Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Nonlinear Association Between Monocyte-to-HDL Ratio and Mortality in COPD: Evidence from NHANES
Authors Tian T, She T, Qu X, Li R
Received 25 August 2025
Accepted for publication 27 November 2025
Published 12 December 2025 Volume 2025:20 Pages 4005—4018
DOI https://doi.org/10.2147/COPD.S563173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Tulei Tian,1,* Tianyu She,2,* Xiangkun Qu,1 Rui Li3
1Department of Respiratory and Critical Care Medicine, the Affiliated Bozhou Hospital of Anhui Medical University, Bozhou, Anhui, People’s Republic of China; 2Department of Medical Imaging Function, Xi’an Electric Power Central Hospital, Xi’an, Shaanxi, People’s Republic of China; 3Traditional Chinese Medicine Internal Medicine, The Third Affiliated Hospital of Liaoning University Traditional Chinese Medicine, Shenyang, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rui Li, Email [email protected] Tulei Tian, Email [email protected]
Background: Chronic Obstructive Pulmonary Disease (COPD) represents a leading cause of mortality worldwide, with systemic inflammation being a key pathological feature. The association between the emerging inflammatory marker monocyte to high-density lipoprotein cholesterol ratio (MHR) and the risk of all-cause mortality in COPD patients remains unclear.
Methods: Data from COPD patients in the 1999– 2018 NHANES database were analyzed using Cox regression models to assess the association between MHR and all-cause mortality risk. Restricted cubic spline (RCS) modeling was used to explore nonlinear associations and identify inflection points. Time-dependent ROC curves were utilized to evaluate the predictive accuracy of MHR. Subgroup and sensitivity analyses were performed to ensure the robustness of the results.
Results: This study included 1768 COPD patients and observed 606 all-cause deaths during a mean follow-up of 92 months. After adjusting for confounding factors, MHR level was significantly and positively associated with all-cause mortality risk (HR = 2.10, 95% CI: 1.53– 2.89). RCS analysis revealed a nonlinear relationship between MHR and all-cause mortality risk (non-linear P = 0.004). A turning point analysis indicated a threshold effect of MHR at 0.29: mortality risk increased significantly above this value (HR = 2.52, P < 0.001) and decreased significantly below it (HR = 0.02, P = 0.006). Sex-stratified analysis showed that the association between MHR and mortality risk tended to be linear in men, while it was nonlinear in women. Time-dependent ROC analysis showed AUC values for MHR at 12, 36, 72, and 120 months were 0.73, 0.79, 0.78, and 0.81, respectively.
Conclusion: Elevated MHR serves as an important risk marker for all-cause mortality in COPD patients. This association exhibits nonlinear characteristics with threshold effects, suggesting that MHR has potential value in prognostic assessment of COPD patients.
Keywords: chronic obstructive pulmonary disease, monocyte to HDL-C ratio, MHR, mortality, nonlinear association, NHANES
Introduction
Chronic obstructive pulmonary disease (COPD) is a respiratory condition characterized by persistent airflow limitation. It is a prevalent condition worldwide, with an estimated 10.3% of the adult population affected, and also represents the third leading cause of mortality globally, exerting significant pressure on healthcare systems.1–3 Given the highly heterogeneous nature of the disease course and clinical manifestations, precise assessment of patients’ long-term mortality risk is crucial for guiding clinical decision-making and improving individualized prognosis.4 Therefore, identifying biomarkers that reflect key pathophysiological processes (particularly systemic inflammation and metabolic imbalance) and are easily applicable in clinical settings to facilitate effective risk stratification5 has become a research focus in this field.
In this context, the monocyte-to-high-density lipoprotein cholesterol ratio (MHR), an indicator integrating inflammatory and lipid metabolic status that can be measured through routine blood tests, has attracted researchers’ interest.6–8 Biologically, monocytes are important innate immune cells whose counts in peripheral blood often reflect systemic inflammation levels, and their infiltration and activation play a key pro-inflammatory role in the pathophysiology of various chronic inflammatory diseases, such as COPD.7,9
On the other hand, high-density lipoprotein cholesterol (HDL-C) not only mediates reverse cholesterol transport but also exerts important anti-inflammatory, antioxidant, and endothelial protective effects.7,8,10 Therefore, MHR is considered to comprehensively reflect the imbalance between pro-inflammatory drivers (represented by increased monocytes) and anti-inflammatory/protective mechanisms (represented by decreased HDL-C levels) in the body, an imbalance closely associated with adverse clinical outcomes.6,7 Previous research has extensively confirmed the prognostic value of MHR: in the field of cardiovascular disease, elevated MHR has been demonstrated to be an independent predictor of coronary artery disease severity, major adverse cardiovascular events (MACE), heart failure, and stroke risk.11,12 Moreover, the prognostic significance of MHR in chronic respiratory diseases has increasingly attracted attention. A recent cohort study conducted among asthma patients in the United States confirmed that elevated MHR is independently associated with increased risk of all-cause mortality.13 Additionally, studies on COPD patients suggest that there may be a possible link between MHR and the risk of cardiovascular comorbidities among these individuals.14 These findings in different respiratory diseases further highlight the broad potential of MHR, as a comprehensive indicator reflecting inflammatory-metabolic imbalance, in chronic disease risk assessment.
Despite the demonstrated prognostic potential of MHR in cardiovascular diseases11,12 and other respiratory diseases,13 direct evidence for its role as an independent predictor of long-term all-cause mortality risk in COPD patients remains insufficient. Currently, large-scale cohort studies specifically addressing the association between MHR and long-term survival outcomes in COPD populations are still scarce. Given this evidence, the present study leverages the large, nationally representative prospective cohort data from NHANES to systematically assess the independent relationship between baseline MHR levels and long-term all-cause mortality risk in diagnosed COPD patients, and to explore the manifestation of this association across different subgroups. The results of this study are expected to provide a new, clinically applicable biomarker perspective for precise risk stratification in COPD, complementing existing assessment tools.
Methods
Data Source and Participant Selection
The data for this study were derived from NHANES 1999–2018, a major health survey program conducted by the National Center for Health Statistics (NCHS) under the Centers for Disease Control and Prevention (CDC). NHANES employs a complex, multistage probability sampling design to obtain representative information on the health and nutritional status of the non-institutionalized US population, with data collection methods including standardized questionnaire interviews, physical examinations, and laboratory tests. This study was reported in accordance with the STROBE statement guidelines.15 Following approval by the NCHS Ethics Review Board, all NHANES participants provided written informed consent for the research protocols. Given that this research constitutes a secondary analysis of publicly available anonymized data, no additional ethical review approval was required as per relevant regulations.16
The participant selection process for this study was based on 101,316 initial records from the aforementioned NHANES 1999–2018 cycles. First, individuals who were pregnant or under 20 years of age were excluded (N=43,776). Next, participants who were not diagnosed with COPD or had missing relevant data were excluded (N=54,968). Finally, 804 individuals were excluded due to missing data for the key variable MHR, other covariates, or outcome follow-up data (mortality status/follow-up records). After this series of screening steps, a total of 1,768 participants meeting all inclusion criteria were included in the final analysis. As shown in Figure 1, these 1,768 final participants were divided into three groups (tertiles) based on MHR levels: Group T1 (N=591), Group T2 (N=584), and Group T3 (N=593).
