Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Non-Dermatophyte Mold Dominated Onychomycosis in Patients Attending a Rank Higher Specialized Dermatology Clinic in Addis Ababa, Ethiopia
Authors Bitew A ![]() , Osman F, Yassin S
, Osman F, Yassin S
Received 10 January 2022
Accepted for publication 12 March 2022
Published 23 March 2022 Volume 2022:15 Pages 507—518
DOI https://doi.org/10.2147/CCID.S357738
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Adane Bitew,1 Feruza Osman,2 Seid Yassin3
1Department of Medical Laboratory Science, College Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Saint Peter’s Specialized Tuberculosis Referral Hospital, Addis Ababa, Addis Ababa Administrative Region, Ethiopia; 3International Care and Treatment for HIV/AIDS Program, Emergency Operation Center, Addis Ababa, Ethiopia
Correspondence: Adane Bitew, Department of Medical Laboratory Science, College Health Sciences, Addis Ababa University, P.O.Box: 1176, Addis Ababa, Ethiopia, Tel +251911039162, Email [email protected]
Background: Onychomycosis is a common refractory fungal infection associated with significant morbidity. The objective of this study was to determine the prevalence of onychomycosis, and the diversity and species composition of fungal etiological agents.
Materials and Methods: A clinic-based, prospective, non-randomized cross-sectional study was carried out between October 2018 and June 2019 at Rank Higher Specialized Dermatology Clinic, Addis Ababa, Ethiopia. Nail scrapings were collected aseptically from 200 patients clinically identified with nail disorders of fungal origin by dermatologists. Fungal etiological agents were identified microscopically and by culture method following standard procedures.
Results: Among 200 nail scrapings, 161 (80.5%) samples were found out to be culture positive. Of these, 135 (83.9%) samples yielded single colonies while 26 (16.1%) mixed colonies gave a total of 190 isolates. Among the isolates, 25.8% were dermatophytes while 61.1% were non- dermatophytes molds, and 13.1% were yeasts. Females were more likely to present dystrophic nails than men. Patients in the middle age group were more affected. Trichophyton interdigitale, Aspergillus spp, and Candida albicans were the dominant species.
Conclusion: The prevalence rate of onychomycosis in the present study was high. The isolation rate of non-dermatophyte molds was higher than dermatophytes and yeasts. Trichophyton interdigitale, Aspergillus spp, and Candida albicans were the dominant etiological agents. Females and patients in the middle age group were more affected. An increase in the prevalence of non-dermatophyte molds in nail infections dictates further investigation demonstrating how this group of fungi causes onychomycosis.
Keywords: prevalence, species diversity, dermatophytes, non-dermatophyte molds, opportunistic fungi, Ethiopia
Introduction
Onychomycosis or tinea unguium is the most frequent fungal infection of fingernails and toenails. It is caused by dermatophytes, non-dermatophyte mycelial fungi, and yeast.1–3 The infection is less common in fingernails than in toenails and is characterized by nail discoloration, roughening thickening, and splitting.4 The condition is the most common nail abnormality experienced globally, accounting for roughly 50–60% of all nail degenerations.5
Although onychomycosis is not a life-threatening disease, its morbidity is highly considerable. Permanent damage to the nail, high treatment cost, the spread of the infection to other persons, and occupational discomfort, have made the infection a major public health problem.6 Furthermore, the disease can be complicated by cellulitis, osteomyelitis, and soft tissue and bone necrosis in an individual with underlying diseases such as diabetes and HIV.7 Moreover, the psychological and social effects of onychomycosis significantly undermine labor and social lives and as high as 92% psychosocial impact has been reported.8
The prevalence of onychomycosis and its etiological agents vary from one region to another and from place to place in the same region. Geographic, environmental and demographic differences have been identified as major predisposing factors for these variations. Chronic diseases resulting from aging, increased use of immunosuppressive drugs, and an increase in the prevalence of underlying disease (such as HIV) have significantly attributed to an increase in the incidence of onychomycosis by compromising the immune status of the host.1–4,9 Moreover, increased exposure to spas and public swimming pools has also been recognized as a potential risk factor for the rise in mycoses.10,11 While the true magnitude of onychomycosis is far from resolved (ie, prevalence figures in the literature are highly variable), its prevalence, etiological agents, and risk factors associated with the disease are well documented all over the globe. Regrettably, there is only a single study conducted exclusively on onychomycosis in Ethiopia, a country consisting of more than a hundred million people.12 Socioeconomic limitations and other common prevalent health problems have been incriminated as major difficulties for such study. To this effect, the main objectives of this study were to determine the magnitude of the disease, the diversity, and the species composition of fungal pathogens causing onychomycosis.
Materials and Methods
Study Area and Design
This clinic-based, prospective, non-randomized cross-sectional study was carried out between October 2018 and June 2019. The study was conducted at Rank Higher Specialized Dermatology Clinic, Addis Ababa, Ethiopia.
Population
Source of Population
Patients with skin-related diseases seek health service at Rank Higher Specialized Dermatology Clinic.
Study Population
Clinically confirmed onychomycosis patients attending the study site.
Selection and Enrolment of Study Subjects
Inclusion and Exclusion Criteria
Individuals who present clinical pictures of onychomycosis are included. Individuals with other forms of skin-related diseases and those with onychomycosis that have already been under antifungal treatment were excluded from the study.
