")
Back to Journals » Clinical Ophthalmology » Volume 17
Non-Invasive Treatment of Early Diabetic Macular Edema by Multiwavelength Photobiomodulation with the Valeda Light Delivery System
Authors Kaymak H, Munk MR, Tedford SE , Croissant CL, Tedford CE, Ruckert R, Schwahn H
Received 28 April 2023
Accepted for publication 26 October 2023
Published 22 November 2023 Volume 2023:17 Pages 3549—3559
DOI https://doi.org/10.2147/OPTH.S415883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hakan Kaymak,1,2 Marion R Munk,3– 5 Stephanie E Tedford,6 Cindy L Croissant,6 Clark E Tedford,6 Rene Ruckert,4,6 Hartmut Schwahn1
1I.I.O.GbR Breyer Kaymak Klabe, Duesseldorf, Germany; 2Experimental Ophthalmology, University Hospital and Medical Faculty of the University of Saarland, Homburg/Saar, Germany; 3Department of Ophthalmology, Inselspital University Hospital Bern, Bern, Switzerland; 4Eyegnos Consulting, Bern, Switzerland; 5Augenarzt-Praxisgemeinschaft Gutblick AG, Pfäffikon, Switzerland; 6LumiThera, Inc, Poulsbo, WA, USA
Correspondence: Stephanie E Tedford, LumiThera, Inc, Poulsbo, WA, USA, Email [email protected]
Purpose: Diabetes is associated with ocular complications including diabetic macular edema (DME). Current therapies are invasive and include repeated intravitreal injections and laser therapy. Photobiomodulation (PBM) is a treatment (Tx) that utilizes selected wavelengths of light to induce cellular benefits including reduction of inflammation and edema. This single-center, open-label, post-hoc analysis explored the utility of multiwavelength PBM in subjects with DME.
Methods: Analysis included review of data from patients undergoing standard clinical care with an approved and marketed PBM medical device, the Valeda® Light Delivery System. Subjects with early-stage DME with good vision (Best-corrected visual acuity (BCVA) > 20/25, logMAR > 0.1) were evaluated in clinic and treated with one series of multiwavelength PBM (Tx delivered 3x/week over 3– 4 weeks; total of 9 Tx sessions). Clinical, anatomical, and safety parameters were assessed in addition to subjective quality of life.
Results: A total of 30 eyes (19 subjects) were analyzed. Subjects were predominately male (68.4%) with a mean age of 56 ± 14 years. Reductions in central retinal thickness (CRT), resolution of intraretinal fluid (IRF) and improvement in diabetic retinopathy severity scale scores were observed following PBM treatment in select patients. Baseline BCVA remained stable over the follow-up observation period of 3 months post-PBM. Approximately 64% of patients reported subjective improvements in their ocular condition and decreased influence in everyday life. Detailed OCT evaluations confirmed no safety issues related to phototoxicity up to 16 months.
Conclusion: Early-stage DME subjects treated with Valeda multiwavelength PBM showed improvements in clinical and anatomical parameters. The Valeda multiwavelength PBM approach demonstrates a favorable safety profile with no signs of phototoxicity following an independent OCT review. PBM therapy may offer an alternative, non-invasive treatment strategy with a unique mechanism and modality for patients with early-stage DME.
Keywords: photobiomodulation, diabetic macular edema, low level light therapy, diabetic retinopathy, central retinal thickness, Valeda Light Delivery System, DME, PBM, DR, CRT
Introduction
Prevalence of type 1 (T1DM) and type 2 (T2DM) diabetes have reached a state of epidemic highs with the incidence of diabetes increasing at an alarming pace.1–4 Worldwide, diabetes is estimated to affect 463 million people and future estimates suggest an increase to 578 million by the year 2030.1 Diabetes can cause serious sight threatening complications like diabetic retinopathy (DR) and diabetic macular edema (DME).5 Within the first 10 years of living with diabetes, retinopathy can be diagnosed in nearly all T1DM patients and in over 60% of those with T2DM.6 A meta-analysis of pooled incidence of diabetic eye disease among individuals with diabetes in Europe shows a 25.7% and 3.7% prevalence of DR and DME, respectively. A meta-regression shows a higher prevalence of DR in persons with T1DM compared to persons with T2DM (54.4% vs. 25%). In Europe, it is estimated that persons with diabetes affected by any diabetic eye disease will increase from 6.4 to 8.6 million by 2050, of whom 30% will require close monitoring and/or treatment.7
DME is a severe ocular complication of diabetes which affects best-corrected visual acuity (BCVA) and can lead to blindness if left untreated.8 The pathophysiology of DME is complex, involving oxidative stress, mitochondrial dysfunction, elevated concentrations of vascular endothelial growth factor (VEGF) and a breakdown of the inner blood-retinal barrier, resulting in the extracellular fluid accumulation in the macula and decreased vision.9 DME is characterized by cystic thickening of the retina and/or lipid deposition The long-term prognosis for DME is poor, and treatment is recommended immediately, once a patient is diagnosed.10 However, patients are typically not started on treatment before visual impairment is present.11 Evidence from randomized, controlled trials indicates that early intervention in DME is imperative for optimal improvement in vision outcomes.12–14 Improvement in the pathological underpinnings of the disease at earlier stages prior to significant visual impairment is of interest.
