")
Back to Journals » Patient Preference and Adherence » Volume 17
Nonadherence to Immunosuppressants Among Transplant Recipients: Emotional Intelligence as a Predictive Factor During COVID-19 Pandemic
Authors De Pasquale C, Barbagallo N, Veroux M , Pistorio ML, Zerbo D, Giaquinta A, Ekser B , Veroux P
Received 6 July 2023
Accepted for publication 11 October 2023
Published 27 November 2023 Volume 2023:17 Pages 3083—3092
DOI https://doi.org/10.2147/PPA.S426358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Concetta De Pasquale,1 Noemi Barbagallo,2 Massimiliano Veroux,3 Maria Luisa Pistorio,2 Domenico Zerbo,2 Alessia Giaquinta,2 Burcin Ekser,4 Pierfrancesco Veroux2
1Department of Educational Sciences, University of Catania, Catania, Italy; 2Department of General Surgery and Medical-Surgical Specialties, University Hospital of Catania, Catania, Italy; 3Department of Surgical and Medical Sciences and Advanced Technologies, University Hospital of Catania, Catania, Italy; 4Department of Surgery, Indiana University School of Medicine, Indianapolis, IN, USA
Correspondence: Maria Luisa Pistorio, Department of General Surgery and Medical-Surgical Specialties, University Hospital of Catania, Via Santa Sofia, 84, Catania, 95123, Italy, Tel/Fax +390953782629, Email [email protected]
Purpose: To evaluate the association between emotional intelligence and fear of COVID-19 on self-reported adherence, based on a cross-sectional design.
Patients and Methods: Transplants recipient of both sexes aged 23– 75 years old were evaluated at the Organ Transplant Unit, University Hospital of Catania, Italy. Data were analyzed using frequency, descriptives, Spearman and Pearson correlations, Chi-square goodness of fit test, and linear regression. Self-reported adherence was estimated with the Basel Assessment of Adherence with Immunosuppressive Medication Scale (BAASIS). Emotional intelligence and fear of COVID were, respectively, measured with the Emotional Intelligence Scale (EIS) and Multidimensional Assessment of COVID-19 Related Fears Scale (MAC-RF). This was a cross-sectional study of kidney transplant recipients. In reporting this study the authors followed the STROBE guidelines.
Results: A correlation was found between EIS and MAC and between EIS and adherence but there was no correlation between MAC and adherence. A linear regression model was also conducted using a stepwise method, which indicated that EIS was a significant predictor of adherence (p < 0.05).
Conclusion: This study was found that EIS is a predictor of adherence to treatment in transplant patients. Fear of COVID, while positively correlated to EIS, is not correlated to the adherence’s outcome, possibly due to the proper follow-up performed to the patients. Indeed, according to these results, we suggest to provide good follow-ups with recipients, with interviews also based on self-regulation and awareness.
Keywords: adherence, kidney transplant, emotional intelligence, COVID-19
Introduction
Adherence to therapy means the proficiency of the patient to follow medical doctors’ prescriptions regarding the timing, doses, and frequency of taking the drug for the entire therapy’s course.1
A major concern of adherence is being aware of the main reasons that lead patients to be non-adherent to treatment. Diverse studies have shown that patients with chronic diseases tend to have poor adherence.2 Multifariousness aspects influence adherence, such as education, age, number of years since the transplant, income levels, the belief that the therapy is not necessary, social factors, drug regimen factors, and immune suppressants’ side-effects.3–5 Previous studies have shown that, among renal transplant patients, non-adherence can occur early after transplantation. This issue is increasing over time.6,7 Preventing rejection and graft loss, adherence to medication is crucial in recipients. The literature also lists that 35.6% of renal transplant patients are non-adherent to immunosuppressant medication.8 Other variables that influence adherence are psychological factors.9–13 In this study, it has been hypothesized that emotional intelligence could be a factor in this. According to Goleman, every individual is endowed with emotion intelligence from birth. Five components distinguish emotional intelligence: self-awareness, self-regulation, motivation, empathy, and social skills.14 Emotional intelligence is also described as a person's belief about their emotions: being aware of our own emotions without repressing feelings (Goleman, Daniel. “The brain and emotional intelligence: New insights”. Regional Business (2011): 94–95.). This kind of intelligence seems to be useful in various fields, in as much as being capable of identifying and managing emotions. In the literature, a close relationship between emotion and motivation is often underlined.15 Indeed, emotional responses, among many components that characterize it, present a motivational aspect that can direct the individual to perform a certain kind of behaviour aimed at achieving a goal.16,17 This study was conducted during the COVID-19 pandemic. In the pandemic period, adherence to treatment in patients with chronic illness was significantly reduced due to the tough situation regarding reaching hospitals, contacting physicians, or the unavailability of medication.18,19 As mentioned before, many factors influence adherence, and some studies have discovered that the COVID-19 pandemic has impacted some of these factors.20 Other studies have shown that the COVID-19 threats incited the patients to adhere to their care principles, but the restrictions resulting from the pandemic caused difficulties in being adherent to treatments.21
The aim of the study was to evaluate the association between emotional intelligence and fear of COVID-19 on self-reported adherence, based on a cross-sectional design.
