Back to Journals » Cancer Management and Research » Volume 12
Nodal Involvement Pattern in Clinical Stage IA Non-Small Cell Lung Cancer According to Tumor Location
Authors Meng S, Liu G, Wang S, Yang F, Wang J
Received 19 May 2020
Accepted for publication 30 July 2020
Published 26 August 2020 Volume 2020:12 Pages 7875—7880
DOI https://doi.org/10.2147/CMAR.S262623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Shushi Meng, Ganwei Liu, Shaodong Wang, Fan Yang, Jun Wang
Department of Thoracic Surgery, Peking University People’s Hospital, Beijing, People’s Republic of China
Correspondence: Shaodong Wang; Jun Wang
Department of Thoracic Surgery, Peking University People’s Hospital, No. 11, Xizhimen South Street, Beijing 100044, People’s Republic of China
Tel +86 10-88326652
; +86 10-88326650
Email [email protected]; [email protected]
Purpose: The purpose of this study was to investigate lymph node involvement pattern in clinical stage IA non-small cell lung cancer (NSCLC).
Patients and Methods: Clinical stage ⅠA NSCLC patients who underwent lobectomy and lymph node resection were included in this retrospective study. Mediastinal lymph node involvement was distinguished by different lobes and tumor size.
Results: From 2000 to 2015, a total of 759 patients were identified: 282 (37.2%) with tumors in the right upper lobe (RUL), 183 (24.1%) in the left upper lobe (LUL), 124 (16.3%) in the right lower lobe (RLL), 103 (13.6%) in the left lower lobe (LLL), and 67 (8.8%) in the right middle lobe (RML). Patients with tumor size ≤ 1 cm accounted for 19.6%, > 1 and ≤ 2 cm for 47.8%, > 2 and ≤ 3 cm for 32.5%. Patients with pN1 accounted for 8.2%, and pN2 for 12.5%. Among patients with pN2, the inferior mediastinum was involved in 9.7% of RULs and 17.4% of LULs; the superior mediastinum was involved in 52.2% of RLLs and 36.4% of LLLs. Mediastinal lymph node metastasis was found in 13.2% of patients with size > 1 and ≤ 2 cm, and 19.0% of > 2 and ≤ 3 cm. Patients with tumors ≤ 1 cm had no N2 lymph node involved.
Conclusion: Selective lymph node dissection based on tumor location is not recommended in clinical stage ⅠA NSCLC, and systemic lymph node dissection should be performed for NSCLC with size > 1 cm.
Keywords: non-small cell lung cancer, clinical stage ⅠA, lymph node dissection, nodal involvement pattern
Introduction
Lung cancer is the leading cause of cancer death among both men and women.1 The overall 5-year survival rate of non-small cell lung cancer (NSCLC) ranges from 83.9% in ⅠA to 29.6% in IIIB.2 Lymph node involvement pattern is crucial for accurate staging of NSCLC.3 However, there is still controversy over whether to dissect the mediastinal lymph nodes in early lung cancer. From the perspective of skip N2 metastasis and occult mediastinal metastasis in lymph node involvement pattern, some authors consider systemic lymph node dissection to be the only acceptable procedure.4,5 Others have suggested that selective lymph node dissection can be performed according to the primary tumor site in patients with no apparent nodal metastases preoperatively.6–8
In this study, we aimed to examine mediastinal lymph node involvement pattern of clinical stage ⅠA NSCLC patients.
Patients and Methods
Patients
Lung cancer patients who underwent surgery in Peking University People’s Hospital between January 2000 and December 2015 were reviewed. The clinical records included disease history, medication information, surgical records, and pathological results. Preoperative chest computed tomography (CT) was performed in all patients. If the short-axis dimension of lymph nodes was ≥1 cm, positron emission tomography-computed tomography (PET-CT) scan or endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) was performed. We focused on primary NSCLC patients with clinical stage ⅠA who underwent lobectomy and lymph node resection. Cases with positive lymph nodes and multiple tumor lesions were excluded.
