Back to Journals » Journal of Inflammation Research » Volume 19
Nomogram for Predicting Pancreatic Pseudocyst in Hypertriglyceridemic Acute Pancreatitis: A Retrospective Cohort Study
Authors Qi R, Zhong J, Wang H, Li J, Xu J, Yang M, Luo R, Liu Z, Wang H, Cheng L
Received 11 January 2026
Accepted for publication 18 March 2026
Published 9 April 2026 Volume 2026:19 590773
DOI https://doi.org/10.2147/JIR.S590773
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Nadia Andrea Andreani
Rui Qi,1,* Jinzhi Zhong,1,* Hebin Wang,1,* Jing Li,1 Jie Xu,1 Maohui Yang,1 Renying Luo,1 Zuofeng Liu,1 Hao Wang,2,3 Lve Cheng1
1Department of Hepatobiliary Surgery, Affiliated Hospital of Panzhihua University, Panzhihua Hospital of Integrated Traditional Chinese and Western Medicine, Panzhihua, Sichuan, People’s Republic of China; 2Department of Hepatobiliary Surgery, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, Chongqing, People’s Republic of China; 3Department of Hepatobiliary Surgery, The First People’s Hospital of Xianyang City, Xianyang, Shaanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hao Wang, Department of Hepatobiliary Surgery, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, Chongqing, People’s Republic of China, Tel +86-18292929180, Fax +86-23-62887542, Email [email protected] Lve Cheng, Department of Hepatobiliary Surgery, Affiliated Hospital of Panzhihua University, Panzhihua Hospital of Integrated Traditional Chinese and Western Medicine, Panzhihua, 617000, People’s Republic of China, Tel +86-17308147679, Fax +86-812-2213090, Email [email protected]
Purpose: Pancreatic pseudocyst (PPC) is a relatively common local complication of hypertriglyceridemic acute pancreatitis (HTG-AP), frequently associated with prolonged hospital stay and potentially increased need for minimally invasive intervention. However, there is currently no established PPC prediction tool based on early admission indicators for HTG-AP patients.
Patients and Methods: In this retrospective study, 684 HTG-AP patients from January 2017 to January 2025 were included. All the patients were divided into training and validation sets in a 7:3 ratio. The least absolute shrinkage and selection operator regression was utilized for preliminary screening of predictive factors in the training set. Then, multivariate logistic regression was applied to identify potential factors for nomogram construction.
Results: A total of 684 patients were included, with an overall PPC incidence of 15.7%. The model incorporated three predictors: systemic inflammatory response syndrome (SIRS) (odds ratio [OR] = 2.263, 95% confidence interval [CI]: 1.283– 3.991, p = 0.005), C-reactive protein (CRP) (OR = 1.019, 95% CI: 1.013– 1.026, p < 0.001), and lactate (OR = 3.219, 95% CI: 2.182– 4.749, p < 0.001). The nomogram showed good discrimination, with an area under the curve (AUC) of 0.816 (95% CI: 0.759– 0.869) in the training cohort and 0.760 (95% CI: 0.658– 0.854) in the validation cohort. Calibration performance was acceptable, with calibration slopes of 1.000 and 0.773 and Brier scores of 0.100 and 0.108 in the training and validation cohorts, respectively. Decision curve analysis further demonstrated positive net clinical benefit in both cohorts.
Conclusion: SIRS, CRP, and lactate may be associated with the occurrence of PPC in patients with HTG-AP and may have value for early risk assessment. We developed a nomogram for PPC risk stratification in this population; however, further external validation is needed to confirm its generalizability and potential clinical utility.
Keywords: hypertriglyceridemic acute pancreatitis, pancreatic pseudocyst, risk factor, nomogram
Introduction
Hypertriglyceridemic acute pancreatitis (HTG-AP) is an acute inflammatory process of the pancreas induced by severe hypertriglyceridemia.1 Recent studies suggest that its incidence has increased, particularly in regions with a high prevalence of metabolic diseases.2–5 Although most individuals with hypertriglyceridemia are asymptomatic, HTG-AP often has a more abrupt onset and may follow a more severe course than acute pancreatitis of other causes.1,6,7 In the context of the increasing burden of metabolic diseases, refined risk stratification and individualized management of patients with HTG-AP have therefore become key issues in clinical practice.
Pancreatic pseudocyst (PPC) is a relatively common local complication of acute pancreatitis.8 During acute pancreatitis, acinar damage and peripancreatic fat necrosis can disrupt the main pancreatic duct or its branches, and persistent leakage with ongoing inflammation may lead to an encapsulated cystic lesion with a fibrous wall.9 PPC has been reported in approximately 10%–26% of patients with acute pancreatitis.10 Among these, about 40%–50% may resolve spontaneously under close conservative management.11 PPCs that persist, enlarge, or become complicated by infection, bleeding, or rupture generally require endoscopic or surgical drainage and have been associated with longer hospitalization and increased healthcare burden.12
Compared with gallstone- or alcohol-induced acute pancreatitis, HTG-AP is often characterized by significantly elevated serum triglyceride levels and associated metabolic disturbances.13,14 Current experimental and clinical evidence suggests that a key pathophysiological feature of HTG-AP is closely linked to the hydrolysis of large amounts of triglycerides within the pancreas and peripancreatic tissues by pancreatic lipase, leading to high concentrations of free fatty acids (FFAs).15–18 In severe hypertriglyceridemia, FFAs contribute to acinar cell injury and necrosis, partly by triggering intracellular Ca2⁺ overload, mitochondrial dysfunction, and oxidative stress;16,18 in addition, triglyceride-rich lipoproteins and FFAs may increase blood viscosity and promote vascular endothelial injury, thereby contributing to impaired pancreatic microcirculatory perfusion.16,19 Furthermore, during HTG-AP, necrosis of peripancreatic and visceral fat can release large amounts of unsaturated fatty acids, which may further amplify local and systemic inflammation. Increased visceral fat volume is associated with greater disease severity and a higher risk of local complications in acute pancreatitis.20–24 High triglyceride levels are also frequently accompanied by subclinical pancreatic injury and have been proposed to promote chronic ductal inflammation and structural remodeling, potentially predisposing patients to ductal disruption and persistent peripancreatic fluid collections during acute exacerbations.25,26 These mechanisms contribute to the increased propensity of patients with HTG-AP to develop peripancreatic fluid collections, PPC, and other delayed local structural complications.
Although the management of acute pancreatitis has improved over time, early identification of patients at increased risk of PPC remains challenging, particularly in those with HTG-AP. Risk stratification based on clinical and laboratory variables available within 24 hours of admission may facilitate closer monitoring, more individualized follow-up, and earlier clinical decision-making. Predictive nomograms are increasingly used in clinical medicine as practical tools for individualized risk estimation, because they integrate multiple predictors into an intuitive visual model that may facilitate risk stratification and support personalized clinical decision-making. To the best of our knowledge, no nomogram has yet been specifically developed for the early prediction of PPC in patients with HTG-AP using admission-day clinical and laboratory biomarkers. Therefore, this study aimed to develop and validate an early prediction nomogram for PPC in hospitalized patients with HTG-AP.