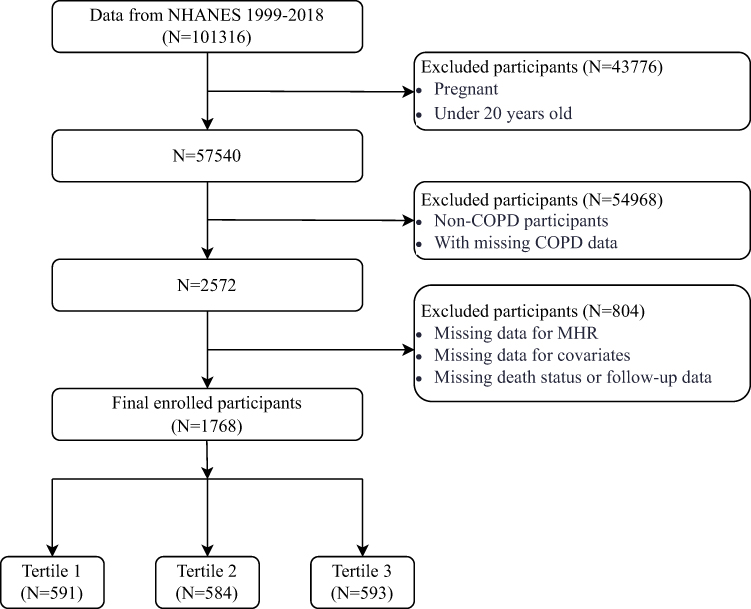 |
Figure 1 Flow chart of the study participants. |
Ascertainment of COPD Status and MHR Calculation
To accurately identify COPD patients within the NHANES database for this study, a validated multi-criteria diagnostic strategy was employed.17–19 Participants were included in the COPD case group if they met any of the following three criteria:
- Pulmonary function tests showing a forced expiratory volume in the first second (FEV1) divided by the forced vital capacity (FVC) of less than 0.7 after bronchodilator administration, aligning with recommendations from the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines;2
- Self-reported physician diagnosis of COPD;
- Age of 40 years or older, currently using COPD-specific treatment medications, and meeting at least one or more of the subsequent criteria: a cumulative smoking history exceeding 100 pack-years, a physician’s diagnosis of either emphysema or chronic bronchitis, or active symptoms indicative of chronic bronchitis. This comprehensive diagnostic approach was adopted to enhance the accuracy of case definition in epidemiological surveys.
In this study, MHR was evaluated as the primary exposure variable. It was calculated as the ratio of monocyte count in blood (unit: ×103/µL) to HDL-C concentration (unit: mg/dL). These indicators were obtained through laboratory testing of participants’ blood samples. The testing process strictly followed NHANES standardized operating procedures, using validated blood analysis techniques to ensure the accuracy and reproducibility of monocyte counts and HDL-C measurements.
Ascertainment of Mortality and Follow-Up Duration
This study determined participants’ survival status and cause of death information by probabilistically matching NHANES participant data with the National Death Index (NDI).20 The follow-up observation period extended until December 31, 2019. The primary outcome event was defined as all-cause mortality, ie, death from any cause. The specific cause of death was determined according to the International Classification of Diseases, Tenth Revision (ICD-10).21 The follow-up time for each participant was calculated from the date of completing the NHANES baseline examination until the earliest of the following dates: date of death, date of loss to follow-up, or the study’s designated follow-up end date.
Description of Covariates
To control for potential confounding factors in the analysis, this study included a series of covariates with data derived from NHANES questionnaires, physical examinations, and laboratory test results. Specifically, these covariates encompassed sociodemographic characteristics (such as age, gender, race, marital status, educational level, and family poverty-income ratio [PIR]), lifestyle factors (involving smoking and drinking status), anthropometric indicators (body mass index [BMI]), clinical comorbidities (including hypertension, diabetes, atherosclerotic cardiovascular disease [ASCVD], and cancer), as well as laboratory test values (including blood eosinophil count). For detailed operational definitions and classification criteria of each covariate, please refer to the Supplementary Methods section of this study.
Statistical Analysis
This study utilized NHANES data from 1999–2018 for statistical analysis, strictly following official guidelines and considering the survey’s complex multi-stage stratified cluster sampling and oversampling design, with appropriate sample weights applied.22 Continuous variables were described using weighted means ± standard deviations or medians (interquartile ranges), with between-group comparisons conducted using weighted one-way analysis of variance (ANOVA) or Kruskal–Wallis tests. Categorical variables were presented as frequencies and weighted proportions, with comparisons among groups performed using weighted Rao-Scott χ2-tests, or Fisher’s exact test when expected counts were low. Variable missingness is detailed in Table S1. Primary analyses were conducted using complete case data. Additionally, we performed multiple imputation using chained equations (MICE) to generate five imputed datasets23,24 to perform sensitivity analyses.
Schoenfeld residual tests confirmed the proportional hazards assumption for Cox regression25 (P for global test > 0.05; see Table S2 and Figure S1). Survival curves were plotted using the Kaplan-Meier method (comparing different MHR tertile groups via Log rank test) to visually demonstrate survival differences before constructing three progressively adjusted Cox models. Model 1 was unadjusted, Model 2 included adjustments for demographic and lifestyle factors, and Model 3 further accounted for clinical comorbidities and laboratory indicators based on Model 2. In these models, MHR was primarily incorporated as a continuous variable, while also being evaluated by tertile grouping. Furthermore, to investigate potential non-linear associations and threshold effects, RCS were employed to fit the association between MHR and mortality risk. All association results are presented as hazard ratios (HRs) with corresponding 95% confidence intervals (CIs).
To further explore the predictive value of MHR, time-dependent receiver operating characteristic (ROC) curve analysis was utilized to comprehensively evaluate the predictive performance of this index for all-cause mortality in COPD patients. Specifically, we calculated the area under the curve (AUC) for MHR at several key follow-up time points: 12 months, 36 months, 60 months, and 120 months, to quantify its predictive discrimination ability.
To ensure the reliability of results, missing data were first handled using multiple imputation by chained equations (MICE, with five iterations), then extreme outliers of MHR (defined as exceeding the mean±3 standard deviations) were excluded. Additionally, subgroup analyses based on key clinical and demographic characteristics were conducted to evaluate the consistency and potential heterogeneity of the association between MHR and mortality risk across different populations.
Data analysis was performed using R software (version 4.3.3, including the survey package) and Free Statistics software (version 2.1.1).26 All statistical tests were two-sided, with P values less than 0.05 considered as the threshold for statistical significance.
Results
Baseline Characteristics of the Participants
Table 1 details the baseline characteristics of the 1,768 participants in this study, stratified by tertiles of MHR [T1 (0.03–0.36), T2 (0.36–0.55), T3 (0.55–6.15)]. Overall, the mean age of participants was 60.45 years (standard error 12.72), with a weighted male proportion of 49.27%. The mean follow-up time was 92.14 months (standard error 56.13). During the follow-up period, a total of 606 all-cause deaths (unweighted count, weighted mortality rate 27.36%).
