Back to Journals » Nursing: Research and Reviews » Volume 12
Norwegian Nurses’ Attitudes Toward Assisted Dying: A Cross-Sectional Study
Authors Hol H ![]() , Vatne S, Orøy A, Rokstad AMM
, Vatne S, Orøy A, Rokstad AMM ![]() , Opdal Ø
, Opdal Ø
Received 5 March 2022
Accepted for publication 17 June 2022
Published 7 July 2022 Volume 2022:12 Pages 101—109
DOI https://doi.org/10.2147/NRR.S363670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Natasha Hodgkinson
Hege Hol,1 Solfrid Vatne,1 Aud Orøy,1 Anne Marie Mork Rokstad,1,2 Øivind Opdal3
1Faculty of Health Science and Social Care, Molde University College, Molde, Norway; 2Norwegian National Centre for Ageing and Health, Vestfold Hospital Trust, Tønsberg, Norway; 3Faculty of Business Administration and Social Sciences, Molde University College, Molde, Norway
Correspondence: Hege Hol, Faculty of Health Science and Social Care, Molde University College, Molde, Norway, Email [email protected]
Purpose: The purpose was to investigate: (a) Norwegian nurses’ attitudes toward assisted dying, and (b) how much nurses receive requests from terminally ill patients for help in dying.
Participants and Methods: A quantitative explorative study was conducted using a web-based cross-sectional survey to collect data. The survey was sent to a total of 734 eligible participants, and 205 clinical nurses participated by completing the survey. Data were analyzed using bivariate statistics and multivariate ordinal regression.
Results: The study revealed that 56% of the participating nurses agreed with the statement that physician-assisted suicide should be allowed, and 48% supported legalization of euthanasia. Nurses in pulmonary wards were more positive about the legalization of physician-assisted suicide (OR = 2.98, CI = 1.34– 6.66, p = 0.008) and euthanasia (OR = 3.51, CI = 1.58– 7.81, p = 0.002) than nurses in oncological wards. Nurses over 30 years old held more negative attitudes about physician-assisted suicide than younger nurses (OR = 0.16, CI = 0.07– 0.39, p < 0.001; and OR = 0.45, CI = 0.21– 0.96, p = 0.038), and nurses with postgraduate education held more negative attitudes than nurses with a bachelor’s degree (OR = 0.46, CI = 0.24– 0.88, p = 0.019). A total of 118 nurses (58%) had received at least one request about assisted dying in their clinical practice.
Conclusion: Our results provide insight into clinical nurses’ attitudes toward assisted dying. Their attitudes were influenced by their age, education, and practice in different wards. Support for legalization of assisted dying is higher in the general Norwegian population than among nurses and receiving requests for assisted dying is not unusual for clinical nurses.
Keywords: euthanasia, physician-assisted suicide, nursing, web-based survey
Introduction
Assisted dying is a term that includes both physician-assisted suicide and euthanasia.1 These definitions correspond to the Dutch definitions1 and have been used in previous Norwegian studies.2,3 Physician-assisted suicide is conducted by “a physician who intentionally helps a person to commit suicide by providing drugs for self-administration, at that person`s voluntary and competent request.”2 Euthanasia is defined as a “physician intentionally killing a person by injecting drugs, at that person`s voluntary and competent request.”2
The practice of assisted dying is illegal in Norway and the other Scandinavian countries, in contrast to several countries like Netherlands, Belgium, Luxembourg, Canada, and the Australian states Victoria and Western Australia, where assisted dying is legalized.4 Today, the subject has not yet reached the political agenda in Norway;5 debates and research about assisted dying mostly involve physicians, lawyers, psychologists, and philosophers. The Nordic Nursing Association (which includes Denmark, Sweden, the Faroe Islands, and Norway) stated that they were against physician-assisted suicide and euthanasia in a 2009 press release.6 Since then, the Norwegian Nursing Association has not expressed an opinion publicly; however, the ethical guidelines for Norwegian nurses include statements that nurses do not contribute to euthanasia and do not assist in a patient’s suicide,7 and the Norwegian Medical Association supports this opinion.3 In public discussions about assisted dying, physicians are prominent, and Norwegian nurses take little part.3
Several international studies have investigated nurses’ attitudes toward assisted dying in different contexts and have found that their opinions were influenced by their age, religion, culture, field of nursing specialty, expectations from society, work across professional boundaries, and collaboration with physicians.8 A study from Finland, where assisted dying is illegal, reported that 82% of the 1003 participating nurses agreed that a person has the right to decide their own death;9 furthermore, 77% personally considered a euthanasia request in certain situations,9 compared to 48% of 249 participants in a study by Freeman et al with Canadian nurses who provided medical assistance in dying in hospice care settings.10 In an Australian survey of 1218 participants, 78% of nurses in critical care were more willing to support euthanasia for incurable patients if it was legal, compared to 58% in aged care and 33% in palliative care.11 In France, 65% of 602 district nurses favored legalizing euthanasia.12 It seems that frequent contact with dying patients, as well as increased knowledge and experience in palliative care, strengthens nurses’ critical attitudes toward euthanasia and leads them to be less supportive of euthanasia.9,12,13 However, in the study by Freeman et al, 75% of 249 palliative care nurses supported an individual’s right to decide their own death.10 Nurses’ religiosity has been a strong indicator of negative attitudes toward and disagreement with the legalization of assisted dying;13–16 however, a study of nurses in Denmark and Sweden who viewed themselves as religious reported that they had a positive attitude toward euthanasia.17 Previous studies have also indicated that gender plays an important role, as men were more in favor of euthanasia then women.8,9,12 Furthermore, several studies found that younger nurses with less clinical experience were more positive in their attitudes toward assisted dying.9,10,12,15