Material and Methods
Patients
This single-center retrospective cohort study included HTG-AP patients hospitalized at the Affiliated Hospital of Panzhihua University between January 2017 and January 2025. The patient selection process is shown in Figure 1. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Affiliated Hospital of Panzhihua University (Approval No. 2022-10-027). Written informed consent for participation was obtained from all patients. This study is reported in accordance with the RECORD guidelines.
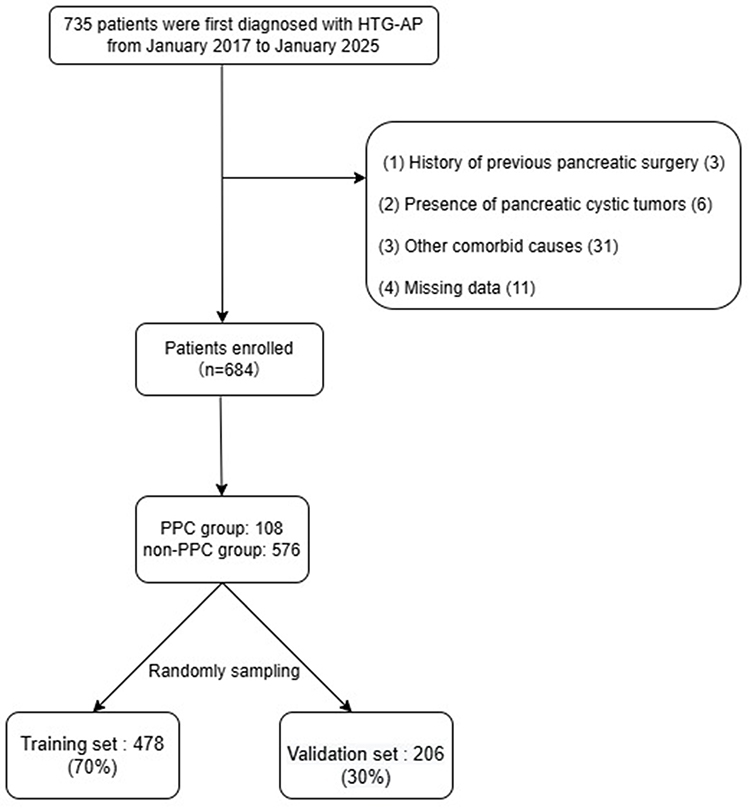 |
Figure 1 Flowchart of the study. Abbreviations: PPC, pancreatic pseudocyst; HTG-AP, hypertriglyceridemic acute pancreatitis. |
The inclusion criteria were: (a) age ≥ 18; (b) first episode of acute pancreatitis, diagnosed according to the 2012 revised Atlanta criteria; (c) etiology considered to be HTG-AP; (d) clearly documented time of symptom onset, with an interval of ≤ 72 h from onset to admission at our hospital; (e) completion of standardized baseline laboratory tests within 24 h after admission at our hospital; (f) at least one abdominal CT or MRI performed within 7 days of symptom onset at our hospital; and (g) at least one follow-up abdominal CT or MRI performed ≥ 4 weeks after symptom onset during follow-up for the index episode at our hospital.
The exclusion criteria were: (a) prior diagnosis of chronic pancreatitis or recurrent acute pancreatitis, history of severe pancreatic trauma, or previous pancreatic surgery; (b) concomitant pancreatic cystic neoplasm; (c) acute pancreatitis attributable to biliary, alcohol-related, surgery-related, or drug-induced causes, or cases with mixed or disputed etiologies; (d) unknown time of symptom onset, or first CT/MRI examination at our hospital demonstrating mature cystic lesions; (e) no follow-up abdominal CT or MRI ≥ 4 weeks after symptom onset during follow-up for the index episode at our hospital; (f) pregnancy, lactation, or concomitant malignancy; and (g) incomplete or missing key clinical or imaging data.
Definitions
Acute pancreatitis was diagnosed according to the 2012 revised Atlanta classification.27 The diagnosis requires at least two of the following three features: (1) acute onset of persistent upper abdominal pain radiating to the back; (2) serum amylase and/or lipase levels ≥ three times the upper limit of normal; and (3) characteristic imaging findings of acute pancreatitis affecting the pancreas and/or peripancreatic tissues (contrast-enhanced CT, MRI, or abdominal ultrasonography).
In patients meeting the above diagnostic criteria for acute pancreatitis, HTG-AP was defined according to criteria commonly used in recent systematic reviews and multicenter cohort studies:7,28–30 (1) serum triglyceride (TG) level ≥ 11.3 mmol/L (1000 mg/dL) measured shortly after symptom onset, or TG level of 5.6–11.3 mmol/L (500–1000 mg/dL) with lactescent serum; (2) no alternative etiologies sufficient to explain the episode of pancreatitis were found based on medical history, physical examination, and imaging, such as common bile duct stones, alcohol use, ERCP-related pancreatitis, or drug-induced pancreatitis; and (3) consensus judgment by two senior pancreatology specialists that hypertriglyceridemia was the primary or an important contributing etiologic factor.
The primary outcome was the occurrence of PPC during follow-up. PPC was defined according to the revised Atlanta classification and subsequent imaging descriptions of local complications, including only de novo lesions arising after the index HTG-AP episode. The diagnostic criteria were:27,31–33 (1) a local complication developing ≥ 4 weeks after the onset of the index HTG-AP episode; (2) a round or ovoid cystic lesion located in the pancreas and/or peripancreatic region, with predominantly homogeneous fluid content on contrast-enhanced CT, MRI, or endoscopic ultrasonography; (3) complete encapsulation by a well-defined wall of granulation and fibrous tissue, without an epithelial lining; and (4) absence, or only a minimal amount, of non-liquid necrotic material within the cavity, such that the lesion did not meet the imaging criteria for walled-off necrosis.
Data Collection
Throughout the study period, the management strategy for HTG-AP patients at our center remained consistent, primarily guided by national and international guidelines for acute pancreatitis and HTG-AP, along with standardized institutional protocols. Diagnostic and therapeutic decisions were made by an experienced pancreas team within these guidelines. After the acute phase, HTG-AP patients were routinely advised to undergo follow-up contrast-enhanced abdominal CT or MRI 4–6 weeks after symptom onset to evaluate recovery and prognosis. All imaging exams in the analysis were reviewed independently by two senior radiologists blinded to the study data. Discrepancies were resolved by discussion and consensus.
The main variables collected were: (a) demographic and clinical characteristics, including age, sex, body mass index (BMI), history of diabetes, hypertension, smoking, alcohol use, and presence of systemic inflammatory response syndrome (SIRS) within 24 h of admission; and (b) laboratory parameters within 24 h of admission, including hemoglobin, uric acid, white blood cell count and absolute neutrophil count, platelet count, alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, total bilirubin, direct bilirubin, total protein, albumin, serum calcium, serum creatinine, blood glucose, triglycerides, C-reactive protein (CRP), and arterial blood lactate.
