Back to Journals » Journal of Inflammation Research » Volume 19
Non-Conventional and Emerging Autoantibodies in Sjögren’s Disease
Authors Lee AYS ![]()
Received 1 January 2026
Accepted for publication 17 February 2026
Published 3 March 2026 Volume 2026:19 593107
DOI https://doi.org/10.2147/JIR.S593107
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chaim Putterman
Adrian YS Lee1,2
1Department of Clinical Immunology & Allergy, Westmead Hospital & ICPMR, Sydney, NSW, Australia; 2Centre for Immunology & Allergy Research, Westmead Institute for Medical Research, The University of Sydney, Sydney, NSW, Australia
Correspondence: Adrian YS Lee, Department of Clinical Immunology, ICPMR & Westmead Hospital, Hawkesbury Road, Westmead, Sydney, NSW, 2145, Australia, Tel +61 2 8890 5555, Email [email protected]
Abstract: Sjögren’s disease (SjD) is a chronic autoimmune disease that is characterised by dryness symptoms, arthralgias, systemic disease and B-cell hyperactivity. Serum autoantibodies are key pathological features of this disease. Anti-Ro52, anti-Ro60 and anti-La immunoglobulin G autoantibodies (sometimes known as antinuclear antibodies) are perhaps the most well-known autoantibodies, are important in the formal classification criteria for SjD and exist in up to 70% of patients. Rheumatoid factors, which are present in approximately 50% of patients, can reveal important prognostic information regarding the development of B-cell lymphomas. Beyond these autoantibodies, there are several emerging and novel autoantibodies associated with SjD that hold promise in identifying clinical features of SjD and facilitating the diagnosis of patients who lack the classic SjD-associated autoantibodies. These include anti-fodrin antibodies, anti-muscarinic acetylcholine receptor 3 antibodies and those autoantibodies traditionally associated with systemic lupus erythematosus. This narrative review article provides an updated review of these autoantibodies, discussing their potential clinical utility and the current limitations. Although many clinical associations have been identified, the routine clinical use of these autoantibodies is hampered by issues such as poor diagnostic sensitivity, contradictory associations, heterogeneous studies and small single-cohort studies. Further research using harmonised testing and large, multicentre cohorts is required to explore and validate the utility of these autoantibodies.
Keywords: antibodies, autoantibodies, B cells, Sjögren’s disease
Introduction
Sjögren’s disease (SjD) is a systemic autoimmune disease that predominantly affects females, resulting in dryness (sicca) symptoms, arthralgias and fatigue, and involving various organs. It imparts a significant burden to patients’ quality of life, particularly as there are currently no approved targeted therapies in existence. As a clinically heterogeneous disorder, the condition may be unified by the presence of B-cell hyperactivity and autoantibodies in a substantial proportion of patients.1,2 As such, there are several ongoing trials on SjD targeting B cells and plasma cells.3 SjD may exist in isolated or primary form, or be associated with other autoimmune diseases, including systemic lupus erythematosus (SLE).
Autoantibodies in SjD originate from self-reactive B cells and may target a number of nuclear, cellular and extracellular antigens, reflecting the B-cell hyperactivity of the disease.4 While autoantibodies also have a natural or physiological role in health, these autoantibodies in SjD may be directly pathogenic and induce apoptosis of salivary gland cells, leading to salivary gland dysfunction.5 Early studies have identified serum antibodies in SjD patients reacting with salivary gland antigens by indirect immunofluorescence microscopy. These may be of any isotype and are believed to bind keratin as one of their antigenic targets.6,7 Immunoglobulin G (IgG) autoantibodies towards ribonucleoprotein proteins, Ro52/tripartite motif-containing protein 21 (TRIM21), Ro60 and La, are particularly common in SjD patients and encompass the spectrum of antinuclear antibodies (ANA) commonly measured by fluorescence microscopy on HEp2 substrate. However, ANA screening may miss detection of these specific SjD-associated autoantibodies (ie, be negative), even with the sensitive HEp-2000 for detection of anti-Ro60 autoantibodies.8 In cohort studies, these autoantibodies are present in around 70–80% for Ro52/Ro60 IgG and 40% for La IgG;9,10 however, they are not specific for SjD and may be found in other systemic autoimmune diseases. Clinically, anti-Ro52/Ro60 IgG autoantibodies (also termed SS-A antibodies) are important in the identification of SjD, and are an important disease feature in the American College of Rheumatology (ACR)/European Alliance of Associations of Rheumatology (EULAR) 2016 classification criteria.11 Anti-La IgG are not included in these criteria since these antibodies have low clinical utility in the identification of SjD patients,12 although they were included in the earlier 2012 Sjögren’s International Collaborative Clinical Alliance (SICCA) criteria.13 Nevertheless, these autoantibodies may help to stratify patients into serological subsets, recognising patients at risk of serious systemic manifestations.10,14
Another common autoantibody, rheumatoid factor (RhF), is an autoantibody of any isotype directed against the Fc portion of circulating IgG. RhF is found in approximately half of SjD patients,9 and featured in earlier SjD classification criteria in combination with a positive ANA test by immunofluorescence microscopy.13 Like the classic Ro52/Ro60 and La IgG autoantibodies, RhF remains an important prognostic marker of disease and is associated with more severe disease15 and the future development of mucosa-associated lymphoid tissue (MALT) lymphomas.16 Occasionally, the RhF-producing B cells may acquire somatic and B-cell receptor mutations that may cause them to acquire cryoprecipitating properties and form cryoglobulins. These occur in approximately 9% of SjD patients, and may cause serious end-organ damage when they precipitate and deposit in tissue.17 These observations highlight the importance of accurate serological profiling of patients through autoantibodies.
There are several areas of unmet need for SjD and autoantibodies. Owing to the clinical heterogeneity and sometimes subtle clinical presentation, SjD continues to be poorly diagnosed and recognised, particularly when patients lack the classic SjD-related autoantibodies discussed above.18 This calls for the investigation for alternative autoantibody biomarkers that can help in diagnosing these cases. Furthermore, stratification of patients into those at risk of specific systemic manifestations would be highly desirable, particularly as patients remark about the unpredictability of their disease.2 Therefore, biomarkers such as autoantibodies may be useful. Anti-Ro52, -Ro60, -La and RhF are commonly measured autoantibodies in SjD and either are currently or were previously part of the classification criteria.19 This narrative review examines less common and novel autoantibodies that have been or are being explored in the literature. Many of these have putative clinical associations; however, further studies to validate these findings in other cohorts are required.
Review Study Selection
A narrative review was undertaken to examine “non-conventional” and “emerging” autoantibodies in SjD. These were defined as any serum autoantibody that is novel and/or less well established in the diagnosis, monitoring, prediction or prognostication of SjD patients. Hence, these were autoantibodies other than anti-Ro52, -Ro60, -La IgG or RhF. The author focused on all isotypes and any assay for measurement. PubMed (MEDLINE) and Google Scholar databases were searched with the following combination of phrases: “Sjögren’s”, “Sjögren’s disease”, “Sjögren’s syndrome”, “autoantibody”, “biomarker”, “novel” and “new”. Only publications published in English were considered and no restrictions on publication date were made. Results from the included publications were analysed and summarised for each autoantibody. Key diagnostic information, including prevalence, sensitivity and specificity, was extracted (where present) and pooled.
