Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
Nonergot dopamine-receptor agonists for treating Parkinson's disease – a network meta-analysis
Authors Thorlund K ![]() , Wu P, Druyts E, Eapen S, Mills E
, Wu P, Druyts E, Eapen S, Mills E
Received 3 January 2014
Accepted for publication 3 March 2014
Published 7 May 2014 Volume 2014:10 Pages 767—776
DOI https://doi.org/10.2147/NDT.S60061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Kristian Thorlund,1,2,4 Ping Wu,3,4 Eric Druyts,3,4 Shawn Eapen,3,4 Edward J Mills2–4
1Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, ON, Canada; 2Stanford Prevention Research Center, Stanford University, Stanford, CA, USA; 3Faculty of Health Sciences, University of Ottawa, Ottawa, ON, Canada; 4Redwood Outcomes, Vancouver, BC, Canada
Objective: To compare the efficacy of the three nonergot dopamine-receptor agonists (DAs) pramipexole, ropinirole, and rotigotine for the treatment of early and advanced Parkinson's disease (PD).
Materials and methods: Bayesian network meta-analyses were performed separately for early and advanced PD, and at time points 11–16 and 24–28 weeks. Outcomes for early PD included improvement on the Unified Parkinson's Disease Rating Scale (UPDRS) activities in daily life (UPDRS-II), motor function (UPDRS-III), and their subtotal (UPDRS-II + III). Outcomes for advanced PD also included daily “off time” (hours), but not UPDRS-II + III.
Results: Totals of 23 and 24 trials informed early and advanced PD analyses. For early PD UPDRS-II at 11–16 weeks, pramipexole and rotigotine were statistically significantly superior to placebo, but ropinirole was not. For UPDRS-III and UPDRS-II + III, all DAs were statistically significantly better than placebo and exhibited similar improvements. At 24–28 weeks, results were also statistically significant for all DAs versus placebo, and the magnitudes of improvements were similar for pramipexole, ropinirole and rotigotine. Advanced PD improvements on UPDRS-II, UPRDS-III, and off time were statistically significant for pramipexole, ropinirole, and rotigotine versus placebo. At 11–16 weeks, rotigotine yielded slightly smaller effects than ropinirole and pramipexole, but credible intervals on differences were wide. For off time, results were near identical. At 24–28 weeks, results were similar for all three outcomes. Ropinirole yielded a slightly higher improvement on UPDRS-III, but a slightly smaller improvement in off time.
Conclusion: Our analyses suggest that pramipexole, ropinirole, and rotigotine exhibit similar efficacy in the treatment of early and advanced PD.
Keywords: Parkinson's disease, dopamine-receptor agonists, network meta-analysis
Background
Parkinson’s disease (PD) is a progressive neurodegenerative disorder that affects about 10 million people worldwide annually.1,2 PD is characterized by movement-related symptoms, such as bradykinesia, dyskinesia, rigidity, and tremor.1 Over time, PD may also cause symptoms of depression and dementia.1 The disease can therefore have a severe impact on patients’ quality of life, especially at its later stages (ie, moderate-to-severe PD).
Currently, no cure exists for PD, but a number of pharmacological therapies have been shown to suppress key disease-related symptoms, and possibly delay progression to later stages of the disease. Conventional first-line treatment for PD is levodopa, a precursor to the neurotransmitter dopamine, which can cross the protective blood–brain barrier and increase dopamine concentrations. In the central nervous system, levodopa is converted into dopamine by the DOPA decarboxylase. However, the peripheral conversion of levodopa into dopamine can often cause long-term permanent adverse effects (eg, motor fluctuations or dyskinesia).3,4 For this reason, levodopa is typically coadministered with a peripheral DOPA decarboxylase inhibitor (DDCI), such as carbidopa or benserazide, which counterintuitively has been demonstrated to improve levodopa treatment considerably. However, long-term adverse events still remain with the addition of DDCI, and for this reason some recommend putting off levodopa treatment as long as possible.5
Early stage levodopa-naïve PD patients may therefore receive other active agents, and levodopa-experienced patients may be switched to these agents. Other agents may also be useful in advanced-stage PD patients as adjuvant therapy to levodopa, when the effects of levodopa have started to fade. Dopamine-receptor agonists (DAs) are a viable alternative to levodopa in early stage PD patients, as well as a commonly used adjuvant therapy in advanced-stage PD patients.6 The first generation of DAs, the ergot DAs, are not commonly used in practice, due to firm evidence of increased risk of valvular heart disease.7 Second-generation DAs, the nonergot DAs, are now the conventional choice. It has been shown that initiating therapy with nonergot DAs reduces the risk of motor-complication development at later stages (in contrast to levodopa). However, some controversy remains, since DAs do not produce dopamine in the striatum (as levodopa does), and thus potentially this leads to destruction of the substantia nigra, resulting in an attenuation of the effect of levodopa if initiated at a later stage.
Few randomized clinical trials (RCTs) and systematic reviews have established the efficacy and safety of DAs as alternative treatments to levodopa in early stage PD patients and as adjuvant therapy to levodopa in advanced-stage PD patients.8,9 No analysis to date has investigated whether these therapies exhibit similar efficacy profiles, or whether some therapies work better than others. For this reason, network meta-analysis was undertaken to explore the comparative efficacy of the available nonergot DAs – rotigotine, ropinirole, and pramipexole – on key efficacy outcomes. The comparative efficacy of the three nonergot DAs was established at two time points after completed dose titration: 11–16 weeks and 24–28 weeks.