The patients were divided into five groups according to the tumor location: right upper lobe (RUL), right middle lobe (RML), right lower lobe (RLL), left upper lobe (LUL), and left lower lobe (LLL). At the same time, according to tumor size, they were divided into three groups: T1a (≤1 cm), T1b (>1 and ≤2 cm), and T1c (>2 and ≤3 cm). The stations and zones of lymph nodes and staging of lung cancer were performed according to the 8th Edition Lung Cancer Stage Classification.3 Patients with N1 lymph node involved were divided into three subgroups: extra-lobar (only 10/11 involved), intra-lobar (only 12/13/14 involved), and both (both involved). The N2 population was divided into superior mediastinal lymph nodes (SM: 2, 3, 4, 5, 6) and inferior mediastinal lymph nodes (IM: 7, 8, 9). Patients with N2 lymph node involved were divided into three subgroups: N2a1 (single-station N2 without N1 involvement), N2a2 (single-station N2 with N1 involvement), and N2b (multiple-station N2 involvement), according to the zone and number of lymph nodes involved. Moreover, they were divided into N0N2 group (skip metastases, no N1, but N2 involved) and N1N2 group (both N1 and N2 involved).
Ethics Statement
The study protocol was approved by the Ethics Committee of Peking University People’s Hospital (approval number: 2018PHB144-01). Written informed consent was obtained from each participant and the study was conducted in accordance with the guidelines in the Declaration of Helsinki.
Statistical Analysis
Continuous variables were described as mean ± S.D. and categorical variables were described as number and proportion.
Results