Sample Size Determination
The sample size was calculated by employing the formula for a single proportion sample size calculation by taking a 95% confidence interval, a 5% margin of error, and a prevalence of onychomycosis from earlier work12 conducted at Addis Ababa (0.133 or 13%) as shown below.
n= (Zα/2)2 P (p-1)/d2 where
Z=standard normal value corresponding to 95% confidence interval for a two-sided test which is equal to 1.96
P= prevalence of onychomycosis (11.3%) from the earlier study
D=margin of error which is equal to 5%; substituting these into the formula, n=154 but we added 3/4th of our sample size to increase the chance of isolating fungi from patients who came to our study site rising our study population to 200.
Data Collection Procedure
Demographic Data
The socio-demographic data (age, gender) and history of the previous antifungal treatment of each study subject were obtained from a Laboratory request form completed by attending dermatologists.
Data Quality Assurance and Quality Control
Pre-Analytical
Socio-demographic characteristics of study participants (age, sex, etc.) and clinical and treatment information were collected from the request form and laboratory logbook.
Analytical
The performance of autoclaves, incubators, reagents, microscopes, and the microbiological quality of culture medium (the sterility of culture media and growth performance of each culture medium) were evaluated as per standard procedures before they are used. Collection of clinical samples and transportation was carried out following an aseptic procedure. Inoculation of clinical samples was performed under a level II safety cabinet.
Post-Analytical
All the extracted information such as laboratory findings were checked for eligibility, completeness, and consistency and recorded before entry into a statistical tool. The data were also kept in a secure location. Fungal isolates were stored as per the standard operational procedure (SOP) of Addis Ababa University.
Ethics Approval and Consent to Participate
Ethical approval of this study was obtained from the Internal Review Board (IRB) of the Department of Medical Laboratory Science, College of Health Sciences, Addis Ababa University (Protocol number: DRERC/401/19/MLS/). Our study was carried out in complies with the declaration of Helsinki and signed written informed consent from all participants or their legally authorized representatives was obtained.
Laboratory Investigation
Sample Collection and Inoculation
Nail scrapings were collected by rubbing the active edge of the affected nail with sterile blades, one for each study subject. Before collection, the nail was cleaned with 70% (v/v) ethanol. The sample was then collected and transferred into a sterile plastic petri-dish correctly labeled with the name, age, sex of each patient, and date of collection. All collected specimens were then brought to the Department of Medical Laboratory Sciences, College of Health sciences following standard procedure. Part of each nail scrapings was examined for the presence of fungal elements (arthroconidia, macro and/or microconidia, and chlamydospores) microscopically after digesting the specimen for 5–10 minutes with 20% Potassium Hydroxide (KOH) supplemented with 5% glycerol solution using 10 and 40 magnification power objective lenses. The other portion of each specimen was inoculated on duplicate Sabouraud’s Dextrose Agar (SDA) plates supplemented with chloramphenicol (100µgml−1), gentamycin (50 µgml−1), and cycloheximide (100µgml−1) under safety cabinet level II. One of the duplicates of SDA plates contains no cycloheximide. Chloramphenicol, gentamycin SDA, and cycloheximide are products of Oxoid, Basingstoke. All plates were incubated at 25° C aerobically for up to four weeks. Culture plates were examined twice a week for any fungal growth. Culture plates with no growth were recorded as negative after four weeks of incubation at 25°C aerobically.
Fungal Culture Identification
Fungi were identified by studying the microscopic and macroscopic characteristics of each culture. Pigmentation of the obverse and the reverse side, texture, topography, and rate of growth of each culture were considered for macroscopic identification. Microscopic characteristics of fungi were studied by employing a lactophenol cotton blue (LPCB) staining procedure. Briefly, a drop of LPCB stain was placed on a clean glass slide. A piece of fungal culture was placed on clean glass slides containing LPCB. Stained slides were then covered with a cover slide and examined for macro and micro-conidia, chlamydospores, arthroconidia, the morphology of reproductive structures, and special structures of hyphae such as spirals, pectinate, and racquet hyphae, by using Low (10X) and high (40X) objective lenses. In most cases of non-dermatophyte molds or yeast identification, cultures were considered positive when the same single organism grew on repeated cultured samples obtained from the same untreated patient. Many mycological laboratory texts and manuals were used as reference materials in the process of identification. Features seen in the stained slide were compared with established characteristics of fungal features using mycology atlases.13–15
Results
Sex and Age Profile of Study Subjects
The sex and age profile of study subjects is depicted in Table 1. Nail scrapings were collected from 200 outpatient study participants in which the number of female study participants (136; 68%) outnumbered that of male study participants (64; 32%) where the female-male ratio was 2:1. The ages of the study participant ranged from 2 to 72 years. The number of study subjects across the age group was variable in which the age group of 25–44 years was the highest (93; 46.5%) followed by age groups of 15–24 (49; 24.5%) and 45–64 (27; 13.5%), respectively.