Materials and Methods
Study Participants
Data collection took place in period the between March 2021 and July 2022. Eighty kidney transplant recipients of both sexes, aged 23–75 years old, were evaluated while attending the Organ Transplant Unit, University Hospital of Catania, Italy. Participants were reached by telephone, using the follow-up list containing patients’ contact number, to explain the main objectives of the study and to ask for their willingness to participate. If so, they were given an appointment to fill in the required questionnaires. Before proceeding with the questionnaires, each participant had the opportunity to read all the information regarding the study and give their informed consent. The selection was based on the following criteria: age greater than 18 years, having had a kidney transplant at least 18 months earlier, because, according to the literature on the topic, in the first period after the transplant recipients are more adherent, while non-adherence problems tend to increase 12 months after the transplant,6,7 a kidney transplant from a deceased or living donor, and having no psychiatric disorders that could have influenced cognitive or emotional issues. The exclusion criteria were as follows: recipients with psychiatric disorders and recipients with rejection or adverse events, because these affect adherence.
Baseline psychiatric assessment was performed using two cross-sectional symptom rating scales, DSM 5 level 1 and 2, to examine any critical psychopathological domains. All recipients included in the study were receiving standardized immunosuppressive therapy: Tacrolimus, Mychophenolate, Mofetil and Steroids; and none of them were taking psychiatric drugs such as antipsychotics and/or antidepressants.
The present study was approved by the ethics committee of University of Catania (Section of Psychology) and carried out according to the Declaration of Helsinki (World Medical Association, 2013). Prior to inclusion in the study, we received written informed consent from all participants.
All organs were donated voluntarily with written informed consent and this was conducted in accordance with the Declaration of Istanbul.
Measures
The tests administered were the following: Emotional Intelligence Scale (EIS) to evaluate emotional intelligence, Multidimensional Assessment of COVID-19 Related Fears Scale (MAC-RF) to evaluate the fears of COVID-19, and Basel Assessment of Adherence to Immunosuppressive Medications Scale (BAASIS) for the analysis of therapeutic adherence.
EIS Scale
The EIS is a tool consisting of 33 items, three of which are expressed in a negative form, which can be evaluated on a scale of five intervals (0 = strongly disagree, 5 = strongly agree). The scale measures the individual perception of one’s emotional abilities by tracing them to three macro-dimensions: F1, evaluation and expression of emotions in relation to others (eg, “I know when it’s time to talk about my personal problems”); F2, evaluation and expression emotions in relation to oneself (eg, “I am aware of the emotions I feel”); and F3, regulation and use of emotions (eg, “I use a good mood to face obstacles”). The internal consistency values of each scale are satisfactory for factor 1, Evaluation of the emotions of others (α = 0.68), and factor 2, Evaluation and expression of one’s emotions (α = 0.64), and good for factor 3, Regulation and use of emotions/mood (α = 0.71).
MAC Scale
The MAC-RF is a self-report questionnaire consisting of eight items, assessable on a five-interval scale (0 = very different from me, 4 = very similar to me), each of which identifies eight forms of fear related to the COVID-19 pandemic. The total score (from 0 to 32) makes it possible to ascertain the presence of psychological suffering and/or pathological fears: higher scores in specific items indicate higher levels of the type of fear corresponding to that item. In addition, the scale analyzes four dimensions: bodily domain (items 1–2); interpersonal domain (items 3–4); cognitive domain (items 5–6); and behavioral domain (items 7–8). Scores of the MAC-RF can range from 0 to 32, with higher scores indicating higher COVID-19 related fears. The MAC-RF showed a good internal consistency (Cronbach’s alpha = 0.84).
BAASIS Scale
The BAASIS is a self-report instrument to assess medication nonadherence in transplantation developed by the Leuven‐Basel Research Group (LBARG). The BAASIS follows the recently published taxonomy of medication adherence (Vrijens et al, 201222). As a measure of medication adherence, the BAASIS is considered a valuable tool for assessing medication adherence in clinical practice and in research with transplant recipients (Cleemput et al, 200723; Dobbels et al, 201024; De Bleser et al, 201125). Several studies provide evidence on its psychometric properties (Marsicano et al, 201326; Tielen, 201427). The BAASIS instrument measures adherence over the last 4 weeks: the scale consists in/on five questions based on adherence's implementation and persistence: patients’ taking, skipping, timing (±2 h from the prescribed time, TM), and persistence to treatment. The general interpretation of the BAASIS scale consists of verifying if the patient is taking the medications as prescribed or if they are missing a dose (could be 2 or more), if the treatment has been interrupted or changed, the time of deviation or the discontinuation of the therapy without physician's consent.
Statistical Analysis
Data were analyzed using SPSS software, version 29.0. Frequency analysis was conducted to describe and identify patient’s characteristics. Descriptive statistics were performed to identify the mean, standard deviation, median, and variables’ normality. Chi-square goodness of fit test of BAASIS was used to assess the adherence to treatment. Bivariate correlation of Rho di Spearman was performed among adherence and EIS. Then a bivariate correlation of Pearson was conducted to assess the relationship between MAC and EIS. Last, a linear regression analysis method stepwise was used to determine EIS as a predictive factor to adherence.
Results
Participants and Procedures
Of the 80 interviewed patients (sample size calculation = 67, 95% CI = ±5%), 52.9% were women, 47.1% were men, 55.7% were from south Italy, and 44.3% were from north Italy. Patients ages ranged from 23 to 75 years and most of the sample were in the age group 45–55 years (43%). Regarding education, 55.7% finished high school, 25.7% had just the secondary school, and the rest of the sample was divided between primary school and college or higher degree. Most of the sample (64.3%) had received dialysis treatment in a range between 0–5 years (Table 1). Others demographic variables and tests of proportion are shown in Table 1.
