Back to Journals » Research and Reports in Urology » Volume 18
Normal Reference Values for Testicular Volume in Adult Somali Men: A Retrospective Study
Authors Osman KA ![]() , Maqul AH, Farah AA, Sahal AO, Osman WA
, Maqul AH, Farah AA, Sahal AO, Osman WA ![]()
Received 9 April 2026
Accepted for publication 11 June 2026
Published 15 June 2026 Volume 2026:18 615746
DOI https://doi.org/10.2147/RRU.S615746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Guglielmo Mantica
Khalid Abdukadir Osman,1,2 Abdulfatah Hassan Maqul,2,3 Abdullahi Abdi Farah,2,4 Abdirahman Omar Sahal,2,5 Walid Abdulkadir Osman6
1Faculty of Medicine, Mogadishu University, Mogadishu, Somalia; 2Radiology Department, Sahan Diagnostic Center, Mogadishu, Somalia; 3Medical Imaging Department, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China; 4Radiology Department, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 5Department of Radiology and Radiotherapy, Makerere University College of Health Sciences, Kampala, Uganda; 6Faculty of Health Sciences, Mogadishu University, Mogadishu, Somalia
Correspondence: Walid Abdulkadir Osman, Email [email protected]
Background: Testicular volume is a critical marker of male reproductive and endocrine health; however, reference values are population-specific. In the absence of ultrasound-based normative data for Somali men, clinicians often rely on external benchmarks that may lead to the misdiagnosis of normal variants. This study aimed to establish ultrasound-derived reference intervals, determine the Minimal Detectable Difference (MDD) for asymmetry, and develop a prediction equation for contralateral volume in Adult Somali men.
Methods: This retrospective study analyzed 212 sonographically normal Somali men (ages 18– 84) at Sahan Diagnostic Center in Mogadishu, Somalia, from June 2022 to December 2025. Volumes were calculated using the standard ellipsoid formula. Statistical analyses included percentile-based reference intervals (2.5th– 97.5th), Cohen’s d for cross-population comparisons, and linear regression to derive a contralateral prediction equation.
Results: Mean testicular volumes were 10.61± 3.07 mL (right) and 10.19± 3.02 mL (left), with a median of 10.0 mL for both. The 95% reference intervals were 5.7– 18.0 mL (right) and 5.2– 17.0 mL (left). The right testis was significantly larger than the left (p < 0.001), and no significant correlation with age was observed. The MDD for asymmetry was 4.1 mL. Notable differences were found compared to European (d = 1.90), West African (d = 1.88), and East and Southeast Asian (d = 0.76– 2.01) cohorts.
Conclusion: These findings establish the first Somali-specific ultrasound benchmarks. Incorporating these intervals and the 4.1 mL MDD into clinical practice will improve diagnostic accuracy in andrological assessments and prevent the misapplication of non-representative global norms.
Keywords: testicular volume, ultrasonography, andrology, sub-Saharan Africa, Somalia
Background
Testicular volume is a practical, quantifiable marker of male reproductive and endocrine function. It is routinely used to support clinical reasoning in infertility evaluation and pubertal development assessment, as it reflects the structural capacity for spermatogenesis and steroidogenesis.1 Because seminiferous tubules constitute most of the testicular parenchyma, testicular size correlates with spermatogenic activity and is commonly interpreted alongside hormone profiles and semen parameters in andrology practice.1,2 Therefore, establishing population-appropriate reference values is essential for distinguishing normal biological variation from clinically meaningful reductions that may indicate testicular dysfunction, prior injury, or the effects of chronic disease.3
Scrotal ultrasonography is widely considered the most objective and reproducible approach for measuring testicular volume in routine care and research, as it directly measures testicular dimensions and applies validated geometric formulas, typically the ellipsoid method.4 In contrast, the Prader orchidometer remains useful for bedside estimation but can systematically overestimate volume because it includes the scrotal wall and peritesticular tissues. Consequently, ultrasound-based norms are preferable when precise reference standardization is required.5 Given that testicular volume is often used as an initial screening indicator before more invasive or costly investigations, reference intervals derived from ultrasonography can improve diagnostic specificity and reduce misclassification in fertility and endocrine pathways.2,4
Multi-ethnic evidence indicates that distributions of male reproductive parameters differ across ancestry and regional backgrounds. This supports the principle that a single universal cutoff for “normal” testicular volume may not be valid for all populations, as it can either pathologize normal variants or fail to detect true pathology.6 In addition, testicular volume also varies meaningfully across the life course and populations, making context-specific norms clinically important. Age-related changes in the male reproductive axis are associated with gradual declines in testicular function and fertility potential, and population studies consistently show reductions in reproductive capacity with advancing age, reinforcing the need to interpret volume values against age-appropriate references.7,8 These considerations are directly relevant to clinical decisions in infertility workups and the monitoring of testosterone-related disorders, where baseline gonadal metrics inform both interpretation and follow-up.3
Despite the clinical relevance of testicular volume measurement, a notable evidence gap exists for adult Somali males, and routine practice may rely on reference ranges developed in different geographic and demographic contexts. Somalia’s distinct environmental exposures, early-life nutritional and health risks, and healthcare access constraints make it scientifically and clinically important to generate local reference values using standardized ultrasonography. Inaccurate norms can adversely affect fertility counseling, evaluation of suspected hypogonadism, and interpretation of andrology imaging in everyday practice. Accordingly, this study aimed to establish ultrasound-derived reference values for right and left testicular volumes among clinically and sonographically normal adult Somali males undergoing scrotal ultrasonography at a diagnostic center in Mogadishu, thereby providing locally relevant benchmarks to support andrological assessment and future research.
