Back to Journals » Patient Preference and Adherence » Volume 12
Novel methods to estimate antiretroviral adherence: protocol for a longitudinal study
Authors Saberi P ![]() , Ming K
, Ming K ![]() , Legnitto D, Neilands TB
, Legnitto D, Neilands TB ![]() , Gandhi M, Johnson MO
, Gandhi M, Johnson MO ![]()
Received 1 March 2018
Accepted for publication 26 April 2018
Published 18 June 2018 Volume 2018:12 Pages 1033—1042
DOI https://doi.org/10.2147/PPA.S166380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Parya Saberi, Kristin Ming, Dominique Legnitto, Torsten B Neilands, Monica Gandhi, Mallory O Johnson
Department of Medicine, University of California San Francisco, San Francisco, CA, USA
Background: There is currently no gold standard for assessing antiretroviral (ARV) adherence, so researchers often resort to the most feasible and cost-effective methods possible (eg, self-report), which may be biased or inaccurate. The goal of our study was to evaluate the feasibility and acceptability of innovative and remote methods to estimate ARV adherence, which can potentially be conducted with less time and financial resources in a wide range of clinic and research settings. Here, we describe the research protocol for studying these novel methods and some lessons learned.
Methods: The 6-month pilot study aimed to examine the feasibility and acceptability of a remotely conducted study to evaluate the correlation between: 1) text-messaged photographs of pharmacy refill dates for refill-based adherence; 2) text-messaged photographs of pills for pill count-based adherence; and 3) home-collected hair sample measures of ARV concentration for pharmacologic-based adherence. Participants were sent monthly automated text messages to collect refill dates and pill counts that were taken and sent via mobile telephone photographs, and hair collection kits every 2 months by mail. At the study end, feasibility was calculated by specific metrics, such as the receipt of hair samples and responses to text messages. Participants completed a quantitative survey and qualitative exit interviews to examine the acceptability of these adherence evaluation methods. The relationship between the 3 novel metrics of adherence and self-reported adherence will be assessed.
Discussion: Investigators conducting adherence research are often limited to using either self-reported adherence, which is subjective, biased, and often overestimated, or other more complex methods. Here, we describe the protocol for evaluating the feasibility and acceptability of 3 novel and remote methods of estimating adherence, with the aim of evaluating the relationships between them. Additionally, we note the lessons learned from the protocol implementation to date. We expect that these novel measures will be feasible and acceptable. The implications of this research will be the identification and evaluation of innovative and accurate metrics of ARV adherence for future implementation.
Keywords: adherence assessment, HIV, hair measures, pill counts, pharmacy refills, remote study, text message, antiretroviral therapy, PrEP
Background
Strict adherence to antiretroviral (ARV) medications is critical for attaining human immunodeficiency virus (HIV) treatment goals, such as sustained suppression of plasma HIV RNA, decreased risk of developing drug resistance, improved quality of life, and reduced risk of HIV transmission.1–3 Commonly used methods to estimate ARV adherence include patient’s self-report, pharmacy refill data, pill counts, medication event monitoring system (MEMS) caps, and analysis of drug levels in a biomatrix (eg, plasma, dried blood spots, and hair). However, there is no gold standard of assessing adherence,1 and clinicians and researchers often resort to the most feasible and cost-effective methods possible, which may result in biased or inaccurate estimates.
Investigators conducting adherence research are often limited to using either self-reported adherence, a subjective and potentially overestimated measure that is prone to recall and social desirability biases,4,5 or other more complex methods, such as pharmacologic measures or electronic drug monitoring, which require expertise and financial resources. Numerous direct measurement methods (eg, quantification of concentrations of active drug or metabolites in the blood,6–8 urine,9 and hair10,11) and indirect methods (eg, patient self-report,12–14 pharmacy refill records,15,16 pill counts,12 and use of MEMS caps12,14) have been employed, but there is no consensus over the best approach to assess medication adherence. Each method has advantages and disadvantages.
Additionally, most ARV adherence research to date has required the physical presence of participants at a study site to take part in studies. This may create difficulties in recruitment and retention given the burden associated with the need to have access to modes of and funds for transportation and the time required for visits. These time and resource costs are further exacerbated when the study requires multiple visits. Furthermore, among people living with HIV (PLWH), perceived stigma or negative social consequences associated with participating in research may be the important barriers to participation.17 In addition to personal inconveniences, these barriers to research participation can result in missing data and potentially biased results.
In this study, we evaluated the feasibility and acceptability of 3 innovative methods to estimate ARV adherence using remote collection of data. These novel methods involve text-messaged photographs of pharmacy refill dates, text-messaged photographs of pills for pill count, and home collection of hair samples. All 3 can be conducted relatively quickly and with limited financial resources in a wide range of health care systems and research settings. Here, we describe our research protocol and lessons learned.
Methods
Study overview and design
We conducted a 6-month study to 1) assess the feasibility and acceptability of novel methods of estimating ARV adherence using text-messaged photographs of pharmacy refill dates and pill counts and home-collected hair samples; 2) examine the feasibility and acceptability of a study where all study activities, including recruitment, consent, hair sample collection, text messaging, and exit interviews, were conducted remotely; and 3) explore the relationship between ARV adherence based on self-report and the 3 novel metrics, specifically text-messaged photographs of pharmacy refill dates and pill counts, and drug levels in hair samples collected at home.