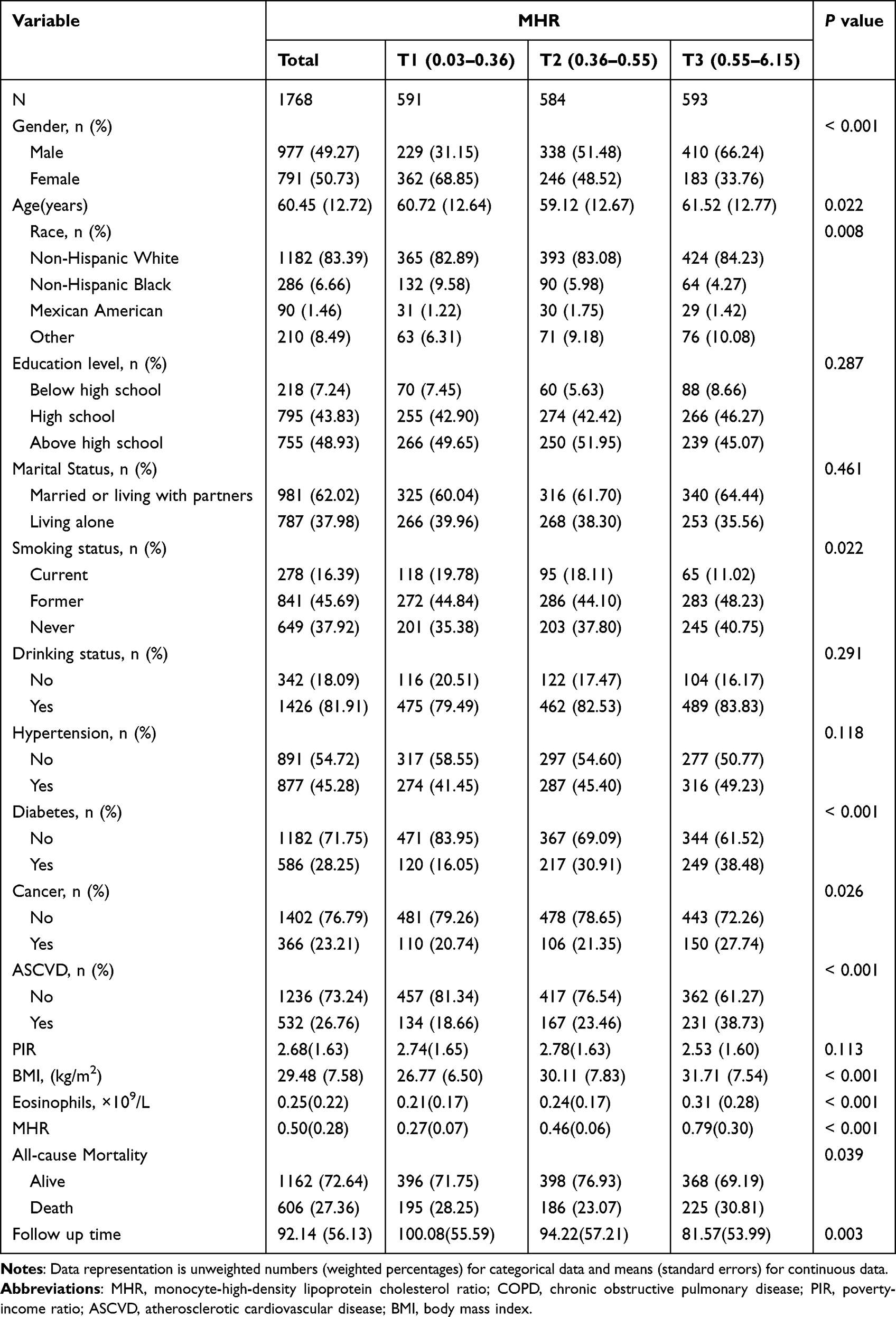 |
Table 1 Baseline Characteristics Stratified by MHR Tertiles |
As shown in Table 1, multiple baseline characteristics exhibited significant differences across MHR tertiles (P<0.05). Relative to the lowest MHR tertile (T1), individuals in the highest tertile (T3) showed higher age, a greater proportion of males, and a higher percentage of non-Hispanic whites. Regarding clinical indicators, T3 participants not only had higher BMI and eosinophil counts but also exhibited lower current smoking rates. However, this group also had significantly higher risks of diabetes, cancer, and ASCVD. On the other hand, the study cohort showed no statistically significant differences in education level, marital status, drinking status, hypertension prevalence, or PIR across different MHR levels.
Associations Between MHR and Mortality
As presented in Table 2, after full adjustment for covariates (Model 3), continuous MHR levels were significantly associated with an increased risk of all-cause mortality (HR=2.10, 95% CI: 1.53–2.89, P<0.001). When analyzed by MHR tertiles, participants in the highest tertile (T3) exhibited a 34% higher risk of all-cause mortality compared to those in the lowest tertile (T1) in the fully adjusted model (HR=1.34, 95% CI: 1.03–1.75, P=0.028). No significant difference in mortality risk was observed between the middle tertile group (T2) and the lowest tertile after adjustment. Correspondingly, the linear trend test across MHR tertiles indicated a statistically significant trend for all-cause mortality risk (Model 3, P for trend = 0.032).
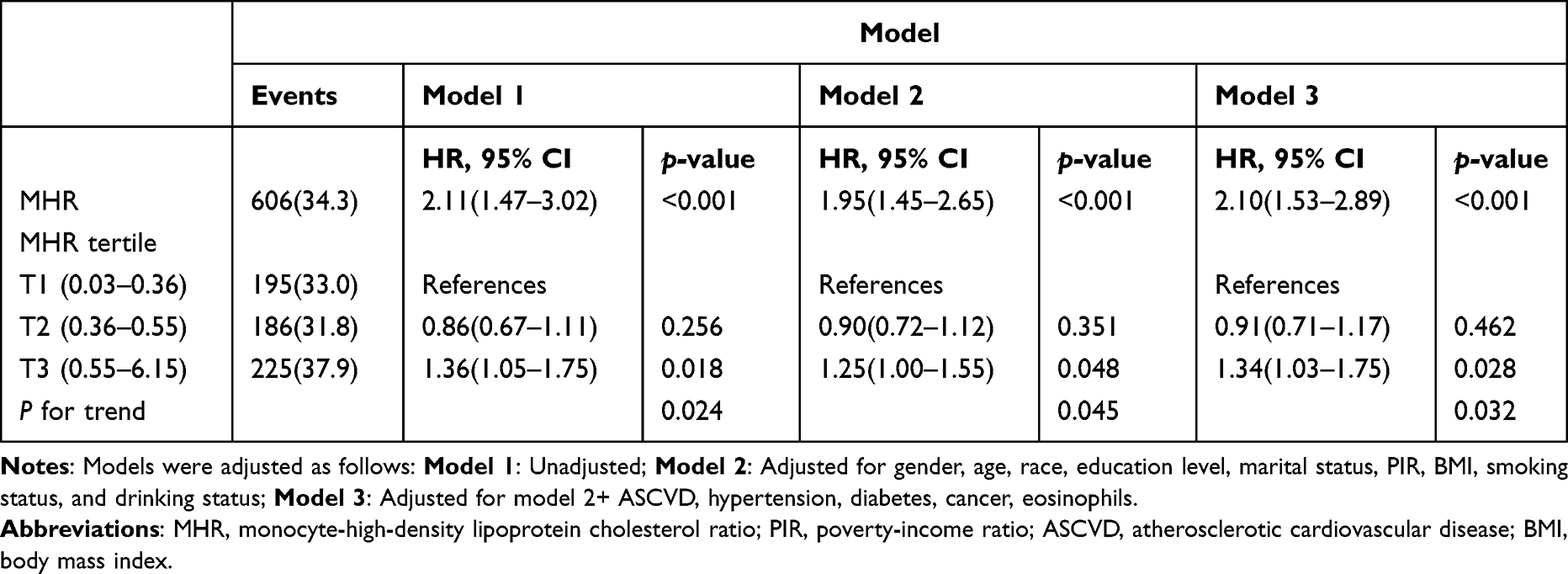 |
Table 2 Association of MHR with All-Cause Mortality in COPD Patients: Weighted Multivariate Analysis |
Kaplan–Meier survival curves (Figure 2) visually demonstrated differences in all-cause mortality among MHR tertile groups, with the highest tertile showing the lowest survival probability. The Log rank test indicated a statistically significant difference among the three groups (p = 0.002).