Several studies have documented nurses in clinical settings receiving requests for assisted dying from patients,8,16,18–21 but few studies—all conducted in the 1990s—reported the numbers of nurses receiving such requests.22 Matzo and Emanual reported that 30% of 441 oncological nurses had received at least one request for physician-assisted suicide and 25% for euthanasia.22 In a study by Asch, 17% of 1139 critical care nurses had received requests from patients or family members to perform physician-assisted suicide or euthanasia.23 More recent research from Canada, where assisted dying is legal, has shown that nurses commonly receive such requests.21
According to international research, then, it seems that nurses are somewhat willing to support euthanasia, although cultural context, legal status, and religion influence their attitudes. Furthermore, experienced nurses working with terminally ill patients seem to vary more in their attitudes toward assisted dying.24
In 2015, the Norwegian Bioethical Survey (NOBAS) conducted a population survey with a sample of 22,660 Norwegians that included questions about their attitudes toward assisted dying.2 The bivariate analyses in the study showed that the majority of the participants agreed with legalizing assisted dying through physician-assisted suicide (73%, N = 2230) and euthanasia (66%, N = 2027). Furthermore, the participants disagreed slightly less with legalized physician-assisted suicide (20%, N = 598) than with euthanasia (24%, N = 706).2
Little is known about how assisted dying affects nurses working in countries where assisted dying is illegal, such as Norway. Since the Norwegian population has a more liberal view than what is reflected in politics and the legislation,2 it is important to know about nurses’ clinical experiences in order to bring their views into professional and public debates. Thus, the purpose of this study was to investigate Norwegian clinical nurses’ attitudes toward assisted dying, by addressing the following research questions: a) What are the attitudes of nurses toward physician-assisted suicide and euthanasia; and b) how much do nurses receive requests for help in dying from terminally ill patients?
Material and Methods
Research Design
This study uses a descriptive cross-sectional survey design.25
Setting and Sample
To get an overview of nurses’ attitudes across Norway, we invited six university hospitals and home care nursing units from six municipalities, covering all health regions of Norway, to participate in this study. Two university hospitals and five home care districts declined to take part, so the sample was recruited from four hospitals and one home care district. The respondents working in hospitals were recruited from two oncological, three pulmonary, one neurological, and two palliative care wards. Inclusion criteria were being a registered nurse, performing bedside patient care, and being proficient in the Norwegian language. Nurses working in leadership positions or administration were excluded.
A staff member at each ward distributed the informational letter by e-mail to 734 eligible participants. We asked the participants to complete and return the questionnaire within two weeks using the computers in the ward. A total of 205 (28%) nurses with a bachelor’s degree participated by returning the questionnaire. The data collection period lasted from October 2017 through February 2018.
Data Collection
Using Questback, we designed an electronic questionnaire with 15 items26,27 on a secure online platform (see Appendix 1). Sociodemographic characteristics such as gender, age, education (bachelor and postgraduate education in nursing), and spirituality (including religious beliefs) were included. Additionally, information about the nurses’ workplace and type of department were collected. The questionnaire also included eight questions from the NOBAS, a validated questionnaire measuring attitudes toward assisted dying.28 The respondents were asked to rate their opinions on a 5-point Likert scale, ranging from 1 = Strongly disagree to 5 = Strongly agree. Finally, we designed a question to learn whether the participants had received requests for assisted dying from patients, and if so, how many times had they received such requests. Response time for the survey was approximately 10 minutes.
Statistical Analysis
IBM SPSS Statistics version 26 and Stata 16 for data analysis were used for statistical analyses.26,29 The data file was screened for missing data. Given that there were very few missing values, all questionnaires were included in the analysis. The analyses included bivariate statistical procedures (crosstabs, chi-square statistics). A multivariable ordinal regression approach was performed in two steps: first, calculating unadjusted effect estimates for the independent variables; and second, multivariable ordinal regression giving adjusted effect estimates. Attitudes toward physician-assisted suicide and euthanasia were used as dependent variables. The following independent variables were used in the analyses: sociodemographic variables such as gender, age, department, and religion; and number of requests from patients who had asked for assisted dying. Statistical significance levels of 0.05 were used, and a 95% confidence interval (CI) was calculated. Items 9–14 were analyzed by Cronbach’s Alpha =0.748.
Ethical Considerations
The study was approved by the Norwegian Regional Committee for Medical Research Ethics Central Norway (reference number 2017/1131) and the Norwegian Center for Research Data (NSD) in 2017 (reference number 997338), and it was conducted in accordance with the Declaration of Helsinki. Due to the sensitive nature of this research topic, we sent the questionnaire to the ethics committees of the university hospitals and the home care districts where the study was conducted, from whom we also obtained approval. We enclosed a declaration of consent in the questionnaire. The questionnaires were fully anonymous and the participants gave their consent to participate by returning the completed questionnaire. To avoid misunderstandings, the information letter and questionnaire included clear definitions and examples of physician-assisted suicide and euthanasia.
