Back to Journals » Nature and Science of Sleep » Volume 14
Non-Constructive Ruminations, Insomnia and Nightmares: Trio of Vulnerabilities to Suicide Risk
Authors Faccini J, Joshi V, Graziani P, Del-Monte J ![]()
Received 22 September 2021
Accepted for publication 19 December 2021
Published 15 March 2022 Volume 2022:14 Pages 433—441
DOI https://doi.org/10.2147/NSS.S339567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Julie Faccini, Vrutti Joshi, Pierluigi Graziani, Jonathan Del-Monte
University of Nîmes, LSP Laboratory, Aix-Marseille University, Marseille, France
Correspondence: Julie Faccini, LSP Laboratory, Aix-Marseille University, 5 Rue Château de l’Horloge, Marseille, 13090, Aix-en-Provence, France, Tel +33 4 42 52 40 00, Email [email protected]
Objective: Nightmare distress, nightmare frequency and anxiety are related to suicidal risk. Ruminations are a factor maximizing the risk of suicide. Research has identified two types of ruminations: constructive ruminations and non-constructive ruminations. As per our knowledge, no study has verified the links between non-constructive ruminations and sleep disorders and their role in the development of suicidal risk. We aimed to highlight the impact of non-constructive ruminations on nightmares, anxiety and insomnia in the development of suicidal risk.
Methods: A total of 429 French participants responded to an anonymous online survey using the Qualtrics® software. To assess variables, we used the Mini Cambridge-Exeter Repetitive Thought Scale, the Suicide Behaviors Questionnaire-Revised, the Nightmare Distress Questionnaire, the Beck Anxiety Inventory, and the Sleep Condition Indicator. Nightmare frequency was assessed by subjective evaluation through a question. We tested the possible effects of confounding variables such as age, gender, marital status and depression (Beck Depression Inventory-II).
Results: Nightmare frequency was found to mediate the link between anxiety and suicidal risk (32.9%). Nightmare distress (37%) and non-constructive thoughts (48%) were also seen to mediate this link. Additionally, we found a moderating effect of insomnia on the link between non-constructive ruminations and suicidal risk (Z = 7.42, p < 0.001).
Conclusion: Our results showed that the frequency of nightmares, distress and non-constructive ruminations are closely related to suicidal risk. The interoperability between these elements and insomnia has thus been newly explored. The processes related to nightmares and suicidal risk as well as the underlying cognitive processes between sleep disorders and suicidal risk have been shed light upon.
Keywords: suicidal risk, sleep disorders, non-constructive ruminations, nightmares
Introduction
On average, 800,000 people die each year worldwide as a result of suicide.1 A significant percentage of deaths from suicide could be prevented. Psychiatric disorders appear as a key antecedent to suicide. Estimates of the proportion of population experiencing a mental illness at the time of their suicide range from ~ 90% in North America to 30–70% in east Asia.2 In particular, suicide is often correlated with a psychiatric diagnosis such as depression, schizophrenia, borderline personality.3 However, not all patients attempt to end their lives. This means that pathology is not considered as the main factor,4 and that a better understanding of the underlying processes is essential. Research has identified many risk factors for suicide including heritability,5 socio-economic factors, age, and gender.6 Sleep disorders are also a determining factor in suicide risk and are frequently cited.7 The Substance Abuse and Mental Health services Administration and the American Association of Suicidology consider sleep disorders as one of the 10 warning signs of suicidal risk.8 According to the literature, this association ranges between a relative risk of 1.95 and 2.95.9 Evidence suggests that sleep disturbances increase the risk of suicide but the understanding of the underlying mechanisms remains unclear. Nightmares appear as one of the specific sleep problems associated with suicidal behavior.10 These are defined as vivid or frightening dreams which cause the individual to wake up. Studies of the general population have indicated that around 2–5% of the adult population report one or more nightmares a week.11 A recent meta-analysis shows that nightmares significantly predicted suicide attempt.12 In fact, nightmares have also been shown to be comorbid with depression, anxiety, and suicide.13 Most research links insomnia and nightmares in their understanding of suicidal risk. However, some studies have shown that insomnia and nightmares independently influence symptoms of psychopathology and suicide risk.14 Consequently, it is essential to understand the interrelationships between specific mental health problems, nightmares, and suicidal behavior to maximize suicide risk assessment and management. Some factors have been identified as mediating the relationship between nightmares and suicidal risk such as perceptions of defeat, entrapment, hopelessness,15,16 belongingness and perceived burdensomeness.17 Two correlates of nightmares are highlighted to understand their impact: the frequency of nightmares and the associated emotional distress. In previous studies, the association between nightmare frequency and suicidal thoughts was fully mediated by nightmare distress.18,19 Although the links between these different factors are known, the underlying processes remain relatively unexplored. Recent evidence throws