Until recently, the standard ophthalmic treatment for patients with visual impairment due to DME was non-pharmacological interventions including laser photocoagulation, which provides vision stabilization. The use of intravitreal treatments (IVT) of agents that inhibit vascular endothelial growth hormone (anti-VEGF) has replaced laser photocoagulation as first-line therapy based on several multi-center clinical trial data demonstrating superiority over laser treatment.15 However, treatments with anti-VEGF agents are invasive, requiring multiple repeated injections into the eye, are expensive, and are only partially effective in some patients. Intravitreal injections also have potential severe sight-threatening complications such as endophthalmitis or retinal detachment.15 The development, testing and application of novel treatment strategies is critical for reducing the impending clinical and socioeconomic burden of diabetic eye disease state and will provide quantifiable benefits to a patient population that demonstrates a significant need for clinical aid.
Photobiomodulation (PBM) involves the use of visible light to near infrared light (NIR) (500–1000 nm) produced by a laser or a non-coherent light source applied to the surface of the body to produce beneficial effects in a wide range of disease states.16–19 The mechanism of PBM at the cellular level has been ascribed to the activation of mitochondrial respiratory chain components resulting in stabilization of metabolic function and initiation of signaling cascades, which promote cellular proliferation and cytoprotection.20–23 A growing body of evidence suggests that Cytochrome c Oxidase (CcO) is a key photoacceptor of light in the far red to NIR spectral range and the primary mode for mechanistic underpinnings.20–23 The utility of PBM in ocular indications has been explored both preclinically and clinically and shows promising results in both clinical, anatomical and quality of life (QoL) endpoints.24–26
Several independent studies show potential benefit of PBM in patients with DME.27–29 Oxidative stress and local inflammatory changes are believed to contribute to progression of DME. PBM shows inhibitory effects on both oxidative stress and inflammatory processes and therefore may be of benefit in DME.27 This series of case studies aimed to investigate through a post-hoc analysis the potential impact of multiwavelength PBM on clinical, anatomical, and QoL parameters in early-stage DME patients with good vision.
Materials and Methods
Study Subjects
This study was retrospective in design and included subjects who had a diagnosis of early-stage DME, best-corrected visual acuity (BCVA) scores of > 20/25 (logMAR > 0.1) with no urgent need for IVT (i.e., no significant acute or persistent edema, no proliferative DR, no acute vision impairment). Patients were included with evidence of DME, either defined by the presence of intraretinal cysts, or diffuse retinal thickening defined by presence of an increased retinal thickness (focally) associated with hyporeflectivity of the outer nuclear layer within the whole 6×6 mm optical coherence tomography (OCT) volume scan, lacking clearly well-defined cystic spaces with or without the presence of accompanying hard exudates (HEs). Patients which had received IVT in the past due to a worse condition at that time, responded well to IVT, and thus had returned to (and maintained) a milder DME were eligible. Eligibility was dependent on the latest IVT (> 6 weeks prior) provided all inclusion criteria were met. Data was evaluated from patients who consented from a single clinical site in Dusseldorf, Germany (MVZ Breyer Kaymak Klabe). Use of patient data was approved at the local ethic committee (No. 2018124 Äk Nordrhein). All patients provided informed consent on the processing and publication of their ocular and QoL data in anonymized form.
Photobiomodulation Treatment
The Valeda® Light Delivery System (Valeda; LumiThera, Inc, Poulsbo, WA, USA) delivered multiwavelength PBM treatment via light emitting diodes (LED) at selected wavelengths (590, 660, and 850 nm). Delivery of multiwavelength PBM provides a multi-targeted approach at the cellular level driving benefits in clinical outcomes. Treatment followed the previously published protocol using a repeated intermittent design. Each treatment series consisted of 9 PBM sessions delivered 3×/week over 3–4 weeks.30,31 Modifications to the protocol were imposed in cases due to scheduling conflicts. Each treatment session took approximately <5 minutes per eye. Each eye was treated independently. Valeda delivered 590 nm (4 mW/cm2) and 850 nm (0.6 mW/cm2) wavelengths combined through the open eyelid and the 660 nm (65 mW/cm2) wavelength through the closed eyelid. Valeda has CE-approval in the European Union.