Table 1 provides an overview of the study. Participants were asked to mail back home-collected hair samples at baseline, 2, 4, and 6 months using the hair collection kits sent to them by study staff. At baseline and once monthly, for 6 months, participants were sent 4 text messages, referred to as Adherence Survey, asking them to 1) rate their ARV medication adherence using a validated self-report item,18 2) text message a photograph of the refill date on the ARV medication bottle that they were using at that time, 3) text message a photograph of the contents inside the ARV medication bottle or pillbox that they were using at that time, and 4) the approximate date when they picked up their latest ARV refill from the pharmacy. Additionally, at baseline and at 6 months, participants were asked about any extra ARV pills that they may have (ie, stock supply of medications). Finally, at 6 months, we conducted quantitative feasibility and acceptability surveys and qualitative exit interviews. We received approval from the University of California, San Francisco (UCSF) Institutional Review Board to conduct this study, and written informed consent was obtained from all participants.
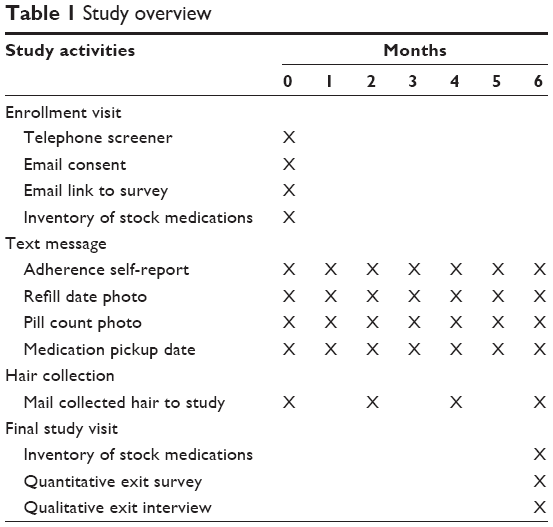 | Table 1 Study overview |
Inclusion and exclusion criteria
Adults living with HIV who met the following criteria were eligible for study participation:
- Being on 1 ARV regimen for at least 3 consecutive months prior to participation and report that they were unlikely to change ARV medications in the next 6 months: to allow enough time for individuals to become familiar with their new regimen, make any changes in case of adverse effects, accumulate sufficient ARV levels in their hair, and allow study staff to monitor 1 ARV regimen during the 6 months of the study.
- Being on ARV regimens containing tenofovir (TFV) (either tenofovir disoproxil fumarate [TDF] or tenofovir alafenamide [TAF]), emtricitabine (FTC), darunavir (DRV), or dolutegravir (DTG): these ARV medications currently have validated assays in hair in the UCSF Hair Analytical Laboratory (HAL) and were part of the first-line regimens recommended at the Department of Health and Human Services guidelines at the time of this study.19 The brand names of ARV regimens that included these medications were Atripla, Complera, Descovy, Emtriva, Genvoya, Odefsey, Prezcobix, Prezista, Stribild, Tivicay, Triumeq, Truvada, and Viread.
- Have access to a mobile telephone that supported photography and transmission of the photographs via text message (note that this included any basic mobile telephone with a camera and a data plan): this allowed participants to take photographs of the refill dates and pill counts to send to study staff.
- Have access to the Internet (through mobile telephones, personal computers, or public computers): this allowed for study staff to email consent forms, baseline surveys, exit quantitative survey, as well as other communications.
Participants who reported receiving automated refills (and thus not having any active role in receiving their next refill through either contacting their pharmacy to generate a new refill or physically picking up their refill from the pharmacy), those who had chronic kidney disease necessitating renallydosed ARVs, and those who were unable to provide hair samples (due to baldness or other reasons, such as wearing a weave that prevented individuals from cutting hair close to the scalp) were excluded from the study.
Recruitment
We advertised on online social media (ie, Facebook and Instagram) to recruit participants nationwide. Participants were offered a total of $270 for all study activities (see Section “Incentive Structure”). We spent a total of US$1,300 over 4 weeks for advertisement. The mean cost per click was ~$0.36, and we had about 2,771 clicks. We narrowed our advertisements to be shown to adults (>18 years of age) living in the USA and used key terms related to HIV; acquired immunodeficiency syndrome (AIDS); lesbian, gay, bisexual, and transgender; homosexuality; ACT UP; and same-sex marriage.
In addition to the online social media advertisements, we created a Facebook page (www.facebook.com/RxPixStudy), a Twitter account (twitter.com/rxpixstudy), and a website (rxpix.ucsf.edu/) to further improve our web presence and provide additional information about the study. We sent a total of 25 emails to organizations serving PLWH nationwide to notify them about our study, posted flyers at clinics serving PLWH in the San Francisco Bay Area, and asked the UCSF Center for AIDS Prevention Studies Community Advisory Board to assist us in recruitment through email, social media, and word of mouth. Finally, through snowball sampling, we offered our participants $10 for each eligible individual they referred who consented to participate in the study.
Enrollment
Participants who emailed, called, or text messaged the study staff were given a brief description of the study, including the study’s interest in collecting hair samples, to assess the participant’s ability and willingness to submit hair samples. Interested individuals were then screened according to the inclusion/exclusion criteria. Those who were eligible and interested were asked for their contact information (including mobile telephone number; other telephone numbers; mailing address; email address; friend or family contact information; and social media [Facebook, Instagram, Twitter, Snapchat, and others] usernames). At this time, participants were scheduled for a 30-minute enrollment call before which they were requested to view “The RxPix Study: What to Expect” video (http://rxpix.ucsf.edu/videos) and gather all of their ARV medication containers in one place for an inventory. During the enrollment call, participants were given an opportunity to ask questions about the study activities, including the hair collection video. If they remained interested, they were then emailed a link to the consent form and baseline survey.