α-Fodrin Antibodies
α-Fodrin is a cytoskeletal protein, encoded by SPTAN1, that provides cellular membrane support and has a role to play in the normal function of apoptosis.20 Small interfering RNA (siRNA) silencing of α-fodrin in non-obese diabetic mice (a murine model for SjD) improved lymphocytic infiltration in lacrimal glands relative to controls, confirming that it is an important autoantigen in the pathogenesis of SjD.21
Research on antibodies targeting this protein (α-fodrin antibodies [AFA]) has historically been interested in the detection of SjD patients lacking the classic Ro/La autoantibodies.22 Therefore, the addition of AFA to the diagnostic algorithm may help to improve diagnostic sensitivity.23 The IgG and IgA isotypes have predominantly been explored by enzyme-linked immunosorbent assay (ELISA), showing a prevalence of up to 55% for AFA IgG and 82% for AFA IgA in SjD; and 71% for AFA IgG and 59% for AFA IgA in SjD with other associated autoimmune diseases.24,25 They may be associated with various features of disease activity, including hypergammaglobulinaemia and neurological disease (Table 1).
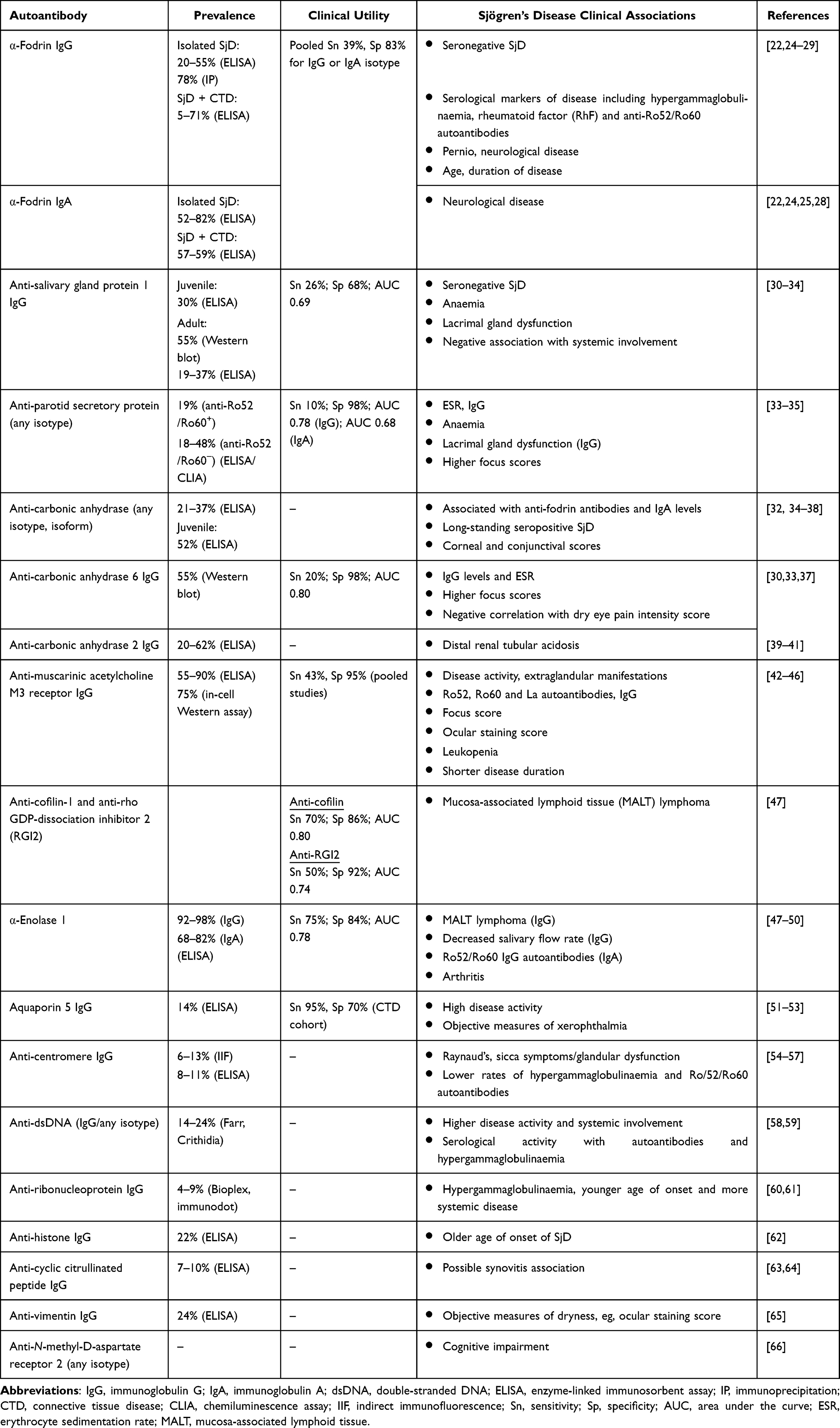 |
Table 1 Overview of Novel and Non-Conventional Serum Autoantibodies in Sjögren’s Disease (SjD) |
A meta-analysis of studies revealed a pooled sensitivity of IgG/IgA AFA of 39% and specificity of 83% for the diagnosis of SjD.26 However, the high prevalence of these autoantibodies in other autoimmune diseases and even healthy donors made some researchers question the diagnostic utility of AFA. Therefore, AFA did not adequately discriminate between SjD patients and these controls on receiver operating characteristics (ROC) curve analysis.25,27
Salivary Gland Protein 1 and Parotid Secretory Protein Antibodies
These autoantibodies have often been studied together (as “tissue-specific” antibodies) in SjD and, therefore, will be considered together in this section. Similarly to AFA, interest in these autoantibodies lies in identifying patients who lack Ro/La autoantibodies, stemming from a murine model of SjD (interleukin 14α transgenic mice [IL14αTG]) that demonstrates autoantibodies to salivary gland protein 1 (SP1) and parotid secretory protein (PSP), with minimal antibodies to Ro/La autoantigens.30 In patients with long-standing seropositive (anti-Ro60+) SjD, these autoantibodies of the IgG and IgM isotype are rare, being found in approximately 10% of patients.36 In addition, anti-PSP and anti-SP1 IgA were found in 10–50% of SjD associated with autoimmune diseases; in contrast, the IgG and IgM isotypes were rarer, and anti-Ro IgG was found less commonly, suggesting that the IgA isotype may be helpful in identifying patients with connective tissue disease (CTD) with associated SjD and who lack Ro52/Ro60 antibodies.36
Autoantibodies (IgG, IgA and IgM) towards these autoantigens may be found in patients with objective evidence of dry eye disease in the absence of Ro52/Ro60/La autoantibodies and SjD. However, it is possible that in these cross-sectional studies, some of these patients would eventually develop SjD or other diseases.30,67 In one study, 19% of SjD sera contained anti-SP1 antibodies (by immunoblot), and these patients also lacked autoantibodies to Ro52/Ro60/La autoantigens.31 Anti-SP1 IgG and IgM – but not anti-PSP isotypes – correlate with tear break-up time.37
In juvenile SjD, the detection of these autoantibodies (of any isotype) generally has low sensitivity for the diagnosis; however, combining them with traditional SjD-related autoantibodies, such as ANA, increases sensitivity at the expense of diagnostic specificity.32 Clinically, these autoantibodies have not demonstrated clinical utility in this group of patients, with no correlations having been found with salivary gland focus score, anti-Ro52/Ro60 autoantibodies or unstimulated salivary flow rate.32
Carbonic Anhydrase Antibodies
Carbonic anhydrase (CA) is an important enzyme in acid–base regulation, found in the exocrine glands, skin and kidney.38 It catalyses the conversion of carbon dioxide to bicarbonate ions and carbonic acid, and is therefore important in normal physiological roles. CA isoforms may be found in cells or secreted in bodily fluids, including saliva.68 CA-1 protein is up-regulated in the salivary gland tissue of SjD patients compared to healthy controls.47 Antibodies to CA and specific isoforms have been studied in SjD. CA isoform antibodies also correlate with disease activity,69 implicating these autoantibodies in the pathology of the disease.
