Back to Journals » Drug Design, Development and Therapy » Volume 18
Novel Strategies Enhancing Bioavailability and Therapeutical Potential of Silibinin for Treatment of Liver Disorders
Authors Selc M ![]() , Macova R
, Macova R ![]() , Babelova A
, Babelova A ![]()
Received 7 August 2024
Accepted for publication 2 October 2024
Published 19 October 2024 Volume 2024:18 Pages 4629—4659
DOI https://doi.org/10.2147/DDDT.S483140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Tin Wui Wong
Michal Selc,1,2 Radka Macova,2,3 Andrea Babelova1,2
1Centre for Advanced Material Application, Slovak Academy of Sciences, Bratislava, Slovakia; 2Department of Nanobiology, Cancer Research Institute, Biomedical Research Center, Slovak Academy of Sciences, Bratislava, Slovakia; 3Department of Genetics, Faculty of Natural Sciences, Comenius University Bratislava, Bratislava, Slovakia
Correspondence: Michal Selc, Centre for Advanced Material Application, Slovak Academy of Sciences, Bratislava, 84511, Slovakia, Tel +421-2-32295-175, Email [email protected]
Abstract: Silibinin, a bioactive component found in milk thistle extract (Silybum marianum), is known to have significant therapeutic potential in the treatment of various liver diseases. It is considered a key element of silymarin, which is traditionally used to support liver function. The main mechanisms of action of silibinin are attributed to its antioxidant properties protecting liver cells from damage caused by free radicals. Experimental studies conducted in vitro and in vivo have confirmed its ability to inhibit inflammatory and fibrotic processes, as well as promote the regeneration of damaged liver tissue. Therefore, silibinin represents a promising tool for the treatment of liver diseases. Since the silibinin molecule is insoluble in water and has poor bioavailability in vivo, new perspectives on solving this problem are being sought. The two most promising approaches are the water-soluble derivative silibinin-C-2’,3-dihydrogen succinate, disodium salt, and the silibinin-phosphatidylcholine complex. Both drugs are currently under evaluation in liver disease clinical trials. Nevertheless, the mechanism underlying silibinin biological activity is still elusive and its more detailed understanding would undoubtedly increase its potential in the development of effective therapeutic strategies against liver diseases. This review is focused on the therapeutic potential of silibinin and its derivates, approaches to increase the bioavailability and the benefits in the treatment of liver diseases that have been achieved so far. The review discusses the relevant in vitro and in vivo studies that investigated the protective effects of silibinin in various forms of liver damage.
Keywords: silybin, bioavailability, liver disease, silibinin-phosphatidylcholine complex, silibinin-C-2‘ 3-dihydrogen succinate
Graphical Abstract:

Introduction
The liver is one of the most important organs in the body and plays a key role in metabolism, protein synthesis, bile production, vitamin and mineral storage, and detoxification while maintaining overall health and body homeostasis.1,2 Liver damage due to liver diseases has become a serious global problem, affecting millions of people around the world, accounting for 4% of all deaths worldwide.3 Chronic liver damage characterized by advanced fibrosis may eventually evolve into liver cirrhosis, which represents a major risk factor for the development of hepatocellular carcinoma (HCC).4,5 Unlike liver cirrhosis, the process of liver fibrosis is reversible as long as the cause of the fibrosis is removed.6,7 Several factors may enhance this process such as alcohol consumption, non-alcoholic steatohepatitis (NASH), viral hepatitis (hepatitis B and hepatitis C), autoimmune hepatitis, nonalcoholic fatty liver disease (NAFLD), and cholestatic liver disease.8 The development of chronic inflammation is a common denominator for the progression of these diagnoses to the fibrotic stage. The inflammatory state promotes the transdifferentiation of hepatic stellate cells into proliferating, contractile and migrating myofibroblasts expressing large amounts of extracellular proteins (eg collagen, vimentin, a smooth muscle actin, and extramuscular myosin).9 As a consequence, a gradual accumulation of these proteins in the extracellular matrix occurs, which impairs the physiological structure and function of the liver. Apoptosis of hepatocytes with scar tissue formation gradually replaces the functional and healthy liver tissue leading after long time to irreversible fibrotic changes.10–13 According to the World Health Organization, more than 750,000 people worldwide died from liver cancer in 2022 reaching the second place among deaths from all cancer diseases. It is estimated that by 2035, liver tumors will be responsible for more than 1 million deaths, of which 90% will be most likely HCC.3,14 The increasing number of patients with liver cancer and the limitations of current therapeutic approaches indicate an emerging need for new and more efficient treatment possibilities. One such could be offered by silibinin, a bioactive component of milk thistle extract (Silybum marianum), belonging to the Asteraceae family.
S. marianum has been used for over 2000 years to treat liver and biliary disorders. The first record of milk thistle can be found in the Old Testament (Genesis 3:18). Since ancient times, the Greeks (Theophrastus of Eresos, 4th century B.C.) and Romans (Pedanios Dioscorides, 50 A.D. and Plinius the Elder, 1st century A.D.) have utilized this herb for their medicinal properties and used as a hepatoprotective agent. The seeds, also known as lady’s thistle or Saint Mary’s thistle, are particularly helpful in protecting and maintaining the liver’s health.15,16 During the Middle Ages, milk thistle was used as an antidote for poisoning due to snake bite. Likewise, in the next centuries, herbalists and scientists recommended the use of milk thistle to treat various diseases, especially liver pathologies. Nowadays, the use of milk thistle in medicine has been well documented for the treatment of liver disorders such as viral hepatitis, nonalcoholic liver disease, alcoholic liver disease, cirrhosis, drug-induced liver injury, and mushroom poisoning.17,18
This scientific review critically examines the literature reporting the use of silibinin, the major bioactive component of silymarin, in the treatment of liver diseases to offer a comprehensive overview of this area’s current state of knowledge. Pharmacodynamics and pharmacokinetics of silibinin, the results of cell culture and animal studies will be discussed together with ongoing clinical trials to gain an overall picture of silibinin advantages for liver protection. Furthermore, possible challenges and directions for future research will be outlined.
Chemistry of Silibinin
For the first time, silibinin was isolated by G. Möschlin within his dissertation work.19 The structure of silibinin was originally described by organic chemist Pelter and pharmacist Hansel in 1968 and 1975.20,21 Silibinin, also called silybin, is a type of polyphenolic flavonoid with a molecular formula of C25H22O10, a molecular weight of 482.44 g/mol, and CAS No. 22888–70-6. Silibinin itself is a mixture of two diastereomers, silybin A (2R, 3R, 10R, 11R) and silybin B (2R, 3R, 10S, 11S), in an approximately equimolar ratio and makes up the majority of the silymarin mixture (approx. 40–60%). Other main components of silymarin are flavonolignans silychristin (15–25%), silydianin (10%), isosilybin A (10%), 2,3-dehydrosilybin (5%), isosilybin B (<5%) and isosilychristin (3%), along with the flavonoid taxifolin (Figure 1).22,23
 |
Figure 1 The main flavonolignans and one flavonoid (taxifolin) of silymarin - an extract from the seeds of Milk thistle (Silybum marianum). Structure of molecules were drawn using ACD/ChemSketch software based on data from the PubChem database.24 |
Silibinin is quite resistant to reduction, but is easily oxidized to 2,3-dehydrosilybin. Long-term heating above 100 °C causes damage to its skeleton structure.25 The molecule of silibinin shows its maximum absorption at a wavelength of 289 nm (Figure 2).
 |
Figure 2 Wave spectrum of pure silibinin (Merck) with a maximum peak 289 nm (Our unpublished data). |
This absorption maximum provides two advantages. The first one is that thanks to this, the amount of silibinin in the cell can be determined. The absorption spectroscopy can be used not only to determine the internalization of pure silibinin effectively but also to determine silibinin complexes or silibinin-coated nanoparticles within the cells. In our laboratory, this method has been applied for the determination of bovine serum albumin (BSA) and sodium oleate-coated iron oxide nanoparticles in A549 cells.26
The second advantage proves to be useful in in vitro release rate studies that measure the quantity of silibinin released from the nanoparticle into the solution. In the case of solid lipid or mesoporous nanoparticles, it has been observed that silibinin exhibits a very slow release at pH 7.4 (physiological), and even after 72 hours, it was not released from the nanoparticle. This slow release is beneficial in the terms of nanoparticle-mediated prolongation of the drug release, which ultimately leads to an increase in its bioavailability.27,28
A similar result was achieved with poly(lactic-co-glycolic acid) and polyethylene glycol (PLGA-PEG)-modified Fe3O4 magnetic nanoparticles displaying 80.4% of silibinin released from the nanoparticles over 2 days.29 On the other side, it has been observed that in case silibinin was bound to gold nanoparticles, more than 70% of silibinin was released from the nanoparticle at pH 7.4 after only 6 hours. Interestingly, if the pH changed to 5 (simulating the pH of the tumor microenvironment), 100% of the silibinin was released from the nanoparticle after 6 hours.30 This release rate of silibinin from gold nanoparticles is even slightly higher than that of silymarin, given that only 42% of silymarin was released from the nanoparticle after 6 hours.31 Such rapid release of silibinin from nanoparticles may not necessarily be disadvantageous. The liver is capable of removing 30–99% of nanoparticles from the bloodstream with the highest distribution occurring within the first 6 hours after administration.32,33 This possibility to design nanoparticles with early or late release of silibinin opens up more opportunities for better treatment of liver pathologies.
Biological Properties of Silibinin
Silibinin is considered the most bioactive component of silymarin.34–36 The three most common effects are attributed to silibinin impact on liver cells: it acts as an antioxidant, modulates inflammation, and alleviates fibrogenesis.
Silibinin possesses the highest antioxidant activity among all silymarin compounds, which is demonstrated by its inhibition of ROS (99.5%) compared to silybin A (68.7%), silybin B (74%), or silymarin (99.2%).37 Silibinin protection of the liver cells from oxidative intracellular-free radicals is mediated by increasing the activity of enzymes such as superoxide dismutase and peroxidase, as well as by increasing the concentration of glutathione.38 Silibinin can also function as a metal chelator. In the model of arsenic-induced hepatotoxicity in rats, silibinin successfully reduced the levels of liver enzymes such as alanine transaminase (ALT), aspartate transaminase (AST), alkaline phosphatase (ALP), gamma-glutamyltransferase (GGT), and bilirubin to the level of control animals. The amount of damaged DNA was also decreased and histologically, no inflammation, necrosis, or vacuolization was observed in the hepatocytes of the arsenic-exposed rats.39 The antioxidant and hepatoprotective effects of silibinin were further confirmed in a model of non-alcoholic steatosis of the liver.40 Rats with NASH that received silibinin-phosphatidylcholine complex as a food supplement showed a lower grade of liver steatosis, decreased plasma insulin, reduced levels of malondialdehyde, O2∙− and glutathione and attenuated inflammatory responses. Interestingly, silibinin also reduced the amount of the TNF-α in this rat model,40 which is in line with its anti-inflammatory properties, that are discussed further.