Materials and methods
Eligibility criteria
We considered the patients, experimental interventions, control interventions, and outcomes (PICO) outlined in the PICO statement presented in Table 1. Separately, we considered patients diagnosed with early and advanced (late) PD who were treatment-naïve to the treatment class being investigated. According to Hoehn and Yahr, a score of less than 3 is early PD, and a score of 3 or more is advanced PD. However, we left this definition to the discretion of the individual trial investigators. The experimental interventions of interest were pramipexole, ropinirole, and rotigotine (nonergot DAs). The control interventions were the older ergot DAs and placebo/levodopa/levodopa + DDCI. Any RCT comparing at least two of these was considered.
 | Table 1 Types of patients, interventions, controls, and outcomes (PICO) considered for the proposed study |
Search strategy
With the assistance of a medical librarian, a search strategy was developed, and a systematic search of the medical literature was conducted using Medline, Embase, and the Cochrane Controlled Trials Register. The database-search strategy was sensitive and broad, utilizing a collection of search terms previously used in published systematic reviews of pharmacotherapies for PD.8,9 The Medline search algorithm is presented in the Supplementary material. Lastly, the bibliographies of all identified relevant studies were used to perform a recursive search of the literature. Articles were independently assessed by two reviewers using predesigned eligibility forms, according to prospectively defined eligibility criteria. There were no language restrictions.
Data extraction
All identified abstracts were scanned in by two pairs of reviewers (KT and PW; and ED and SE) to determine if they met the eligibility criteria. Disagreement was resolved by discussion, and if no agreement could be met, by a third adjudicator (EJM). Data extraction was also conducted independently and in duplicate by two pairs of reviewers (KT and PW; and ED and SE) with disagreement resolved through a third adjudicator (EJM).
Extracted variables
Among the eligible RCTs, a number of variables related to the study design, interventions, and patient characteristics were extracted. For the study design, the following variables were extracted: patient-eligibility criteria, definition of PD, and number of patients and centers. For the interventions, the following variables were extracted: dosage, duration and route of administration for all active and control intervention, allowed cointerventions, and proportion of patients on allowed cointerventions. For patient baseline characteristics, the following variables were extracted: age, proportion of females, disease duration, treatment history, proportion suffering from concomitant neurodegenerative disorders, proportions of patients suffering from other disease-related disorders (eg, proportion suffering from depression, proportion suffering from dementia), and Unified Parkinson’s Disease Rating Scale (UPDRS) scores and UPDRS-domain scores. All patient baseline characteristics were extracted for each intervention arm. Further, all of the outcomes were extracted at all time points between 11 weeks and 28 weeks (after completion of dose titration).
Analyses
Imputation of standard errors
Because the intervention group standard errors (SEs) were not reported in many of the identified trials, these were either approximated from the reported statistics or imputed. In particular, when the variance, standard deviation (SD), or SE of the difference between groups was reported, the intervention-group SE was calculated assuming equal SDs in the two groups. Similarly, when only P-values were reported for the difference between two groups, the SE of the mean difference was first derived, and subsequently the intervention-group SEs were approximated, assuming equal SDs across groups. Where the SE, SD, or variance was only reported at one time point, the same value was imputed for the remaining time points. Lastly, where no data were available to calculate the SE, the median across other trial intervention-group SEs (reported and approximated) was imputed.
Statistical analysis
Network meta-analyses using a Bayesian approach were performed for early PD and advanced PD.10–12 These analyses were performed for both “shorter duration” and “longer duration”. Here, two categories were used. The shorter-duration outcomes were defined as those reported after 11 and 16 weeks of treatment (excluding titration period). The longer-duration outcomes were defined as those reported 24–28 weeks of treatment (excluding titration period). For early PD, analyses were performed on change from baseline on the UPDRS-II, UPDRS-III, and UPDRS-II + III. For advanced PD, analyses were performed on change from baseline on UPDRS-II, UPDRS-III, and reduction from baseline in “off time” (hours/daily).
All of the considered outcomes were continuous, and for that reason, the employed effect measure in all Bayesian network meta-analysis models was the mean difference (MD), which is the difference between the mean change from baseline in two intervention groups (ie, the difference between the mean responses in the two intervention groups). MDs were produced for all comparisons between nonergot DAs and placebo, and estimation uncertainty was represented with 95% credible intervals (CrIs; the Bayesian equivalent of conventional frequentist confidence intervals [CIs]). RCTs reporting continuous data may report either intervention-group mean responses or the calculated mean differences. To account for differences in reporting, the shared-parameter model, outlined in the National Institute for Health and Clinical Excellence technical support document 2, was employed.11 This approach allows for network meta-analyses fully integrating the data in its originally reported format (ie, either intervention-group mean responses or calculated MDs), rather than forcing recalculation of group mean responses to MDs.
For all outcomes, the control-group mean responses were modeled from a normal distribution with a population mean and variance, representing a random-effect “control response” between trials. When two controls existed (ie, placebo and levodopa), each control was modeled via two separate normal distributions, representing two random-effect terms in the model. MDs between interventions were assumed to follow normal distributions, and unexplained between-trial heterogeneity on the mean difference was accounted for using a conventional Bayesian random-effect model. Normal distributions with mean 0 and variance 10,000 were used as noninformative prior distributions for the control-response and MD parameters. For the between-trial standard deviations for control-response and MD parameters, uniform distributions between 0 and 5 were assigned as noninformative priors. Considering the range of values that the control responses and MDs fell within, these priors carries very little information for between-trial heterogeneity estimation. All statistical analyses were conducted in WinBUGS version 1.4.3 (BUGS Project, Cambridge, UK).13 The WinBUGS code and data sets are available from the authors upon request.