Model Development
The occurrence of PPC during follow-up was the outcome variable, with clinical and laboratory parameters within 24 hours of admission as candidate predictors for early PPC risk stratification in HTG-AP patients. Patients with incomplete or missing key clinical or imaging data were excluded, and the final analysis was therefore based on a complete-case approach without imputation. Eligible patients were randomly assigned to the training and validation cohorts in a 7:3 ratio using simple random sampling. The model was developed in the training cohort and validated in the validation cohort. In the training cohort, least absolute shrinkage and selection operator (LASSO) logistic regression was performed for preliminary variable selection. The tuning parameter (lambda) was determined using 10-fold cross-validation with binomial deviance as the criterion, and lambda.1se was selected as the penalty parameter to obtain a more parsimonious model and reduce the risk of overfitting. Predictors with non-zero coefficients at the selected lambda value were then entered into a multivariable logistic regression model to identify independent predictors of PPC and construct the corresponding nomogram. Model performance was evaluated in both cohorts using receiver operating characteristic (ROC) curve analysis and the area under the curve (AUC). Calibration was assessed using calibration plots, calibration slope, intercept, and Brier score, and decision curve analysis (DCA) was performed to evaluate the clinical utility and net benefit of the nomogram across different threshold probabilities.
Statistical Analysis
Statistical analyses were performed using R (version 4.3.0) and SPSS (version 26.0). Categorical variables were presented as frequency and percentage and compared with the chi-square test. Continuous variables with a normal distribution were expressed as mean ± standard deviation and compared with the Student’s t-test. For continuous variables not following a normal distribution, data were presented as median (interquartile range) and compared with the Mann–Whitney U-test. A p-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
From January 2017 to January 2025, our hospital treated 735 patients meeting the diagnostic criteria for HTG-AP. After applying the inclusion and exclusion criteria, 684 patients were included in the analysis (Figure 1). Among the cohort, 108 patients developed PPC during follow-up, with an incidence rate of 15.7%. Of the cohort, 478 patients were assigned to the training set for model development, and 206 patients to the validation set for performance evaluation.
In the training set, 75 patients developed PPC. The PPC group showed significant differences in baseline characteristics compared to the non-PPC group, including higher white blood cell count, total protein, CRP, lactate levels within 24 hours of admission, and higher incidence of SIRS. Other variables were similar between the two groups (Table 1).
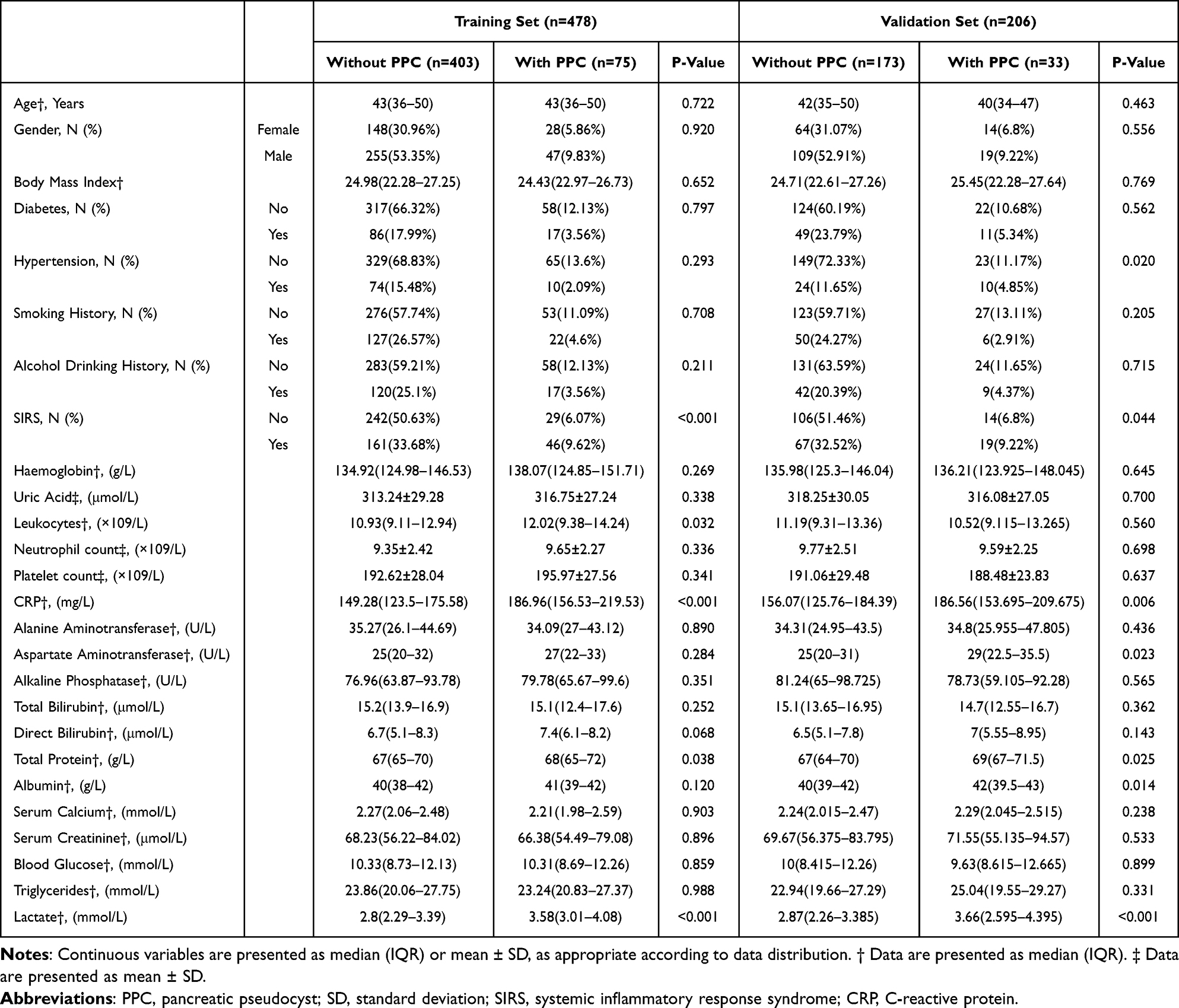 |
Table 1 Baseline Characteristics of Patients with and without Pancreatic Pseudocyst in the Training and Validation Sets |
Variable Selection and Nomogram Construction
In the training set, LASSO regression was used to select candidate predictors, and three key variables were ultimately retained (Figure 2): SIRS, CRP, and lactate. These variables were subsequently entered into a multivariable logistic regression model. The results showed that SIRS (odds ratio [OR] = 2.263, 95% confidence interval [CI]: 1.283–3.991, p = 0.005), CRP (OR = 1.019, 95% CI: 1.013–1.026, p < 0.001), and lactate (OR = 3.219, 95% CI: 2.182–4.749, p < 0.001) were all independently associated with PPC (Table 2). Based on the multivariable logistic regression model, a nomogram was constructed to predict the risk of PPC in patients with HTG-AP (Figure 3).