The mechanism underlying the anti-inflammatory effects of silibinin lies in the modulation of the NFκB protein. NFκB following its activation moves into the nucleus, binds to DNA and acts as a transcription factor triggering the activation of genes involved in inflammatory responses, cell survival, differentiation, and growth.41 In vitro, silibinin inhibited the activation of NFκB and expression of 3-hydroxy-3-methylglutaryl-CoA synthase 2 at the transcriptional and translational levels in healthy mouse hepatocytes.42 Silibinin also reduced oxidative damage and inflammation in oleic acid-induced HepG2 cells by upregulating NRF2, downregulating CYP2E1 and CYP4A, and decreasing intracellular NO levels.43 In vivo, the impact of silibinin on lipotoxicity has been studied in a mouse model of NASH. Silibinin treatment was shown to counteract liver injury by suppressing oxidative stress-mediated lipotoxicity and activity of NFκB p65 and p50 subunits.44
The antifibrotic properties of silibinin have been demonstrated in vitro by the inhibition of profibrotic activity of human hepatic stellate cells, including reduced proliferation and de novo synthesis of procollagen type I via direct inhibition of phosphorylation of ERK, MEK, Raf, and IκBa, eventually being more effective than silymarin.45,46 The inhibition of stellate cells proliferation is dose- and time-dependent, showing that the strongest inhibition of the proliferation of LX-2 cells is achieved after 96 hours by 100 µM (48 µg/mL) silibinin affecting the cell cycle targets eg Akt, p27 or sirtuin signaling.47 In vivo, silibinin also attenuated iron-induced liver fibrosis as well as thioacetamide-induced liver damage in rodents.48,49 On the other hand, neither silibinin nor silymarin were able to decrease the carbon tetrachloride (CCl4)-induced accumulation of collagen in the liver in the rat fibrotic model.50
However, silibinin also possesses additional positive properties beyond those mentioned above. It is highly beneficial in protecting hepatocytes, for example, by preventing the penetration of various toxins into the cell, preventing apoptosis through modulation of intracellular mechanisms, and also by inhibiting the hepatitis C virus infection even more effectively than silymarin.37,51 The anti-hepatocarcinogenic potential of silibinin has also been demonstrated. In a diethylnitrosamine/2-acetylaminofluorene/CCl4-induced HCC model in rats, silibinin inhibited the growth of cancerous lesions at the lowest applied dose (30 times lower than silymarin dose and 40 times lower than total milk thistle extract dose) exhibiting similar or even superior results, compared to silymarin and the total extract.52 Interestingly, the opposite result was achieved by Miguez et al. Comparing the hepatoprotective effect of silymarin and silibinin dihemisuccinate (a soluble form of silibinin) in isolated rat liver cells revealed that 200 times higher (2 mM; 964 µg/mL) concentration of silibinin was required to achieve the same effect as 0.01 mM (4.8 µg/mL) silymarin to effectively protect the cells against allyl alcohol.53
All these properties make silibinin not only a molecule useful in the treatment of liver diseases, but also predict its benefits in the treatment involving other organs such as kidneys, lungs, brain, prostate, or pancreas.54–60
Bioavailability of Silibinin
Silibinin has highly hydrophobic and non-ionizable properties, making it practically insoluble in water (50 μg/mL).61,62 It is poorly soluble in ethanol (0.1 mg/mL) or methanol and insoluble in nonpolar solvents such as chloroform or petrolether. However, the solubility of silibinin increases significantly in various organic solvents, such as acetone, dimethylformamide, or dimethyl sulfoxide (≥20 mg/mL). Importantly, low solubility in water considerably affects its bioavailability. After oral administration in rodents (50 mg/kg dose), silibinin possesses a low absorption efficiency and is rapidly absorbed in the stomach, with a Tmax of approximately 0.5 hours and a t1/2 of approximately 1–2 hours in different tissues or with a Tmax of approximately 1.5 hours and a t1/2 of approximately 3 hours in plasma (Figure 3).63,64
 |
Figure 3 Bioavailability of silibinin in different organs and plasma after a single oral application of pure silibinin at a dose of 50 mg/kg body weight in rodents. Levels of total silibinin was measured by HPLC or LC-MS method. Data were obtained from published levels of silibinin in the tissues and plasma, and represent mean ± SD.63,64 |
Silibinin absorption in the gastrointestinal tract depends on various factors such as the presence of other solubilizing substances like amino acids, cholesterol, fats, flavonoids, proteins, etc. Silibinin is swiftly and equally distributed between the blood and hepatobiliary system, resulting in higher levels of silibinin in bile fluid than in plasma. The absolute oral bioavailability of silibinin in rats was 0.95%.65 Therefore, various approaches to increase the bioavailability of silibinin have been proposed. The most common methods include using a micellar drug delivery system or water-soluble silibinin derivatives as described below.
Micellar Silibinin Delivery System
The water solubility of silibinin can be significantly increased by using a polymeric micellar system, which can act as a potential delivery carrier, thus enhancing its bioavailability. The common approach to reach the formation of a silibinin-phospholipid complex is the use of phosphatidylcholine. As a result, a complex named Silipide (also referred as IdB 1016) is being created, which was demonstrated more than 30 years ago.66,67 After oral administration of Silipide or pure silibinin at a concentration of 200 mg/kg, the maximum concentration of silibinin from Silipide in the rat plasma was more than 20 times higher for both forms, unconjugated and total.68 Four times lower dosage of pure silibinin led to a similar effect in rats as a pure silibinin at a dosage of 200 mg/kg.64 Interestingly, after a single oral administration of pure silibinin at 2.5 times higher dosage, the maximum concentration of total and unconjugated silibinin in plasma was still lower and was found in plasma for a shorter time than in the case of Silipide (Figure 4).65
 |
Figure 4 Level of total (A) and unconjugated (B) silibinin in rat plasma after a single oral application of Silipide (200 mg/kg) or pure silibinin (50, 200, or 500 mg/kg). Data were obtained from published levels of total and unconjugated silibinin in plasma, and represent mean ± SD.64,65,68–70 |
From a pharmacological perspective, silipide treatment significantly improved liver health by effectively reducing inflammation and lipid peroxidation, decreasing plasma insulin and TNF-α, and successfully normalizing liver weight and GSH levels in mice as well as improved liver enzymes ALT, AST, GGT, and total bilirubin in patients with chronic active hepatitis.40,67,71 The effects of silipide shown in rats have also been confirmed in humans in clinical studies. Nine healthy volunteers received a single oral dose of Silipide or silymarin and the amount of the substance in the plasma was monitored after 0.5–12 hours. A plasma level of Silipide was 4 times higher than that of silymarin, in one subject even extremely high - up to 80 times higher.66 Today, this complex is known under the trademark Siliphos® and entered the second phase of clinical testing as a drug for the treatment of liver diseases.72
The second most frequent micellar drug delivery system is the complex silibinin-phosphatidylcholine-vitamin E (trademark Realsil®), which is in the Phase III of clinical trials for the treatment of a steatosis or NASH.73,74 D-α-tocopherol supplementation alone leads to a decrease of collagen α1(Ι) gene expression both in vitro and in vivo in the liver of normal mice and in cultured hepatic stellate cells. The combination of silibinin, phosphatidylcholine, and vitamin E has been found to have hepatoprotective, anti-inflammatory, and antifibrotic effects. This combination has been previously tested to be effective in reducing hepatic fibrosis in rats with bile duct ligation. The complex was administered orally and was successful in preventing liver injury, stellate cell proliferation and activation, as well as collagen deposition.75
Water-Soluble Silibinin Derivatives
An alternative method to increase silibinin bioavailability, water-soluble silibinin derivatives are used. One of the derivates, known as silibinin-C-2’,3-dihydrogen succinate, disodium salt, known as Legalon® SIL (further in the text as Legalon), preserves the hepatoprotective properties of the original silibinin. Legalon has been approved for use in numerous European countries since 1984. This medicine is commonly used to treat Amanita phalloides intoxication. One vial of Legalon contains 528.5 mg of silibinin-C-2’,3-dihydrogen succinate, disodium salt, which corresponds to 315 or 350 mg of silibinin according to HPLC or DNPH analyses.76 Since 1982, many articles have been published showing that after mushroom poisoning and the administration of Legalon alone or in combination with penicillin G, patients survived (almost 93%).76 However, Legalon is suitable not only for this type of liver intoxication. An in vitro study was conducted to determine its effectiveness in reducing the expression of the hepatitis C virus in human hepatoma cells. The study results revealed that treatment with Legalon significantly reduced hepatitis C virus (HCV) RNA and protein levels. Additionally, Legalon downregulated the heme oxygenase-1 RNA while upregulating the Nrf2 protein. These findings indicate that Legalon may be an effective alternative or complementary therapy for the treatment of HCV infection.77 In vitro results have later been confirmed in vivo. Chronically HCV-infected mice were treated daily by intravenous Legalon for 14 days at doses of 61.5, 265, or 469 mg/kg. Legalon effectively blocked viral production across all dosages in a dose-dependent manner. Legalon also resulted in a continuous second-phase viral decline and increased anti-inflammatory and antiproliferative gene expression in human hepatocytes.78 Actually, 8 clinical studies for the treatment of hepatitis C virus are underway (more in the clinical studies section).
Another type of water-soluble form of silibinin is silibinin meglumine, a silibinin-amino-sugar meglumine complex. Results showed that oral silibinin meglumine was an effective in reducing overall lung tumor volume.79 The solubility of silibinin is also increased by the phosphodiester bond that binds two silibinin monomers. Such phosphate-linked silibinin dimers have approximately 50-times higher water solubility, and higher antioxidant activity than pure silibinin monomers.80 The glycosylated derivatives of silibinin demonstrated exceptional solubility in water, exceeding 15 mg/L, almost 40 times more than pure silibinin. Upon a thorough biological evaluation, it was observed that these new derivatives exhibited strong cellular anti-proliferative activities. However, it is important to note that pure silibinin outperformed these derivatives in inhibiting proliferation in HepG2 and Hep3B cell lines.81
Silibinin in Experimental Research
Silibinin properties have been confirmed by many publications. By the end of 2023, more than 2100 publications containing the keywords “silibinin” or “silybin” were uploaded to PubMed. On the other hand, over 1300 publications contained the keyword “isosilybin OR silydianin OR silychristin OR isosilychristin OR taxifolin OR dehydrosilybin OR dehydrosilibinin”. As expected, the number of publications containing the keyword silymarin is the highest (over 4500 by the end of 2023) because it is a general group of all milk thistle flavonolignans and flavonoids. Nevertheless, an average of almost 100 new scientific articles with “silibinin” have been published every year since 2000 (Figure 5). Of note, the second most researched silymarin molecule – taxifolin shows an average of almost 50 new articles added every year despite the fact that taxifolin occurs in various other organisms.
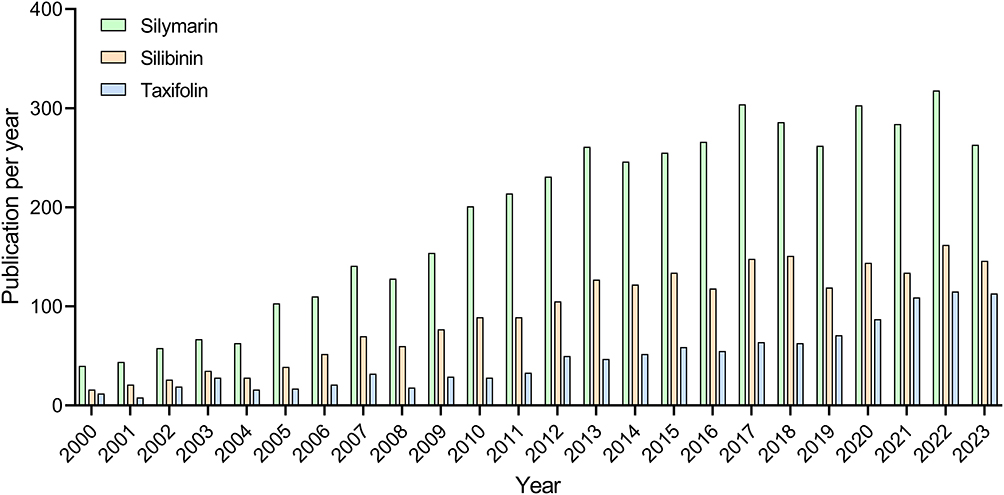 |
Figure 5 The number of publications since 2000, according to the PubMed database, in which the word silymarin, silibinin, or taxifolin is mentioned. On average, there have been almost 200 new publications with silymarin, 100 with silibinin, and 50 with taxifolin per year since 2000. However, since 2014, the number of new publications has increased significantly, with an average of almost 280 new publications with silymarin, 140 with silibinin, and 80 with taxifolin being published annually. |
In vitro Experiments
Several in vitro experiments have been published aiming to determine the effect of silibinin and its derivatives on liver tumor cells, particularly HepG2, HuH7 hepatocytes, and Hep3B cells. Multiple studies typically include the measurement of cytotoxicity/proliferation using the MTT assay. Analyzing the results from 14 of these publications (cited in Table 1), the estimated average IC50 value of pure silibinin reached approximately 230 µM in HepG2 cells after 24 hours of exposure (Figure 6). Fewer publications are available for HuH7 and Hep3B cells, however, the cytotoxic profiles seem to be similar as for HepG2 cells. In the case of non-tumor mouse cell lines AML12 and FL83B and primary rat hepatocytes, the IC50 value exceeds 300 µM. The original findings and relevant citations are described in Table 1. These results show that in human cancer cell lines, silibinin inhibited growth, promoted apoptosis, suppressed HIF-1α accumulation, activated Akt, reduced VEGF, and improved pyroptosis.82 Silibinin also affected liver cell metabolism by regulating triglycerides, nitric oxide, oxidative stress, glucolipid metabolism and reduced lipid accumulation.43 Importantly, silibinin was able to reduce the genotoxic effect of Benzo[a]pyrene, bleomycin, and aflatoxin B1.83 In non-cancerous human cells, silibinin was shown to reduce ROS production and inhibit the pro-fibrogenic actions of hepatic stellate cells (HSC) by reducing mRNA levels of TGF-β1, COL1A1, TIMP-1, and MMP-2.46 Silibinin also inhibited the proliferation and motility of cells and de novo synthesis of extracellular matrix components. Similar effects were observed in animal cells, especially mouse lines and mouse and rat primary hepatocytes.