Ophthalmic Examination
Clinical outcomes included BCVA as assessed by objective refraction (KR-800, Topcon Healthcare, Germany). Anatomical outcomes utilized OCT (Cirrus 5000 and Cirrus 6000, Carl Zeiss, Germany) imaging performed before PBM treatment at Baseline, immediately after the 9 treatment sessions (Month 1) and at ~ 3 months follow-up (Month 3). Presence of DME was defined by the presence of intraretinal ± subretinal fluid (SRF) ± presence of HEs on OCT. Presence of intraretinal fluid (IRF) was defined either by the presence of intraretinal cysts and/or by the presence of diffuse retinal thickening. Diffuse retinal thickening was present in the case of an increased retinal thickness (focally) associated with hyporeflectivity of the outer nuclear layer, lacking clearly well-defined cystic spaces. Subjects received IVT if they met the indications in accordance with the Statement of the German Ophthalmological Society, the German Retina Society, and the Professional Association of Ophthalmologists in Germany on treatment of DME.32 Using the OCT-images, the following anatomical parameters were assessed by an independent leading retinal imaging expert (Marion R. Munk) to establish both safety and anatomical benefits: central 1 mm subfield retinal thickness (CRT), retinal volume (RV), presence of IRF, SRF, HE, epiretinal membrane (ERM), disorganization of inner retinal layers (DRIL), and vitreomacular traction (VMT). Safety parameters including Integrity of photoreceptor layers (PR) and integrity of retinal pigment epithelium (RPE) were evaluated. Wide field color fundus images (CaliforniaTM, Optos LLC, Dunfermline, UK) were taken before and after PBM treatment and were analyzed to evaluate the diabetic retinopathy severity score (DRSS). The number and intervals of IVTs that became necessary due to a deterioration in the patient’s visual performance or other factors as individually decided by the treating ophthalmologist were analyzed as a parameter to assess PBM treatment. Efficacy and safety data over a follow-up observation period extending up to 16 months were analyzed. Approximately three months after initial PBM treatment, a site-specific customized questionnaire using the Likert scale was delivered to assess individual subjective evaluation of QoL, visual performance, influence on everyday life, and attitudes towards PBM.
Statistics
Statistical analyses and illustrations were performed using Microsoft Excel 2015 (Microsoft Co., Seattle USA), SPSS Statistics (IBM Inc., New York, USA) and language R (www.r-project.org). For the comparison of CRT and CRV during the 3 visits, a linear mixed effects model was used. For the comparison of categorical outcomes in IRF, SRF, HE, ERM, DRIL, VMT, PR, RPE, and DRSS during the 3 visits the McNemar´s test was employed. Due to the pilot nature of this retrospective analysis of patient data, not all parameters could be analyzed for all patients.
Results
Subject Characteristics
A total of 19 subjects (30 eyes) were evaluated. Patients with DME and good vision were treated with one series of 9 multiwavelength PBM sessions using Valeda and were followed for an average of 371.33 ± 135.36 days. Follow-up periods extended up to 16 months post-PBM treatment if data was available. Data was collected from a higher number of male subjects (n = 13, 68.4%) versus female (n = 6, 31.6%) with a mean age of 56 ± 14 years (range: 27–76 years). At Baseline, all subjects presented with good BCVA at 0.08 ± 0.13 logMAR (range: −0.1–0.4 logMAR). A total of 6 subjects (31.6%) were diagnosed with T1DM, 12 subjects (63.2%) with T2DM and 1 subject (5.3%) with T3DM. The mean interval between DM diagnosis until PBM treatment was 33.3 (SD 12.80), 18.17 (SD 7.93), and 3 years, respectively. A total of 12 subjects (63.0%) reported no changes in lifestyle (i.e., pregnancy; weight loss; trying of different lifestyles; work loss; changes in diet, drinking behavior and sugar intake) during PBM treatment.
Clinical Results
HbA1c Values
The mean HbA1c values during and after PBM treatment for subjects with T1DM, T2DM, and T3DM were as follows: T1DM, 8.0% and 7.7%; T2DM, 7.7% and 7.9%; T3DM 9.5% and 8.5%. A total of 11 subjects (58.0%) reported a stable Hb1Ac value.
Best-Corrected Visual Acuity
Mean BCVA at Baseline was 0.08 ± 0.13 logMAR (n = 30), 0.06 ± 0.09 logMAR (n = 30) at Month 1, and 0.08 ± 0.09 logMAR (n = 30) at Month 3. BCVA scores were maintained following PBM treatment with no statistically significant difference observed in BCVA at follow-up visits.
Central Retinal Thickness
Mean CRT was slightly elevated and above normal values in these early, good vision subjects. Mean CRT at Baseline was 293.6 ± 50.3 µm and significantly reduced at Month 1 to 284.1 ± 39.4 µm (p = 0.04; n = 30, LME model). At Month 3, CRT was 289.2 ± 46.9 µm which was not statistically significant (Table 1; Figure 1).
 |
Table 1 PBM Effect on Anatomical Outcomes |
 |
Figure 1 Reduction of CRT Following PBM Treatment. OCT imaging for the selected subject showed a reduction of CRT and HE following PBM treatment. Abbreviations: CRT, central retinal thickness; HE, hard exudates. |
Retinal Volume
Mean RV at Baseline was 10.28 ± 0.76 mm3 and 10.28 ± 0.78 mm3 at Month 1 (n = 28). At Month 3, mean RV was 10.25 ± 0.79 mm3 (n = 29) (Table 1). No statistically significant changes were observed between visits (p > 0.05).