light upon non-constructive ruminations.20 Rumination is a mental process characterized by repetitive, prolonged, and recurrent thinking about one’s concerns and one’s experience. This is a factor maximizing the risk of suicide.21 Research has identified two types of ruminations: constructive ruminations and non-constructive ruminations, or repetitive negative thoughts.20 Constructive ruminations labelled “concrete, experiential thinking”, have been identified as adaptive for individuals.20 Conversely, non-constructive ruminations, labelled “abstract, analytical thinking” are identified as highly detrimental to mental health. To our knowledge, no study has investigated the relationship between non-constructive ruminations and nightmares. Slavish22 highlighted the impact of ruminations on the loss of sleep quality in his study. Given the deleterious nature of non-constructive ruminations, in contrast to constructive ruminations, it seems interesting to study this type of rumination more precisely in its relationship with nightmares and suicidal risk. In fact, a recent study has demonstrated that sleep-deprived individuals are ineffective at suppressing unwanted thoughts leading to emotional dysregulation.23 Another recent study24 found a strong relationship between nightmares and intrusive thoughts. These latter data tend to explain the major role of the interoperability of cognitive factors such as intrusive thoughts and rumination with nightmares. Their psychopathological repercussions are expressed in particular through the risk of suicide. Indeed, this very specific cognitive factor appears to be a disrupter of the relationship between emotional regulation, cognitive regulation and the psychopathological substrates of sleep such as insomnia and nightmares. Given the interdependence of insomnia, nightmares, and suicidal risk, it seems relevant to investigate the mediating role of non-constructive ruminations. According to our knowledge, no study has verified the links between non-constructive ruminations, anxiety, distress associated with nightmares and their frequency on the development of mental illness and suicide risk. We aim to highlight the role of non-constructive ruminations in the potential action of nightmares in the development of suicidal risk.
Methods
A total of 695 participants were evaluated using the Qualtrics® software (https://www.qualtrics.com); the participants were required to respond to an anonymous online survey. After checking the data (missing data, inconsistent responding) (n=266), data from 429 participants was retained for statistical analysis. The survey was executed and accessible between March 29 to May 11, 2020. The questionnaire was distributed on social media (Facebook, WhatsApp and Twitter) to allow the greatest possible recruitment of participants. An introductory message was included at the beginning of the online survey, informing the participants about the purpose of the study, the use of data, and the study procedures. The message also informed the participants that their participation was totally voluntary and that their identities would be kept confidential. The recruited individuals were correctly informed of the researcher’s objectives, methods, institutional affiliations, expected benefits and potential risks of the research, the inconvenience it may cause and any other relevant aspects of the research. The individuals were informed of their right to refuse to participate or to withdraw from it at any time without retaliatory action conforming to the Declaration of Helsinki. Informed consent was thus obtained virtually from the participants before participation. Upon the confirmation of consent, the participants were asked to complete and submit only one online self-report survey each including the collection of demographic data. The total duration of the research protocol was approximately 30 minutes. The inclusion criteria were to speak, read and understand French fluently and to be at least 18 years old. The Ethics Committee of the University of Aix-Marseille approved the study 2,020,012,307 in accordance with the Declaration of Helsinki.
Measures
The Beck Depression Inventory II (BDI-II)25 assesses severity of depression symptoms over the past 2 weeks. This questionnaire has 13 items with answer options that range from 0 to 3 points, with a possible maximum score of 39. Scores> 4 indicate no depression, score>7 indicate mild depression, score>15 indicate moderate depression and score>16 indicate severe depression. The BDI-II demonstrated an acceptable internal consistency (α=0.93).
The Mini Cambridge-Exeter Repetitive Thought Scale (Mini-CERTS)26 is a short, 16-item questionnaire used to measure constructive and non-constructive ruminations. The items were rated on a 1–4 scale (1 = almost never, 4 = almost always). Participants were instructed to rate the items in order to reflect how they typically think when they are confronted to a difficult situation. In our study, the scores represent only non-constructive ruminations. The Mini-CERTS demonstrated an acceptable internal consistency (α=0.71).
The Suicide Behaviors Questionnaire-Revised (SBQ-R)27 is a four question self-report measure which has been used to assign a designation of high or low suicide risk. The SBQ-R assesses lifetime suicidal ideation and/or suicide attempts. A score ≥7 indicates that participants are in the high suicidal risk group, while scores <7 placed participants in the low suicidal risk group. The internal consistency is satisfactory (α=0.80).