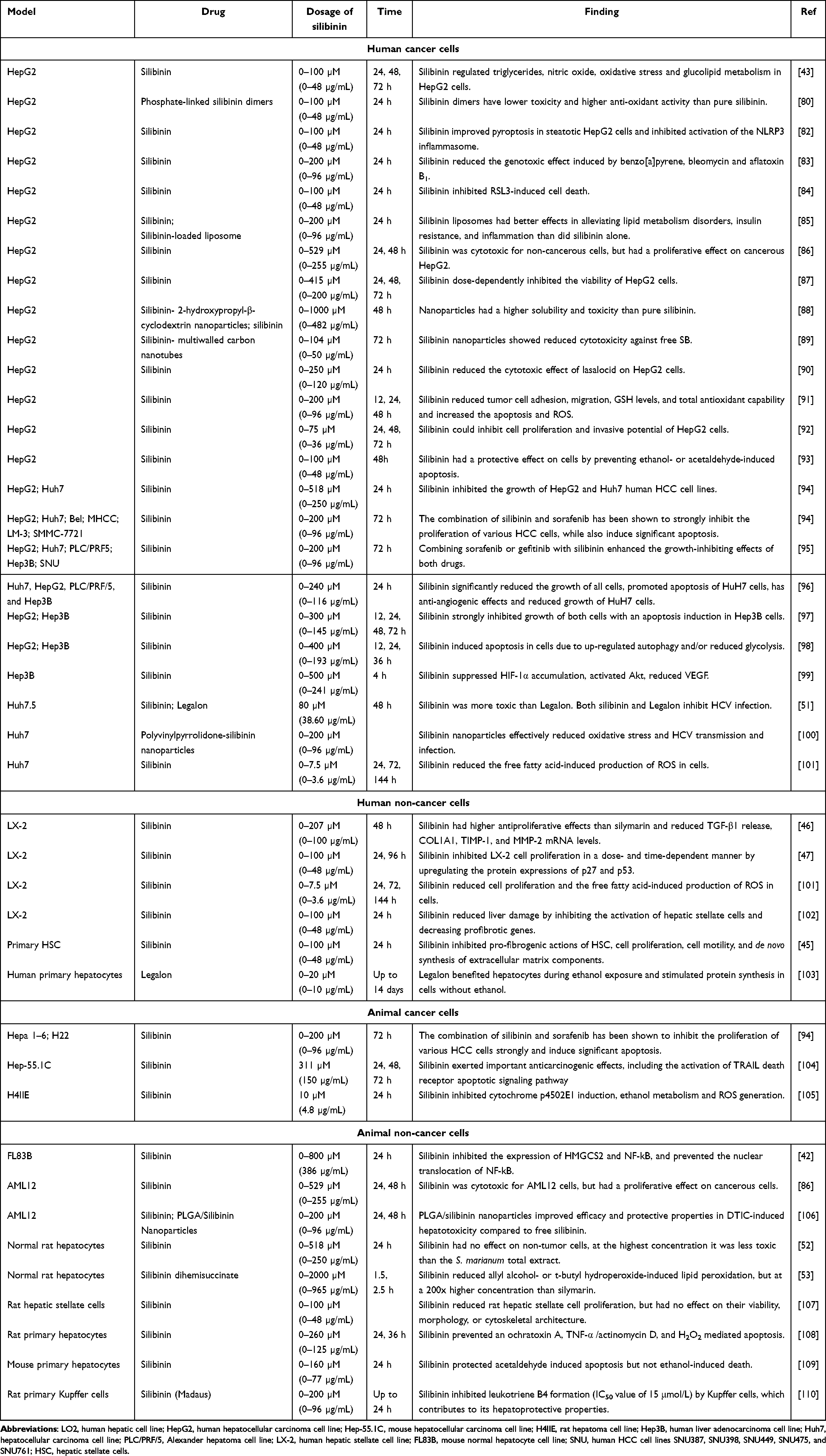 |
Table 1 The Effect of Silibinin on Human and Rodent Cancerous or Noncancerous Cells |
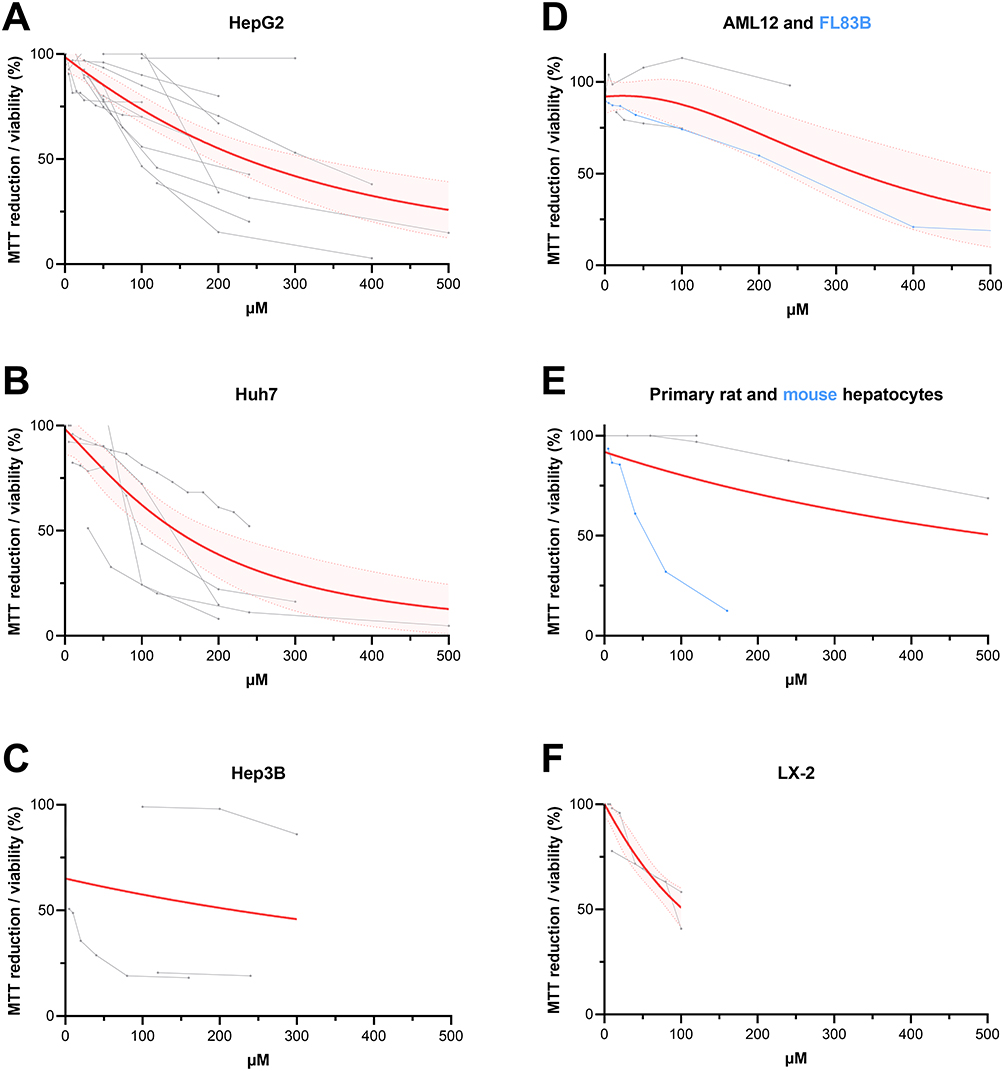 |
Figure 6 The cell viability/reduction rate of MTT dye after 24 hours of exposure to silibinin in cancerous HepG2 (A), Huh7 (B), Hep3B (C) or noncancerous AML12, FL83B (D), LX-2 (F), human (A–C, F) or animal (D) cell lines or primary animal hepatocytes (E). The gray lines represent the measurements from the values published in articles. The red line represents the Lorentzian (Cauchy) model of nonlinear regression from grey lines with a 95% confidence level. Citations for selected cell lines and time point 24h are available in Table 1. |
In vivo Experiments
Based on the results of in vitro experiments, in vivo studies are designed basically according to two main criteria – used silibinin drug and administration route. The used substance is either pure silibinin or modified silibinin (most often a water-soluble derivative or a combination of phospholipids). The methods of drug administration involve per os (either supplemented by diet or by gavage), intraperitoneal, and intravenous applications. Performing administration route per os, the average applied dose was 150 mg/kg applied at average of 25 doses, with approximately 2700 mg/kg total dose of applied silibinin. Intraperitoneal administration was performed at an average of 8 doses with the total injected dose of silibinin approximately 350 mg/kg. Intravenous administration resulted in 40 mg/kg of total injected silibinin applied at an average of 4.5 doses. A more detailed summary of individual experiments, concentrations of silibinin, and administered doses can be found in Supplementary Table 1. The differences between the doses of pure silibinin and modified silibinin were not significant (Figure 7). The original findings and relevant citations are described in Table 2.
 |
Table 2 The Effect of Silibinin on Animals in vivo |
 |
Figure 7 The total dose of silibinin was calculated as a single dose of silibinin multiplied by number of administrations as given in respective publications. Each dot represents one in vivo experiment with silibinin, the grey dot represents pure silibinin, the green dot corresponds to water-soluble silibinin, the red dot represents the combination with phospholipids, the blue dot represents silibinin nanoparticles, and the yellow dot represents other combinations (with vitamin E, Puert tea or collagenase I). The lines represent mean ± SEM. All publications are mentioned in Table 2. Shapiro–Wilk normality test was used to test distribution. Statistical differences are calculated by unpaired t-test with Welch’s correction. The original findings and relevant citations are described in Table 2 and Supplementary Table 1. |
Silibinin in vivo exhibited a range of hepatoprotective effects, making it a promising therapeutic agent for various liver diseases. It activated macrophages and suppressed necroptosis and necroinflammation, while simultaneously reduced serum liver enzyme levels and improved histological status. This reduction in liver enzymes depends on the type of silibinin molecule and the route of administration. Serum ALT and AST levels are least reduced by pure silibinin administered intravenously, while modified silibinin administered intravenously reduced liver disease the most (Figure 8A and B). If the decrease in ALT and AST levels when calculating the total dose given to the animal is considered, it can observed that intravenously administered modified silibinin is about 25 times more effective than orally administered pure silibinin, and 5 times more effective than intraperitoneally administered pure silibinin (Figure 8C and D).
 |
Figure 8 Effect of pure silibinin (grey dot) and modified silibinin (green dot: water-soluble silibinin; red dot: combination with phospholipids; blue dot: silibinin nanoparticles; yellow dot: the combination with other supplements) on the serum level of ALT and AST according to the published data. The values are expressed as the ratio of the treated to the untreated diseased animal (A and B). 100% - animal model of disease; 0% - healthy animal. Efficacy is expressed as the ratio of ALT or AST to the total administered dose of silibinin, normalized to per os pure silibinin as the smallest changes were detected compared to other routes of administration (C and D). Shapiro–Wilk normality test was used to test distribution. Statistical differences were calculated by Welch and Brown-Forsythe one-way ANOVA with Dunnett correction. *(p<0.05), **(p<0.01), ***(p<0.001), ****(p<0.0001). The original findings and relevant citations are described in Table 2 and Supplementary Table 1. |
Clinical Studies
Clinical studies using silibinin started in 1980–1981 when the use of Legalon (silibinin-C-2’,3-dihydrogen succinate, disodium salt) was investigated in 18 cases of Amanita phalloides intoxication. It has been found that the intravenous administration of silibinin, up to 48 hours following mushroom ingestion, was an effective measure in preventing severe liver damage.173 Since then, the use of silibinin has been recorded in the US database, where the National Library of Medicine currently registers 22 clinical trials related to silibinin, while another 8 trials have been registered in the EU Clinical Trials Register. These clinical studies focus apart from the main topic of liver protection on the treatment of other different diseases such as lung, brain, prostate, and kidney diseases that also could benefit from silibinin. For this review, only studies for the treatment of liver disease (n = 17) are included, and these can be divided into two groups:
- studies that employed water-soluble derivate of silibinin as the drug (n = 11),
- studies that used the silibinin-phospholipid complex (n = 6).
The water-soluble derivative of silibinin was represented by Legalon. Just for one study, Silibinin meglumine derivative was used.174 Interestingly, 9 out of 11 studies focused on the effects of silibinin derivative on hepatitis C virus infection175–178 and one study focused on the clinical testing of Legalon as an antidote for Amanita phalloides poisoning (NCT00915681).
