Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Non-Pharmacological Breathlessness Action Plans for People with COPD and Their Support People: A Scoping Review and Survey of Current Practice
Authors Luckett T ![]() , Roberts MM, Chaudhry MT, Hancock J, Ruttle L, Siemionow M, Smith K, River J, Johnson M
, Roberts MM, Chaudhry MT, Hancock J, Ruttle L, Siemionow M, Smith K, River J, Johnson M ![]() , Smith TA
, Smith TA ![]() , Johnston KN
, Johnston KN ![]() , Hutchinson A
, Hutchinson A ![]() , Swan F
, Swan F ![]() , Pearson M, Crooks MG
, Pearson M, Crooks MG ![]() , Kochovska S, Keijzers G, Keedwell A, Agar MR, Currow DC, Rhee J, Erfani E, Williams MT
, Kochovska S, Keijzers G, Keedwell A, Agar MR, Currow DC, Rhee J, Erfani E, Williams MT
Received 7 October 2025
Accepted for publication 13 February 2026
Published 11 March 2026 Volume 2026:21 568299
DOI https://doi.org/10.2147/COPD.S568299
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Tim Luckett,1 Mary M Roberts,2 Muneeba Tariq Chaudhry,1 John Hancock,3 Lennette Ruttle,4 Marina Siemionow,5 Kate Smith,6 Jo River,1 Miriam Johnson,7 Tracy Ann Smith,2 Kylie N Johnston,8 Ann Hutchinson,7 Flavia Swan,7 Mark Pearson,7 Michael G Crooks,7 Slavica Kochovska,1,9 Gerben Keijzers,10– 12 Anna Keedwell,13 Meera R Agar,1 David C Currow,1,14 Joel Rhee,15 Eila Erfani,16,17 Marie T Williams8
1Faculty of Health, University of Technology Sydney (UTS), Sydney, Australia; 2Department of Respiratory and Sleep Medicine, Westmead Hospital, Sydney, Australia; 3Person Living with COPD, Sydney, Australia; 4Support Person, Sydney, NSW, Australia; 5Support Person, Canberra, ACT, Australia; 6Lung Foundation Australia, Brisbane, Australia; 7Wolfson Palliative Care Research Centre, Hull York Medical School, University of Hull, Hull, UK; 8University of South Australia, Adelaide, Australia; 9College of Medicine and Public Health, Flinders University, Adelaide, Australia; 10Department of Emergency Medicine, Gold Coast Hospital and Health Service, Gold Coast, Australia; 11Faculty of Health Sciences and Medicine, Bond University, Gold Coast, Australia; 12School of Medicine and Dentistry, Griffith University, Gold Coast, Australia; 13Palliative Care, Bendigo Health, Bendigo, Australia; 14Flinders Ageing Alliance, Flinders University, Adelaide, Australia; 15Faculty of Medicine & Health, University of New South Wales (UNSW), Sydney, Australia; 16Computer and Data Science Discipline, Australian Catholic University (ACU), Sydney, Australia; 17School of Information Systems and Technology Management, UNSW, Sydney, Australia
Correspondence: Tim Luckett, University of Technology Sydney, Faculty of Health, Jones Street, Sydney, NSW, 2007, Australia, Email [email protected]
Introduction: Breathlessness action plans guide people to self-manage acute-on-chronic breathlessness episodes using non-pharmacological strategies to help breathing and overcome panic. We aimed to identify plans available for people with chronic obstructive pulmonary disease (COPD) and describe their development, content, quality, use, and evidence for benefit.
Methods: Two descriptive methodologies were used, overseen by a team of people with COPD and carers/support persons, clinicians and researchers: 1) A scoping review (academic databases, internet) identified English-language plans and research; 2) An online survey of plan-users and clinicians about their plan-related experience and perceived benefits. Each plan underwent appraisal by a person with COPD/support person and clinician/researcher using the Patient Education Materials Assessment Tool (PEMAT), content analysis and reading grade assessment.
Results: Of 69 plans identified, 88% (n=61/69) included breathing techniques, 78% (n=54/69) positioning, 65% (n=45/69) airflow, 36% (n=25/69) relaxation/distraction, 30% (n=21/69) stopping/slowing, 22% (n=15/69) remaining calm, 13% (n=13/69) reassurance, 7% (n=5/69) support from others and 4% (n=3/69) loosening clothing. The 48 plans that could be PEMAT-analysed scored an average of 64% for understandability and 68% for actionability. Their median reading grade was 8.2 (inter-quartile range 2.2). We identified efficacy support from only one pre/post study and feasibility/acceptability from qualitative data in two feasibility trials, each focusing on a different plan. In the survey, 67% (n=31/46) of plan-users self-reported avoiding calling an ambulance over the past year by using their plan. 93% (n=94/101) of clinicians perceived patient benefit in the form of increased confidence/reduced anxiety, 60% (n=61/101) reduced frequency of episodes, 53% (54/101) reduced need for ambulance/emergency department, and 41% (41/101) increased activities of daily living, while 4% (4/101) were unsure of any benefit.
Discussion: Despite multiple plans being available, few studies have assessed acceptability or efficacy. Further research is needed to evaluate net effects on self-management, breathlessness-related outcomes and healthcare usage.
Plain Language Summary: Breathlessness action plans are short guides that can help people with chronic obstructive pulmonary disease (COPD) manage episodes of sudden breathlessness. The plans use simple strategies without medications like breathing techniques, positioning, or using a fan. We found 69 plans, but only a few have been properly tested. People using the plans said they could sometimes avoid calling an ambulance. Most clinicians felt the plans gave patients more confidence and reduced anxiety. More research is needed to show how well they work and whether they can reduce the need for emergency care.
Keywords: dyspnea, dyspnoea, self-management, patient education
Introduction
Chronic obstructive pulmonary disease (COPD) is a common cause of chronic or “persistent” breathlessness that negatively impacts activities of daily living and psychosocial wellbeing.1 On top of everyday levels of “background” or “continuous” breathlessness, some people experience acute-on-chronic episodes of worsening breathlessness.2 Episodic breathlessness can sometimes be due to a COPD exacerbation that requires medical treatment of underlying pathology (eg infection, inflammation).3 At other times, causes can be exertional (eg physical activity, talking), emotional (eg panic, anger), or environmental (eg airborne pollutants, changes in temperature), usually resolving without medical treatment in under 15 minutes.4–7 Episodes sometimes occur without obvious explanation and can be very frightening, making people feel that they are “gasping for breath”, “suffocating” and “about to die”.8–10 In these situations, people understandably call an ambulance or present to the Emergency Department (ED), only to discover that medical treatment was not required. Approximately 0.5% of all ED attendances may be caused by breathlessness from COPD, of which one third are discharged directly to home.11 This suggests at least some could have been managed in the community with greater cost-effectiveness.
Best practice management of breathlessness recognises the multi-dimensional nature of symptom experience and seeks to manage “thinking” and “functioning” domains as well as “breathing” itself.12 Although high-grade evidence is lacking, people with COPD and other breathlessness-causing conditions describe successfully self-managing episodes using a range of non-pharmacological strategies. These include breathing techniques, positioning, pacing, airflow (eg from a hand-held fan) and relaxation techniques, as well as pharmacological treatments such as short-acting inhaled bronchodilators and oxygen.5–8,10,13
Family members and others who are present during a breathlessness episode (“support people”) can make valuable contributions by providing a calm and reasoned presence, assisting with management, and documenting what works to plan for future episodes.14 However, support people may themselves be distressed by breathlessness episodes and call for medical assistance even when the person with COPD is confident it’s under control. For these reasons, support people are key stakeholders in any interventions to improve self-management of breathlessness episodes.