Intraretinal Fluid
All 30 eyes enrolled showed IRF at Baseline: intraretinal cysts were present in 27 eyes (90.0%) and diffuse retinal thickening without clearly well-defined hyporeflective cystic spaces was present in 3 eyes (10.0%). IRF was completely resolved in 10/30 eyes (33.3%) following PBM treatment at Month 1 (p < 0.0001; McNemar´s test). At Month 3, 24/30 eyes (80.0%) showed IRF (p < 0.0001; McNemar´s test) (Figure 2). IRF within the central 1 mm subfield was present in 21/30 eyes (70.0%) at Baseline but in only 16/30 eyes (53.3%) at Month 1 and at Month 3. A significant decrease in central 1 mm subfield IRF was observed (p = 0.06; McNemar´s test).
 |
Figure 2 Reduction of IRF Following PBM Treatment. IRF at Baseline was present in all 30 eyes, in 20/30 eyes at Month 1, and in 24/30 eyes at Month 3. A statistically significant decrease could be found between Baseline and Months 1 and 3 (*p < 0.0001; McNemar´s test). Abbreviation: IRF, intra-retinal fluid. |
Subretinal Fluid and Hard Exudates
SRF was present in only 1/30 eyes (3.3%) analyzed at Baseline. This SRF was fully resorbed at Month 1 and none of the eyes developed SRF from Baseline to Month 3. HEs were present in 20/30 eyes (66.7%) at Baseline. At Month 1, 16/20 eyes (80.0%) showed HE; thus, in 20.0% of eyes HEs were fully resorbed. However, this finding was not statistically significant (p = 0.13; McNemar´s test). At Month 3, 19/20 eyes (95.0%) showed HEs (p = 1.00; McNemar´s test) compared to Baseline.
Additional OCT Parameters
In 8 eyes (26.7%), ERM was detectable at Baseline and Month 1, and in 9 eyes (30.0%) at Month 3. During Baseline, Month 1, and Month 3, no changes in DRIL or in VMT were observed.
Integrity of Photoreceptor Layers and Retinal Pigment Epithelium
No loss of outer retinal integrity (integrity of ELM, EZ and IZ) could be found in 18/30 eyes (60.0%) analyzed at Baseline and Month 1. No loss of outer retinal integrity was observed in 16 eyes (53.3%) at Month 3. In the remaining 12 eyes (40.0%), where a loss of PR integrity was detectable already at Baseline, it remained stable following PBM treatment at Month 1 which was maintained through Month 3. For 7/12 eyes (58.3%), previous focal laser scars were the underlying source of loss in integrity. After 3 Months, 2 eyes (6.7%) showed PR disintegrity, which was not present at Baseline. In 1 eye (3.3%), a small focal EZ disruption developed exactly below an intraretinal cyst which has decreased in size at Month 3. The other eye had drusen due to age-related macular degeneration and a small focal EZ disruption developed at the site of a druse. In 22/30 eyes (73.3%) no loss of RPE integrity was identified. In the remaining 8 eyes, RPE defects could be detected at every visit, however in 5 eyes this was due to focal laser scars. No changes in RPE integrity status were found between the 3 visits. No adverse events (ocular or systemic) were reported by subjects during the study period.
Diabetic Retinopathy Severity Scale
Optos wide field images were available prior (n = 28) and approximately 3 months after PBM treatment (n = 24). In 21/24 eyes (87.5%) assessed, no change in DRSS score was found. One eye improved from mild NPDR (DRSS score: 35) to very mild NPDR (DRSS score: 20). In 3 eyes, DRSS improved from moderately severe NPDR (DRSS score: 47) to moderate NPDR (DRSS score: 43) with one additional IVT after the PBM treatment (Table 2; Figure 3).
 |
Table 2 PBM Effect on DRSS |
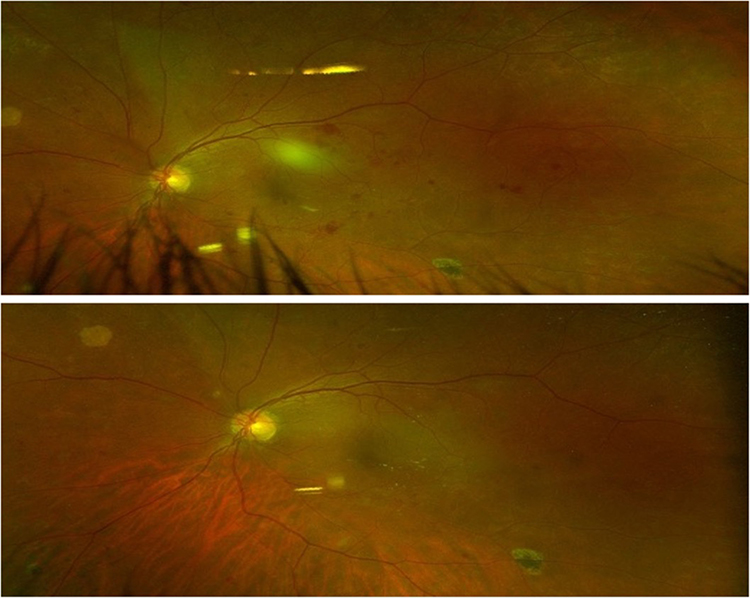 |
Figure 3 DRSS pre- and post-PBM. A selected patient showing a one-step improvement in DRSS scoring from 47 (moderate DR) to 43. Significant reduction of hemorrhage and IRMAs is seen in color fundus imaging from Baseline (top) after PBM treatment (bottom) at Month 1. The CVA slightly increased from 0.08 ± 0.12 to 0.06 ± 0.08 (logMAR). Abbreviations: CVA, corrected visual acuity; DR, diabetic retinopathy; DRSS, diabetic retinopathy severity score; IRMA, Intraretinal microvascular abnormalities; PBM, Photobiomodulation. |
Requirements for IVT with Anti-VEGF
Before PBM treatment, 9/30 eyes (30.0%) had previously received at least one IVT (range from a total of 2 to 30 IVTs; mean: 12 ± 9 IVTs). IVT treatment timepoints ranged from 31–610 days prior; 21 eyes (70.0%) that were evaluated were IVT treatment naive. After PBM treatment, 3/9 eyes (33.3%) which previously received IVT and 5/21 eyes (23.8%) of the treatment naive group received IVT based on the treating physicians’ decision. Accordingly, 6/9 eyes (67.0%) which previously received IVT and 16/21 eyes (76.2%) that were treatment naïve did not require IVT in the 3 months following PBM therapy. In the additional 371 days follow-up, 62.0% of eyes did not require any IVT (2/9 eyes which previously received IVT and 13/21 treatment naive eyes). The mean number of days for the 15 eyes from the last (9th) PBM treatment session to the first IVT post-PBM was 82.67 ± 52.10 days with a median of 67 days.