Legalon treatment proved to be successful in hepatitis C virus-coinfected patients with previous peginterferon-ribavirin treatment failure. The treatment with 5, 10, 15, or 20 mg/kg/day of Legalon for 14 days showed no significant adverse events or drug–drug interactions, but importantly, viral load after the two highest dosages was undetectable. This suggested silibinin a promising option for patients with HIV/HCV-coinfection.175,176 Moreover, it displayed significant antiviral activity also in patients with established HCV recurrence on the graft who did not respond to standard therapies and was well tolerated by patients during the peri-transplant period.177,178
The study in which a silibinin derivative – silibinin meglumine – was used was performed in 2016 and involved patients with the drug-induced liver damage. Currently, there is no recommended therapy for the treatment of drug-induced liver injury, so the study aimed to compare the effect of silibinin meglumine versus patients with only supportive treatment or no treatment. In the silibinin group, patients received 450 mg silibinin meglumine oral tablets for 24 days. There was a significant resumption rate of ALT and AST in the silibinin group.174
Clinical studies based on silibinin-phospholipid complexes involve silibinin and phosphatidylcholine complex, known as Silipide or IdB1016 (Siliphos), or a complex of silibinin, phosphatidylcholine, and vitamin E acetate (α-tocopherol) (Realsil), which is in the phase III of clinical testing.73,74,179 Silibinin–phosphatidylcholine complex capsules were found to be more effective in providing superior bioavailability compared to conventional silymarin tablets, probably by facilitating the transit of the substance across the gastrointestinal mucosa.66,180
An interesting question about a maximum-tolerated dose despite very little to no adverse effects of silibinin treatment has not yet been answered. A Phase I study investigated the maximum tolerated dose per day of Siliphos in patients with advanced hepatocellular carcinoma and hepatic dysfunction. Three participants enrolled in the trial, consumed 2 g of Siliphos per day. By day 56, there was a significant improvement in the liver function abnormalities and inflammatory biomarkers of the one patient, but all of them died within 23 to 69 days of enrolling, likely due to hepatic failure. The maximum tolerated dose could not be established, and it is unclear whether the deaths were caused by the study drug.181
In a phase I/II study, the effects of Siliphos in patients with chronic hepatitis C and varying degrees of liver fibrosis were monitored. After 12 weeks of treatment with Siliphos (120, 240, or 360 mg of silibinin), body iron stores were reduced, particularly in patients with stage III or IV fibrosis.182
The effects of the second silibinin-phospholipid complex were investigated in patients with NAFLD. Oral administration of Realsil (303 mg of silibinin-phospholipid complex, 10 μg of vitamin D, and 15 mg of vitamin E) twice a day for 6 months significantly improved various factors estimated in patients such as glycemia, insulinemia, HOMA-IR, ALT, C-reactive protein, and thiobarbituric acid reactive substance.183
Different preparation of Realsil (silibinin 94 mg, phosphatidylcholine 194 mg, and vitamin E acetate 50% 89.28 mg) improved oxidant/antioxidant status and lipid composition in liver steatosis or steatohepatitis-diagnosed patients. NAFLD patients orally receiving Realsil twice a day for 12 months displayed improved steatosis, lobular inflammation, hepatocellular ballooning, plasma levels of AST, ALT, or γGT, and insulin level. This provides a solid base for further research and development of effective treatments for NAFLD or NASH employing silibinin.73,74
Administration of Realsil also led to positive results in patients with chronic hepatitis C treated with Pegylated-Interferon-α2b and Ribavirin. Patients who received Realsil once daily for 12 months in addition to this conventional treatment showed improved liver function and reduced levels of liver scarring markers. The improvement has been attributed to the direct effect of Realsil on hepatic stellate cells and its antioxidant properties.179
Legalon is a drug that is currently used in medical practice. However, when it comes to clinical studies, Siliphos and Realsil are more commonly studied in non-alcoholic steatohepatitis, non-alcoholic fatty liver disease, and liver fibrosis, which are already involved in phase III studies. A list of all clinical trials with silibinin, but not silymarin is given in Table 3.
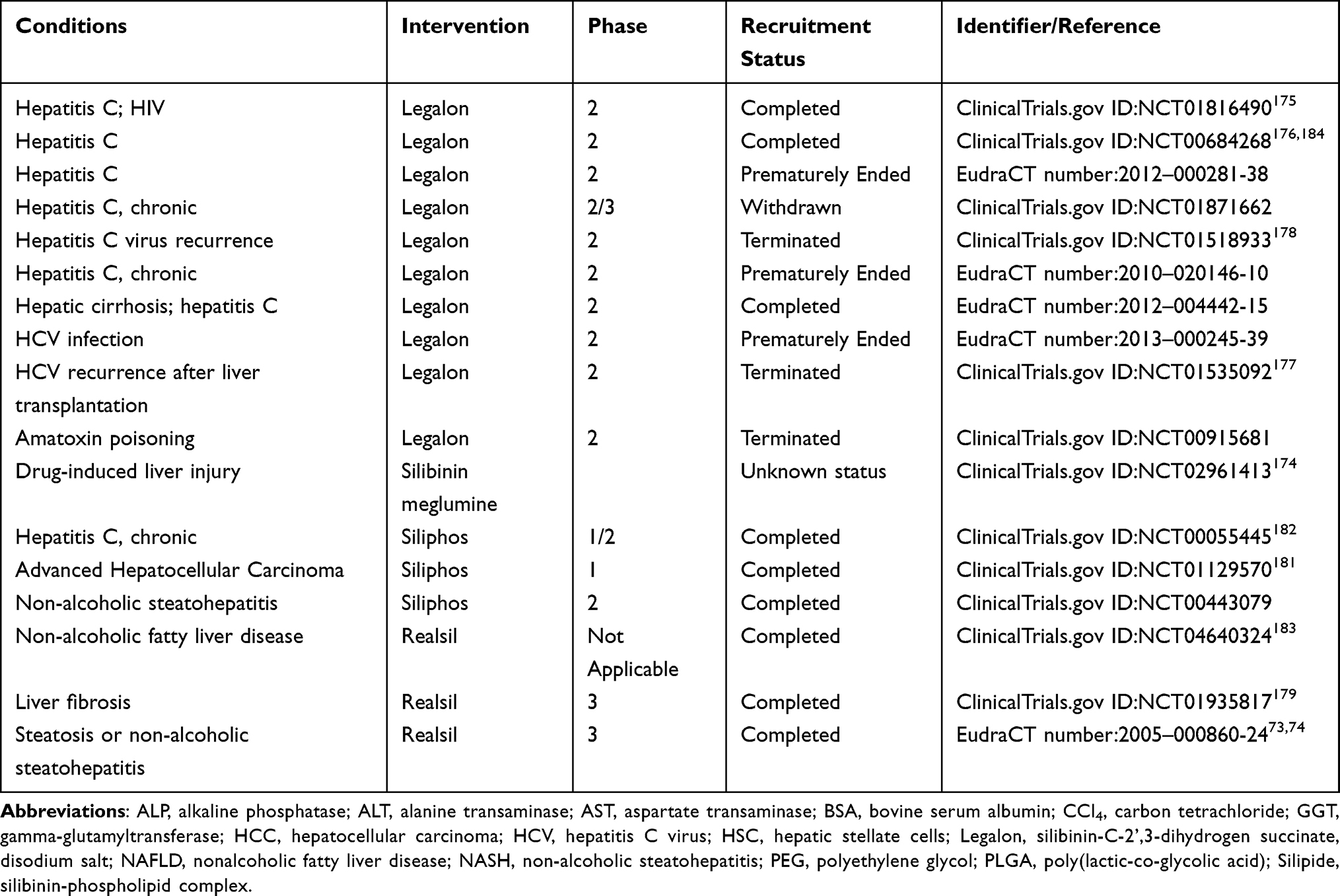 |
Table 3 List of Clinical Trials Involving Silibinin Therapies for Treating Liver Diseases |
Adverse Effects of Silibinin
Silibinin is very well tolerated, and no serious side effects were observed in clinical or in vivo studies. On the other hand, milk thistle ingestion may cause gastrointestinal problems, headaches, skin reactions, neuropsychological events, arthralgia, rhinoconjunctivitis, impotence, and anaphylaxis. However, causality is rarely addressed in available reports. Adverse effects incidence was approximately equal in milk thistle and control groups in randomized trials.185 As mentioned below, the toxicity tests were conducted not only with pure silibinin, but also with Siliphos.
Based on the results of an acute toxicity study in adult female Wister rats, it can be inferred that the LD50 of orally administrated pure silibinin is higher than 2000 mg/kg. No signs of morbidity or mortality were observed in animals; however, some changes were observed in renal function test parameters and lipid profile (higher bilirubin, creatinine, cholesterol, triglycerides, ALT, and AST) and also a significant increase in the weight of rats after 14 days after being administered single oral doses of silibinin (2000 mg/kg).131 For the intravenous administration of silibinin, the LD50 dose was determined to be 1,056 mg/kg in mice.186
Toxicology tests performed with Siliphos revealed oral acute toxicity to be >5,000 mg/kg in rats, dogs, and monkeys. The 26-week chronic toxicity study confirmed that Siliphos at a dose of 2,000 mg/kg/day was safe in both rats and monkeys. Converted, this would be equivalent to a daily dose of 160 g for an adult person (80 kg).72
The Future in Silibinin Nanomaterials
A promising approach for the treatment of liver diseases apart from the water-soluble derivatives of silibinin and silibinin-lipid complexes is the use of silibinin nanomaterials.187 Nanomaterial properties offer a favorable platform for the improvement of silibinin biocompatibility and targeted tissue enrichment given by higher surface-to-volume ratio or amendment of the solubility. Interestingly, it has been shown that silibinin nanoparticles reach almost 2000 times higher solubility than pure silibinin at pH 6.8. Moreover, silibinin nanoparticles inhibited the proliferation of HepG2 cells more effectively than free silibinin.88 This may be associated to higher accumulation of silibinin - approximately a 100 times higher level of silibinin was detected in the liver when administered in the form of nanoparticles.100 Surely, silibinin nanoparticles can also be functionalized with another molecule, which can further improve therapeutical effect. For example, silibinin-loaded bovine serum albumin nanoparticles resulted in a higher silibinin concentration with a longer duration in rat plasma than pure silibinin.164,188 In addition, after intravenous application of albumin-based silibinin nanoparticles, there is a significantly higher uptake into activated hepatic stellate cells than inactive ones.165 Other types of nanoparticles with confirmed hepatoprotective effects are dextran-phenylboronic acid-silibinin nanoparticles, carboxylated multiwalled carbon nanotubes or PLGA nanoparticles.89,106,189 The biodistribution of silibinin nanoparticles is primarily directed to the liver, where 50% of the administered dose has been detected after half an hour. After 3 hours, around 45% of the administered dose of silibinin nanoparticles was still in the liver.106 A high amount of nanoparticles in the liver is a consequence of their natural biodistribution. In mice, usually 23% of nanoparticles from the administered dose were found in the liver, 27% in the spleen, 7% in the lungs, 5% in the kidneys, 4% in the heart and 4% in the blood following the intravenous application.33 For in vivo models of liver diseases, this is an indisputable benefit, allowing passive targeting of the nanoparticles to the organ.
Among all nanomaterials, silibinin-coated gold nanoparticles may represent a suitable approach for the treatment of liver diseases. The neutral spherical gold nanoparticles alone were thought to mediate hepatoprotective effects, which were confirmed in alcohol-methamphetamine-induced liver injury. Reduction of pro-inflammatory factors, oxidative stress, the activity of Kupffer and hepatic stellate cells leading to slowing down of fibrogenesis through modulation of signaling pathways AKT/PI3K and MAPK as a result of exposure to gold nanoparticles was confirmed in a rat model.190 Given that silibinin coating could importantly increase the therapeutic potential of these nanoparticles, silibinin-gold nanoparticles might be a promising tool for more effective combating of liver fibrosis. Actually, similar outcome has been recently reported for silymarin – gold nanoparticles revealing stronger hepatoprotective effect of silymarin-gold nanoparticle platform compared to silymarin and gold nanoparticles alone.31
Conclusion
Silibinin, a major bioactive component of silymarin, has drawn increasing interest from medical scientific fields for its potential to meaningfully extend available tools for the prevention and treatment of liver diseases. The disadvantage concerning its poor solubility in water and consequent poor bioavailability can be improved by the water-soluble derivatives or the complex formation with phosphatidylcholine. The water-soluble Legalon is already approved in many European countries. The silibinin-phosphatidylcholine complex Siliphos is recently in Phase 3 testing, confirming its significant capability in liver protection and cancer prevention. Moreover, water-soluble derivatives are 5 times more effective after intraperitoneal administration and 25 times more effective after intravenous administration than the orally administered pure silibinin in reducing ALT and AST levels. This modified silibinin demonstrates higher efficacy even at lower total doses. With intraperitoneal administration, on average 10 times lower dose is needed, and with intravenous administration, around 100 times less total dose is required to reach the same effect as with oral administration.
Silibinin gold nanoparticles show enormous potential in increasing the biodistribution of silibinin into the liver. In some cases, this led to a more effective reduction of ALT and AST levels in rodents than by silibinin-phosphatidylcholine complexes. Such synergistic effects of silibinin and gold nanoparticles could be favorably used for highly efficient management of liver disease in future.
Abbreviations
ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BSA, bovine serum albumin; CCl4, carbon tetrachloride; GGT, gamma-glutamyltransferase; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; HSC, hepatic stellate cells; Legalon, silibinin-C-2',3-dihydrogensuccinate, disodium salt; NAFLD, nonalcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; PEG, polyethylene glycol; PLGA, poly(lactic-co-glycolic acid); Silipide, silibinin-phospholipid complex.