 |
Table 2 Multivariable Logistic Regression Analysis for Predictors of Pancreatic Pseudocyst in the Training Cohort |
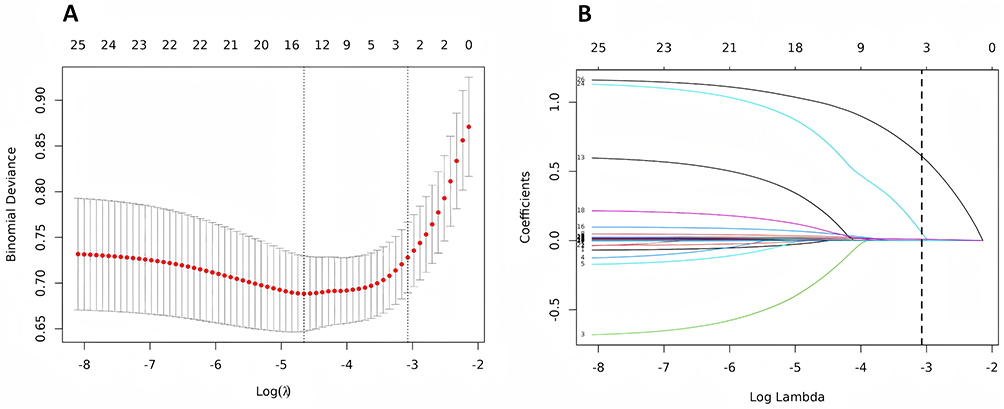 |
Figure 2 LASSO regression for predictor selection. (A) Cross-validation curve of the LASSO regression analysis; (B) Coefficient path plot of the candidate risk variables. |
 |
Figure 3 Nomogram for predicting the risk of pancreatic pseudocyst in patients with hypertriglyceridemic acute pancreatitis. |
Performance of the Prediction Nomogram
In the training cohort, the nomogram demonstrated good discrimination, with an AUC of 0.816 (95% CI, 0.759–0.869), while in the validation cohort the AUC was 0.760 (95% CI, 0.658–0.854) (Figure 4A and B). ROC comparison further showed that the nomogram yielded higher AUCs than each individual predictor alone in both cohorts. In the training cohort, the AUCs of SIRS, CRP, and lactate alone were 0.607 (95% CI, 0.545–0.669), 0.722 (95% CI, 0.651–0.793), and 0.738 (95% CI, 0.673–0.799), respectively. In the validation cohort, the corresponding AUCs were 0.594 (95% CI, 0.501–0.684), 0.651 (95% CI, 0.540–0.763), and 0.712 (95% CI, 0.601–0.813), respectively. Calibration performance was good in the training cohort and acceptable in the validation cohort. Specifically, in the training cohort, the calibration slope was 1.000 (95% CI, 0.778–1.295), the intercept was 0.000 (95% CI, −0.412 to 0.433), and the Brier score was 0.100; in the validation cohort, the calibration slope was 0.773 (95% CI, 0.475–1.171), the intercept was −0.332 (95% CI, −0.890 to 0.238), and the Brier score was 0.108 (Figure 4C and D). Decision curve analysis demonstrated that the nomogram yielded a positive net benefit over the treat-all and treat-none strategies across a clinically relevant range of threshold probabilities in both cohorts (Figure 4E and F).
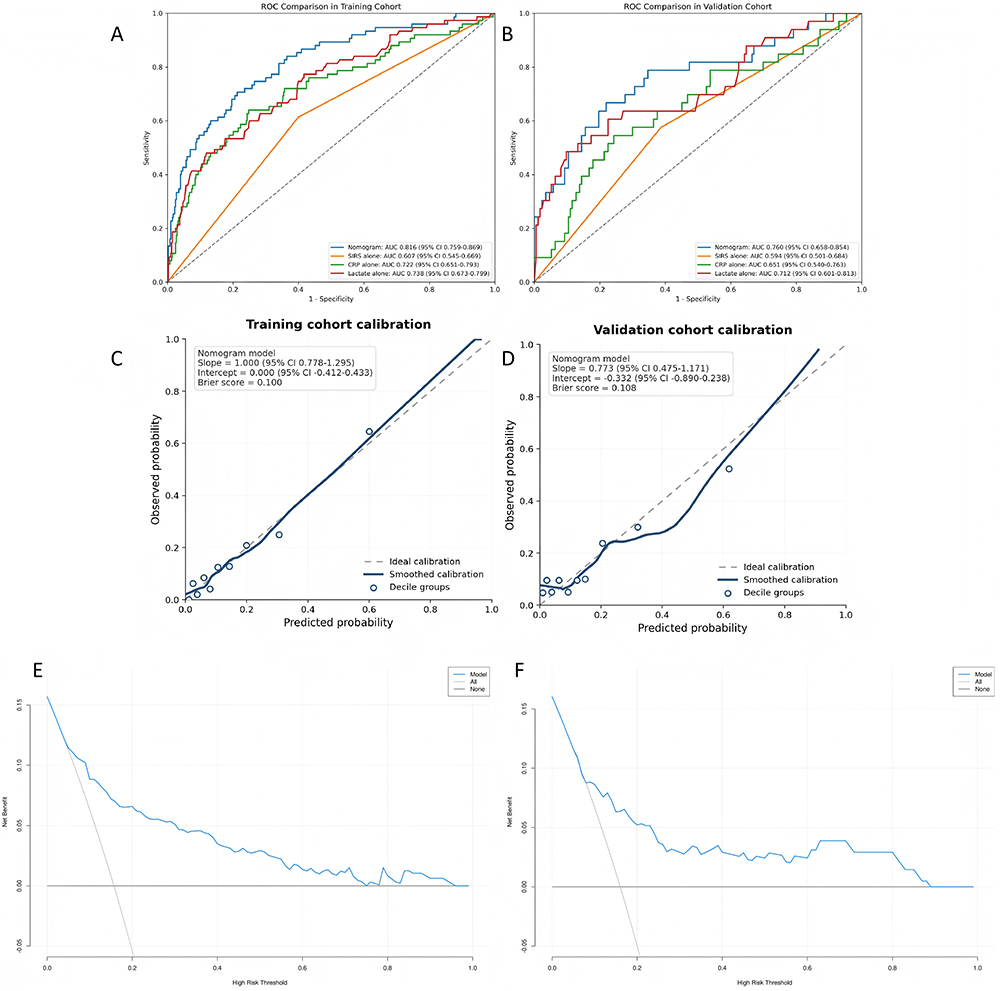 |
Figure 4 Performance of the nomogram for predicting the risk of pancreatic pseudocyst in patients with hypertriglyceridemic acute pancreatitis; (A) Receiver operating characteristic curves comparing the nomogram with SIRS alone, CRP alone, and lactate alone in the training cohort; (B) Receiver operating characteristic curves comparing the nomogram with SIRS alone, CRP alone, and lactate alone in the validation cohort; (C) Calibration curve in the training cohort; (D) Calibration curve in the validation cohort; (E) Decision curve analysis in the training cohort; (F) Decision curve analysis in the validation cohort. Abbreviation: AUC, area under the receiver operating characteristic curve. |
Discussion
We developed an early prediction model for PPC risk in patients with HTG-AP using clinical and laboratory parameters obtained within 24 hours of admission. SIRS, CRP, and lactate were identified as independent predictors and incorporated into the final model. The model showed favorable performance in the training cohort and acceptable performance in the validation cohort, suggesting that it may have value for early risk stratification and follow-up planning in hospitalized patients with HTG-AP.