The Nightmare Distress Questionnaire (NDQ)28 is a 13-item measure used to assess the distress related to nightmares. Participants are asked to rate the items according to their frequency from never to always. Scores range from 0–52. The internal consistency is good (α=0.88).
Nightmare frequency (NF) was measured by asking participants “In the past 3 months, on average, how often have you had nightmares?”. Participants could answer: no nightmares; one night/month; two nights/month; one night/week; two to three nights/week; four nights/week; five nights/week; six to seven nights/week. Responses were converted to a score ranging from 0 to 8, 8 representing the highest frequency.
The Beck Anxiety Inventory (BAI)29 was designed to assess anxiety levels. It contains 21 items that measure anxiety-related symptoms. Subjects were asked to rate the severity of their anxiety on 4- point Likert scales (0–3). It was shown to have a satisfactory internal consistency (α=0.85).
The Sleep Condition Indicator (SCI), which is an 8-item rating scale, was used to assess insomnia. Subjects were asked to rate the severity of their nighttime and daytime symptoms on 4- point Likert scales (0–3), the items are reversed. The cut-off value is ≤ 16. The French version of the SCI scale has shown a good internal consistency (α=0.87).30
Statistical Analysis
The statistical analyses were conducted with “Jamovi software”. Descriptive statistics were calculated for all study variables. We tested the possible effects of confounding variables such as age, gender and marital status on all clinical variables (frequency and distress related to nightmares, level of depression, level of anxiety, sleep disorders, level of non-constructive ruminations and level of suicidal risk). Pearson correlational analyses were calculated for nightmare frequency, nightmare distress (NDQ), Insomnia (SCI), non-constructive ruminations (Mini-CERTS), anxiety (BAI) and suicide risk (SBQ-R). Regression analysis was conducted. The variable to be predicted was suicide risk, predictors were the frequency of nightmares, nightmare distress, non-constructive ruminations, and anxiety level. Mediation analyses were conducted to better understand the relationship between anxiety and suicidal risk by mediating nightmare frequency, nightmare distress and non-constructive ruminations. Finally, we conducted a moderation analysis of the insomnia variable on the relationship between the non-constructive rumination predictor and the suicide risk predictor variable.
Results
Socio-demographic data for the total sample are presented in Table 1. Descriptive statistics were used to assess the mean and standard deviation of the scores of nightmare’s frequency (M=2.51; SD=1.63), the Beck Depression Inventory-II (BDI-II; M=7.02; SD=5.57), the Beck Anxiety Inventory (BAI, M=12.19; SD=9.77), the Sleep Condition Indicator (SCI, M=17.61; SD=7.51), the Nightmares Distress Questionnaire (NDQ, M=11.85; SD =8.8), the Suicide Behaviors Questionnaire Revised (SBQR; M=5.76; SD=3.03) and the Cambridge-Exeter Repetitive Thought Scale (Mini-CERT, M=17.91; SD=4.51). We tested for the effects of confounding variables on all clinical variables. We tested for the effect of gender, marital status and age. For the age variable, we created two groups based on the median (41 years). The results are presented in Tables 2–4. No effect was found.31 These results highlight the homogeneity of the sample. Further statistical processing was carried out on the full sample.