Acknowledgments
This study was performed during the implementation of the project Building-up Centre for advanced materials application of the Slovak Academy of Sciences, ITMS project code 313021T081 supported by Research & Innovation Operational Programme funded by ERDF. This work was supported by VEGA grant [No. 2/0116/22, Slovakia] and APVV grant [No. APVV-16-0579, Slovakia]. Author team thank to V. Nemethova from Selecta Biotech SE for creating a graphical abstract using the BioRender program.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Qian H, Chao X, Williams J, et al. Autophagy in liver diseases: a review. Mol Aspects Med. 2021;82:100973. doi:10.1016/j.mam.2021.100973
2. Kalra A, Yetiskul E, Wehrle CJ, Physiology TF. Liver.; Treasure Island. (FL): StatPearls Publishing; 2023.
3. Devarbhavi H, Asrani SK, Arab JP, Nartey YA, Pose E, Kamath PS. Global burden of liver disease: 2023 update. J Hepatol. 2023;79(2):516–537. doi:10.1016/j.jhep.2023.03.017
4. Dhar D, Baglieri J, Kisseleva T, Brenner DA. Mechanisms of liver fibrosis and its role in liver cancer. Exp Biol Med. 2020;245(2):96–108. doi:10.1177/1535370219898141
5. Friedman SL. Hepatic fibrosis and cancer: the silent threats of metabolic syndrome. Diabetes Metab J. 2024;48(2):161–169. doi:10.4093/dmj.2023.0240
6. Issa R, Williams E, Trim N, et al. Apoptosis of hepatic stellate cells: involvement in resolution of biliary fibrosis and regulation by soluble growth factors. Gut. 2001;48(4):548–557. doi:10.1136/gut.48.4.548
7. Iredale JP, Benyon RC, Pickering J, et al. Mechanisms of spontaneous resolution of rat liver fibrosis. Hepatic stellate cell apoptosis and reduced hepatic expression of metalloproteinase inhibitors. J Clin Invest. 1998;102(3):538–549. doi:10.1172/JCI1018
8. Aydin MM, Akcali KC. Liver fibrosis. Turk J Gastroenterol. 2018;29(1):14–21. doi:10.5152/tjg.2018.17330
9. Kisseleva T, Brenner D. Molecular and cellular mechanisms of liver fibrosis and its regression. Nat Rev Gastroenterol Hepatol. 2021;18(3):151–166. doi:10.1038/s41575-020-00372-7
10. Iredale JP. Models of liver fibrosis: exploring the dynamic nature of inflammation and repair in a solid organ. J Clin Invest. 2007;117(3):539–548. doi:10.1172/JCI30542
11. Roehlen N, Crouchet E, Baumert TF. Liver Fibrosis: mechanistic Concepts and Therapeutic Perspectives. Cells. 2020;9(4):875. doi:10.3390/cells9040875
12. Surendran SP, Thomas RG, Moon MJ, Jeong YY. Nanoparticles for the treatment of liver fibrosis. Int J Nanomed. 2017;12:6997–7006. doi:10.2147/IJN.S145951
13. Zhou WC, Zhang QB, Qiao L. Pathogenesis of liver cirrhosis. World J Gastroenterol. 2014;20(23):7312–7324. doi:10.3748/wjg.v20.i23.7312
14. Globocan. Global Cancer Observatory: cancer Today. Lyon, France: International Agency for Research on Cancer. Published 2022. Available from: https://gco.iarc.fr/today.
15. Akhtar MN, Saeed R, Saeed F, et al. Silymarin: a review on paving the way towards promising pharmacological agent. Int J Food Prop. 2023;26(1):2256–2272. doi:10.1080/10942912.2023.2244685
16. Verdura S, Cuyàs E, Ruiz-Torres V, et al. Lung Cancer Management with Silibinin: a Historical and Translational Perspective. Pharmaceuticals. 2021;14(6):559. doi:10.3390/ph14060559
17. Federico A, Dallio M, Loguercio C. Silymarin/Silybin and Chronic Liver Disease: a Marriage of Many Years. Molecules. 2017;22(2):191. doi:10.3390/molecules22020191
18. Abenavoli L, Izzo AA, Milić N, Cicala C, Santini A, Capasso R. Milk thistle (Silybum marianum): a concise overview on its chemistry, pharmacological, and nutraceutical uses in liver diseases. Phytother Res. 2018;32(11):2202–2213. doi:10.1002/ptr.6171
19. Möschlin G, Biedermann D, Vavříková E, et al. Chemistry of silybin. Nat Prod Rep. 2014;31(9):1138–1157. doi:10.1039/C3NP70122K
20. Pelter A, Hänsel R. The structure of silybin (Silybum substance E6), the first flavonolignan. Tetrahedron Lett. 1968;9(25):2911–2916. doi:10.1016/S0040-4039(00)89610-0
21. Pelter A, Hänsel R. Struktur des Silybins: i. Abbauversuche. Chem Ber. 1975;108(3):790–802. doi:10.1002/cber.19751080312
22. Fenclova M, Novakova A, Viktorova J, et al. Poor chemical and microbiological quality of the commercial milk thistle-based dietary supplements may account for their reported unsatisfactory and non-reproducible clinical outcomes. Sci Rep. 2019;9(1):11118. doi:10.1038/s41598-019-47250-0
23. Dunnick JK, Singh B, Nyska A, Peckham J, Kissling GE, Sanders JM. Investigating the Potential for Toxicity from Long-Term Use of the Herbal Products, Goldenseal and Milk Thistle. Toxicol Pathol. 2011;39(2):398–409. doi:10.1177/0192623310394211
24. Kim S, Chen J, Cheng T, et al. PubChem 2023 update. Nucleic Acids Res. 2023: 51(D1):D1373–D1380. doi:10.1093/nar/gkac956
25. Biedermann D, Vavrikova E, Cvak L, Kren V. Chemistry of silybin. Nat Prod Rep. 2014;31(9):1138–1157. doi:10.1039/C3NP70122K
26. Svitkova B, Selc M, Nemethova V, et al. Plate reader spectroscopy as an alternative to atomic absorption spectroscopy for the assessment of nanoparticle cellular uptake. Heliyon. 2022;8(11):e11595. doi:10.1016/j.heliyon.2022.e11595
27. Zhang JQ, Liu J, Li XL, Jasti BR. Preparation and Characterization of Solid Lipid Nanoparticles Containing Silibinin. Drug Deliv. 2007;14(6):381–387. doi:10.1080/10717540701203034
28. Nawaz Q, Fuentes-Chandía M, Tharmalingam V, Ur Rehman MA, Leal-Egaña A, Boccaccini AR. Silibinin releasing mesoporous bioactive glass nanoparticles with potential for breast cancer therapy. Ceram Int. 2020;46(18):29111–29119. doi:10.1016/j.ceramint.2020.08.083
29. Amirsaadat S, Pilehvar-Soltanahmadi Y, Zarghami F, Alipour S, Ebrahimnezhad Z, Zarghami N. Silibinin-loaded magnetic nanoparticles inhibit hTERT gene expression and proliferation of lung cancer cells. Artif Cells Nanomed Biotechnol. 2017;45(8):1649–1656. doi:10.1080/21691401.2016.1276922
30. Ravi R, Zeyaullah M, Ghosh S, et al. Use of gold nanoparticle-silibinin conjugates: a novel approach against lung cancer cells. Front Chem. 2022;10:1018759. doi:10.3389/fchem.2022.1018759
31. Abdullah AS, El Sayed IET, El-Torgoman AMA, et al. Preparation and Characterization of Silymarin-Conjugated Gold Nanoparticles with Enhanced Anti-Fibrotic Therapeutic Effects against Hepatic Fibrosis in Rats: role of MicroRNAs as Molecular Targets. Biomedicines. 2021;9(12):1767. doi:10.3390/biomedicines9121767
32. Zhang YN, Poon W, Tavares AJ, McGilvray ID, Chan WCW. Nanoparticle–liver interactions: cellular uptake and hepatobiliary elimination. J Control Release. 2016;240:332–348. doi:10.1016/j.jconrel.2016.01.020
33. Kumar M, Kulkarni P, Liu S, Chemuturi N, Shah DK. Nanoparticle biodistribution coefficients: a quantitative approach for understanding the tissue distribution of nanoparticles. Adv Drug Deliv Rev. 2023;194:114708. doi:10.1016/j.addr.2023.114708
34. Gheybi F, Khooei A, Hoseinian A, et al. Alleviation of Acetaminophen-induced liver failure using silibinin nanoliposomes: an in vivo study. Biochem Biophys Res Commun. 2023;676:103–108. doi:10.1016/j.bbrc.2023.07.045
35. Jiang HH, Yan FS, Shen L, Ji HF. Silymarin versus Silibinin: differential Antioxidant and Neuroprotective Effects against H 2 O 2 -induced Oxidative Stress in PC12 Cells. Nat Prod Commun. 2016;11(5):1934578X1601100. doi:10.1177/1934578X1601100520
36. Bijak M. Silybin, a Major Bioactive Component of Milk Thistle (Silybum marianum L. Gaernt.)—Chemistry, Bioavailability, and Metabolism. Molecules. 2017;22(11):1942. doi:10.3390/molecules22111942
37. Polyak SJ, Morishima C, Lohmann V, et al. Identification of hepatoprotective flavonolignans from silymarin. Proc Natl Acad Sci U S A. 2010;107(13):5995–5999. doi:10.1073/pnas.0914009107
38. Kostek H, Szponar J, Tchórz M, Majewska M, Lewandowska-Stanek H. Silibinin and its hepatoprotective action from the perspective of a toxicologist. Przegl Lek. 2012;69(8):541–543.
39. Muthumani M, Prabu SM. Silibinin potentially protects arsenic-induced oxidative hepatic dysfunction in rats. Toxicol Mech Methods. 2012;22(4):277–288. doi:10.3109/15376516.2011.647113
40. Haddad Y, Vallerand D, Brault A, Haddad PS. Antioxidant and Hepatoprotective Effects of Silibinin in a Rat Model of Nonalcoholic Steatohepatitis. Evid Based Complement Alternat Med. 2011;2011:1–10. doi:10.1093/ecam/nep164
41. Loguercio C, Festi D. Silybin and the liver: from basic research to clinical practice. World J Gastroenterol. 2011;17(18):2288. doi:10.3748/wjg.v17.i18.2288
42. Kang DY, Sp N, Do Park K, Lee HK, Song KD, Yang YM. Silibinin inhibits in vitro ketosis by regulating HMGCS2 and NF-kB: elucidation of signaling molecule relationship under ketotic conditions. Vitro Cell Dev Biol Anim. 2019;55(5):368–375. doi:10.1007/s11626-019-00351-6
43. Liu Y, Yu Q, Chen Y. Effect of silibinin on CFLAR-JNK pathway in oleic acid-treated HepG2 cells. Biomed Pharmacother. 2018;108:716–723. doi:10.1016/j.biopha.2018.09.089
44. Salamone F, Galvano F, Cappello F, Mangiameli A, Barbagallo I, Li Volti G. Silibinin modulates lipid homeostasis and inhibits nuclear factor kappa B activation in experimental nonalcoholic steatohepatitis. Transl Res. 2012;159(6):477–486. doi:10.1016/j.trsl.2011.12.003
45. Trappoliere M, Caligiuri A, Schmid M, et al. Silybin, a component of sylimarin, exerts anti-inflammatory and anti-fibrogenic effects on human hepatic stellate cells. J Hepatol. 2009;50(6):1102–1111. doi:10.1016/j.jhep.2009.02.023
46. Hosseini SY, Kalantar K, Shahin K, et al. Comparison of the in vitro antifibrogenic effects of Silymarin, Silybin A and 18α-Glycyrrhizin on activated hepatic stellate cells. Jundishapur J Nat Pharm Prod. 2017;12(4). doi:10.5812/jjnpp.40285
47. Ezhilarasan D, Evraerts J, Sid B, et al. Silibinin induces hepatic stellate cell cycle arrest via enhancing p53/p27 and inhibiting Akt downstream signaling protein expression. Hepatobiliary Pancreat Dis Int. 2017;16(1):80–87. doi:10.1016/S1499-3872(16)60166-2
48. Masini A, Ceccarelli D, Giovannini F, Montosi G, Garuti C, Pietrangelo A. Iron-induced oxidant stress leads to irreversible mitochondrial dysfunctions and fibrosis in the liver of chronic iron-dosed gerbils. The effect of silybin. J Bioenerg Biomembr. 2000;32(2):175–182. doi:10.1023/A:1005512014280
49. Xie Y, Hao HP, Wang H, Wang ZX, Wang GJ. Reversing effects of silybin on TAA-induced hepatic CYP3A dysfunction through PXR regulation. Chin J Nat Med. 2013;11(6):645–652. doi:10.1016/S1875-5364(13)60075-8
50. Muriel P, Moreno MG, Hernández MDC, Chávez HE, Alcantar LK. Resolution of liver fibrosis in chronic CCl4 administration in the rat after discontinuation of treatment: effect of silymarin, silibinin, colchicine and trimethylcolchicinic acid. Basic Clin Pharmacol Toxicol. 2005;96(5):375–380. doi:10.1111/j.1742-7843.2005.pto_06.x
51. Blaising J, Lévy PL, Gondeau C, et al. Silibinin inhibits hepatitis C virus entry into hepatocytes by hindering clathrin-dependent trafficking. Cell Microbiol. 2013;15(11):1866–1882. doi:10.1111/cmi.12155
52. Yassin NYS, AbouZid SF, El-Kalaawy AM, Ali TM, Almehmadi MM, Ahmed OM. Silybum marianum total extract, silymarin and silibinin abate hepatocarcinogenesis and hepatocellular carcinoma growth via modulation of the HGF/c-Met, Wnt/β-catenin, and PI3K/Akt/mTOR signaling pathways. Biomed Pharmacother. 2022;145:112409. doi:10.1016/j.biopha.2021.112409
53. Miguez MP, Anundi I, Sainz-Pardo LA, Lindros KO. Comparative study of the hepatoprotective effect of silymarin and silybin on isolated rat hepatocytes. Toxicol In Vitro. 1994;8(4):581–583. doi:10.1016/0887-2333(94)90021-3