Results
As shown in Table 1, 91% (n = 182) of respondents were female, 38% (n = 78) were 20–29 years old, and 42% (n = 85) had postgraduate education. Fifty-eight percent (n = 118) of the respondents had at least once received a request from patients for help with assisted dying. Nurses working in pulmonary wards (70%, n = 37) and palliative teams (88%, n = 14) received significantly more requests than nurses working in the other departments (significance p = 0.001).
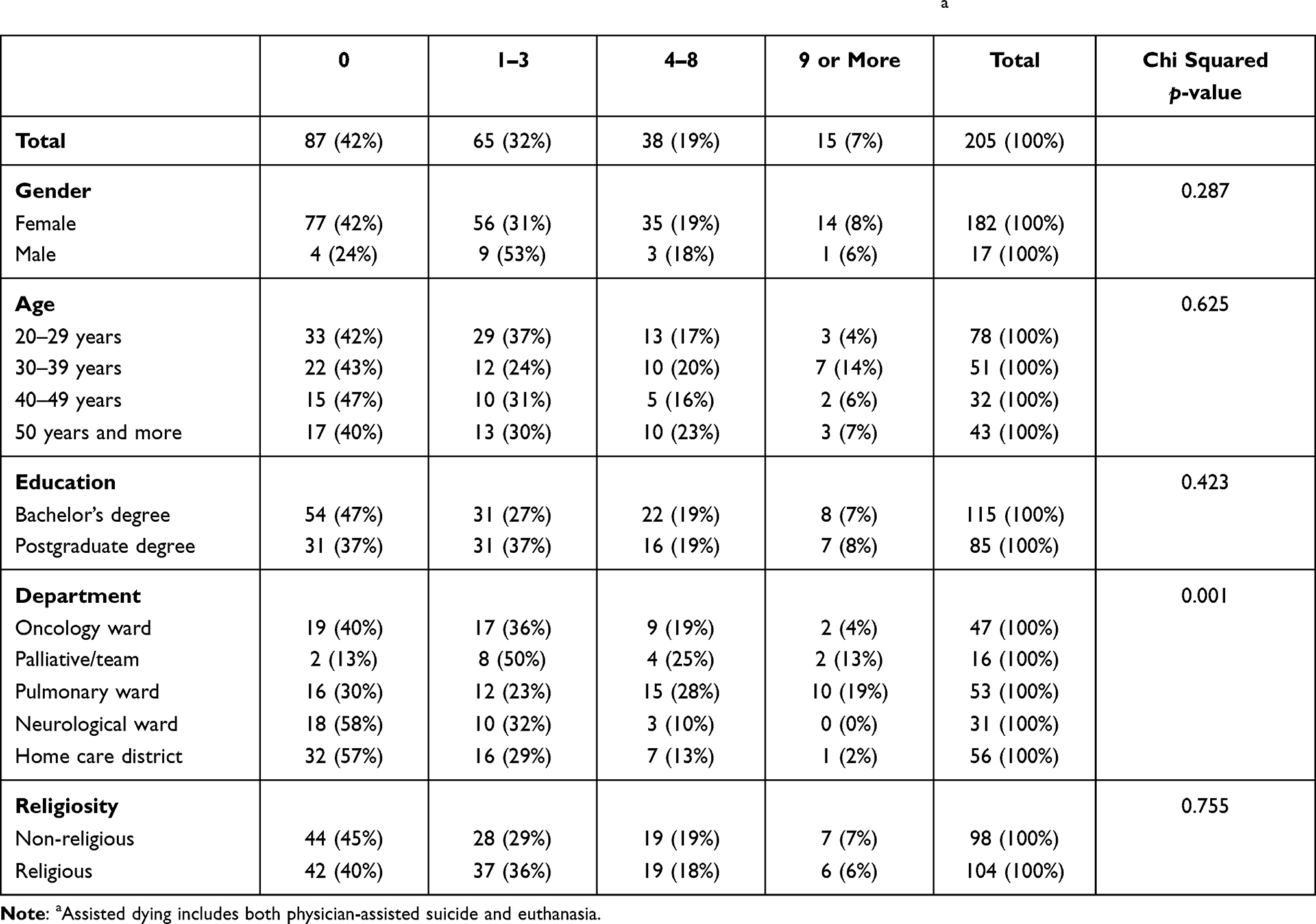 |
Table 1 How Many Times a Request Was Received from a Patient Requesting Assisted Dyinga |
The nurses’ attitudes toward legalization of physician-assisted suicide and euthanasia are presented in Table 2. The proportion of the participants who “somewhat” or “strongly” agreed with legalizing physician-assisted suicide (56% n=114) and euthanasia (48% n = 98) was larger than the proportion who “somewhat” or “strongly” disagreed (36%, n = 72, and 41%, n = 84, respectively).