In recent years, metabolic abnormalities, particularly the relationship between elevated triglycerides and acute pancreatitis onset and severity, have gained increasing attention.17,28,34 Existing evidence suggests that in HTG-AP, elevated serum triglycerides are associated with excessive free fatty acid release, which can damage pancreatic acinar cells, induce oxidative stress, impair mitochondrial function, and exacerbate inflammation and injury.16,35 Hypertriglyceridemia and increased chylomicrons may also contribute to microcirculatory dysfunction in the pancreas, a common feature of HTG-AP.15,36 These mechanisms may worsen local pancreatic injury and increase fluid accumulation, influencing PPC development. Some studies have identified risk factors associated with PPC occurrence. Lu Hao et al found that age of onset, smoking, and severe acute pancreatitis were risk factors for PPC in chronic pancreatitis patients.37 Fengjie Ji et al suggested that markers like lactate dehydrogenase, hemoglobin, albumin, and calcium might be associated with PPC development in acute pancreatitis patients.38 However, most studies have not independently analyzed HTG-AP. This study developed a predictive model for early identification of high-risk HTG-AP patients using accessible clinical and laboratory data, filling a gap in HTG-AP prediction.
Previous studies suggest that HTG-AP may be associated with a more severe inflammatory response and higher complication risk compared to other causes of acute pancreatitis, and early SIRS presence is linked to more severe outcomes.13,39,40 SIRS is a systemic inflammatory response triggered by infectious or non-infectious insults, often manifesting early in acute pancreatitis.40,41 Mechanistically, SIRS contributes to PPC development through several pathways: pro-inflammatory mediators damage pancreatic acinar cells, immune cell infiltration exacerbates tissue damage, and microcirculatory disturbances promote fluid accumulation.40,42 When exudates are encapsulated by fibrous tissue, they may evolve into PPC. Stress-induced gluconeogenesis, associated with SIRS, can lead to hyperglycemia, increasing the metabolic burden on the pancreas and sustaining inflammation.43,44 In our cohort, early SIRS in HTG-AP patients was associated with a higher risk of subsequent PPC, aligning with these mechanisms and suggesting that close monitoring of SIRS may help identify patients at higher risk for local complications.
CRP is an acute-phase reactant synthesized by the liver. During acute pancreatitis (AP), CRP levels are a marker of systemic inflammation and significantly associated with disease severity.45,46 Several international consensus guidelines indicate that CRP >150 mg/L within 48 hours of admission is a warning sign for severe AP.47 Studies have also suggested that CRP >150 mg/L within 48–72 hours of AP onset may predict necrotizing pancreatitis with high sensitivity and specificity.48 A systematic review and meta-analysis by Wu et al found that CRP is an important biomarker for assessing AP severity.49 A prospective multicenter study by Cui et al showed that elevated CRP levels on admission may serve as an independent risk factor for pancreatic fluid accumulation after AP.50 Elevated CRP levels are often associated with an increased risk of local complications in AP patients.51 Clinical studies show that patients with peripancreatic fluid accumulation have higher CRP levels within 48 hours compared to those without;52 acute peripancreatic fluid collection is a precursor lesion for PPC formation.27 Although Solakoglu et al did not directly investigate PPC, they found that elevated CRP levels were closely associated with local pancreatic fluid accumulation and pseudocyst formation.52 Our study further confirms the significant correlation between CRP and the occurrence of PPC in HTG-AP patients, confirming CRP as a key biomarker for early PPC prediction.
Lactate is a byproduct of tissues under hypoxic or metabolic stress, reflecting tissue perfusion and metabolic status. Elevated lactate levels may indicate microcirculatory disturbances and tissue hypoxia.53 During the acute phase of AP, multi-organ dysfunction and pancreatic microcirculatory disturbances lead to tissue hypoxia, resulting in increased lactate levels.54 Elevated lactate is a marker of AP severity and may independently predict the risk of organ failure.54,55 A retrospective study by Shu et al of 329 patients found that AP patients with elevated lactate levels had higher incidences of pancreatic necrosis and multi-organ dysfunction than those with normal lactate levels.54 A prospective study by Xu et al showed that moderate to severe AP patients had significantly higher lactate levels than mild AP patients, and high lactate levels may independently predict organ failure occurrence.55 In HTG-AP patients, very high triglyceride levels may exacerbate peripancreatic fat necrosis and inflammation, promoting lactate production and worsening the condition.56 These findings are consistent with our observation that elevated lactate levels suggest an increased risk of PPC in HTG-AP patients, highlighting the clinical value of early lactate monitoring.
The nomogram proposed in this study is structurally simple and may be readily applied in the early clinical setting. Compared with single-parameter assessment and some conventional pancreatitis severity scoring approaches that incorporate multiple clinical and laboratory variables, this model may be easier to use at the bedside during the early stage of hospitalization.57,58 Clinical guidelines also emphasize the importance of early severity assessment in acute pancreatitis.27,59,60 Previous studies have shown that nomogram-based models can predict several clinically relevant outcomes in acute pancreatitis, including persistent organ failure, readmission, and mortality, supporting their use as practical tools for individualized risk assessment.61,62 Representative studies have reported favorable discrimination for nomograms predicting persistent organ failure on admission, 30-day readmission, and short-term mortality in acute pancreatitis.63–65 Against this background, our study extends the application of this type of predictive tool to the early prediction of pancreatic pseudocyst risk in patients with HTG-AP using variables available within 24 hours of admission. The predictive value of the nomogram may derive from the complementary information captured by SIRS, CRP, and lactate. SIRS reflects the systemic inflammatory response, CRP reflects the acute-phase inflammatory burden, and lactate may indicate tissue hypoperfusion and metabolic stress. Rather than suggesting a direct biological synergistic mechanism, the combination of these variables may reflect different pathophysiological dimensions associated with PPC development, thereby providing a more comprehensive basis for early risk assessment in patients with HTG-AP. Because all three variables are routinely available within 24 hours of admission, the nomogram may be incorporated into the early admission assessment workflow, either as part of a standardized admission form or through integration into an electronic medical record system. Patients identified as having elevated predicted risk may then undergo closer monitoring, more individualized follow-up planning, and earlier repeat imaging when clinically indicated. Early identification of high-risk patients may facilitate more individualized management and may ultimately contribute to improved clinical outcomes.66
This study has several limitations. First, as a single-center retrospective study, it is subject to potential selection bias and residual confounding, which may affect the robustness of the findings. Second, although the model showed acceptable performance in the validation cohort, the relatively wide confidence interval of the validation AUC indicates limited precision and suggests some uncertainty in model stability, likely related to the modest sample size and number of PPC events in the validation cohort. Third, the model has not yet been externally validated, and its generalizability requires further assessment in independent cohorts. Fourth, direct comparison with established composite clinical scores such as BISAP was not performed; therefore, the added value of the nomogram over existing scoring systems remains to be further evaluated. Finally, the model did not include potentially relevant variables such as pancreatic necrosis or ductal disruption, which may have limited its predictive performance. Future studies should validate and refine the model in larger, multicenter, prospective cohorts with broader clinical variables to improve its generalizability and clinical applicability.