Scenario analysis for UPDRS-II + III in early PD
In a key RCT on early PD patients by Giladi et al14 comparing rotigotine to ropinirole, the reported UPDRS-II + III response with ropinirole was substantially higher than that observed in other trials, which led to concerns about including this trial. In three other identified ropinirole trials of similar patient populations and study duration (Rascol et al,15 Singer et al,16 and Watts et al17) the UPDRS-II + III improvements were highly homogeneous, and ranged from 5.20 to 7.52. By contrast, the reported improvement on UPDRS-II + III in the Giladi et al trial was 11.0. A forest plot of the ropinirole arm UPDRS-II + III responses from the four trials visually shows clear heterogeneity between Giladi et al and the other three trials, and the estimated degree of heterogeneity across the four trials, I2=90% (95% CI 76%–95%), was high. By contrast, a forest plot of the three trials by Rascol et al,15 Singer et al,16 and Watts et al17 visually suggests no or very little heterogeneity, and the estimated degree of heterogeneity across the three trials, I2=0 (95% CI 0%–73%), with the upper bound of the CIs lying below the lower bound of the confidence interval from the forest plot, including Giladi et al. Collectively, these heterogeneity assessments raise concern about the validity of including the trial by Giladi et al. For this reason, our primary analysis excluded the trial by Giladi et al, but a second scenario analysis included the trial by Giladi et al. Lastly, to test the robustness of the SD imputations, we conducted sensitivity analyses excluding all trials where full imputation was performed (ie, only those where no other trial statistics were available to approximate the SE).
Results
Summary of the evidence base
For early PD, a total of 23 trials were included,14–36 of which 20 trials informed the analysis for the 11- to 16-week time point,15,16,18–28,30–36 and eleven trials informed the analyses for the 24- to 28-week time point.14–17,19–21,28–30,33 Two trials compared two nonergot DAs head to head,14,27 while indirect evidence for the comparison of DAs was available from trials comparing any of the nonergot DAs with placebo, with levodopa + DDCI, and with ergot DAs (Figure 1). For advanced PD, a total of 22 trials were included,38–59 of which 13 trials informed the analysis for the 11- to 16-week time point,38,39,41–44,46,47,50,53,57–559 and 13 trials informed the analyses for the 24- to 28-week time point.40,42,44,45,48–52,54–57 One trial compared two nonergot DAs head to head,18 while indirect evidence for the comparison of DAs was available from trials comparing any of the nonergot DAs with levodopa + DDCI and with ergot DAs (Figure 2). An overview of included trials for early PD and advanced PD, and the outcomes and time points informed by each of these trials, are presented in the Supplementary material. The treatment networks for each of the outcomes in the early PD and advanced PD analyses are presented in Figures 1 and2, respectively. Note that although some RCTs that included levodopa only (ie, no DDCI) were identified, none of these collectively contributed any indirect evidence, and so they were excluded.