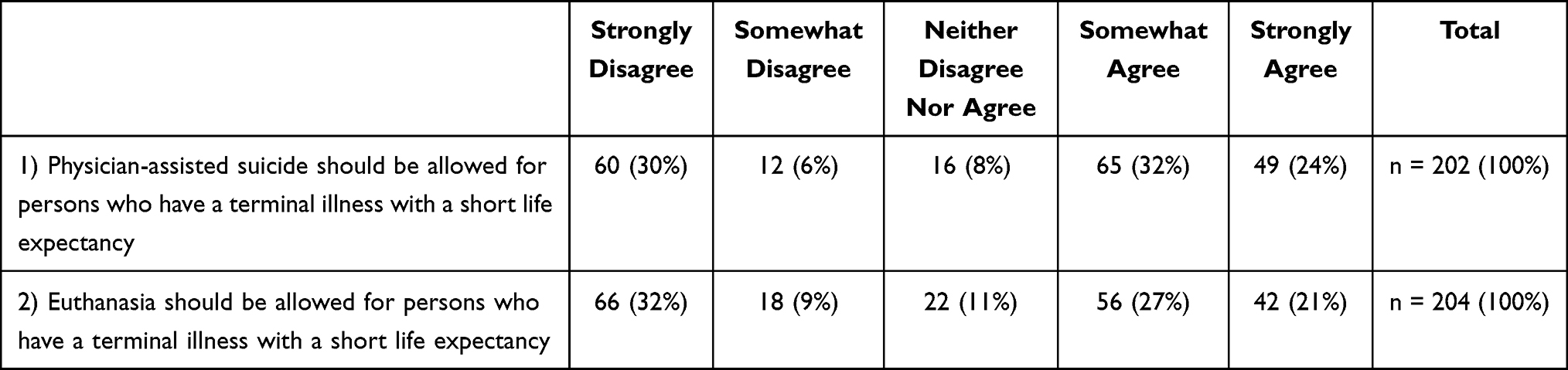 |
Table 2 Nurses’ Attitudes Toward Legalization of Physician-Assisted Suicide and Euthanasia |
The results of the multivariate ordinal regression analysis are shown in Table 3. In terms of age, there was a significant and definite gradient toward lower odds of higher levels of agreement with physician-assisted suicide: for the oldest age group (above 50 years), with OR = 0.16 (95% CI, 0.07–0.39, p <0.001), the odds for higher levels of agreement were 84% lower compared with those in the youngest age group (20–29 years). Having a postgraduate education in nursing, with OR = 0.46 (95% CI, 0.24–0.88, p = 0.019), reduced the odds of a higher level of agreement with physician-assisted suicide by 54% compared to those with a bachelor’s degree. For the variable of departments, nurses on the pulmonary wards showed OR = 2.98 (95% CI, 1.34–6.66, p = 0.008); the odds of a higher level of agreement with physician-assisted suicide was 198% higher for these nurses compared to those working on oncology wards. The variable of gender shows no significant results. In the unadjusted analysis, non-religious respondents were more likely to agree (p=0.001); however, in the multivariate (adjusted) regression analysis, religiosity was no longer significant. The variable of experience in receiving a request was not statistically significant in the bivariate analysis (unadjusted), with OR = 0.92 (95% CI = 0.55–1.52, p = 0.737), and was therefore excluded from the multivariable analysis (adjusted).
