigation with balanced salt solution, which was followed by corneal soaking with riboflavin (0.1% riboflavin sodium phosphate ophthalmic solution VibeX Rapid: Avedro, Inc) for 10 minutes, followed by pulsed CXL using Avedro KXL system (Avedro, USA). One second’s pulsed interval was used at a power of 30 mW/cm2 with an irradiation time of 4 minutes and a total treatment time of 8 minutes with a total energy delivered of 7.2 J/cm2. A bandage soft contact lens was then applied till full corneal re-epithelialization was achieved.
The recorded follow-ups of patients included the data at 2- to 3-month follow-up interval and at the last follow-up visit.
The electronic medical files were used to classify the enrolled patients into two groups depending on the received treatment protocol; group 1 patients received our proposed novel treatment protocol, while group 2 patients received conventional CXL treatment (pulsed light accelerated CXL at a power of 30 mW/cm2 with an irradiation time of 4 minutes). Comparisons between both groups were performed regarding the visual and topographic outcomes. Furthermore, efficacy and safety indices were performed for the two treatment modalities, and evaluation of the refractive and topographic stability along the follow-up periods were compared between both groups.
Statistical Analysis
Data were collected, revised, coded, and entered to the Statistical Package for Social Science (IBM SPSS), version 23. The quantitative data were presented as mean, standard deviations and ranges when parametric. Qualitative variables were presented as numbers and percentages. Comparisons between the two groups regarding qualitative data were done using Chi-square test, comparisons regarding quantitative data with parametric distribution were done using independent t-test, while comparisons regarding quantitative data with non-parametric distribution were done using Mann–Whitney test. Comparisons between two paired groups with quantitative data and