")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Novel Follicular Unit Excision Device That Reduces Graft Injury and Improves Ergonomics in Hair Transplantation Surgery
Authors Park JH
Received 28 April 2023
Accepted for publication 1 August 2023
Published 3 August 2023 Volume 2023:16 Pages 2009—2019
DOI https://doi.org/10.2147/CCID.S416257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Video abstract presented by Jae Hyun Park.
Views: 118
Jae Hyun Park
Dana Plastic Surgery Clinic, Gangnam-gu, Seoul, Korea
Correspondence: Jae Hyun Park, Dana Plastic Surgery Clinic, Samju Building 10F, Gandnamdaero 606, Gangnam-gu, Seoul, Korea, Tel +82-2-512-0922, Fax +82-2-512-0942, Email [email protected]
Purpose: Follicular unit excision (FUE) surgery is becoming increasingly popular and the number of grafts transplanted in a single session is increasing. Furthermore, complicated surgeries and those requiring a longer surgical time such as non-shaven FUE and long hair FUE are more actively being performed worldwide. The main aim in FUE surgery is to obtain the best quality grafts while minimizing follicular damage during donor harvest. This article describes a novel FUE device that achieves these goals.
Patients and Methods: We describe a novel FUE device with Bluetooth function, fingertip touch sensor, multiphasic movement, automated operation by setting the interval time between punching motions, ergonomic design, various innovative functions, and an easily upgradable application used to operate the handpiece. We also report the concept of design, mechanism of action, methods of use, and effect of each innovative function.
Results: The various state-of-the-art features of the device minimize the risk of follicular injury when working with a wide variety of scalp and hair follicle types and conditions. In addition, it enables successful donor harvesting by reducing the surgeon’s workload and improving ergonomics.
Conclusion: We introduce an innovative and new device for use in FUE surgery. This novel device has the potential to increase the convenience, scalability, and safety of FUE surgery.
Keywords: FUE, follicular unit excision, hair transplant, alopecia, ergonomics, hair follicle
Introduction
Since the first introduction of follicular unit excision (FUE) surgery in 2002,1 it has become increasingly popular because of its advantages of less postoperative pain and no linear strip scars compared with follicular unit strip surgery.2 In the FUE method, a cylindrical punch is inserted to dissect around the hair follicle, followed by graft extraction.3 Most follicular injury occurs when the cylindrical punch dissects the hair follicle from the surrounding tissue. However, follicular injuries of FUE grafts are not simply classified into intact and transected follicles; hair follicles harvested by the FUE method can cause minor injuries such as paring, fracture, and dermal papilla injury.4 Furthermore, a study in which transplanted hair follicles collected by the FUE method were transplanted into nude mice proved that hair follicles with minor injuries have a lower survival rate than intact hair follicles.5 Therefore, it is very important to minimize hair follicle damage such as paring, fracture, and transection to successfully perform FUE surgery.
FUE surgery is very labor-intensive, physical, and mentally burdensome for the surgeon. The operation time ranges from 3–5 hours to 9–10 hours. In addition, megasessions with more than 3000–4000 grafts are also commonly performed,6 and surgeries that require much longer operation times, such as non-shaven FUE and long hair FUE, are being conducted.7,8 An extended surgical time may contribute to lower graft quality and increased follicular damage.9 Therefore, it is very important to improve the ergonomics and reduce the operation time for patients, doctors, and assistant staff.10,11
Many types of FUE devices have already been introduced. Devroye’s WAW FUE device uses a trumpet-shaped hybrid punch tip in the effort to reduce follicular injury. Trivellini’s punch device is equipped with advanced functions such as multiphasic movement and suction-assisted function. All-purpose Intelligent punch by Umar has a very convenient function; the scalp type has been classified into several representative ones, and the surgeon can simply select the corresponding mode. In addition, Umar also developed an all-purpose FUE device that minimizes hair follicular damage through the so-called “minimal-assist-navigation” phenomenon using a frustoconical, textured end designed punch that can cover all scalp types. He also introduced a function that allows easy extraction of the graft lodged within the punch lumen. All of these existing devices possess various innovative and brilliant functions in their own ways, but the focus has been on reducing follicular damage or graft transection with few pursuing harmonious innovations incorporating ergonomics.