“Action plans” are written educational resources that outline strategies patients can use to better self-manage their chronic conditions.15 Two kinds of action plan are relevant for self-management by people with COPD and their support persons: COPD action plans that focus on pharmacological management of medical events underlying a COPD exacerbation (eg using bronchodilators, antibiotics and/or corticosteroids) and breathlessness action plans that advise on non-pharmacological management of breathlessness episodes caused by factors other than an exacerbation. By summarizing key strategies in brief, easy-to-digest ways, such plans have potential to prompt people with COPD and support persons how to manage episodes when they are too distressed to remember.
Cochrane reviews have concluded that COPD action plans can result in a lower probability of respiratory-related hospital admissions and improvements in health-related quality of life.16,17 In contrast, no review has yet synthesised the evidence on breathlessness action plans. The current research set out to fill this gap by identifying available breathlessness action plans, describing their development, content, quality, use, and evidence for benefit.
Materials and Methods
Two methodologies were used: a scoping review and survey of current practice. The research was co-designed by a project team comprising 50% people with COPD (DD, JH) and support persons (LR, MS) (collectively termed “plan-users”) in partnership with project and investigator team members from academic (TL, JR, AH, SK, MP, EE), medical (MJ, TS, GK, AK, DC, MA), physiotherapy (MW, KJ, FS), nursing (MR, KS), exercise physiology (MC) and psychology (EK) perspectives.
Methods for the scoping review are reported in accordance with guidance from the PRISMA-ScR checklist (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews).18 The protocol for the scoping review was not pre-registered. Survey methods are reported in accordance with the Checklist for Reporting Results of Internet E-Surveys (CHERRIES).19 The survey was approved by the University of Technology Sydney (UTS) Human Research Ethics Committee (HREC) (approval number ETH23-8389). The study complied with the Declaration of Helsinki.
Scoping Review
Inclusion Criteria
We defined breathlessness action plans as guides that summarise what to do when breathlessness becomes worse using simple, non-pharmacological strategies to help breathing and thinking. These two domains were prioritised over the functioning domain of breathlessness because plans focus on acute episodes that require people to pause activities of daily living. We focused on plans that were designed for persons living with COPD / their support persons, or intended for general use across health conditions. Plans that were targeted toward conditions other than COPD or children and their parents were excluded.
Articles were considered eligible if they described the development or content of breathlessness action plans or evaluated plan-related impacts using any research design.
For practical reasons, both plans and articles had to be written in English, but no limits were set on time since publication. Given nuances in terms used to describe breathlessness and its emotional impacts, translation software was deemed inadequate, and the team lacked resources for best-practice forward-backward translation by a fluent speaker.
Information Sources
Four academic databases (Medline, CINAHL, PsycInfo, CENTRAL), the internet, and specific professional association/peak bodies websites were searched to source plans and studies available in the public domain.
Search Strategy
Academic database searches were conducted in November 2023, updated in January 2025. See Box 1 for search terms used for Medline as an example.
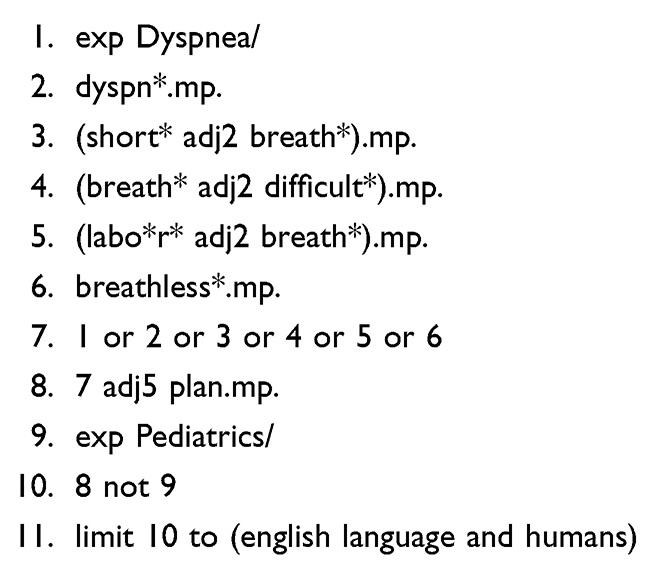 |
Box 1 Search Terms Used for Medline |
Internet searches were conducted in October 2023 using the Google search engine in the Microsoft Edge browser. Searches initially used no country limits, and then applied limits for English-speaking OECD (Organisation for Economic Co-operation and Development) countries as the most likely sources for plans with linguistic and cultural relevance to users living in Australia, our country of primary interest. “&pws = 0” was added to each search to prevent results being influenced by previous searches, which is otherwise the default for Google. Search terms included: (plan or “action plan” or guide or manage) AND “shortness of breath”, breathless* or dyspn*. One reviewer appraised Google results against eligibility criteria until 10 consecutive pages (ie 100 results) were found to be ineligible. Finally, websites for national and jurisdiction-based peak bodies for respiratory conditions and palliative care in each OECD country were hand-searched individually for plans. Links were followed to other pages that looked potentially relevant.
Selection
Screening and selection were undertaken by a single reviewer (TL or a research assistant), with discussion between team members used to resolve uncertainties.
Data Items and Charting
Data were extracted into Excel spreadsheet templates developed by the team. Data items for plans included the name, country of origin, organisational affiliation and any contact details, source (including URL for websites), date, target disease and user group and content. Data were extracted by a single reviewer.
Data items for articles included authors, date of publication, country, methods, results and conclusions.
Critical Appraisal
The Patient Education Materials Assessment Tool – Printable Materials (PEMAT-P) was used to assess the understandability and actionability of plans identified.20 Each plan was reviewed against PEMAT-P criteria by two project team members - a “plan-user” and clinician or academic. Readability was assessed using the Flesch-Kincaid formula administered through the Sydney Health Literacy Lab, with grade 8 or lower considered optimal in in accordance with guidelines.21–23
Risk of bias for evaluative studies was appraised by two academic reviewers (TL, MC) using the Cochrane tool for randomised (ROB-2) or non-randomised (ROBINS-IV2) trials as appropriate.24 Any disagreements were resolved by discussion.
Synthesis of Plans
Plans identified by the scoping review were pooled for analysis with those reported in the survey (see below), removing any duplicates. Plan characteristics and content on non-pharmacological strategies and help-seeking were categorised and coded by two researchers (MC, TL) using content analysis, with any disagreements resolved by discussion.
Literature Synthesis
Results from evaluative studies were synthesised narratively.
Survey
Participants
People were eligible to participate if they were: 1) persons living with COPD or their support persons from Australia or New Zealand (ANZ) with experience of using a breathlessness action plan and able to complete questionnaires in English; or 2) clinicians from any discipline and speciality working in OECD countries with experience of developing and/or delivering breathlessness action plans to people with COPD. We focused on OECD countries to increase the comparability of social and healthcare contexts. Clinicians from a non-English speaking OECD country were eligible if they provided data in English.
Participants were recruited using the following methods: 1) invitations circulated through Email lists and websites of relevant national peak bodies, as well as ANZ networks for older people (Supplementary file 1); 2) social media posts; 3) direct approach to clinician-researchers through the investigators’ networks; 4) a direct approach by Email and telephone to ANZ Respiratory Medicine and Specialist Palliative Care services (limited to ANZ for feasibility reasons); 6) posters displayed in ANZ health services and public venues well-used by older people; and 7) snowball recruitment. The survey announcement is included as Supplementary file 1. No incentives were offered for survey completion.