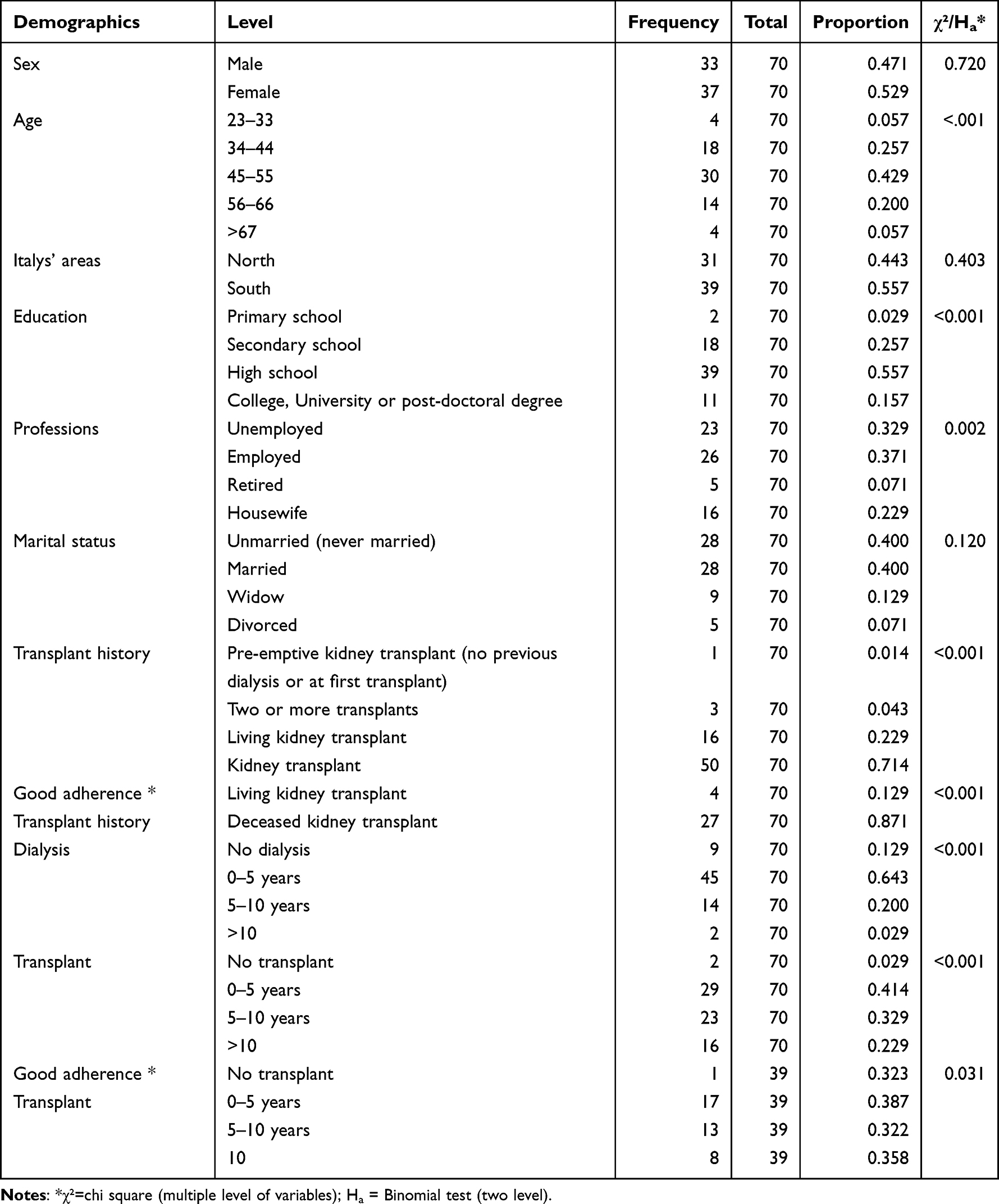 |
Table 1 Participants Demographic Characteristics |
Table 2 shows the mean, standard deviation, median, and variables’ normality of scales measures used in our study. Results indicate that distribution is normal because critical values do not exceed the range between +2.00 and −2.00, with acceptable skewness and kurtosis values.
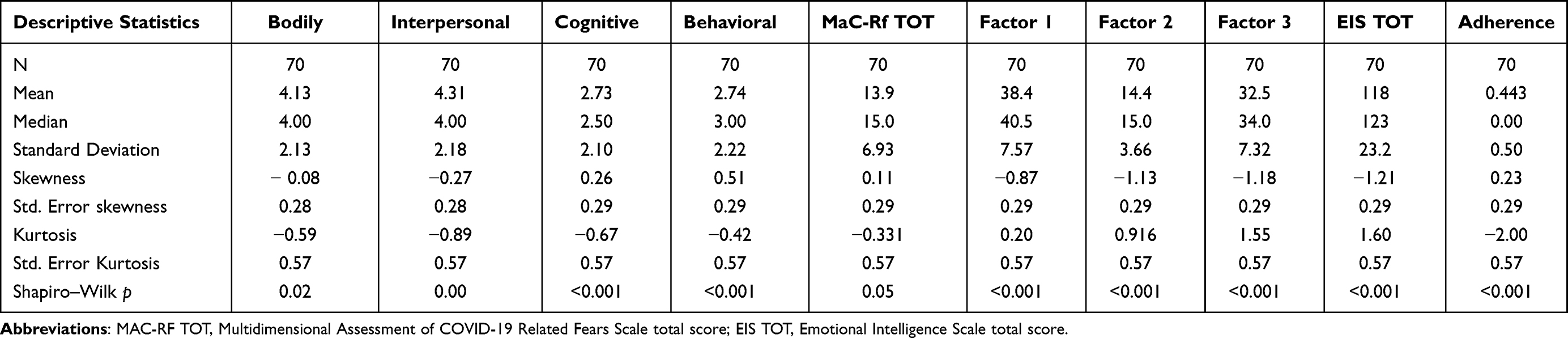 |
Table 2 Mean, Standard Deviation, Median, and Variables’ Normality |
BAASIS results are shown in Table 3, calculated with Chi-square goodness of fit test.