Data collection
Qualtrics (Qualtrics, Provo, UT, USA; version March 2017), a data collection software to conduct online surveys, was used to obtain informed consent and collect initial demographic and clinical data, and for the final exit survey. The links to these surveys were emailed to participants. The baseline survey included questions regarding demographics (age, race/ethnicity, sex/gender, sexual orientation, income, and education), use of alcohol or other substances, HIV clinical outcomes (CD4+ cell count, detectability of HIV viral load) engagement in HIV care, names of ARV medications, medication adherence over the past 30 days based on the visual analog scale20 and the rating scale,18 barriers to and facilitators of adherence,21,22 and familiarity of use of technology for health care.
At baseline and for months 1 through 6, we collected adherence data using text messaging. For this, we used the services of a company named Mosio, which offers text messaging software for clinical research, to automate the sending of our Adherence Surveys on a monthly basis and reminder text messages as needed. During the study, we used text messaging, telephone, and email to contact participants. The qualitative exit interviews were conducted by telephone and were audio-recorded.
Study outcomes
Study outcomes included the feasibility and acceptability of the various methods of estimating ARV medication adherence (ie, text-messaged photographs of pharmacy refill dates and pill counts and home-collected hair samples), the feasibility and acceptability of a study where all study activities were conducted remotely, and the relationship between the various methods of ARV medication adherence estimation.
For feasibility and acceptability of our adherence-estimating methods and the remote research methodology, at 6 months, we conducted a quantitative survey among all study participants and a qualitative exit interview with one-third of participants who met the criteria for the following categories: 1) On Time: those who responded to the Adherence Survey and sent hair samples within the “early window period”, that is, within 5 days after the Adherence Survey was sent and 11 days after hair kit was sent (N=12); 2) Early Inconsistent Hair Samples: participants who sent 1 or more hair samples up to 6 days after the “early window period” for hair sample, that is, 11 days after hair kit was sent (N=5); 3) Late Inconsistent Hair Samples: participants who sent 1 or more hair samples at least 7 days after the “early window period” for hair samples or not at all (N=5); 4) Inconsistent Texts: those who at any point in the study responded to the Adherence Surveys after the “early window period” for text message (ie, within 5 days after the Adherence Survey was sent) or did not complete the Adherence Survey at all (N=3); and 5) Least Consistent: participants who responded to the Adherence Surveys after the text message and sent their hair samples after the “early window period” or not at all (N=6).
During these interviews, participants were asked about 1) the difficulties with each study component (text messaging, hair collection, etc.); 2) the likelihood of participating in other studies using a similar design; 3) the perceptions on privacy and security of data; 4) the perceptions on the potential impact of study procedures on their medication adherence, 5) the advantages and disadvantages of participating in an entirely remotely conducted research project, and 6) the problems with the collection of hair samples or ease of following hair collection instructions. Exit interviews lasted about 30 minutes and were audio-recorded for analysis.
In addition to the list of specific technological problems (eg, mobile telephone breaks in service, email-related issues, etc.), we examined the feasibility using prespecified feasibility measures, which were evaluated by specific metrics as listed in Table 2.
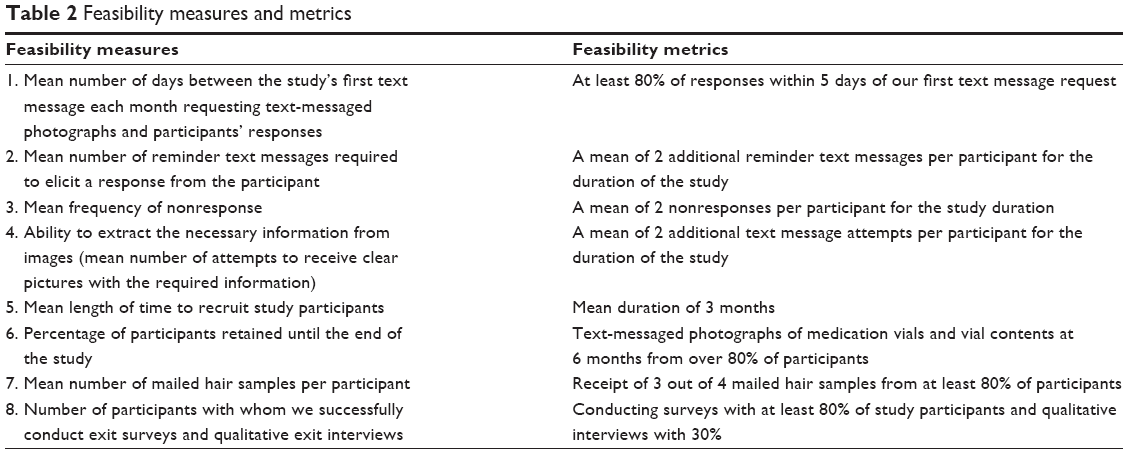 | Table 2 Feasibility measures and metrics |
Text messaging
The mobile telephone number of enrolled participants was entered into a Health Insurance Portability and Accountability Act-compliant clinical research text messaging software called Mosio. For individuals who were taking >1 ARV pill per day (eg, those not on fixed-dose combinations), we chose to study a particular target ARV based on a prespecified hierarchy (TDF > FTC > DRV > DTG > TAF). The hierarchy was based on the amount of research performed on specific ARV levels in hair. At this time, participants were sent 4 sequential text messages:
- Thinking back over the past 30 days, please rate your ability to take all your medications as prescribed: 1) Excellent, 2) Very good, 3) Good, 4) Fair, 5) Poor, and 6) Very poor.18
- Thanks! Next, please text me a photo of the refill date on the bottle you are using now.