There is a need for a new device that can reduce hair follicle damage and improve ergonomics. Herein, we report a novel versatile device that improves the ergonomics during the FUE procedure, acquires high quality grafts, shortens the operative time, and improves the overall operation process. This article describes the features and use of the novel FUE device, reports the authors’ experiences, and includes a literature review to help hair restoration surgeons optimize their surgical techniques and obtain better quality grafts.
Patients and Methods
Ethical Statement
Institutional Review Board approval was not required or sought as this study was not a prospective or systematic investigation of FUE treatment but followed general principles for routine FUE.
Novel Ergonomic FUE Device
A new FUE device was developed to achieve the goals of minimizing hair follicle damage, shortening the operation time, and improving ergonomics. The device is equipped with a variety of new technologies, enabling everyone from novice surgeons to expert FUE practitioners to experience a new surgical environment and improved surgical results.
This device is compatible with most existing punch tips of various diameters and shapes. Aside from the design or shape of the punch tip, this paper mainly seeks to discuss the functional parts of the handpiece that operates the punch tip and technical portion of the software setting.
Multiphasic Movement
The scalp tissue is composed of the following five layers from outside inward: skin (epidermis and dermis), subcutaneous tissue, galea aponeurosis, loose connective tissue and pericranium.12 As hair follicles on the scalp are mainly located within the fat layer, the FUE punch reaches the subcutaneous adipose tissue through the epidermis and dermis.13 These three layers have very different properties. The epidermis and dermis are hard and dense, while the subcutaneous fat layer is loose and has low density.
The principle of multiphasic motion is that each of the three layers with distinct properties must be approached with different motions. Surgical devices such as the Powered Cole Isolation Device and the Trivellini system are equipped with a multiphasic movement function.14 Our novel second-generation device has been upgraded from the biphasic movement of the first-generation device to multiphasic movement (Figure 1).
 |
Figure 1 Setting the multiphasic movement sequence on a tablet PC. The multiphasic movement sequence is precisely controlled and manipulated by computerized programming to achieve clockwise rotation, counterclockwise rotation, oscillation, and vibration; the surgeon controls the order of these movements, time, power, and oscillating arc. |
Various Punch Movements
Trephine-shaped punches are categorized as manual and motorized punches. The manual punch exerts low torque oscillatory movements. There is currently a wide variety of motorized punch machines available, and a robotic FUE machine has been developed.15 The motorized punch is controlled and manipulated very precisely by computerized programming. The representative movements of the motorized punch are clockwise rotation, counterclockwise rotation, oscillation, and vibration (Figure 2). (Supplemental Video 1)
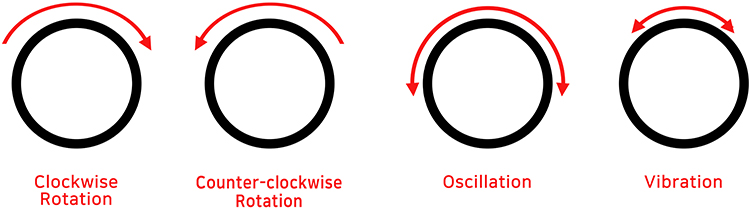 |
Figure 2 Clockwise rotation, counterclockwise rotation, oscillation, and vibration. |
Rotation
The rotating motion of the punch has an increased risk of twisting or distortion of hair follicles, leading to graft transection. However, the rotating motion has the advantage of a relatively fast operation speed. Thus, the rotating motion allows swift and easy tissue dissection, even through tough or thick tissue. The new FUE device enables the surgeon to regulate the speed and motion. In addition, the rotation can be operated in both the clockwise and counterclockwise directions.
Stable Oscillation: Delicate Intelligent Digital Control
Graft torsion is one of the major causes of follicular injury in FUE. One good way to reduce graft torsion is to use oscillatory movement.16 However, many hair surgeons are reluctant to use the oscillatory movement owing to its slower speed compared with rotation. Increasing the oscillation speed inevitably causes inertia due to the sudden change in direction, and the influence of this change must be overcome to enable fast and stable oscillatory motion. Increased speed in oscillation creates increased torque, which inevitably leads to greater inertial motion.
The concept of inertia is very important when it comes to oscillation.17 Inertia refers to the tendency of an object to maintain its state of motion or rest unless it is subjected to an external force. The moment of inertia is a physical quantity that indicates the degree to which an object maintains its rotational motion. The moment of inertia acts on a rotating punch. The inertial mass is the degree to which it is difficult to cause a change in velocity for the same force, while the moment of inertia is the degree to which it is difficult to cause a change in angular velocity for the same torque. The moment of inertia is measured in kg/m2. For two objects with constant density and shape, the moment of inertia is greater for the object with the greater mass; for two objects with the same density, shape, and mass, the moment of inertia is greater for the object with more parts farther from the axis of rotation. In addition, even for the same object, the moment of inertia varies depending on the selected axis of rotation.