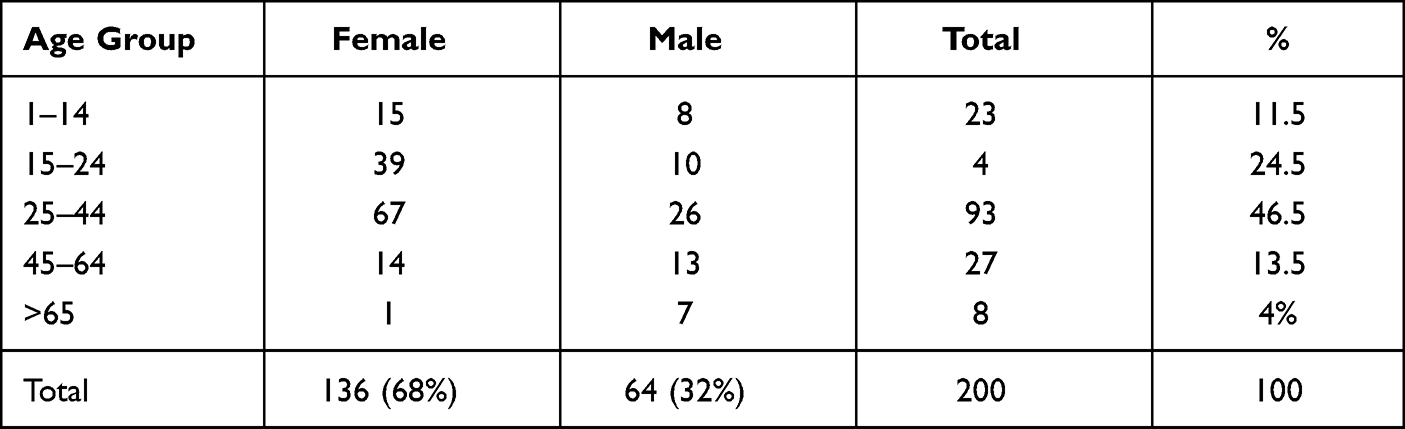 |
Table 1 Age and Gender Profile of Study Participants (n=200) |
Out of 200 nail scrapings collected and cultured, fungal species grew from 161 (80.5%) nail scrapings. Out of 161 culture-positive scrapings, 65.8% (106/161) and 34.2% (55/161) were reported from female and male study subjects, respectively. Consequently, the isolation rate of fungi was higher in females than in male study subjects. The distribution of fungal isolates varies regarding age. In general, the percentage positivity rate per age group depicted those patients in the age group of 15–44 were more affected (68.9; 111/200) than the other age groups (Table 2).
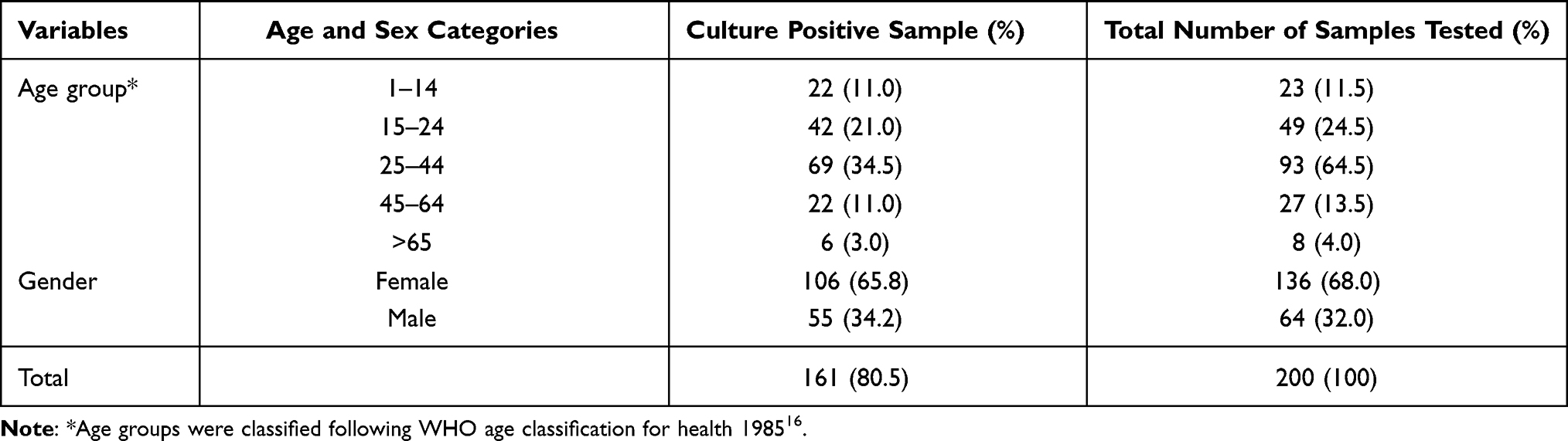 |
Table 2 Frequency of Culture-Positive Samples with Gender and Age (n= 200) |
Diversity and Species Composition of Fungal Isolates
The diversity and species composition of fungi isolated in the current study is presented in Table 3. Among 200 nail scrapings, 161 (80.5%) samples were found out to be culture positive. Of these 135 (83.9%) samples yielded single colonies while 26 (16.1%) mixed colonies gave a total of 190 isolates. Among the study population, fungi showed no visible fungal growth in 39 (16.5%) samples even though samples were collected from lesions compatible with onychomycosis. Among the isolates, 25.8% (49/190) were dermatophytes while 61.1% (116/190) were non- dermatophytes mycelial fungi, and 13.1% (25/190) were yeasts. The frequency of dermatophytes in their descending order was T. interdigitale (16; 32.7%), T. rubrum (8; 16.3%), T. verrucosum (6; 12.2%), M. audouinii (6; 12.2%), T. soudanense (5; 10.2%), T. violaceum (4; 8.2%), T. tonsurans (3; 6.1%), and M. ferrugineum (1; 2.0%). Among 49 dermatophyte isolates, 27 (55. 1%) were anthropophilic while 23 (44.9%) were zoophilic. Moreover, 42 (85.7%) were species of the genus Trichophyton while the remaining 7 (14.3%) were members of the genus Microsporum. Species of Aspergillus, (30; 25.4%), Cladosporium (14; 11.9%), Fusarium (12; 10.2%), Penicillium (11; 9.3%), Scytalidium dimidiatum (11; 9.3%), Alternaria (10; 8.5%), and Curvularia (10; 8.5%) were the dominant isolates among non-dermatophyte mycelial fungi. Of 25 yeast isolates, 64. 0% (16/25) was accounted for by C. albicans.