CA-6 is secreted in saliva and plays a role in the production of saliva from acinar and ductal cells.68 As such, it has received special attention as an autoantigen in SjD, particularly as these autoantibodies are found in mouse models of SjD that lack the traditional Ro52/Ro60/La autoantibodies.30 Higher levels of serum anti-CA6 IgG and IgM have been noted in SjD patients compared with healthy donors and disease controls,33 and the IgA isotype is relatively prevalent (38%) in patients with long-standing SjD.36 Anti-CA-6 IgG is present in up to half of SjD patients, and is correlated with serum IgG levels and higher minor salivary gland biopsy focus scores.33
Furthermore, given the enzyme’s role in the modulation of acid–base balance, others have studied the autoantibody’s putative links with acid–base disorders in SjD. Anti-CA-6 IgG is associated with lower serum sodium and potassium, higher urinary pH and higher urinary bicarbonate, suggesting associations with a urinary acidification defect.70,71 Anti-CA-2 IgG was detected in 20–61% of SjD patients, and higher levels were found in SjD patients with distal renal tubular acidosis (RTA).39,40 Experimental data seem to support the role of CA autoantibodies in the pathogenesis of RTA. PL/J mice immunised with human CA-2 induced autoantibodies to this antigen and salivary gland focal lymphocytic sialadenitis.72 These mice had defects in urinary acidification, suggesting that the autoantibodies are likely to be pathogenic in the pathogenesis of RTA.73
Muscarinic Acetylcholine M3 Receptor Antibodies
Muscarinic acetylcholine M3 receptor (M3R) is a G protein-coupled receptor found in major salivary glands and is involved in mediating salivation. Mice deficient in this receptor have deficiencies in salivation.74 Anti-M3R may be directed against several components of the M3R, but most commonly targets the second extracellular domain.75 In in vitro experiments, sera derived from SjD patients positive for anti-M3R differentially modulated intracellular calcium influx from cevimeline-treated salivary gland cell lines. Antibodies to the second extracellular loop of this receptor loop inhibited this calcium influx, whereas those directed to the N-terminus and first extracellular loop potentiated the calcium influx.42 In addition, SjD anti-M3R IgG was found to cause the internalisation of M3R and major histocompatibility class-I on human submandibular gland cell lines, which may present a novel mechanism for the targeting of these cells for destruction by natural killer (NK) cells.76 In contrast, in BALB/c mice immunised with peptides of the second extracellular loop, the induction of anti-M3R IgG led to antibody deposition in salivary glands. However, this did not result in the reduction of salivary or tear flow up to 20 weeks post-induction. Furthermore, the transfer of IgG from immunised mice into recipient mice did not elicit evidence for exocrine gland dysfunction. These data indicate that anti-M3R modulate receptor activity but are unlikely to be pathogenic.77
Similarly, the clinical utility of anti-M3R has been somewhat disappointing. Anti-M3R IgG (to specific extracellular loops) is present in approximately 50% of SjD patients,42 and is elevated compared to disease controls (rheumatoid arthritis [RA] and SLE) and non-SjD sicca patients.43 However, on ROC curve analysis, the autoantibodies could not adequately distinguish between SjD and SLE patients,43,78 and showed poor sensitivity in diagnosing SjD from healthy controls.44 In contrast to the data in the previous paragraph, there is no demonstration of any correlation between these autoantibodies and objective salivary flow rate.42,45 The autoantibodies, however, identified younger SjD patients and patients with greater disease manifestations, including IgG levels and focus scores.43,78
Cofilin-1, α-Enolase and Rho GDP-Dissociation Inhibitor 2 Antibodies
Using mass spectrometry, cofilin-1, α-enolase, annexin A2 and rho GDP-dissociation inhibitor 2 (RGI2) were found to be overexpressed in the parotid salivary gland tissue of SjD patients compared to non-SjD controls.47,48 Therefore, researchers tested the clinical utility of autoantibodies to these autoantigens. IgG to cofilin-1, α-enolase and RGI2 was able to discriminate between SjD patients with MALT lymphomas and those without, with an area under the curve (AUC) of at least 0.74.47
Given that α-enolase is overexpressed in the salivary gland tissue of SjD patients, their role in SjD salivary gland pathology has been studied. Mass spectrometry of a submandibular gland cell line (SMG-C6) that overexpresses α-enolase revealed an up-regulation of proteins related to immunodulation, metabolism and salivary secretion.48 As such, anti-α-enolase IgG levels were also associated with decreased salivary flow rate in SjD patients.48 However, anti-α-enolase IgG and IgA antibodies have limited association with other clinical manifestations, apart from, possibly, arthritis and high urine pH.49,50
Aquaporin Antibodies
Aquaporins (AQP) are cellular membrane water channels found in various organs, including the kidneys and exocrine glands.79 Autoantibodies to these channels have received interest from researchers in various autoimmune diseases. Serum and cerebrospinal fluid AQP4 IgG are characteristic of neuromyelitis optica, and may coexist in up to 20% of SjD patients.80 AQP proteins may be expressed on human salivary glands,51 and AQP5 expression is down-regulated in SjD salivary glands.81,82
Using ELISA, serum anti-AQP1 and AQP5 IgG were higher in SjD patients than in healthy controls, but only anti-AQP5 levels were higher than in other patients with CTD.52 At a cut-off of 18.79 ng/mL, anti-AQP5 antibodies had an AUC of 0.86, with a sensitivity of 95% and specificity of 70%, compared to the CTD cohort.52 The clinical value of anti-AQP5 is mixed. One study did not find any correlation with disease activity or serological parameters;52 however, when using a EULAR Sjögren’s Syndrome Disease Activity Index (ESSDAI) cut-off of 14, anti-AQP5 was independently associated with high ESSDAI SjD patients.53 In another study, the presence of IgG towards AQP proteins was associated with more severe xerophthalmia using the van Bijsterveld scoring assessment.51 Differences in these associations between studies probably reflect differences in assays and collected clinical parameters.