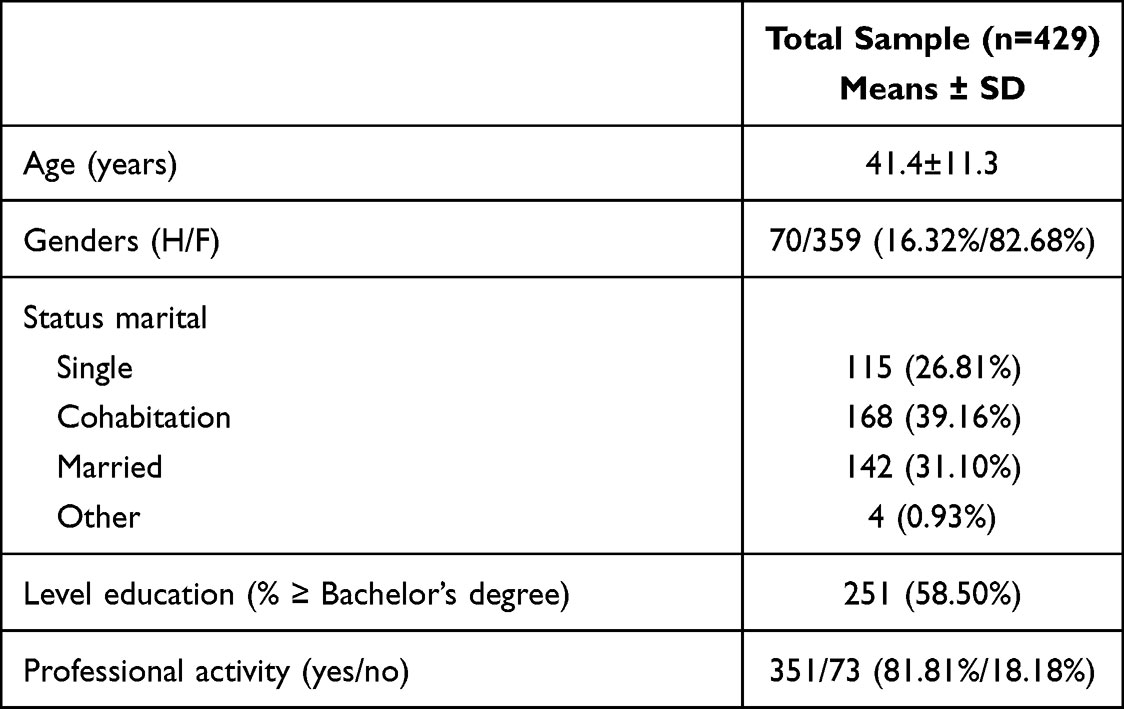 |
Table 1 Presentation of Socio-Demographic Data for the Full Sample (n=429) |
 |
Table 2 Comparison of Clinical Variables Between Genders |
 |
Table 3 Comparison of Clinical Variables Between Age Groups (Median Age: 41 Years) |
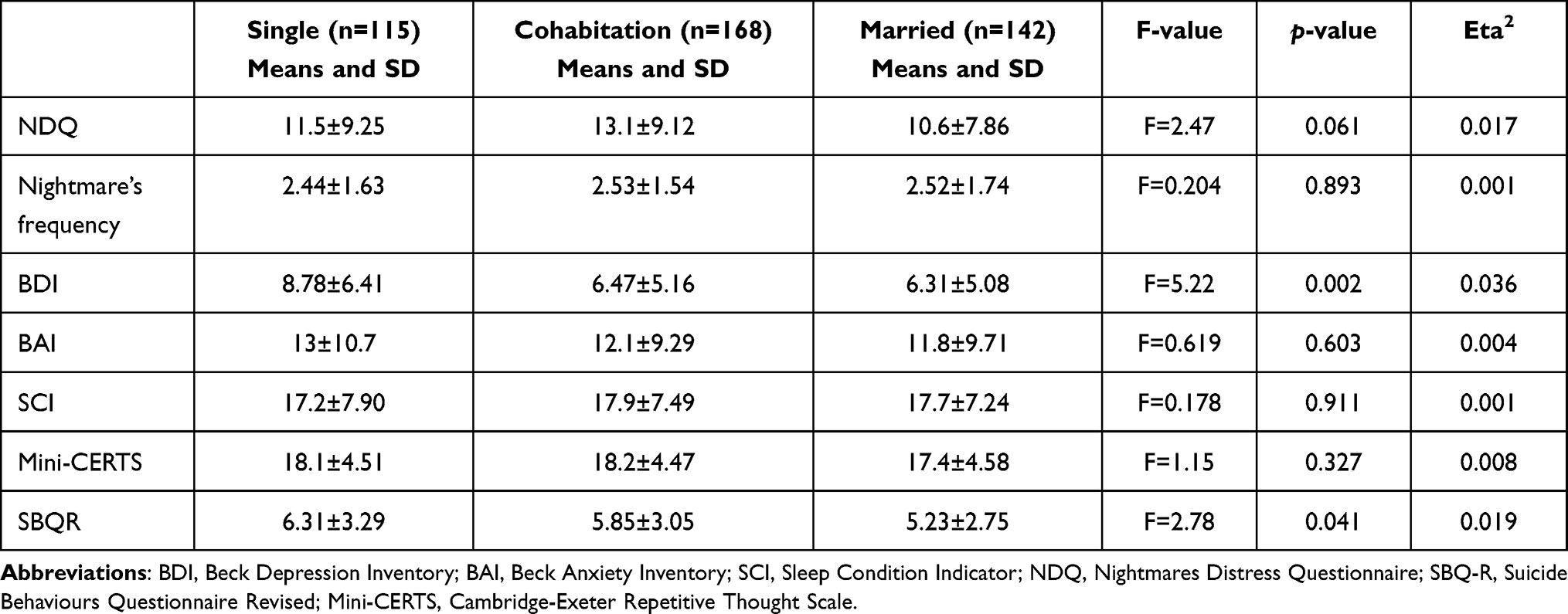 |
Table 4 Comparison of Clinical Variables Between Marital Status (n=425) |
Correlations among the psychometric measures are shown in Table 5. All variables are positively correlated with each other. Insomnia is negatively (reversed items) and significantly correlated to all other variables.