A total of 1730 NSCLC patients underwent lobectomy and lymph node resection in our department between January 2000 and December 2015. According to the enrollment criteria, 759 patients with clinical stage ⅠA were included in the study, 371 males (48.9%) and 388 females (51.1%), with a mean age of 60.3 ± 10.3 years. The main characteristics are shown in Table 1. Tumors most often occurred in the RUL (n = 282, 37.2%), followed by LUL (n = 183, 24.1%), RLL (n = 124, 16.3%), LLL (n = 103, 13.6%), and RML (n = 67, 8.8%). The most common pathological type was adenocarcinoma (n = 640, 84.3%), followed by squamous cell carcinoma (n = 93, 12.3%). Video-assisted thoracoscopic surgery (VATS) was the most frequently selected surgical approach (n = 722, 95.1%), and thoracotomy was also performed (n = 37, 4.9%). A total of 655 patients (86.3%) had systemic lymph node dissection, and the proportion in the RUL was the highest (n = 257, 91.1%). In terms of tumor size, T1b group (>1 and ≤2 cm) accounted for 47.8% (n = 363), T1c group (>2 and ≤3 cm) for 32.5% (n = 247), and T1a group (≤1 cm) for 19.6% (n = 149).
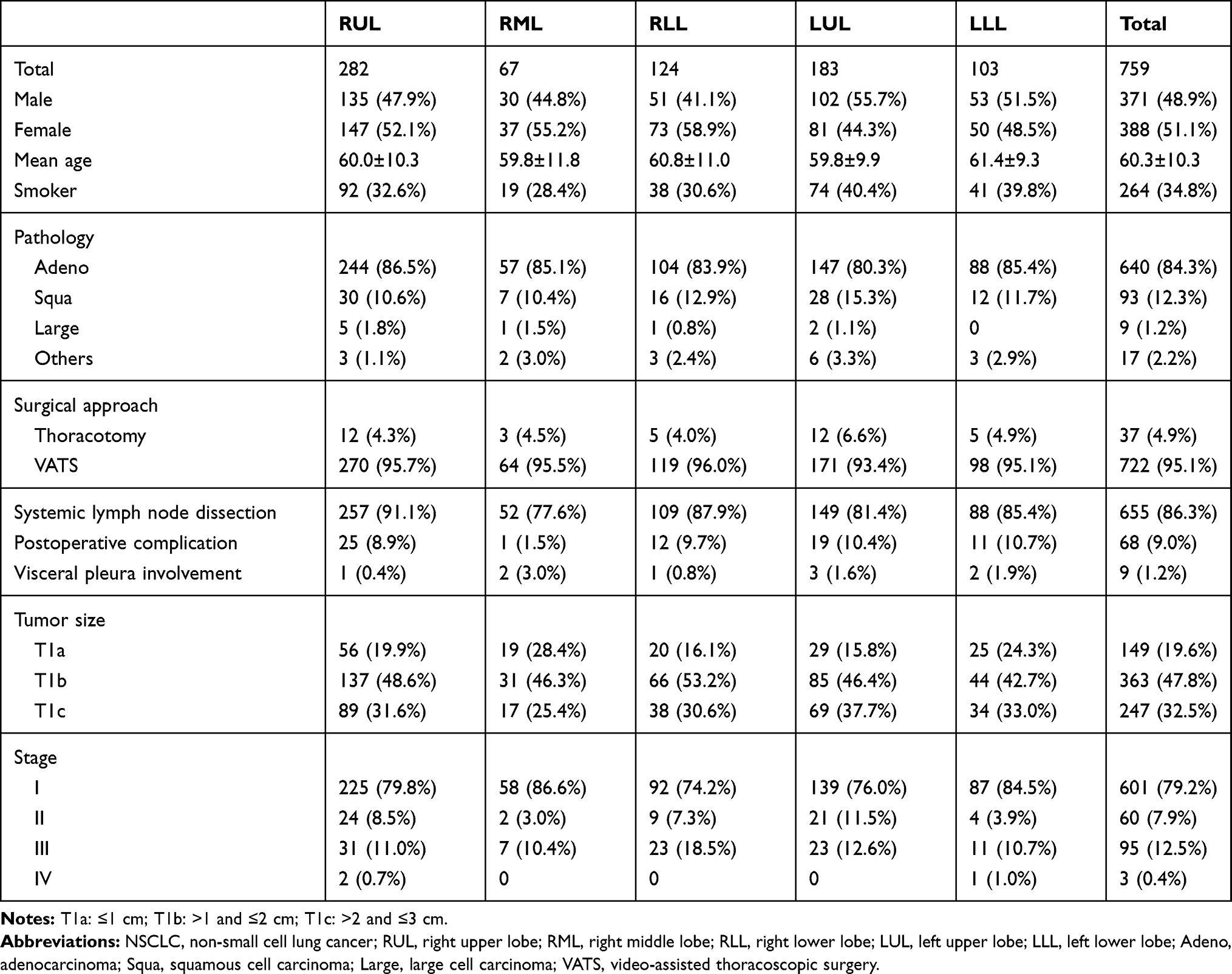 |
Table 1 Main Characteristics of NSCLC Patients in Clinical Stage I a |
The involvement of lymph nodes in each lobe is shown in Table 2. In 759 cases, pN0 accounted for the largest proportion (n=601, 79.2%), pN1 for 8.2% (n=62), and pN2 for 12.5% (n=95). There were 28 intralobar involved cases (3.7%) and 26 extralobar involved cases (3.4%). A total of 3.2% of cases were classified into N2a1 (n = 24), 3.8% into N2a2 (n = 29), and 5.5% into N2b (n = 42).
 |
Table 2 Nodal Involvement Pattern in Each Lobe |
The involvement of lymph nodes in different tumor sizes is shown in Table 3. No pN2 was found in the T1a group, which meant that no mediastinal lymph node metastasis occurred in NSCLC with the ≤1 cm size. In the T1b and T1c groups, the proportion of pN2 was13.2% (n = 48) and 19.9% (n = 47), respectively.
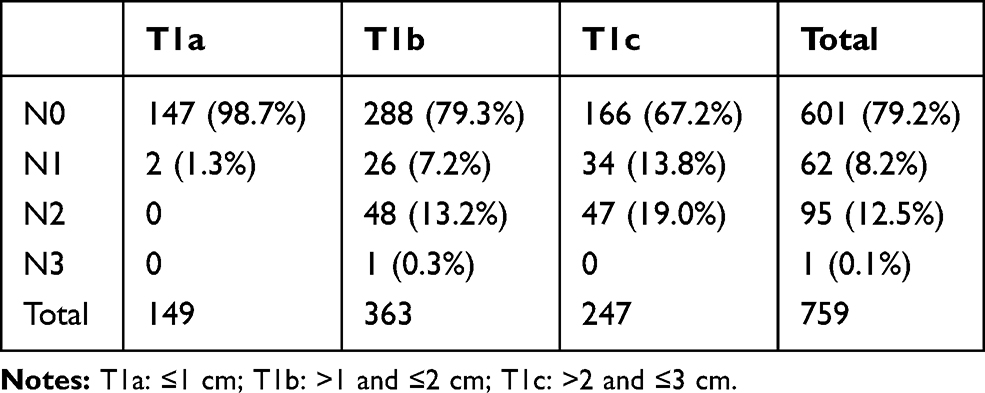 |
Table 3 Nodal Involvement Pattern in Different Tumor Sizes |
The distribution of pN2 in each lobe is shown in detail in Supplementary Tables 1–5.