- Thanks! Next, please text me a photo of the pills you have left in the bottle you are using now.
- Great! Finally, please text me the date when you actually picked up your most recent refill (take your best guess).
These messages were responded to during the initial telephone enrollment meeting so that participants could ask questions, their mobile telephones could be tested for text messaging photographs, any technical issues around picture quality and text messaging could be resolved, and study staff could collect baseline data.
In addition to baseline, participants were asked these questions for months 1 through 6. Participants who did not respond were sent an automated reminder text message 1 and 4 days after they received these text messages. To encourage participants to send us their text message responses in a timely manner, we created an “early window period” of 5 days after receipt of the Adherence Survey as a metric of performance.
Hair sample
Medication concentrations in hair reflect drug uptake from the systemic circulation over weeks to months and provide a mean measure of ARV exposure.23,24 The UCSF HAL has pioneered the use of small hair samples to monitor ARV medication adherence,10,11,24–39 has developed methods to extract and analyze ARV levels from hair,31,32 and demonstrated that hair ARV levels are the strongest independent predictor of virologic success.11,28,29,39 Unlike phlebotomy, hair collection is noninvasive and does not require specific skills, sterile equipment, or specialized storage conditions. In a prior study,40 we had demonstrated that the home collection of hair was feasible and acceptable, and that there was a high degree of correlation and agreement between ARV levels in hair collected by trained study staff and at home by participants, as well as between hair collected from the back and side of the head, all without the evidence of measurement bias.
The UCSF HAL performed the assays for ARV levels in hair. With its predecessor (the Drug Studies Unit) formed in 1977, this laboratory is equipped with modern facilities and highly trained staff to provide fully automated analysis for drugs and metabolites. The HAL has developed and reported methods to analyze TFV as well as other ARVs in human hair samples using liquid chromatography/tandem mass spectrometry (LC/MS-MS).24,28,29,31,32,41–44 Most of the HAL assays have been peer reviewed and approved by the National Institutes of Health’s Division of AIDS Clinical Pharmacology and Quality Assurance Program.45 Hair samples are collected using previously described methods, the proximal section (side closest to the scalp) is cut to 1.0 cm (representing the past month of exposure), the relevant ARV is extracted using optimized methods and analyzed via LC/MS-MS. For example, TFV in participants on either TDF or TAF is extracted with 50% methanol/water containing 1% trifluroacetic acid, 0.5% hydrazine dihydrochloride, and internal standard in a 37°C shaking water bath overnight (>12 hours) and analyzed by LC/MS-MS.41 The relative error (%) and precision (coefficients of variation) for spiked quality control hair samples at low, medium, and high concentrations are all <15%. This method to analyze TFV levels in hair was validated from 0.002 to 0.400 nanogram per milligram (ng/mg) hair, with a lower limit of quantitation at 0.002 ng/mg.42,46 In addition to TFV and FTC, HAL will analyze hair ARV levels for DRV and DTG.
We mailed participants hair collection kits containing 2 alcohol wipes, 1 piece of aluminum foil (cut into 4 × 4 inches), 2 adhesive labels, a sealable storage plastic bag (marked with the participant’s unique identification number), 2 desiccant packs, and a self-posted envelope addressed to our university office. These kits included detailed instructions for hair collection (http://rxpix.ucsf.edu/hair-collection-instructions) and the video link on our website demonstrating home collection of hair (http://rxpix.ucsf.edu/videos). Hair collection kits were mailed at baseline, 2, 4, and 6 months, and were sent 11 days before the sample due date. To encourage the participants to mail us their hair samples in a timely manner, we defined an “early window period” of 11 days after mailing of the hair collection kit as the goal. Hair samples can be stored at room temperature and are not biohazardous, so are easy to store and ship. The HAL was asked to provide hair ARV levels based on the prespecified ARV hierarchy (TDF > FTC > DRV > DTG > TAF). In other words, if a participant was taking multiple ARVs that could have been measured, the HAL used this hierarchy to determine the order of analysis while being attentive to the amount of hair sample available.
Incentive structure
We offered a total of $270 for the timely completion of all study activities, which was provided to participant via ClinCard, a reloadable debit card that enabled remote participant reimbursements via a web-based portal. The incentive breakdown included $10 for baseline test text messages and $15 for 4 text messages at months 1 through 6, $5 for timely text message response (ie, text message photographs sent within 5 days of request) each month, $10 for the baseline survey, and $20 for the exit survey/interview. We used a gradually increasing incentive structure for the hair sample collection and shipment: $15 for the receipt of baseline hair sample, $20 for the 2-month hair sample, $25 for the 4-month hair sample, and $30 for the 6-month hair sample. Participants were offered an additional $5 for each hair sample mailed in a timely manner (ie, postmarked within 11 days after mail-out of hair kit).