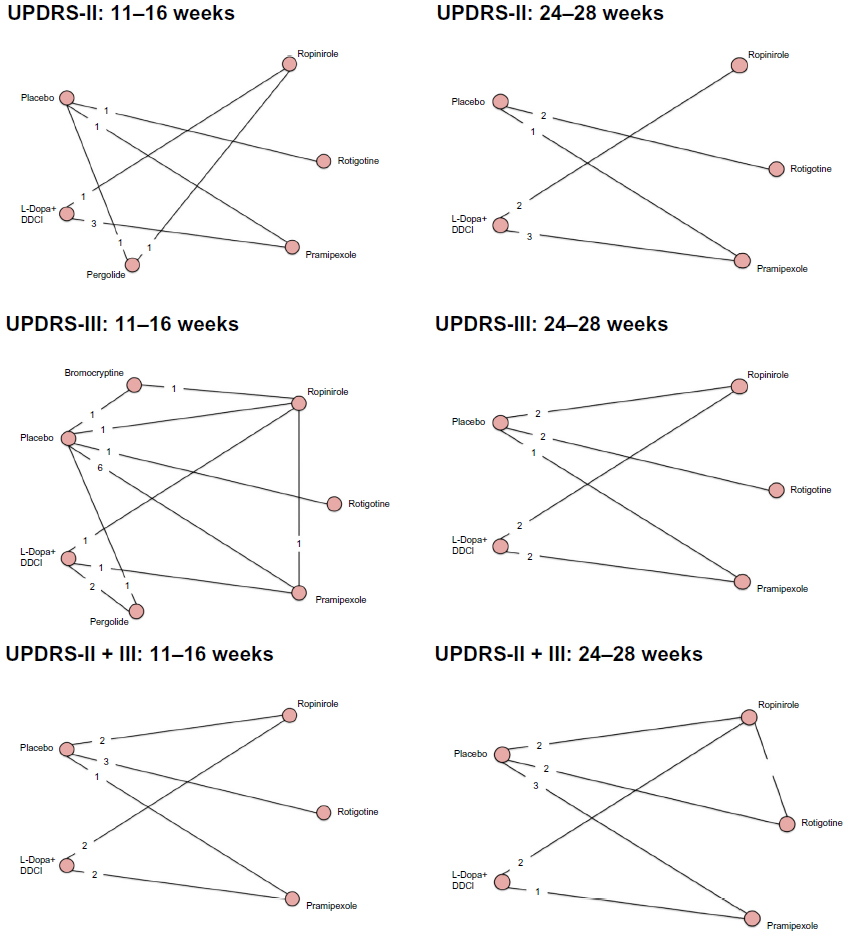 | Figure 1 Treatment networks for the three outcomes at the two time points for early Parkinson’s disease. The circles (nodes) represent each of the interventions where randomized clinical trial (RCT) data were available for the particular outcome. The lines between circles show which pair-wise comparisons were informed by RCTs, and the numbers on the lines show the number of RCTs informing a particular comparison. |
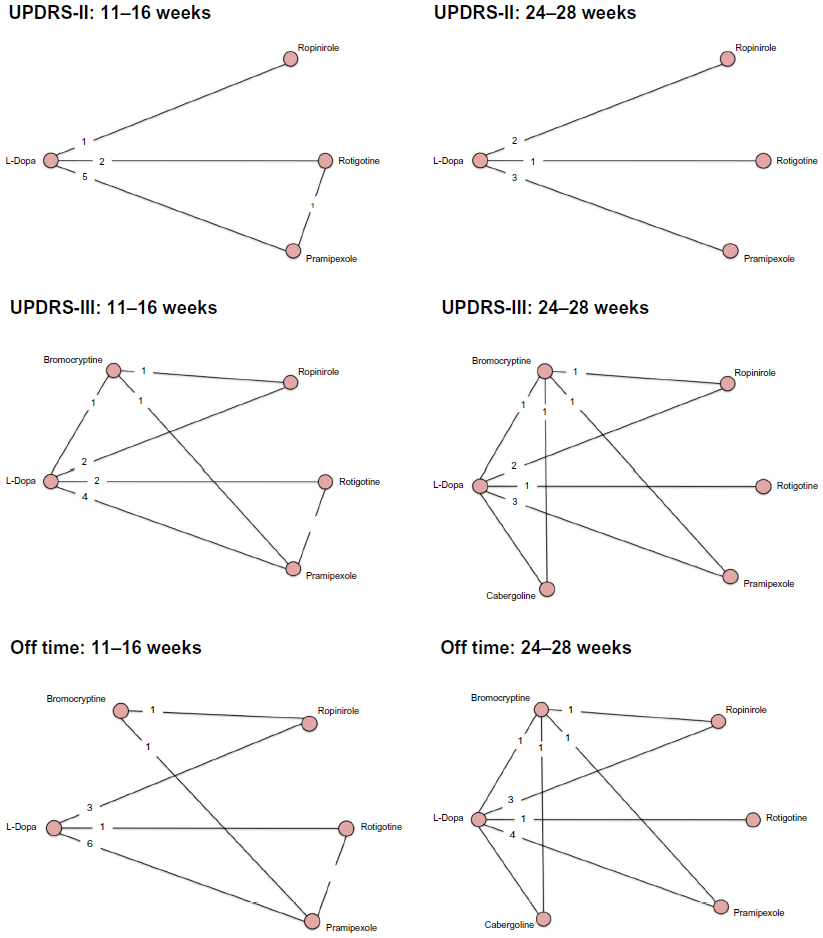 | Figure 2 Treatment networks for the three outcomes at the two time points for advanced Parkinson’s disease. The circles (nodes) represent each of the interventions where randomized clinical trials (RCT) data was available for the particular outcome. The lines between circles show which pair wise comparisons were informed by RCTs, and the number in the lines show the number of RCTs informing a particular comparison. |
Summary of patient and treatment characteristics
The included trials were similar in terms of key patient characteristics (eg, age, disease duration, disease severity) (Supplementary material). For both early PD and advanced PD, the average age generally fell within 60–65 years, with SDs indicating a patient population of ages ranging from 50 to 75 years. For early PD patients, the average PD duration was 1–2 years, with SDs indicating a patient population ranging from <1 year to about 5 or 6 years. Patients’ disease severity according to Hoehn and Yahr staging generally fell at stages I or II, with only a minor proportion of patients being staged at III. For advanced PD patients, the average PD duration generally fell within 4–10 years, but with SDs indicating a patient population ranging from 2 years’ PD history to up to 15 or 20 years’ history. Patients’ disease severity according to the Hoehn and Yahr was, on average, larger than 2.5, with a large proportion of patients being at PD stage III or above. For both early PD and advanced PD patients, doses of administered DAs as well as backbone levodopa (+ DDCI) varied moderately (Supplementary material). Allowed background medication (eg, concomitant deprenyl or anticholinergics) and the proportions of patients receiving such medications also varied, and for many trials were not well reported.
Results of the network meta-analysis
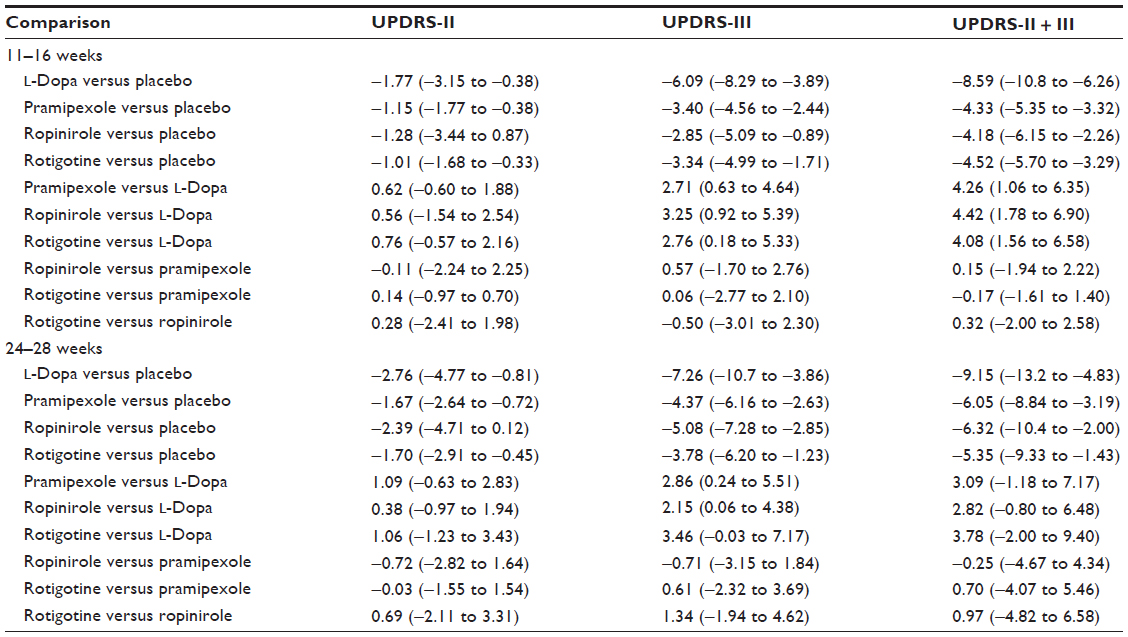
Table 2 presents the network meta-analysis results for early PD patients. For all outcomes and time points, pramipexole, ropinirole, rotigotine and levodopa (+ DDCI) compared with placebo yielded “statistically significant” MDs (ie, 95% CrIs did not overlap 0.00), with the exception of ropinirole versus placebo for UPDRS-II. For UPDRS-II at the 11- to 16-week time point, mean improvements associated with pramipexole, ropinirole, and rotigotine (the three DAs) were similar, ranging from −1.01 (rotigotine) to −1.28 (ropinirole). Levodopa was associated with a slightly higher mean improvement of −1.77, and 95% CrIs were overlapping for all interventions. For UPDRS-III at the 11- to 16-week time point, mean improvements associated with the three DAs were similar, ranging from −2.85 (ropinirole) to −3.40 (pramipexole). Levodopa was associated with a substantially higher mean improvement of −6.09, which was significantly better than all DAs. For the subtotal of UPDRS-II + III at the 11- to 16-week time point, mean improvements associated with the three DAs were also similar, −4.18 (ropinirole) to −4.52 (rotigotine), and levodopa was associated with mean improvement of −8.59 (again, significantly better than all DAs).