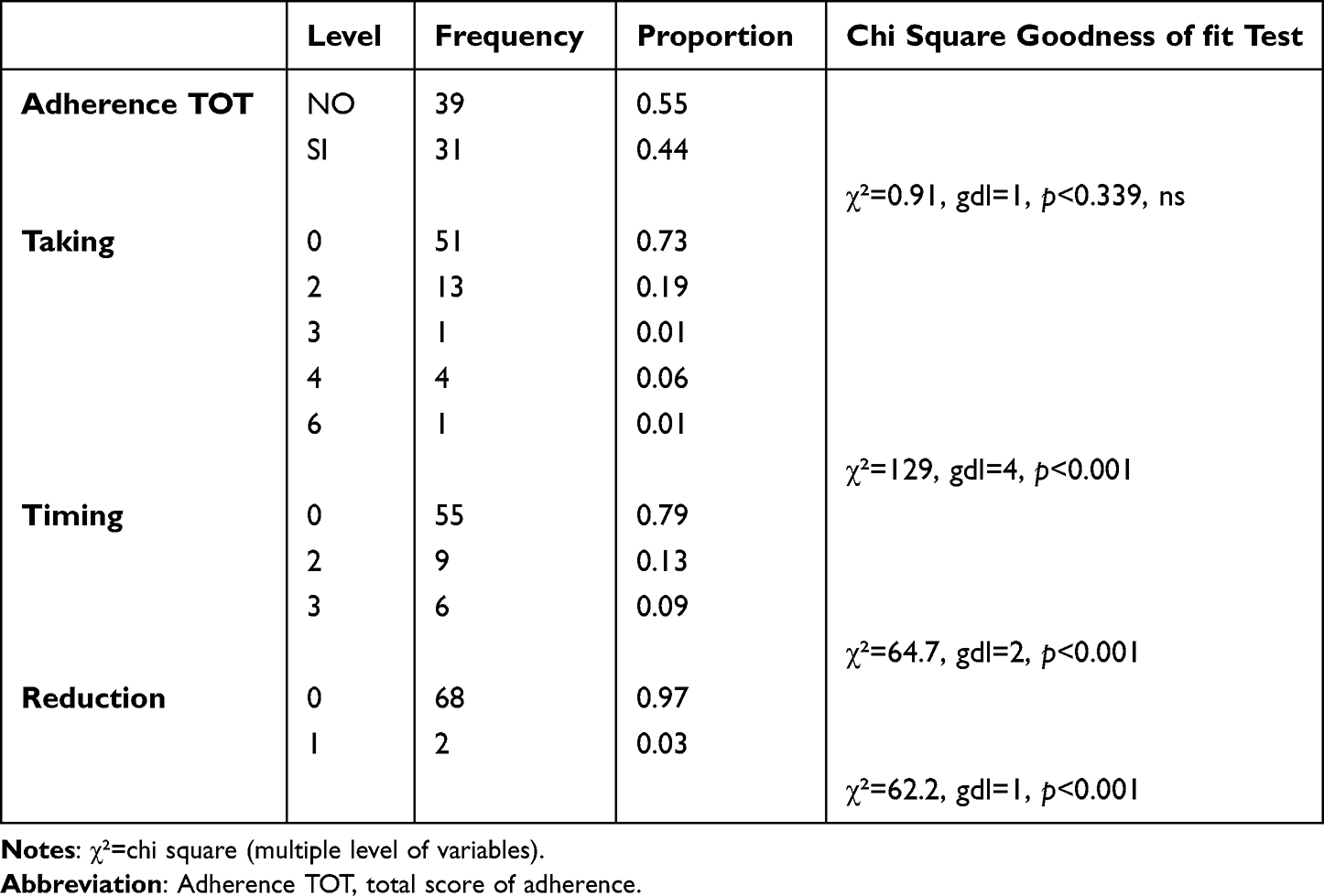 |
Table 3 Chi Square Goodness of Fit Test of BAASIS |
Table 3 shows the results of adherence: first we investigated the sample proportion and the frequency. The results revealed that 39 patients were adherent to the therapy (“NO” means “I never skipped or changed the therapy”) and 31 were not adherent. The levels are shown in the Table 3 indicate how many times the patient interfered with the medications.
Table 4 shows the relationship between EIS and adherence. Adherence showed a significant correlation between EIS factors: adherence positively correlates with EIS total score (r=0.32, p<0.01), factor 1 (r=0.32, p<0.01), factor 2 (r=0.39, p<0.01), and factor 3 (r=0.33, p<0.01). Spearman correlation was performed.