We extracted the following information from the ARV medication vial photographs: medication name, total number of tablets dispensed at the time of refill, and refill date. From the photograph of the contents of their ARV medication vial, we counted the number of tablets remaining to establish adherence based on pill count.47,48 Additionally, at baseline and months 2, 4, and 6, we asked participants to mail us home-collected hair samples using our hair collection kits after viewing an online demonstration of the process. Finally, we conducted online exit surveys and telephone interviews with participants to evaluate the acceptability of our research methodology and their experience with the home collection of hair samples. Ability to comply with monthly text messaging and frequency of late or nonresponse constituted parameters for assessing the feasibility of this novel adherence-estimating method. Our ability to conduct a completely remote research project was used to evaluate the overall feasibility of our study design. Participants’ responses to exit surveys and interviews were used to assess acceptability via quantitative and qualitative methods.
Sample size estimates
Self-reported adherence and TFV levels in hair have a 0.34 correlation at 8 weeks.26 Given that self-report is subjective and is frequently overestimated, 0.34 is the minimum correlation that we required between our novel text message-based adherence measure and TFV levels in hair. To detect a minimum correlation of ≥0.34 at 6 months, we needed a minimum of 65 participants. We assumed a 20% attrition during the course of the study to calculate the total number of participants that we needed to enroll at baseline (N=82).
Planned data analysis
For our future data analysis, one-way frequency tables will be generated for all feasibility and acceptability measures. Audio-recorded interviews will be transcribed by a transcriptionist. For analysis of these recordings, broad themes will be identified, refined through discussion, and entered into a matrix using Microsoft Excel where each column corresponds to a theme and each row represents a case. This method allows for the identification of patterns in the distribution of themes for data analysis.49 One investigator will categorize each interview (N=31) using this matrix. Another investigator will double code a random subsample (N=7) of the interviews, and coding discrepancies will be discussed by the 2 authors until consensus is reached or arbitrated by the first author. Collectively, the results from the quantitative exit survey analyses will complement the qualitative interview data.
Measures
Self-reported ARV medication adherence was evaluated by the adherence rating scale.18 This single item has been linked to more objective adherence estimates, that is, MEMS caps. The approximate correlation with adherence percentage based on MEMS caps is as follows: very poor=0%, poor=20%, fair=40%, good=60%, very good=80%, and excellent=100%.
We will calculate refill date-based measure of adherence (from text-messaged photos of ARV regimen vials) using the medication possession ratio (MPR) and proportion of days covered (PDC) formulas.50 MPR is the ratio of the sum of days’ supply for all fills in a specific period divided by the number of days in the period. PDC is the total number of days’ supply in a specific period “covered” divided by the number of days in the period. MPR may result in an overestimation of adherence because it does not take overlapping days into account; therefore, it will be capped at 100%. These formulas yield a value of 0%–100%.
We will calculate pill count-based ARV adherence using the methods established by Bangsberg and Kalichman.47,48,51 It will be estimated by the difference between tablets counted by the study staff in 2 consecutive text-messaged photographs sent by the participant (eg, difference between the current and previous pill counts) divided by the total doses prescribed in a certain time period (eg, total number of tablets that should have been taken during the 30 days). This value will take into account the number of pills dispensed during that time period. This formula yields a value of 0%–100%.
Finally, ARV levels in hair at baseline, and months 2, 4, and 6 will be measured as ng/mg hair and will be log-transformed to reduce skewed levels. We will assess hair concentrations as continuous measures. Prior studies have shown a graded relationship between hair ARV levels and virologic outcomes.11,28,43
Statistical analysis
First, we will conduct univariate analyses (eg, one-way frequency tables, measures of central tendency, and variability) to participants’ baseline and exit surveys and standings on the feasibility measures listed in Table 2. We will then describe the correlation of ARV levels in hair averaged across baseline, and months 2, 4, and 6 with adherence estimated based on the rating scale, refill dates, and pill counts averaged over the 6-month study. Next, we will investigate the longitudinal relationship of ARV refill data, pill count, and ARV levels in hair at months 2, 4, and 6. These analyses will take advantage of the longitudinal nature of the data by using multilevel mixed-effects or generalized estimating equation models with separate between-subjects and within-subjects effects for the ARV predictor52,53 with the latter optionally parameterized to represent the average within-participant change in adherence over time since baseline. Changes since baseline in adherence will enable us to investigate whether adherence changed as a result of joining the study. Maximum likelihood estimation or multiple imputation will be used to address the missing data in inferential analyses under the missing at random assumption.54 Finally, we will conduct additional exploratory analyses as necessary.
Ethics approval and consent to participate
We received approval from the UCSF Institutional Review Board (IRB) to conduct this study and written consent from all participants.
Discussion
We have established a protocol, which we describe here for remotely conducting a study to assess the acceptability and feasibility of novel ARV medication adherence measurement approaches. While analyses evaluating the outcomes of the study are currently under way, the protocol established for this study was implemented successfully and offers guidance for others seeking to conduct research using similar methodologies. The advantages of tracking medication adherence both remotely and by these novel methods may translate to other HIV- and non-HIV-related studies; however, the implementation of the protocol to date has led to various lessons learned.
Contact information
Because all activities were conducted remotely with no face-to-face contact with participants, it was critical to collect and maintain multiple sources of contact information from enrollees. Relying on mobile telephone numbers only is insufficient in the not infrequent occurrence of lost or stolen telephones. Similarly, relying on email contact was often inadequate, as some individuals did not monitor their email accounts with regularity. Rather, a combination of text messaging, emailing, and telephone calls was often needed to minimize the study attrition and loss to follow-up. Additionally, we collected social media contact information.