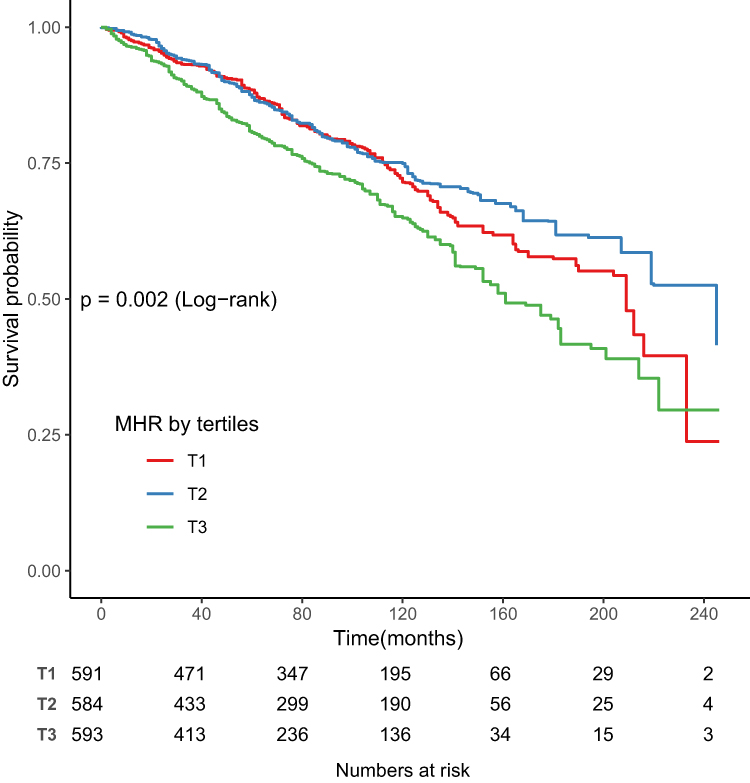 |
Figure 2 Kaplan–Meier survival curves for all-cause mortality by tertiles of MHR (T1–T3). Group differences were tested using the Log rank test. |
Detection of Nonlinear Relationships
To thoroughly investigate the specific association pattern between MHR and mortality risk, we employed RCS regression to develop both unadjusted and multivariable-adjusted models. As shown in Figure 3A, the RCS curve from the unadjusted model revealed a significant nonlinear association between MHR and all-cause mortality risk, which remained significant after multivariable adjustment (Figure 3B; P for nonlinearity = 0.004). Further threshold effect analysis (Table 3) identified a turning point at an MHR of 0.29: below this value, mortality risk was significantly decreased (adjusted HR = 0.02, 95% CI: 0.00–0.32, P = 0.006); above this threshold, the risk increased markedly (adjusted HR = 2.52, 95% CI: 1.93–3.29, P < 0.001). Likelihood ratio tests yielded P values less than 0.001, indicating that segmented threshold models better capture the complex nonlinear relationship between MHR and mortality risk than simple linear models.
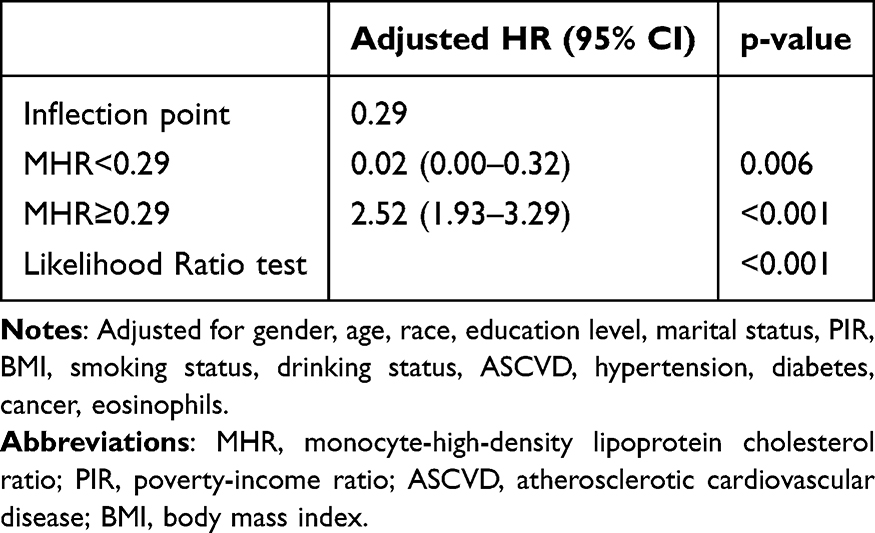 |
Table 3 Threshold Effect Analysis of MHR on All-Cause Mortality in Participants with COPD |
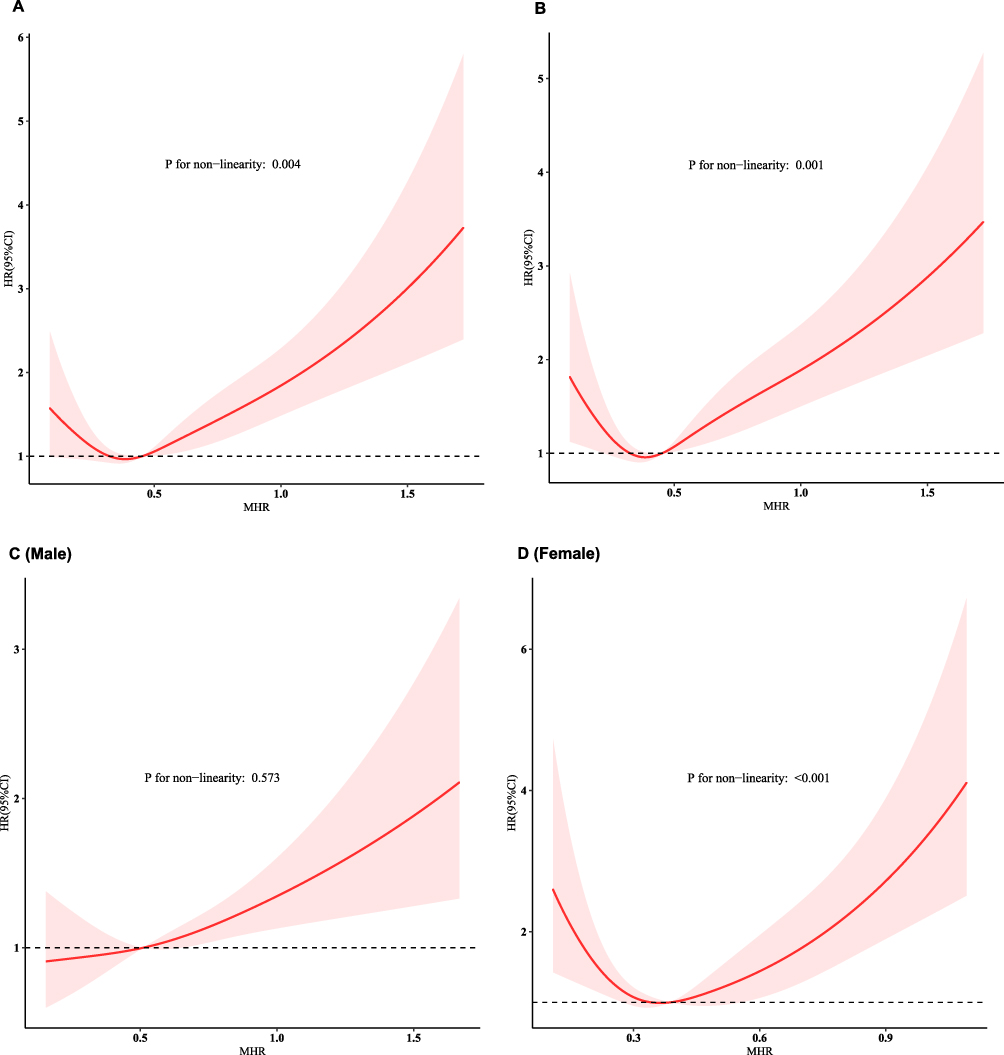 |
Figure 3 Restricted cubic spline visualization of weighted MHR associations with all-cause mortality among COPD patients. (A) Unadjusted mo (B) Fully adjusted model including gender, age, race, education level, marital status, PIR, BMI, smoking and drinking status, ASCVD, hypertension, diabetes, cancer, and eosinophils; (C) Male; (D) Female. The solid line represents the smooth fitted curve, with the shaded area indicating the 95% confidence interval. |
Sex-stratified analyses (Figure 3) revealed significant differences in the association patterns between MHR and mortality risk among males and females. In the male group, the RCS curve did not demonstrate a significant nonlinear relationship (nonlinearity test P = 0.573), suggesting that the association between MHR and mortality risk is more likely to be linear (Figure 3C). In contrast, the female group exhibited a significant nonlinear association (nonlinearity test P < 0.001), indicating a complex nonlinear dose-response relationship between MHR and all-cause mortality risk (Figure 3D). These results suggest that the impact of MHR on mortality risk may differ by sex, with the dynamics being more complex for females. This highlights the need for further attention to sex-specific risk management strategies.