Conclusion
This study suggests that SIRS, CRP, and lactate may be associated with the development of PPC in patients with HTG-AP and may contribute to early risk assessment. Based on these factors, we developed an early prediction model for PPC risk stratification in this population. Although the model showed potential clinical value, further external validation is required to establish its generalizability and support its broader use in clinical practice.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Lve Cheng, upon reasonable request.
Ethics Approval and Informed Consent
Written informed consent was obtained from all participants. Individuals cannot be identified based on the data presented. We declare to ensure the confidentiality of patient data. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Affiliated Hospital of Panzhihua University (Approval No. 2022-10-027). This study is reported in accordance with the RECORD guidelines.
Author Contributions
Rui Qi: Conceptualization, Data Curation, Formal Analysis, Investigation, Methodology, Validation, Visualization, and Writing—Original Draft. Jinzhi Zhong: Formal Analysis, Methodology, Resources, Software, Validation, and Writing—Review & Editing. Hebin Wang: Methodology, Project Administration, Resources, Software, and Writing—Review & Editing. Jing Li: Conceptualization, Methodology, Project Administration, Resources, Software, Supervision, and Writing—Review & Editing. Jie Xu: Conceptualization, Data Curation, Formal Analysis, Supervision, and Writing—Review & Editing. Maohui Yang: Conceptualization, Project Administration, Supervision, and Writing—Review & Editing. Renying Luo: Conceptualization, Formal Analysis, Supervision, and Writing—Review & Editing. Zuofeng Liu: Conceptualization, Supervision, and Writing—Review & Editing. Hao Wang: Conceptualization, Project Administration, Supervision, Writing—Original Draft, and Writing—Review & Editing. Lve Cheng: Conceptualization, Project Administration, Supervision, Writing—Original Draft, and Writing—Review & Editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Key Laboratory of Characteristic Biomedicine of Panzhihua City (Grant No. 25TSSWYY0010) and the Affiliated Hospital of Panzhihua University (Grant No. PYYZ-2022-20).
Disclosure
The authors report no conflicts of interest in this work.
References
1. de Pretis N, Amodio A, Frulloni L. Hypertriglyceridemic pancreatitis: epidemiology, pathophysiology and clinical management. United European Gastroenterol J. 2018;6(5):649–12. doi:10.1177/2050640618755002
2. Lu J, Wang Z, Mei W, et al. A systematic review of the epidemiology and risk factors for severity and recurrence of hypertriglyceridemia-induced acute pancreatitis. BMC Gastroenterol. 2025;25(1):374. doi:10.1186/s12876-025-03954-4
3. Lin XY, Zeng Y, Zhang ZC, Lin ZH, Chen LC, Ye ZS. Incidence and clinical characteristics of hypertriglyceridemic acute pancreatitis: a retrospective single-center study. World J Gastroenterol. 2022;28(29):3946–3959. doi:10.3748/wjg.v28.i29.3946
4. Jin M, Bai X, Chen X, et al. A 16-year trend of etiology in acute pancreatitis: the increasing proportion of hypertriglyceridemia-associated acute pancreatitis and its adverse effect on prognosis. J Clin Lipidol. 2019;13(6):947–53.e1. doi:10.1016/j.jacl.2019.09.005
5. Fu ZH, Zhao ZY, Liang YB, et al. Impact of metabolic syndrome components on clinical outcomes in hypertriglyceridemia-induced acute pancreatitis. World J Gastroenterol. 2024;30(35):3996–4010. doi:10.3748/wjg.v30.i35.3996
6. Shafiq S, Patil M, Gowda V, Devarbhavi H. Hypertriglyceridemia-Induced Acute Pancreatitis - Course, Outcome, and Comparison with Non-Hypertriglyceridemia Associated Pancreatitis. Indian J Endocrinol Metab. 2022;26(5):459–464. doi:10.4103/ijem.ijem_206_22
7. Carr RA, Rejowski BJ, Cote GA, Pitt HA, Zyromski NJ. Systematic review of hypertriglyceridemia-induced acute pancreatitis: a more virulent etiology? Pancreatology. 2016;16(4):469–476. doi:10.1016/j.pan.2016.02.011
8. Chatila AT, Bilal M, Guturu P. Evaluation and management of acute pancreatitis. World J Clin Cases. 2019;7(9):1006–1020. doi:10.12998/wjcc.v7.i9.1006
9. Lerch MM, Stier A, Wahnschaffe U, Mayerle J. Pancreatic pseudocysts: observation, endoscopic drainage, or resection? Dtsch Arztebl Int. 2009;106(38):614–621. doi:10.3238/arztebl.2009.0614
10. Kluszczyk P, Tobiasz A, Madej A, Wosiewicz P, Mrowiec S, Jabłońska B. Pancreatic Pseudocysts: evolution of Treatment Approaches. J Clin Med. 2025;14(17):6152. doi:10.3390/jcm14176152
11. Koo JG, Liau MYQ, Kryvoruchko IA, Habeeb TA, Chia C, Shelat VG. Pancreatic pseudocyst: the past, the present, and the future. World J Gastrointest Surg. 2024;16(7):1986–2002. doi:10.4240/wjgs.v16.i7.1986
12. Tan JH, Zhou L, Cao RC, Zhang GW. Identification of risk factors for pancreatic pseudocysts formation, intervention and recurrence: a 15-year retrospective analysis in a tertiary hospital in China. BMC Gastroenterol. 2018;18(1):143. doi:10.1186/s12876-018-0874-z
13. Bálint ER, Fűr G, Kiss L, et al. Assessment of the course of acute pancreatitis in the light of aetiology: a systematic review and meta-analysis. Sci Rep. 2020;10(1):17936. doi:10.1038/s41598-020-74943-8
14. Adiamah A, Psaltis E, Crook M, Lobo DN. A systematic review of the epidemiology, pathophysiology and current management of hyperlipidaemic pancreatitis. Clin Nutr. 2018;37(6 Pt A):1810–1822. doi:10.1016/j.clnu.2017.09.028
15. Qiu M, Zhou X, Zippi M, et al. Comprehensive review on the pathogenesis of hypertriglyceridaemia-associated acute pancreatitis. Ann Med. 2023;55(2):2265939. doi:10.1080/07853890.2023.2265939
16. Guo YY, Li HX, Zhang Y, He WH. Hypertriglyceridemia-induced acute pancreatitis: progress on disease mechanisms and treatment modalities. Discov Med. 2019;27(147):101–109.