Data Collection
Data were collected from November to December 2023 by means of open, online, anonymous questionnaires administered using the Qualtrics™ platform. Participants reporting on more than one plan were asked to complete a separate questionnaire for each one. For this reason, no attempt was made to prevent multiple entries from the same individual. Participants were given the option of responding less anonymously via telephone/videoconference at a convenient time if they preferred. If participants chose the latter option, an interviewer took notes directly into the online questionnaire on the person’s behalf rather than audio-recorded the interview for transcription. Submission of the online survey was taken as evidence of consent, while verbal consent was collected from people who chose to complete an interviewer-assisted survey. Approval for these forms of consent was received from the University of Technology Sydney’s Human Research Ethics Committee (approval number ETH23-8697) on the grounds that these were less burdensome to participants and placed fewer and demands on digital literacy than requiring written consent, and that all data were self-reported and therefore self-selected by participants.
Two versions of the questionnaire were available – one for plan-users, and one for clinicians (see Supplementary file 2). The questionnaire was designed by the project and investigator teams (see above for membership), and was not tested prior to data collection. Items in each version were listed in the same order on a single page for each participant. Participants were encouraged to complete and submit the questionnaire at a single sitting but could change their responses to any item during this window. At the end of the questionnaire, participants were invited to upload or Email a copy of their breathlessness action plan for review. Participants were also invited to Email or phone the research team to express interest in partnering on future co-design of an optimal breathlessness action plan.
Survey Analysis
Closed items on the questionnaires were analysed using descriptive statistics; open questions were thematically analysed using an inductive approach by two researchers (TL, MC), with disagreements resolved by discussion. Incomplete questionnaires were included in the analysis, with the number of participants being presented for each item. No inferential analyses or statistical power considerations were used.
Results
The Results section will begin with a summary of breathlessness action plans identified across sources before reporting findings on research evidence identified by the scoping review and then survey responses from people with COPD, support persons and clinicians.
Breathlessness Action Plans
A total of 69 plans were identified across the scoping review and survey (literature searches n=1; internet search n=38; survey n=40; with 10 duplicates removed). Figure 1 shows the proportion of all 69 plans recommending each non-pharmacological strategy. The order varied in which strategies were recommended, except if stopping or slowing down was recommended, in which case this nearly always came first.
 |
Figure 1 Non-pharmacological strategies recommended by all breathlessness action plans (n=69). |
Just over two-thirds (69%) (n=48/69) of plans could be subjected to PEMAT analysis because survey respondents omitted to attach the remaining 21 plans or describe them in enough detail. These 48 plans originated from the UK (42%; n=20/48), Australia (40%; n=19/48), New Zealand (10%; n=5/48), USA (4%; n=2/48), Canada (2%; n=1/48) or Singapore (2%; n=1/48). Of the plans from the UK, 70% (n=14/20) were sourced from various National Health Service (NHS) trusts. These plans provided similar guidance but were appraised separately due to their differing formats.
Of the 48 plans, 40% (n=19/48) used images or graphics to supplement information. Advice on seeking medical management was included in 44% (n=21/48) of plans. A prompt to seek emergency care was included in 29% (n=14/48). Supplementary information was available for 73% (n=35/48) of plans. 27% plans (n=13/48) had capacity to be personalised.
The average word count for plans was 157 words, with a median reading grade of 8.2 (inter-quartile range 2 to15). The average PEMAT score across all plans was 64% for understandability and 68% for actionability. The two plans achieving the highest understandability score (88%) differed from the 10 plans that achieved the highest score for actionability (100%). See Supplementary file 3 for details of each plan.
Scoping Review
Searches of academic databases returned 258 records of which one met inclusion criteria, with an additional four papers identified from personal records of the collaborative team (see Figure 2).
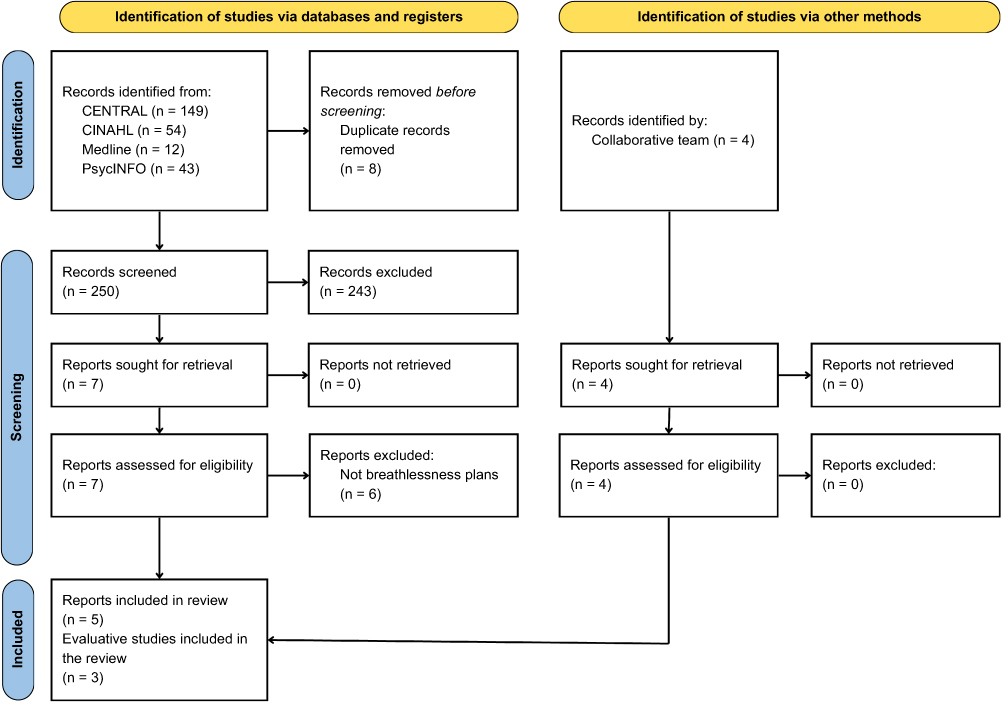 |
Figure 2 Flow diagram of reports identified and screened. |
Only one evaluative study was identified, which assessed a plan designed by the Royal Melbourne Hospital’s Advanced Lung Disease Service (ALDS) (Plan 38 in Supplementary file 3).25 The study was an uncontrolled pre/post investigation that included 26 participants with COPD. The intervention went beyond a breathlessness action plan to also include information leaflets, breathlessness education and a hand-held fan. Results identified clinically important improvements in “on average” and “at worst” breathlessness severity measured by numerical rating scales (NRS) between baseline and 6 weeks follow-up, as well as improvements in breathlessness-related quality of life in a sub-group with high anxiety at baseline. However, effects from the plan could not be separated from those of other components, measurements did not focus on episodes rather than daily levels of persistent breathlessness, and no measures were taken of emergency service use. The report of this study did not meet criteria B1 or B2 (confounding variables) of the ROBINS-IV2 checklist for proceeding with a more detailed risk-of-bias assessment.
Two further articles reported qualitative data on the feasibility and acceptability of two breathlessness action plans. The first of these tested an educational intervention for UK paramedics that made use of a plan following a BREATHE mnemonic: Be reassured, Resting position, Exercises to slow breathing, Airflow across lower face/nasal passages, Time to settle, Help with fears and worries, and Education for the patient and carer (Plan 36 in Supplementary file 3).26 People calling an ambulance for a breathlessness episode were supported by paramedics to follow the BREATHE steps, and then given a laminated copy of the plan to self-administer during future episodes. During the study’s semi-structured interviews, one of the paramedics involved in testing stated:
“I think that [the laminated plan] was good and I think that that’s really helpful for relatives to be able to use to coach people through, because I would notice that after sort a five minutes of me coaching them they would start to step in, because it’s not hard, and so I think that was effective”.