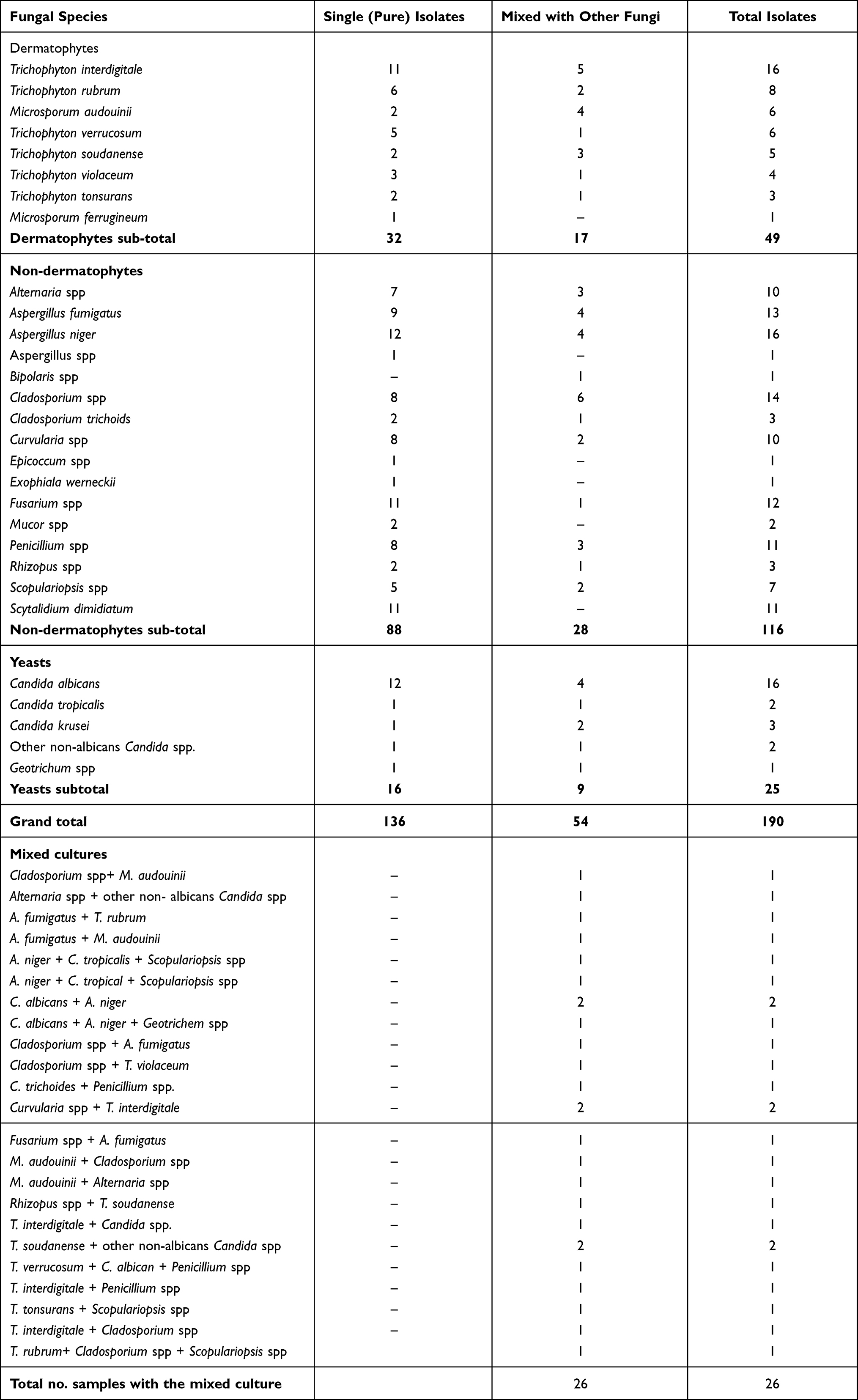 |
Table 3 The Diversity and Species Composition of Fungal Isolates in Patients with Clinically Confirmed Onychomycosis (n=200) |
Correlation of Direct Microscopy with Culture
Culturing was more efficient than direct microscopic examination. Fungal pathogens were detected in 61 (30.5%) clinical samples microscopically while fungi grew in 161 (80.5%) clinical samples. Out of 200 clinical samples, 55 (27.5%) were positive both in culture and microscopically. Six (3%) samples were microscopic positive but culture negative. One hundred six (53.0%) negative clinical samples microscopically were found out to be positive in culture. Thirty-three (16.5%) samples were turned out to be negative both microscopically and in culture (Table 4).