17. Rajalingamgari P, Khatua B, Summers MJ, et al. Prospective observational study and mechanistic evidence showing lipolysis of circulating triglycerides worsens hypertriglyceridemic acute pancreatitis. J Clin Invest. 2024;135(1). doi:10.1172/JCI184785.
18. Murphy MJ, Sheng X, MacDonald TM, Wei L. Hypertriglyceridemia and acute pancreatitis. JAMA Intern Med. 2013;173(2):162–164. doi:10.1001/2013.jamainternmed.477
19. Zhang Y, He W, He C, et al. Large triglyceride-rich lipoproteins in hypertriglyceridemia are associated with the severity of acute pancreatitis in experimental mice. Cell Death Dis. 2019;10(10):728. doi:10.1038/s41419-019-1969-3
20. Patel K, Trivedi RN, Durgampudi C, et al. Lipolysis of visceral adipocyte triglyceride by pancreatic lipases converts mild acute pancreatitis to severe pancreatitis independent of necrosis and inflammation. Am J Pathol. 2015;185(3):808–819. doi:10.1016/j.ajpath.2014.11.019
21. Higaki Y, Nishida T, Matsumoto K, et al. Effect of abdominal visceral fat on mortality risk in patients with severe acute pancreatitis. JGH Open. 2021;5(12):1357–1362. doi:10.1002/jgh3.12681
22. Noel P, Patel K, Durgampudi C, et al. Peripancreatic fat necrosis worsens acute pancreatitis independent of pancreatic necrosis via unsaturated fatty acids increased in human pancreatic necrosis collections. Gut. 2016;65(1):100–111. doi:10.1136/gutjnl-2014-308043
23. Zhu L, Yuan L, Wang T, et al. Relation between triglycerides and the severity of acute pancreatitis combined with nonalcoholic fatty liver disease: a retrospective study. BMC Gastroenterol. 2023;23(1):313. doi:10.1186/s12876-023-02951-9
24. Xie J, Xu L, Pan Y, et al. Impact of visceral adiposity on severity of acute pancreatitis: a propensity score-matched analysis. BMC Gastroenterol. 2019;19(1):87. doi:10.1186/s12876-019-1015-z
25. Ahmed Ali U, Issa Y, Hagenaars JC, et al. Risk of Recurrent Pancreatitis and Progression to Chronic Pancreatitis After a First Episode of Acute Pancreatitis. Clin Gastroenterol Hepatol. 2016;14(5):738–746. doi:10.1016/j.cgh.2015.12.040
26. Edmiston T, Vishnupriya K, Chanmugam A. Recurrent acute pancreatitis: a harbinger for irreversible chronic pancreatitis. Hosp Pract. 2024;52(1–2):5–12. doi:10.1080/21548331.2024.2348990
27. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
28. Mosztbacher D, Hanák L, Farkas N, et al. Hypertriglyceridemia-induced acute pancreatitis: a prospective, multicenter, international cohort analysis of 716 acute pancreatitis cases. Pancreatology. 2020;20(4):608–616. doi:10.1016/j.pan.2020.03.018
29. Fan Z, Zhang Y, Li J, et al. Global burden and characterization of hypertriglyceridemia-induced acute pancreatitis: results from a systematic review and a multi-center cohort study. Sci China Life Sci. 2025;68(10):3010–3020. doi:10.1007/s11427-024-2900-6
30. Edu AV, Pahomeanu MR, Ghiță AI, et al. Hypertriglyceridemia-Induced Acute Pancreatitis-The Milky Way Constellation-The Seven-Year Experience of a Large Tertiary Centre. Diagnostics (Basel). 2024;14(11). doi:10.3390/diagnostics14111105.
31. Zhu H, Du Y, Wang K, Li Z, Jin Z. Consensus guidelines on the diagnosis and treatment of pancreatic pseudocyst and walled-off necrosis from a Chinese multiple disciplinary team expert panel. Endosc Ultrasound. 2024;13(4):205–217. doi:10.1097/eus.0000000000000080
32. Tyberg A, Karia K, Gabr M, et al. Management of pancreatic fluid collections: a comprehensive review of the literature. World J Gastroenterol. 2016;22(7):2256–2270. doi:10.3748/wjg.v22.i7.2256
33. Zhao K, Adam SZ, Keswani RN, Horowitz JM, Miller FH. Acute Pancreatitis: revised Atlanta Classification and the Role of Cross-Sectional Imaging. AJR Am J Roentgenol. 2015;205(1):W32–41. doi:10.2214/AJR.14.14056
34. Pascual I, Sanahuja A, García N, et al. Association of elevated serum triglyceride levels with a more severe course of acute pancreatitis: cohort analysis of 1457 patients. Pancreatology. 2019;19(5):623–629. doi:10.1016/j.pan.2019.06.006
35. Cheng X, Zhan Y, Wang Z, et al. A single-center experience of non-bioartificial DFAPP support systems among Chinese patients with hyperlipidemic moderate/severe acute pancreatitis. Sci Rep. 2024;14(1):1128. doi:10.1038/s41598-024-51761-w
36. Kotan R, Peto K, Deak A, Szentkereszty Z, Nemeth N. Hemorheological and Microcirculatory Relations of Acute Pancreatitis. Metabolites. 2022;13(1):4. doi:10.3390/metabo13010004
37. Hao L, Pan J, Wang D, et al. Risk factors and nomogram for pancreatic pseudocysts in chronic pancreatitis: a cohort of 1998 patients. J Gastroenterol Hepatol. 2017;32(7):1403–1411. doi:10.1111/jgh.13748
38. Ji F, Tang W, Yan W, et al. A nomogram to predict the occurrence of pseudocyst in patients with acute pancreatitis. Pancreatology. 2024;24(6):863–869. doi:10.1016/j.pan.2024.08.007
39. Lu Z, Zhang G, Guo F, et al. Elevated triglycerides on admission positively correlate with the severity of hypertriglyceridaemic pancreatitis. Int J Clin Pract. 2020;74(3):e13458. doi:10.1111/ijcp.13458
40. Suzuki M, Sai JK, Shimizu T. Acute pancreatitis in children and adolescents. World J Gastrointest Pathophysiol. 2014;5(4):416–426. doi:10.4291/wjgp.v5.i4.416
41. Walkowska J, Zielinska N, Tubbs RS, Podgórski M, Dłubek-Ruxer J, Olewnik Ł. Diagnosis and Treatment of Acute Pancreatitis. Diagnostics (Basel). 2022;12(8). doi:10.3390/diagnostics12081974