Remote payment
The use of reloadable debit cards allowed for remote and timely disbursement of payment for participation in study activities. We, therefore, established tips for the optimal use of the cards. When mailing out ClinCards, we recommend that study staff consider waiting until the participant has confirmed the receipt of the card in the mail before registering the card to the individual and adding funds to the card. This avoids fraud resulting from others intercepting the card and allows the study to reuse the card should the envelope be returned in the mail. We also learned that it was wise to include a short information sheet with the mailed ClinCard, emphasizing that participants should treat the card like cash and to contact the study immediately if the card is lost or stolen, with the intent that this would preempt participant questions and assist with managing lost cards. We have created such an information sheet for our future research: http://rxpix.ucsf.edu/clincard-quick-info.
Home collection of hair samples
The use of home hair collection for medication adherence estimation offers great promise, but has never been attempted on the scale implemented in this study. The benefit of this method is that hair samples do not require a cold chain or biohazard precautions for storage or shipment. They provide a mean measure of drug uptake and exposure over weeks to months. However, they require a specialty laboratory, such as HAL for analysis and reporting. We noted a few important steps to help improve efficiency in data collection and data accuracy above and beyond our approach. We recommend including the participant’s unique identification number on the return envelope as well as the included sealable storage plastic bag. This facilitates the identification and documentation of the hair sample even if the participant fails to place it inside the storage bag provided. Additionally, a great deal of staff effort went into following up with participants about late or missing hair samples. We later realized that it assisted some participants to be notified by text or email on the day that we mailed out the hair kits so they knew to expect it in the mail. Another method that may work is to frequently remind participants of their study schedule dates at specific time points (eg, monthly).
Text messaging of photographs
The photographed documentation of refill dates from medication vials was likewise an innovative aspect of the study. This approach is simple and cost-effective, and provides an objective measure of medication adherence. The limitation of this approach is that some participants reported that their prescription label was on a medication box, which they had thrown away; therefore, we recommend instructing participants in this scenario to take a picture of the refill date as soon as they pick up the refill, rather than waiting until their monthly text date. Another challenge of the study protocol was that we were unable to document how many participants may have switched to receive their refills in an automated manner. This would have made them ineligible to originally enroll in the study as part of our exclusion criteria.
Similarly, photographed documentation of pill counts to elicit adherence is a novel method of estimating adherence. It too is simple and cost-effective, and provides an objective measure of medication adherence. However, in certain cases, it was difficult to track pills a participant may have taken that came from places other than their medication bottle (eg, borrowed pills from a partner or friend, pills taken during a hospital stay). We, therefore, recommend the inclusion of survey items to evaluate the occurrence and frequency of these deviations from the standard practice of taking pills from a designated prescription bottle. Finally, even though we inquired about stock medications, many participants did not know how many pills they had in addition to the ones they were using from their most recent medication bottle or had so many that they were unable to report an accurate count. Even though it may be time consuming, spending more time with each participant after enrollment and at the end of the study to establish an accurate number of stock medications will be very helpful to understanding pill count discrepancies.
Other limitations of this study include the potential lack of generalizability due to voluntary response bias, in that participants were self-selected volunteers for this research. Additionally, information related to demographics and other medical data were self-reported and, therefore, subject to recall bias.
In summary, this is the first study to examine the 3 novel methods to estimate ARV medication adherence among PLWH. Upon completion of data collection, we will analyze qualitative and quantitative data to examine the feasibility and acceptability of the remotely conducted research and the various methods to estimate ARV adherence, as well as the correlation of these estimations with each other. The expected outcome of this study is that these 3 novel methods will be feasible and acceptable, will have high levels of correlation with each other, and will contribute to the future adherence research. Since hair collection does not require a cold chain or biohazard precautions for storage or shipment, and estimation of adherence based on text-messaged photographs of pill counts and refill dates is objective and cost-effective, these methods may be the important steps to expanding objective adherence monitoring tools in the context of HIV treatment and prevention studies worldwide.
Acknowledgments