Centromere Antibodies
While centromere IgG antibodies (ACA) are regarded as a sensitive marker for scleroderma, and they may signify SjD associating with this disease,83 ACA may also exist in SjD patients with no scleroderma features. Using immunoprecipitation methods, the majority of ACA in SjD targets centromere protein C (CENP-C) alone, and rarely targets both CENP-C and centromere protein B (CENP-B).84
ACA has a prevalence of approximately 6–13% in SjD,54–57 and 3% of SjD patients negative for Ro52/Ro60/La autoantibodies have ACA,85 indicating that this may be a helpful biomarker in a small fraction of cases. ACA+ SjD patients tend to be older, to have Raynaud’s phenomenon, sclerodactyly and left ventricular diastolic dysfunction, and to be seronegative for Ro52, Ro60 and La autoantibodies.54,56,86 ACA+ patients also tend to have higher disease activity (ESSDAI) than ACA− patients.54
An area of interest in ACA+ patients lies in the salivary gland pathology. Studies are conflicting over whether ACA+ patients have higher salivary gland focus scores than ACA− patients, with some studies finding lower focus scores,57 others finding no difference,54,87 and another finding slightly higher focus scores55 in ACA+ patients. Nevertheless, the salivary glands of ACA+ patients tend to have a higher degree of fibrosis histologically.57 Indeed, using single-cell interrogation from minor salivary gland biopsies from ACA+ and ACA− patients, ACA+ patient biopsies demonstrated an enrichment of memory B cells and age-associated B cells, and gene signatures of fibrosis and transforming growth factor (TGF)-β signalling.88
Systemic Lupus Erythematosus-Associated Autoantibodies
Anti-double-stranded DNA (dsDNA) may be found in SjD, particularly when associated with SLE.89 Occasionally, patients with primary SjD and no features of SLE may develop new anti-dsDNA and clinical features of SLE,90 highlighting the importance of monitoring SjD patients and retesting autoantibodies, particularly when new clinical features emerge. In primary SjD, these autoantibodies may exist in around 14–24% of individuals with no features of SLE, and identify patients who have hypergammaglobulinaemia, greater systemic involvement and disease activity.58,59
Anti-ribonucleoprotein (RNP) may be found in both SLE and mixed connective tissue disease (MCTD).83 However, similarly to anti-dsDNA, its presence in SjD without SLE/MCTD signifies SjD patients with an earlier onset of disease, higher systemic burden and higher levels of IgG. Complications include interstitial lung disease, myositis and Raynaud’s phenomenon.60,61
Histone antibodies are commonly detected in SLE, and may be found in drug-induced lupus erythematosus and other autoimmune rheumatic disorders. Directed against histones – structures that chromatin can be wrapped around – antibodies towards these structures commonly make their appearance in SLE and drug-induced lupus erythematosus.91 In SjD, serum histone IgG was present in 22% of patients and a subset of patients with late-onset disease was identified. No other clinical features were associated with this autoantibody and there was no evidence of SLE overlap syndrome in any of these patients.62
Other Autoantibodies
The presence of other autoantibodies in SjD may signify another associated autoimmune disorder. For example, anti-mitochondrial-M2 IgG may be found in SjD patients with concomitant primary biliary cirrhosis.92 However, a range of single-cohort or smaller studies have explored other autoantibodies in SjD patients in the absence of their associated autoimmune disorder. Anti-cyclic citrullinated peptide IgG autoantibodies have been regarded as a specific marker for RA; yet, in the absence of RA, they can be present in up to 10% of SjD patients. Although they are not associated with any SjD clinical features or RhF, one study found an association with synovitis,63 whereas a later study did not.64 These studies examined patients with isolated SjD and excluded those with associated RA from their analyses.
Vimentin is a filament protein that forms the structural cytoskeleton of a cell. Anti-vimentin IgG can be found in various autoimmune diseases. One cohort study found these autoantibodies in 24% of SjD patients, and the levels positively correlated with dryness measures, including ocular surface staining score and unstimulated whole salivary flow rate.65 In SjD associated with other autoimmune diseases, including RA, this prevalence may be increased to approximately 66%.93
Finally, in a single cohort of SjD patients, anti-N-methyl-D-aspartate (NMDA) receptor subtype 2 IgG/A/M in the serum and cerebrospinal fluid was associated with poor memory and learning scores.66 These are of particular interest since anti-NMDA antibodies may be seen in patients with NMDA receptor autoimmune encephalitis. Further work in other cohorts is required to replicate these findings.
Discussion and Concluding Remarks
Since autoantibodies have become important diagnostic and prognostic biomarkers in autoimmune diseases, attention has turned to more accurately phenotyping SjD patients, particularly when they lack the classic SjD-associated autoantibodies such as anti-Ro60. However, the generally low prevalence of these novel serum autoantibodies in the seronegative SjD population, and their limited ability to discriminate these patients from controls, limits their clinical utility.31 Moreover, and particularly with respect to earlier studies, it is unclear whether anti-Ro52 was tested, which may affect the classification of “seronegative” patients, since “SS-A” and “anti-Ro” are now somewhat ambiguous terms.94
A tremendous number of studies have been dedicated to lesser known and non-conventional serum autoantibodies in SjD in an attempt to improve diagnoses and define clinical subsets (Table 1). However, as of now, these studies have largely been restricted to either small numbers of SjD patients or homogeneous single cohorts. Moreover, some early studies used differing classification criteria to define SjD patients and most studies did not report what treatments, if any, these patients were receiving. This introduces a significant selection bias. The controls for these studies have also been variable. For example, some used SLE as their disease controls,28 whereas others used hospital staff as their healthy donors.78 These controls and their ages would vastly affect the immunoassay cut-off that defines positivity and, hence, the diagnostic performance of the autoantibody under investigation.
Furthermore, a major challenge in autoantibody diagnostics is standardisation of testing, as heterogeneity exists in the preanalytical handling of samples, testing methodology and the definitions of a positive result, among other things. For instance, immunoprecipitation assays, as used in a few studies,25 offer reduced analytical sensitivity but better specificity than immunoblot assays.95 For analytical validity, a few studies utilised more than one assay to measure and report their autoantibody results (eg, Refs25,31), but the majority of studies used one assay (ELISA), and for in-house assays, no details were provided about the validation of the assay, including its accuracy and precision. All these sources of variation may account for the vast differences in prevalence of these autoantibodies reported across the studies, and may explain differences in clinical associations and apparently conflicting utility (Table 1). Therefore, future research in well-defined SjD and control cohorts, using validated assays, is required to improve the validity and generalisability of these findings. Ideally, studies should also test autoantibodies using more than one assay and should describe assay validation procedures.
Study design is an important consideration in the assessment of evidence strength. Most studies have been observational, cross-sectional studies of SjD cohorts. While these make for quick and convenient recruitment, cross-sectional studies generally offer a weak study design and cannot readily offer insights into the longitudinal benefits of biomarker assessment.96 This limits the clinical translatability of these studies, since no study has yet demonstrated the potential to alter usual clinical practice for SjD.
From a practical and clinical point of view, the autoantibodies reviewed may be broadly classified as 1) those for diagnosing SjD patients apart from other CTD, such as SLE, and/or healthy donors; 2) those potentially identifying seronegative SjD patients; or 3) those identifying/predicting specific disease manifestations of SjD. The diagnostic antibodies, such as AFA, generally offer good diagnostic specificity for SjD and have reasonable discriminatory power (AUC around 0.70–0.80), but have poorer sensitivity. Therefore, their potential use may be for ruling in disease rather than screening for SjD. These statistics are dependent on the prevalence of SjD and the controls, and the ideal situation is differentiating SjD from non-SjD sicca, which may lack the classic anti-Ro52/Ro60/La autoantibodies. Since most studies have not examined this control cohort of patients, further evaluation is required before these antibodies may be considered for routine clinical use. In addition, given that anti-Ro52/Ro60 (SS-A) already demonstrates favourable specificity,97 it remains to be determined how these newer autoantibodies may fit into the routine clinical work-up of a patient with SjD. In the latest Outcome Measures in Rheumatology (OMERACT) Working Party for the development of SjD guidelines,98 novel autoantibodies were considered but ultimately not recommended for routine measurement in clinical trials.