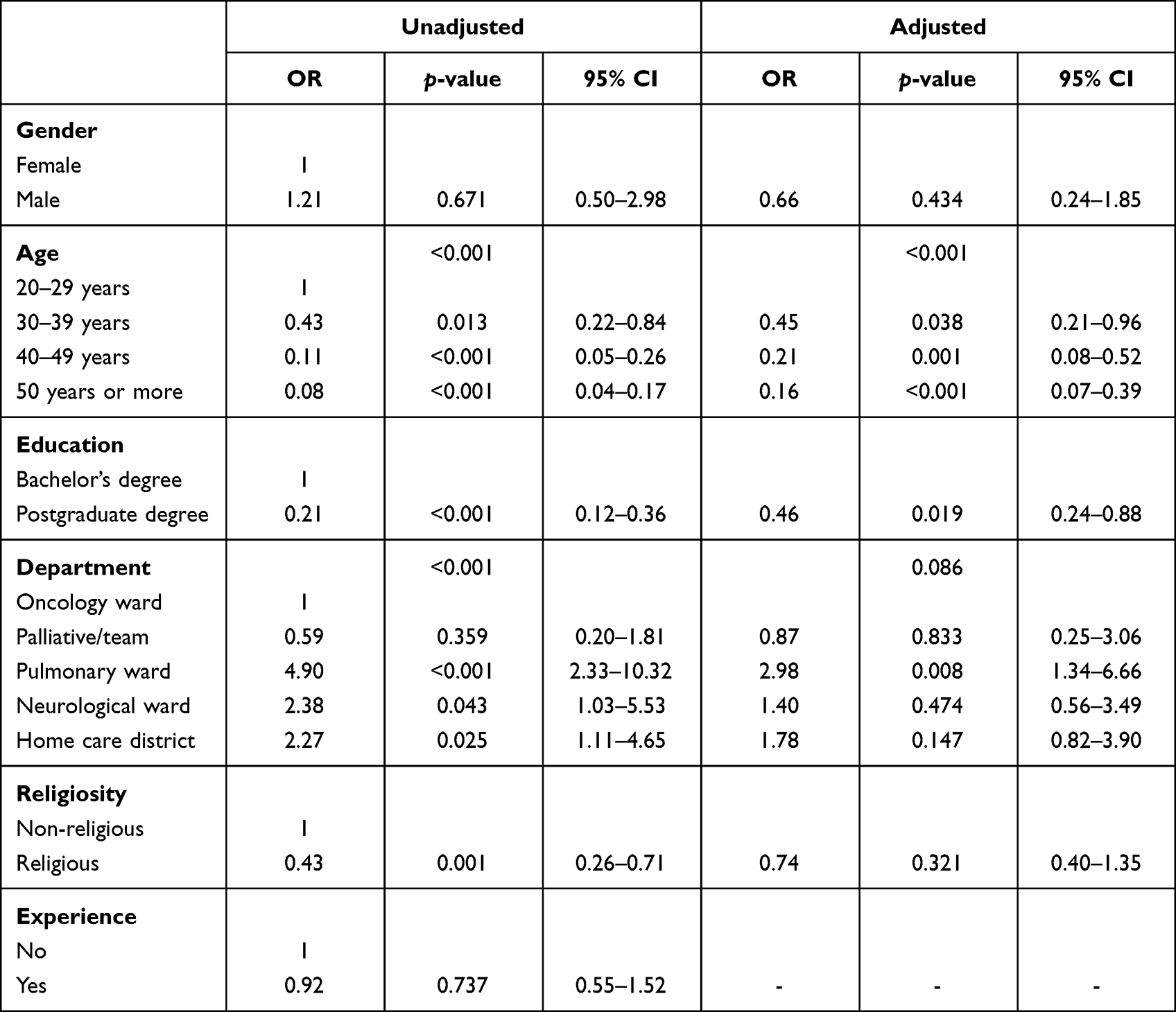 |
Table 3 Multivariable Ordinal Regression: “Physician-Assisted Suicide Should Be Allowed for Persons Who Have a Terminal Illness with a Short Life Expectancy” |
The results of the ordinal multivariate regression in attitudes toward euthanasia are shown in Table 4. The results are largely similar to the results of attitudes toward physician-assisted suicide (Table 3); however, some differences were revealed. Nurses in pulmonary wards show higher odds for agreement with euthanasia than physician-assisted suicide, with OR = 3.51 (95% CI, 1.58–7.81, p = 0.002); the odds of a higher degree of agreement with euthanasia are 251% higher for respondents working in pulmonary wards compared to nurses working in oncology wards. Having a postgraduate education led to lower odds of agreement with euthanasia than with physician-assisted suicide, with OR = 0.31 (95% CI, 0.16–0.60, p <0.001). The odds for agreement with euthanasia were thus 69% lower.
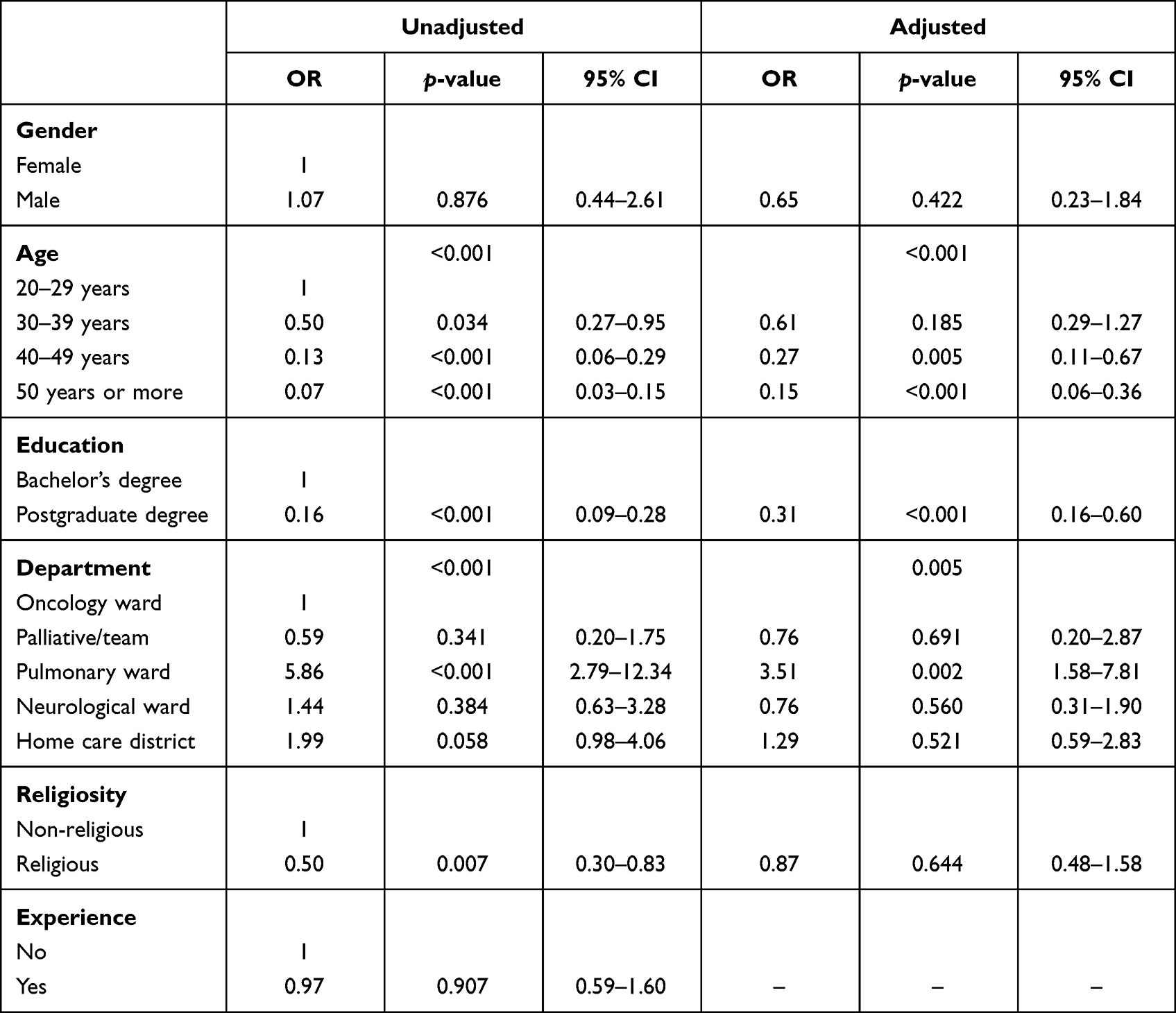 |
Table 4 Multivariable Ordinal Regression: “Euthanasia Should Be Allowed for Persons Who Have a Terminally Illness with a Short Life Expectancy” |
Discussion
In this study, the purpose was to investigate Norwegian nurses’ attitudes toward assisted dying, and how much they have received requests from terminally ill patients for help in dying.