42. Li J, Yang WJ, Huang LM, Tang CW. Immunomodulatory therapies for acute pancreatitis. World J Gastroenterol. 2014;20(45):16935–16947. doi:10.3748/wjg.v20.i45.16935
43. Yang X, Zhang R, Jin T, et al. Stress Hyperglycemia Is Independently Associated with Persistent Organ Failure in Acute Pancreatitis. Dig Dis Sci. 2022;67(5):1879–1889. doi:10.1007/s10620-021-06982-8
44. Sreedharan R, Khanna S, Shaw A. Perioperative glycemic management in adults presenting for elective cardiac and non-cardiac surgery. Perioper Med (Lond). 2023;12(1):13. doi:10.1186/s13741-023-00302-6
45. Skouras C, Zheng X, Binnie M, et al. Increased levels of 3-hydroxykynurenine parallel disease severity in human acute pancreatitis. Sci Rep. 2016;6:33951. doi:10.1038/srep33951
46. Li J, Chen Z, Li L, et al. Interleukin-6 is better than C-reactive protein for the prediction of infected pancreatic necrosis and mortality in patients with acute pancreatitis. Front Cell Infect Microbiol. 2022;12:933221. doi:10.3389/fcimb.2022.933221
47. Leppäniemi A, Tolonen M, Tarasconi A, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019;14(1):27. doi:10.1186/s13017-019-0247-0
48. Farkas N, Hanák L, Mikó A, et al. A Multicenter, International Cohort Analysis of 1435 Cases to Support Clinical Trial Design in Acute Pancreatitis. Front Physiol. 2019;10:1092. doi:10.3389/fphys.2019.01092
49. Wu H, Liao B, Ji T, Huang J, Ma K, Luo Y. Diagnostic value of CRP for predicting the severity of acute pancreatitis: a systematic review and meta-analysis. Biomarkers. 2024;29(7):494–503. doi:10.1080/1354750X.2024.2415463
50. Cui ML, Kim KH, Kim HG, et al. Incidence, risk factors and clinical course of pancreatic fluid collections in acute pancreatitis. Dig Dis Sci. 2014;59(5):1055–1062. doi:10.1007/s10620-013-2967-4
51. Fujiwara J, Matsumoto S, Sekine M, Mashima H. C-reactive protein predicts the development of walled-off necrosis in patients with severe acute pancreatitis. JGH Open. 2021;5(8):907–914. doi:10.1002/jgh3.12605
52. Solakoglu T, Kucukmetin NT, Akar M, Koseoglu H. Acute peripancreatic fluid collection in acute pancreatitis: incidence, outcome, and association with inflammatory markers. Saudi J Gastroenterol. 2023;29(4):225–232. doi:10.4103/sjg.sjg_443_22
53. Gürün Kaya A, Ş n Ö, M Ö, et al. The relation of lactate level and carbon dioxide pressure discrepancies between transcutaneous and arterial measurements. Tuberk Toraks. 2024;72(2):120–130. doi:10.5578/tt.202402920
54. Shu W, Wan J, Chen J, et al. Initially elevated arterial lactate as an independent predictor of poor outcomes in severe acute pancreatitis. BMC Gastroenterol. 2020;20(1):116. doi:10.1186/s12876-020-01268-1
55. Xu SX, Wang NZ, Yao GH, Ding YB, Xu CF. Elevated venous lactate level as an early predictive marker of organ failure in acute pancreatitis: a retrospective study. Eur Rev Med Pharmacol Sci. 2024;28(6):2179–2185. doi:10.26355/eurrev_202403_35721
56. Wu J, Liang Y, Tang X, et al. Ultra-early indicators of acute hypertriglyceridemic pancreatitis may influence treatment decision-making. Sci Rep. 2025;15(1):1572. doi:10.1038/s41598-025-85847-w
57. Yeung YP, Lam BY, Yip AW. APACHE system is better than Ranson system in the prediction of severity of acute pancreatitis. Hepatobiliary Pancreat Dis Int. 2006;5(2):294–299.
58. Zhou H, Mei X, He X, Lan T, Guo S. Severity stratification and prognostic prediction of patients with acute pancreatitis at early phase: a retrospective study. Medicine (Baltimore). 2019;98(16):e15275. doi:10.1097/MD.0000000000015275
59. Yang K, Song Y, Su Y, Li C, Ding N. Establishment and Validation of an Early Predictive Model for Severe Acute Pancreatitis. J Inflamm Res. 2024;17:3551–3561. doi:10.2147/JIR.S457199
60. Luo X, Wang J, Wu Q, et al. A modified Ranson score to predict disease severity, organ failure, pancreatic necrosis, and pancreatic infection in patients with acute pancreatitis. Front Med (Lausanne). 2023;10:1145471. doi:10.3389/fmed.2023.1145471
61. Shi N, Zhang X, Zhu Y, et al. Predicting persistent organ failure on admission in patients with acute pancreatitis: development and validation of a mobile nomogram. HPB (Oxford). 2022;24(11):1907–1920. doi:10.1016/j.hpb.2022.05.1347
62. Ding L, Zheng P, Li XY, et al. Nomogram for the Prediction of 30-Day Readmission in Acute Pancreatitis. Dig Dis Sci. 2022;67(8):4112–4121. doi:10.1007/s10620-021-07236-3
63. Li C, Ren Q, Wang Z, Wang G. Early prediction of in-hospital mortality in acute pancreatitis: a retrospective observational cohort study based on a large multicentre critical care database. BMJ Open. 2020;10(12):e041893. doi:10.1136/bmjopen-2020-041893
64. Zou K, Huang S, Ren W, et al. Development and Validation of a Dynamic Nomogram for Predicting in-Hospital Mortality in Patients with Acute Pancreatitis: a Retrospective Cohort Study in the Intensive Care Unit. Int J Gen Med. 2023;16:2541–2553. doi:10.2147/IJGM.S409812
65. Pan LN, Pan SA, Lei BH, Hong GL, Chen KW. Development of a Novel Nomogram Incorporating Red Blood Cell Distribution Width-Albumin Ratio for the Prediction of 30-day Mortality in Acute Pancreatitis Patients. Emerg Med Int. 2022;2022:1573931. doi:10.1155/2022/1573931
66. Gravito-Soares M, Gravito-Soares E, Gomes D, Almeida N, Tomé L. Red cell distribution width and red cell distribution width to total serum calcium ratio as major predictors of severity and mortality in acute pancreatitis. BMC Gastroenterol. 2018;18(1):108. doi:10.1186/s12876-018-0834-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.