(Paramedic, focus group 6). The second article reported a UK feasibility trial of an online intervention called SELF-BREATHE, co-designed with patients with chronic breathlessness from any cause.27 Participants received help with developing a personalised action plan for episodes, as well as support for more general self-management. The feasibility focus of the trial and complex nature of the intervention did not allow for effects on quantitative outcomes to be discerned between the action plan compared to other components. However, a quote from one participant with COPD suggested she found the action plan component helpful in self-managing episodes: “It was good [SELF-BREATHE] because obviously when you have a breathing attack you automatically just clam up and panic. But it was nice to be able to have that information to hand”. (Interviewer: “What did you find useful when you had these breathlessness attacks?”) “The [breathing] techniques and everything, especially with the pursed lips, the relaxation. The bending over and breathing from the diaphragm that helped”. (Female, COPD, 41–50 years). Because the SELF-BREATHE plan was personalised, it could not be included either in the article or our synthesis.
Two other articles described the American Thoracic Society’s (ATS) action plan for managing sudden and severe episodes of breathlessness that the ATS has termed “breathlessness crises” (Plan 37 in Supplementary file 3).28,29 This plan and others identified by the scoping review’s internet searches are synthesised below, alongside those identified by the survey.
Survey
Plan-Users (People Living with COPD or Support Persons)
Of 87 respondents to the plan-user survey, 47% (n=41/87) were excluded from analyses because: 6% (n=5/87) included nil data, 14% (n=12/87) said they would like a plan but did not have one, 14% (n=12/87) focused exclusively on pharmacological strategies, 8% (n=7/87) focused on everyday breathlessness rather than episodic, 3% (n=3/87) reported using a COPD action plan with no breathlessness-related component, and 2% (n=2/87) provided responses that were difficult to interpret.
The 46 plan-users included in the analysis were 44 people with COPD and two support persons. Their reports varied widely with regard to frequency of breathlessness episodes, most commonly being two to three times over the past year (26%; n=12/46). See Table 1 for sample characteristics.
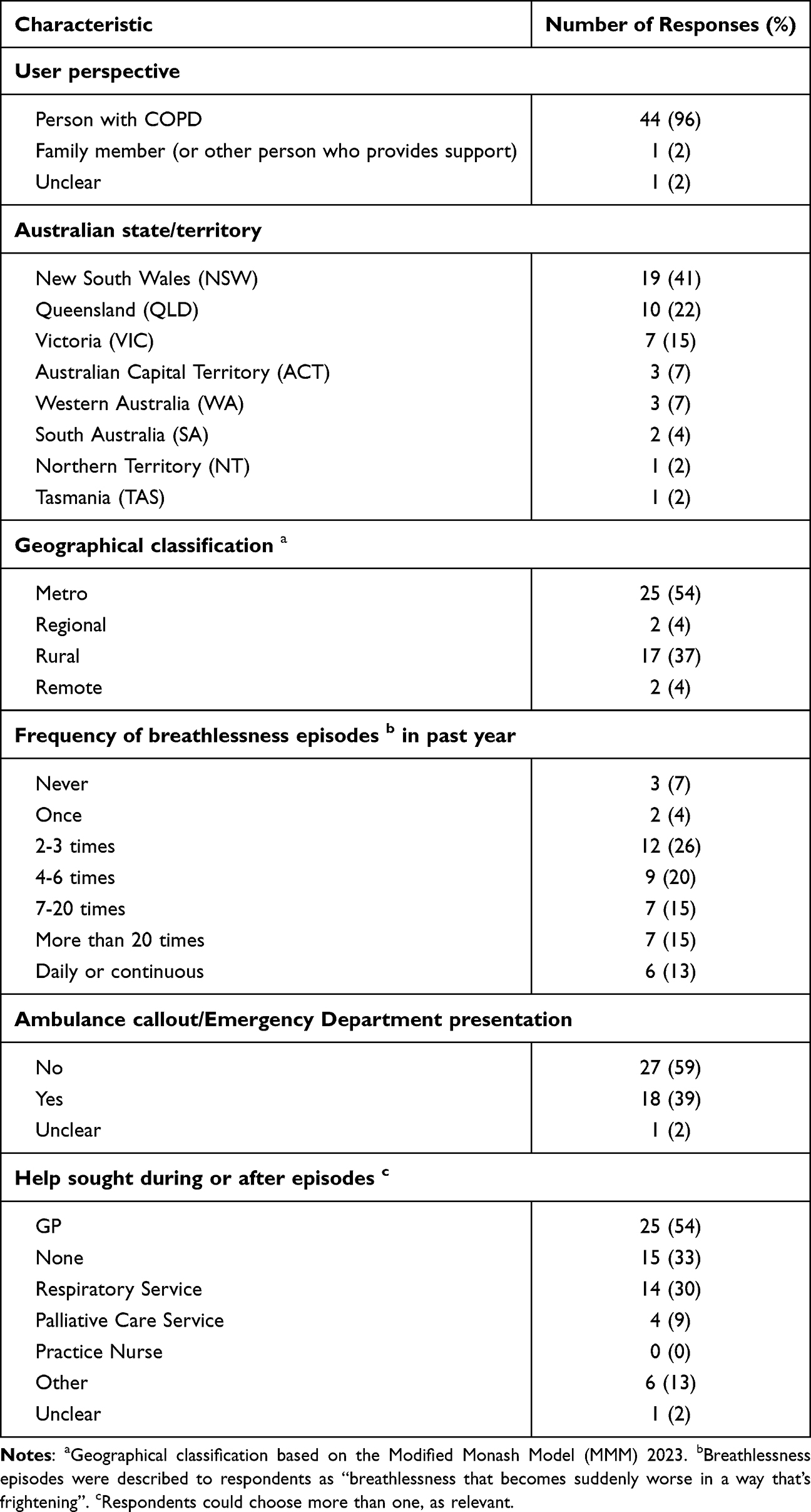 |
Table 1 Summary Characteristics of Plan Users Responding to the Survey (n=46) |
Half (n=23/46) of plan-users had received a breathlessness plan from a clinician, and half from other sources. Two-thirds (n=31/46) of those reporting plan use felt that the plan had helped them avoid calling an ambulance over the past year. See Table 2 for details of plan use.