Quality of Life (QoL)
The QoL questionnaire assessed subjective influence and improvement on daily life. Three months after PBM treatment, 64.0% of patients continued to report subjective improvements in respect to their ocular condition, while 36.0% of the patients had reported subjective improvement, but could not assess if this improvement was continuing. No patient reported a worsening of his/her ocular condition after PBM treatment. Additionally, 64.0% of the patients noted a decrease in the influence of their ocular condition on their everyday life after PBM treatment (Figure 4).
 |
Figure 4 Improvement in Quality of Life following PBM. A. Three months after PBM treatment, 64.0% of subjects continued to report subjective improvements. B. Three months after PBM treatment, 64.0% of subjects reported a decrease in the influence of their ocular condition on their everyday life. |
Discussion
The current study evaluated the effect of multiwavelength PBM delivered by the Valeda Light Delivery System on early-stage DME subjects with good vision. Following one series of PBM treatment, benefits in several anatomical parameters as measured by OCT imaging and subjective evaluation on QoL were observed. Subjects enrolled showed good vision at Baseline so consequently, no PBM beneficial effect on BCVA scores was observed; however, BCVA scores remained stable. The PBM treatment was well tolerated, with no signs of phototoxicity observed based on both functional and anatomical outcomes assessed.
Pharmacologic therapy using anti-angiogenic compounds via IVT is standard of care and known to be effective in various ocular conditions including DME,33 despite the inherent risks for ocular and systemic side effects. The subjects enrolled in this pilot study showed early-stage DME where IVT therapy was not yet required. The benefit of treating earlier stage DME with non-invasive PBM is that anatomical improvements in macular edema or DRSS may be seen and could delay or reduce the need for more invasive and risky treatment options including IVT. Additionally, long term destructive effects of macular edema leading to disintegrity of retinal cell connectivity and alteration of the outer retinal layers could be prevented. Anti-VEGF trials (i.e., The RISE, RIDE, BOLT, VIVID, and VISTA studies) also suggest that earlier intervention in DME is critical to achieving optimal improvement in clinical outcomes (i.e., loss of visual acuity).13,14,34–36 Sham- or laser-treated patients crossed over to ranibizumab or aflibercept treatment after 24 months achieve smaller visual acuity gains than those who started treatment at the onset of their respective study.13,35 PBM provides a unique approach to non-invasively initiate treatment with potential to impact both clinical and anatomical outcomes. Despite the benefits of the anti-VEGF medications, not all patients respond equally well. In the RISE, RIDE, VIVID, and VISTA studies, around 60% of patients did not achieve a 15-letter improvement in visual acuity.13,14,34–36 These are usually the patients who do not show high VEGF levels, but rather high levels of other cytokines, such as IL-6.37–39Therefore, alternate therapeutic options, or those that could be employed with additive clinical benefit are of high impact in the field.
Following PBM treatment, 76.0% of the treatment naive eyes diagnosed with DME did not require IVT (according to their attending ophthalmologist based on a worsening of fluid) for 3 months following PBM treatment, and 62.0% of the treatment naive eyes did not require IVT for at least 12 months following PBM treatment. In a conventional setting, it is recommended to delay IVT in early DME patients until visual acuity decreases or morphological changes are observed. In the majority of study patients, an IVT was not required for more than one year after the diagnosis and subsequent initial PBM treatment.
OCT imaging can be used for screening, classification, monitoring, and treatment evaluation of DME. OCT provides information on CRT and distinct morphological features of the edema and persistent morphological changes after DME treatment.33 For the subjects analyzed retrospectively in this study, all morphological parameters either showed a significant improvement (CRT and IRF) or a stabilization following PBM treatment which was maintained up to 3 months. Moreover, it is important to mention that the treated patients had nearly normal CRT due to the early stage of DME and good vision, therefore a huge step in improvement was not expected. A stabilization of these parameters is of value for patients with early-stage DME to postpone subsequent invasive therapies.