parametric distribution were done using Paired t-test, while comparisons between two paired groups with quantitative data and non-parametric distribution were done using Wilcoxon test. The confidence interval was set to 95% and the margin of error accepted was set to 5%. So, the p-value was considered significant if >0.05.
Results
The present study included 32 eyes of 32 patients with post LASIK ectasia. Twenty-two eyes received the novel treatment protocol (group 1), while 10 eyes received accelerated CXL protocol. The age range of the recruited cohort was 24 to 37 years, with a mean ± SD of 30.00 years ± 3.62 for group 1 and 29.27 years ± 3.44 for group 2 patients. The female-to-male percentage was 68.1% (15 eyes) to 31.9% (7 eyes) for group 1 and 70% (7 eyes) to 30% (3 eyes) for group 2, and the right eyes’ percentage was 59% (13 eyes) and 60% (6 eyes) for both groups, respectively.
On analyzing the preoperative parameters in both groups, statistically significant differences were detected regarding the preoperative UDVA, SE, topographic cylindrical component, RMS of coma aberration and HOAs. All these values were better in group 1 compared to group 2 (Table 1).
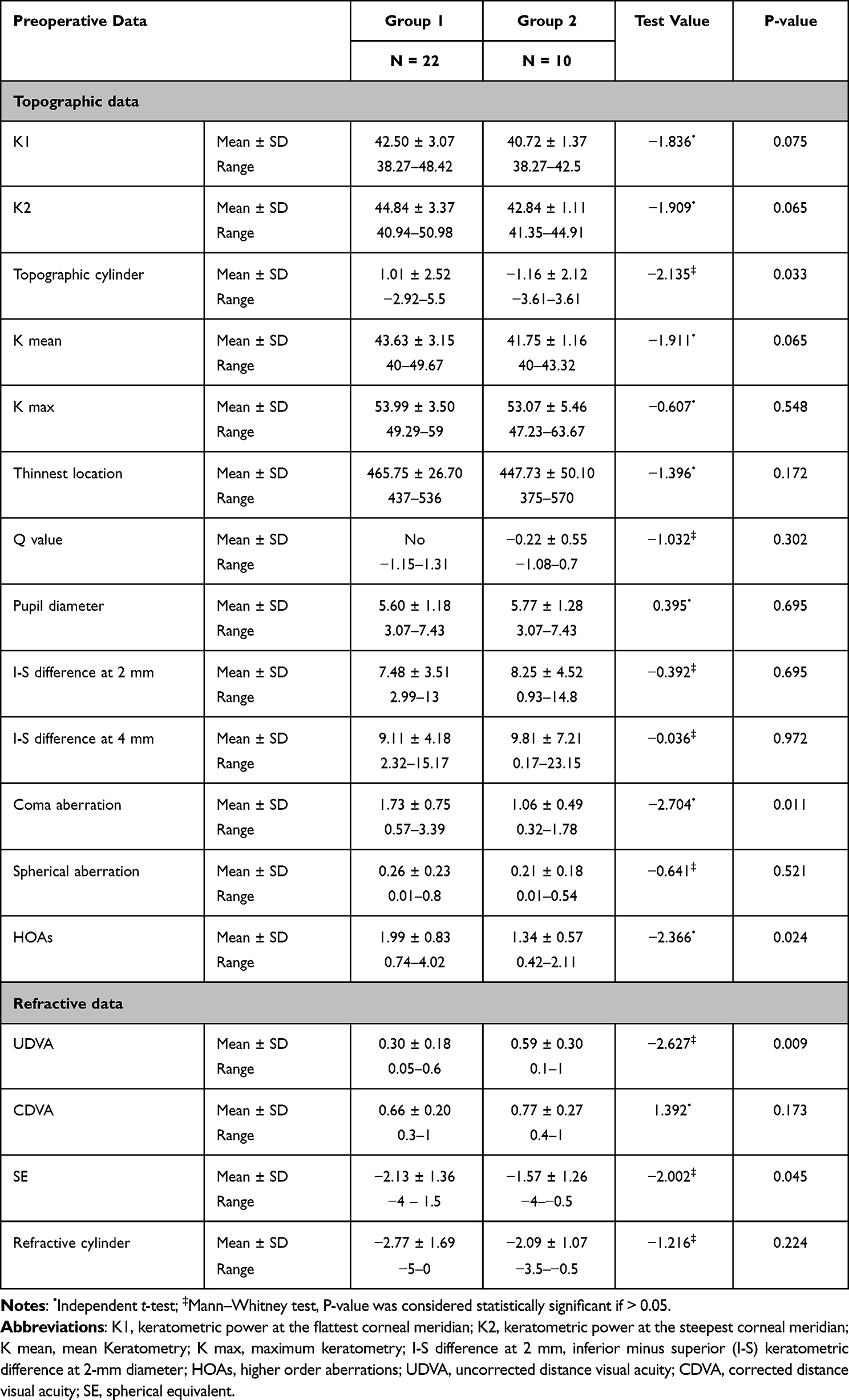 |
Table 1 Comparison Between the Two Enrolled Groups in Regard to the Preoperative Visual and Topographic/Tomographic Parameters |
In regard to the treatment results, patients of group 1 obviously had statistically significant differences between the pre- and postoperative (at the 2- to 3-month follow-up visit) values for most of the evaluated visual and topographic/tomographic indices, with significant improvements in all parameters (Table 2). On the other hand, patients of group 2 showed stability of most of the evaluated visual and topographic parameters 2 to 3 months postoperatively, with no significant postoperative changes (except for the K max and the I-S keratometric difference at 4 mm that showed significant postoperative reduction) (Table 3).