 |
Table 5 Correlations Between Clinical Variables |
A multiple linear regression assessed the first hypothesis which stated that frequency of nightmares, nightmare distress and non-constructive ruminations are associated with suicide risk. The overall regression was significant (R2=0.23, p< 0.01). Frequency of nightmares (S.E.=0.16, p.< 0.01), non-constructive ruminations (S.E.=0.30, p.<0.001) and significant trends exist for anxiety level (S.E.=0.092, p=0.082) and nightmare distress (S.E.=0.13, p=0.085) (see Table 6).
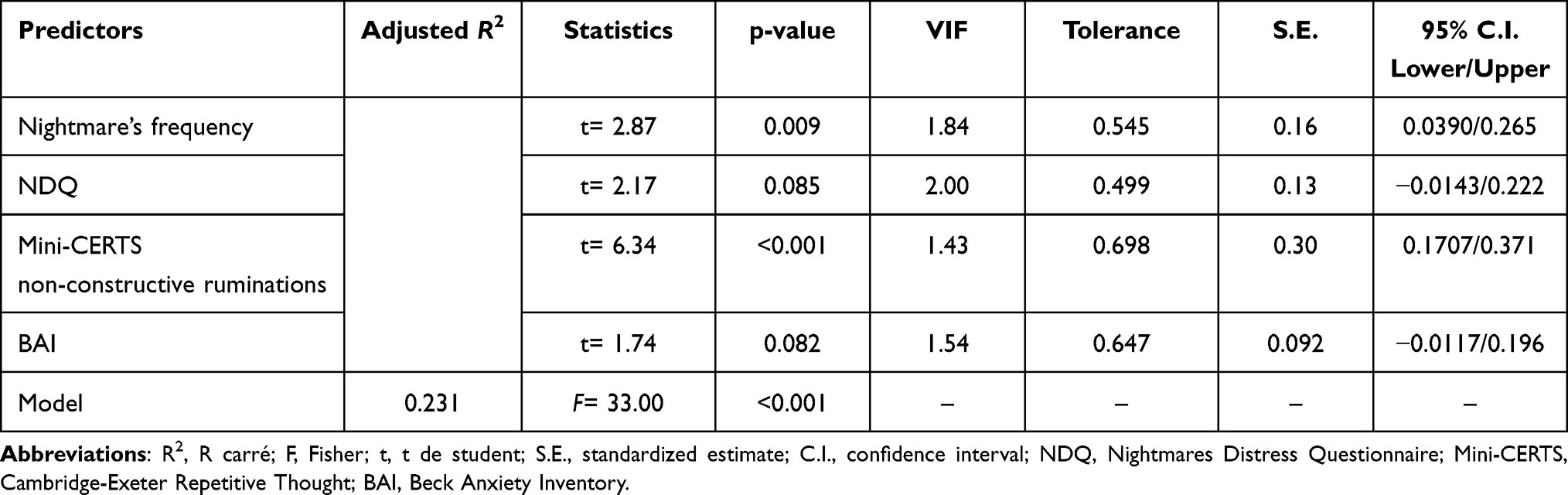 |
Table 6 Predicting SBQR Total Score from Clinical Variables (Nightmare’s Frequency, NDQ, Mini-CERTS and BAI) |
Results of the mediation analysis for the relation between anxiety and suicidal ideation are summarized in Figure 1. Unadjusted for covariates, the total effect of anxiety on suicidal risk was significant. The mediational analysis indicated that all the total indirect effect and all specific indirect effects were significant. First, the anxiety score also showed a significant indirect effect on SBQR score mediated by the non-constructive ruminations score (Mini-CERTS) (Estimate = 0.0513, I.C 95% [0.0339–0.0687], Z=5.77, p.<0.001) with an indirect effect of 48%. The Sobel test confirmed a mediating effect of the non-constructive ruminations (Z=5.86 p<0.001). The anxiety score showed a significant indirect effect on SBQ-R score mediated by the frequency of nightmares (Estimate = 0.0353, I.C 95% [0.0207–0.0498], Z=4.76, p.<0.001) with an indirect effect of 32.9%. The Sobel test shows a trend in the mediator effect (Z=1.60, p=0.10). The anxiety score also showed a significant indirect effect on SBQR score mediated by the Nightmare’s distress (Estimate = 0.0396, I.C 95% [0.0232–0.0561], Z=4.72, p.<0.001) with an indirect effect of 37%. The Sobel test confirmed a mediating effect of the BAI total score (Z=4.359, p<0.001). The result of the moderation analysis is presented in Figure 1. We evaluated the effect of the non-constructive ruminations on suicidal risk at different levels of insomnia. Results show a significant negative (reversed items) effect (Average-Estimate = 0.0217, [0.0388–0.0447], Z=7.42, p.<0.001).