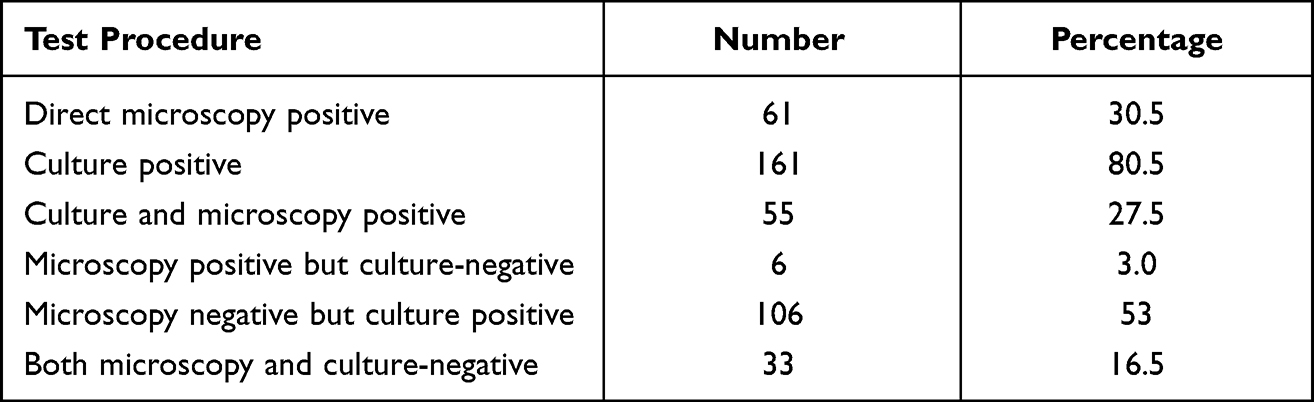 |
Table 4 Correlation of Direct Microscopy with Culture |
Distribution of Fungal Isolates Based on Gender
The distribution of fungal isolates according to gender was depicted in Table 5. Out of 190 isolates, 127 were recovered from female study participants while the remaining 63 isolates were recovered from male study participants.
 |
Table 5 Distribution of Fungal Isolates According to Gender (n=190) |
Distribution of Fungal Isolates Based on Age
The distribution of fungal isolates according to the age group is shown in Table 6. The distribution of fungal isolates varied along with age groups. Of a total of 190 fungal isolates, 111 (69%) were isolated in the age group of 15–24 and 25–44 years.
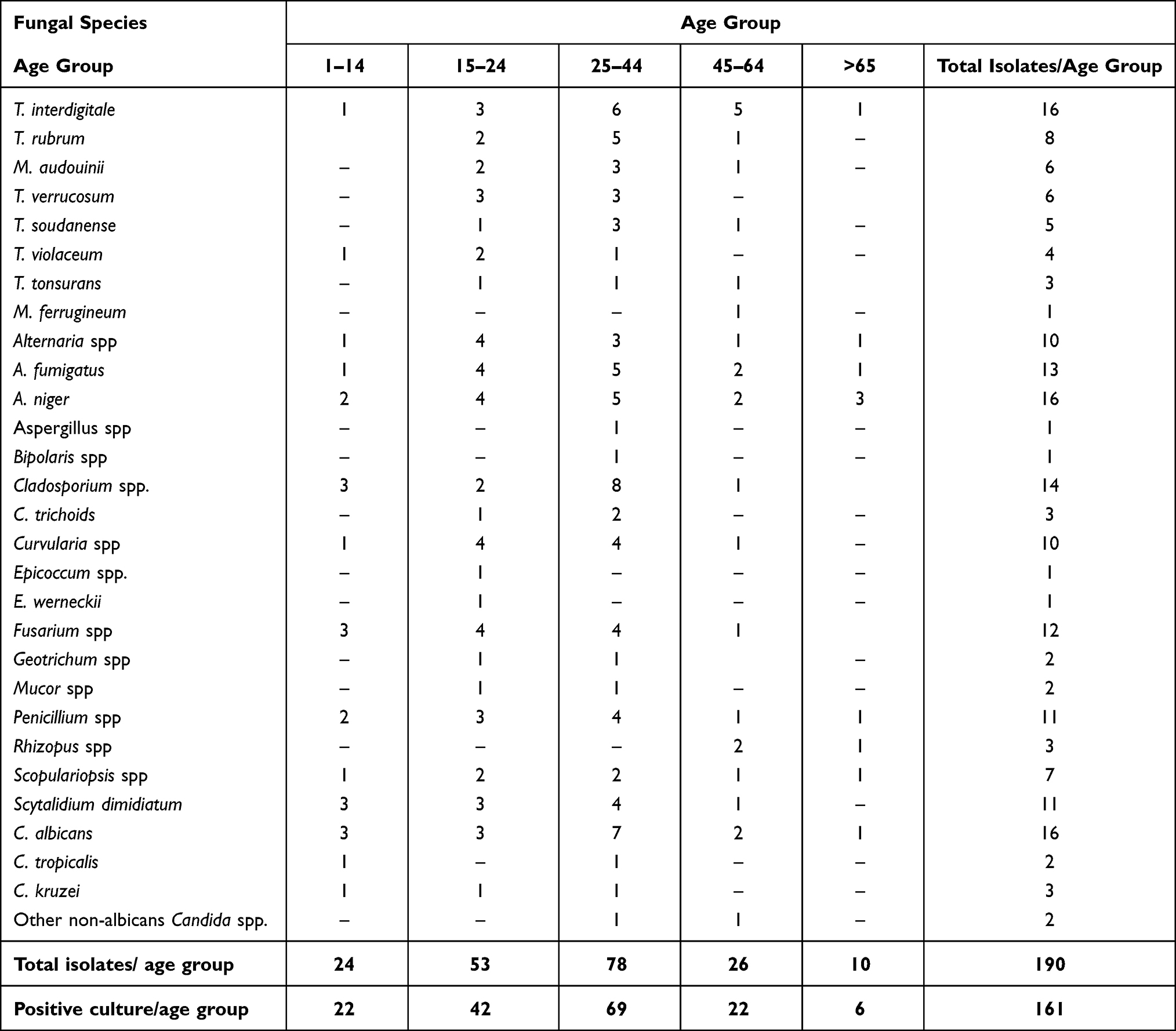 |
Table 6 Distribution of Fungal Isolates According to Age Groups (n=190) |
Discussion
In Ethiopia, like most developing countries, studies on the burden of fungal infections, in general, are a neglected area of study. Socioeconomic constraints and giving precedence to other common predominant health issues (ie, malaria, sexually transmitted disease, tuberculosis, and diarrheal disease) have been incriminated for neglecting studies on fungal diseases. Furthermore, treating fungal infections of the nail as a cosmetic concern rather than one of the actual medical implications by health workers and the general population is another reason for the less attention given to fungal infections including onychomycosis. To this effect, a precise assessment of the magnitude of onychomycosis and the diversity of its etiological agents is indispensable since it gives an estimate of the burden of the disease. This, in turn, enables us to estimate the potential demand for medical treatment and the economic impact of the infection. In line with we conducted the current study. In the present study, a total of 200 nail scrapings collected from clinically confirmed patients with onychomycosis were evaluated microbiologically of which fungal pathogens were isolated in 80.5% of study subjects. The overall prevalence rate of onychomycosis in this study was higher than in a similar study conducted in Ethiopia,12 but comparable to the prevalence rates reported by studies conducted in India17 and Brazil.18 Given that Ethiopia is a developing country situated in the sub-Sahara region of the globe having a wet humid climate that is suitable for fungal growth, the emergence of widespread and frequent use of communal bathing facilities, and low awareness of the onychomycosis may be a possible explanation for the high prevalence rate of the disease in the current study.