The Influence of Context
The study revealed that more than 56% of the participating nurses agreed with the statement that physician-assisted suicide should be allowed for persons who have a terminal illness with a short life expectancy and 48% supported legalization of euthanasia, even though assisted dying is illegal in Norway. However, compared with the findings reported in the NOBAS study, the participants hold a more restrictive attitude toward assisted dying than the general Norwegian population.2 According to the NOBAS study, the population has been growing to favor assisted dying, an attitude also appearing in countries with a legal framework for assisted dying.2,17,30 Literature in the international context argues that people seem to value their right to autonomy and their freedom to choose their own death in cases of physical deterioration, depression, weariness with life, and loss of dignity.9 This might be seen in the high number of nurses in this study who received requests for assisted dying from terminally ill patients. The number of requests for assisted dying varied according to the context in which the nurses worked: a higher proportion of nurses working in the pulmonary and palliative wards received requests than those working in home care. These results might be explained by the limited number of terminally ill patients who die in private homes, according to public reports.31,32 A study among Canadian palliative care nurses, where nurse practitioners may perform assisted dying, revealed that 76% received such requests.10
As assisted dying is not legal in Norway, we have no knowledge of whether nurses are involved in assisted dying. A study by Gaasø et al reported that a majority of Norwegian physicians were opposed to assisted dying; however, their study also indicated that the proportion in favor of legalization has increased since 1993.3 Førde et al reported in a survey that physicians seem to have a more liberal end-of-life practice and reported that six physicians had hastened death within the last 12 months; all of them were younger than 50 years.33 This may give an idea of the scope of clandestine assisted dying in Norway, indicating that it is rare among Norwegian physicians.33
Experience and Education
Nurses’ attitudes toward legalization are well-documented in international studies, with some variation in the findings.8 Previous research supports our findings, revealing that younger nurses more often agree with the legalization of assisted dying than older nurses. Additionally, nurses with more work experience were less willing to participate in decision-making processes concerning euthanasia.30 One explanation given is that younger nurses are raised in a more liberal environment and that they have less experience with dying patients and illness.15,30
We find it interesting that nurses with a postgraduate education were less supportive of physician-assisted suicide and euthanasia. Such findings are also reported in studies from other countries, including where assisted dying is legal.10,30 This might indicate a basic attitude among experienced nurses, especially those with postgraduate education in palliative care, which holds that nurses should not participate in actions that hasten a patient’s death but rather alleviate patients’ suffering as long as they live. However, a new Australian study reports that health professionals with a high level of education had a more positive attitude toward assisted dying.24
Workplace
This study revealed that nurses working in pulmonary wards both got more requests and had more positive attitudes about assisted dying. We found no support in the literature for similar differences in nurses’ attitudes depending on their clinical area. This might be explained by the fact that previous studies investigated only one clinical specialty and made no comparisons between specialties or type of wards.13 In pulmonary wards, nurses meet patients with chronic obstructive pulmonary disease (COPD) and cancer, as well as patients with severe respiratory problems and subsequently high levels of anxiety, which nurses find difficult to relieve. A Norwegian study by Jerpseth et al found that patients with COPD are particularly vulnerable due to their life-threatening illness.34 Nurses may face ethical dilemmas and difficulties in dealing with and alleviating the suffering of these patients and thus may be more inclined to hold liberal attitudes toward assisted dying. Furthermore, our sample of palliative-care and oncology nurses reported similar attitudes toward assisted dying as those reported in other studies9,10—namely, that nurses in these wards more strongly disapproved of assisted dying.30 This may be related to the fact that assisted dying conflicts with the principles of palliative care philosophy, which disapproves of participating in acts that unnaturally hasten death.30
Nurses’ Ethical Dilemma