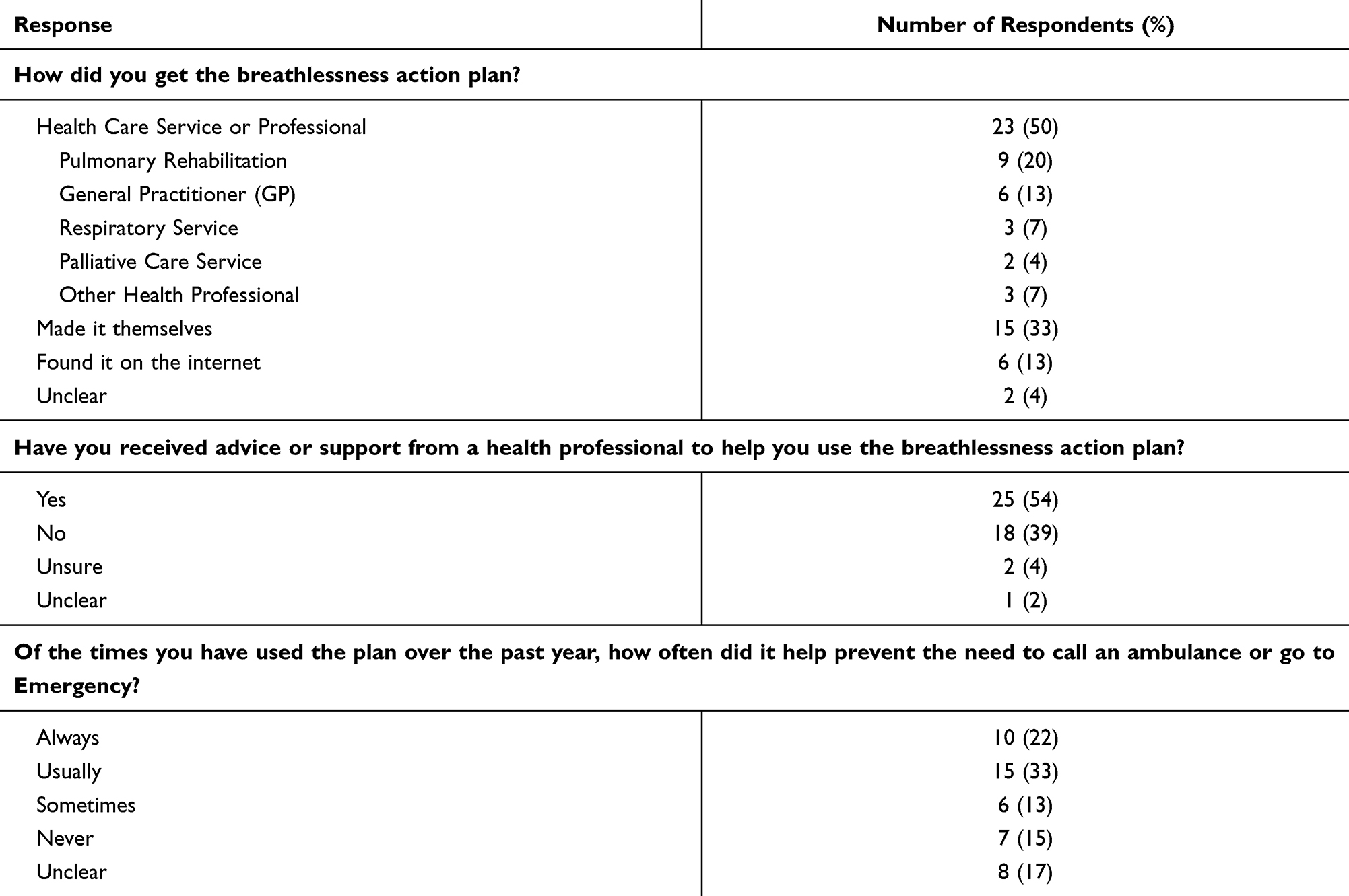 |
Table 2 Summary of Plan Use as Reported by People with COPD (n=45) and One Support Person |
Clinicians Recommending and /or Using Plans with People with COPD in Their Care
Of the 142 respondents who started the clinician survey, 3% (n=4/142) were excluded because they did not provide any data, 6% (n=8/142) because they provided demographic data only, and 1% (n=2/142) because they were from a non-OECD country. Of the 128 included in the analysis, 73% (n=93/128) completed all items. See Table 3 for sample characteristics.
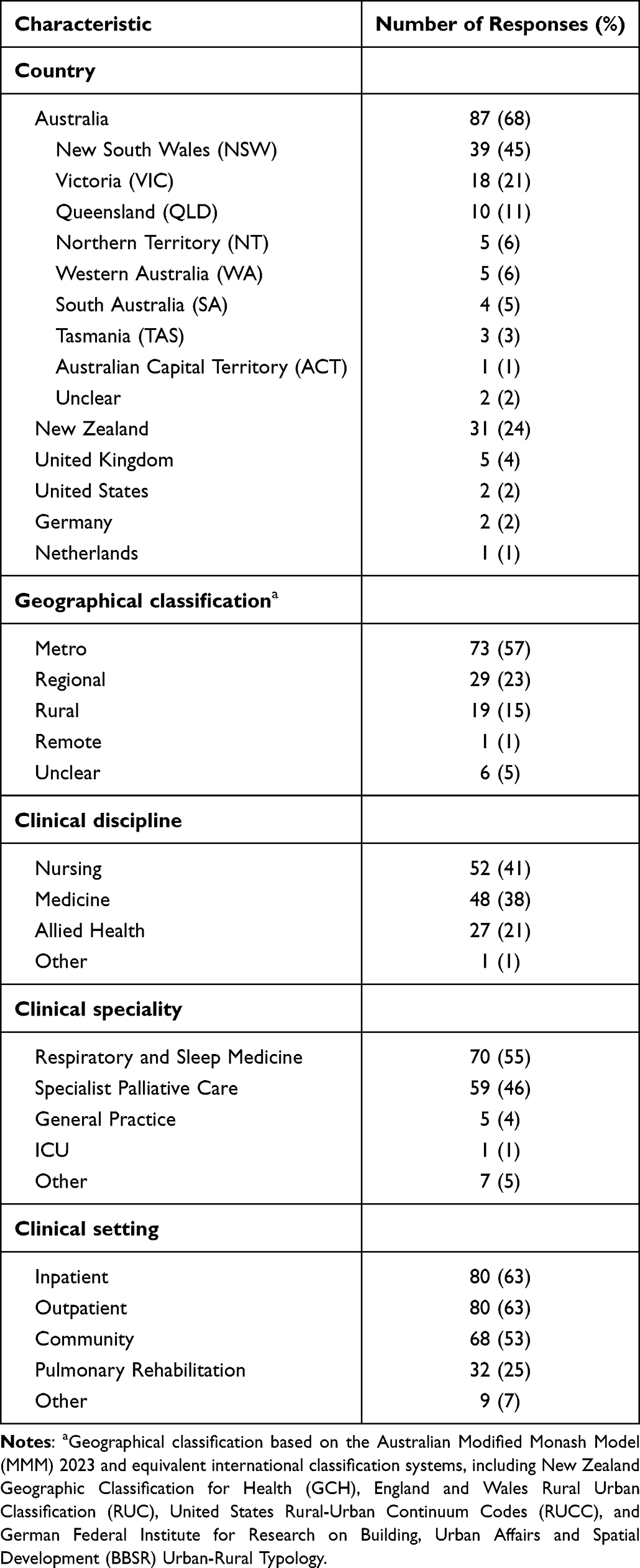 |
Table 3 Summary Characteristics of Clinicians Responding to the Survey (n=128) |
Of 127 clinician respondents who answered the question on what proportion of patients with COPD they recommended a plan to, 44% (n=56/127) answered “most”, 27% (n= 34/127) “some”, 19% (n=24/127) “all” and 10% (n=13/127) “only a very small proportion”.
Plans were most often developed by the clinician or service they worked for through clinical experience (50%; n=63/127), adapted from other plans (49%; n=62/127), based on evidence or recommendations from literature (31%; n=40/127), or direct patient input (23%; n=29/127).
The majority (79%; n=100/127) of respondents monitored effectiveness, most often through feedback from patients (95%; n=95/127) or families (65%; n=65/127). Less commonly, they used: medical record reviews (19%; n=19/127), surveys of patients or families (8%; n=8/127), clinical trials (8%; n=8/127), clinical observation (4%; n=4/127) or clinical assessment tools for breathlessness (2%; n=2/127). Forty-four percent (n=56/127) of clinicians perceived that “most” patients given a plan benefitted, 35% (n=45/127) “some” and 6% (n=7/127) “all”, with 13% (n=17/127) “unsure”. Figure 3 summarises responses of 101 clinicians who reported on the kinds of benefits they thought patients derived from the plan.
 |
Figure 3 Proportions of clinician survey respondents reporting different kinds of benefits from using a breathlessness action plan (n=101). Note: “Other” benefits included an increased understanding of breathlessness, increased self-efficacy/empowerment, and clarity on what to do when sick. |
When asked how they introduced plans to patients, 93 clinicians responded as follows: by explaining how to use it (76%; n=71/93), personalising it to each patient (69%; n=65/93), a paper copy or weblink (63%; n=59/93), checking the patient’s ability to use the plan (45%; n=42/93) and “other” methods (9%; n=8/93). See Table 4 for an overview of additional education/resources provided alongside the plan.