Discussion
The aim of the present study was to determine the specifics of the relationship between nightmares and suicidal risk. First, we aimed to measure the impact of non-constructive ruminations on suicide risk and sleep disorders linked to the anxiety level. Non-constructive ruminations are defined as a non-constructive mode of thinking about the causes and consequences of one’s mood or condition in the abstract; they focus on past and future events rather than on the present moment.20 Research has examined the role of ruminations in the nightmare-suicide risk relationship without distinguishing constructive from non-constructive ruminations. Firstly, non-constructive ruminations were seen to be positively correlated with suicidal risk, nightmare frequency, nightmare distress and insomnia. Our results are in line with the literature.21,32 Secondly, in our linear regression model, non-constructive ruminations appear to be significantly associated with suicidal risk. More specifically, this variable most influences suicidal risk when associated with nightmare frequency, nightmare distress and anxiety. Results show that non-constructive thoughts are associated with the frequency of nightmares and nightmare distress in explaining the suicidal risk (Table 4). These findings corroborate the literature. Research has highlighted the role of anxiety as a factor associated with both nightmares and suicidal risk.13 Indeed, it appears that nightmare distress mediates the link between anxiety and suicidal risk. Non-constructive ruminations also mediate this link. In addition, the scope of the mediation is important. Moreover, the Sobel test shows a trend in the mediator effect of the frequency of nightmares. We believe that perhaps the sample size does not allow us to confirm this mediation.
On the other hand, our results demonstrate a moderating effect of insomnia on the link between non-constructive ruminations and suicidal risk. To our knowledge, our study is the first to uncover these strong links between these variables. We can hypothesize that insomnia alters the process of memory suppression.23 This alteration would allow non-constructive ruminations to erupt into consciousness, thus generating an increase in anxiety and a deterioration in sleep quality.23,33,34 This vicious circle would then become a ground of vulnerability to suicidal risk in populations. In parallel, the frequency of nightmares and the distress linked to them would play a reinforcing role in the vicious circle, significantly increasing the risk of suicide.
Our results clearly show that nightmare frequency, distress and non-constructive ruminations are closely related to suicidal risk. These data highlight the interrelatedness of nightmares, insomnia, anxiety and non-constructive ruminations on suicide risk.
We hypothesize that those therapeutic treatments specifically targeting non-constructive ruminations, nightmares and insomnia are important avenues of research to reduce suicide risk in vulnerable populations. Intrusive thought exposure approaches have been shown to be effective in anxiety and depressive syndromes35 and a better understanding of the role of non-constructive rumination would enhance the therapeutic effectiveness of CBT on nightmares.36
We suggest that future research should confirm our results especially in a psychiatric population. It would be interesting to examine the importance of these factors in relation to the psychiatric disorder groups most at risk, such as thymic, psychotic or personality disorders. Furthermore, another promising area of research would be to explore the links between interoception, rumination, sleep and sleep disorders and suicide risk. On the other hand, a better understanding of the influence of conscious nightmare recall on the cognitive and emotional functioning of individuals seems important. The current study has some limitations that need to be taken into account. The major limitation of this study is the self-selection bias generated by the online survey. However, the data seems to be consistent with previous studies evaluating similar variables and also using online survey.37,38 Another limitation is that our sample is not gender equivalent. Indeed, our population was overwhelmingly female. Studies tend to show that women are more vulnerable to nightmares.39 However, suicide risk has a gender-specific profile.40 For this reason, the data from our study cannot be considered as representative of the general population. Finally, no psychometric test was used to assess the frequency of nightmares. We aimed to take a more comprehensive approach by considering this frequency over a period of 3 months instead of 1 month. As pointed out in Robert’s study,41 a prospective measurement (narrative diaries and checklists) would have allowed a more precise measurement of the frequency of nightmares. However, extending this retrospective measure to a 3-month period, rather than a 1-month period, would be the closest to capture the reality of the participants’ experience of nightmares. In conclusion, this study highlights the complex links between sleep disorders, nightmares, non-constructive ruminations and suicidal risk. More specifically, our results suggest that non-constructive ruminations mediate the link between anxiety and suicidal risk and that insomnia would be a moderator of the link between non-constructive ruminations and suicidal risk. We believe that highlighting these relationships can serve to better understand suicidal risk and, to a certain extent, help in the construction of new therapeutic tools.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Preventing suicide, a global imperative; 2014.