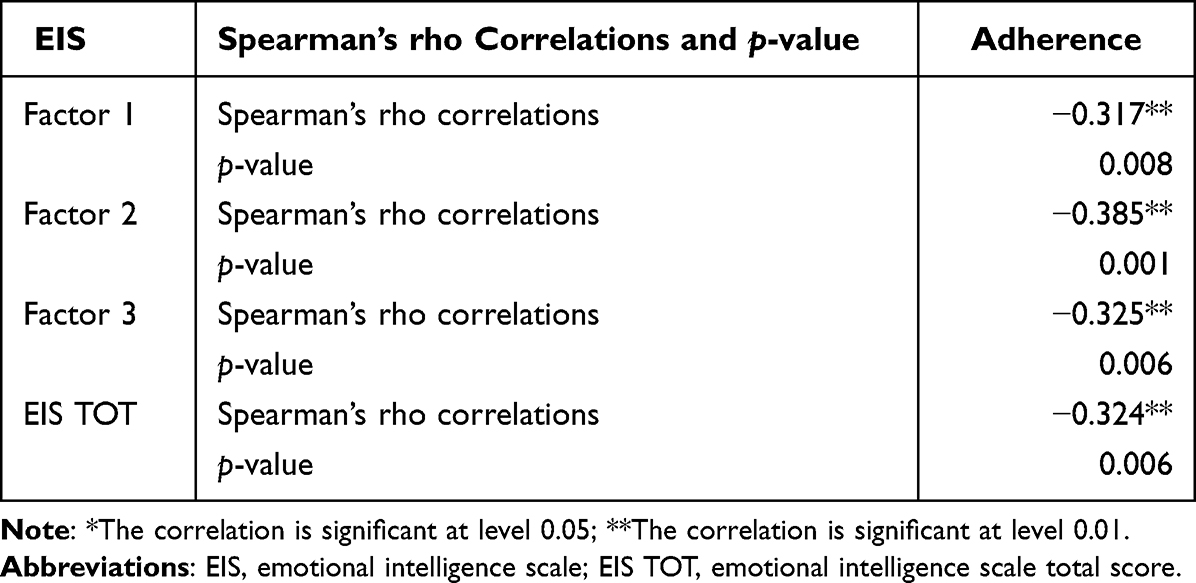 |
Table 4 Spearman’s Rho Correlations Among EIS and Adherence* |
Regarding bivariate correlation results between the EIS scale and MAC scale, Table 5 shows that total EIS score positively correlates with interpersonal domain (r=0.25, p<0.05) and the behavioral domain (r=0.27, p<0.01). Also, factors 1 and 3 positively correlate with the interpersonal domain (r=0.24, p<0.05; r=0.27, p<0.05, respectively). The Behavioural domain positively correlates with factor 2 (r=0.32, p<0.01) and with factor 3 (r=0.31, p<0.01). Total Mac score positively correlates with factor 3 (r=0.27, p<0.05). Pearson correlations were performed.
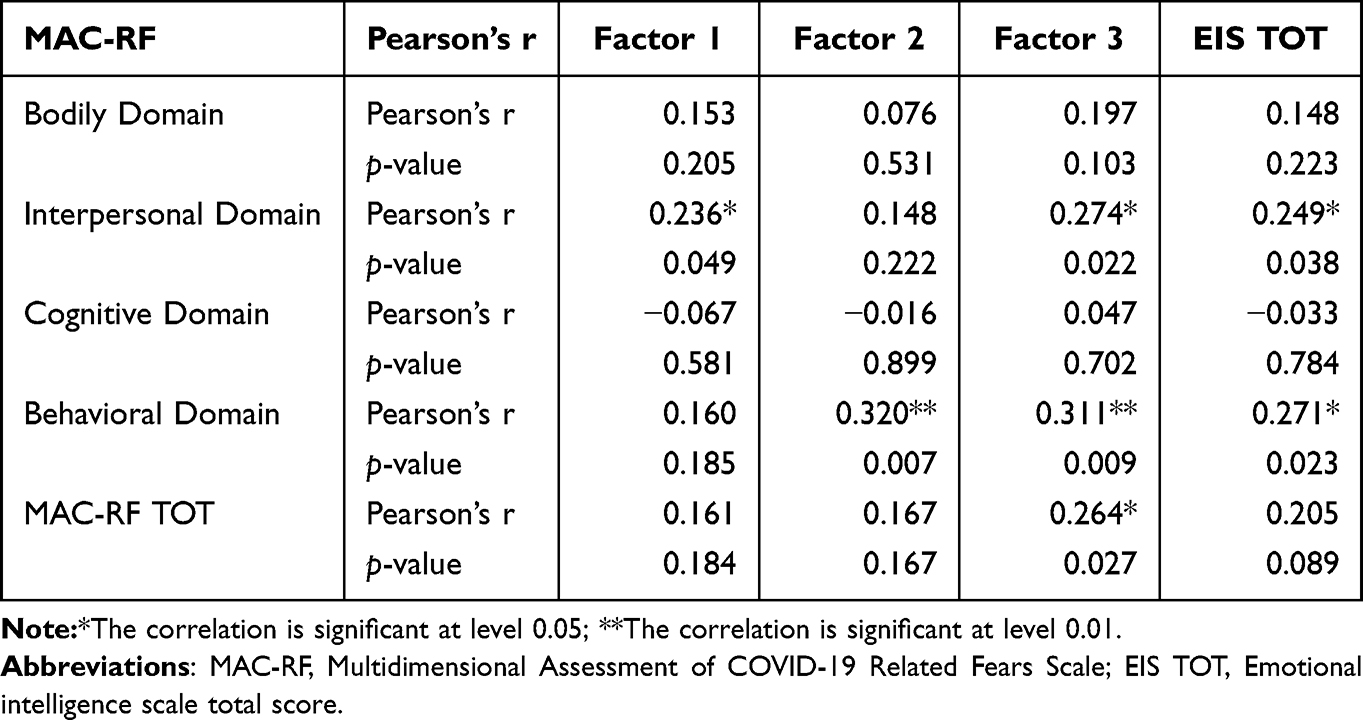 |
Table 5 Pearson’s r Correlations Among MAC-RF Domains, MAC-RF Total Score, EIS Factors, and EIS Total Score* |
The linear regression analysis stepwise method is shown in Table 6. Dependent variables are adherence, while independent variables are the total score of MAC scale, and the total score of EIS scale. The stepwise linear regression showed that the variable that influences adherence is EIS, in particular we have a variance proportion of R2=0.12 (R2 change=0.08, p<0.05) and the value of Beta indicates that EIS predict negatively the adherence (R2=0.12, Beta=−0.35, p=0.003). According to the results, our sample with high levels of EIS presents good adherence.