Visual acuity was not improved; in no cases was there a significant worsening of this outcome measure. Based on the functional and anatomical outcomes, no signs of phototoxicity could be identified and no ocular or systemic side effects were detected or self-reported by any subjects. This demonstrates the favorable safety profile of PBM treatment with Valeda and is in keeping with the excellent safety profile reported in PBM treatment delivered to other ocular and non-ocular indications.31,36,40,41
Similar to our results, several groups have published previous reports in DME showing anatomical benefit following PBM treatment.27–29 A pilot study (n = 21) evaluating PBM at 670 nm delivered at 25, 100 or 200 mW/cm2 thrice weekly for 4 weeks shows significant reduction at all three settings in central macular thickness (CMT) at 2 months. Treatment with PBM was well tolerated at settings up to 200 mW/cm2 with no significant side effects. Resolution of IRF at month 2 was observed in select patients and remained dry out to 6 months without additional intervention.28 Tang et al evaluated PBM (670 nm) treatment in patients with non-center involving DME. This non-randomized, consecutive, case series (n = 4) showed positive effects following PBM delivered for 160 secs per day for 2–9 months. PBM treatment caused a significant reduction in focal retinal thickening in all treated eyes. No adverse effects attributable to therapy were noted by the patients or study investigators during the study period.27 Eells et al likewise evaluated 670 nm PBM treatment 3 days/week for 8 weeks in treatment resistant DME patients and saw reductions in CRT and over one line improvement in BCVA at 6 months on.29
Subsequent to our study, a Phase 2 randomized controlled trial evaluating PBM in eyes with CI-DME and good visual acuity was reported by the DRCR.net. One eye of each subject (n = 135) was randomized 1:1 to a 670-nm light emitting PBM eye patch or a device emitting broad-spectrum white light. Subjects were treated for 90 seconds twice daily for 4 months. The recently published report shows no effect of PBM on clinical (BCVA) or anatomic central subfield thickness (CST) endpoints from PBM treatment as delivered using their PBM device and protocol. A thorough evaluation of PBM on OCT anatomical outcomes aside from CST was not provided in the report. Of note, PBM was well-tolerated over 4 months of twice daily use with no serious adverse events reported.
In the field of PBM, we are presented with a large number of illumination parameters such as wavelength, fluence, power density, pulse structure, treatment time and treatment interval as well as distinct tissue scatter and absorption parameters for each wavelength. In addition, the cellular targets are not equivalent across wavelengths. PBM devices are not standardized or regulated to ensure consistent and reliable outputs. These factors may significantly contribute to discrepancies observed in the field across clinical trials. Further research is necessary to fully elucidate the precise parameters for PBM best effects and to optimize treatment amongst indications and at the patient level. The current study employed the Valeda Light Delivery System which delivers a unique multiwavelength PBM approach designed to target specific cellular substrates. The Valeda design delivers a uniform, expanding bundle of non-coherent light to the retinal tissue. Valeda has been employed in multiple clinical trials evaluating multiwavelength PBM in dry AMD.31,41,42 Furthermore, the multiwavelength PBM approach Valeda employs was similarly delivered in the TORPA II study (i.e., combination 590, 670 and 790 nm) in dry AMD using alternate devices. These studies employed the same treatment protocol as used in the current study (i.e., 9 PBM treatments delivered over 3–4 weeks) and showed immediate and sustained improvement in aspects of clinical and anatomical function in dry AMD subjects. The current study explored the translation of observed ocular benefits with multiwavelength PBM treatment delivered via Valeda to the DME patient population.
Limitations of this study includes its case series design and lack of a randomized control arm. Another limitation may be that treatment naïve as well as pretreated patients were included. While the current study reports on small numbers, this is an exploratory evaluation showing potential for benefit in this patient population. Further studies will be necessary to corroborate these findings.
Conclusion
The results of this pilot study provide supportive evidence that repeated multiwavelength PBM treatments delivered over a period of 3 to 4 weeks is a non-invasive and safe treatment option for patients with early-stage DME patients with good vision. The anatomical benefits and subjective evaluations suggest disease-modifying effects with PBM treatment in patients with early-stage DME. These data add to the beneficial effects noted in prospective clinical trials for dry AMD using Valeda and expands the potential safe and effective utility of multiwavelength PBM to DME. These data support further investigations of prospective, randomized control trials to study the potential of PBM treatment as a therapeutic approach for early-stage DME patients and other ocular indications that share overlapping pathology.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This case series consisted of a post-hoc analysis of patients undergoing standard clinical care with an approved and marketed medical device. Use of patient data was approved at the local ethic committee (No. 2018124 Äk Nordrhein). As this was a retrospective analysis on consented patient data, the study was not included in a registry. Informed consent was obtained from all subjects. All methods were carried out in accordance with relevant guidelines and regulations. This study complies with the Declaration of Helsinki.