Time-Dependent Predictive Performance of MHR for All-Cause Mortality in COPD Patients
To assess the predictive value of MHR for all-cause mortality risk over time in COPD patients, we conducted time-dependent ROC analyses. The results demonstrated that the time-dependent AUC values at 12, 36, 60, and 120 months were 0.73 (0.67–0.78), 0.79 (0.75–0.82), 0.78 (0.76–0.81), and 0.81 (0.79–0.84), respectively (Figure 4A and B). These findings indicate that MHR has strong discriminative power for short-term (12-month) mortality risk, with predictive performance showing a notable improvement as the follow-up period extends.
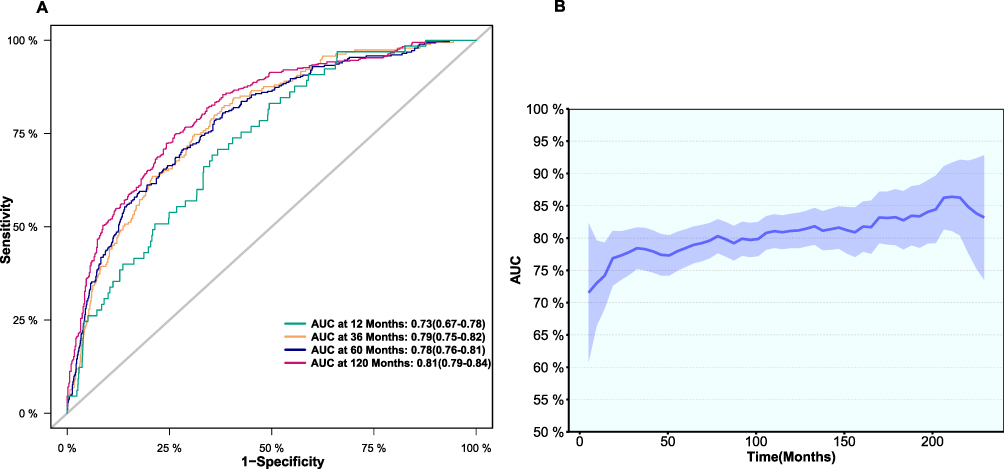 |
Figure 4 ROC Curves and Time-dependent AUCs of MHR for Mortality Risk Assessment in COPD Patients. Notes: (A) show ROC curves of MHR for all-cause mortality at 12, 36, 60, and 120 months, with corresponding AUC values and 95% confidence intervals. (B) present time-dependent AUCs throughout follow-up, with shaded areas representing 95% confidence intervals. |
Overall, MHR exhibits substantial prognostic value, particularly during longer follow-up periods, maintaining significant utility and strong discriminative capacity across all time points.
Sensitivity Analysis and Subgroup Analysis
To assess the robustness of the main findings, two sensitivity analyses were conducted. First, we used MICE multiple imputation to handle missing covariates (generating 5 datasets, analysis including N=2303), with results (Table S3) largely consistent with the association estimates in the main analysis (Table 2). Second, after excluding extreme outliers of MHR (> mean±3SD, analysis including N=1750), the re-analyzed results (Table S4) similarly showed that the direction and statistical significance of the association between MHR and mortality risk were consistent with the main analysis results. Additionally, subgroup analyses based on baseline demographic and clinical characteristics (Figure 5) aimed to explore potential heterogeneity of this association across different populations. Interaction tests showed that no stratification variable exhibited significant effect modification on the association between MHR and the risk of all-cause mortality (all P for interaction > 0.05).
