Back to Journals » Nature and Science of Sleep » Volume 14
Nocturnal Oxygen Desaturation Index Correlates with Respiratory Depression in Post-Surgical Patients Receiving Opioids – A Post-Hoc Analysis from the Prediction of Opioid-Induced Respiratory Depression in Patients Monitored by Capnography (PRODIGY) Study
Authors Liew LQ, Law LSC, Seet E ![]() , Di Piazza F
, Di Piazza F ![]() , Liu KE, Sim MA, Chua VTY, Weingarten TN, Khanna AK, Ti LK
, Liu KE, Sim MA, Chua VTY, Weingarten TN, Khanna AK, Ti LK
Received 21 December 2021
Accepted for publication 23 March 2022
Published 26 April 2022 Volume 2022:14 Pages 805—817
DOI https://doi.org/10.2147/NSS.S351840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Lydia QN Liew,1 Lawrence SC Law,1 Edwin Seet,2 Fabio Di Piazza,3 Katherine E Liu,4 Ming Ann Sim,1 Vanessa TY Chua,1 Toby N Weingarten,5 Ashish K Khanna,6 Lian Kah Ti1,2 On behalf of the PRediction of Opioid-induced respiratory Depression In patients monitored by capnoGraphY (PRODIGY) Group Investigators
1National University Hospital, Singapore, Singapore; 2National University of Singapore, Yong Loo Lin School of Medicine, Singapore; 3Medtronic Core Clinical Solutions, Study and Scientific Solutions, Rome, Italy; 4Patient Monitoring Clinical Research, Medtronic, Minneapolis, MN, USA; 5Departments of Anesthesiology and Perioperative Medicine, Mayo Clinic College of Medicine and Science, Rochester, MN, USA; 6Wake Forest School of Medicine, Winston-Salem, North Carolina, US & Outcomes Research Consortium, Cleveland, OH, USA
Correspondence: Lian Kah Ti, Yong Loo Lin School of Medicine, National University of Singapore, 21 Lower Kent Ridge Road, Singapore, 119077, Singapore, Tel +65 6779 5555, Email [email protected]
Purpose: Postoperative monitoring of respiratory status on general care wards typically consists of intermittent checks of oxyhemoglobin saturation and respiratory rate, allowing substantial unmonitored time for severe opioid induced respiratory depression (RD) to develop unnoticed. Oxygen desaturation index (ODI) can be computed solely by continuous pulse oximetry monitoring. In this post-hoc analysis, we evaluate whether nocturnal ODI correlates with RD.
Patients and Methods: The PRODIGY trial (NCT02811302) was a multinational study conducted where adult patients receiving parenteral opioids on the general care floor were continuously monitored by blinded pulse oximetry and capnography monitoring to detect episodes of RD. An RD episode was defined as: respiratory rate ≤ 5 breaths/min (bpm) for ≥ 3 minutes, oxygen saturation (SpO2) ≤ 85% for ≥ 3 minutes, end-tidal carbon dioxide (EtCO2) ≤ 15 or ≥ 60 mm Hg for ≥ 3 minutes, apnea episode lasting > 30 seconds, or any respiratory opioid-related adverse event. Data were used to calculate nocturnal (00:00 ─ 06:00) ODI4% based on desaturation episodes (4% decrease from mean oxyhemoglobin saturation in the past 120 seconds, lasting ≥ 10 seconds). Continuous monitoring began after a patient received parenteral opioids, allowing identification of potential RD and ODI4% episodes during opioid therapy. The average number of ODI4% episodes (≥ 1, ≥ 5, ≥ 10, ≥ 15 episodes/hour) were analyzed. Logistic regression and area under the receiver operating characteristic curve (AUC) were computed.
Results: A final cohort of 1072 (out of 1335) patients had sufficient data, with 76% (N=817/1072) having ≥ 1 episode of ODI4%. Multivariable logistic regression showed that ODI4% was strongly associated with RD, with greater risk for higher ODI4% scores: ≥ 5 episodes/hour odds ratio 2.59 (95% CI 1.72– 3.89, p< 0.0001); ≥ 10 episodes/hour 3.39 (95% CI 1.80– 6.39, p=0.0002); ≥ 15 episodes/hour 4.71 (95% CI 1.93– 11.47, p=0.0006).There was no significant association between ODI4% and respiratory adverse events.