Interest in some of these autoantibodies (eg, SP1 antibodies) in identifying seronegative SjD patients – or patients who lack the classic SjD-associated autoantibodies – is a particular focus.31 However, a limited number of studies has been performed in this area and, as these were cross-sectional studies, it is possible that these patients will go on to develop autoantibodies as their disease evolves.99 Seronegative SjD patients may also be a product of insensitive assays, as one study found that line immunoassays, which are commonly used to detect Ro52/Ro60/La autoantibodies, may not detect anti-Ro60 if its expression is too low.100 Salivary autoantibody testing for anti-Ro60 is a promising strategy to identify a subset of possible SjD patients who have demonstrable objective sicca, yet lack serum anti-Ro60.101
A final concern is about the translatability of many of the studies, in that many of the identified clinical associations (Table 1) can already be readily determined using standard and accessible clinical tests, with the possible exception of the assessments for cognitive impairment and MALT lymphoma (Table 1). For instance, anti-M3R antibodies are associated with disease activity and leukopaenia, which are already assessed using pre-existing tests and tools. Thus, these autoantibodies offer pathogenic insight but are yet to demonstrate clinical utility. These studies also highlight the difference between statistical significance and clinical significance. Many studies have analysed a large number of disease parameters (eg, Ref32) and statistically significant associations would arise by chance. Future studies are required to assess the clinical effect size and relevance, particularly regarding the potential to change clinical practice.
Newer studies are now taking a “shotgun” approach to identifying novel autoantibodies in SjD by probing protein and peptide arrays with patient and control sera.102,103 Although there are some promising candidates in identifying seronegative cohorts,103 validation in other and larger cohorts is required. Furthermore, some of these autoantibodies have limited clinical utility,104 and for these to be helpful in a practical sense, they would need to demonstrate equal or superior utility to the current conventional autoantibodies and biomarkers. This highlights the need for ongoing research and validation in patient cohorts. In summary, this review highlights several novel and non-conventional serum autoantibodies in SjD, and explores areas for future research. As markers of immune dysregulation, their identification not only aids with understanding the pathology of SjD, but also identifies potential therapeutic targets. While none of the autoantibodies explored so far has been validated for routine clinical use, upcoming studies are likely to clarify their potential utility.
Data Sharing Statement
Data sharing is not applicable as no new data were generated.
Author Contributions
The author has made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; has agreed on the journal to which the article has been submitted; and agrees to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
AL received a speaker honorarium and consultancy fees from Novartis. The author reports no other conflicts of interest in this work.
References
1. Lee AYS, Wang JJ, Gordon TP, Reed JH. Phases and Natural History of Sjögren’s Disease: a New Model for an Old Disease? Arthritis Care Res. 2023;75(7):1580–12. doi:10.1002/acr.25011
2. Lee AYS, Zembrzuska H, Franke KB, et al. Patients’ perspectives of living with Sjögren disease: a systematic review of qualitative studies from the OMERACT Sjögren Disease Working Group. Semin Arthritis Rheum. 2026;77:152929. doi:10.1016/j.semarthrit.2026.152929
3. Pelkas C, Franke KB, Vincent FB, Rischmueller M. Novel therapies in Sjögren’s disease: a systematic review of the literature. Best Pract Res Clin Rheumatol. 2025;39(4):102084. doi:10.1016/j.berh.2025.102084
4. Lee AY, Qi Z, Jackson KJ, Reed JH. Self-reactive B cells are increased in all major stages of peripheral development in Sjögren’s disease. Immunol Cell Biol. 2025;103(4):401–410. doi:10.1111/imcb.70005
5. Sisto M, Lisi S, Lofrumento D, D’Amore M, Scagliusi P, Mitolo V. Autoantibodies from Sjögren’s syndrome trigger apoptosis in salivary gland cell line. Ann N Y Acad Sci. 2007;1108(1):418–425. doi:10.1196/annals.1422.044
6. Manthorpe R, Permin H, Tage-Jensen U. Auto-antibodies in Sjögren’s syndrome. With special reference to liver-cell membrane antibody (LMA). Scand J Rheumatol. 1979;8(3):168–172. doi:10.3109/03009747909114450
7. Saku T, Shibata Y, Cheng J, Okabe H, Ikari N, Yagi Y. Autoantibodies to keratin in Sjögren’s syndrome. J Oral Pathol Med. 1990;19(1):45–48. doi:10.1111/j.1600-0714.1990.tb00781.x
8. Lee AYS, Beroukas D, Brown L, et al. Identification of a unique anti-Ro60 subset with restricted serological and molecular profiles. Clin Exp Immunol. 2021;203(1):13–21. doi:10.1111/cei.13508
9. Brito-Zerón P, Acar-Denizli N, Ng WF, et al. How immunological profile drives clinical phenotype of primary Sjögren’s syndrome at diagnosis: analysis of 10,500 patients (Sjögren Big Data Project). Clin Exp Rheumatol. 2018;36(3):102–112.
10. Lee AYS, Putty T, Lin MW, et al. Isolated anti-Ro52 identifies a severe subset of Sjögren’s syndrome patients. Front Immunol. 2023;14:1115548. doi:10.3389/fimmu.2023.1115548
11. Shiboski CH, Shiboski SC, Seror R, et al. American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: a Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017;69(1):35–45. doi:10.1002/art.39859
12. Baer AN, McAdams DeMarco M, Shiboski SC, et al. The SSB-positive/SSA-negative antibody profile is not associated with key phenotypic features of Sjögren’s syndrome. Ann Rheum Dis. 2015;74(8):1557–1561. doi:10.1136/annrheumdis-2014-206683
13. Shiboski SC, Shiboski CH, Criswell L, et al. American College of Rheumatology classification criteria for Sjögren’s syndrome: a data-driven, expert consensus approach in the Sjögren’s International Collaborative Clinical Alliance cohort. Arthritis Care Res. 2012;64(4):475–487. doi:10.1002/acr.21591
14. Bettacchioli E, Saraux A, Tison A, et al. Association of Combined Anti-Ro52/TRIM21 and Anti-Ro60/SSA Antibodies With Increased Sjögren Disease Severity Through Interferon Pathway Activation. Arthritis Rheumatol. 2024;76(5):751–762. doi:10.1002/art.42789
15. Maślińska M, Mańczak M, Kwiatkowska B. Usefulness of rheumatoid factor as an immunological and prognostic marker in PSS patients. Clin Rheumatol. 2019;38(5):1301–1307. doi:10.1007/s10067-019-04438-z
16. Goules AV, Chatzis L, Pezoulas VC, et al. Identification and evolution of predictors of Sjögren’s disease-associated mucosa-associated lymphoid tissue lymphoma development over time: a case-control study. Lancet Rheumatol. 2024;6(10):e693–e702. doi:10.1016/S2665-9913(24)00183-8
17. Quartuccio L, Baldini C, Priori R, et al. Cryoglobulinemia in Sjögren Syndrome: a Disease Subset that Links Higher Systemic Disease Activity, Autoimmunity, and Local B Cell Proliferation in Mucosa-associated Lymphoid Tissue. J Rheumatol. 2017;44:161465.
18. Lee AYS, Rischmueller M. The diagnosis and misdiagnosis of Sjögren disease. Intern Med J. 2024;54(5):833–835. doi:10.1111/imj.16395
19. Price EJ, Benjamin S, Bombardieri M, et al. Executive summary: British Society for Rheumatology guideline on management of adult and juvenile onset Sjögren disease. Rheumatology. 2024;64(2):396–408. doi:10.1093/rheumatology/keae218
20. Nellikka RK, Sreeja JS, Dharmapal D, et al. α-Fodrin is required for the organization of functional microtubules during mitosis. Cell Cycle. 2019;18(20):2713–2726. doi:10.1080/15384101.2019.1656476
21. Sun XL, Pang CY, Liu Y, Zhang W, Wang YF. Small Interfering RNA Targeting α-Fodrin Suppressing the Immune Response of Sjögren’s Syndrome Mice. Chin Med J. 2018;131(22):2752–2754. doi:10.4103/0366-6999.238761
22. Lawind MF, Alyasky A, Elwan NM, Mourad H, Al-Bendary A. Alpha-fodrin autoantibodies are reliable diagnostic markers for juvenile and adult Sjogren’s syndrome. Egypt J Immunol. 2004;11(1):75–81.