Acknowledgments
The abstract of this paper was presented at the Association for Research in Vision and Ophthalmology Conference as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in ARVO Journals: https://iovs.arvojournals.org/article.aspx?articleid=2774919.
Funding
There is no funding to report.
Disclosure
HK and HS have received partial funding from LumiThera to support the current research efforts. ST, CLC, MRM, RR and CT are all employed by LumiThera as full-time employees or consultants. The authors report no other conflicts of interest in this work.
References
1. Antonetti DA, Klein R, Gardner TW. Diabetic retinopathy. N Engl J Med. 2012;366(13):1227–1239. doi:10.1056/NEJMra1005073
2. Ding J, Wong TY. Current epidemiology of diabetic retinopathy and diabetic macular edema. Curr Diab Rep. 2012;12(4):346–354. doi:10.1007/s11892-012-0283-6
3. Cheung N, Mitchell P, Wong TY. Diabetic retinopathy. Lancet. 2010;376(9735):124–136. doi:10.1016/S0140-6736(09)62124-3
4. Bullard KM, Cowie CC, Lessem SE, et al. Prevalence of Diagnosed Diabetes in Adults by Diabetes Type - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(12):359–361. doi:10.15585/mmwr.mm6712a2
5. Singh A, Stewart JM. Pathophysiology of diabetic macular edema. Int Ophthalmol Clin. 2009;49(2):1–11. doi:10.1097/IIO.0b013e31819fd164
6. Shani M, Eviatar T, Komaneshter D, et al. Diabetic retinopathy -incidence and risk factors in a community setting- a longitudinal study. Scand J Prim Health Care. 2018;36(3):237–241.
7. Li JQ, Welchowski T, Schmid M, et al. Prevalence, incidence and future projection of diabetic eye disease in Europe: a systematic review and meta-analysis. Eur J Epidemiol. 2020;35(1):11–23. doi:10.1007/s10654-019-00560-z
8. Davidov E, Breitscheidel L, Clouth J, et al. Diabetic retinopathy and health-related quality of life. Graefes Arch Clin Exp Ophthalmol. 2009;247(2):267–272. doi:10.1007/s00417-008-0960-y
9. Ferris FL, Patz A. Macular edema. A complication of diabetic retinopathy. Surv Ophthalmol. 1984;28(Suppl):452–461. doi:10.1016/0039-6257(84)90227-3
10. Augustin A, Loewenstein A, Kuppermann BD. Macular edema. General pathophysiology. Dev Ophthalmol. 2010;47:10–26.
11. Baker CW, Glassman AR, Beaulieu WT, et al. Effect of initial management with aflibercept vs laser photocoagulation vs observation on vision loss among patients with diabetic macular edema involving the center of the macula and good visual acuity: a randomized clinical trial. JAMA. 2019;321(19):1880–1894. doi:10.1001/jama.2019.5790
12. Heier JS, Korobelnik J-F, Brown DM, et al. Intravitreal aflibercept for diabetic macular edema: 148-week results from the vista and VIVID Studies. Ophthalmology. 2016;123(11):2376–2385. doi:10.1016/j.ophtha.2016.07.032
13. Brown DM, Nguyen QD, Marcus DM, et al. Long-term outcomes of ranibizumab therapy for diabetic macular edema: the 36-month results from two Phase III trials: RISE and RIDE. Ophthalmology. 2013;120(10):2013–2022. doi:10.1016/j.ophtha.2013.02.034
14. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology. 2012;119(4):789–801. doi:10.1016/j.ophtha.2011.12.039
15. Falavarjani KG, Nguyen QD. Adverse events and complications associated with intravitreal injection of anti-VEGF agents: a review of literature. Eye. 2013;27(7):787–794. doi:10.1038/eye.2013.107
16. Chung H, Dai T, Sharma SK, et al. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2012;40(2):516–533. doi:10.1007/s10439-011-0454-7
17. Hashmi JT, Huang -Y-Y, Osmani BZ, et al. Role of low-level laser therapy in neurorehabilitation. Pm r. 2010;2(12 Suppl 2):S292–305. doi:10.1016/j.pmrj.2010.10.013
18. Tata DB, Waynant RW. Laser Therapy: a review of its mechanism of action and potential medical applications. Laser Photon Rev. 2010;5(1):1–12. doi:10.1002/lpor.200900032