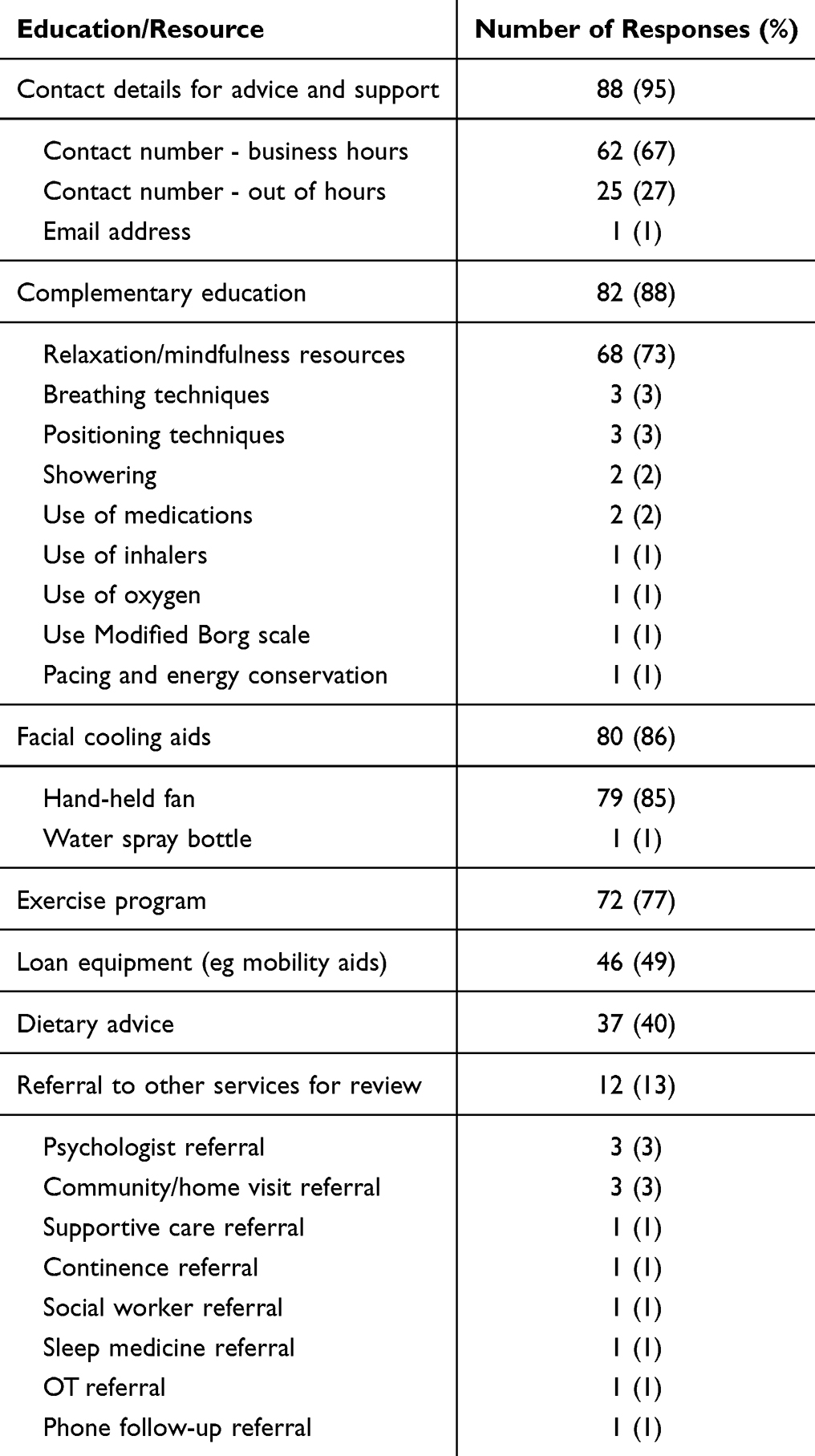 |
Table 4 Proportions of Clinician Survey Respondents Providing Additional Education and Resources to Patients and/or Families Alongside a Breathlessness Plan (n=93) |
Discussion
In comparison with COPD action plans, action plans for acute-on-chronic breathlessness episodes have received much less research attention. We found quantitative evidence for efficacy limited to one pre/post evaluation with a small sample and high risk of bias.25 There is also limited qualitative evidence for feasibility/acceptability of two other plans in the form of single data excerpts from two trials.26,27 Despite this paucity of evidence, 69 breathlessness action plans were identified either on the internet, in use by clinicians, or developed by plan-users themselves. These plans made similar recommendations regarding non-pharmacological strategies for episodic breathlessness. However, the 48 plans we could analyse in detail presented advice in diverse ways. PEMAT ratings for understandability and actionability were also found to vary between plans, with half using language above reading level grade 8 recommended for health information. Our cross-sectional survey data provide initial, limited evidence for efficacy as perceived by plan users and clinicians, which requires substantiation from future research. Most plan-users reported that their plan had reduced their need to seek emergency care for at least some episodes over the past year. Most clinician respondents also perceived there to be patient benefits, but this was based mostly on anecdotal evidence rather than research or quality assurance.
Plan Characteristics
Half the plans we identified were above the recommended reading level. This is especially concerning because COPD is associated with lower education levels and cognitive impairment.30,31 Reports from both user and clinician survey respondents suggest that plans may be commonly accessed or self-developed without related education and support. Indeed, user survey responses highlighted an unmet need for better breathlessness-related support more generally. This is consistent with research suggesting that health care professionals under-recognise breathlessness and have limited understanding of non-pharmacological strategies.32–35 Action plans might therefore serve a useful purpose in promoting breathlessness management among clinicians, as well as patients.
Only a few plans that we identified invited patients to personalise them, with a focus on medication dose/frequency and telephone numbers for support. Personalisation may be especially important in relation to advising when to seek emergency care. The plans in our pool recommended various thresholds for deciding this, including failure of non-pharmacological strategies, emergence of other symptoms besides breathlessness, and waiting for a specified time period. Surprisingly few plans referenced the complementary use of a COPD action plan. Qualitative research shows that uncertainty about when to seek emergency care in response to breathlessness can be a major concern for people with COPD and their support persons.9,36 Advice should take into account each person’s COPD features, comorbidities, mental health and social support, reviewing as these evolve over time. This will align with international consensus that COPD self-management requires person-centred, iterative support from clinicians to identify needs, set goals and evaluate and re-adjust management strategies.37
Perceived Benefit
Our survey found that users and clinicians alike perceived benefits from plans. Although self-reported data are no substitute for objective measures of healthcare usage, user perceptions that plans helped them to avoid unnecessary emergency care raise the possibility of potential gains in self-efficacy, which has been shown by previous research to be important for psychological wellbeing and willingness to engage in physical and social activities.38–40 Clinicians perceived increased confidence and reduced anxiety to be the most likely patient benefit from using the plan, with the second most likely being reduced frequency of episodes. Research continues to examine the “vicious cycle” between anxiety and breathlessness with the aim of informing interventions that can target both.41–43
Future Research Directions
Our scoping review identified a paucity of rigorous evaluative research on breathlessness action plans to date. This might stem, in part, from challenges with measuring real-time effects on breathlessness episodes. The paramedic study included in our review found that NRS measurement of breathlessness intensity every six minutes was deemed acceptable by patients and paramedics.26 However, methods for observing episodes when these are not attended by a health professional may be intrusive and/or confounded by myriad factors influencing severity and duration.5,6 Equally, whilst controlled observations have been recommended by some authors, this may reduce real-world interpretability and relevance of findings.