Methods
Study Design and Setting
This retrospective, record-based study was conducted in the Radiology Department of Sahan Diagnostic Center, a private facility in Mogadishu, Somalia. The center primarily receives referrals from other hospitals, with occasional self-referred (walk-in) patients. Main indications for scrotal ultrasonography included routine health screening, scrotal pain, and infertility workup.
Study Population and Eligibility
Scrotal ultrasonography reports of men aged ≥18 years who underwent the procedure between June 2022 and December 2025 were retrieved from the hospital information system. Records were eligible if the examination was clinically and sonographically normal, with no scrotal pathology reported. Reports were excluded if they documented any condition likely to alter testicular size or anatomy, including varicocele, testicular atrophy, epididymo-orchitis, undescended testes, torsion, testicular mass, large hydrocele, prior orchidectomy, or incomplete or nonspecific ultrasound findings. Of the 836 reports reviewed, 212 met the inclusion criteria and were included in the final analysis. The participant flowchart is shown in Figure 1.
 |
Figure 1 Participant flow diagram. Of 836 scrotal ultrasound reports reviewed, 624 were excluded due to documented pathology (varicocele, atrophy, epididymo‑orchitis, undescended testis, torsion, mass, hydrocele, prior orchidectomy, or incomplete findings). The remaining 212 men met inclusion criteria and were analyzed. The term “sonographically normal” is used to reflect that this was a clinical sample, not a community‑based healthy cohort. |
Ultrasound Examination Protocol
All examinations were performed using a Samsung WS80A ultrasound machine with a high-frequency broadband linear transducer (L3-12A, 3–12 MHz). To optimize axial resolution of the testicular parenchyma, high-frequency settings were utilized. Scrotal ultrasonography was performed with the patient in both supine and standing positions. Measurements for volume calculation were taken in the supine position, which was the standard position used for final volume calculation. The standing position was used for additional clinical assessment (eg, varicocele evaluation). Grayscale imaging of both testes was obtained in longitudinal and transverse planes, with measurement of maximal testicular dimensions (length, width, and height). Testicular and epididymal size and echogenicity were assessed bilaterally. Color Doppler ultrasound was used to evaluate testicular and peritesticular blood flow. All scans were performed by a single consultant radiologist (AHM, one of the authors, with 9 years of experience) to ensure consistency. A representative ultrasound image showing testicular dimension measurements is presented in Figure 2.
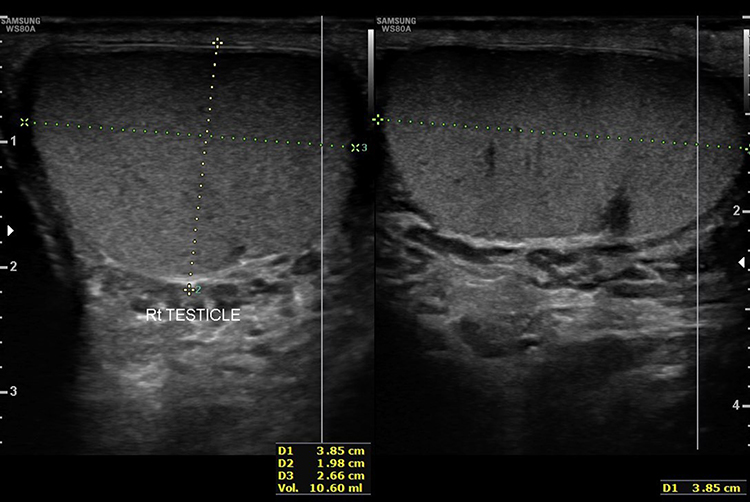 |
Figure 2 Representative ultrasound image of a testis. Transverse and longitudinal views demonstrating measurement of length (L), width (W), and height (H) using calipers. Volume was automatically calculated by the Samsung WS80A machine using the ellipsoid formula: Volume = L × W × H × 0.52. |
Testicular Volume Calculation
Testicular volume was calculated automatically by the ultrasound machine using the standard ellipsoid formula:6 The machine (Samsung WS80A) applied the formula: Volume (mL) = Length × Width × Height × 0.52. Because individual dimensions (length, width, height) were not available in the archived reports, the analysis used the recorded calculated volumes for the right and left testis only.
Data Extraction
Data were extracted from the radiology information system by a single author (KAO) into a dedicated, anonymized dataset. Extracted variables included age (in years) and calculated volumes (in mL) for the right and left testis. All entries were independently double-checked for accuracy by another author (WAO). For patients with multiple scans, only the most recent ultrasound report was included to avoid duplication.