54. Liu K, Zhou S, Liu J, Wang Y, Zhu F, Liu M. Silibinin attenuates high-fat diet-induced renal fibrosis of diabetic nephropathy. Drug Des Devel Ther. 2019;13:3117–3126. doi:10.2147/DDDT.S209981
55. Ma Z, Zang W, Wang H, Wei X. Silibinin enhances anti-renal fibrosis effect of MK-521 via downregulation of TGF-β signaling pathway. Hum Cell. 2019;33(2):330–336. doi:10.1007/s13577-019-00314-9
56. Mateen S, Raina K, Agarwal R. Chemopreventive and Anti-Cancer Efficacy of Silibinin Against Growth and Progression of Lung Cancer. Nutr Cancer. 2013; 65(sup1):3–11. doi:10.1080/01635581.2013.785004
57. Verdura S, Cuyàs E, Llorach-Parés L, et al. Silibinin is a direct inhibitor of STAT3. Food Chem Toxicol. 2018;116:161–172. doi:10.1016/j.fct.2018.04.028
58. Tehrani FK, Ranji N, Kouhkan F, Hosseinzadeh S. Apoptosis induction and proliferation inhibition by silibinin encapsulated in nanoparticles in MIA PaCa-2 cancer cells and deregulation of some miRNAs. Iran J Basic Med Sci. 2020;23(4):469–482. doi:10.22038/IJBMS.2020.39427.9349
59. Zhu W, Zhang JS, Young CYF. Silymarin inhibits function of the androgen receptor by reducing nuclear localization of the receptor in the human prostate cancer cell line LNCaP. Carcinogenesis. 2001;22(9):1399–1403. doi:10.1093/carcin/22.9.1399
60. Addeo RS. A New Opportunity for the Treatment of Brain Metastasis from Lung Cancer. J Exp Pharmacol. 2021;13:901–903. doi:10.2147/JEP.S326871
61. Gandey S, Aparna V, Kandarapu R. Preparation and Biological Evaluation of Silybin Liposomes for the Treatment of Liver Disorders. J Pharm Res Int. 2021;33(39A):186–200. doi:10.9734/jpri/2021/v33i39A32159
62. Yu JN, Zhu Y, Wang L, et al. Enhancement of oral bioavailability of the poorly water-soluble drug silybin by sodium cholate/phospholipid-mixed micelles. Acta Pharmacol Sin. 2010;31(6):759–764. doi:10.1038/aps.2010.55
63. Zhao J, Agarwal R. Tissue distribution of silibinin, the major active constituent of silymarin, in mice and its association with enhancement of Phase II enzymes: implications in cancer chemoprevention. Carcinogenesis. 1999;20(11):2101–2108. doi:10.1093/carcin/20.11.2101
64. Xu P, Zhou H, Li YZ, et al. Baicalein Enhances the Oral Bioavailability and Hepatoprotective Effects of Silybin Through the Inhibition of Efflux Transporters BCRP and MRP2. Front Pharmacol. 2018;9:1115. doi:10.3389/fphar.2018.01115
65. Wu JW, Lin LC, Hung SC, Chi CW, Tsai TH. Analysis of silibinin in rat plasma and bile for hepatobiliary excretion and oral bioavailability application. J Pharm Biomed Anal. 2007;45(4):635–641. doi:10.1016/j.jpba.2007.06.026
66. Barzaghi N, Crema F, Gatti G, Pifferi G, Perucca E. Pharmacokinetic studies on IdB 1016, a silybin-phosphatidylcholine complex, in healthy human subjects. Eur J Drug Metab Pharmacokinet. 1990;15(4):333–338. doi:10.1007/BF03190223
67. Comoglio A, Leonarduzzi G, Carini R, et al. Studies on the Antioxidant and Free Radical Scavenging Properties of Idb 1016 A New Flavanolignan Complex. Free Radic Res Commun. 1990;11(1–3):109–115. doi:10.3109/10715769009109673
68. Morazzoni P, Magistretti MJ, Giachetti C, Zanolo G. Comparative bioavailability of Silipide, a new flavanolignan complex, in rats. Eur J Drug Metab Pharmacokinet. 1992;17(1):39–44. doi:10.1007/BF03189986
69. Morazzoni P, Montalbetti A, Malandrino S, Pifferi G. Comparative pharmacokinetics of silipide and silymarin in rats. Eur J Drug Metab Pharmacokinet. 1993;18(3):289–297. doi:10.1007/BF03188811
70. Marhol P, Bednář P, Kolářová P, et al. Pharmacokinetics of pure silybin diastereoisomers and identification of their metabolites in rat plasma. J Funct Foods. 2015;14:570–580. doi:10.1016/j.jff.2015.02.031
71. Buzzelli G, Moscarella S, Giusti A, Duchini A, Marena C, Lampertico M. A pilot study on the liver protective effect of silybin-phosphatidylcholine complex (IdB1016) in chronic active hepatitis. Int J Clin Pharmacol Ther Toxicol. 1993;31(9):456–460.
72. Kidd P, Head K. A review of the bioavailability and clinical efficacy of milk thistle phytosome: a silybin-phosphatidylcholine complex (Siliphos). Altern Med Rev. 2005;10(3):193–203.
73. Loguercio C, Andreone P, Brisc C, et al. Silybin combined with phosphatidylcholine and vitamin E in patients with nonalcoholic fatty liver disease: a randomized controlled trial. Free Radic Biol Med. 2012;52(9):1658–1665. doi:10.1016/j.freeradbiomed.2012.02.008
74. Stiuso P, Scognamiglio I, Murolo M, et al. Serum Oxidative Stress Markers and Lipidomic Profile to Detect NASH Patients Responsive to an Antioxidant Treatment: a Pilot Study. Oxid Med Cell Longev. 2014;2014:1–8. doi:10.1155/2014/169216
75. Di Sario A, Bendia E, Taffetani S, et al. Hepatoprotective and antifibrotic effect of a new silybin–phosphatidylcholine–Vitamin E complex in rats. Dig Liver Dis. 2005;37(11):869–876. doi:10.1016/j.dld.2005.05.011
76. Mengs U, Pohl RT, Mitchell T. Legalon® SIL: the Antidote of Choice in Patients with Acute Hepatotoxicity from Amatoxin Poisoning. Curr Pharm Biotechnol. 2012;13(10):1964–1970. doi:10.2174/138920112802273353
77. Mehrab-Mohseni M, Sendi H, Steuerwald N, Ghosh S, Schrum LW, Bonkovsky HL. Legalon-SIL downregulates HCV core and NS5A in human hepatocytes expressing full-length HCV. World J Gastroenterol. 2011;17(13):1694. doi:10.3748/wjg.v17.i13.1694
78. DebRoy S, Hiraga N, Imamura M, et al. Hepatitis C virus dynamics and cellular gene expression in uPA‐SCID chimeric mice with humanized livers during intravenous silibinin monotherapy. J Viral Hepat. 2016;23(9):708–717. doi:10.1111/jvh.12551
79. Cufí S, Bonavia R, Vazquez-Martin A, et al. Silibinin meglumine, a water-soluble form of milk thistle silymarin, is an orally active anti-cancer agent that impedes the epithelial-to-mesenchymal transition (EMT) in EGFR-mutant non-small-cell lung carcinoma cells. Food Chem Toxicol. 2013;60:360–368. doi:10.1016/j.fct.2013.07.063
80. Romanucci V, Gravante R, Cimafonte M, et al. Phosphate-Linked Silibinin Dimers (PLSd): new Promising Modified Metabolites. Molecules. 2017;22(8):1323. doi:10.3390/molecules22081323
81. Xi JJ, Cao Y, He RY, et al. Design, Synthesis and Biological Evaluation of Glycosylated Derivatives of Silibinin as Potential Anti-Tumor Agents. Drug Des Devel Ther. 2023;17:2063–2076. doi:10.2147/DDDT.S404036
82. Mai M, Wang Y, Luo M, et al. Silibinin ameliorates deoxycholic acid-induced pyroptosis in steatotic HepG2 cells by inhibiting NLRP3 inflammasome activation. Biochem Biophys Rep. 2023;35:101545. doi:10.1016/j.bbrep.2023.101545
83. Angeli JPF, Barcelos GRM, Serpeloni JM, Barbosa JF, Nersesyan A, Mantovani MS. Evaluation of the genotoxic and anti-genotoxic activities of Silybin in human hepatoma cells (HepG2). Mutagenesis. 2010;25(3):223–229. doi:10.1093/mutage/gep064
84. Duan W, Ou Z, Huang Y, et al. Silibinin Inhibits Cell Ferroptosis and Ferroptosis-Related Tissue Injuries. Antioxidants. 2023;12(12):2119. doi:10.3390/antiox12122119
85. Yan B, Zheng X, Wang Y, et al. Liposome-Based Silibinin for Mitigating Nonalcoholic Fatty Liver Disease: dual Effects via Parenteral and Intestinal Routes. ACS Pharmacol Transl Sci. 2023;6(12):1909–1923. doi:10.1021/acsptsci.3c00210
86. Şumnulu D. Contrary to known silibinin is not an anticancer agent and liver protective supplement. Genetika. 2023;55(2):553–564. doi:10.2298/GENSR2302553S
87. Vakili Zahir N, Nakhjavani M, Hajian P, Shirazi FH, Mirzaei H. Evaluation of Silibinin Effects on the Viability of HepG2 (Human hepatocellular liver carcinoma) and HUVEC (Human Umbilical Vein Endothelial) Cell Lines. Iran J Pharm Res. 2018;17(1):261–267.
88. Wu W, Zu Y, Wang L, et al. Preparation, characterization and antitumor activity evaluation of silibinin nanoparticles for oral delivery through liquid antisolvent precipitation. RSC Adv. 2017;7(86):54379–54390. doi:10.1039/C7RA10242A
89. Tan JM, Karthivashan G, Arulselvan P, Fakurazi S, Hussein MZ. Characterization and In Vitro Sustained Release of Silibinin from pH Responsive Carbon Nanotube-Based Drug Delivery System. J Nanomater. 2014;2014:1–10. doi:10.1155/2014/439873
90. Radko L, Cybulski W, Rzeski W. Cytoprotective effect of silybin against lasalocid-induced toxicity in HepG2 cells. Pol J Vet Sci. 2013;16(2):275–282. doi:10.2478/pjvs-2013-0038
91. Zhang S, Yang Y, Liang Z, et al. Silybin-Mediated Inhibition of Notch Signaling Exerts Antitumor Activity in Human Hepatocellular Carcinoma Cells. PLoS One. 2013;8(12):e83699. doi:10.1371/journal.pone.0083699
92. Momeny M, Khorramizadeh MR, Ghaffari SH, et al. Effects of silibinin on cell growth and invasive properties of a human hepatocellular carcinoma cell line, HepG-2, through inhibition of extracellular signal-regulated kinase 1/2 phosphorylation. Eur J Pharmacol. 2008;591(1–3):13–20. doi:10.1016/j.ejphar.2008.06.011
93. Song XY, Liu PC, Liu WW, et al. Protective effects of silibinin against ethanol- or acetaldehyde-caused damage in liver cell lines involve the repression of mitochondrial fission. Toxicol In Vitro. 2022;80:105330. doi:10.1016/j.tiv.2022.105330
94. Mao J, Yang H, Cui T, et al. Combined treatment with sorafenib and silibinin synergistically targets both HCC cells and cancer stem cells by enhanced inhibition of the phosphorylation of STAT3/ERK/AKT. Eur J Pharmacol. 2018;832:39–49. doi:10.1016/j.ejphar.2018.05.027
95. Gu HR, Park SC, Choi SJ, et al. Combined treatment with silibinin and either sorafenib or gefitinib enhances their growth-inhibiting effects in hepatocellular carcinoma cells. Clin Mol Hepatol. 2015;21(1):49. doi:10.3350/cmh.2015.21.1.49
96. Lah JJ, Cui W, Hu KQ. Effects and mechanisms of silibinin on human hepatoma cell lines. World J Gastroenterol. 2007;13(40):5299. doi:10.3748/wjg.v13.i40.5299
97. Varghese L, Agarwal C, Tyagi A, Singh RP, Agarwal R. Silibinin efficacy against human hepatocellular carcinoma. Clin Cancer Res. 2005;11(23):8441–8448. doi:10.1158/1078-0432.CCR-05-1646
98. Yang J, Sun Y, Xu F, et al. Autophagy and glycolysis independently attenuate silibinin-induced apoptosis in human hepatocarcinoma HepG2 and Hep3B cells. Hum Exp Toxicol. 2021;40(12):2048–2062. doi:10.1177/09603271211017609
99. García-Maceira P, Mateo J. Silibinin inhibits hypoxia-inducible factor-1α and mTOR/p70S6K/4E-BP1 signalling pathway in human cervical and hepatoma cancer cells: implications for anticancer therapy. Oncogene. 2009;28(3):313–324. doi:10.1038/onc.2008.398
100. Liu C-H, Lin -C-C, Hsu W-C, et al. Highly bioavailable silibinin nanoparticles inhibit HCV infection. Gut. 2017;66(10):1853–1861. doi:10.1136/gutjnl-2016-312019
101. Anfuso B, Giraudi P, Tiribelli C, Rosso N. Silybin Modulates Collagen Turnover in an In Vitro Model of NASH. Molecules. 2019;24(7):1280. doi:10.3390/molecules24071280
102. Rashidi M, Afarin R, Shakerian E, Asadizadeh S, Salehipour-Bavarsa S. The Effects of Silibinin on Gene Expression of NOX1, NOX2, and the Production of Reactive Oxygen Species in TGFb Treated Liver Stellate Cells. J Isfahan Med Sch. 2022;40(664):172–178. doi:10.48305/jims.v40.i664.0172
103. Van Pelt JF, Verslype C, Crabbe T, Zaman Z, Fevery J. Primary human hepatocytes are protected against prolonged and repeated exposure to ethanol by silibinin-dihemisuccinate. Alcohol Alcohol. 2003;38(5):411–414. doi:10.1093/alcalc/agg099
104. Bousserouel S, Bour G, Kauntz H, Gossé F, Marescaux J, Raul F. Silibinin inhibits tumor growth in a murine orthotopic hepatocarcinoma model and activates the TRAIL apoptotic signaling pathway. Anticancer Res. 2012;32(7):2455–2462.