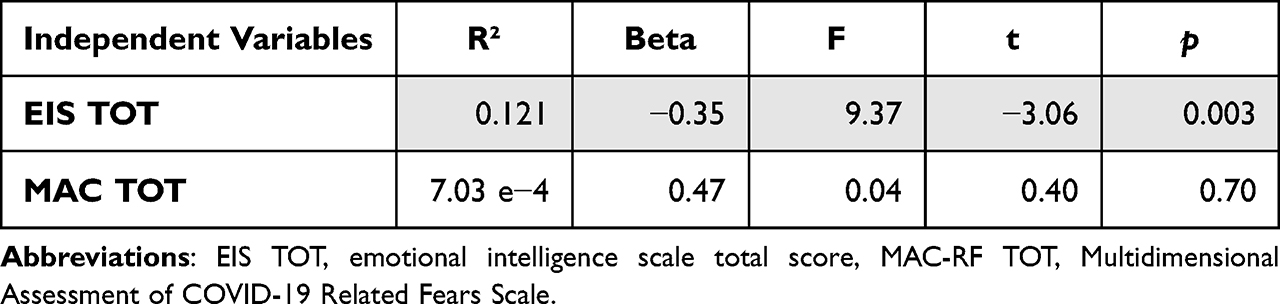 |
Table 6 Linear Regression Analysis Stepwise Method with Adherence as the Dependent Variable |
Discussion
Patients with chronic illness, especially during the COVID-19 pandemic, have experienced difficulties in taking medication and prescribed due to the unavailability of health care professionals caused by isolation measures and the interruption of services. These stressful measures mostly impacted chronically ill patients in fact, and recipients need to frequently visit the hospital due to the routine follow-up. Despite all, health care systems handled the situation in various way to ensure the care´s endurance.28–31 To achieve good adherence, previous studies showed that patients need to be well-informed about medication regimen, indeed patients that are knowledgeable are highly motivated to be adherent.32,33 Motivation and self-regulation in psychology has been already correlated to adherence behaviour.34–36 In various studies it was found that good adherence is associated with a good understanding of the consequences of not taking the medications as prescribed.37 Other studies also showed that compliance declines over the course of time not just in patients who suffer from renal disease, but also on all types of organ transplantation. Patient compliance is greater in the early post-transplant period. Thus, in the early post-transplant period recipients are more compliant.38 Also a proper follow-up is a main factor that leads the patient to be adherent to treatment,39,40 indeed the follow-up’s purpose is to assure the patient is remaining healthy while identifying problems that could arise, and intervene to mitigate complications.41,42
The main objective of our study was to see if the pandemic could impact vulnerability in transplant patients with respect to their adherence treatment and if emotional intelligence had played a fundamental role in the management of the latter. The results, albeit limited by a cross-sectional study, provide us with interesting consideration regarding the management of transplant patient compliance. First, MAC, or fear of COVID-19, has no positive correlation with adherence, while several significant and positive correlations emerge between its domains and EIS total score and its factors. Particularly interesting is the interpersonal domain which correlates with all the factors and with the total score except for the factor 2 (which concerns the relationship with oneself). The same can be said of the domain relating to behavior towards others. Regarding adherence to treatment, there are strong significant correlations with all factors of emotional intelligence with adherence. This result is then confirmed by the regression. We can therefore state that, while the fear of the COVID-19 pandemic does not prove to be fundamental in relation to therapeutic adherence, the impact of emotional intelligence is particularly important in our study. Emotional intelligence, often underestimated, in fact becomes the fundamental engine for effectively managing the intervention protocol for the patient and his management after the transplant. Adherence is in fact the result of what is a path of awareness, and adherence to the effectiveness of the intervention and the medical protocol.6,43,44 The practical implications of the study are to give indications on the importance of emotional intelligence in the management of the transplant patient. Emotional intelligence includes a set of skills including the person’s ability to be aware of their emotions, but also to know how to express them adequately. According to literature, the central element of emotional intelligence is self-awareness. This can be defined as the ability to recognize an emotion when it manifests itself.16–18 Transplant patients may have difficulty identifying their emotional experience and expressing it adequately. It is clear that one of the fundamental objectives of post-transplant follow-up can be the development of a good level of self-awareness, a basic element for good adaptation and effective adherence to treatment. Knowing how to control one’s emotions seems to be the basis of psychological well-being and emotional stability, especially when it comes to extremely intense or long-lasting emotional states, often present in our patients. Achieving a good level of competence on an emotional level is one of the primary objectives of a psychotherapeutic path with transplant patients, within which the person is supported in developing the ability to recognize and accept the emotional experiences experienced, thus becoming capable of coping with stress and negative emotions with more functional and adaptive strategies.16–18
In this study no patient randomization was performed, also generalizing the results was difficult due to the low number of participants. The limitations mainly concern the research design: as a cross-sectional type, it was not possible to draw inferences about the post-COVID period or to verify if there was a longitudinal effect of the pandemic, especially regarding the fear of contracting the virus and the therapeutic adherence. To strengthen the effect of the pandemic, it would have been necessary to compare it with a pre-pandemic group, and the lack of objective measures of adherence is another limitation of this study. Moreover, the design required patients to go to the clinic. Thus, there is selection bias, as nonadherent people are less likely to attend clinic appointments. Also, if the patients had high levels of fear related to COVID-19 they may not come to the clinic. Further, people with psychiatric disorders were excluded.