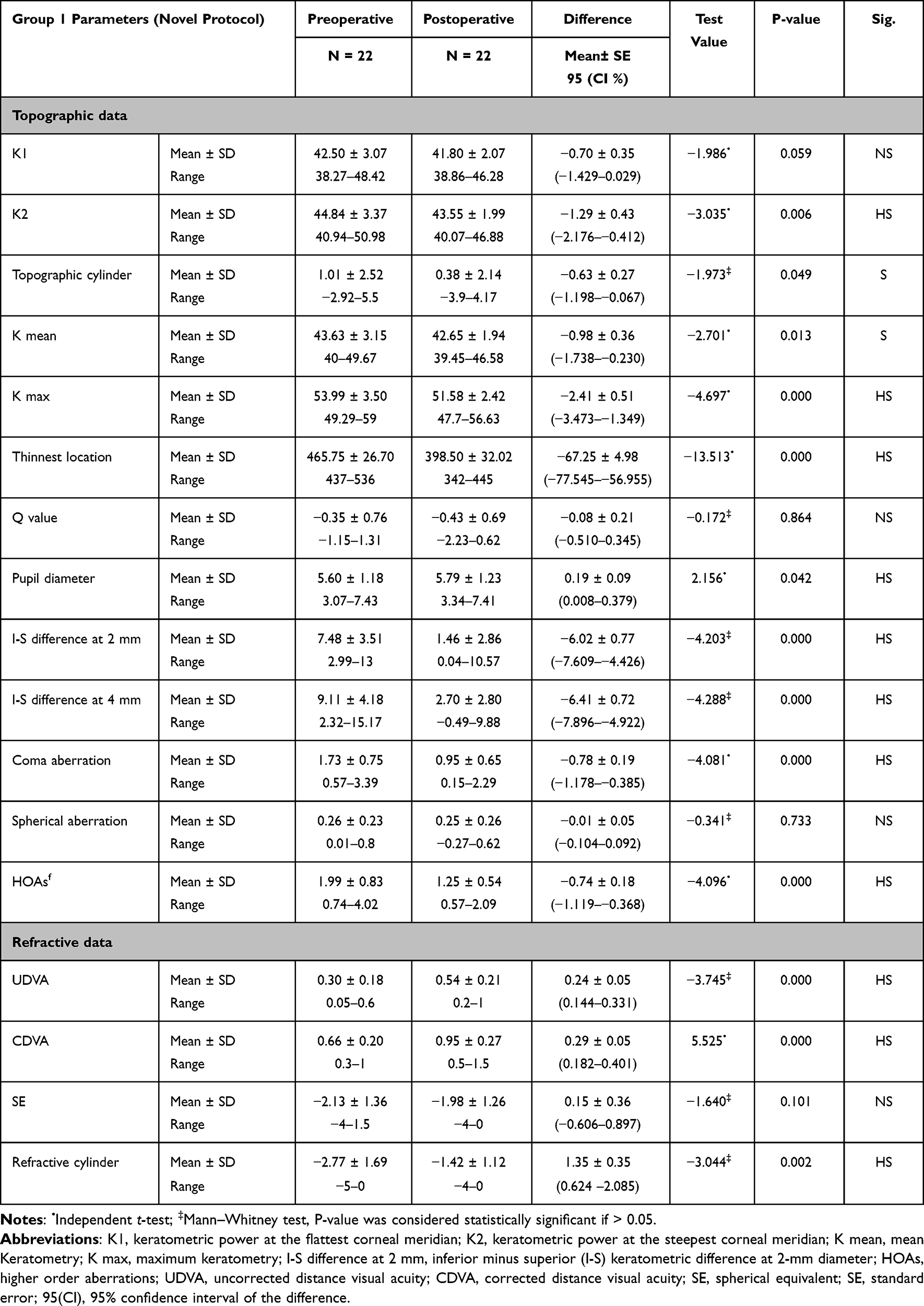 |
Table 2 Comparison Between the Pre and Postoperative Visual and Topographic/Tomographic Parameters for Patients of Group 1 (Who Performed the Novel Treatment Protocol) |
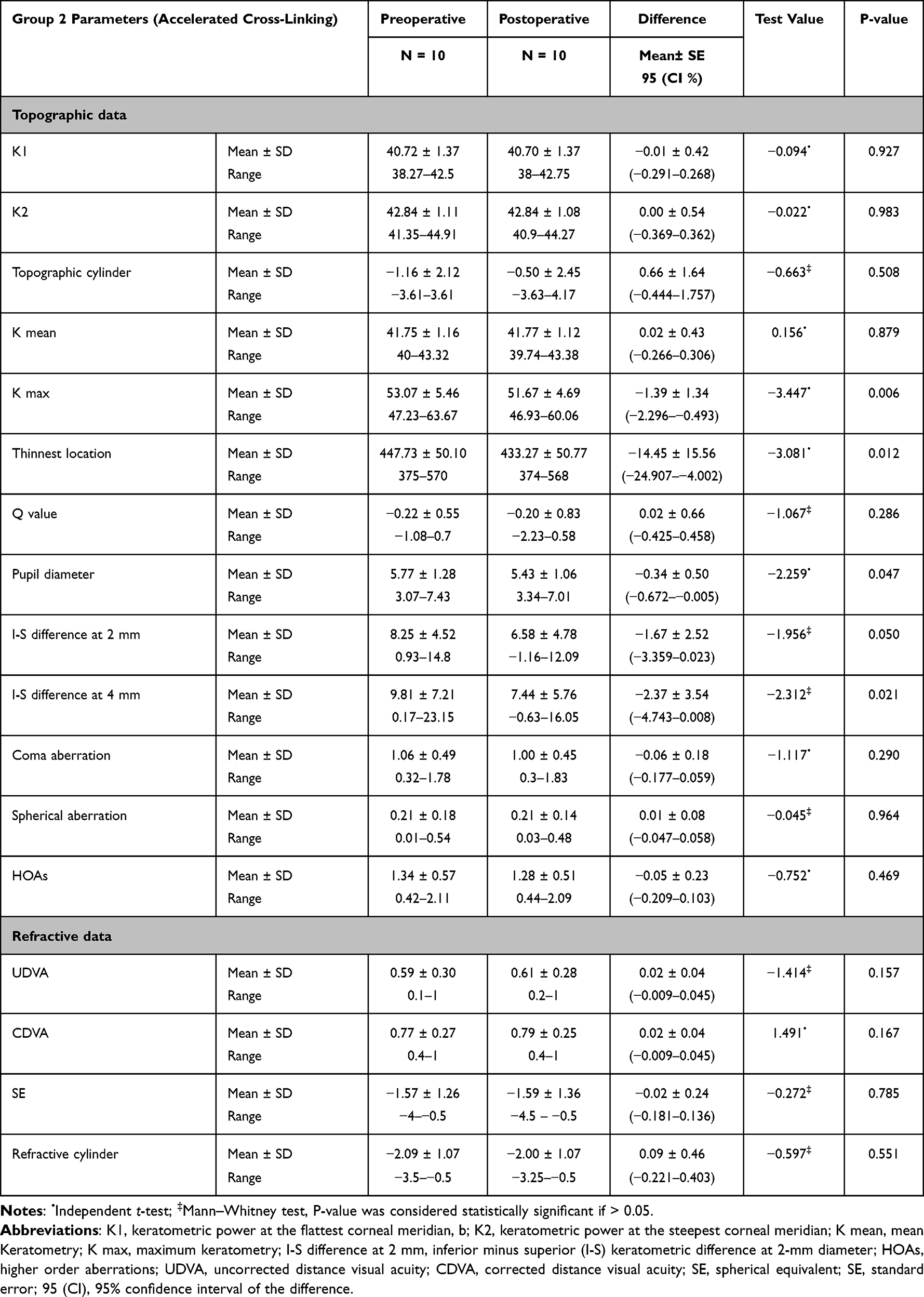 |
Table 3 Comparison Between the Pre- and Postoperative Visual and Topographic/Tomographic Parameters for Patients of Group 2 (Who Performed Cross-Linking Treatment Protocol) |
Regarding the visual and topographic stability of patients, detected by comparing the postoperative parameters between the 2- to 3-month and the last follow-up visit (patients’ follow-up period ranged from 20 to 37 months, with a mean ± SD of 17.2 months ± 10.2), the results showed a noticeable stability of the evaluated parameters for both groups, with statistically insignificant differences between the values at the first and last follow-up visit, except for one patient of group 2, who showed significant progression of some of his evaluated parameters postoperatively (namely UDVA, CDVA, SE, K max, and coma aberration), and hence he needed a redo for the CXL 18 months after the first treatment.
The efficacy and safety indices of the two performed procedures were calculated,16 showing values above the cut-off values for both groups (efficacy index value of 1.58 ± 0.80 and 1.04 ± 0.09 for groups 1 and 2, respectively, and safety index value of 0.90 ± 0.50 and 0.86 ± 0.15 for groups 1 and 2, respectively). The efficacy index was significantly higher in group 1 compared to group 2.
In patients of group 1, 18 out of 22 eyes (81.8%) showed significant postoperative coinciding (in both the value and axis) between the refractive and topographic cylindrical components.
The medical records were also checked for any reported postoperative complications, mainly corneal edema denoting endothelial damage. The results showed no reported significant complications.