Conclusion: Nocturnal ODI4% was highly correlated with RD among hospitalized patients receiving parenteral opioids. Patients with a high ODI4%, especially with ≥ 15 episodes/hour, are more likely to experience RD and should be evaluated for the need of closer monitoring after opioid administration.
Keywords: opioids, oxygen desaturation index, respiratory depression, sleep apnea
Introduction
Opioids are the cornerstone of analgesic therapy for hospitalized patients, but carry the risk of opioid induced respiratory depression (RD), which can lead to respiratory failure, resulting in severe morbidity and mortality.1 Alarmingly, the incidence of RD on general care wards exceeds 40%, but is often unrecognized by routine monitoring.2–5 It is thus important to identify patients who are at risk for severe RD, ideally before they receive opioids, in order to implement mitigating measures such as closer oxygenation and ventilation monitoring after opioid therapy is initiated.2
The Prediction of Opioid-induced respiratory Depression in patients monitored by capnoGraphY (PRODIGY) trial was conducted to create a multivariable risk prediction tool to classify patients as low, intermediate, and high risk for RD. The observational trial enrolled medical and surgical patients receiving parenteral opioids on the general care floor, and RD episodes were identified using blinded continuous capnography and pulse oximetry.4
The most commonly available monitoring modality for respiratory events is the pulse oximeter, which determines arterial oxygen saturation and pulse rate. The pulse oximeter is most commonly used intermittently, but can also be used continuously. Although intermittent pulse oximetry is standard of care at most institutions, capnography monitoring assesses ventilation directly, and when used continuously, can reduce the incidence of RD.6 Although it does not assess ventilation directly, continuous pulse oximetry monitoring allows the calculation of the oxygen desaturation index (ODI), the hourly average number of oxygen desaturation episodes, defined as a percentage decrease in saturation from the average saturation in the preceding 120 seconds, and lasting >10 seconds. ODI4% at a threshold of 15 episodes per hour has been shown to be a sensitive and specific tool in predicting moderate to severe obstructive sleep apnea.7,8 However, the relationship between ODI and RD, as detected by continuous oximetry and capnography, has not been evaluated. The primary aim of this post-hoc study was to evaluate whether nocturnal ODI4%, using continuous pulse oximetry alone, correlates with RD in the PRODIGY cohort, to test the hypothesis that high ODI4% scores would be correlated with RD. The secondary aim was to determine if oxygen desaturation was associated with adverse patient outcomes.
Materials and Methods
PRODIGY Trial
The PRODIGY trial (www.clinicaltrials.gov NCT02811302) was conducted from April 7, 2017, to May 11, 2018, at 16 sites in Asia, Europe, and the United States, in accordance with the Declaration of Helsinki and all local regulatory requirements. The protocol was approved by the institutional review board or research ethics committee of each participating site.4 All patients provided written informed consent before enrollment. Eligible patients included adults (≥18, 20, and 21 years in United States/Europe, Japan, and Singapore, respectively) who were anticipated to receive parenteral opioids on the general care floor following surgery or a medical procedure and gave informed consent. The following patients were excluded: 1. Those whose hospital stay was anticipated to be <24 hours; 2. Those who received intrathecal opioids; 3. Those with American Society of Anesthesiology (ASA) physical status V or higher; 4. Those with an active Do Not Resuscitate status; 5. Those who were ventilated or intubated; 6. Those unwilling or unable to comply with monitoring procedures; 7. Those who were part of a vulnerable population, such as a patient who could not understand the purpose and risks of the trial; and 8. Those who were participating in a confounding clinical trial.4 A total of 1495 patients were enrolled in the trial, with a final analysis cohort of 1335 patients. As an observational trial, each site continued its standard practices in opioid prescription and administration, which included both patient controlled analgesia and nurse-administered analgesia on an as-needed basis. In a post-hoc analysis, the most common opioids administered during the PRODIGY trial included hydromorphone, fentanyl, oxycodone, and morphine, with a median post-procedure dosage of 16.0 (IQR 3.3–52.0) morphine milligram equivalents (MME).9 Upon arrival on the general care floor and receipt of parenteral opioids, patients began continuous, blinded pulse oximetry and capnography monitoring (Capnostream™ 20p bedside monitor or 35 portable respiratory monitor with Nellcor™ pulse oximetry, Medtronic, Boulder, CO, US), alongside standard of care monitoring. The sampling frequency of pulse oximetry and capnography was 20 readings per second, with a 7 second oximetry signal average. Blinded, continuous pulse oximetry and capnography monitoring always occurred simultaneously, and continued for up to 48 hr on the general care floor.