2. Turecki G, Brent DA, Gunnell D, et al. Suicide and suicide risk. Nat Rev Dis Primers. 2019;5(1):74. doi:10.1038/s41572-019-0121-0
3. Cao J, Chen JM, Kuang L, et al. Abnormal regional homogeneity in young adult suicide attempters with no diagnosable psychiatric disorder: a resting state functional magnetic imaging study. Psychiatry Res. 2015;231(2):95–102. doi:10.1016/j.pscychresns.2014.10.011
4. De Leo D, Draper BM, Snowdon J, et al. Suicides in older adults: a case-control psychological autopsy study in Australia. J Psychiatr Res. 2013;47(7):980–988. doi:10.1016/j.jpsychires.2013.02.009
5. Galfalvy H, Haghighi F, Hodgkinson C, et al. A genome-wide association study of suicidal behavior. Am J Med Genet B Neuropsychiatr Genet. 2015;168(7):557–563. doi:10.1002/ajmg.b.32330
6. Fernquist RM. Gender equality and the sex differential in suicide rates using gender-age standardized data. Arch Suicide Res. 1999;5:255–260. doi:10.1080/13811119908258336
7. Andrews S, Hanna P. Investigating the psychological mechanisms underlying the relationship between nightmares, suicide and self-harm. Sleep Med Rev. 2020;54:101352. doi:10.1016/j.smrv.2020.101352
8. Bernert RA, Joiner TE. Sleep disturbances and suicide risk: a review of the literature. Neuropsychiatr Dis Treat. 2007;3(6):735–743. doi:10.2147/ndt.s1248
9. Bernert RA, Kim JS, Iwata NG, et al. Sleep disturbances as an evidence-based suicide risk factor. Curr Psychiatry Rep. 2015;17(3). doi:10.1007/s11920-015-0554-4
10. Drapeau CW, Nadorff MR. Suicidality in sleep disorders: prevalence, impact, and management strategies. Nat Sci Sleep. 2017;9:213–226. doi:10.2147/NSS.S125597
11. APA. Diagnostic and Statistical Manual of Mental Disorders.
12. Harris LM, Huang X, Linthicum KP, et al. Sleep disturbances as risk factors for suicidal thoughts and behaviours: a meta-analysis of longitudinal studies. Sci Rep. 2020;10(1):13888. doi:10.1038/s41598-020-70866-6
13. Lancee J, Schrijnemaekers NCML. The association between nightmares and daily distress. Sleep Biol Rhythms. 2013;11:14–19. doi:10.1111/j.1479-8425.2012.00586.x
14. Lee R, Suh S. Nightmare distress as a mediator between nightmare frequency and suicidal ideation. Dreaming. 2016;26:308–318. doi:10.1037/drm0000039
15. Littlewood DL, Gooding PA, Panagioti M, et al. Nightmares and suicide in posttraumatic stress disorder: the mediating role of defeat, entrapment, and hopelessness. J Clin Sleep Med. 2016;12(3):393–399. doi:10.5664/jcsm.5592
16. Russell K, Rasmussen S, Hunter SC. Insomnia and nightmares as markers of risk for suicidal ideation in young people: investigating the role of defeat and entrapment. J Clin Sleep Med. 2018;14(5):775–784. doi:10.5664/jcsm.7104
17. Suh S, Schneider M, Lee R, et al. Perceived interpersonal burdensomeness as a mediator between nightmare distress and suicidal ideation in nightmare sufferers. Front Psychol. 2016;7:1805. doi:10.3389/fpsyg.2016.01805
18. Nadorff MR, Anestis MD, Nazem S, et al. Sleep disorders and the interpersonal-psychological theory of suicide: independent pathways to suicidality? J Affect Disord. 2014;152–154:505–512. doi:10.1016/j.jad.2013.10.011
19. Golding S, Nadorff MR, Winer ES, et al. Unpacking sleep and suicide in older adults in a combined online sample. J Clin Sleep Med. 2015;11(12):1385–1392. doi:10.5664/jcsm.5270
20. Watkins ER. Constructive and unconstructive repetitive thought. Psychol Bull. 2008;134(2):163–206. doi:10.1037/0033-2909.134.2.163
21. Rogers ML, Schneider ME, Tucker RP, et al. Overarousal as a mechanism of the relation between rumination and suicidality. J Psychiatr Res. 2017;92:31–37. doi:10.1016/j.jpsychires.2017.03.024
22. Slavish DC, Graham-Engeland JE. Rumination mediates the relationships between depressed mood and both sleep quality and self-reported health in young adults. J Behav Med. 2014;38(2):204–213. doi:10.1007/s10865-014-9595-0
23. Harrington MO, Cairney SA. Sleep loss gives rise to intrusive thoughts. Trends Cogn Sci. 2021;25(6):434–436. doi:10.1016/j.tics.2021.03.001
24. Nadorff MR, Titus CE, Pate AR. A meaningful step toward understanding the cause and impact of nightmares. J Clin Sleep Med. 2019;15(2):179–180. doi:10.5664/jcsm.7608
25. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory–II. San Antonio, TX: Psychological Corporation; 1996.