 | Table 2 Analysis of early Parkinson’s disease population |
For UPDRS-II at the 24- to 28-week time point, mean improvements associated with the three DAs were similar, ranging from −1.67 (pramipexole) to −2.39 (ropinrole).Levodopa was associated with a slightly higher mean improvement of −2.76, and 95% CrIs were overlapping for all interventions. For UPDRS-III at the 24- to 28-week time point, mean improvements associated with the three DAs were similar, ranging from −3.78 (rotigotine) and −4.37 (pramipexole) to −5.18 (ropinirole). Levodopa was associated with a higher mean improvement of −7.26, and levodopa was significantly superior to pramipexole and ropinirole, and marginally significantly superior to rotigotine. For the subtotal of UPDRS-II + III at the 24- to 28-week time point, mean improvements associated with the three DAs were also similar, ranging from −5.35 (rotigotine) to −6.32 (ropinirole). Levodopa was associated with mean improvement approximately 50% larger than that of the DAs, but CrIs were wide. Under the scenario analysis including the trial by Giladi et al, the mean improvement of pramipexole was relatively unchanged at 6.18 (95% CrI −8.79 to −3.50), the mean improvement associated with ropinirole increased to −7.11 (95% CrI −10.1 to −4.00), and the mean improvement associated with rotigotine decreased to −5.02 (95% CrI −8.52 to −1.50). For all early PD analyses, sensitivity analyses excluding all trials with fully imputed SDs excluded a maximum of two trials per analysis (but generally zero or one), and did not have a notable impact on results.
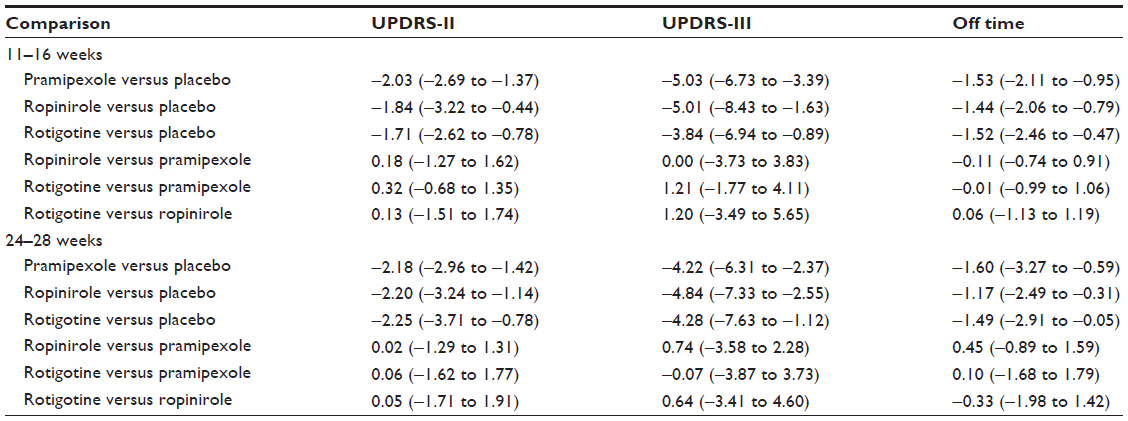
Table 3 presents the network meta-analysis results for advanced PD patients. For all outcomes and time points, pramipexole, ropinirole, rotigotine compared with placebo yielded statistically significant mean differences. For UPDRS-II at the 11- to 16-week time point, mean improvements associated with pramipexole, ropinirole, and rotigotine were similar, ranging from −1.71 (rotigotine) to −2.03 (pramipexole). For UPDRS-III at the 11- to 16-week time point, mean improvements associated with the three DAs were similar, ranging from −3.84 (rotigotine) to −5.03 (pramipexole). For off time at the 11- to 16-week time point, mean improvements associated with the three DAs were also similar, ranging from −1.44 (ropinirole) to −1.52 and −1.53 for pramipexole and ropinirole, respectively.
 | Table 3 Analysis of advanced Parkinson’s disease population |
For UPDRS-II at the 24- to 28-week time point, mean improvements associated with the three DAs were similar, ranging from −2.18 (pramipexole) to −2.25 (rotigotine). For UPDRS-III at the 24- to 28-week time point, mean improvements associated with the three DAs were similar, ranging from −4.22 (pramipexole) to −4.84 (ropinirole). For off time at the 24- to 28-week time point, mean improvements associated with the three DAs were also similar, ranging from −1.17 (ropinirole) to −1.60 (pramipexole). For all advanced PD analyses, sensitivity analyses excluding all trials with fully imputed SDs excluded a maximum of two trials per analysis (but generally zero or one), and did not have a notable impact on results.