23. Hernández-Molina G, Nuñez-Alvarez C, Avila-Casado C, et al. Usefulness of IgA Anti-α-fodrin Antibodies in Combination with Rheumatoid Factor and/or Antinuclear Antibodies as Substitute Immunological Criterion in Sjögren Syndrome with Negative Anti-SSA/SSB Antibodies. J Rheumatol. 2016;43(10):1852–1857. doi:10.3899/jrheum.151315
24. Witte T, Matthias T, Arnett FC, et al. IgA and IgG autoantibodies against alpha-fodrin as markers for Sjögren’s syndrome. Systemic lupus erythematosus J Rheumatol. 2000;27(11):2617–2620.
25. Zandbelt MM, Vogelzangs J, Van De Putte LB, Van Venrooij WJ, Van Den Hoogen FH. Anti-alpha-fodrin antibodies do not add much to the diagnosis of Sjögren’s syndrome. Arthritis Res Ther. 2004;6(1):R33–R38. doi:10.1186/ar1021
26. Hu Q, Wang D, Chen W. The accuracy of the anti-α-fodrin antibody test for diagnosis of Sjögren’s syndrome: a meta-analysis. Clin Biochem. 2013;46(15):1372–1376. doi:10.1016/j.clinbiochem.2013.04.020
27. Rostamian A, Baradaran A, Mottaghi P, Salesi M, Karimifar M, Mansouri V. Evaluation of Diagnostic Accuracy of Alpha-Fodrin Antibody in Iranian Patients with Sjogren’s Disease. Adv Biomed Res. 2022;11(1):64. doi:10.4103/abr.abr_260_20
28. de Seze J, Dubucquoi S, Fauchais AL, et al. Autoantibodies against alpha-fodrin in Sjögren’s syndrome with neurological manifestations. J Rheumatol. 2004;31(3):500–503.
29. Turkçapar N, Olmez U, Tutkak H, Duman M. The importance of alpha-fodrin antibodies in the diagnosis of Sjögren’s syndrome. Rheumatol Int. 2006;26(4):354–359. doi:10.1007/s00296-005-0607-9
30. Shen L, Suresh L, Lindemann M, et al. Novel autoantibodies in Sjogren’s syndrome. Clin Immunol. 2012;145(3):251–255. doi:10.1016/j.clim.2012.09.013
31. Shen L, Kapsogeorgou EK, Yu M, et al. Evaluation of salivary gland protein 1 antibodies in patients with primary and secondary Sjogren’s syndrome. Clin Immunol. 2014;155(1):42–46. doi:10.1016/j.clim.2014.08.009
32. Thatayatikom A, Jun I, Bhattacharyya I, et al. The Diagnostic Performance of Early Sjögren’s Syndrome Autoantibodies in Juvenile Sjögren’s Syndrome: the University of Florida Pediatric Cohort Study. Front Immunol. 2021;12:704193. doi:10.3389/fimmu.2021.704193
33. Wang ZM, Yang YS, Qi X, et al. Comparison and clinical analysis of tissue-specific autoantibody levels in primary Sjögren’s disease and other connective tissue diseases. Clin Exp Rheumatol. 2025;43(12):2060–2068. doi:10.55563/clinexprheumatol/tt1e0x
34. Jin Y, Li J, Chen J, et al. Tissue-Specific Autoantibodies Improve Diagnosis of Primary Sjögren’s Syndrome in the Early Stage and Indicate Localized Salivary Injury. J Immunol Res. 2019;2019:3642937. doi:10.1155/2019/3642937
35. Karakus S, Baer AN, Akpek EK. Clinical Correlations of Novel Autoantibodies in Patients with Dry Eye. J Immunol Res. 2019;2019:7935451. doi:10.1155/2019/7935451
36. De Langhe E, Bossuyt X, Shen L, Malyavantham K, Ambrus JL, Suresh L. Evaluation of Autoantibodies in Patients with Primary and Secondary Sjogren’s Syndrome. Open Rheumatol J. 2017;11(1):10–15. doi:10.2174/1874312901711010010
37. Hubschman S, Rojas M, Kalavar M, Kloosterboer A, Sabater AL, Galor A. Association Between Early Sjögren Markers and Symptoms and Signs of Dry Eye. Cornea. 2020;39(3):311–315. doi:10.1097/ICO.0000000000002171
38. Inagaki Y, Jinno-Yoshida Y, Hamasaki Y, Ueki H. A novel autoantibody reactive with carbonic anhydrase in sera from patients with systemic lupus erythematosus and Sjögren’s syndrome. J Dermatol Sci. 1991;2(3):147–154. doi:10.1016/0923-1811(91)90060-B
39. Ono M, Ono M, Watanabe K, Miyashita Y, Inagaki Y, Ueki H. A study of anti-carbonic anhydrase II antibodies in rheumatic autoimmune diseases. J Dermatol Sci. 1999;21(3):183–186. doi:10.1016/S0923-1811(99)00032-8
40. Takemoto F, Hoshino J, Sawa N, et al. Autoantibodies against carbonic anhydrase II are increased in renal tubular acidosis associated with Sjogren syndrome. Am J Med. 2005;118(2):181–184. doi:10.1016/j.amjmed.2004.07.049
41. Kino-Ohsaki J, Nishimori I, Morita M, et al. Serum antibodies to carbonic anhydrase I and II in patients with idiopathic chronic pancreatitis and Sjögren’s syndrome. Gastroenterology. 1996;110(5):1579–1586. doi:10.1053/gast.1996.v110.pm8613065
42. Tsuboi H, Matsumoto I, Wakamatsu E, et al. New epitopes and function of anti-M3 muscarinic acetylcholine receptor antibodies in patients with Sjögren’s syndrome. Clin Exp Immunol. 2010;162(1):53–61. doi:10.1111/j.1365-2249.2010.04188.x
43. Mona M, Mondello S, Hyon JY, et al. Clinical usefulness of anti-muscarinic type 3 receptor autoantibodies in patients with primary Sjögren’s syndrome. Clin Exp Rheumatol. 2021;39(4):795–803. doi:10.55563/clinexprheumatol/gy6udz
44. Deng C, Hu C, Chen S, et al. Meta-analysis of anti-muscarinic receptor type 3 antibodies for the diagnosis of Sjögren syndrome. PLoS One. 2015;10(1):e0116744. doi:10.1371/journal.pone.0116744
45. Zuo J, Williams AE, Park YJ, et al. Muscarinic type 3 receptor autoantibodies are associated with anti-SSA/Ro autoantibodies in Sjögren’s syndrome. J Immunol Methods. 2016;437:28–36. doi:10.1016/j.jim.2016.07.003
46. Kovács L, Marczinovits I, György A, et al. Clinical associations of autoantibodies to human muscarinic acetylcholine receptor 3(213–228) in primary Sjogren’s syndrome. Rheumatology. 2005;44(8):1021–1025. doi:10.1093/rheumatology/keh672
47. Cui L, Elzakra N, Xu S, Xiao GG, Yang Y, Hu S. Investigation of three potential autoantibodies in Sjogren’s syndrome and associated MALT lymphoma. Oncotarget. 2017;8(18):30039–30049. doi:10.18632/oncotarget.15613
48. Wei P, Xing Y, Li B, Chen F, Hua H. Proteomics-based analysis indicating α-enolase as a potential biomarker in primary Sjögren’s syndrome. Gland Surg. 2020;9(6):2054–2063. doi:10.21037/gs-20-814
49. Nezos A, Cinoku I, Mavragani CP, Moutsopoulos HM. Antibodies against citrullinated alpha enolase peptides in primary Sjogren’s syndrome. Clin Immunol. 2017;183:300–303. doi:10.1016/j.clim.2017.09.012
50. Olivares-Martínez E, Hernández-Ramírez DF, Núñez-álvarez CA, Llorente L, Hernandez-Molina G. α-enolase is an antigenic target in primary Sjögren’s syndrome. Clin Exp Rheumatol. 2019;37(3):29–35.