The nurses participating in our study were less positive about legalizing assisted dying than the Norwegian population in general. This might lead to diverging attitudes and expectations when terminally ill patients meet nurses in practice. A request from a terminally ill patient that is refused by a nurse, in countries where it is illegal to assist dying, might harm the relationship between patient and nurse and have consequences for further terminal care.13 Respecting patient autonomy is an important issue in the euthanasia debate and in healthcare ethics;35 however, the Code of Ethics for Nurses takes the position that nurses should not participate in physician-assisted suicide or euthanasia, because these acts are in direct violation of saving lives.7 Furthermore, the ethics code also point out that suffering should be alleviated. The opposition to legalization of assisted dying in Norway, particularly from the Norwegian Medical Association and the Norwegian Nurse Association, has probably been an important reason for political parties not to raise this issue.3 Gaasø et al argue that without the support of these two key professions and their associations, it might be difficult to envision the implementation of assisted dying in Norway.3
Limitations and Strengths
This study explores Norwegian clinical nurses’ attitudes toward assisted dying and their experience of requests for assisted dying from terminally ill patients. The sample covers participants from all health regions in Norway—specifically four university hospitals and one home care district in a larger city, all central to the care of terminally ill patients. Small hospitals and nursing homes were excluded. Therefore, our study is not representative of the full population of nurses in Norway. This study is not a random sample of nurses, and there is always a risk of bias in study designs that rely on self-reported questionnaires as the source of outcome information. The use of a validity-tested questionnaire (NOBAS), with accepted definitions of assisted dying, is considered a strength.2 Due to the chosen design in this study, it was not possible to examine the study reliability using inter-rater reliability or test-retest reliability, which is relevant in connection with measurement reliability. Finally, the low response rate of 28% needs to be taken into consideration when interpreting the results.
Conclusion
Our results provide an insight into Norwegian clinical nurses’ attitudes toward and experiences with assisted dying, revealing that about half of the participants agreed that euthanasia and physician-assisted suicide should be legalized and that receiving requests for assisted dying is not unusual, especially in pulmonary wards. However, the support for legalization of assisted dying is even higher in the general population. The findings that support for legalized assisted dying is lower among nurses with postgraduate education and palliative-care experience should be taken into consideration when planning the education of future nurses.
Acknowledgments
The authors thank all participants who completed the survey questionnaire, along with the ethics committees and staff at the university hospitals and the home care districts who facilitated this study. They also thank the researchers in the NOBAS study for permission to use their questionnaire. Special thanks to Professor Petter Laake, Molde University College and University of Oslo, and Professor Stål Bjørkly, Molde University College, who made a significant contribution to the statistical design and the multivariate regression analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Molde University College provided PhD funding for Hege Hol (NO971555483VAT).
Disclosure
All authors declare that they have no conflicts of interest in this study.
References
1. Griffiths J, Weyers H, Adams M. Euthanasia and Law in Europe. Bloomsbury Publishing; 2008.
2. Magelssen M, Supphellen M, Nortvedt P, Materstvedt LJ. Attitudes towards assisted dying are influenced by question wording and order: a survey experiment. BMC Med Ethics. 2016;17(1):24. doi:10.1186/s12910-016-0107-3
3. Gaasø OM, Rø KI, Bringedal B, Magelssen M. Doctors’ attitudes to assisted dying. Tidsskr nor Laegeforen. 2019;139(1):31–35. doi:10.4045/tidsskr.18.0391
4. Mroz S, Dierickx S, Deliens L, Cohen J, Chambaere K. Assisted dying around the world: a status quaestionis. Ann Palliat Med. 2021;10(3):3540–3553. doi:10.21037/apm-20-637
5. Kleiven DJ, Hartling O, Ståhle F, Horn MA, Magelssen M. Dødshjelp: livverk, praksis og holdninger i de skandinaviske land [Norwegian]. In: Horn MA, Kleiven DJ, Magelssen M, editors. Dødshjelp i Norden? Etikk, klinikk og politikk. NOASP Cappelen Damm akademisk; 2020:51–73.
6. Press release on euthanasia. The Nordic network; 2009. Available from: https://www.nsf.no/Content/809824/NSF-154464-v1-Pressemelding_om_autanasi.pdf.
7. Norwegian Nurses Organisation. Ethical guidelines for nurses. Available from: https://www.nsf.no/vis-artikkel/2193841/17036/Yrkesetiske-retningslinjer-for-sykepleiere.