In the RUL, 31 of 282 cases (11.0%) were N2 involved. A total of 12 (4.3%) were skip metastases, and their pN2 status only existed in SM. Nineteen patients (6.7%) had both N1 and N2 involved. Three of 31patients (9.7%) had pN2 status both in the SM and the IM, and their subcarinal lymph nodes (Station 7) were all involved. The other 28 (90.3%) had pN2 status only in the SM. Moreover, 137 patients in the RUL were classified into the T1b group, of whom 18 (13.1%) had N2 involved. Eighty-nine patients were classified into T1c group, and 13 (14.6%) had N2 involved.
In the RML, 7 of 67 cases (10.4%) were N2 involved. A total of 3 (4.5%) were skip metastases. Four patients (6.0%) had both N1 and N2 involved. Five of 7 patients (71.4%) had pN2 status found both in the SM and IM, while one only in the SM (14.3%) and one only in the IM (14.3%). Moreover, 31 patients in the RML were classified into the T1b group, of whom four (12.9%) had N2 involved. Seventeen patients were classified into the T1c group, and 3 (17.6%) had N2 involved.
In the RLL, 23 of 124 cases (18.5%) were N2 involved. A total of 6 (4.8%) were skip metastases, and their subcarinal lymph nodes (Station 7) were all involved. Seventeen patients (13.7%) had both N1 and N2 involved. Twelve of 23 patients (52.2%) had pN2 status found both in the SM and IM, while the other 11 only in the IM (47.8%). Moreover, 66 patients in the RLL were classified into the T1b group, of whom 10 (15.2%) had N2 involved. Thirty-eight patients were classified into the T1c group, and 13 (34.2%) had N2 involved.
In the LUL, 23 of 183 cases (12.6%) were N2 involved. A total of 7 (3.8%) were skip metastases, all of which were only the SM involved. Sixteen patients (8.7%) had both N1 and N2 involved. Two of 23 patients (8.7%) had pN2 status found both in the SM and IM, while 19 only in the SM (82.6%) and 2 only in the IM (8.7%). Moreover, 85 patients in the LUL were classified into the T1b group, of whom 12 (14.1%) had N2 involved. Sixty-nine patients were classified into the T1c group, and 11 (15.9%) had N2 involved.
In the LLL, 11 of 103 cases (10.7%) were N2 involved. A total of 4 (3.9%) were skip metastases, all of which were only the IM involved. Seven patients (6.8%) had both N1 and N2 involved. Three of 11 patients (27.3%) had pN2 status found both in the SM and IM, while 7 only in the IM (63.6%) and 1 only in the SM (9.1%). Moreover, 44 patients in the LLL were classified into the T1b group, of whom 4 (9.1%) had N2 involved. Thirty-four patients were classified into the T1c group, and 7 (20.6%) had N2 involved.
Discussion
The current common surgical options for lung cancer are VATS and systemic lymph node dissection,9,10 which was reflected in our study. In recent studies,11,12 the incidence of pN1 and pN2 in clinical stage IA NSCLC patients was about 5.9–7.8% and 7.1–10.6%, respectively. The proportions in our study were similar, 8.2% for pN1 and 12.5% forvpN2.