The authors would like to thank the research participants and the UCSF HAL. Research reported in this publication was supported by the National Institute of Mental Health of the National Institutes of Health under Award Numbers R21MH108414 (PI Saberi), K23MH097649 (PI Saberi), K24DA037034 (PI Johnson), and the National Institute of Allergy and Infectious Diseases R01AI098472 (PI Gandhi). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funding agencies have had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Chesney MA. The elusive gold standard. Future perspectives for HIV adherence assessment and intervention. J Acquir Immune Defic Syndr. 2006;43(Suppl 1):S149–S155. | ||
World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. Geneva; World Health Organization; 2003. | ||
Cohen MS, Chen YQ, McCauley M, et al; HPTN 052 Study Team. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505. | ||
Berg KM, Arnsten JH. Practical and conceptual challenges in measuring antiretroviral adherence. J Acq Imm Def. 2006;43:S79–S87. | ||
Kagee A, Nel A. Assessing the association between self-report items for HIV pill adherence and biological measures. Aids Care. 2012;24(11):1448–1452. | ||
Duong M, Piroth L, Peytavin G, et al. Value of patient self-report and plasma human immunodeficiency virus protease inhibitor level as markers of adherence to antiretroviral therapy: relationship to virologic response. Clin Infect Dis. 2001;33(3):386–392. | ||
Brambilla D, Jennings C, Aldrovandi G, et al. Multicenter evaluation of use of dried blood and plasma spot specimens in quantitative assays for human immunodeficiency virus RNA: measurement, precision, and RNA stability. J Clin Microbiol. 2003;41(5):1888–1893. | ||
Cassol S, Salas T, Gill MJ, et al. Stability of dried blood spot specimens for detection of human-immunodeficiency-virus DNA by polymerase chain-reaction. J Clin Microbiol. 1992;30(12):3039–3042. | ||
Kumar AK, Ramachandran G, Kumar P, Kumaraswami V, Swaminathan S. Can urine lamivudine be used to monitor antiretroviral treatment adherence? MedGenMed. 2006;8(4):53. | ||
Gandhi M, Greenblatt RM. Hair it is: the long and short of monitoring antiretroviral treatment. Ann Intern Med. 2002;137(8):696–697. | ||
Gandhi M, Ameli N, Bacchetti P, et al. Atazanavir concentration in hair is the strongest predictor of outcomes on antiretroviral therapy. Clin Infect Dis. 2011;52(10):1267–1275. | ||
Liu H, Golin CE, Miller LG, et al. A comparison study of multiple measures of adherence to HIV protease inhibitors. Ann Intern Med. 2001;134(10):968–977. | ||
Walsh JC, Mandalia S, Gazzard BG. Responses to a 1 month self-report on adherence to antiretroviral therapy are consistent with electronic data and virological treatment outcome. Aids. 2002;16(2):269–277. | ||
Hugen PW, Langebeek N, Burger DM, et al. Assessment of adherence to HIV protease inhibitors: comparison and combination of various methods, including MEMS (electronic monitoring), patient and nurse report, and therapeutic drug monitoring. J Acquir Immune Defic Syndr. 2002;30(3):324–334. | ||
Saberi P, Caswell N, Amodio-Groton M, Alpert P. Pharmacy-refill measure of adherence to efavirenz can predict maintenance of HIV viral suppression. Aids Care. 2008;20(6):741–745. | ||
Grossberg R, Zhang YW, Gross R. A time-to-prescription-refill measure of antiretroviral adherence predicted changes in viral load in HIV. J Clin Epidemiol. 2004;57(10):1107–1110. | ||
DiClemente RJ, Ruiz MS, Sales JM. Barriers to adolescents’ participation in HIV biomedical prevention research. J Acquir Immune Defic Syndr. 2010;54:S12–S17. | ||
Lu M, Safren SA, Skolnik PR, et al. Optimal recall period and response task for self-reported HIV medication adherence. AIDS Behav. 2008;12(1):86–94. | ||
Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. 2016; Available from: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed September 10, 2017. | ||
Amico KR, Fisher WA, Cornman DH, et al. Visual analog scale of ART adherence: association with 3-day self-report and adherence barriers. J Acquir Immune Defic Syndr. 2006;42(4):455–459. | ||
Chesney MA, Ickovics JR, Chambers DB, et al. Self-reported adherence to antiretroviral medications among participants in HIV clinical trials: the AACTG adherence instruments. Patient Care Committee & Adherence Working Group of the Outcomes Committee of the Adult AIDS Clinical Trials Group (AACTG). Aids Care. 2000;12(3):255–266. | ||
Saberi P, Yuan P, John M, Sheon N, Johnson MO. A pilot study to engage and counsel HIV-positive African American youth via telehealth technology. AIDS Patient Care STDS. 2013;27(9):529–532. | ||
Beumer JH, Bosman IJ, Maes R. Hair as a biological specimen for therapeutic drug monitoring. Int J Clin Pract. 2001;55(6):353–357. | ||
Gandhi M, Greenblatt RM, Bacchetti P, et al. A single-nucleotide polymorphism in CYP2B6 leads to > 3-fold increases in efavirenz concentrations in plasma and hair among HIV-infected women. J Infect Dis. 2012;206(9):1453–1461. | ||
Gandhi M, Yang QY, Bacchetti P, Huang Y. Short communication: a low-cost method for analyzing nevirapine levels in hair as a marker of adherence in resource-limited settings. Aids Res Hum Retrov. 2014;30(1):25–28. | ||
Baxi SM, Liu A, Bacchetti P, et al. Comparing the novel method of assessing PrEP adherence/exposure using hair samples to other pharmacologic and traditional measures. J Acquir Immune Defic Syndr. 2014;68(1):13–20. | ||
Hickey MD, Salmen CR, Tessler RA, et al. Antiretroviral concentrations in small hair samples as a feasible marker of adherence in rural Kenya. J Acquir Immune Defic Syndr. 2014;66(3):311–315. | ||
Gandhi M, Ameli N, Bacchetti P, et al; Women’s Interagency HIV Study (WIHS). Protease inhibitor levels in hair strongly predict virologic response to treatment. Aids. 2009;23(4):471–478. | ||