While fewer episodes might lessen patient distress, reduced frequency should not be achieved by avoiding activities of daily living. Instead, future research on breathlessness action plans should aim to increase patients’ confidence that episodes can be successfully controlled and therefore that daily activities can be safely increased, with benefits to physical health and psychosocial wellbeing. Increasing self-efficacy also has potential to encourage uptake and completion of pulmonary rehabilitation for which fear of breathlessness is a documented barrier.44 Importantly, this means that breathlessness action plans may lead to an increase rather than decrease in breathlessness episodes at least in the short term. This renders frequency uninterpretable unless accompanied by contextual measures of daily activity. Data on COPD exacerbations and other medical determinants of activity and acute care use should also be collected as context.
Strengths and Limitations
This is the first review of breathlessness management to have involved persons with lived experience and support persons, who contributed equally with other team members to define the review’s inclusion criteria and appraise included plans. Involvement of this kind can increase the relevance and rigour of reviews, as well as enrich interpretation.45 Involving people with COPD and support persons in rating the quality of plans in particular increased the external validity of our findings.
The main limitation of our survey was the small number of clinicians, people with COPD and especially support persons who participated. Whilst it’s impossible to estimate a response rate, this is likely to have been very low given the number of health services and other organisations we recruited through. Respondents could not be identified as unique (eg through cookies or IP address), and data were unavailable to estimate response, view or participation rates. Open online surveys are also subject to a volunteer effect and other sampling biases that reduce generalisability of findings. To have learned about and accessed the online questionnaire, COPD/support person respondents must have been relatively digitally and health literate although, even then, over a third seemed to have misunderstood the purpose of the survey as did not report having used a plan. Clinician respondents volunteering to take part were likely to have been more proactive than average in supporting their patients with self-management of breathlessness. This means our findings may under-estimate unmet need within the COPD community at large and also provide insights into current “best practice” upon which to build future efforts. When interpreting results on plan benefits from our survey, readers should note that respondents were provided with a list of potential benefits rather than generated these themselves. Another limitation of our research is its cross-sectional nature, which provides only a “snapshot” of practice and plans in rapidly evolving environments, especially online. Increasingly, plan-users might be seeking self-management advice from online tools that use generative artificial intelligence rather than searching for plans from reputable organisations.36 However, to avoid over-burdening team members, we allocated a third of the plans to each pair, potentially reducing inter-rater reliability. Finally, like other formulae available for estimating reading grade, Flesch–Kincaid represents an over-simplification of literacy skills.46
Conclusion
Breathlessness action plans are available online for people with COPD and their support persons and are used in clinical practice. However, plan characteristics and quality are variable, and research evidence regarding efficacy is limited. Further research is needed to evaluate any potential benefits. First and foremost, research should test whether plans improve self-management of breathlessness episodes “in the moment”. Further studies can then explore whether this leads to improvements in breathlessness-related outcomes and healthcare usage. Outcome measurement in future trials should take into account likely relationships between frequency of breathlessness episodes, self-efficacy and activities of daily living.
Abbreviations
COPD, chronic obstructive pulmonary disease; ED, Emergency Department.
Acknowledgments
This paper is dedicated to the fond memory of Don Dennett, who contributed his experience of living with COPD and breathlessness as a member of the project team, but died in May 2025.
We would also like to acknowledge contributions to the review and survey recruitment by Dr Ester Klimkeit who provided early intellectual input to the project and Dr Layla Edwards, Dr Eric Torgbenu and Dr Domenica Disalvo, who worked as research assistants at UTS IMPACCT.
Funding
This research was funded by a Medical Research Future Fund (MRFF) Emerging Priorities and Consumer-Driven Research initiative grant (ID 2023248).
Disclosure
Professor Michael Crooks reports grants, personal fees and/or non-financial support from NIHR, Asthma + Lung UK, AstraZeneca, Chiesi, Sanofi, Synairgen, Orion, and Roche, outside the submitted work. Professor David Currow reports personal fees for Intellectual property payments and advisory payments from Maybe Pharma International Pty Ltd, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Luckett T, San Martin A, Currow DC, Johnson MJ, Barnes-Harris MM, Phillips JL. A systematic review and meta-analysis of studies comparing burden from lung cancer and chronic obstructive pulmonary disease. Palliative Med. 2020;34(10):1291–16. doi:10.1177/0269216320940153
2. Simon ST, Higginson IJ, Benalia H, et al. Episodic and continuous breathlessness: a new categorization of breathlessness. J Pain Sympt Manag. 2013;45(6):1019–1029. doi:10.1016/j.jpainsymman.2012.06.008
3. Burge S, Wedzicha J. COPD exacerbations: definitions and classifications. Eur Respir J. 2003;21(41 suppl):46s–53s. doi:10.1183/09031936.03.00078002
4. Simon ST, Weingärtner V, Higginson IJ, Voltz R, Bausewein C. Definition, categorization, and terminology of episodic breathlessness: consensus by an international delphi survey. J Pain Sympt Manag. 2014;47(5):828–838. doi:10.1016/j.jpainsymman.2013.06.013
5. Simon ST, Bausewein C, Schildmann E, et al. Episodic breathlessness in patients with advanced disease: a systematic review. J Pain Sympt Manag. 2013;45(3):561–578. doi:10.1016/j.jpainsymman.2012.02.022
6. Simon ST, Higginson IJ, Benalia H, et al. Episodes of breathlessness: types and patterns–a qualitative study exploring experiences of patients with advanced diseases. Palliative Med. 2013;27(6):524–532. doi:10.1177/0269216313480255
7. Weingartner V, Scheve C, Gerdes V, et al. Characteristics of episodic breathlessness as reported by patients with advanced chronic obstructive pulmonary disease and lung cancer: results of a descriptive cohort study. Palliat Med. 2015;29(5):420–428. doi:10.1177/0269216314563428
8. Luckett T, Phillips J, Johnson M, et al. Insights from Australians with respiratory disease living in the community with experience of self-managing through an emergency department ‘near miss’ for breathlessness: a strengths-based qualitative study. BMJ open. 2017;7(12):e017536. doi:10.1136/bmjopen-2017-017536
9. Hutchinson A, Galvin K, Johnson MJ. “So, I try not to go” acute-on-chronic breathlessness and presentation to the emergency department: in-depth interviews with patients, carers, and clinicians. J Pain Sympt Manag. 2020;60(2):316–325. doi:10.1016/j.jpainsymman.2020.03.014
10. Linde P, Hanke G, Voltz R, Simon S. Unpredictable episodic breathlessness in patients with advanced chronic obstructive pulmonary disease and lung cancer: a qualitative study. Support Care Cancer. 2018;26(4):1097–1104. doi:10.1007/s00520-017-3928-9
11. Kelly AM, Holdgate A, Keijzers G, et al. Epidemiology, treatment, disposition and outcome of patients with acute exacerbation of COPD presenting to emergency departments in Australia and South East Asia: an AANZDEM study. Respirology. 2018;23(7):681–686. doi:10.1111/resp.13259
12. Spathis A, Booth S, Moffat C, et al. The breathing, thinking, functioning clinical model: a proposal to facilitate evidence-based breathlessness management in chronic respiratory disease. NPJ Prim Care Respiratory Med. 2017;27(1):27. doi:10.1038/s41533-017-0024-z
13. Holland AE, Spathis A, Marsaa K, et al. European respiratory society clinical practice guideline on symptom management for adults with serious respiratory illness. Eur Respir J. 2024;63(6):2400335. doi:10.1183/13993003.00335-2024
14. Reitzel T, Bergmann A, Schloesser K, et al. The experience of episodic breathlessness from the perspective of informal caregivers: a qualitative interview study. Ann Palliative Med. 2022;11(7):2225–2234. doi:10.21037/apm-21-3361
15. Agency for Healthcare research and Quality (AHRQ). Health literacy universal precautions toolkit - make action plans: tool 15. AHRQ. Available from: https://www.ahrq.gov/health-literacy/improve/precautions/tool15.html.