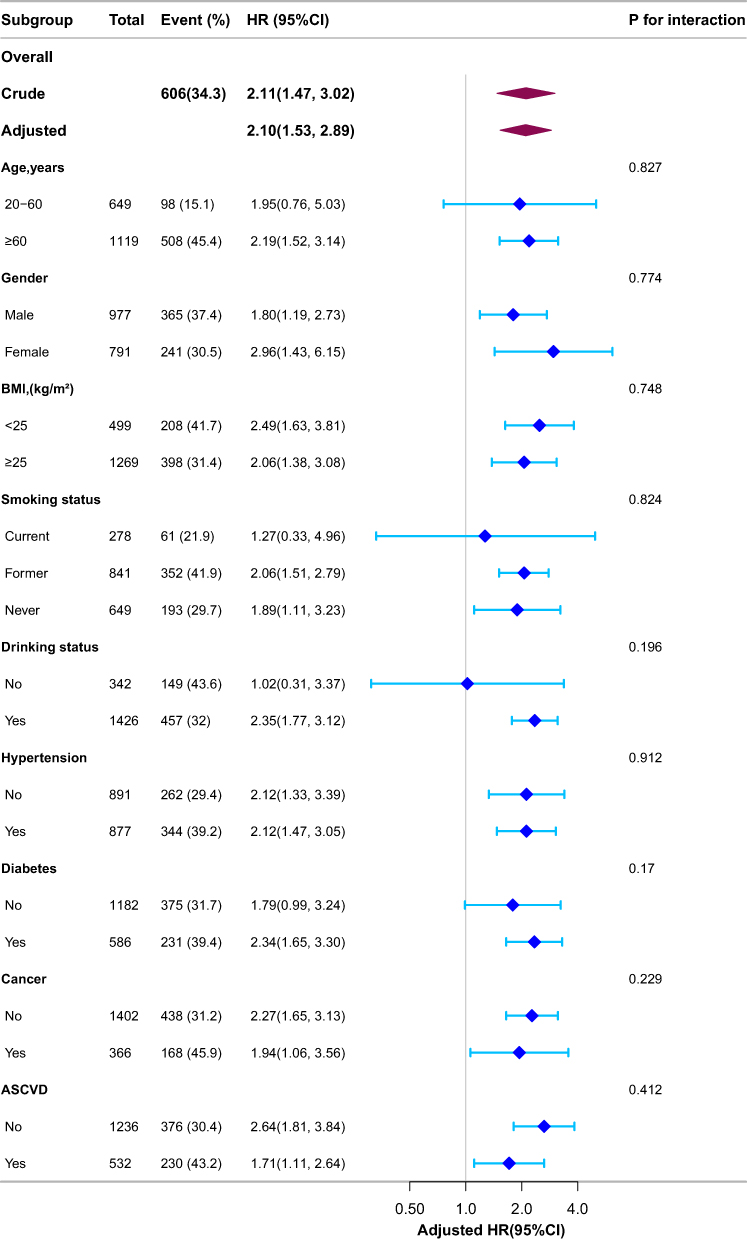 |
Figure 5 Forest plot for subgroup analysis of the weighted association between MHR and all-cause mortality in participants with COPD. Except for the stratification factor itself, subgroup analyses were adjusted for all relevant covariates. Weighted multivariate Cox proportional hazards models were used to estimate hazard ratios (HRs), with interaction p-values reported for each subgroup. |
Discussion
This study utilized data from 1,768 nationally representative participants to investigate the relationship between MHR and all-cause mortality risk in patients with COPD. The results indicated a significant positive correlation between MHR levels and mortality risk, demonstrating a nonlinear relationship: specifically, when MHR exceeded 0.29, the risk of death increased significantly, while levels below this threshold were associated with a negative correlation to mortality risk. Time-dependent ROC analysis showed that MHR has good predictive ability in the short term, with its predictive performance enhancing as follow-up time increases. Additionally, subgroup analysis suggested that the association between MHR and mortality risk may be influenced by gender, highlighting the need to consider this difference in risk management strategies. Overall, these findings indicate that MHR could be a useful and readily accessible biomarker for prognostic evaluation in patients with COPD.
The study revealed that elevated MHR levels were significantly linked to increased all-cause mortality risk in COPD patients, a finding that echoes the prognostic value demonstrated by MHR in other clinical fields.6,8,27,28 For instance, studies on patients with acute myocardial infarction have shown that MHR at admission can serve as an independent indicator for predicting long-term survival rates, with higher MHR indicating worse prognosis.29,30 Notably, the direction of association between MHR and mortality risk observed in our study is consistent with the recent findings by Zhang et al (2025) in an asthma population using the same NHANES dataset, who similarly reported that higher MHR was associated with increased mortality risk.13 Additionally, considering the components of MHR, our results also align with previous understanding of COPD: higher peripheral blood monocyte counts are often viewed as markers of intensified systemic inflammation and associated with poor prognosis,9,31 while lower HDL-C levels have also been confirmed to be related to poor survival status in COPD patients.32,33 Other inflammatory markers, such as C‑reactive protein (CRP), have also been linked to mortality in COPD, even in mild to moderate cases,34 further supporting the role of systemic inflammation and the potential value of MHR as an integrative prognostic indicator.
However, a key distinction in our study lies in the pattern of association between MHR and mortality risk. While Zhang et al (2025) reported a positive linear relationship between MHR and mortality in the asthma cohort,13 the present analysis identified a distinct non-linear association characteristic in the COPD population: when MHR exceeds a certain specific threshold, mortality risk shows an accelerated upward trend. This difference suggests that even within the same large population database, the manner in which MHR affects long-term survival may differ depending on the type of chronic respiratory disease.
MHR, as an integrative indicator, derives its core significance from reflecting the balance between pro-inflammatory forces and protective mechanisms in the body.12,13,35 Specifically, increased circulating monocytes are not only markers of systemic inflammation but also key drivers of atherosclerosis progression, promoting plaque formation by infiltrating the vascular wall, differentiating into macrophages, and releasing inflammatory mediators.7,36,37 On the other hand, decreased HDL-C levels, as the denominator of MHR, signify a decline in its multiple protective functions, including reduced efficiency of reverse cholesterol transport and weakened key roles in anti-inflammation, antioxidation, and maintenance of endothelial health.7,8,10 Therefore, elevated MHR essentially integrates these two unfavorable pathophysiological changes, jointly pointing to an internal environment with increased inflammatory burden and insufficient vascular protection, providing a biological basis for understanding its association with adverse clinical outcomes.
Previous population-based studies have also reported that MHR is associated with all-cause mortality independent of conventional risk factors. 6,8,13 In this context, our findings further highlight the specific relevance of MHR in the COPD population, where chronic inflammation and lipid metabolism abnormalities coexist and may amplify its prognostic significance. The association between high MHR and increased mortality risk in COPD patients observed in this study highly aligns with the above biological mechanisms. Against the backdrop of inherent chronic inflammation in COPD patients,9 the pro-inflammatory/protective imbalance indicated by elevated MHR35 may exacerbate systemic inflammation and accelerate the development of complications such as atherosclerosis,38 thereby explaining the observed increased risk, which is consistent with the prognostic value of MHR in other chronic inflammation-related diseases.7,13,35 Particularly noteworthy is the finding of a significant non-linear relationship between MHR and mortality risk, suggesting that its impact may not be a simple dose accumulation, but rather involves a critical threshold or turning point. After MHR exceeds this threshold, mortality risk accelerates, perhaps reflecting the failure of bodily compensatory mechanisms, depletion or qualitative changes in protective pathways (such as HDL function),10,32 or inflammatory cascade reactions entering an uncontrolled amplification state.36–38 The identification of this non-linear characteristic deepens our understanding of the complex role of MHR in COPD and emphasizes that in clinical risk assessment, attention to specific MHR levels and whether they exceed certain thresholds may be more valuable for guidance than simple categorization. Future research needs to focus on elucidating the precise molecular mechanisms behind this nonlinear pattern.