51. Tzartos JS, Stergiou C, Daoussis D, et al. Antibodies to aquaporins are frequent in patients with primary Sjögren’s syndrome. Rheumatology. 2017;56(12):2114–2122. doi:10.1093/rheumatology/kex328
52. Wang X, Wu H, Zhong B, Zhang L, Wang Y. Autoantibody against aquaporin-5 may be a new diagnostic biomarker for primary Sjögren’s syndrome. Clin Rheumatol. 2024;43(12):3781–3787. doi:10.1007/s10067-024-07190-1
53. Stano S, Cacciapaglia F, Rinaldi A, et al. Anti-aquaporin-5 and anti-poly-U-binding-factor-60kDa protein antibodies in primary Sjögren’s disease patients: preliminary data and correlation with disease activity indices. Clin Exp Rheumatol. 2024;42(12):2420–2426. doi:10.55563/clinexprheumatol/ku7y1q
54. Lee KE, Kang JH, Lee JW, et al. Anti-centromere antibody-positive Sjögren’s syndrome: a distinct clinical subgroup? Int J Rheum Dis. 2015;18(7):776–782. doi:10.1111/1756-185X.12684
55. Baer AN, Medrano L, McAdams-DeMarco M, Gniadek TJ. Association of Anticentromere Antibodies With More Severe Exocrine Glandular Dysfunction in Sjögren’s Syndrome: analysis of the Sjögren’s International Collaborative Clinical Alliance Cohort. Arthritis Care Res. 2016;68(10):1554–1559. doi:10.1002/acr.22859
56. Tsukamoto M, Suzuki K, Takeuchi T. Clinical and Immunological Features of Anti-centromere Antibody-Positive Primary Sjögren’s Syndrome. Rheumatol Ther. 2018;5(2):499–505. doi:10.1007/s40744-018-0126-2
57. Nakamura H, Kawakami A, Hayashi T, et al. Anti-centromere antibody-seropositive Sjögren’s syndrome differs from conventional subgroup in clinical and pathological study. BMC Musculoskelet Disord. 2010;11(1):140. doi:10.1186/1471-2474-11-140
58. Kwon EJ, Lee BW, Park Y, Lee JJ, Park SH, Kwok SK. AB0637 The clinical characteristics of Korean primary Sjögren’s syndrome (pSS) patients with positive anti-double-stranded DNA (anti-dsDNA) antibody by the Farr method. Ann Rheum Dis. 2023;82(Suppl 1):1521. doi:10.1136/annrheumdis-2023-eular.3594
59. Schmidt NS, Voss A, Nilsson AC, Terslev L, Just SA, Lindegaard HM. Salivary gland ultrasound is associated with the presence of autoantibodies in patients with Sjögren’s syndrome: a Danish single-centre study. PLoS One. 2022;17(12):e0265057. doi:10.1371/journal.pone.0265057
60. Abbara S, Seror R, Henry J, et al. Anti-RNP positivity in primary Sjögren’s syndrome is associated with a more active disease and a more frequent muscular and pulmonary involvement. RMD Open. 2019;5(2):e001033. doi:10.1136/rmdopen-2019-001033
61. Cheng F, Wang YL, Ai XY, et al. Clinical features of anti-RNP-positive primary Sjögren’s syndrome. Clin Rheumatol. 2025;44(7):2911–2917. doi:10.1007/s10067-025-07499-5
62. Lee AYS. Histone antibodies in primary Sjögren’s disease. J Clin Pathol. 2025;78(4):287–288. doi:10.1136/jcp-2024-209803
63. Gottenberg JE, Mignot S, Nicaise-Rolland P, et al. Prevalence of anti-cyclic citrullinated peptide and anti-keratin antibodies in patients with primary Sjögren’s syndrome. Ann Rheum Dis. 2005;64(1):114–117. doi:10.1136/ard.2003.019794
64. Atzeni F, Sarzi-Puttini P, Lama N, et al. Anti-cyclic citrullinated peptide antibodies in primary Sjögren syndrome may be associated with non-erosive synovitis. Arthritis Res Ther. 2008;10(3):R51. doi:10.1186/ar2420
65. Bagavant H, Araszkiewicz AM, Rasmussen A, et al. Anti-vimentin antibodies are associated with higher severity of Sjögren’s disease. Clin Immunol. 2023;247:109243. doi:10.1016/j.clim.2023.109243
66. Lauvsnes MB, Maroni SS, Appenzeller S, et al. Memory dysfunction in primary Sjögren’s syndrome is associated with anti-NR2 antibodies. Arthritis Rheum. 2013;65(12):3209–3217. doi:10.1002/art.38127
67. Everett S, Vishwanath S, Cavero V, et al. Analysis of novel Sjogren’s syndrome autoantibodies in patients with dry eyes. BMC Ophthalmol. 2017;17(1):20. doi:10.1186/s12886-017-0412-8
68. Supuran CT. Carbonic anhydrases as drug targets--an overview. Curr Top Med Chem. 2007;7(9):825–833. doi:10.2174/156802607780636690
69. Pertovaara M, Parkkila S, Korpela M. Anti-carbonic anhydrase autoantibodies and serum beta-2 microglobulin correlate with the ClinESSDAI score in patients with Sjögren’s syndrome. Clin Exp Rheumatol. 2017;35(2):351.