16. Lenferink A, Brusse‐Keizer M, van der Valk P, et al. Self‐management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;8(8). doi:10.1002/14651858.CD011682.pub2
17. Howcroft M, Walters EH, Wood‐Baker R, Walters JAE. Action plans with brief patient education for exacerbations in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;2016(12). doi:10.1002/14651858.CD005074.pub4
18. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Internal Med. 2018;169(7):467–473. doi:10.7326/M18-0850
19. Eysenbach G. Improving the quality of web surveys: the checklist for reporting results of internet E-surveys (CHERRIES). J Med Internet Res. 2004;6(3):e34–e34. doi:10.2196/jmir.6.3.e34
20. Shoemaker SJ, Wolf MS, Brach C. Development of the patient education materials assessment tool (PEMAT): a new measure of understandability and actionability for print and audiovisual patient information. Patient Educ Couns. 2014;96(3):395–403. doi:10.1016/j.pec.2014.05.027
21. Canberra Health Literacy Hub. Writing health information for consumers. Available from: https://cbrhl.org.au/health-services-providers/writing-patient-information/.
22. Kincaid JP, Fishburne RP, Rogers RL, Chissom BS. Derivation of new readability formulas (automated readability index, fog count, and flesch reading ease formula) for Navy enlisted personnel. Research Branch Report. 1975: 8–75.
23. The University of Sydney. Sydney health literacy lab. Available from: https://www.sydneyhealthliteracylab.org.au/.
24. Higgins J, Thomas J, Chandler J, et al. eds. Cochrane Handbook for Systematic Reviews of Interventions Version 6.5. Cochrane; 2024.
25. Qian MYY, Politis J, Thompson M, et al. Individualized breathlessness interventions may improve outcomes in patients with advanced COPD. Respirology. 2018;23(12):1146–1151. doi:10.1111/resp.13324
26. Hutchinson A, Allgar V, Cohen J, et al. Mixed-methods feasibility cluster randomised controlled trial of a paramedic-administered breathlessness management intervention for acute-on-chronic breathlessness (BREATHE): study findings. ERJ Open Res. 2022;8(4):00257–2022. doi:10.1183/23120541.00257-2022
27. Reilly CC, Maddocks M, Chalder T, Bristowe K, Higginson IJ. A randomised, controlled, feasibility trial of an online, self-guided breathlessness supportive intervention (SELF-BREATHE) for individuals with chronic breathlessness due to advanced disease. ERJ Open Res. 2023;9(2):00508–2022. doi:10.1183/23120541.00508-2022
28. Schneidman A, Reinke L, Donesky D, CarrieriKohlman V, Carrieri-Kohlman V. Sudden breathlessness. Am J Respir Crit Care Med. 2022;205(11):P22–P24. doi:10.1164/rccm.20511P22
29. Mularski RA, Reinke LF, Carrieri-Kohlman V, et al. An official American thoracic society workshop report: assessment and palliative management of dyspnea crisis. Ann Am Thoracic Soc. 2013;10(5):S98–S106. doi:10.1513/AnnalsATS.201306-169ST
30. Zhang Z, Yang P, Xiao G. Prevalence and risk factors of cognitive impairment in COPD: a systematic review and meta‐analysis. Public Health Nurs. 2025;42(3):1389–1407. doi:10.1111/phn.13524
31. Zhang H, Hu D, Xu Y, Wu L, Lou L. Effect of pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis of randomized controlled trials. Ann Med. 2022;54(1):262–273. doi:10.1080/07853890.2021.1999494
32. Collier A, Rowett D, Allcroft P, Greene A, Currow DC. Academic detailing of general practitioners by a respiratory physician for diagnosis and management of refractory breathlessness: a randomised pilot study. BMC Health Serv Res. 2015;15(1):1–5. doi:10.1186/s12913-015-0861-9
33. Johnston KN, Young M, Kay D, Booth S, Spathis A, Williams MT. Attitude change and increased confidence with management of chronic breathlessness following a health professional training workshop: a survey evaluation. BMC Med Educ. 2020;20(1):1–14. doi:10.1186/s12909-020-02006-7
34. Curran J, Elliott R, Fry M. A survey of community nurses’ knowledge and strategies used to relieve breathlessness in people with chronic obstructive pulmonary disease. British J Commun Nurs. 2023;28(8):384–392. doi:10.12968/bjcn.2023.28.8.384
35. Ahmadi Z, Sandberg J, Shannon-Honson A, Vandersman Z, Currow DC, Ekström MJ. Is chronic breathlessness less recognised and treated compared with chronic pain? A case-based randomised controlled trial. Eur Respir J. 2018;52(3):1800887. doi:10.1183/13993003.00887-2018
36. Hasnain M, Hayat A, Hussain A. Revolutionizing chronic obstructive pulmonary disease care with the open AI application: chatGPT. Ann Biomed Eng. 2023;51(10):2100–2102. doi:10.1007/s10439-023-03238-6
37. Effing TW, Vercoulen JH, Bourbeau J, et al. Definition of a COPD self-management intervention: international expert group consensus. Eur Respir J. 2016;48(1):46–54. doi:10.1183/13993003.00025-2016
38. Selzler A-M, Habash R, Robson L, Lenton E, Goldstein R, Brooks D. Self-efficacy and health-related quality of life in chronic obstructive pulmonary disease: a meta-analysis. Patient Educ Couns. 2020;103(4):682–692. doi:10.1016/j.pec.2019.12.003
39. Yi Q-F, Yang G-L, Yan J. Self-efficacy intervention programs in patients with chronic obstructive pulmonary disease: narrative review. Int J Chronic Obstr. 2021;Volume 16:3397–3403. doi:10.2147/COPD.S338720
40. Ekström M. Why treatment efficacy on breathlessness in laboratory but not daily life trials? The importance of standardized exertion. Curr Opin Support Palliative Care. 2019;13(3):179–183. doi:10.1097/SPC.0000000000000444
41. Schloesser K, Bergmann A, Eisenmann Y, et al. Interaction of panic and episodic breathlessness among patients with life-limiting diseases: a cross-sectional study. Ann Palliat Med. 2023;12(5):900–911. doi:10.21037/apm-22-1304
42. Baglow D, Johnston K, Williams M. Existential aspects of breathlessness in serious disease. Curr Opin Support Palliat Care. 2024;18(4):183–190. doi:10.1097/spc.0000000000000736
43. Bleazard L, Walker K, Ashton S, Faull C. ‘It helps my anxiety because I’m managing my breathlessness’: a qualitative exploration of anxiety and breathlessness in patients with advanced chronic respiratory disease receiving specialist palliative care. medRxiv. 2025;
44. Cox NS, Oliveira CC, Lahham A, Holland AE. Pulmonary rehabilitation referral and participation are commonly influenced by environment, knowledge, and beliefs about consequences: a systematic review using the theoretical domains framework. J Physiother. 2017;63(2):84–93. doi:10.1016/j.jphys.2017.02.002
45. Oliver S, Liabo K, Stewart R, Rees R. Public involvement in research: making sense of the diversity. J Health Serv Res Policy. 2015;20(1):45–51. doi:10.1177/1355819614551848
46. Jindal P, MacDermid JC. Assessing reading levels of health information: uses and limitations of flesch formula. Educ Health. 2017;30(1):84–88. doi:10.4103/1357-6283.210517
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.