Conclusion
This study found that EIS is a predictor of adherence to treatment in transplant patients. Fear of COVID, while positively correlated to EIS, is not correlated to the adherence’s outcome, possibly due to the proper follow-up performed to the patients. Indeed, according to these results, we suggest to provide good follow-ups with recipients, with interviews also based on self-regulation and awareness.
Acknowledgments
The authors would like to thank all participants who volunteered their time to participate in the study. Also, we would like to thank the collaborating authors for their contributions. Finally, we wish to thank the Scientific Bureau of the University of Catania for language support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Laederach-Hofmann K, Bunzel B. Noncompliance in organ transplant recipients: a literature review. Gen Hosp Psychiatry. 2000;22(6):412–424. doi:10.1016/s0163-8343(00)00098-0
2. Chisholm MA, Lance CE, Williamson GM, Mulloy LL. Development and validation of the immunosuppressant therapy adherence instrument (ITAS). Patient Educ Couns. 2005;59(1):13–20. doi:10.1016/j.pec.2004.09.003
3. Zanga G, Drzewiscki E, Tagliani P, et al. Predictors of adherence and persistence to disease-modifying therapies in multiple sclerosis. Ther Adv Neurol Disord. 2021;14:17562864211031099. doi:10.1177/17562864211031099
4. Villeneuve C, Rousseau A, Rerolle JP, et al. Adherence profiles in kidney transplant patients: causes and consequences. Patient Educ Couns. 2020;103(1):189–198. doi:10.1016/j.pec.2019.08.002
5. Yeam CT, Chia S, Tan HCC, Kwan YH, Fong W, Seng JJB. A systematic review of factors affecting medication adherence among patients with osteoporosis. Osteoporos Int. 2018;29(12):2623–2637. doi:10.1007/s00198-018-4759-3
6. Zachciał J, Uchmanowicz I, Czapla M, Krajewska M, Banasik M. The association between psychosocial and age-related factors with adherence to immunosuppressive therapies after renal transplantation. J Clin Med. 2022;11(9):2386. doi:10.3390/jcm11092386
7. Massey EK, Tielen M, Laging M, et al. The role of goal cognitions, illness perceptions and treatment beliefs in self-reported adherence after kidney transplantation: a cohort study. J Psychosom Res. 2013;75(3):229–234. doi:10.1016/j.jpsychores.2013.07.006
8. Balsamo M, Murdock KK, Carlucci L. Psychological factors in adherence to COVID-19 public health restrictions in Italy: a path model testing depressed mood, anxiety, and co-rumination via cellphone. PLoS One. 2022;17(12):e0278628. doi:10.1371/journal.pone.0278628
9. Schäfer-Keller P, Steiger J, Bock A, Denhaerynck K, De Geest S. Diagnostic accuracy of measurement methods to assess non-adherence to immunosuppressive drugs in kidney transplant recipients. Am J Transplant. 2008;8(3):616–626. doi:10.1111/j.1600-6143.2007.02127.x
10. Fornaro M, De Berardis D, Iasevoli F, et al. Treatment adherence towards prescribed medications in bipolar-II acute depressed patients: relationship with cyclothymic temperament and “therapeutic sensation seeking” in response towards subjective intolerance to pain. J Affect Disord. 2013;151(2):596–604. doi:10.1016/j.jad.2013.07.004
11. De Pasquale C, Pistorio ML, Veroux P, et al. Quality of life and mental health in kidney transplant recipients during the COVID-19 Pandemic. Front Psychiatry. 2021;12:645549. doi:10.3389/fpsyt.2021.645549
12. Pistorio ML, Veroux M, Trigona C, et al. Psychological and emotional aspects in living donor kidney transplantation. Transplant Proc. 2019;51(1):124–127. doi:10.1016/j.transproceed.2018.04.085
13. Pistorio ML, Veroux M, Giaquinta A, et al. A study on emotional-affective aspects and the perception of general health in kidney transplant subjects. Transplant Proc. 2015;47(7):2135–2138. doi:10.1016/j.transproceed.2015.01.034