70. Jin YB, Dai YJ, Chen JL, et al. Anti-carbonic anhydrase II antibody reflects urinary acidification defect especially in proximal renal tubules in patients with primary Sjögren syndrome. Medicine. 2023;102(2):e32673. doi:10.1097/MD.0000000000032673
71. Pertovaara M, Bootorabi F, Kuuslahti M, Pasternack A, Parkkila S. Novel carbonic anhydrase autoantibodies and renal manifestations in patients with primary Sjogren’s syndrome. Rheumatology. 2011;50(8):1453–1457. doi:10.1093/rheumatology/ker118
72. Nishimori I, Bratanova T, Toshkov I, et al. Induction of experimental autoimmune sialoadenitis by immunization of PL/J mice with carbonic anhydrase II. J Immunol. 1995;154(9):4865–4873. doi:10.4049/jimmunol.154.9.4865
73. Takemoto F, Katori H, Sawa N, et al. Induction of anti-carbonic-anhydrase-II antibody causes renal tubular acidosis in a mouse model of Sjogren’s syndrome. Nephron Physiol. 2007;106(4):63–68. doi:10.1159/000104873
74. Nakamura T, Matsui M, Uchida K, et al. M3 muscarinic acetylcholine receptor plays a critical role in parasympathetic control of salivation in mice. J Physiol. 2004;558(2):561–575. doi:10.1113/jphysiol.2004.064626
75. Sumida T, Tsuboi H, Iizuka M, Asashima H, Matsumoto I. Anti-M3 muscarinic acetylcholine receptor antibodies in patients with Sjögren’s syndrome. Mod Rheumatol. 2013;23(5):841–845. doi:10.3109/s10165-012-0788-5
76. Namkoong E, S-w L, Kim N, Choi Y, Park K. Effect of anti-muscarinic autoantibodies on leukocyte function in Sjögren’s syndrome. Mol Immunol. 2017;90:136–142. doi:10.1016/j.molimm.2017.07.007
77. Chen Y, Zheng J, Huang Q, et al. Autoantibodies against the Second Extracellular Loop of M3R Do neither Induce nor Indicate Primary Sjögren’s Syndrome. PLoS One. 2016;11(2):e0149485. doi:10.1371/journal.pone.0149485
78. Jayakanthan K, Ramya J, Mandal SK, Sandhya P, Gowri M, Danda D. Younger patients with primary Sjögren’s syndrome are more likely to have salivary IgG anti-muscarinic acetylcholine receptor type 3 antibodies. Clin Rheumatol. 2016;35(3):657–662. doi:10.1007/s10067-016-3186-0
79. Verkman AS. Aquaporins. Curr Biol. 2013;23(2):R52–55. doi:10.1016/j.cub.2012.11.025
80. Akaishi T, Takahashi T, Fujihara K, et al. Impact of comorbid Sjögren syndrome in anti-aquaporin-4 antibody-positive neuromyelitis optica spectrum disorders. J Neurol. 2021;268(5):1938–1944. doi:10.1007/s00415-020-10377-6
81. Chivasso C, D’Agostino C, Parisis D, Soyfoo MS, Delporte C. Involvement of aquaporin 5 in Sjögren’s syndrome. Autoimmun Rev. 2023;22(3):103268. doi:10.1016/j.autrev.2023.103268
82. Nakamura H, Tanaka T, Zheng C, et al. Correction of LAMP3-associated salivary gland hypofunction by aquaporin gene therapy. Sci Rep. 2022;12(1):18570. doi:10.1038/s41598-022-21374-2
83. Lee AYS, Ang EB. A clinical overview of autoantibodies in general practice rheumatology. Br J Gen Pract. 2014;64(626):e599–e601. doi:10.3399/bjgp14X681601
84. Gelber AC, Pillemer SR, Baum BJ, et al. Distinct recognition of antibodies to centromere proteins in primary Sjogren’s syndrome compared with limited scleroderma. Ann Rheum Dis. 2006;65(8):1028–1032. doi:10.1136/ard.2005.046003
85. Collins K, Mitchell S, Griffiths B, Bowman SJ, Ng WF. Potential diagnostic utility of anti-centromere antibody in primary Sjögren’s syndrome in the UK. Clin Rheumatol. 2012;31(7):1147–1148. doi:10.1007/s10067-012-2005-5
86. Zou S, Zhang R, Yang D, et al. Clinical manifestations and immune correlations in anti-centromere antibody-positive and anti-SSA/Ro antibody-positive primary Sjögren’s syndrome: a retrospective analysis. PLoS One. 2025;20(8):e0322845. doi:10.1371/journal.pone.0322845
87. Shimizu T, S-y N, Nakamura H, Takagi Y, Sumi M, Kawakami A. Anti-centromere antibody positivity is an independent variable associated with salivary gland ultrasonography score in Sjögren’s syndrome. Sci Rep. 2024;14(1):5303. doi:10.1038/s41598-024-55767-2
88. Inamo J, Takeshita M, Suzuki K, et al. Comparative single-cell and spatial profiling of anti-SSA-positive and anti-centromere-positive Sjögren’s disease reveals common and distinct immune activation and fibroblast-mediated inflammation. Nat Commun. 2025;16(1):8299. doi:10.1038/s41467-025-63935-9
89. Yao Q, Altman RD, Wang X. Systemic lupus erythematosus with Sjögren syndrome compared to systemic lupus erythematosus alone: a meta-analysis. J Clin Rheumatol. 2012;18(1):28–32. doi:10.1097/RHU.0b013e31823ecbdf
90. Satoh M, Yamagata H, Watanabe F, et al. Development of anti-Sm and anti-DNA antibodies followed by clinical manifestation of systemic lupus erythematosus in an elderly woman with long-standing Sjögren’s syndrome. Lupus. 1995;4(1):63–65. doi:10.1177/096120339500400113
91. Lee AYS. Clinical use of anti-histone antibodies in idiopathic and drug-induced lupus. Immunol Med. 2022;45(4):180–185. doi:10.1080/25785826.2022.2060168
92. Deng X, Li J, Hou S, Ci B, Liu B, Xu K. Prevalence and impact of Sjögren’s syndrome in primary biliary cholangitis: a systematic review and meta-analysis. Ann Hepatol. 2022;27(6):100746. doi:10.1016/j.aohep.2022.100746
93. Li Y-H, Gao Y-P, Dong J, et al. Identification of a novel autoantibody against self-vimentin specific in secondary Sjögren’s syndrome. Arthritis Res Ther. 2018;20(1):30. doi:10.1186/s13075-017-1508-5
94. Lee AYS. Standardisation of the term “anti-Ro/SSA” in patients with Sjögren’s disease and other disorders. Clin Exp Rheumatol. 2024;42(12):2544–2545. doi:10.55563/clinexprheumatol/ys8gtf
95. Beroukas D, Roberts-Thomson PJ, Gordon TP, Lee AYS. Immunoprecipitation assays for the detection of specific extractable nuclear antigen autoantibodies: a role in the modern immunology laboratory? Pathology. 2025;57(1):120–121. doi:10.1016/j.pathol.2024.08.008
96. Wang X, Cheng Z. Cross-Sectional Studies: strengths, Weaknesses, and Recommendations. Chest. 2020;158(1):S65–S71. doi:10.1016/j.chest.2020.03.012
97. Vílchez-Oya F, Balastegui Martin H, García-Martínez E, Corominas H. Not all autoantibodies are clinically relevant. Classic and novel autoantibodies in Sjögren’s syndrome: a critical review. Front Immunol. 2022;13:1003054. doi:10.3389/fimmu.2022.1003054
98. Gordon RA, Nguyen Y, Foulquier N, et al. The Sjögren’s Working Group: the 2023 OMERACT meeting and provisional domain generation. Semin Arthritis Rheum. 2024;65:152378. doi:10.1016/j.semarthrit.2024.152378
99. Lee AYS, Lin MW. Serological intermolecular epitope spreading in a patient with primary Sjögren’s syndrome. BMJ Case Rep. 2023;16(5):e254632. doi:10.1136/bcr-2023-254632
100. Lee AYS, Beroukas D, Wienholt L, Gordon TP. Validation of a commercial line blot for the detection of serum anti-Ro60 autoantibodies. Pathology. 2022;54(7):900–903. doi:10.1016/j.pathol.2022.05.009
101. Tsaliki M, Cavett J, Kurien BT, et al. A cross-sectional observational study of patients with sicca with salivary autoantibodies defines a potential new phenotype of Sjögren’s disease. Ann Rheum Dis. 2025;84(8):1354–1362. doi:10.1016/j.ard.2025.03.012
102. Engelke F, Budde P, De Vita S, et al. Identification of novel autoantibodies in Sjögren’s disease. Front Immunol. 2025;16:1524940. doi:10.3389/fimmu.2025.1524940
103. Parker M, Zheng Z, Lasarev MR, et al. Novel autoantibodies help diagnose anti-SSA antibody negative Sjögren disease and predict abnormal labial salivary gland pathology. Ann Rheum Dis. 2024;83(9):1169–1180. doi:10.1136/ard-2023-224936
104. Longobardi S, Lopez-Davis C, Khatri B, et al. Autoantibodies identify primary Sjögren’s syndrome in patients lacking serum IgG specific for Ro/SS-A and La/SS-B. Ann Rheum Dis. 2023;82(9):1181–1190. doi:10.1136/ard-2022-223105
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.