The equation for the moment of inertia from dimensional analysis is:

where m is the mass, r is the distance from the center of a mass to the axis of rotation or the length that characterizes an object such as the radius, and k is the inertia constant that changes depending on the shape of the object.
The inertia constant is a value that changes according to the arrangement of mass inside an object. For example, the rotational inertia can change depending on the position of the axis that becomes the reference (Figure 3). When k=1, the object is a very thin cylinder and r is the radius of the cylinder. When k=2/5, the object is a solid sphere. When k=1/2, the object is a solid cylinder or disk.
 |
Figure 3 Rotational inertia. |
With a large amount of inertia, the kinetic energy of the inertial movement is continuously transmitted to the surgeon’s dominant hand holding the handpiece, which inevitably increases hand fatigue and reduces accuracy with time. Also, in fast oscillatory movement, it is important that the axis of oscillatory movement is steady. If the tip oscillates with a high speed and high torque or the device is mechanically designed to have some deviation in its axis, the resulting trembling in addition to the inertia energy of oscillation is transmitted to the surgeon’s fingertips, intensifying fatigue in the hands, reducing accuracy, and possibly preventing delicate manipulations. Therefore, with the new device, acceleration is adjusted through precise digital control function to reduce vibration/rebound. First, the device is set up to subdivide the pulse output per rotation into a very large number of about 1000 or more. Second, the electricity supply is controlled so that it gradually increases, which prevents sudden speed changes when the oscillation motion is started. Third, when approaching the target oscillatory arc, the electric supply is supplied in the reverse direction to put a brake on the rotation and achieve a gentle stop of the rotation (Figure 4). The inertia (vibration/rebound) caused by the oscillation motion can be adjusted by modulating the starting section of the brake.
 |
Figure 4 Stable oscillation: delicate intelligent digital control. When approaching the target oscillatory arc, the electric supply is supplied in the reverse direction to achieve a gentle stop of the rotation. |
Vibration
In a rotating FUE punch, vibration can be thought of as oscillation that moves rapidly in both directions with a very small arc. Its purpose is mainly to separate rather than cut the target graft in the subcutaneous layer from the perifollicular tissue. Therefore, in multiphasic movement, this mode is usually applied at the end of the oscillation or rotation modes. It is helpful in fibrotic skin with tethering, very long grafts, or tough, rubbery skin.
There have been other instruments with a multiphasic movement function. Usually, the rotation can be set to rotate to only one side, unlike this device which can rotate either clockwise or counter-clockwise as desired. Due to the nature of the multiphasic FUE device, which must perform 2–3 different motions within 0.1 to 0.4~0.5 seconds, oscillation is very fast and strong, either resulting in higher rotational inertia (vibration/rebound) caused by oscillation motion or too slow oscillation speed. However, the big difference in this new device is that it is capable of fast and stable oscillation. (Supplementary Video 2)
Ergonomic Handpiece Design
The existing handpieces are generally round. This novel device was designed for an easy grip with a streamlined shape and minimized size through 3D scan modeling after consideration of various postures, gripping methods, and hand sizes for each operator (Figure 5). As a result, the fatigue in the operator’s hand is expected to be reduced.
 |
Figure 5 Existing round-shaped handpiece versus the new streamlined ergonomic handpiece. |
Fingertip Touch Sensor Switch
Most motorized FUE punches have foot pedals. This novel device is uniquely equipped with a fingertip touch sensor switch (Figure 6). With the fingertip touch sensor, the starting point of the motion can be freely adjusted with fine differences by the surgeon’s cognitive function. When one punch is finished and the device is moving to the next target, the punch tip is centered on the targeted graft and scores around the hair follicle. At this time, the punch can be operated by pressing the switch in advance just before touching the scalp over the targeted graft or by simultaneously pressing the skin with slight pressure for activation.
 |
Figure 6 Fingertip touch sensor switch. |
If the dissection starts after pressing the skin with a certain force, the pressure is released as cutting commences, and the hair follicles pop up. Such fine and delicate manipulation or control is possible through experience and may vary with the punching angle, hair thickness, and skin type, and may be more feasible with a delicate finger switch than with a foot pedal.