The primary outcome of the PRODIGY trial was to determine the incidence of RD on the general care floor, and to derive a risk prediction tool to identify patients at high, intermediate, or low respiratory depression risk.10 An RD episode was defined as: respiratory rate ≤5 breaths/min (bpm) for ≥3 minutes, oxygen saturation (SpO2) ≤85% for ≥3 minutes, end-tidal carbon dioxide (EtCO2) ≤15 or ≥60 mm Hg for ≥3 minutes, apnea episode lasting >30 seconds, or any respiratory opioid-related adverse event.4 Combined pulse oximetry and capnography data for each patient were reviewed by an independent clinical event committee composed of 4 experts in respiratory and ventilation monitoring, to confirm the presence or absence of ≥1 RD episode, and exclude artifacts. Oximetry and capnography data were evaluated together. Committee members had access to time records of opioid use on the general care floor, with all other patient history blinded. Each of the 5768 adjudicated RD episodes were reviewed independently by 3 clinical event committee members, with the final adjudication determined by majority agreement.4
Outcomes Measures
The original objective of the PRODIGY trial was to derive a risk prediction tool to assess patient risk for opioid-induced respiratory depression on the general care floor.4 The purpose of this post-hoc analysis was to determine whether nocturnal oximetry patterns are associated with RD and adverse patient outcomes. Nocturnal oximetry patterns were defined using ODI4%. This article complies with the reporting guidelines in the strengthening the reporting of observational studies in epidemiology (STROBE) statement.
Patient Cohort
This analysis included PRODIGY patients who received opioids and started continuous pulse oximetry and capnography monitoring on the general care floor. Patients without overnight continuous monitoring data were excluded (N=263).
Oximetry Data Processing
Continuous nocturnal pulse oximetry data was defined as data collected between the hours of 00:00 and 06:00. This represented the time in which the patients were most likely to be asleep. Although 13 patients underwent multiple nights of monitoring, only the first night of post-procedure monitoring was considered for each patient, to achieve a more consistent length of continuous monitoring across patients. ODI was calculated based on desaturation episodes defined by a 4% decrease in saturation from the average blood oxygen saturation in the past 120 seconds, lasting at least 10 seconds. The average number of ODI4% episodes per hour was determined automatically for each patient and incorporated into the analysis. We selected ODI4% because other studies have demonstrated that it can predict obstructive sleep apnea. In particular, ODI4% with a cut-off of ≥15 events/hour has been shown to have high sensitivity, specificity, and accuracy in predicting moderate to severe obstructive sleep apnea (OSA).7,8
Statistics
The data was summarized by descriptive statistics or frequencies and percentages for continuous and categorical variables, respectively. Wilcoxon signed rank tests or Kruskal-Wallis tests were performed to compare continuous variables, and Chi-square tests performed to compare categorical variables. Correlation was determined using Spearman rho. Statistical tests were 2-sided with statistical significance accepted at P<0.05. Outliers were defined as observations with ≥3 times the standard deviation. Missing data were not imputed for this analysis.
To explore the association between ODI and RD, a univariable analysis was performed, with ODI4% cutoffs of ≥1 episode during continuous monitoring, as well as an average of ≥5, ≥10, and ≥15 episodes per hour, based on previous clinical evidence that these frequencies are associated with a higher rate of postoperative complications.7,8,11 Significant factors in the univariable analysis were analyzed with a multivariable regression model.