8. Vijayalakshmi P, Nagarajaiah Reddy PD, Suresh B, Suresh BM. Indian nurses’ attitudes toward euthanasia: gender differences. Omega. 2018;78(2):143–160. doi:10.1177/0030222816688576
9. Terkamo-Moisio A, Kvist T, Kangasniemi M, Laitila T, Ryynänen O, Pietilä A. Nurses’ attitudes towards euthanasia in conflict with professional ethical guidelines. Nurs Ethics. 2017;24(1):70–86. doi:10.1177/0969733016643861
10. Freeman LA, Pfaff KA, Kopchek L, Liebman J. Investigating palliative care nurse attitudes towards medical assistance in dying: an exploratory cross-sectional study. J Adv Nurs. 2020;76(2):535–545. doi:10.1111/jan.14252
11. Kitchener BA. Nurse characteristics and attitudes to active voluntary euthanasia: a survey in the Australian Capital Territory. J Adv Nurs. 1998;28(1):70–76. doi:10.1046/j.1365-2648.1998.00775.x
12. Bendiane M, Galinier A, Favre R, et al. French district nurses’ opinions towards euthanasia, involvement in end-of-life care and nurse–patient relationship: a national phone survey. J Med Ethics. 2007;33(12):708–711. doi:10.1136/jme.2006.018374
13. Holt J. Nurses’ attitudes to euthanasia: the influence of empirical studies and methodological concerns on nursing practice. Nurs Philos. 2008;9(4):257–272. doi:10.1111/j.1466-769X.2008.00373.x
14. Bendiane M, Bouhnik A, Galinier A, Favre R, Obadia Y, Peretti-Watel P. French hospital nurses’ opinion about euthanasia and physician-assisted suicide: a national phone survey. J Med Ethics. 2009;35(4):238–244. doi:10.1136/jme.2008.025296
15. Berghs M, De Casterle BD, Gastmans C. The complexity of nurses’ attitudes toward euthanasia: a review of the literature. J Med Ethics. 2005;31(8):441–446. doi:10.1136/jme.2004.009092
16. Inghelbrecht E, Bilsen J, Mortier F, Deliens L. The role of nurses in physician-assisted deaths in Belgium. CMAJ. 2010;182(9):905. doi:10.1503/cmaj.091881
17. Cohen J, Van Landeghem P, Carpentier N, Deliens L. Different trends in euthanasia acceptance across Europe: a study of 13 western and 10 central and Eastern European countries, 1981–2008. Eur J Public Health. 2013;23(3):378–380. doi:10.1093/eurpub/cks186
18. De Bal N, Dierckx de Casterlé B, Beer TD, Gastmans C. Involvement of nurses in caring for patients requesting euthanasia in Flanders (Belgium): a qualitative study. Int J Nurs Stud. 2006;43(5):589–599. doi:10.1016/j.ijnurstu.2005.08.003
19. Denier Y, Dierckx de Casterlé B, De Bal N, Gastmans C. “It’s intense, you know”: nurses’ experiences in caring for patients requesting euthanasia. Med Health Care Philos. 2010;13(1):41–48. doi:10.1007/s11019-009-9203-1
20. Elmore J, Wright DK, Paradis M. Nurses’ moral experiences of assisted death: a meta-synthesis of qualitative research. Nurs Ethics. 2018;25(8):955–972. doi:10.1177/0969733016679468
21. Pesut B, Thorne S, Stager ML, et al. Medical assistance in dying: a review of Canadian nursing regulatory documents. Policy Polit Nurs Pract. 2019;20(3):113–130. doi:10.1177/1527154419845407
22. Matzo M, Emanual E. Oncology nurses’ practices of assisted suicide and patient-requested euthanasia. Oncology Nursing Forum. 1997;24:1725–1732.
23. Asch DA. The role of critical care nurses in euthanasia and assisted suicide. N Engl J Med. 1996;334(21):1374–1379. doi:10.1056/NEJM199605233342106
24. O’Connor M, Martin C, Wilmott L, Haywood D, Lawrence BJ, Breen LJ. Australian health professionals’ attitudes toward voluntary assisted dying: a cross-sectional survey. Soc Sci. 2021;10(11):429. doi:10.3390/socsci10110429
25. Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. Sage Publications; 2017.
26. Polit D, Beck C. Nursing Research: Generating and Assessing Evidence for Nursing Practice.
27. Martinussen M, Araï D, Friborg O, et al. Kvantitativ Forskningsmetodologi i Samfunns- og Helsefag [Norwegian]. Fagbokforlaget Vigmostad & Bjørke AS; 2010.
28. Magelssen M, Supphellen M, Nortvedt P NOBAS–Norwegian Bioethics Attitude Survey. Available from: http://bioetikk.no/wp-content/uploads/2018/05/NOBAS-rapport-2015.pdf.
29. Field A. Discovering Statistics Using IBM SPSS Statistics. SAGE Publications; 2018.
30. Terkamo-Moisio A, Gastmans C, Ryynänen OP, Pietila AM. Finnish nurses’ attitudes towards their role in the euthanasia process. Nurs Ethics. 2019;26(3):700–714. doi:10.1177/0969733017720850
31. Institute of Public Health F. D3a: dødsfall etter dødssted og bofylke. Antall dødsfall; 2018. Available from: http://statistikkbank.fhi.no/dar/.
32. Institute of Public Health F. D3b: dødsfall etter dødssted og dødsårsak. Antall dødsfall. 2018; Available from: http://statistikkbank.fhi.no/dar/.
33. Førde R, Aasland OG. Are end-of-life practices in Norway in line with ethics and law? Acta Anaesthesiol Scand. 2014;58(9):1146–1150. doi:10.1111/aas.12384
34. Jerpseth H, Dahl V, Nortvedt P, Halvorsen K. Older patients with late‐stage COPD: their illness experiences and involvement in decision‐making regarding mechanical ventilation and noninvasive ventilation. J Clin Nurs. 2018;27(3–4):582–592. doi:10.1111/jocn.13925
35. Beauchamp TL, Childress JF. Principles of Biomedical Ethics. Oxford University Press; 2001.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.