When using the fingertip switch, the long button in the form of a lever at the tip of the handpiece is pressed with one of the surgeon’s fingers to start a preset programmed motion. It is very convenient to operate the punch without a foot pedal, as this removes the need to look for the pedal during surgery, which is especially useful when the patient is in sitting position and the surgeon is standing behind the patient. When using a traditional foot pedal, the surgeon must stand on one leg during harvesting, putting strain on the spine, hip, knee, and ankle (Figure 7).11
 |
Figure 7 Comparison of surgeon’s posture when using a foot pedal versus the fingertip touch sensor. With the traditional foot pedal switch (A; left), the surgeon stands on one foot inducing a non-ergonomic and uncomfortable posture. Using the fingertip touch sensor (B; right) disperses the surgeon’s weight and provides an ergonomic and more comfortable posture. Adapted from. Park JH, Kim NR, Manonukul K. Ergonomics in follicular unit excision surgery. J Cosmet Dermatol. 2022;21:2146–2152. © 2021 The Authors. Journal of Cosmetic Dermatology published by Wiley Periodicals LLC. Creative Commons.11 |
Each surgeon also has a different hand size, way of holding the handpiece, surgical style, and operative position (Figure 8). To accommodate these diverse needs, the device has a 29-mm-long lever-type switch; a light touch on any part of the switch activates the device. The action of releasing the finger and pressing it again for every harvest leads to severe fatigue of the finger muscles, and the punching motion may become unstable as the action of the finger increases.
 |
Figure 8 Various ways of holding the handpiece. The 29-mm-long fingertip touch sensor switch accommodates various holding methods. |
These problems have been solved by the creation of a switch with a slightly convex arch shape and elasticity. These two properties mean that the finger switch returns to its starting position by itself due to elasticity and restoring force, even if it is pressed lightly (Figure 6). However, if finger fatigue occurs, the foot pedal can be used instead. Moreover, the sequence and interval of the device can be set up in advance, enabling it to be used without the finger switch.
Totally Computerized Digital Control Punching Program by Sequence and Interval Program Setting
The surgeon becomes used to punching after repeating the same motion hundreds to thousands of times. If the motion is multiphasic, the parameters composed of a combination of rotation, oscillation, and vibration are performed in the sequence preset by computer programming; this process is hereafter referred to as one sequence.
It is possible to combine the desired parameters by mixing the following four modes: clockwise rotation, counterclockwise rotation, oscillation, and vibration. Any combination is possible as desired by the surgeon. For oscillation, the arc can be set up to 720 degrees in units of 30 degrees. The order of each mode is also very conveniently interchangeable by simply dragging the segment with the finger on the touchscreen.
One circular excision generally takes a short sequence of about 200–600 ms but can be set in various ways and lengths according to the needs of the operator. After one sequence is finished (ie, the target graft is scored and completely dissected), the surgeon moves the punch to the next target. After the punch is placed above the next target graft, the surgeon presses the foot pedal or fingertip touch sensor to execute another sequence. In other words, a certain period of repetition creates a certain rhythm and an interval of a certain degree of similarity between excisions. This interval can be set in advance in units of 100 ms. The preset sequence and interval repeat indefinitely as the surgeon turns on the interval function on the screen and presses the touch sensor once; this process is stopped when the sensor is pressed again. This novel function not only saves the effort of stepping on the foot pedal or pressing on the finger switch thousands of times during the surgery, but also allows the surgeon to completely focus on the punching itself. The interval function can be turned on or off to suit the surgeon’s preference or needs.
Counting the Number of Punches
Each time a sequence is repeated (ie, one graft is scored), the number of punches is accurately counted. An alarm sounds when the target number is reached. This is very useful in actual clinical practice. When using other FUE devices, the surgeon must continuously check the punch count on the screen until the target number is reached. However, the alarm function of the novel device provides convenience and efficiency.