19. Rojas JC, Gonzalaz-Lima F. Low level light therapy of the eye and brain. Dovepress. 2011;2011(3):49–67.
20. Grossman N, Schneid N, Reuveni H, et al. 780 nm low power diode laser irradiation stimulates proliferation of keratinocyte cultures: involvement of reactive oxygen species. Lasers Surg Med. 1998;22(4):212–218. doi:10.1002/(SICI)1096-9101(1998)22:4<212::AID-LSM5>3.0.CO;2-S
21. Karu T, Pyatibrat L, Kalendo G. Irradiation with He-Ne laser increases ATP level in cells cultivated in vitro. J Photochem Photobiol B. 1995;27(3):219–223. doi:10.1016/1011-1344(94)07078-3
22. Karu TI, Kolyakov SF. Exact action spectra for cellular responses relevant to phototherapy. Photomed Laser Surg. 2005;23(4):355–361. doi:10.1089/pho.2005.23.355
23. Eells JT, Wong-Riley MTT, VerHoeve J, et al. Mitochondrial signal transduction in accelerated wound and retinal healing by near-infrared light therapy. Mitochondrion. 2004;4(5–6):559–567. doi:10.1016/j.mito.2004.07.033
24. Muste JC, Kalur A, Iyer A, et al. Photobiomodulation therapy in age-related macular degeneration. Curr Opin Ophthalmol. 2021;32(3):225–232. doi:10.1097/ICU.0000000000000742
25. Geneva II. Photobiomodulation for the treatment of retinal diseases: a review. Int J Ophthalmol. 2016;9(1):145–152.
26. Eells JT, Gopalakrishnan S, Valter K. Near-Infrared Photobiomodulation in Retinal Injury and Disease. Adv Exp Med Biol. 2016;854:437–441.
27. Tang J, Herda AA, Kern TS. Photobiomodulation in the treatment of patients with non-center-involving diabetic macular oedema. Br J Ophthalmol. 2014;98(8):1013–1015. doi:10.1136/bjophthalmol-2013-304477
28. Shen W, Teo KYC, Wood JPM, et al. Preclinical and clinical studies of photobiomodulation therapy for macular oedema. Diabetologia. 2020;63(9):1900–1915. doi:10.1007/s00125-020-05189-2
29. Nonarath HJ. 670nm photobiomodulation modulates bioenergetics and oxidative stress, in rat Müller cells challenged with high glucose. PLoS One. 2021;16(12):e0260968.
30. Burton B, Parodi MB, Jürgens I, et al. LIGHTSITE II randomized multicenter trial: evaluation of multiwavelength photobiomodulation in non-exudative age-related macular degeneration. Ophthalmol Therap. 2023;12(2):953–968. doi:10.1007/s40123-022-00640-6
31. Markowitz SN, Devenyi RG, Munk MR, et al. A double-masked, randomized, sham-controlled, single-center study with photobiomodulation for the treatment of dry age-related macular degeneration. Retina. 2020;40(8):1471–1482. doi:10.1097/IAE.0000000000002632
32. German Society of Ophthalmology (DOG) geschaeftsstelle@ dog. org, German Retina Society (RG), Professional Association of Ophthalmologists in Germany (BVA). Statement of the German Ophthalmological Society, the German Retina Society, and the Professional Association of Ophthalmologists in Germany on treatment of diabetic macular edema: dated August 2019. Ophthalmologe. 2021;118(Suppl 1):40–67. doi:10.1007/s00347-020-01244-w
33. Schmidt-Erfurth U, Garcia-Arumi J, Bandello F, et al. Guidelines for the management of diabetic macular edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2017;237(4):185–222. doi:10.1159/000458539
34. Michaelides M, Kaines A, Hamilton RD, et al. A prospective randomized trial of intravitreal bevacizumab or laser therapy in the management of diabetic macular edema (BOLT study) 12-month data: report 2. Ophthalmology. 2010;117(6):1078–1086.e2. doi:10.1016/j.ophtha.2010.03.045
35. Brown DM, Schmidt-Erfurth U, Do DV, et al. Intravitreal aflibercept for diabetic macular edema: 100-week results from the vista and VIVID Studies. Ophthalmology. 2015;122(10):2044–2052. doi:10.1016/j.ophtha.2015.06.017
36. Ao J, Chidlow G, Wood JPM, et al. Safety profile of slit-lamp-delivered retinal laser photobiomodulation. Transl Vis Sci Technol. 2020;9(4):22. doi:10.1167/tvst.9.4.22
37. Funatsu H, Noma H, Mimura T, et al. Association of vitreous inflammatory factors with diabetic macular edema. Ophthalmology. 2009;116(1):73–79. doi:10.1016/j.ophtha.2008.09.037
38. Vujosevic S, Micera A, Bini S, et al. Aqueous humor biomarkers of Müller cell activation in diabetic eyes. Invest Ophthalmol Vis Sci. 2015;56(6):3913–3918. doi:10.1167/iovs.15-16554
39. Hillier RJ, Ojaimi E, Wong DT, et al. Aqueous humor cytokine levels as biomarkers of disease severity in diabetic macular edema. Retina. 2017;37(4):761–769. doi:10.1097/IAE.0000000000001210
40. Bensadoun RJ. Photobiomodulation or low-level laser therapy in the management of cancer therapy-induced mucositis, dermatitis and lymphedema. Curr Opin Oncol. 2018;30(4):226–232. doi:10.1097/CCO.0000000000000452
41. Merry GF, Munk MR, Dotson RS, et al. Photobiomodulation reduces drusen volume and improves visual acuity and contrast sensitivity in dry age-related macular degeneration. Acta Ophthalmol. 2017;95(4):e270–e277. doi:10.1111/aos.13354
42. Perich L, Improvement of visual function and electroretinography following photobiomodulation (Valeda) treatment in dry age-related macular degeneration subjects (ELECTROLIGHT); 2021.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.