Discussion
The results of our network meta-analysis suggest that compared with placebo, the three nonergot DAs pramipexole, ropinirole, and rotigotine are all equally effective in improving activities in daily life (UPDRS-II), motor function (UPDRS-III), and reducing daily hours of off time (analyzed for advanced PD only). Our analysis also suggests that for patients with early PD, levodopa + DDCI provides greater improvement in motor function than nonergot DAs. However, there was statistical evidence to suggest that levodopa + DDCI provides greater benefit on activities in daily life.
The conducted network meta-analyses results come with a number of strengths and limitations. Our extensive literature search ensured the inclusion of all relevant RCTs, and a detailed trial-eligibility evaluation ensured that the RCTs were highly comparable in terms of patient populations and baseline characteristics. Our analyses gain clinical relevance in that we looked at both early and advanced PD. Furthermore, the robustness of results was checked in a number of scenario analyses taking out potential outliers. The homogeneity across trials was improved by separating results into narrow time intervals. However, a few of the outcomes within each time interval were only sparsely informed, and thus were associated with wide CrIs. The similarity of key trial characteristics was checked to ensure that it was reasonable to combine them in a network meta-analysis. Unfortunately, limited data were available on the proportion of patients receiving concomitant therapies (eg, percentage of patients concomitantly on deprenyl), as well as patients’ prior use of levodopa and other agents. As such, it was not possible to examine the influence of these variables on treatment effects directly. Visual inspection of the data available on concomitant medication suggests some nonnegligible variation between trials. This raises some concerns about confounding. However, it is important to remember that DAs compared with other medications target different pathways or points on the pathophysiological cascade leading to PD symptoms, and thus would still exhibit an effect regardless of current concomitant medications. Therefore, the expected degree of confounding is likely negligible.
The findings of our network meta-analyses are generalizable to patients who share characteristics similar to those randomized in the included trials, and patients receiving similar doses of the considered interventions to those administered in the included trials. In particular, in early PD patients, the similar efficacy of pramipexole, ropinirole, and rotigotine on activities in daily life and motor function, as well as the superiority of levodopa on motor function, can be expected whenever these are administered within the dose ranges that are common in the clinical trials. Further, similar efficacy can be expected in patients of age approximately 45–75 years, who have generally not been diagnosed with PD for longer than 4 years, and whose disease severity generally corresponds to Hoehn and Yahr staging below III. For advanced PD, similar efficacy of pramipexole, ropinirole, and rotigotine can be expected whenever these are administered within the dose ranges that are common in the clinical trials. Additionally, similar efficacy can be expected in patients of age approximately 45–75 years, who have generally been diagnosed with PD for about 4–10 years (but ranging up to 20 years) and whose disease severity generally corresponds to Hoehn and Yahr staging above 2.5 (ie, 3 or above).
Due to the large number of efficacy outcomes assessed in this study, we did not consider adverse events. Future network meta-analyses comparing DAs, levodopa and potentially other agents should also consider safety issues. Our network meta-analysis, therefore, has merit in informing the efficacy part of clinical practice decision making, but other sources of evidence, such as systematic reviews reporting on safety issues, should be considered in this equation. This is particularly important for the comparison of DAs with levodopa, due to the long-term adverse effects commonly known to be associated with levodopa.
Overall, our network meta-analyses suggest the three nonergot dopamine receptor agonists pramipexole, ropinirole, and rotigotine exhibit similar if not equal efficacy over time for the important outcomes activity in daily life, motor function for patients with early and advanced PD, and off time for patients with advanced PD.
Disclosure
KT and EJM have previously consulted with Merck, Pfizer, Novartis, Janssen, and Gilead on systematic review issues. In addition, they have received grants from the Canadian Institutes of Health Research (CIHR) and been consultants to the Canadian Agency for Drugs and Technology in Health and the US Agency for Healthcare Research and Quality (AHRQ). KT’s salary is supported by CIHR. EJM’s salary is supported by a CIHR Canada Research Chair. ED, PW, and SE have no conflicts of interest to report. The authors originally prepared this study as a health-technology assessment (HTA) report submission for UCB Canada Inc., and subsequently rewrote the report into a manuscript. Funding for the HTA report was provided by UCB Canada Inc. The authors had full and independent control over the methods, analyses, and preparation of the HTA report, and UCB Canada had no role in the preparation of the manuscript.