Weight and Center of Gravity of the FUE Handpiece
The FUE handpiece must be as light as possible so that it is easy to handle and the muscles of the surgeon’s hands and arms are less fatigued, even after a long operation. The novel device is operated by downloading the application to the tablet PC and communicating with the main body via Bluetooth. To reduce the weight of the handpiece, the main body is installed in a separately connected box and placed on the floor of the operating room or on a surgical cart. The handpiece receives the operation command signal through a Y-shaped line, with one line connected to the main body and the other connected to power. The novel FUE handpiece only weighs 95 g, making it the lightest among existing FUE devices. Moreover, as the surgeon mainly grips the anterior part of the handpiece, the center of gravity is toward the front, making the device feel lighter than its actual weight (Figure 9).
 |
Figure 9 Center of gravity is toward the front of handpiece so that it feels lighter than its actual weight. The center of gravity resides in the anterior part of the handpiece, where the surgeon mostly grips during surgery, making it feel lighter than its actual weight. |
Bluetooth-Based FUE Machine
Most motorized FUE machines are driven by a hardware control body. However, in the new FUE device, the application is downloaded from the tablet PC and the handpiece is controlled by Bluetooth. This allows for much more sophisticated and complex software programs and can be easily modified. The addition of a new function does not necessitate another purchase, as the upgraded version can simply be distributed and downloaded.
360-Degree Surround/Ultrathin Foot Pedal
Most conventional foot pedals have a rectangular structure that is stepped on from one side. However, the novel FUE device is specially designed to be 360-degree responsive and is activated by pressing it from any angle by checking its position with the toe. Furthermore, it is specialized in hair transplant surgery to be very thin to prevent excessive flexion of the surgeon’s ankle.
Other Convenient and Innovative Functions on the User Interphase
The novel FUE device has many innovative and diverse user-friendly features. As mentioned above, an alarm sounds when the target number of follicles is reached. In addition, with a simple touch, the surgeon can request various modes of the punching motion, namely rotation, oscillation, and vibration. The power, oscillating arc, sequence, and duration are all easily set and manipulated. When various punching sequences are used, the surgeon can easily view the applied sequences after the surgery. A memory function provides further convenience as it stores up to five frequently used sequence parameters for easy application (Figure 10).
 |
Figure 10 User interface with various convenient and innovative functions. ①: time and date, ②: hand/foot switch button, ③: interval setting, ④: memory, ⑤: total number of punches, ⑥: total operation time, ⑦: target number of grafts, ⑧: alternative timer, ⑨: sequence, ⑩: power and oscillating arc setting, ⑪: selection button for multiphasic sequence, ⑫: detailed information of all the sequences used, ⑬: targeted time to finish the surgery. |
Long Hair FUE
Preview long hair transplantation was first proposed in 2006.18 Hair follicles with long hair shafts were harvested by Follicular unit strip surgery. In 2016, long hair FUE was first reported with the advantages of donor preview.19 Park et al emphasized the curl preview effect when transplanting long hair,20 and developed an open window punch for long hair FUE and acquired a patent. This long hair FUE punch is designed to have one or multiple narrow open slots at the distal end. Other researchers have also introduced long hair FUE methods.21,22
The principle of long hair FUE is to harvest hair follicles with the hair shaft intact while preventing the surrounding hair from being caught by the rotating punch tip (Figure 11), which requires oscillation. Initially, the open punch returns to its starting position. However once oscillation starts, hair is automatically encased in the punch lumen without necessarily inserting hair into the slot before every graft scoring. This enables a much simpler and more rapid surgery.
 |
Figure 11 Extracted long hair FUE grafts. |
Conclusion
Conventional FUE devices have been mainly focused on the effort to reduce follicular injury. Now it is time to kill two birds with one stone by acquiring best quality grafts by reducing follicular injury at the same time improving the ergonomic environment for the surgeons. The novel FUE device is in line with such an effort. It helps surgeons operate in an optimal surgical environment with less fatigue. Comprehension and utilization of the various functions of the novel device in clinical practice will allow surgeons to produce excellent surgical results.
Data Sharing Statement
In addition to photographic evidence showing interval changes that appear in the manuscript, complete medical records of the presented cases are stored in the treating clinic, in line with the standard of care.
Ethics and Consent
All procedures in studies involving human participants were performed in accordance with the Declaration of Helsinki (as revised in 2013). All patients provided informed consent for the case details and images to be published in this report.
Acknowledgments
We thank Kelly Zammit, BVSc, from Edanz for editing a draft of this manuscript.
Funding
There is no funding to report.
Disclosure
JH Park has patents and ownership interest with Seson Medical Company. The author reports no other conflicts of interest in this work.