Figures 2 and 3 illustrate the pre and postoperative sagittal curvature map of Sirius topography for a patient of groups 1 and 2, respectively. Figure 2 shows the patient’s topography about 2 months following the novel treatment protocol, showing significant improvements in the topographic parameters, while Figure 3 shows an obvious topographic stability with no improvement about 2 years following the conventional CXL treatment.
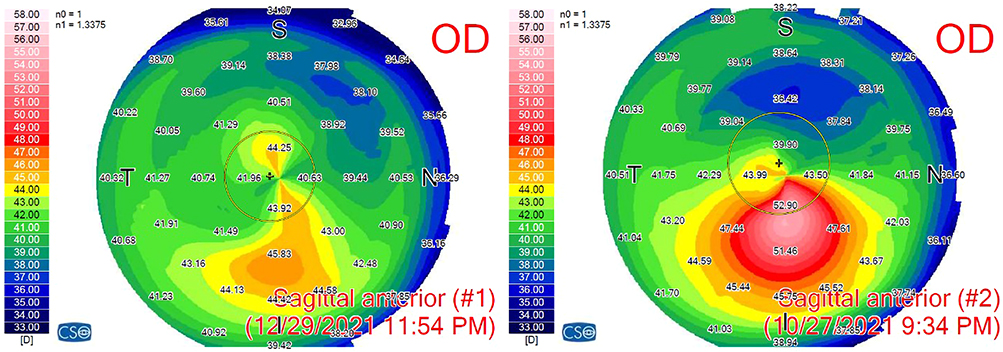 |
Figure 2 The pre (on the right side) and the post (on the left side) operative (about 2 months following the novel treatment protocol) sagittal anterior curvature map of Sirius topography for a patient of group 1, showing significant improvements in the topographic parameters. |
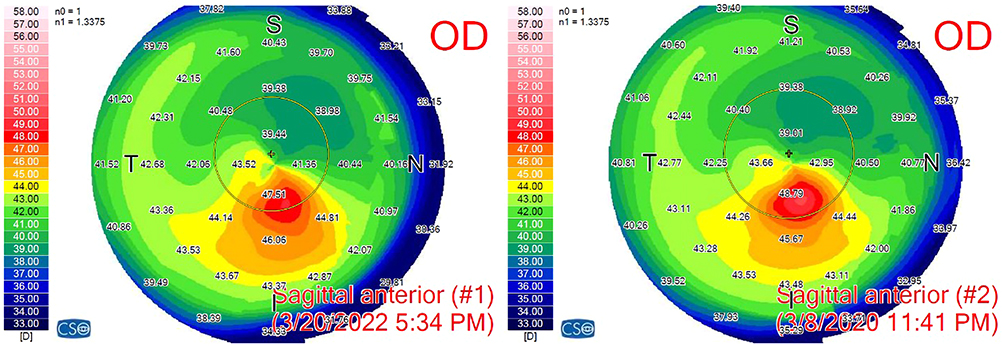 |
Figure 3 The pre (on the right side) and the post (on the left side) operative (about 2 years following cross-linking treatment) sagittal anterior curvature map of Sirius topography for a patient of group 2, showing stability of the ectatic condition with no significant improvements in the topographic parameters. |
Discussion
Owing to the exponentially increasing number of LASIK candidates worldwide, safety measures and proper preoperative selection of patients is mandatory. However, the incidence of post LASIK ectasia, although rare, remains a major concern for ophthalmic surgeons.17 Although a constellation of preoperative and/or operative features are very frequently found in post LASIK ectasia cases, the absence of such features in some rare instances confounds our understanding of this devastating complication.12
In all the previous trials of CXL in cases with post LASIK ectasia, the effective CXL only involved the anterior corneal layer, so the major portion of the CXL effect is rather consumed in strengthening the corneal flap rather than the deeper corneal stroma, and this will lead to a lower overall CXL effect for the effective residual stromal bed that actively shares in maintaining the corneal integrity post LASIK.
The present study results obviously showed significant improvements in most of the evaluated parameters in patients of group 1 at the 2 to 3-month follow-up visit, with stability along the follow-up visits and no documented regression in any patient, whereas patients of group 2 (though having milder ectasia from the beginning) developed stability of their condition starting from the 2 to 3-month visit, with recorded progression of the post LASIK ectasia in 1 patient (10%).