In our study, females were more vulnerable to fungal nail infections than male study subjects. Isolation of a large number of fungi in females 66.8% than males 33.2% was in line with differences in the number of female and male subjects enrolled in the study. In literature, the prevalence rates of onychomycosis regarding sex are highly variable. Brilhante et al19 demonstrated that females are more affected than males, while Ahuja et al20 and Satpathi et al21 reported that males are more prone to onychomycosis than females. Routine household activities involving water by females are the major predisposing risk factors for a higher prevalence of onychomycosis in females.19 In urban Ethiopia, household activities such as laundry without a washing machine, cooking, and house cleaning are mainly practiced by females. This may explain a high prevalence of onychomycosis in females than males in our study.
There are still inconsistent reports about the magnitude of onychomycosis about age. In our study, the frequency of onychomycosis in patients in the age group of 1–14 years was comparably higher than those reported by Bitew and Sinkenesh12 and Ahmed and Gupta.22 There are still inconsistent reports about the prevalence of onychomycosis in adults and elders. A study conducted by Jain and Sehgal,23 revealed a higher prevalence rate of onychomycosis in the age group of 20–40 years of age whereas, a similar study carried out by Grover24 demonstrated that the prevalence rate of onychomycosis is the highest in study subjects above 55 years of age. In our study, patients with ages between 15–44 were more affected than the other age groups. The prevalence of rate of onychomycosis in the age group of ≥ 65 years in our study was about 3.7%. Our result was in line with that of Veer et al6 who reported a higher prevalence rate in patients with middle age (30–40 years), infrequent in the elderly, and the least in children.
In our study, out of 161 culture-positive samples, 83.9% of samples yielded single colonies while 16.1% mixed colonies gave a total of 190 isolates. No visible fungal growth was demonstrated in 19.5% samples even though samples were collected from lesions compatible with onychomycosis clinically warranting that clinical diagnosis of onychomycosis is not dependable and hence at least supported by microbiological techniques. The isolation rate of different groups of fungi implicated in causing nail infection varies from study to study. In this study, non-dermatophytes mycelial fungi outnumbered those of dermatophytes and yeasts. Our finding was in contrast to previous studies12,25,26 that demonstrated dermatophytes were the most encountered fungi in onychomycosis followed by yeasts and then by non-dermatophyte molds, respectively. In line with our finding, however, non-dermatophyte mold dominated onychomycosis with a prevalence rate of 69.3% was reported in Malaysia by Ramalingam et al.27 Still, an equal incidence of onychomycosis caused by dermatophytes and yeasts has been reported by Gupta et al.28
The diversity and species composition of fungi isolated in our study were so enormous. About 40 isolates belonging to eight species of Microsporum and Trichophyton were isolated of which 42 (85.7%) were species of the genus Trichophyton while the remaining 7 (14.3%) were members of the genus Microsporum. T. rubrum and T. interdigitale were the most frequently isolated dermatophytes accounting for 50% of dermatophytes in our study. T. rubrum and T. interdigitale as a major cause of onychomycosis have been documented by different authors.25,29 Brilhante et al19 documented those yeasts, particularly C. albicans, emerged as an important cause of onychomycosis and our result was consistent with this finding. Of 25 yeast isolates, 64.0% were accounted by C. albicans. Repeated contact with water has been incriminated for an increase of yeasts in onychomycosis.25
Interestingly, in the current study, the occurrence of onychomycosis caused by non-dermatophyte molds outnumbered the occurrence of nail infections caused by both dermatophytes and yeasts. Initially, non-dermatophyte molds have been considered as laboratory contaminants but are now considered to be emerging pathogens of onychomycosis by many authors including Gupta et al30 and Nenoff et al.31 The species of Aspergillus, Fusarium, Penicillium, Scytalidium dimidiatum, Scopulariopsis spp, Alternaria, and Curvularia were the dominant isolates among non-dermatophyte mycelial fungi. The diversity and species composition of major non-dermatophyte mold isolates were in concordance with previously reported studies conducted in Mexico, North America, and Europe.32–34
An increase in the prevalence of non-dermatophyte molds in skin-related infections has been highlighted in other many published studies.10,11,27,32,33,35–38 However, the extent to which non-dermatophyte fungi cause dermatophytosis/onychomycosis is still a subject of debate. Therefore, further investigations demonstrating how this group of fungi causes infection are needed.