References
1. Rassman WR, Bernstein RM, McClellan R, Jones R, Worton E, Uyttendaele H. Follicular unit extraction: minimally invasive surgery for hair transplantation. Dermatol Surg. 2002;28(8):720–728. doi:10.1046/j.1524-4725.2002.01320.x
2. Kim YS, Na YC, Park JH. Comparison of postoperative pain according to the harvesting method used in hair restorative surgery. Arch Plast Surg. 2019;46(03):241–247. doi:10.5999/aps.2018.00843
3. Garg AK, Garg S. Donor harvesting: follicular unit excision. J Cutan Aesthet Surg. 2018;11(4):195–201. doi:10.4103/JCAS.JCAS_123_18
4. Park JH, You SH. Various types of minor trauma to hair follicles during follicular unit extraction for hair transplantation. Plast Reconstr Surg Glob Open. 2017;5(3):e1260. doi:10.1097/GOX.0000000000001260
5. Kwack MH, Kim MK, You SH, Kim N, Park JH. Comparative graft survival study of follicular unit excision grafts with or without minor injury. Dermatol Surg. 2021;47(5):e191–e194. doi:10.1097/DSS.0000000000002878
6. Gan YY, Du LJ, Hong WJ, Hu ZQ, Miao Y. Theoretical basis and clinical practice for FUE megasession hair transplantation in the treatment of large area androgenic alopecia. J Cosmet Dermatol. 2021;20(1):210–217. doi:10.1111/jocd.13432
7. Park JH, You SH, Kim NR. Nonshaven follicular unit extraction: personal experience. Ann Plast Surg. 2019;82(3):262–268. doi:10.1097/SAP.0000000000001679
8. Park JH, You SH, Kim NR, Ho YH. Long hair follicular unit excision: personal experience. Int J Dermatol. 2021;60(10):1288–1295. doi:10.1111/ijd.15648
9. Ahmad M, Mohmand MH. Effect of surgeon’s workload on rate of transection during follicular unit excision/extraction (FUE). J Cosmet Dermatol. 2020;19(3):720–724. doi:10.1111/jocd.13078
10. Williams KL, Gupta AK, Schultz H. Ergonomics in hair restoration surgeons. J Cosmet Dermatol. 2016;15(1):66–71. doi:10.1111/jocd.12188
11. Park JH, Kim NR, Manonukul K. Ergonomics in follicular unit excision surgery. J Cosmet Dermatol. 2022;21(5):2146–2152. doi:10.1111/jocd.14376
12. Tolhurst DE, Carstens MH, Greco RJ, Hurwitz DJ. The surgical anatomy of the scalp. Plast Reconstr Surg. 1991;87:603–612. doi:10.1097/00006534-199104000-00001
13. Park JH. Interfollicular unit distance variation by differences in depth. Dermatol Surg. 2019;45(12):1742–1745. doi:10.1097/DSS.0000000000001770
14. Gupta AK, Love RP, Mohebi P, Trivellini R. Advances in hair transplantation technology: multiphasic device for follicular unit excision. Skinmed. 2019;17(4):241–246.
15. Rose PT, Nusbaum B. Robotic hair restoration. Dermatol Clin. 2014;32(1):97–107. doi:10.1016/j.det.2013.09.008
16. Garg A, Garg S. Overview of follicular extraction. Indian J Plast Surg. 2021;54(04):456–462. doi:10.1055/s-0041-1739244
17. Becker HS. The power of inertia. Qual Sociol. 1995;18(3):301–309. doi:10.1007/BF02393344
18. Pitchon M. Preview long-hair follicular unit transplantation: an immediate temporary vision of the best possible final result. Hair Transpl Forum Int. 2006;16(4):113–119. doi:10.33589/16.4.0113
19. Boaventura O. Long hair FUE and the donor area preview. Hair Transpl Forum Int. 2016;26(5):200–202. doi:10.33589/26.5.0200
20. Park JH, Kim NR, Manonukul K. Eyebrow transplantation using long hair follicular unit excision technique. Plast Reconstr Surg Glob Open. 2021;9(5):e3598. doi:10.1097/GOX.0000000000003598
21. Umar S, Lohlun B, Ogozuglu T, Carter MJ. A novel follicular unit excision device for all-purpose hair graft harvesting. Clin Cosmet Investig Dermatol. 2021;14:1657–1674. doi:10.2147/CCID.S333353
22. Trivellini R, Perez-Meza D, Renaud HJ, Gupta AK. Preview long hair follicular unit excision: an up-and-coming technique. J Cosmet Dermatol. 2021;20(11):3422–3426. doi:10.1111/jocd.14026
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.