van Zyl GU, van Mens TE, McIlleron H, et al. Low lopinavir plasma or hair concentrations explain second-line protease inhibitor failures in a resource-limited setting. J Acquir Immune Defic Syndr. 2011;56(4):333–339. | ||
Baxi SM, Greenblatt RM, Bacchetti P, et al; Women’s Interagency HIV Study (WIHS). Nevirapine concentration in hair samples is a strong predictor of virologic suppression in a prospective cohort of HIV-infected patients. PLoS One. 2015;10(6):e0129100. | ||
Huang Y, Gandhi M, Greenblatt RM, Gee WN, Lin ET, Messenkoff N. Sensitive analysis of anti-HIV drugs, efavirenz, lopinavir and ritonavir, in human hair by liquid chromatography coupled with tandem mass spectrometry. Rapid Commun Mass Sp. 2008;22(21):3401–3409. | ||
Huang Y, Yang QY, Yoon K, et al. Microanalysis of the antiretroviral nevirapine in human hair from HIV-infected patients by liquid chromatography-tandem mass spectrometry. Anal Bioanal Chem. 2011;401(6):1923–1933. | ||
Gandhi M, Mwesigwa J, Aweeka F, et al; Prevention of Malaria and HIV disease in Tororo (PROMOTE) study. Hair and plasma data show that lopinavir, ritonavir, and efavirenz all transfer from mother to infant in utero, but only efavirenz transfers via breastfeeding. J Acquir Immune Defic Syndr. 2013;63(5):578–584. | ||
Liu AY, Yang QY, Huang Y, et al. Strong relationship between oral dose and tenofovir hair levels in a randomized trial: hair as a potential adherence measure for pre-exposure prophylaxis (PrEP). PLoS One. 2014;9(1):e83736. | ||
Olds PK, Kiwanuka JP, Nansera D, et al. Assessment of HIV antiretroviral therapy adherence by measuring drug concentrations in hair among children in rural Uganda. Aids Care. 2015;27(3):327–332. | ||
Bartelink IH, Savic RM, Mwesigwa J, et al. Pharmacokinetics of lopinavir/ritonavir and efavirenz in food insecure HIV-infected pregnant and breastfeeding women in Tororo, Uganda. J Clin Pharmacol. 2014;54(2):121–132. | ||
Cohan D, Natureeba P, Koss CA, et al. Efficacy and safety of lopinavir/ritonavir versus efavirenz-based antiretroviral therapy in HIV-infected pregnant Ugandan women. Aids. 2015;29(2):183–191. | ||
Gandhi M, Glidden DV, Liu A, et al. Strong correlation between concentrations of tenofovir (TFV) emtricitabine (FTC) in hair and TFV diphosphate and FTC triphosphate in dried blood spots in the iPrEx open label extension: implications for pre-exposure prophylaxis adherence monitoring. J Infect Dis. 2015;212(9):1402–1406. | ||
Koss CA, Natureeba P, Mwesigwa J, et al. Hair concentrations of antiretrovirals predict viral suppression in HIV-infected pregnant and breastfeeding Ugandan women. Aids. 2015;29(7):825–830. | ||
Saberi P, Neilands TB, Ming K, et al. Strong correlation between concentrations of antiretrovirals in home-collected and study-collected hair samples: implications for adherence monitoring. J Acquir Immune Defic Syndr. 2017;76(4):e101–e103. | ||
Yang QY, Liu AY, Gandhi M, Greenblatt RM, Gee W, Huang Y. LC/LC/MS assay of tenofovir in human hair for pre-exposure prophylaxis. Paper presented at: Association of Pharmaceutical Sciences (AAPS) Annual Meeting 2010; New Orleans, LA. | ||
Liu A, Vittinghoff E, Gandhi M, et al. Validating measures of tenofovir drug exposure in a U.S. pre-exposure prophylaxis trial. Paper presented at: 17th Conference on Retroviruses and Opportunistic Infections (CROI); 2010; San Francisco, CA. | ||
Gandhi M, Ameli N, Bacchetti P, et al. Concentrations of efavirenz in hair are strongly correlated with virologic response (Paper 692). Paper presented at: 16th Conference on Retroviruses and Opportunistic Infections (CROI) 2009; Montreal, Canada. | ||
Baxi SM, Greenblatt RM, Bacchetti P, et al. Nevirapine concentrations in hair is a strong predictor of virologic suppression and toxicities. PLoS One. 2015;10(6):e0129100. | ||
DiFrancesco R, Tooley K, Rosenkranz SL, et al. Clinical pharmacology quality assurance for HIV and related infectious diseases research. Clin Pharmacol Ther. 2013;93(6):479–482. | ||
Liu A, Gandhi M, Bacchetti P, et al. Validating hair as a biological marker of tenofovir drug exposure in HIV pre-exposure prophylaxis (PrEP). Paper presented at: 18th Conference on Retroviruses and Opportunistic Infections (CROI); 2011; Boston, MA. | ||
Kalichman SC, Amaral CM, Cherry C, et al. Monitoring medication adherence by unannounced pill counts conducted by telephone: reliability and criterion-related validity. HIV Clin Trials. 2008;9(5):298–308. | ||
Kalichman SC, Amaral CM, Stearns H, et al. Adherence to antiretroviral therapy assessed by unannounced pill counts conducted by telephone. J Gen Intern Med. 2007;22(7):1003–1006. | ||
Miles MB, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook. 2nd ed. Thousand Oaks, CA: Sage Publications; 1994. | ||
Hess LM, Raebel MA, Conner DA, Malone DC. Measurement of adherence in pharmacy administrative databases: a proposal for standard definitions and preferred measures. Ann Pharmacother. 2006;40(7–8):1280–1288. | ||
Bangsberg DR, Hecht FM, Charlebois ED, Chesney M, Moss A. Comparing objective measures of adherence to HIV antiretroviral therapy: electronic medication monitors and unannounced pill counts. Aids Behav. 2001;5(3):275–281. | ||
Neuhaus JM, Kalbfleisch JD. Between- and within-cluster covariate effects in the analysis of clustered data. Biometrics. 1998;54(2):638–645. | ||
Allison P. Fixed Effects Regression Methods for Longitudinal Data Using SAS. Cary, NC: SAS Institute; 2005. | ||
Carpenter JR, Kenward MG, White IR. Sensitivity analysis after multiple imputation under missing at random: a weighting approach. Stat Methods Med Res. 2007;16(3):259–275. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.