Statistical Analysis
Data were analyzed using SPSS (version 26, IBM Corp., Armonk, NY, USA). Descriptive statistics (mean, standard deviation, median, minimum, maximum) were calculated for age and testicular volumes. Because testicular volumes were not normally distributed, non-parametric methods were applied for all hypothesis tests. Percentile-based reference values (2.5th, 5th, 10th, 25th, 50th, 75th, 90th, 95th, and 97.5th percentiles) were derived for right and left testicular volumes. Age groups (18–30, 31–40, 41–50, 51–60, and ≥61 years) were chosen to ensure approximately equal sample sizes where possible and to align with clinically relevant decades. The Wilcoxon signed-rank test was used to compare right and left testicular volumes, and the proportion of participants with a larger right testis, a larger left testis, and equal volumes was calculated. Spearman’s rank correlation coefficient was used to assess the relationship between age and testicular volumes for each side.
The minimal detectable difference (MDD) for right-left asymmetry was calculated by first deriving the standard deviation of the difference between right and left testicular volumes from the individual standard deviations and the correlation coefficient, then computing the MDD at the 95% confidence level. This MDD represents the smallest difference between right and left volumes that exceeds 95% measurement error. Cohen’s d effect sizes were calculated to compare the right testicular volume of our Somali sample with published means from other populations, with effect sizes of 0.2, 0.5, and 0.8 interpreted as small, medium, and large, respectively. The right testis was chosen because it is often slightly larger and more consistently measured.9 Linear regression was used to derive a prediction equation for left testicular volume from right testicular volume. The standard error of the estimate (SEE) was calculated to quantify prediction accuracy. A p-value < 0.05 was considered statistically significant for all hypothesis tests.
Ethical Considerations
Ethical approval was obtained from the National Institute of Health – Somalia (Ref: NIH/SNREB/013/MAR/2026) before any data were accessed. This study involved the secondary use of existing clinical imaging records and was conducted in strict accordance with the Declaration of Helsinki. To protect patient privacy, all data were anonymized at collection, with unique study codes replacing any direct identifiers. Data were stored on a password-protected computer accessible only to the research team, and results are presented as aggregate data only, ensuring that no individual can be identified. Because this was a retrospective study utilizing anonymized data extracted from existing medical records, the requirement for individual informed consent was not applicable; a formal waiver of informed consent was granted by the ethics review committee, as the research posed minimal risk to subjects. The principal investigator maintained the data security throughout the study period.
Results
Participant Characteristics and Testicular Volume Summary
A total of 212 sonographically normal adult Somali men aged 18 to 84 years were included in the analysis. The mean age was 35.5 ± 13.1 years. The mean volume of the right testis was 10.61 ± 3.07 mL (range: 3.3–20.0 mL), and the left testis was 10.19 ± 3.02 mL (range: 4.4–20.0 mL), with medians of 10.0 mL for both. Table 1 summarizes participant characteristics and testicular volumes.
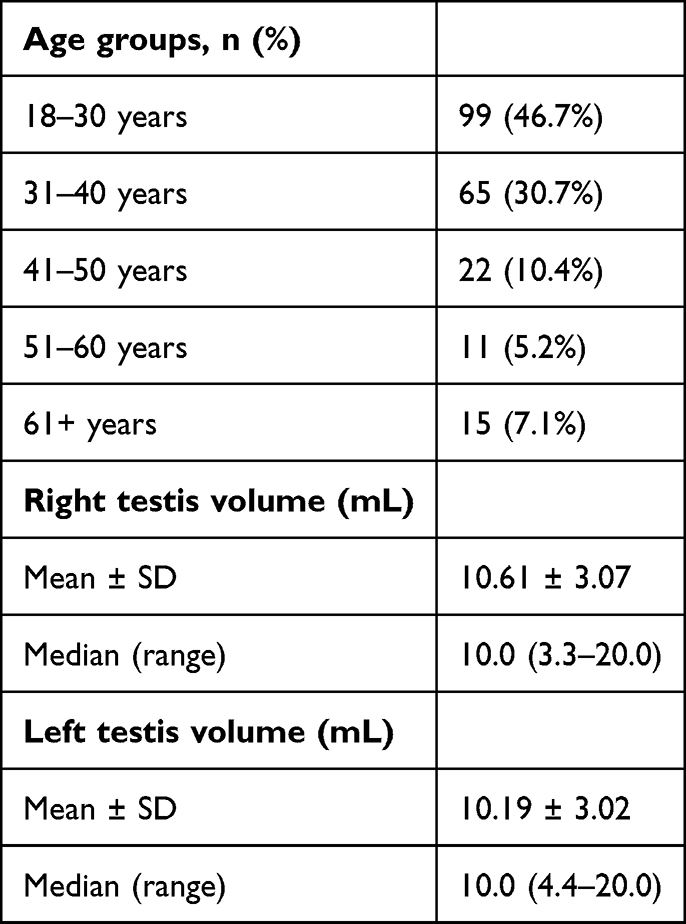 |
Table 1 Participant Characteristics and Testicular Volume Summary |
Normative Reference Values
Percentile-based reference values for testicular volume are summarized in Table 2. The 95% reference intervals, defined as the 2.5th to 97.5th percentiles, were 5.7–18.0 mL for the right testis and 5.2–17.0 mL for the left testis.