References
National Institute for Health and Clinical Excellence. Parkinson’s disease: diagnosis and management in primary and secondary care. 2006. Available from: http://www.nice.org.uk/CG035 Accessed March 19, 2011. | |
Parkinson’s Disease Foundation. Statistics on Parkinson’s. Available from: http://www.pdf.org/en/parkinson_statistics Accessed July 26, 2013. | |
Sweet RD, McDowell FH. Five years’ treatment of Parkinson’s disease with levodopa. Therapeutic results and survival of 100 patients. Ann Intern Med. 1975;83(4):456–463. | |
Lesser RP, Fahn S, Snider SR, Cote LJ, Isgreen WP, Barrett RE. Analysis of the clinical problems in parkinsonism and the complications of long-term levodopa therapy. Neurology. 1979;29(9 Pt 1):1253–1260. | |
Royal Pharmaceutical Society of Great Britain, British Medical Association. British National Formulary. London: BMJ Group; 2009. | |
Brooks DJ. Dopamine agonists: their role in the treatment of Parkinson’s disease. J Neurol Neurosurg Psychiatr. 2000;68(6):685–689. | |
Steiger M, Jost W, Grandas F, Van Camp G. Risk of valvular heart disease associated with the use of dopamine agonists in Parkinson’s disease: a systematic review. J Neural Transm. 2009;116(2):179–191. | |
Kulisevsky J, Pagonabarraga J. Tolerability and safety of ropinirole versus other dopamine agonists and levodopa in the treatment of Parkinson’s disease: meta-analysis of randomized controlled trials. Drug Saf. 2010;33(2):147–161. | |
Leentjens AF. The role of dopamine agonists in the treatment of depression in patients with Parkinson’s disease: a systematic review. Drugs. 2011;71(3):273–286. | |
Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. 2004;23(20):3105–3124. | |
Dias S, Welton N, Sutton A, Ades A. NICE technical support document 2: A generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. 2011. Available from: http://www.nicedsu.org.uk/TSD2%20General%20meta%20analysis%20corrected%2015April2014.pdf. Accessed March 19, 2011. | |
Mills EJ, Ioannidis JP, Thorlund K, Schunemann HJ, Puhan MA, Guyatt GH. How to use an article reporting a multiple treatment comparison meta-analysis. JAMA. 2012;308(12):1246–1253. | |
Lunn D, Spiegelhalter D, Thomas A, Best N. The BUGS project: evolution, critique and future directions. Stat Med. 2009;28(25):3049–3067. | |
Giladi N, Boroojerdi B, Korczyn AD, Burn DJ, Clarke CE, Schapira AH. Rotigotine transdermal patch in early Parkinson’s disease: a randomized, double-blind, controlled study versus placebo and ropinirole. Mov Disord. 2007;22(16):2398–2404. | |
Rascol O, Brooks DJ, Korczyn AD, De Deyn PP, Clarke CE, Lang AE. A five-year study of the incidence of dyskinesia in patients with early Parkinson’s disease who were treated with ropinirole or levodopa. 056 Study Group. N Engl J Med. 2000;342(20):1484–1491. | |
Singer C, Lamb J, Ellis A, Layton G. A comparison of sumanirole versus placebo or ropinirole for the treatment of patients with early Parkinson’s disease. Mov Disord. 2007;22(4):476–482. | |
Watts RL, Lyons KE, Pahwa R, et al. Onset of dyskinesia with adjunct ropinirole prolonged-release or additional levodopa in early Parkinson’s disease. Mov Disord. 2010;25(7):858–866. | |
Mizuno Y, Kondo T, Hasegawa K, et al. Transdermal rotigotine in early stage Parkinson’s disease: a randomized, double-blind, placebo-controlled trial. Mov Disord. 2013;28(10):1447–1450. | |
Parkinson Study Group. Pramipexole vs levodopa as initial treatment for Parkinson disease: a randomized controlled trial. Parkinson Study Group. JAMA. 2000;284(15):1931–1938. | |
Shannon KM, Bennett JP Jr, Friedman JH. Efficacy of pramipexole, a novel dopamine agonist, as monotherapy in mild to moderate Parkinson’s disease. The Pramipexole Study Group. Neurology. 1997;49(3):724–728. | |
Kulisevsky J, López-Villegas D, García-Sánchez C, Barbanoj M, Gironell A, Pascual-Sedano B. A six-month study of pergolide and levodopa in de novo Parkinson’s disease patients. Clin Neuropharmacol. 1998;21(6):358–362. | |
Barone P, Bravi D, Bermejo-Pareja F, et al. Pergolide monotherapy in the treatment of early PD: a randomized, controlled study. Pergolide Monotherapy Study Group. Neurology. 1999;53(3):573–579. | |
Barone P, Poewe W, Albrecht S, et al. Pramipexole for the treatment of depressive symptoms in patients with Parkinson’s disease: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2010;9(6):573–580. | |
Wong KS, Lu CS, Shan DE, Yang CC, Tsoi TH, Mok V. Efficacy, safety, and tolerability of pramipexole in untreated and levodopa-treated patients with Parkinson’s disease. J Neurol Sci. 2003;216(1):81–87. | |
Kieburtz K. Twice-daily, low-dose pramipexole in early Parkinson’s disease: a randomized, placebo-controlled trial. Mov Disord. 2011; 26(1):37–44. | |
Parkinson Study Group. A controlled trial of rotigotine monotherapy in early Parkinson’s disease. Arch Neurol. 2003;60(12):1721–1728. | |
Thomas A, Bonanni L, Di Iorio A, et al. End-of-dose deterioration in non ergolinic dopamine agonist monotherapy of Parkinson’s disease. J Neurol. 2006;253(12):1633–1639. | |
Poewe W, Rascol O, Barone P, et al. Extended-release pramipexole in early Parkinson disease: a 33-week randomized controlled trial. Neurology. 2011;77(8):759–766. | |
Sampaio C, Bronzova J, Hauser RA, et al. Pardoprunox in early Parkinson’s disease: results from 2 large, randomized double-blind trials. Mov Disord. 2011;26(8):1464–1476. | |
Jankovic J, Watts RL, Martin W, Boroojerdi B. Transdermal rotigotine: double-blind, placebo-controlled trial in Parkinson disease. Arch Neurol. 2007;64(5):676–682. | |
Hauser RA, Schapira AH, Rascol O, et al. Randomized, double-blind, multicenter evaluation of pramipexole extended release once daily in early Parkinson’s disease. Mov Disord. 2010;25(15):2542–2549. | |