26. Douilliez C, Heeren A, Lefèvre N, et al. [Validation of the French version of a questionnaire that evaluates constructive and nonconstructive repetitive thoughts]. Can J Behav Sci. 2014;46:185–192. French. doi:10.1037/a0033185
27. Osman A, Bagge CL, Gutierrez PM, et al. The suicidal behaviors questionnaire-revised (SBQ-R): validation with clinical and nonclinical samples. Assessment. 2001;8(4):443–454. doi:10.1177/107319110100800409
28. Böckermann M, Gieselmann A, Pietrowsky R. What does nightmare distress mean? Factorial structure and psychometric properties of the Nightmare Distress Questionnaire (NDQ). Dreaming. 2014;24(4):279–289. doi:10.1037/a0037749
29. Beck AT, Epstein N, Brown G, et al. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893–897. doi:10.1037//0022-006x.56.6.893
30. Bayard S, Lebrun C, Maudarbocus KH, et al. Validation of a French version of the sleep condition indicator: a clinical screening tool for insomnia disorder according to DSM-5 criteria. J Sleep Res. 2017;26(6):702–708. doi:10.1111/jsr.12556
31. Sawilowsky S. New effect size rules of thumb. J Mod Appl Stat Methods. 2009;8(2):467–474. doi:10.22237/jmasm/1257035100
32. Hedström AK, Bellocco R, Hössjer O, et al. The relationship between nightmares, depression and suicide. Sleep Med. 2021;77:1–6. doi:10.1016/j.sleep.2020.11.018
33. Bentley KH, Franklin JC, Ribeiro JD, et al. Anxiety and its disorders as risk factors for suicidal thoughts and behaviors: a meta-analytic review. Clin Psychol Rev. 2016;43:30–46. doi:10.1016/j.cpr.2015.11.008
34. Hobson JA, Gott JA, Friston KJ. Minds and brains, sleep and psychiatry. Psychiatr Res Clin Pract. 2021;3:12–28. doi:10.1176/appi.prcp.20200023
35. Janssen M, Heerkens Y, Kuijer W, et al. Effects of mindfulness-based stress reduction on employees’ mental health: a systematic review. PLoS One. 2018;13(1):e0191332. doi:10.1371/journal.pone.0191332
36. Lancee J, Spoormaker VI, Krakow B, et al. A systematic review of cognitive-behavioral treatment for nightmares: toward a well-established treatment. J Clin Sleep Med. 2008;4(5):475–480. doi:10.5664/jcsm.27285
37. Solomonova E, Picard-Deland C, Rapoport I, et al. Stuck in a lockdown: dreams, bad dreams, nightmares, and their relationship to stress, depression and anxiety during the COVID-19 pandemic. PLoS One. 2021;16(11):e0259040. doi:10.31234/osf.io/hbm84
38. Jiang W, Ren Z, Yu L, et al. A network analysis of post-traumatic stress disorder symptoms and correlates during the COVID-19 pandemic. Front Psychiatry. 2020;11:568037. doi:10.3389/fpsyt.2020.568037
39. Schredl M, Göritz AS. Nightmare frequency and feminine and masculine sex roles: an online survey. Dreaming. 2021;31(2):164–172. doi:10.1037/drm0000162
40. Hawton K. Sex and suicide. Gender differences in suicidal behaviour. Br J Psychiatry. 2000;177:484–485. doi:10.1192/bjp.177.6.484
41. Robert G, Zadra A. Measuring nightmare and bad dream frequency: impact of retrospective and prospective instruments. J Sleep Res. 2008;17(2):132–139. doi:10.1111/j.1365-2869.2008.00649.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.