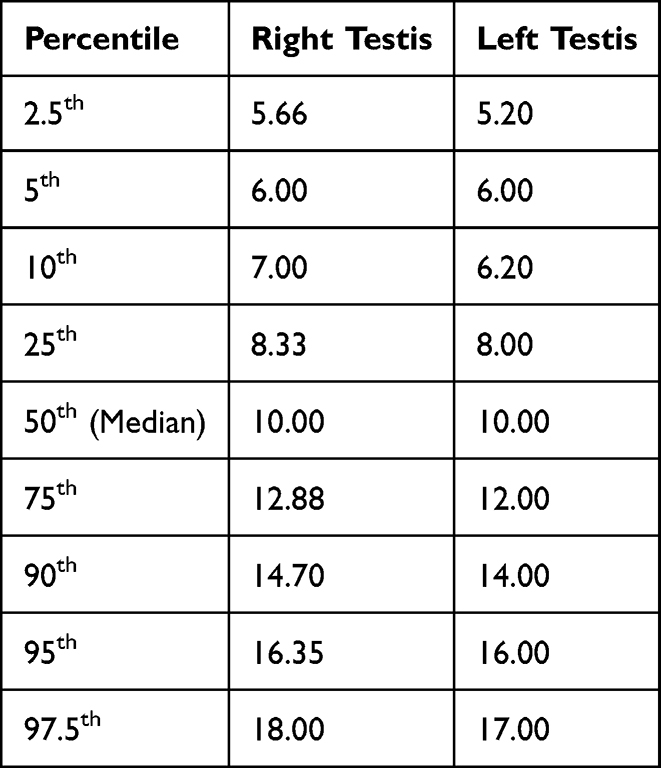 |
Table 2 Percentile Distribution of Testicular Volumes (mL) |
Right-Left Comparison and Age Correlation
A Wilcoxon signed-rank test revealed a statistically significant difference between the volumes of the right and left testes (Z = −3.918, p < 0.001), with the right testis being significantly larger than the left. Of the 212 participants, 99 (46.7%) had a larger right testis, 55 (25.9%) had a larger left testis, and 58 (27.4%) had equal volumes. Spearman’s rank correlation analysis demonstrated no significant correlation between age and testicular volume for either the right testis (ρ = 0.098, p = 0.156) or the left testis (ρ = 0.064, p = 0.357). However, a strong positive correlation was observed between the volumes of the right and left testes (ρ = 0.882, p < 0.001). These findings are summarized in Table 3.
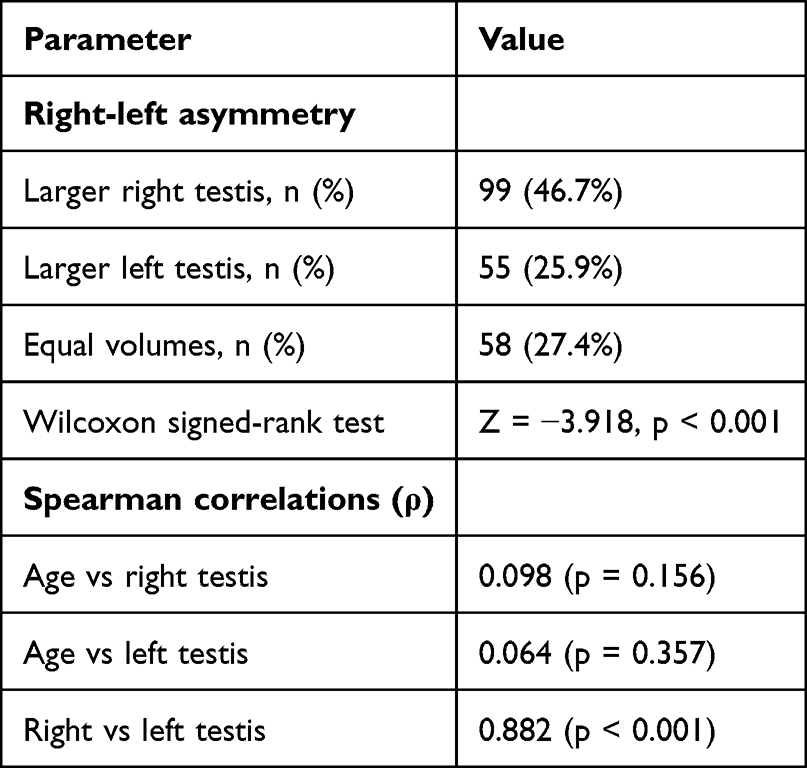 |
Table 3 Right-Left Comparison and Age Correlation |
Minimal Detectable Difference and Prediction Equation
The minimal detectable difference (MDD) for right-left asymmetry was 4.1 mL. This means that a difference between right and left testicular volumes must exceed 4.1 mL to be considered a true asymmetry beyond measurement error at the 95% confidence level.