14. Goleman D 2007. Emotional Intelligence.
15. De Pasquale C, Pistorio ML, Veroux M, et al. Psychological and psychopathological aspects of kidney transplantation: a systematic review. Front Psychiatry. 2020;11:106. doi:10.3389/fpsyt.2020.00106
16. Boyatzis RE. The behavioral level of emotional intelligence and its measurement. Front Psychol. 2018;9:1438. doi:10.3389/fpsyg.2018.01438
17. Goldstein S, Princiotta D, Naglieri JA. Handbook of Intelligence: Evolutionary Theory, Historical Perspective, and Current Concepts. Springer Science + Business Media; 2015. doi:10.1007/978-1-4939-1562-0
18. Volpi NC, Polani D. Goal-directed empowerment: combining intrinsic motivation and task-oriented behavior. IEEE Trans Cogn Dev Syst. 2023;15(2):361–372. doi:10.1109/TCDS.2020.3042938
19. Norouzi S, Arefi Majd F, Sistani S, Mirzaee M, Ahmadian L. A pragmatically before-after trial of tele-visits vs face-to-face visits for chronic patients during the COVID-19 pandemic: patient-reported adherence. Int J Med Inform. 2023;172:105003. doi:10.1016/j.ijmedinf.2023.105003
20. Olmastroni E, Galimberti F, Tragni E, Catapano AL, Casula M. Impact of COVID-19 pandemic on adherence to chronic therapies: a systematic review. Int J Environ Res Public Health. 2023;20(5):3825. doi:10.3390/ijerph20053825
21. Maffoni M, Traversoni S, Costa E, et al. Medication adherence in the older adults with chronic multimorbidity: a systematic review of qualitative studies on patient’s experience. Eur Geriatr Med. 2020;11(3):369–381. doi:10.1007/s41999-020-00313-2
22. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
23. Cleemput I, Dobbels F. Measuring patient-reported outcomes in solid organ transplant recipients: an overview of instruments developed to date. Pharmacoeconomics. 2007;25(4):269–286. doi:10.2165/00019053-200725040-00002
24. Dobbels F, Berben L, De Geest S, et al. The psychometric properties and practicability of self-report instruments to identify medication nonadherence in adult transplant patients: a systematic review. Transplantation. 2010;90(2):205–219. doi:10.1097/TP.0b013e3181e346cd
25. De Bleser L, Dobbels F, Berben L, et al. The spectrum of nonadherence with medication in heart, liver, and lung transplant patients assessed in various ways. Transpl Int. 2011;24(9):882–891. doi:10.1111/j.1432-2277.2011.01296.x
26. Marsicano Ede O, Fernandes Nda S, Colugnati F, et al. Transcultural adaptation and initial validation of Brazilian-Portuguese version of the Basel assessment of adherence to immunosuppressive medications scale (BAASIS) in kidney transplants. BMC Nephrol. 2013;14:108. doi:10.1186/1471-2369-14-108
27. Tielen M, van Exel J, Laging M, et al. Attitudes to medication after kidney transplantation and their association with medication adherence and graft survival: a 2-year follow-up study. J Transplant. 2014;2014:675301. doi:10.1155/2014/675301
28. Zahmatkeshan N, Khademian Z, Zarshenas L, Rakhshan M. Experience of adherence to treatment among patients with coronary artery disease during the COVID-19 pandemic: a qualitative study. Health Promot Perspect. 2021;11(4):467–475. doi:10.34172/hpp.2021.59
29. Kurotschka PK, Serafini A, Demontis M, et al. General practitioners’ experiences during the first phase of the COVID-19 pandemic in Italy: a critical incident technique study. Front Public Health. 2021;9:623904. doi:10.3389/fpubh.2021.623904
30. Haldane V, De Foo C, Abdalla SM, et al. Health systems resilience in managing the COVID-19 pandemic: lessons from 28 countries. Nat Med. 2021;27(6):964–980. doi:10.1038/s41591-021-01381-y
31. Achille MA, Ouellette A, Fournier S, Vachon M, Hébert MJ. Impact of stress, distress and feelings of indebtedness on adherence to immunosuppressants following kidney transplantation. Clin Transplant. 2006;20(3):301–306. doi:10.1111/j.1399-0012.2005.00478.x
32. De Geest S, Dobbels F, Abraham I, Vanhaecke J. Clinical risk associated with appointment non-compliance in heart transplant recipients. The First European Symposium on Non-Compliance in Transplantation: Abstr 3; 1999.
33. Alfonsson S, Johansson K, Uddling J, Hursti T. Differences in motivation and adherence to a prescribed assignment after face-to-face and online psychoeducation: an experimental study. BMC Psychol. 2017;5(1):3. doi:10.1186/s40359-017-0172-5
34. Hagger MS, Koch S, Chatzisarantis NLD, Orbell S. The common sense model of self-regulation: meta-analysis and test of a process model. Psychol Bull. 2017;143(11):1117–1154. doi:10.1037/bul0000118
35. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/s0022-3999(99)00057-4
36. Leventhal H, Phillips LA, Burns E. The Common-Sense Model of Self-Regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. 2016;39(6):935–946. doi:10.1007/s10865-016-9782-2
37. Aguiar J, Ribeiro M, Pedro AR, Martins AP, da Costa FA. Awareness about barriers to medication adherence in cardiovascular patients and strategies used in clinical practice by Portuguese clinicians: a nationwide study. Int J Clin Pharm. 2021;43(3):629–636. doi:10.1007/s11096-020-01174-2
38. Dew MA, Roth LH, Thompson ME, Kormos RL, Griffith BP. Medical compliance and its predictors in the first year after heart transplantation. J Heart Lung Transplant. 1996;15(6):631–645.
39. Neuberger J. Follow-up of liver transplant recipients. Best Pract Res Clin Gastroenterol. 2020;46–47:101682. doi:10.1016/j.bpg.2020.101682
40. Lucey MR, Terrault N, Ojo L, et al. Long-term management of the successful adult liver transplant: 2012 practice guideline by the American association for the study of liver diseases and the American society of transplantation. Liver Transpl. 2013;19(1):3–26. doi:10.1002/lt.23566
41. Wolff G, Strecker K, Vester U, Latta K, Ehrich JH. Non-compliance following renal transplantation in children and adolescents. Pediatr Nephrol. 1998;12(9):703–708. doi:10.1007/s004670050531
42. Griva K, Davenport A, Harrison M, Newman SP. Non-adherence to immunosuppressive medications in kidney transplantation: intent vs. forgetfulness and clinical markers of medication intake. Ann Behav Med. 2012;44(1):85–93. doi:10.1007/s12160-012-9359-4
43. Gustavsen MT, Midtvedt K, Lønning K, et al. Evaluation of tools for annual capture of adherence to immunosuppressive medications after renal transplantation - A single-centre open prospective trial. Transpl Int. 2019;32(6):614–625. doi:10.1111/tri.13412
44. Helmy R, Scalso de Almeida S, Denhaerynck K, et al. Prevalence of medication nonadherence to co-medication compared to immunosuppressants in heart transplant recipients: findings from the international cross-sectional BRIGHT study. Clin Ther. 2019;41(1):130–136. doi:10.1016/j.clinthera.2018.11.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.