For the multivariable logistic regression model, 39 risk factors were included during model derivation, including 38 risk factors from the original PRODIGY analysis, along with ODI4%. The risk factors considered from the original PRODIGY analysis included: age (<60 or ≥60 in decades), body mass index (BMI), sex, current smoker, length of surgery, high risk surgery, open surgery, opioid naivety, administration of one or multiple opioids, aortic aneurysm, aortic valve disease, chronic heart failure, coronary artery disease, hypertension, mitral valve disease, myocardial infarction, orthostatic hypotension, pulmonary hypertension, chronic pain, liver failure, multi-organ dysfunction syndrome, sepsis, type I diabetes, type II diabetes, muscular dystrophy, kidney failure, acute bronchitis, asthma, chronic bronchitis, chronic obstructive pulmonary disorder, chronic restrictive lung disease, emphysema, pulmonary fibrosis, sleep disordered breathing, cerebral aneurysm, peripheral vascular disease, stroke, and transient ischemic attack.4 Sleep disordered breathing included 1) medical history of obstructive sleep apnea, 2) use of continuous positive airway pressure (CPAP), or 3) confirmation of the STOP questions in the STOP-BANG questionnaire.4 Goodness of fit was assessed with the Hosmer-Lemeshow test, along with the area under the curve (AUC). Statistical analyses were performed using SAS Version 9.4 (SAS Institute, Cary, NC, USA).
Results
Participants
The PRODIGY dataset included continuous pulse oximetry and capnography monitoring of 1335 patients. Between hours 00:00 and 06:00, the average length of monitoring was 5.6 ± 1.1 hours. A total of 263 patients did not have monitoring data during the night hours, and were excluded from the analysis, for a final cohort of 1072 patients, defined as the ODI analysis set (Figure 1). The demographics and clinical characteristics of this patient cohort are described in Table 1. Among this cohort, 52% of patients (N=560/1072) experienced at least 1 episode of respiratory depression during continuous monitoring.
 |
 |  | Table 1 Patient Demographic and Clinical Characteristics |
 |
Figure 1 Flow chart of PRODIGY patients included in analysis. |
Overnight Oxygen Desaturation Readings
During nocturnal monitoring, 76% of patients (N=817/1072) had at least one ODI4% episode and a median of 0.8 (IQR 0.2–2.7) episodes per hour of ODI4%. Oxygen desaturation was significantly more common in patients with ≥1 RD episode, with 79% of patients (N=442/560) with ≥1 RD episode experiencing at least one ODI4% episode, compared to 73% of patients (N=375/512) without RD (p=0.029). The median total number of ODI4% episodes among patients with and without RD (5.0 [IQR 1.0–9.0] vs 4.0 [IQR 0.0–13.1]) was also significantly different (p<0.001). Among patients with or without ODI4% episodes, the median post-procedure opioid doses were 15.1 (IQR 3.5–43.2) MME and 10.0 (IQR 1.5–34.8) MME, respectively (p=0.010) (Table 1).
Analysis of Oxygen Desaturation and Respiratory Depression Occurrence
To explore the association between ODI4% and RD, we performed univariable analysis of ODI4% episodes with the occurrence of RD. The presence of ≥1 episode of ODI4% was significantly associated with RD occurrence, with an adjusted odds ratio (OR) 1.37 (95% confidence interval [CI] 1.03–1.81, p=0.029). The OR increased as the number of episodes per hour increased (Table 2).
 |
Table 2 Univariable Logistic Regression of Respiratory Depression Occurrence and ODI4% |
Significant factors in the univariable analysis were analyzed with a multivariable regression model to examine the relationship between ODI4% and RD. These factors included the length of continuous monitoring during the overnight hours, geography, opioid naivety, age, male sex and sleep disordered breathing (Figure 2, Supplementary Tables 1–4). As the cutoffs for ODI4% episodes increased from 5 episodes/hour to 10 episodes/hour or 15 episodes/hour, the adjusted OR for RD increased from 2.59 (95% CI 1.72–3.89, p<0.0001) to 3.39 (95% CI 1.80–6.39, p=0.0002), to 4.71 (95% CI 1.93–11.47, p=0.0006), respectively (Table 3). Each logistic regression model had an AUC >0.72, with Hosmer-Lemeshow p-values between 0.30 and 0.71 (Supplementary Tables 1–4). The multivariable regression model also consistently showed age, male gender, a history of sleep disordered breathing, and geographical location in Asia to be associated with RD. At a cutoff of at least 2 episodes of nocturnal RD, the adjusted OR for age ≥80 vs <60 years old was 2.66 (95% CI 2.66–14.38, p<0.0001). For males, the adjusted OR was 1.53 (95% CI 1.53–2.66, p<0.0001), a history of sleep disordered breathing, 1.02 (95% CI 1.02–2.41, p=0.041), and a geographical location in Asia increased the odds of RD to 1.57 (95% CI 1.57–3.32, p<0.0001).