The linear regression equation for predicting left testicular volume from right testicular volume was: left volume (mL) = 0.98 + 0.87 × right volume. The standard error of the estimate (SEE) was 1.42 mL, indicating that approximately 68% of predicted left volumes fall within ±1.42 mL of the true value. The coefficient of determination (R2) was 0.778, meaning that 77.8% of the variance in left testicular volume is explained by right testicular volume.
Comparison with Other Populations: Cohen’s d Effect Sizes
Cohen’s d effect sizes comparing Somali men to other populations ranged from moderate (Vietnam, d = 0.76) to extremely large (Italy, d = 3.77), as detailed in Table 4.
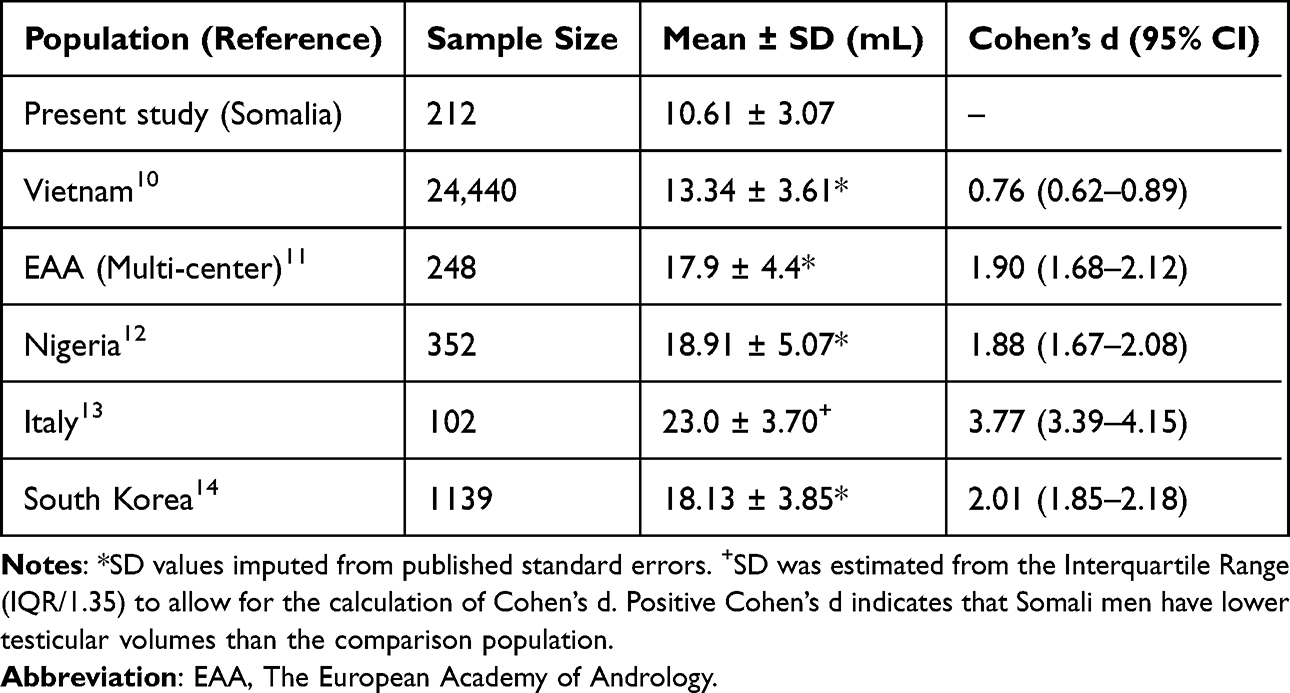 |
Table 4 Comparison of Right Testicular Volume: Somali vs International Populations |
Discussion
This study provides the first ultrasound-based reference values for testicular volume in sonographically normal adult Somali men. The mean volumes observed (right: 10.61 mL; left: 10.19 mL) are lower than those reported in many other populations, where adult mean or median testicular volumes measured by ultrasound typically range from 13–19 mL. For example, regional studies from Saudi Arabia report mean testicular volumes of 12.0 mL (right) and 11.2 mL (left), while data from Nigeria demonstrate notably higher mean volumes of 18.46 mL (right) and 17.01 mL (left).15,16 Healthy Vietnamese fathers had a mean volume of 13.6 mL,10 healthy fertile European men in the EAA multi-center study had a mean volume of approximately 17 mL with lower limits of normal of 12 mL (right) and 11 mL (left),11 and healthy Nigerian adults and other African cohorts often show mean volumes in the 17–19 mL range.12,17,18 A large Caucasian adult sample also reported median ultrasound volumes of 13.9 mL (right) and 12.7 mL (left) using the ellipsoid formula.19 These differences highlight the importance of population-specific reference intervals and caution against applying external norms that may pathologize normal variants or miss true pathology.