105. Brandon-Warner E, Sugg JA, Schrum LW, McKillop IH. Silibinin inhibits ethanol metabolism and ethanol-dependent cell proliferation in an in vitro model of hepatocellular carcinoma. Cancer Lett. 2010;291(1):120–129. doi:10.1016/j.canlet.2009.10.004
106. Durymanov M, Permyakova A, Reineke J. Pre-treatment With PLGA/Silibinin Nanoparticles Mitigates Dacarbazine-Induced Hepatotoxicity. Front Bioeng Biotechnol. 2020;8:495. doi:10.3389/fbioe.2020.00495
107. Fuchs EC, Weyhenmeyer R, Weiner OH. Effects of silibinin and of a synthetic analogue on isolated rat hepatic stellate cells and myofibroblasts. Arzneimittelforschung. 1997;47(12):1383–1387.
108. Essid E, Dernawi Y, Petzinger E. Apoptosis Induction by OTA and TNF-α in Cultured Primary Rat Hepatocytes and Prevention by Silibinin. Toxins (Basel). 2012;4(11):1139–1156. doi:10.3390/toxins4111139
109. Song XY, Li RH, Liu WW, et al. Effect of silibinin on ethanol- or acetaldehyde-induced damage of mouse primary hepatocytes in vitro. Toxicol In Vitro. 2021;70:105047. doi:10.1016/j.tiv.2020.105047
110. Dehmlow C, Erhard J, De Groot H. Inhibition of Kupffer cell functions as an explanation for the hepatoprotective properties of silibinin. Hepatology. 1996;23(4):749–754. doi:10.1053/jhep.1996.v23.pm0008666328
111. Tang S, Zhang X, Duan Z, et al. The novel hepatoprotective mechanisms of silibinin-phospholipid complex against D-GalN/LPS-induced acute liver injury. Int Immunopharmacol. 2023;116:109808. doi:10.1016/j.intimp.2023.109808
112. Vanzan DF, Goma EP, Locatelli FR, et al. Evaluation of Silybin Nanoparticles against Liver Damage in Murine Schistosomiasis mansoni Infection. Pharmaceutics. 2024;16(5):618. doi:10.3390/pharmaceutics16050618
113. Chen LJ, Lin G XX. Lrp6 genotype affects individual susceptibility to nonalcoholic fatty liver disease and silibinin therapeutic response via wnt/β-catenin-cyp2e1 signaling. Int J Biol Sci. 2021;17(14):3936–3953. doi:10.7150/ijbs.63732
114. Liu Y, Xu W, Zhai T, You J, Chen Y. Silibinin ameliorates hepatic lipid accumulation and oxidative stress in mice with non-alcoholic steatohepatitis by regulating CFLAR-JNK pathway. Acta Pharm Sin B. 2019;9(4):745–757. doi:10.1016/j.apsb.2019.02.006
115. Liu Y, Wang Z, Kong F, et al. Triterpenoids Extracted From Antrodia cinnamomea Mycelia Attenuate Acute Alcohol-Induced Liver Injury in C57BL/6 Mice via Suppression Inflammatory Response. Front Microbiol. 2020;11:1–13. doi:10.3389/fmicb.2020.01113
116. Wang W, Zhai T, Luo P, Miao X, Wang J, Chen Y. Beneficial effects of silibinin on serum lipids, bile acids, and gut microbiota in methionine-choline-deficient diet-induced mice. Front Nutr. 2023;10:1257158. doi:10.3389/fnut.2023.1257158
117. Zhao ZW, Chang JC, Lin LW, Tsai FH, Chang HC, Wu CR. Comparison of the hepatoprotective effects of four endemic Cirsium species extracts from Taiwan on CCl4-induced acute liver damage in C57BL/6 mice. Int J Mol Sci. 2018;19(5):1329. doi:10.3390/ijms19051329
118. Zhu T, Huang X, Zhu H, et al. Analysis of bioactive components and synergistic action mechanism of ShuGan-QieZhi Capsule for treating non-alcoholic fatty liver disease. Phytomedicine. 2024;123:155173. doi:10.1016/j.phymed.2023.155173
119. Hu WY, Ma XH, Zhou WY, Li STT XX, Sun H. Preventive effect of Silibinin in combination with Pu-erh tea extract on non-alcoholic fatty liver disease in ob/ob mice. Food Funct. 2017;8(3):1105–1115. doi:10.1039/c6fo01591c
120. Xu R, Qiu S, Zhang J, et al. Silibinin Schiff Base Derivatives Counteract CCl4-Induced Acute Liver Injury by Enhancing Anti-Inflammatory and Antiapoptotic Bioactivities. Drug Des Devel Ther. 2022;16:1441–1456. doi:10.2147/DDDT.S356847
121. Lee HU, Bae EA, Kim DH. Hepatoprotective Effects of Irisolidone on tert-Butyl Hyperoxide-Induced Liver Injury. Biol Pharm Bull. 2005;28(3):531–533. doi:10.1248/bpb.28.531
122. Chen C, Liu X, Qi S, Dias CP, Yan A, Zhang J. Hepatoprotective effect of Phellinus linteus mycelia polysaccharide (PL-N1) against Acetaminophen-induced liver injury in mouse. Int J Biol Macromol. 2020;154:1276–1284. doi:10.1016/j.ijbiomac.2019.11.002
123. Salimi-Sabour E, Tahri RA, Asgari A, Ghorbani M. The novel hepatoprotective effects of silibinin-loaded nanostructured lipid carriers against diazinon-induced liver injuries in male mice. Pestic Biochem Physiol. 2023;197:105643. doi:10.1016/j.pestbp.2023.105643
124. Huo X, Meng X, Zhang J, Zhao Y. Hepatoprotective effect of different combinations of 18α-and 18β-Glycyrrhizic acid against CCl4-induced liver injury in rats. Biomed Pharmacother. 2020;122:1–9. doi:10.1016/j.biopha.2019.109354
125. Khawaja G, El-Orfali Y. Silibinin’s Effects against Methotrexate-Induced Hepatotoxicity in Adjuvant-Induced Arthritis Rat Model. Pharmaceuticals. 2024;17(4):431. doi:10.3390/ph17040431
126. Yao J, Zhi M, Gao X, Hu P, Li C, Yang X. Effect and the probable mechanisms of silibinin in regulating insulin resistance in the liver of rats with non-alcoholic fatty liver. Braz J Med Biol Res. 2013;46(3):270–277. doi:10.1590/1414-431X20122551
127. Sahibzada MUK, Sadiq A, Zahoor M, Naz S, Shahid M, Qureshi NA. Enhancement of bioavailability and hepatoprotection by silibinin through conversion to nanoparticles prepared by liquid antisolvent method. Arab Journal Chem. 2020;13(2):3682–3689. doi:10.1016/j.arabjc.2020.01.002
128. Yao J, Zhi M, Minhu C. Effect of silybin on high-fat-induced fatty liver in rats. Braz J Med Biol Res. 2011;44(7):652–659. doi:10.1590/S0100-879X2011007500083
129. Conti M, Malandrino S, Magistretti MJ. Protective Activity of Silipide on Liver Damage in Rodents. Jpn J Pharmacol. 1992;60(4):315–321. doi:10.1254/jjp.60.315
130. Fang C, Zhang J, Han J, et al. Tiaogan Jiejiu Tongluo Formula attenuated alcohol-induced chronic liver injury by regulating lipid metabolism in rats. J Ethnopharmacol. 2023;317:116838. doi:10.1016/j.jep.2023.116838
131. Ain QU, Saleem U, Ahmad B, Khalid I. Pharmacological screening of silibinin for antischizophrenic activity along with its acute toxicity evaluation in experimental animals. Front Pharmacol. 2023;14. doi:10.3389/fphar.2023.1111915
132. Beydilli H, Yilmaz N, Cetin ES, et al. Evaluation of the protective effect of silibinin against diazinon induced hepatotoxicity and free-radical damage in rat liver. Iran Red Crescent Med J. 2015;17(4). doi:10.5812/ircmj.17(4)2015.25310
133. Ezhilarasan D, Karthikeyan S, Vivekanandan P. Ameliorative effect of silibinin against N-nitrosodimethylamine-induced hepatic fibrosis in rats. Environ Toxicol Pharmacol. 2012;34(3):1004–1013. doi:10.1016/j.etap.2012.07.004
134. Raghu R, Jesudas B, Bhavani G, Ezhilarasan D, Karthikeyan S. Silibinin mitigates zidovudine-induced hepatocellular degenerative changes, oxidative stress and hyperlipidaemia in rats. Hum Exp Toxicol. 2015;34(11):1031–1042. doi:10.1177/0960327114567765
135. Raghu R, Karthikeyan S. Zidovudine and isoniazid induced liver toxicity and oxidative stress: evaluation of mitigating properties of silibinin. Environ Toxicol Pharmacol. 2016;46:217–226. doi:10.1016/j.etap.2016.07.014
136. Ramanathan R, Sivanesan K. Evaluation of ameliorative ability of Silibinin against zidovudine and isoniazid-induced hepatotoxicity and hyperlipidaemia in rats: role of Silibinin in Phase I and II drug metabolism. Chem Biol Interact. 2017;273:142–153. doi:10.1016/j.cbi.2017.06.008
137. Sozen H, Celik OI, Cetin ES, et al. Evaluation of the Protective Effect of Silibinin in Rats with Liver Damage Caused by Itraconazole. Cell Biochem Biophys. 2015;71(2):1215–1223. doi:10.1007/s12013-014-0331-8
138. Serviddio G, Bellanti F, Giudetti AM, et al. A Silybin-Phospholipid Complex Prevents Mitochondrial Dysfunction in a Rodent Model of Nonalcoholic Steatohepatitis. J Pharmacol Exp Ther. 2010;332(3):922–932. doi:10.1124/jpet.109.161612
139. Dagli Gul AS, Boyuk Ozcan G, Arihan O. Silibinin as a promising treatment for diabetes: insights into behavioral and metabolic changes in an animal model. Food Sci Nutr. 2024;12(5):3336–3345. doi:10.1002/fsn3.3999
140. Bouderba S, Sanchez-Martin C, Villanueva GR, Detaille D, Koceïr EA. Beneficial effects of silibinin against the progression of metabolic syndrome, increased oxidative stress, and liver steatosis in Psammomys obesus, a relevant animal model of human obesity and diabetes. J Diabetes. 2014;6(2):184–192. doi:10.1111/1753-0407.12083
141. Cui CX, Deng JN, Yan L, et al. Silibinin Capsules improves high fat diet-induced nonalcoholic fatty liver disease in hamsters through modifying hepatic de novo lipogenesis and fatty acid oxidation. J Ethnopharmacol. 2017;208:24–35. doi:10.1016/j.jep.2017.06.030
142. Wang Y, Wang L, Liu Z, Zhang D, Zhang Q. In Vivo Evaluation of Silybin Nanosuspensions Targeting Liver. J Biomed Nanotechnol. 2012;8(5):760–769. doi:10.1166/jbn.2012.1444
143. Saxena N, Dhaked RK, Nagar DP. Silibinin ameliorates abrin induced hepatotoxicity by attenuating oxidative stress, inflammation and inhibiting Fas pathway. Environ Toxicol Pharmacol. 2022;93:103868. doi:10.1016/j.etap.2022.103868
144. Schümann J, Prockl J, Kiemer AK, Vollmar AM, Bang R, Tiegs G. Silibinin protects mice from T cell-dependent liver injury. J Hepatol. 2003;39(3):333–340. doi:10.1016/S0168-8278(03)00239-3
145. Jiang T, Xu J, Lu Y, Chen X, Li Y. Network Pharmacology Analysis and Experimental Validation to Explore the Anti-inflammatory Mechanism of Asiatic Acid on Alcoholic Steatohepatitis. Mediators Inflamm. 2022;1708030. doi:10.1155/2022/1708030
146. Lee SJ, Nam MJ, Lee DE, et al. Silibinin ameliorates O-GlcNAcylation and inflammation in a mouse model of nonalcoholic steatohepatitis. Int J Mol Sci. 2018;19(8). doi:10.3390/ijms19082165
147. Huber A, Thongphasuk P, Erben G, et al. Significantly greater antioxidant anticancer activities of 2,3-dehydrosilybin than silybin. Biochim Biophys Acta. 2008;1780(5):837–847. doi:10.1016/j.bbagen.2007.12.012