Analysis of the preoperative data in the two enrolled cohorts showed that both visual quantity (UDVA, CDVA, SE, cylindrical component) and quality (RMS of coma aberration and HOAs) indices were higher in group 1 patients (who received the novel protocol) compared to group 2 patients (who received CXL protocol). That is why CXL was the treatment of choice for the latter cohort with early ectasia stages. Furthermore, some cases were chosen to be enrolled in group 2 rather than group 1 owing to their thin flap thickness (below 100 um as measured by preoperative AS-OCT) that rendered performing the novel protocol unsafe with possible development of buttonholes or other flap-related complications.
Furthermore, it is to be noted that the preoperative Q value for patients of both groups was within normal ranges or even lower (−0.22 ± 0.55 and −0.35 ± 0.76 for groups 1 and 2, respectively). In contrast to keratoconus (KC), the Q values are not elevated in cases with post myopic LASIK ectasia, as all of these patients previously performed myopic ablation that rendered the cornea oblate (with the possibility of having positive Q values previously that regressed into negative values with ectasia development). Moreover, the Q value in patients of group 1 was relatively higher than group 2 patients after performing the ectasia treatment protocol (although the difference was statistically insignificant). This can be attributed to the topo-guided laser treatment in patients of group 1 which can induce further increase in the Q value.
Many previous studies have explored the role of CXL in managing cases of early post LASIK ectasia, with some promising results for the visual and topographic parameters.6–8,18 In a study by Kymionis et al19 on a small cohort of patients having KC and post LASIK ectasia, corneal confocal microscopy showed full-thickness keratocytes repopulation in the anterior and mid-corneal stroma 6 months following the CXL treatment, with preservation of the corneal endothelium and no significant detectable morphological changes. Some studies showed the long-term stability and effectiveness of conventional CXL,7,20 while others declared that better outcomes could be obtained using the transepithelial accelerated CXL protocols,17,21,22 owing to the reduced corneal haze and lesser keratocyte apoptosis and induced inflammation compared to its conventional counterpart.
Once the ectatic progression has stabilized, regularization of the corneal surface using customized PRK can significantly reduce the refractive error and hence improve the visual outcomes following CXL for post LASIK ectasia cases.23 Kanellopoulos has introduced his simultaneous PRK and CXL “Athens protocol” for managing cases of KC,10 and then Kanellopoulos and Binder showed promising results for using the Athens protocol in managing 32 cases of post LASIK ectasia,12 where the UDVA improved in 27 eyes, was unchanged in 4 eyes, and worsened in 1 eye, and the refractive error was significantly reduced in 27 of the 32 eyes (84.3%).
In a study by Wallerstein et al,24 an approach of “under-flap CXL” was introduced for managing early, mild, newly diagnosed cases of post LASIK ectasia before significant deterioration. This involves soaking the stromal bed with riboflavin, repositioning the flap, then applying ultraviolet (UV) light to the corneal surface. This study proposed that this technique would probably halt the ectatic progression by strengthening the corneal tissue under the flap. By eliminating the need to remove the epithelium, it can also minimize the postoperative complications of standard epi-off CXL, minimize patient’s discomfort, and significantly reduce the recovery time. Along a relatively short follow-up period of 6 months, and including a small cohort of eight eyes, the study results showed stability (with no improvement) of each of CDVA, efficacy index, safety index, K max, and corneal irregularity index. The technique used in this study is similar to our proposed technique in avoiding the loss of CXL effect within the flap tissue. Yet, no regularization of the corneal surface is achieved using this technique, and this may explain the stationary rather than regressive course of ectasia in such cases of the aforementioned study.
We have previously published our proposed novel treatment protocol for managing KC cases with variable degrees,13 with proven efficacy, safety, and stability. The technique has also shown very promising visual and topographic outcomes in managing cases of post LASIK ectasia as per the present study results. Compared to the group which performed conventional CXL protocol, the group which performed the novel treatment protocol showed significant improvement in various parameters at the 2- to 3-month follow-up and no cases developed any postoperative relapses along a follow-up period that reached up to 3 years.