The normal testicular volume ranges we established for Somali men are 5.7–18.0 mL for the right testis and 5.2–17.0 mL for the left testis (95% reference intervals). A volume below 5.7 mL (right) or 5.2 mL (left) is unusually low and may signal a problem such as low testosterone (hypogonadism), past infection of the testicle (orchitis), or testicular shrinkage (atrophy), warranting further evaluation. For comparison, in healthy European men the lower limits of normal are higher – 12 mL for the right testis and 11 mL for the left – confirming that Somali men naturally have smaller testes.11 Volumes above 18.0 mL (right) or 17.0 mL (left) are very uncommon in Somali men; however, these values still lie within or below the upper limits seen in other healthy populations.13,18 Therefore, a large testis in a Somali man is not necessarily abnormal – it simply means he is at the high end of his own population’s normal range.
We observed a statistically significant right-left asymmetry, with a right-sided predominance in 46.7% of participants compared to 25.9% for the left. This finding aligns with existing literature suggesting that anatomical or developmental variations frequently result in a larger right testis.11,20,21 Clinical thresholds for adolescents – such as an absolute volume difference >2 mL or an atrophy index ≥20% – are widely used to identify pathology.20 However, our data suggest that mild asymmetry is often physiological. This is supported by Srinivas et al,22 who found that in healthy prepubertal boys, a Volume Differential Index (VDI) of up to 27% (95th percentile) represents normal variation. Furthermore, 27.4% of our participants had equal volumes, and the absolute differences observed were generally minimal. The average right‑left difference in our cohort was only 0.42 mL, which is far below the 2 mL clinical threshold. More importantly, we calculated a minimal detectable difference (MDD) of 4.1 mL – the threshold above which an individual’s asymmetry can be considered real (beyond measurement error). Since our MDD (4.1 mL) exceeds the 2 mL clinical cutoff, applying the 2 mL rule to Somali men would incorrectly classify many healthy individuals as having pathological asymmetry. Consequently, mild asymmetry alone should not be interpreted as pathological unless accompanied by other clinical abnormalities or exceeding this threshold.
In the present cohort, no significant correlation was found between age and testicular volume. This finding is consistent with a growing body of literature reporting weak or absent age-volume associations in adult populations.12 This suggests that once physiological maturity is reached, intrinsic biological variation – rather than chronological aging – is the dominant factor influencing testicular volume throughout the adult lifespan.23 However, this contrasts with studies showing that testicular volume increases through puberty, peaks in early to mid-adulthood, then remains relatively stable until about 50–60 years before declining.24–26 The lack of age association in our data may be explained by the relatively small number of older participants (n = 15 over 60 years), which limits power to detect late-life decline. Alternatively, age-related volume decline may be less pronounced in this population, or the cross-sectional design may obscure longitudinal changes. The observed peak mean volume in the 41–50-year age group (right: 12.65 mL) is an unexpected finding that may be due to chance or selection bias and should be interpreted with caution.
The derived prediction equation (Left = 0.98 + 0.87 × Right; SEE = 1.42 mL) is a clinically useful tool for estimating contralateral testicular volume when only one side is reliably measurable. This high level of symmetry is consistent with robust right-left correlations reported in other ultrasound-based series.27,28 For example, if a patient has a right testicular volume of 12 mL, the expected left volume would be approximately 11.4 mL (95% prediction interval: 8.6–14.2 mL). Volumes falling outside this range should prompt evaluation for pathological asymmetry rather than normal biological variation.
There are several reasons why Somali men might have lower testicular volumes than other populations. Contributing factors could include genetic ancestry, early life nutrition, exposure to environmental heat stress, and socioeconomic conditions. For example, chronic heat exposure is known to impair testicular function, and nutritional deficits during development can affect testicular growth.29 Differences in methodology across studies—such as inter‑observer variability, the type of ultrasound equipment and its built‑in calculation software—may also account for the observed variations. The same testis measured by different sonographers can yield meaningfully different volumes; even among experienced observers, inter‑observer agreement for detecting clinically significant asymmetry (≥20% volume difference) can be poor.30 Furthermore, the calculated volume depends heavily on the formula used by the ultrasound system. Built‑in software is not always accurate relative to the ellipsoid formula recommended by current guidelines: using the same raw dimensions but different constants (0.71 vs 0.52) produced a 26.76% difference in volume.31 We emphasize the need for true community‑based studies to confirm these reference intervals.
Very large to extremely large effect sizes (Cohen’s d = 1.88–3.77) were observed when comparing Somali men to European,11,13 West African,12 and East Asian14 reference populations, with a more moderate difference against the Vietnamese cohort10 (d = 0.76). This means that using European or West African reference intervals would misclassify a substantial proportion of healthy Somali men as having abnormally small testes, leading to unnecessary investigations and potential misdiagnosis. These quantitative comparisons reinforce the necessity of population-specific norms and support the establishment of locally derived reference ranges rather than reliance on universal cutoffs.