This study revealed a significant association between MHR and all-cause mortality risk in COPD. Overall analysis demonstrated a nonlinear relationship between MHR and mortality risk. Notably, subgroup analysis by sex indicated that, in males, the association between MHR and mortality risk was more linear, with no significant non-linear relationship observed (P = 0.573), suggesting a more direct relationship between increasing MHR and elevated mortality risk in the progression of COPD.13 In contrast, the non-linear association between MHR and all-cause mortality risk was more pronounced in females (P < 0.001), indicating that the relationship may be influenced by additional factors, potentially related to the effects of sex hormones such as estrogen, which play a complex role in modulating inflammation and immune responses,39–41 leading to more complex changes in mortality risk at similar MHR levels in female COPD patients.42,43 Therefore, risk management strategies for COPD patients should consider the non-linear relationship between MHR and mortality risk, and further research is warranted to validate the impact of sex differences. By integrating MHR levels with relevant clinical characteristics, we can potentially predict all-cause mortality risk in COPD patients more accurately, thus providing a stronger basis for personalized treatment approaches.
The core strength of this study lies in its reliance on NHANES, a large, nationally representative population cohort resource, and its integration of reliable long-term mortality outcome data, thereby systematically examining the previously less-explored non-linear association pattern between MHR and COPD mortality risk. However, interpretation of the study results still requires careful consideration of its inherent limitations. First, the observational design of the study inherently limits causal inference; the observed association between increased MHR and elevated mortality risk does not necessarily equate to a direct pathophysiological driving effect. Second, our analysis is based on baseline MHR levels at a single time point, failing to capture the dynamic trajectory of this indicator over time and its cumulative impact on long-term prognosis. Third, despite adjustments for multiple covariates, the risk of residual confounding remains, such as lifestyle factors, specific therapeutic interventions, or fine clinical phenotypes of COPD that are either unmeasured or typically lack detail in NHANES data, all of which may potentially interfere with the observed associations.
Conclusion
This study, based on analysis of the nationally representative NHANES data, demonstrates that MHR is significantly associated with all-cause mortality risk in COPD patients. Importantly, this association exhibits a nonlinear pattern, with mortality risk accelerating after MHR levels exceed specific thresholds. This finding suggests that MHR may be a valuable, easily accessible indicator for COPD prognostic assessment, particularly in identifying high-risk individuals, though its clinical application value still awaits further validation and mechanistic elucidation by future research.
Data Sharing Statement
The datasets relevant to this study are available for access on the NHANES website (https://www.cdc.gov/nchs/nhanes/index.htm).
Ethics Approval and Consent to Participate
In accordance with Article 32, items 1 and 2 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (issued on February 18, 2023), research using publicly available or anonymized data is exempt from ethical review. This study used data from the publicly available NHANES, whose protocols were approved by NCHS Ethics Review Committee. All participants provided informed consent, and the data analyzed are fully anonymized and contain no sensitive personal information; therefore, no additional local institutional ethics approval was required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Key Developmental Program of Bozhou City (bzzc2024017), the School Fund of Anhui Medical University (2023xkj199), and Anhui Provincial Health and Scientific Research Project (AHWJ2023BAc20106).
Disclosure
The authors declare that they have no known competing financial or personal interests that could have appeared to influence the work reported in this paper.
References
1. GBD. Diseases and injuries collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2019;396:1204–1222. doi:10.1016/S0140-6736(20)30925-9
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2024 report. 2024. Available from: https://goldcopd.org/wp-content/uploads/2024/03/GOLD-2024-Chinese-Edition_03.04.24_WMV.pdf.
3. World Health Organization (WHO). Chronic obstructive pulmonary disease (COPD) fact sheet. 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
4. Roca J, Vargas C, Cano I, et al. Chronic obstructive pulmonary disease heterogeneity: challenges for health risk assessment, stratification and management. J Transl Med. 2014;12(Suppl 2):S3. doi:10.1186/1479-5876-12-S2-S3
5. Xu J, Zeng Q, Li S, Su Q, Fan H. Inflammation mechanism and research progress of COPD. Front Immunol. 2024;15:1404615. doi:10.3389/fimmu.2024.1404615
6. Kılıç N, Tasci G, Yılmaz S, Öner P, Korkmaz S. Monocyte/HDL cholesterol ratios as a new inflammatory marker in patients with schizophrenia. J Pers Med. 2023;13(2):276. doi:10.3390/jpm13020276
7. Romo-Cordero A, González-Sierra M, Quevedo-Abeledo JC, et al. The ratio of monocytes to HDL-cholesterol is associated with cardiovascular risk and insulin resistance in patients with rheumatoid arthritis. Life. 2023;13(10):1995. doi:10.3390/life13101995
8. Sahpolat M, Ayar D, Ari M, Karaman MA. Elevated monocyte to high-density lipoprotein ratios as an inflammation markers for schizophrenia patients. Clin Psychopharmacol Neurosci. 2021;19(1):112–116. doi:10.9758/cpn.2021.19.1.112
9. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
10. Riwanto M, Landmesser U. High density lipoproteins and endothelial functions: mechanistic insights and alterations in cardiovascular disease. J Lipid Res. 2013;54(12):3227–3243. doi:10.1194/jlr.R037762
11. Liu HT, Jiang ZH, Yang ZB, Quan XQ. Monocyte to high-density lipoprotein ratio predict long-term clinical outcomes in patients with coronary heart disease: a meta-analysis of 9 studies. Medicine. 2022;101(33):e30109. doi:10.1097/MD.0000000000030109
12. Jiang M, Yang J, Zou H, Li M, Sun W, Kong X. Monocyte-to-high-density lipoprotein-cholesterol ratio (MHR) and the risk of all-cause and cardiovascular mortality: a nationwide cohort study in the United States. Lipids Health Dis. 2022;21(1:30. doi:10.1186/s12944-022-01638-6
13. Zhang Q, Xia J, Zhuang R, Wen J, Wang C. Association between monocyte-high-density lipoprotein cholesterol ratio and mortality in a population with asthma: a cohort study. Lipids Health Dis. 2025;24(1:59. doi:10.1186/s12944-025-02484-y
14. Yakar HI, Kanbay A. Could monocyte level/HDL cholesterol ratio predict cardiovascular diseases in patients with COPD? Niger J Clin Pract. 2020;23(4):450–455. doi:10.4103/njcp.njcp_54_19
15. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. Int J Surg. 2014;12(12):1500–1524. doi:10.1016/j.ijsu.2014.07.014
16. National Center for Health Statistics. National health and nutrition examination survey: ethics review board (ERB) approval. Available from: https://www.cdc.gov/nchs/nhanes/about/erb.html?CDC_AAref_Val=https://www.cdc.gov/nchs/nhanes/irba98.htm.
17. Chen Z, Li W, Tang Y, Zhou P, He Q, Deng Z. The neutrophil-lymphocyte ratio predicts all-cause and cardiovascular mortality among United States adults with COPD: results from NHANES 1999-2018. Front Med Lausanne. 2024;11:1443749. doi:10.3389/fmed.2024.1443749
18. Agarwal S, Rokadia H, Senn T, Menon V. Burden of cardiovascular disease in chronic obstructive pulmonary disease. Am J Prev Med. 2014;47(2):105–114. doi:10.1016/j.amepre.2014.03.014
19. Llanos JP, Ortega H, Germain G, et al. Health characteristics of patients with asthma, COPD and asthma-COPD overlap in the NHANES database. Int J Chron Obstruct Pulmon Dis. 2018;13:2859–2868. doi:10.2147/COPD.S167379
20. Centers for Disease Control and Prevention (CDC). National center for health statistics. Available from: https://www.cdc.gov/nchs/data-linkage/mortality-public.htm.