In our proposed treatment protocol, topo-guided PRK is performed, followed by customized PTK to transmit the laser treatment to the corneal stroma at all the treated areas. This is followed by CXL. By doing this treatment sequence, we can improve the visual quality by regularizing the corneal surface, and at the same time we can increase the depth of the cross-linked corneal tissue in the previous LASIK residual stromal bed, especially at the cone location which is the weakest corneal area. This would subsequently improve the efficacy of CXL, bearing in mind that performing the CXL at the flap level would not effectively alter the corneal biomechanical properties, as the flap is no longer calculated as an integral part of the corneal stroma following the LASIK procedure. Hence, cross-linking the deeper corneal tissue is much more beneficial than cross-linking the flap stroma.
Furthermore, our study results showed no evidence of postoperative complications, with no signs of corneal edema denoting endothelial damage along the long follow-up interval of the study. This adds to the efficacy and safety of the proposed technique in managing post LASIK ectasia cases.
Our study is not without limitations. Its retrospective nature and the relatively small enrolled cohorts mandate the conduction of future longitudinal studies on larger cohorts to reinforce our study results and give more credibility to our proposed technique in managing post LASIK ectasia cases. Furthermore, performing specular microscopy and confocal microscopy in future studies can give more comprehensive overview of the treatment effect. Moreover, using the AS-OCT in future studies to measure the demarcation line depth from the flap interface following the proposed treatment protocol could elucidate its deeper and hence more effective CXL.
Conclusions
In conclusion, the present study validates the use of our previously published protocol in cases having post LASIK ectasia with proven efficacy, safety, and stability, providing regularization for the corneal surface while simultaneously avoiding the unnecessary loss of the CXL effect in the LASIK flap that no longer shares in the corneal biomechanical strength.
Data Sharing Statement
Available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consents
This study was approved by the ethical committee of Ain Shams University (FMASU-R-190/2022). The institutional review board of Ain Shams University granted a waiver of informed consents, owing to the retrospective nature of the study. Patients data were kept anonymous with utmost confidentiality.
Acknowledgment
The authors would like to thank the statistician Mr Hesham Elkady for the performance of the statistical analysis of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boxer Wachler BS, Christie JP, Chandra NS, Chou B, Korn T, Nepomuceno R. Intacs for keratoconus. Ophthalmology. 2003;110(5):1031–1040. doi:10.1016/S0161-6420(03)00094-0
2. Binder PS. Analysis of ectasia after laser in situ keratomileusis: risk factors. J Cataract Refract Surg. 2007;33(9):1530–1538. doi:10.1016/j.jcrs.2007.04.043
3. Chen MC, Lee N, Bourla N, Hamilton DR. Corneal biomechanical measurements before and after laser in situ keratomileusis. J Cataract Refract Surg. 2008;34(11):1886–1891. doi:10.1016/j.jcrs.2008.06.035
4. Santhiago MR, Giacomin NT, Smadja D, Bechara SJ. Ectasia risk factors in refractive surgery. Clin Ophthalmol. 2016;10:713–720. doi:10.2147/OPTH.S51313
5. Spadea L, Cantera E, Cortes M, Conocchia NE, Stewart CW. Corneal ectasia after myopic laser in situ keratomileusis: a long-term study. Clin Ophthalmol. 2012;6:1801–1813. doi:10.2147/OPTH.S37249
6. Brooks NO, Greenstein S, Fry K, Hersh PS. Patient subjective visual function after corneal collagen crosslinking for keratoconus and corneal ectasia. J Cataract Refract Surg. 2012;38(4):615–619. doi:10.1016/j.jcrs.2011.11.029
7. Hafezi F, Kanellopoulos J, Wiltfang R, Seiler T. Corneal collagen crosslinking with riboflavin and ultraviolet A to treat induced keratectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2007;33(12):2035–2040. doi:10.1016/j.jcrs.2007.07.028
8. Hersh PS, Greenstein SA, Fry KL. Corneal collagen crosslinking for keratoconus and corneal ectasia: one-year results. J Cataract Refract Surg. 2011;37(1):149–160. doi:10.1016/j.jcrs.2010.07.030
9. Alhayek A, Lu PR. Corneal collagen crosslinking in keratoconus and other eye diseases. Int J Ophthalmol. 2015;8(2):407–418. doi:10.3980/j.issn.2222-3959.2015.02.35
10. Kanellopoulos AJ. Comparison of sequential vs same-day simultaneous collagen cross-linking and topography-guided PRK for treatment of keratoconus. J Refract Surg. 2009;25(9):S812–S818. doi:10.3928/1081597X-20090813-10
11. Krueger RR, Kanellopoulos AJ. Stability of simultaneous topography-guided photorefractive keratectomy and riboflavin/UVA cross-linking for progressive keratoconus: case reports. J Refract Surg. 2010;26(10):S827–S832. doi:10.3928/1081597X-20100921-11
12. Kanellopoulos AJ, Binder PS. Management of corneal ectasia after LASIK with combined, same-day, topography-guided partial transepithelial PRK and collagen cross-linking: the Athens protocol. J Refract Surg. 2011;27(5):323–331. doi:10.3928/1081597X-20101105-01
13. Yousif MO, Elkitkat RS, Edrees ES, Elkitkat RS. Introducing a revised tissue saving protocol for combined topography-guided photorefractive keratectomy and cross linking in keratoconic corneas. Cornea. 2022;13:10–97.