The prognosis of single-station N2 (N2a) is generally considered good.13 In our study, patients with N2a (n = 53) accounted for 55.8% of pN2 cases, which was consistent with previous studies. In the RUL group, Station 4 was the most common single-station metastasis (17/18, 94.4%), while Station 5 was the most frequent in LUL (9/16, 56.3%). Station 7 was the most common single-station metastasis both in RLL and LLL (10/11, 90.9% and 5/6, 83.3%, respectively). This may be related to the different lymphatic anatomy between the sides.14
Skip metastases (n = 32) occurred in 4.2% of patients with clinical stageⅠA NSCLC, which was similar to previous studies.15,16 There were 24 pN2a1 cases in total (3.2%). Some studies have suggested that overall survival and recurrence-free survival rates of pN2a1 cases are similar to pN1, and have significantly better survival rates than pN1N2.17
No pN2 status occurred in NSCLC with tumor size ≤1 cm, which indicates that mediastinal lymph node dissection may not be necessary for NSCLC ≤1cm. The pN2 status accounted for a considerable proportion in the T1b and T1c (13.2% and 19.0%, respectively), and even reached 15.2% and 34.2% in RLL, which suggests that mediastinal lymph node dissection should be performed for NSCLC with size >1 cm. Among patients with pN2, 9.7% of RUL and 17.4% of LUL had the IM involved; as for the SM involved, 52.2% of RLL and 36.4% of LLL were found. This suggests that selective lymph node dissection based on tumor location is not convincing.
There were 3 of 31 cases in RUL that had Station 7 involved (9.7%), and 3 of 23 in LUL also (13.0%). Upper lobe tumor with only the IM involved was found in 2 of 54 cases (3.7%). Lower lobe tumor with only the SM involved was found in 1 of 34 case (2.9%). These findings were similar to previous studies.18–20 It has been suggested that Station 7 dissection is unnecessary if there is no IM involved in the LUL cases.20 However, in our study, 2 of 23 LUL cases (8.7%) showed Station 7 metastasis without the SM involved. Given the results in our study, we cannot agree with the previous opinion.
All cases that the SM involved in LLL had pN1, but 3 cases in RLL were the SM involved without pN1 (3/12, 25.0%). All cases with the SM involved in RLL had Station 7 metastasis. This suggests that the SM metastases of RLL NSCLC may require the involvement of Station 7. Similarly, the IM metastases of RUL NSCLC were also related to Station 7. There was no such involvement of Station 7 in left lobes.
We believe that systemic lymph node dissection should be performed for NSCLC with size >1cm.
Several studies had investigated recurrence and survival outcomes related to systemic lymph node dissection and selective dissection. A meta-analysis of six cohort studies concluded that there was no significant difference in overall survival and disease-free survival between the two dissection methods.21 Selective lymph node dissection had significant benefits in relation to operating time and blood loss.21,22 Some studies have shown that lobe-specific selective dissection and systemic dissection were similar in local, regional, or distant recurrence.7,8 However, it has also been found that selective dissection caused by patient-related factors has a higher recurrence rate.22
There were some limitations in our study. First, there was only one patient with T1N3 (1/759, 0.1%), which may be different from the real world situation but it did not affect our main conclusion about mediastinal lymph nodes. Second, our conclusions were based on a single-center retrospective study. Additionally, considering that the postoperative follow-up time of some patients was <5 years, our study only described the nodal involvement pattern, without evaluation of prognosis. However, lymph node involvement pattern directly affects the staging and adjuvant treatment of patients, so it is still of some importance.
Conclusion
We conclude that selective lymph node dissection based on tumor location is not recommended in clinical stage ⅠA NSCLC, and systemic lymph node dissection should be performed for NSCLC with size >1cm.
Abbreviations
NSCLC, non-small cell lung cancer; CT, computed tomography; PET-CT, positron emission tomography-computed tomography; EBUS-TBNA, endobronchial ultrasound-guided transbronchial needle aspiration; RUL, right upper lobe; RML, right middle lobe; RLL, right lower lobe; LUL, left upper lobe; LLL, left lower lobe; SM, superior mediastinum; IM, inferior mediastinum; VATS, video-assisted thoracoscopic surgery.
Acknowledgments
The authors thank all the patients included in this study.
Disclosure
The authors report no conflicts of interest related to this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30.
2. Asamura H, Goya T, Koshiishi Y, et al. A Japanese lung cancer registry study: prognosis of 13,010 resected lung cancers. J Thorac Oncol. 2008;3:46–52.
3. Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The eighth edition lung cancer stage classification. Chest. 2017;151(1):193–203.
4. Kotoulas CS, Foroulis CN, Kostikas K, et al. Involvement of lymphatic metastatic spread in non-small cell lung cancer accordingly to the primary cancer location. Lung Cancer. 2004;44(2):183–191.
5. Saeteng S, Tantraworasin A, Euathrongchit J, Lertprasertsuke N, Wannasopha Y. Nodal involvement pattern in resectable lung cancer according to tumor location. Cancer Manag Res. 2012;4:151–158.