The increased prevalence of immune-compromised population resulted from an increase in life expectancy accompanied with chronic disease, an increase in underlying diseases that suppress host immunity and sustaining patients by drugs, chemicals, and mechanical processes that compromise physical barriers to infection, suppress immune mechanisms, or upset the balance of normal flora have been causing hosts to be more susceptible not only to pathogenic fungi but also to all fungi that were once considered opportunistic fungi.34,39 Human demographic changes that have been taking place across the globe could be one of the best possible reasons for non-dermatophyte mold-dominated onychomycosis seen in our study. Therefore, our study suggests that information about the immune status of study subjects in similar studies in the future appears to be mandatory since fungal diseases caused by opportunistic fungi have been increasing.
Limitations of the Study
This study has many limitations. The increased prevalence of onychomycosis now than in the past is largely related to increased numbers of immune-compromised human hosts. Lack of information about the immune status of study participants was the major limitation of the study as most non-dermatophyte molds and yeasts are opportunistic pathogens. Due to lack of facilities and resources, unable to determine the antifungal susceptibility profile of the fungal isolates in the present study was another limitation of our study. The small sample size was another limitation.
Conclusions
The prevalence rate of onychomycosis in the present study was high. The isolation rate of non-dermatophyte molds was higher than dermatophytes and yeasts. Trichophyton interdigitale, Aspergillus spp, and Candida albicans were the dominant etiological agents. Females and patients in the middle age group were more affected. An increase in the prevalence of non-dermatophyte molds in skin-related infections dictates further investigations demonstrating how this group of fungi causes onychomycosis.
Abbreviations
HIV, human immunodeficiency virus; SOP, standard operating procedure; V/V, volume by volume; SDA, sabouraud dextrose agar; KOH, potassium hydroxide; LPCB, lactophenol cotton blue; 10X, ten times objective lens; 40, forty times objective lens; Cont’d, continued.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author and can be obtained upon reasonable request.
Acknowledgments
We would like to acknowledge the attending dermatologists at Rand specialized dermatology clinic for critical review of patients from the viewpoint of clinical presentation. We are also very grateful to the patients who participated in the study. We would like to extend our thanks for Feruza Osman for allowing us to extract important information from her unpublished thesis work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no financial and non-financial competing interests for the manuscript.
References
1. Faergemann J, Baran R. Epidemiology, clinical presentation and diagnosis of onychomycosis. Br J Dermatol. 2003;65:1–4. doi:10.1046/j.1365-2133.149.s65.4.x
2. Gupta AK, Jain HC, Lynde CW, MacDonald P, Cooper EA, Summerbell RC. Prevalence and epidemiology of onychomycosis in patients visiting physicians’ offices: a multicenter Canadian survey of 15,000 patients. J Am Acad Dermatol. 2000;43:244–248. doi:10.1067/mjd.2000.104794
3. Martínez-Herrera E, Schlager-Ospino H, Torres-Guerrero Eet al. Frequency of mixed onychomycosis with total nail dystrophy in patients attended in a Guatemalan dermatology center. Infection. 2018;22:105–109. doi:10.22354/in.v22i2.716
4. Thomas J, Jacobson GA, Narkowich CK, Peterson GM, Burnet H. Toenail onychomycosis: an important global disease burden. J Clin Pharm. 2010;35:497–519.
5. Gupta AK, Stec N. Recent advances in therapies for onychomycosis and its management [version 1; peer review: 2 approved]. F1000Research. 2019;8(F1000 Faculty Rev):968. doi:10.12688/f1000research.18646.1
6. Veer P, Patwardhan NS, Damle S. Study of onychomycosis: prevailing fungi and pattern of infection. Indian J Med Microbiol. 2007;25:53–56. doi:10.1016/S0255-0857(21)02235-0
7. Levy L. Epidemiology of onychomycosis in special-risk populations. J Am Podiatr Med Assoc. 1997;87:546–550. doi:10.7547/87507315-87-12-546
8. Lateur N. Onychomycosis: beyond cosmetic distress. J Cosmet Dermatol. 2006;5:171–177. doi:10.1111/j.1473-2165.2006.00246.x
9. Gupta A, Versteeg S, Shear N. Onychomycosis in the 21st century: an update on diagnosis, epidemiology, and treatment. J Cutan Med Surg. 2017;21:525–539. doi:10.1177/1203475417716362
10. Hwang SM, Suh MK, Ha GY. Onychomycosis due to non dermatophyte molds. Annals Dermatolo. 2012;24:175–180. doi:10.5021/ad.2012.24.2.175
11. Moreno G, Arenas R. Other fungi causing onychomycosis. Clin Dermatol. 2010;28:160–163. doi:10.1016/j.clindermatol.2009.12.009
12. Bitew A, Wolde S. Prevalence, risk factors, and spectrum of fungi in patients with onychomycosis in Addis Ababa, Ethiopia: a prospective study. J Trop med. 2019;6:1–7. doi:10.1155/2019/3652634
13. Larone DH. Medically Important Fungi: A Guide to Identification.
14. Frey D, Oldfield RJ, Bridger RC. Color atlas of pathogenic fungi. In: A Color Atlas Pathogenic Fungi.
15. Kern M. Medical Mycology, a Self-Instructional Text.
16. World Health Organization. Provisional guidelines on standard international age classifications, Vol. 74, Statistical Papers, Series M. New York, NY, USA; 1982.