This study has several limitations. First, the retrospective, single‑center design limits generalizability. Second, the sample was derived from a clinical population (men referred for scrotal ultrasound, including for infertility or pain), not a community‑based healthy cohort, introducing potential selection bias. Third, individual testicular dimensions (length, width, height) were not archived, preventing independent verification of volume calculations. Fourth, intra-observer reliability was not assessed since there were no repeat measurements, and inter-observer reliability could not be evaluated because all scans were performed by single radiologist. Fifth, the number of older participants (≥61 years, n=15) was small, limiting conclusions about age‑related changes. Sixth, hormonal parameters (testosterone, LH, FSH) and semen analysis were not available, limiting functional interpretation of the reference intervals. Seventh, anthropometric data such as BMI were not collected, despite their potential relevance to testicular volume. Finally, tribal or genetic ancestry information was not available, precluding analysis of hereditary influences.
Conclusion
This study establishes the first ultrasound-derived reference intervals for testicular volume in sonographically normal adult Somali men. The 95% reference ranges are 5.7–18.0 mL for the right testis and 5.2–17.0 mL for the left testis. Compared to European, West African, and East Asian populations, Somali men had substantially lower testicular volumes. The minimal detectable difference (4.1 mL) provides a clinically actionable threshold for asymmetry. No significant correlation with age was observed, although the small proportion of participants aged ≥61 years (7.1%) limits the ability to draw firm conclusions about testicular volume stability in later decades. These reference intervals should be adopted in routine andrology practice in Somalia and similar East African populations. Using external norms could incorrectly label normal Somali men as having “small testes,” leading to unnecessary investigations or misdiagnosis of hypogonadism. In contrast, a genuinely reduced volume relative to these local norms would be a more specific indicator of testicular dysfunction. Future prospective, community‑based studies should include hormonal and semen parameters, inter‑observer reliability assessment, anthropometric measurements, and genetic/tribal information to validate and extend these findings.
Data Sharing Statement
The datasets used and analyzed in this study are available from the corresponding author upon a reasonable request.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the National Institute of Health – Somalia (Ref: NIH/SNREB/013/MAR/2026). A waiver of informed consent was granted.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors declare no competing interests in this work.
References
1. Lotti F, Maggi M. Ultrasound of the male genital tract in relation to male reproductive health. Hum Reprod Update. 2015;21(1):56–10. doi:10.1093/humupd/dmu042
2. Kristo A, Dani E. The correlation between ultrasound testicular volume and conventional semen parameters in albanian subfertile males. Open Access Maced J Med Sci. 2014;2(3 SE–B–Clinical Sciences):464–466. doi:10.3889/oamjms.2014.081
3. Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(5):1715–1744. doi:10.1210/jc.2018-00229
4. Hsieh ML, Huang ST, Huang HC, Chen Y, Hsu YC. The reliability of ultrasonographic measurements for testicular volume assessment: comparison of three common formulas with true testicular volume. Asian J Androl. 2009;11(2):261–265. doi:10.1038/aja.2008.48
5. Sotos JF, Tokar NJ. Appraisal of testicular volumes: volumes matching ultrasound values referenced to stages of genital development. Int J Pediatr Endocrinol. 2017;2017:7. doi:10.1186/s13633-017-0046-x
6. Henkel R, Elbardisi H, Majzoub A, Arafa M. Racial differences in male fertility parameters in 2,996 men examined for infertility in a single center. Arab J Urol. 2025;23(4):255–265. doi:10.1080/20905998.2025.2470045
7. Gunes S, Hekim GNT, Arslan MA, Asci R. Effects of aging on the male reproductive system. J Assist Reprod Genet. 2016;33(4):441–454. doi:10.1007/s10815-016-0663-y
8. Frungieri MB, Calandra RS, Bartke A, Matzkin ME. Male and female gonadal ageing: its impact on health span and life span. Mech Ageing Dev. 2021;197:111519. doi:10.1016/j.mad.2021.111519
9. Lowe JS, Anderson PG. Chapter 16 - male reproductive system. In: Lowe JS, Anderson PG, editors. Stevens & Lowe’s Human Histology, (Fourth Edition). Mosby; 2015:319–336. doi:10.1016/B978-0-7234-3502-0.00016-4
10. Nguyen Hoai B, Hoang L, Tran D, et al. Ultrasonic testicular size of 24,440 adult Vietnamese men and the correlation with age and hormonal profiles. Andrologia. 2022;54(2):e14333. doi:10.1111/and.14333
11. Lotti F, Frizza F, Balercia G, et al. The European Academy of Andrology (EAA) ultrasound study on healthy, fertile men: an overview on male genital tract ultrasound reference ranges. Andrology. 2022;10(S2):118–132. doi:10.1111/andr.13260
12. Owoicho IE, Anthony GE, Othniel IK, et al. Establishing normative mean sonographic testicular volumes in adult males: a study in North-Central Nigeria. Eur Mod Stud J. 2025;9(1):54–59. doi:10.59573/emsj.9(1).2025.5
13. Boeri L, Capogrosso P, Ventimiglia E, et al. Testicular volume in infertile versus fertile white-European men: a case-control investigation in the real-life setting. Asian J Androl. 2021;23(5):501–509. doi:10.4103/aja.aja_93_20
14. Bahk JY, Jung JH, Jin LM, Min SK. Cut-off value of testes volume in young adults and correlation among testes volume, body mass index, hormonal level, and seminal profiles. Urology. 2010;75(6):1318–1323. doi:10.1016/j.urology.2009.12.007
15. Alsahafi RA, Alsahafi E, Abduljabbar AH, Wazzan MA. Determining the normal size and values of the testicles in adult population in the western region, Saudi Arabia. Int J Approx Reason. 2017;5:1176–1181.