6. Han H, Chen H. Selective lymph node dissection in early-stage non-small cell lung cancer. J Thorac Dis. 2017;9:2102–2107.
7. Shapiro M, Kadakia S, Lim J, et al. Lobe-specific mediastinal nodal dissection is sufficient during lobectomy by video-assisted thoracic surgery or thoracotomy for early-stage lung cancer. Chest. 2013;144:1615–1621.
8. Darling GE, Allen MS, Decker PA, et al. Randomized trial of mediastinal lymph node sampling versus complete lymphadenectomy during pulmonary resection in the patient with N0 or N1 (less than hilar) non-small cell carcinoma: results of the American College of Surgery Oncology Group Z0030 Trial. J Thorac Cardiovasc Surg. 2011;141:662–670.
9. Whitson BA, Groth SS, Andrade RS, Habermann EB, Maddaus MA, D’Cunha J. T1/T2 non-small-cell lung cancer treated by lobectomy: does tumor anatomic location matter? J Surg Res. 2012;177:185–190.
10. Paul S, Isaacs AJ, Treasure T, Altorki NK, Sedrakyan A. Long term survival with thoracoscopic versus open lobectomy: propensity matched comparative analysis using SEER-Medicare database. BMJ. 2014;349:g5575.
11. Zhao JL, Guo HW, Yang P, Jiang DZ, Tian H. Selective lymph node dissection for clinical T1 stage non-small cell lung cancer. Transl Cancer Res. 2019;8:2820–2828.
12. Chen B, Wang X, Yu X, et al. Lymph node metastasis in Chinese patients with clinical T1 non-small cell lung cancer: A multicenter real-world observational study. Thorac Cancer. 2019;10:533–542.
13. Łochowski M, Łochowska B, Rębowski M, Brzeziński D, Cieślik-Wolski B, Kozak J. Five-year survival analysis and prognostic factors in patients operated on for non-small cell lung cancer with N2 disease. J Thorac Dis. 2018;10:3180–3186.
14. Riquet M. Anatomic basis of lymphatic spread from carcinoma of the lung to the mediastinum: surgical and prognostic implications. Surg Radiol Anat. 1993;15:271–277.
15. Gorai A, Sakao Y, Kuroda H, et al. The clinicopathological features associated with skip N2 metastases in patients with clinical stage IA non-small-cell lung cancer. Eur J Cardiothorac Surg. 2015;47:653–658.
16. Liang RB, Yang J, Zeng TS, et al. Incidence and distribution of lobe-specific mediastinal lymph node metastasis in non-small cell lung cancer: data from 4511 resected cases. Ann Surg Oncol. 2018;25(11):3300–3307.
17. Yazgan S, Ucvet A, Gursoy S, Samancilar O, Yagci T. Single-station skip-N2 disease: good prognosis in resected non-small-cell lung cancer (long-term results in skip-N2 disease). Interact Cardiovasc Thorac Surg. 2019;28:247–252.
18. Asamura H, Nakayama H, Kondo H, Tsuchiya R, Naruke T. Lobe-specific extent of systematic lymph node dissection for non-small cell lung carcinomas according to a retrospective study of metastasis and prognosis. J Thorac Cardiovasc Surg. 1999;117:1102–1111.
19. Aokage K, Yoshida J, Ishii G, Hishida T, Nishimura M, Nagai K. Subcarinal lymph node in upper lobe non-small cell lung cancer patients: is selective lymph node dissection valid? Lung Cancer. 2010;70:163–167.
20. Shimada Y, Saji H, Kakihana M, et al. Retrospective analysis of nodal spread patterns according to tumor location in pathological N2 non-small cell lung cancer. World J Surg. 2012;36:2865–2871.
21. Han H, Zhao Y, Chen H. Selective versus systematic lymph node dissection (other than sampling) for clinical N2-negative non-small cell lung cancer: a meta-analysis of observational studies. J Thorac Dis. 2018;10:3428–3435.
22. Maniwa T, Okumura T, Isaka M, et al. Recurrence of mediastinal node cancer after lobe-specific systematic nodal dissection for non-small-cell lung cancer. Eur J Cardiothorac Surg. 2013;44:e59–e64.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.