148. Tong TC, Hernandez M, Richardson WH, et al. Comparative Treatment of α-Amanitin Poisoning With N-Acetylcysteine, Benzylpenicillin, Cimetidine, Thioctic Acid, and Silybin in a Murine Model. Ann Emerg Med. 2007;50(3):282–288. doi:10.1016/j.annemergmed.2006.12.015
149. Wu X, Zeng J, Hu J, et al. Hepatoprotective effects of aqueous extract from lingzhi or reishi medicinal mushroom Ganoderma lucidum (Higher Basidiomycetes) on α-amanitin-induced liver injury in mice. Int J Med Mushrooms. 2013;15(4):383–391. doi:10.1615/IntJMedMushr.v15.i4.60
150. Liu G, Liu X, Zhang Y, et al. Hepatoprotective effects of polysaccharides extracted from Zizyphus jujube cv. Huanghetanzao. Int J Biol Macromol. 2015;76:169–175. doi:10.1016/j.ijbiomac.2015.01.061
151. Wu H, Tang S, Huang Z, Zhou Q, Zhang P, Chen Z. Hepatoprotective effects and mechanisms of action of triterpenoids from lingzhi or reishi medicinal mushroom Ganoderma lucidum (Agaricomycetes) on α-amanitin-induced liver injury in mice. Int J Med Mushrooms. 2016;18(9):841–850. doi:10.1615/IntJMedMushrooms.v18.i9.80
152. Jayaraj R, Deb U, Bhaskar ASB, GBKS P, Rao PVL. Hepatoprotective efficacy of certain flavonoids against microcystin induced toxicity in mice. Environ Toxicol: Int J. 2007;22(5):472–479. doi:10.1002/tox.20283
153. Salamone F, Galvano F, Marino A, et al. Silibinin improves hepatic and myocardial injury in mice with nonalcoholic steatohepatitis. Dig Liver Dis. 2012;44(4):334–342. doi:10.1016/j.dld.2011.11.010
154. Akbari-Kordkheyli V, Azizi S, Khonakdar-Tarsi A. Effects of silibinin on hepatic warm ischemia-reperfusion injury in the rat model. Iran J Basic Med Sci. 2019;22(7):789–796. doi:10.22038/ijbms.2019.34967.8313
155. Hashem RM, Hassanin KMA, Rashed LA, Mahmoud MO, Hassan MG. Effect of silibinin and vitamin E on the ASK1-p38 MAPK pathway in D-galactosamine/lipopolysaccharide induced hepatotoxicity. Exp Biol Med. 2016;241(11):1250–1257. doi:10.1177/1535370216636719
156. Qajari NM, Shafaroudi MM, Gholami M, Khonakdar-Tarsi A. Silibinin treatment results in reducing OPA1&MFN1 genes expression in a rat model hepatic ischemia–reperfusion. Mol Biol Rep. 2020;47(5):3271–3280. doi:10.1007/s11033-020-05383-w
157. Yanaşoğlu E, Büyükavcı M, Çetinkaya A, et al. Silibinin Effect on Methotrexate-Induced Hepatotoxicity in Rats. Eurasian J Med. 2022;54(3):264–269. doi:10.5152/eurasianjmed.2022.20371
158. Benko T, Frede S, Gu Y, et al. Glycine pretreatment ameliorates liver injury after partial hepatectomy in the rat. J Invest Surg. 2010;23(1):12–20. doi:10.3109/08941930903469466
159. Horváth MÉ, González-Cabello R, Blázovics A, et al. Effect of silibinin and vitamin E on restoration of cellular immune response after partial hepatectomy. J Ethnopharmacol. 2001;77(2–3):227–232. doi:10.1016/S0378-8741(01)00298-7
160. Zarpou S, Mosavi H, Bagheri A, Shafaroudi MM, Khonakdar-Tarsi A. NF-κB and NLRP3 gene expression changes during warm hepatic ischemia-reperfusion in rats with and without silibinin. Gastroenterol Hepatol Bed Bench. 2021;14(3):267–275. doi:10.22037/ghfbb.v14i3.2171
161. Das S, Roy P, Pal R, Auddy RG, Chakraborti AS, Mukherjee A. Engineered Silybin Nanoparticles Educe Efficient Control in Experimental Diabetes. PLoS One. 2014;9(7):e101818. doi:10.1371/journal.pone.0101818
162. Türel I, Özbek H, Erten R, Öner AC, Cengiz N, Yilmaz O. Hepatoprotective and anti-inflammatory activities of Plantago major L. Indian J Pharmacol. 2009;41(3):120–124. doi:10.4103/0253-7613.55211
163. Yıldız O, Can Z, Saral Ö, et al. Hepatoprotective Potential of Chestnut Bee Pollen on Carbon Tetrachloride-Induced Hepatic Damages in Rats. Evid Based Complement Alternat Med. 2013;2013:1–9. doi:10.1155/2013/461478
164. Ding Y, Zhang S, Sun Z, et al. Preclinical validation of silibinin/albumin nanoparticles as an applicable system against acute liver injury. Acta Biomater. 2022;146:385–395. doi:10.1016/j.actbio.2022.04.021
165. Luo S, Yang Y, Zhao T, et al. Albumin-Based Silibinin Nanocrystals Targeting Activated Hepatic Stellate Cells for Liver Fibrosis Therapy. ACS Appl Mater Interfaces. 2023;15(6):7747–7758. doi:10.1021/acsami.2c19269
166. Qiao JB, Fan QQ, Xing L, et al. Vitamin A-decorated biocompatible micelles for chemogene therapy of liver fibrosis. J Control Release. 2018;283:113–125. doi:10.1016/j.jconrel.2018.05.032
167. Zhang X, Zhang Q, Peng Q, et al. Hepatitis B virus preS1-derived lipopeptide functionalized liposomes for targeting of hepatic cells. Biomaterials. 2014;35(23):6130–6141. doi:10.1016/j.biomaterials.2014.04.037
168. Luo J, Zhang Z, Zeng Y, Dong Y, Ma L. Co-encapsulation of collagenase type I and silibinin in chondroitin sulfate coated multilayered nanoparticles for targeted treatment of liver fibrosis. Carbohydr Polym. 2021;263:117964. doi:10.1016/j.carbpol.2021.117964
169. Lu C, Li X, Liang X, et al. Liver Targeting Albumin-Coated Silybin-Phospholipid Particles Prepared by NabTM Technology for Improving Treatment Effect of Acute Liver Damage in Intravenous Administration. AAPS Pharm Sci Tech. 2019;20(7):293. doi:10.1208/s12249-019-1504-y
170. Yang Q, Tan T, He Q, et al. Combined Amphiphilic Silybin Meglumine Nanosuspension Effective Against Hepatic Fibrosis in Mice Model. Int J Nanomed. 2023;18:5197–5211. doi:10.2147/IJN.S407762
171. Tuchweber B, Sieck R, Trost W. Prevention by silybin of phalloidin-induced acute hepatoxicity. Toxicol Appl Pharmacol. 1979;51(2):265–275. doi:10.1016/0041-008X(79)90469-1
172. Li W, Zhou C, Fu Y, et al. Targeted delivery of hyaluronic acid nanomicelles to hepatic stellate cells in hepatic fibrosis rats. Acta Pharm Sin B. 2020;10(4):693–710. doi:10.1016/j.apsb.2019.07.003
173. Hruby K, Csomos G, Fuhrmann M, Thaler H. Chemotherapy of Amanita phalloides Poisoning with Intravenous Silibinin. Hum Toxicol. 1983;2(2):183–195. doi:10.1177/096032718300200203
174. Zhang B, Jiang G, Wang L, et al. An analysis of silybin meglumine tablets in the treatment of drug‐induced liver injury as assessed for causality with the updated Roussel Uclaf Causality Assessment Method using a nationwide database. Br J Clin Pharmacol. 2023;89(4):1329–1337. doi:10.1111/bcp.15575
175. Braun DL, Rauch A, Aouri M, et al. A Lead-In with Silibinin Prior to Triple-Therapy Translates into Favorable Treatment Outcomes in Difficult-To-Treat HIV/Hepatitis C Coinfected Patients. PLoS One. 2015;10(7):e0133028. doi:10.1371/journal.pone.0133028
176. Ferenci P, Scherzer T, Kerschner H, et al. Silibinin Is a Potent Antiviral Agent in Patients With Chronic Hepatitis C Not Responding to Pegylated Interferon/Ribavirin Therapy. Gastroenterology. 2008;135(5):1561–1567. doi:10.1053/j.gastro.2008.07.072
177. Mariño Z, Crespo G, D’Amato M, et al. Intravenous silibinin monotherapy shows significant antiviral activity in HCV-infected patients in the peri-transplantation period. J Hepatol. 2013;58(3):415–420. doi:10.1016/j.jhep.2012.09.034
178. Rendina M, D’Amato M, Castellaneta A, et al. Antiviral activity and safety profile of silibinin in HCV patients with advanced fibrosis after liver transplantation: a randomized clinical trial. Transpl Int. 2014;27(7):696–704. doi:10.1111/tri.12324
179. Malaguarnera M, Motta M, Vacante M, et al. Silybin-vitamin E-phospholipids complex reduces liver fibrosis in patients with chronic hepatitis C treated with pegylated interferon α and ribavirin. Am J Transl Res. 2015;7(11):2510–2518.
180. Méndez-Sánchez N, Dibildox-Martinez M, Sosa-Noguera J, Sánchez-Medal R, Flores-Murrieta FJ. Superior silybin bioavailability of silybin–phosphatidylcholine complex in oily-medium soft-gel capsules versus conventional silymarin tablets in healthy volunteers. BMC Pharmacol Toxicol. 2019;20(1):5. doi:10.1186/s40360-018-0280-8
181. Siegel AB, Narayan R, Rodriguez R, et al. A Phase I Dose-Finding Study of Silybin Phosphatidylcholine (Milk Thistle) in Patients With Advanced Hepatocellular Carcinoma. Integr Cancer Ther. 2014;13(1):46–53. doi:10.1177/1534735413490798
182. Bares JM, Berger J, Nelson JE, et al. Silybin Treatment is Associated With Reduction in Serum Ferritin in Patients With Chronic Hepatitis C. J Clin Gastroenterol. 2008;42(8):937–944. doi:10.1097/MCG.0b013e31815cff36
183. Dallio M, Masarone M, Romeo M, et al. PNPLA3, TM6SF2, and MBOAT7 Influence on Nutraceutical Therapy Response for Non-alcoholic Fatty Liver Disease: a Randomized Controlled Trial. Front Med Lausanne. 2021;8:734847. doi:10.3389/fmed.2021.734847
184. Rutter K, Scherzer TM, Beinhardt S, et al. Intravenous Silibinin as ‘Rescue Treatment’ for On-Treatment Non-Responders to Pegylated Interferon/Ribavirin Combination Therapy. Antivir Ther. 2011;16(8):1327–1333. doi:10.3851/IMP1942
185. Mulrow C, Lawrence V, Jacobs B, et al. Milk thistle: effects on liver disease and cirrhosis and clinical adverse effects. Evid Rep Technol Assess. 2000;(21):1–3.
186. YHTPAD Yaoxue Tongbao. Bulletin of Pharmacology. 1983;18:404.
187. Sahibzada MUK, Sadiq A, Khan S, et al. Fabrication, characterization and in vitro evaluation of silibinin nanoparticles: an attempt to enhance its oral bioavailability. Drug Des Devel Ther. 2017;11:1453–1464. doi:10.2147/DDDT.S133806
188. Tartari APS, Peczek SH, Fin MT, Ziebarth J, Machado CS, Mainardes RM. Bovine Serum Albumin Nanoparticles Enhanced the Intranasal Bioavailability of Silybin in Rats. Pharmaceutics. 2023;15(12):2648. doi:10.3390/pharmaceutics15122648
189. Wang Y, Wei H, Li K, et al. Ros-responsive dextran-phenylboronic acid-silibinin nanoparticles for targeting delivery of BAPTA-AM to effectively eliminate calcium overload-mediated inflammatory cascades and mitochondrial apoptosis: alleviating acute liver injury. Chem Eng J. 2024;480:148283. doi:10.1016/j.cej.2023.148283
190. de Carvalho TG, Garcia VB, de Araújo AA, et al. Spherical neutral gold nanoparticles improve anti-inflammatory response, oxidative stress and fibrosis in alcohol-methamphetamine-induced liver injury in rats. Int J Pharm. 2018;548(1):1–14. doi:10.1016/j.ijpharm.2018.06.008
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.