16. Anakwue AM, Nwosu C, Idigo F, Nwogu U, Maduka B. Sonographic determination of normal testicular volume in an adult Nigerian population. 2021.
17. Innocent MC, Asomugha LA, Ukamaka MN, Aronu ME. Ultrasound measured testicular volume in Nigerian adults: relationship of the three formulae with height, body weight, body-surface area, and body-mass index. Int J Adv Med Heal Res. 2016;3(2):85–90. doi:10.4103/2349-4220.195940
18. Tijani KH, Oyende BO, Awosanya GO, Ojewola RW, Yusuf AO. Assessment of testicular volume: a comparison of fertile and sub-fertile West African men. African J Urol. 2014;20(3):136–140. doi:10.1016/j.afju.2014.05.001
19. Pilatz A, Rusz A, Wagenlehner F, Weidner W, Altinkilic B. Reference values for testicular volume, epididymal head size and peak systolic velocity of the testicular artery in adult males measured by ultrasonography TT - Sonografische Referenzwerte für Hodenvolumina, Nebenhodenkopfgröße und systolische Flussgeschwindigkeit der A. testicularis bei Männern. Ultraschall Med. 2013;34(04):349–354. doi:10.1055/s-0032-1313077
20. Vaganée D, Daems F, Aerts W, et al. Testicular asymmetry in healthy adolescent boys. BJU Int. 2018;122(4):654–666. doi:10.1111/bju.14174
21. Berg WT, Avellino GJ, Hwang K, Sigman M. Thresholds for testicular size discrepancy in fertile men with and without varicocele. Fertil Steril. 2020;114(3):e95–e96. doi:10.1016/j.fertnstert.2020.08.291
22. Srinivas R, Thomas RJ, Sebastian T, Kurian JJ. Testicular volume in a cohort of prepubertal Indian children. J Indian Assoc Pediatr Surg. 2019;24(3):192. doi:10.4103/jiaps.JIAPS_100_18
23. Fui MNT, Hoermann R, Wittert G, Grossmann M. Testicular volume and clinical correlates of hypothalamic–pituitary–testicular function: a cross-sectional study in obese men. Asian J Androl. 2020;22(4).
24. Well D, Yang H, Houseni M, et al. Age-related structural and metabolic changes in the pelvic reproductive end organs. Semin Nucl Med. 2007;37(3):173–184. doi:10.1053/j.semnuclmed.2007.01.004
25. Lasiene K, Gasiliunas D, Juodziukyniene N, Dabuzinskiene A, Vitkus A, Zilaitiene B. Age-related morphological peculiarities of human testes. Folia Morphol. 2021;80(1):122–126. doi:10.5603/FM.a2020.0033
26. Yang H, Chryssikos T, Houseni M, et al. The effects of aging on testicular volume and glucose metabolism: an investigation with ultrasonography and FDG-PET. Mol Imaging Biol. 2011;13(2):391–398. doi:10.1007/s11307-010-0341-x
27. Spaggiari G, Granata ARM, Santi D. Testicular ultrasound inhomogeneity is an informative parameter for fertility evaluation. Asian J Androl. 2020;22(3):302–308. doi:10.4103/aja.aja_67_19
28. Liu C, Liu X, Zhang X, et al. Referential values of testicular volume measured by ultrasonography in normal children and adolescents: z-score establishment. Front Pediatr. 2021;9:648711. doi:10.3389/fped.2021.648711
29. Ko SH. Effects of heat stress-induced sex hormone dysregulation on reproduction and growth in male adolescents and beneficial foods. Nutrients. 2024;16(17):3032. doi:10.3390/nu16173032
30. Sorokin I, Welliver C, Elebyjian L, Feustel PJ, McCullough A. Interinstitutional variability in testicular volumes and varicocele presence by ultrasound: surprising discrepancies and implications for clinical decision making. Urology. 2015;85(5):1079–1084. doi:10.1016/j.urology.2015.02.018
31. Cai D, Wu S, Li Y, Chen Q. Validity of measurements of testicular volume obtained by a built-in software of ultrasound systems: with formula recommended by updated guidelines as reference. J Ultrason. 2020;20(82):e181–e184. doi:10.15557/JoU.2020.0030
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Lymphadenopathies: A Retrospective Study of Epidemiology, Characteristics, Diagnosis and Treatment Outcomes of Patients in a Tertiary Hospital in Mogadishu-Somalia
Kıratlı K, Bulut M, Ali MA, Aysin M, Ali AM, Mohamed Hirsi I, Bashir AM
Infection and Drug Resistance 2025, 18:557-566
Published Date: 30 January 2025