14. Padmanabhan P, Rachapalle Reddi S, Sivakumar PD. Topographic, tomographic, and aberrometric characteristics of post-LASIK ectasia. Optom Vis Sci. 2016;93(11):1364–1370. doi:10.1097/OPX.0000000000000922
15. Hafezi F, Kling S, Gilardoni F, et al. Individualized corneal cross-linking with riboflavin and UV-A in ultrathin corneas: the sub400 protocol. Am J Ophthalmol. 2021;224(4):133–142. doi:10.1016/j.ajo.2020.12.011
16. Gomel N, Negari S, Frucht-Pery J, Wajnsztajn D, Strassman E, Solomon A. Predictive factors for efficacy and safety in refractive surgery for myopia. PLoS One. 2018;13(12):e0208608. doi:10.1371/journal.pone.0208608
17. Tian M, Zhang X, Jian W, Sun L, Shen Y, Zhou X. Long-term follow-up of accelerated transepithelial corneal crosslinking for post-LASIK Ectasia: a Pilot Prospective Observational Study. Front Bioeng Biotechnol. 2021;9:809262. doi:10.3389/fbioe.2021.809262
18. Salgado JP, Khoramnia R, Lohmann CP, Winkler von Mohrenfels C. Corneal collagen crosslinking in post-LASIK keratectasia. Br J Ophthalmol. 2011;95(4):493–497. doi:10.1136/bjo.2010.179424
19. Kymionis GD, Diakonis VF, Kalyvianaki M, et al. One-year follow-up of corneal confocal microscopy after corneal cross-linking in patients with post laser in situ keratosmileusis ectasia and keratoconus. Am J Ophthalmol. 2009;147(5):774–778.e1. doi:10.1016/j.ajo.2008.11.017
20. Yildirim A, Cakir H, Kara N, et al. Corneal collagen crosslinking for ectasia after laser in situ keratomileusis: long-term results. J Cataract Refract Surg. 2014;40(10):1591–1596. doi:10.1016/j.jcrs.2014.01.042
21. Kobashi H, Rong SS, Ciolino JB. Transepithelial versus epithelium-off corneal crosslinking for corneal ectasia. J Cataract Refract Surg. 2018;44(12):1507–1516. doi:10.1016/j.jcrs.2018.08.021
22. Stulting RD, Trattler WB, Woolfson JM, Rubinfeld RS. Corneal crosslinking without epithelial removal. J Cataract Refract Surg. 2018;44(11):1363–1370. doi:10.1016/j.jcrs.2018.07.029
23. Kanellopoulos AJ. Post-LASIK ectasia. Ophthalmology. 2007;114(6):1230. doi:10.1016/j.ophtha.2007.03.041
24. Wallerstein A, Adiguzel E, Gauvin M, Mohammad-Shahi N, Cohen M. Under-flap stromal bed CXL for early post-LASIK ectasia: a novel treatment technique. Clin Ophthalmol. 2016;11:1–8. doi:10.2147/OPTH.S118831
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.