17. Adekhandi S, Pal S, Sharma N, Juyal D, Sharma M, Dimri D. Incidence and epidemiology of onychomycosis in patients visiting a tertiary care hospital in India. Cutis. 2015;95:E20–E25.
18. De Carvalho Ribeiro CS, Zaitz C, de Souza Framil VM, de Carvalho Ottoboni TS, de Carvalho Tonoli MS, Ribeiro RP. Descriptive study of onychomycosis in a hospital in Sao Paulo. Braz J Microbiol. 2015;46:485–492. doi:10.1590/S1517-838246220130541
19. Brilhante RSN, Cordeiro RA, Medrano DJA, et al. Onychomycosis in Cear´a (Northeast Brazil): epidemiological and laboratory aspects. Mem Inst Oswaldo Cruz. 2005;100:131–135. doi:10.1590/S0074-02762005000200005
20. Ahuja S, Malhotra S, Charoo H. Etiological agents of onychomycosis from a tertiary care hospital in central Delhi, India. Indian J Fundam Appl Life Scie. 2011;1:4.
21. Satpathi P, Achar A, Banerjee D, Maiti A, Sengupta M, Mohata A. Onychomycosis in Eastern India - a study in a peripheral tertiary care center. J Pak Assoc Dermatol. 2013;23:14–19.
22. Ahmed M, Gupta S. A clinico-mycological study of onychomycosis. Egypt Dermatol Online J. 2000;6:4.
23. Jain S, Sehgal VN. Onychomycosis: an epidemioetiologic perspective. Intern J Dermatol. 2000;39:100–103. doi:10.1046/j.1365-4362.2000.00808.x
24. Grover S. Clinico-mycological evaluation of onychomycosis at Bangalore and Jorhat. Indian J Dermatol Venereol Leprol. 2003;69:284–286.
25. Gelotar P, Vachhani S, Patel B, Makwana N. The prevalence of fungi in fingernail onychomycosis. J Clin Diagn Res. 2013;5:1–3.
26. Mϋgge C, Haustein UF, Nenoff P. Causative agents of onychomycosis – a retrospective study. J Ger Soc Dermatol. 2006;4:218–228.
27. Ramalingam R, Kunalan S, Tang MM. The mycology of onychomycosis: a 5- year retrospective review (2011–2015) in hospital Kuala Lumpur. Med J Malays. 2017;72:190–192.
28. Gupta M, Sharma N, Kanga A, Mahajan V, Tegta G. Onychomycosis: clinico-mycologic study of 130 patients from Himachal Pradesh, India. Indian J Dermatol Venereol Leprol. 2007;73:389–392. doi:10.4103/0378-6323.37055
29. Alvarez MI, Gonz´alez LA, Castro LA. Onychomycosis in Cali, Colombia. Mycopathologia. 2004;158:181–186. doi:10.1023/BYCO.0000041866.85314.e4
30. Gupta AK, Drummond-Main C, Cooper EA, Brintnell W, Piraccini BM, Tosti A. Systematic review of non-dermatophyte mold onychomycosis: diagnosis, clinical types, epidemiology, and treatment. J Am Acad Dermatol. 2012;66:494–502. doi:10.1016/j.jaad.2011.02.038
31. Nenoff P, Kruger C, Ginter-Hanselmeyer G, Tietz HJ. Mycology – an update. Part 1: dermatomycoses: causative agents, epidemiology, and pathogenesis. J German Soc Dermatol. 2014;12:188–210.
32. Tisti A, Piraccini BM, Lorenzi S. Onychomycosis caused by non-dermatophytes: clinical features and response to treatment of 59 cases. J Am Acad Dermatol. 2000;42:217–424. doi:10.1016/S0190-9622(00)90129-4
33. Bonifaz A, Angular CP, Ponce RM. Onychomycosis by molds: report of 78 cases. Europ J Dermatol. 2007;17:70–72.
34. Singh N. Trends in the epidemiology of opportunistic fungal infections: predisposing factors and the impact of antimicrobial use practices. Clin Infect Dis. 2001;33:169. doi:10.1086/323895
35. Gregoriou S, Mpali N, Vrionia G, Hatzidimitriou E, Chryssou S-E, Rigopoulos D. Epidemiology of onychomycosis in an academic nail unit in South Greece during three years. Skin Appendage Disord. 2020;6:102–107103. doi:10.1159/000504812
36. GuptaID AK, Taborda VBA, Taborda PRO, Shemer A, Summerbell RC, Nakrieko KA. High prevalence of mixed infections in global onychomycosis. PLoS One. 2020. doi:10.1371/journal.pone.0239648
37. Sakkas H, Kittas C, Kapnisi G, et al. Onychomycosis in Northwestern Greece over 7 years. Pathogens. 2020;9:851–859. doi:10.3390/pathogens9100851
38. Feruza O. Characterization of Dermatophytes and Non-Dermatophytes Isolated from Patients with Onychomycosis at Rank Dermatology Clinic [Unpublished Master’s thesis]. Addis Ababa University; 2019:1–63.
39. Richardson M, Lass-Florl C. Changing epidemiology of systemic fungal infections. Clin Microbiol Infect. 2008;14(Suppl. 4):5–24. doi:10.1111/j.1469-0691.2008.01978.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.