Brooks DJ, Abbott RJ, Lees AJ, et al. A placebo-controlled evaluation of ropinirole, a novel D2 agonist, as sole dopaminergic therapy in Parkinson’s disease. Clin Neuropharmacol. 1998;21(2):101–107. | |
Whone AL, Watts RL, Stoessl AJ, et al. Slower progression of Parkinson’s disease with ropinirole versus levodopa: the REAL-PET study. Ann Neurol. 2003;54(1):93–101. | |
Oertel WH, Wolters E, Sampaio C, et al. Pergolide versus levodopa monotherapy in early Parkinson’s disease patients: the PELMOPET study. Mov Disord. 2006;21(3):343–353. | |
Navan P, Findley LJ, Jeffs JA, Pearce RK, Bain PG. Double-blind, single-dose, cross-over study of the effects of pramipexole, pergolide, and placebo on rest tremor and UPDRS part III in Parkinson’s disease. Mov Disord. 2003;18(2):176–180. | |
Korczyn AD, Brunt ER, Larsen JP, Nagy Z, Poewe WH, Ruggieri S. A 3-year randomized trial of ropinirole and bromocriptine in early Parkinson’s disease. The 053 Study Group. Neurology. 1999;53(2):364–370. | |
Adler CH, Sethi KD, Hauser RA, et al. Ropinirole for the treatment of early Parkinson’s disease. The Ropinirole Study Group. Neurology. 1997;49(2):393–399. | |
Poewe WH, Rascol O, Quinn N, et al. Efficacy of pramipexole and transdermal rotigotine in advanced Parkinson’s disease: a double-blind, double-dummy, randomised controlled trial. Lancet Neurol. 2007;6(6):513–520. | |
Koller W, Lees A, Doder M, Hely M. Randomized trial of tolcapone versus pergolide as add-on to levodopa therapy in Parkinson’s disease patients with motor fluctuations. Mov Disord. 2001;16(5):858–866. | |
Lieberman A, Olanow CW, Sethi K, et al. A multicenter trial of ropinirole as adjunct treatment for Parkinson’s disease. Ropinirole Study Group. Neurology. 1998;51(4):1057–1062. | |
Pinter MM, Pogarell O, Oertel WH. Efficacy, safety, and tolerance of the non-ergoline dopamine agonist pramipexole in the treatment of advanced Parkinson’s disease: a double blind, placebo controlled, randomised, multicentre study. J Neurol Neurosurg Psychiatry. 1999;66(4):436–441. | |
Schapira AH, Barone P, Hauser RA, et al. Extended-release pramipexole in advanced Parkinson disease: a randomized controlled trial. Neurology. 2011;77(8):767–774. | |
Mizuno Y, Yanagisawa N, Kuno S, et al. Randomized, double-blind study of pramipexole with placebo and bromocriptine in advanced Parkinson’s disease. Mov Disord. 2003;18(10):1149–1156. | |
Lieberman A, Ranhosky A, Korts D. Clinical evaluation of pramipexole in advanced Parkinson’s disease: results of a double-blind, placebo-controlled, parallel-group study. Neurology. 1997;49(1):162–168. | |
Hutton JT, Koller WC, Ahlskog JE, et al. Multicenter, placebo-controlled trial of cabergoline taken once daily in the treatment of Parkinson’s disease. Neurology. 1996;46(4):1062–1065. | |
Mizuno Y, Abe T, Hasegawa K, et al. Ropinirole is effective on motor function when used as an adjunct to levodopa in Parkinson’s disease: STRONG study. Mov Disord. 2007;22(13):1860–1865. | |
Trenkwalder C, Kies B, Rudzinska M, et al. Rotigotine effects on early morning motor function and sleep in Parkinson’s disease: a double-blind, randomized, placebo-controlled study (RECOVER). Mov Disord. 2011;26(1):90–99. | |
Pahwa R, Stacy MA, Factor SA, et al. Ropinirole 24-hour prolonged release: randomized, controlled study in advanced Parkinson disease. Neurology. 2007;68(14):1108–1115. | |
Barone P, Lamb J, Ellis A, Clarke Z. Sumanirole versus placebo or ropinirole for the adjunctive treatment of patients with advanced Parkinson’s disease. Mov Disord. 2007;22(4):483–489. | |
Guttman M. Double-blind comparison of pramipexole and bromocriptine treatment with placebo in advanced Parkinson’s disease. International Pramipexole-Bromocriptine Study Group. Neurology. 1997;49(4):1060–1065. | |
Möller JC, Oertel WH, Köster J, Pezzoli G, Provinciali L. Long-term efficacy and safety of pramipexole in advanced Parkinson’s disease: results from a European multicenter trial. Mov Disord. 2005;20(5):602–610. | |
LeWitt PA, Lyons KE, Pahwa R. Advanced Parkinson disease treated with rotigotine transdermal system: PREFER Study. Neurology. 2007;68(16):1262–1267. | |
Im JH, Ha JH, Cho IS, Lee MC. Ropinirole as an adjunct to levodopa in the treatment of Parkinson’s disease: a 16-week bromocriptine controlled study. J Neurol. 2003;250(1):90–96. | |
Inzelberg R, Nisipeanu P, Rabey JM, et al. Double-blind comparison of cabergoline and bromocriptine in Parkinson’s disease patients with motor fluctuations. Neurology. 1996;47(3):785–788. | |
Rektorová I, Rektor I, Bares M, et al. Pramipexole and pergolide in the treatment of depression in Parkinson’s disease: a national multicentre prospective randomized study. Eur J Neurol. 2003;10(4):399–406. | |
Brunt ER, Brooks DJ, Korczyn AD, Montastruc JL, Stocchi F. A six-month multicentre, double-blind, bromocriptine-controlled study of the safety and efficacy of ropinirole in the treatment of patients with Parkinson’s disease not optimally controlled by L-dopa. J Neural Transm. 2002;109(4):489–502. | |
Steiger MJ, El-Debas T, Anderson T, Findley LJ, Marsden CD. Double-blind study of the activity and tolerability of cabergoline versus placebo in parkinsonians with motor fluctuations. J Neurol. 1996;243(1):68–72. | |
Wermuth L. A double-blind, placebo-controlled, randomized, multi-center study of pramipexole in advanced Parkinson’s disease. Eur J Neurol. 1998;5(3):235–242. | |
Rascol O, Lees AJ, Senard JM, Pirtosek Z, Montastruc JL, Fuell D. Ropinirole in the treatment of levodopa-induced motor fluctuations in patients with Parkinson’s disease. Clin Neuropharmacol. 1996;19(3):234–245. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.