21. World Health Organization (WHO). International classification of diseases, 10th Revision (ICD-10). Available from: https://icd.who.int/browse10/2019/en.
22. National Center for Health Statistics (NCHS). NHANES analytic guidelines, 2011–2018. Hyattsville, MD: Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. 2021. Available from: https://wwwn.cdc.gov/nchs/nhanes/analyticguidelines.aspx.
23. van Buuren S. Oudshoorn CGM: multivariate imputation by chained equations: MICE V1.0 user manual. 2021. Available from: https://stefvanbuuren.name/publication/2000-01-01_vanbuuren2000/.
24. Tian TL, Qu XK, Zhang HB, et al. Association between advanced lung cancer inflammation index and all-cause and cause-specific mortality among asthma patients: a cohort study. Front Nutr. 2025;12:1519271. doi:10.3389/fnut.2025.1519271
25. Zhang YB, Chen C, Pan XF, et al. Associations of healthy lifestyle and socioeconomic status with mortality and incident cardiovascular disease: two prospective cohort studies. BMJ. 2021;373:n604. doi:10.1136/bmj.n604
26. Ruan Z, Lu T, Chen Y, et al. Association between psoriasis and nonalcoholic fatty liver disease among outpatient US adults. JAMA Dermatol. 2022;158:745–753. doi:10.1001/jamadermatol.2022.1609
27. Chen J, Zhong Z, Shi D, et al. Association between monocyte count to high-density lipoprotein cholesterol ratio and mortality in patients undergoing peritoneal dialysis. Nutr Metab Cardiovasc Dis. 2021;31(7):2081–2088. doi:10.1016/j.numecd.2021.03.014
28. Bolayir A, Gokce SF, Cigdem B, et al. Monocyte/high-density lipoprotein ratio predicts the mortality in ischemic stroke patients. Neurol Neurochir Pol. 2018;52(2):150–155. doi:10.1016/j.pjnns.2017.08.011
29. Villanueva DLE, Tiongson MD, Ramos JD, Llanes EJ. Monocyte to high-density lipoprotein ratio (MHR) as a predictor of mortality and major adverse cardiovascular events (MACE) among ST elevation myocardial infarction (STEMI) patients undergoing primary percutaneous coronary intervention: a meta-analysis. Lipids Health Dis. 2020;19(1):55. doi:10.1186/s12944-020-01242-6
30. Sun M, Zhao D, Zhang Y, et al. Prognostic utility of monocyte to high-density lipoprotein ratio in patients with acute coronary syndrome: a meta-analysis. Am J Med Sci. 2020;359(5):281–286. doi:10.1016/j.amjms.2020.01.018
31. Aldonyte R, Jansson L, Piitulainen E, Janciauskiene S. Circulating monocytes from healthy individuals and COPD patients. Respir Res. 2003;4(1):11. doi:10.1186/1465-9921-4-11
32. Kotlyarov S. High-density lipoproteins: a role in inflammation in COPD. Int J Mol Sci. 2022;23(15):8128. doi:10.3390/ijms23158128
33. Zafirova-Ivanovska B, Stojkovikj J, Dokikj D, et al. The level of cholesterol in COPD patients with severe and very severe stage of the disease. Open Access Maced J Med Sci. 2016;4(2):277–282. doi:10.3889/oamjms.2016.063
34. Man SF, Connett JE, Anthonisen NR, Wise RA, Tashkin DP, Sin DD. C-reactive protein and mortality in mild to moderate chronic obstructive pulmonary disease. Thorax. 2006;61(10):849–853. doi:10.1136/thx.2006.059808
35. Ganjali S, Gotto AM, Ruscica M, et al. Monocyte-to-HDL-cholesterol ratio as a prognostic marker in cardiovascular diseases. J Cell Physiol. 2018;233(12):9237–9246. doi:10.1002/jcp.27028
36. Prame Kumar K, Nicholls AJ, Wong CHY. Partners in crime: neutrophils and monocytes/macrophages in inflammation and disease. Cell Tissue Res. 2018;371(3):551–565. doi:10.1007/s00441-017-2753-2
37. Ferrucci L, Fabbri E. Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nat Rev Cardiol. 2018;15(9):505–522. doi:10.1038/s41569-018-0064-2
38. Duru Z, Altunel O, Alabay B, et al. Elevated monocyte-to-high-density lipoprotein ratio as an indicator of systemic inflammation in patients with branch retinal vein occlusion. Beyoglu Eye J. 2021;6(3):212–216. doi:10.14744/bej.2021.94547
39. Matera MG, Ora J, Calzetta L, Rogliani P, Cazzola M. Sex differences in COPD management. Expert Rev Clin Pharmacol. 2021;14(3):323–332. doi:10.1080/17512433.2021.1888713
40. Draijer C, Hylkema MN, Boorsma CE, et al. Sexual maturation protects against development of lung inflammation through estrogen. Am J Physiol Lung Cell Mol Physiol. 2016;310(2):L166–L174. doi:10.1152/ajplung.00119.2015
41. Silveyra P, Fuentes N, Rodriguez Bauza DE. Sex and gender differences in lung disease. Adv Exp Med Biol. 2021;1304:227–258. doi:10.1007/978-3-030-68748-9_14
42. Tam A, Tanabe N, Churg A, Wright JL, Hogg JC, Sin DD. Sex differences in lymphoid follicles in COPD airways. Respir Res. 2020;21(1:46. doi:10.1186/s12931-020-1311-8
43. Barnes PJ, Burney PG, Silverman EK, et al. Chronic obstructive pulmonary disease. Nat Rev Dis Primers. 2015;1(1):15076. doi:10.1038/nrdp.2015.76
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Short-Term Oxygen Therapy Outcomes in COPD
Soumagne T, Maltais F, Corbeil F, Paradis B, Baltzan M, Simão P, Abad Fernández A, Lecours R, Bernard S, Lacasse Y
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1685-1693
Published Date: 28 July 2022
The Association of Renin-Angiotensin System Blockades and Mortality in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease and Acute Respiratory Failure: A Retrospective Cohort Study
Ruan Z, Li D, Hu Y, Qiu Z, Chen X
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2001-2011
Published Date: 1 September 2022
Effects of Low-Carbohydrate and Low-Fat Diets on Morbidity and Mortality of COPD
Hu H, Qiu Y, Shen N, Chen H, Zhang J, Wang Y, Shi X, Li M
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:2443-2455
Published Date: 16 November 2024
Association Between Advanced Lung Cancer Inflammation Index and Mortality in US Adults with Chronic Obstructive Pulmonary Disease
Su X, Rao H, Zhao C, Zhang X, Li D
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2481-2492
Published Date: 18 July 2025
Association of Weight-Adjusted Waist Index with All-Cause and Cardiovascular Mortality in Patients with Chronic Obstructive Pulmonary Disease: A Retrospective Cohort Study
Zhang X, Zhang W, Hu Y, Yang G, Liu S, Hao W, Qu Y
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3647-3658
Published Date: 11 November 2025