 |
Table 3 Multivariable Analysis of Association Between Number of Episodes of ODI4% and Average Number of Respiratory Depression Episodes/Hour |
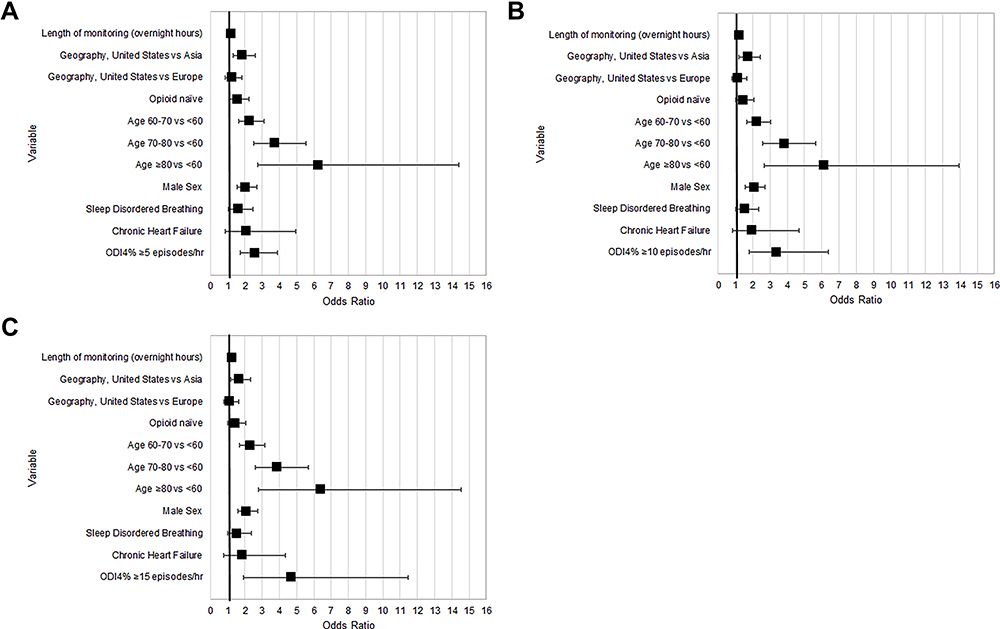 |
Figure 2 Multivariable logistic regression model to evaluate the association between respiratory depression occurrence and oxygen desaturation episodes using ODI4% occurring (A) ≥5 episodes per hour; (B) ≥10 episodes per hour; and (C) ≥15 episodes per hour. |
Association of Oxygen Desaturation with Patient Outcomes
Analysis of respiratory adverse events and ODI4% score found no significant association between the variables, including when evaluated at different ODI episode per hour cutoffs (Table 4). Evaluation of 30-day readmission rates found that 90% of patients re-admitted within 30 days of discharge had at least 1 episode of ODI4%, compared to 76% of patients who were not re-admitted after discharge (p=0.031). There were no other significant differences in 30-day readmissions when considering oxygen desaturation indexes (Table 4).
 |
Table 4 Association Between Oxygen Desaturation Index and Respiratory Adverse Events and 30-Day Readmission After Discharge, Among All 1335 Patients Enrolled in the Trial |
Discussion
Our results showed that both the occurrence of ODI4% and the number of ODI4% events were associated with the incidence of RD. The risk of RD increased significantly in a stepwise manner as the number of episodes of ODI4% increased. A threshold of ≥15 episodes of ODI4% was independently associated with an adjusted OR of 4.7 for RD. This association suggests that ODI4% is strongly correlated with RD. Patients with ≥15 episodes/hour of ODI4% are at a higher risk of RD and should be monitored closely with continuous capnography in addition to continuous pulse oximetry. In addition, our study consistently showed age, male gender, a history of sleep disordered breathing and geographical location in Asia to be associated with RD. This is consistent with the findings of the original PRODIGY study.4 Even in the subset of patients analyzed with varying cut-offs of ODI4% occurrences, the factors found to contribute to RD were consistent with the original PRODIGY score.
In the original PRODIGY study, the PRODIGY score was calculated using a combination of oximetry and capnography to predict RD with an OR 6.07 (95% CI 4.44–8.30, p<0.001).4 Capnography, which assesses ventilation directly, is superior compared to continuous oximetry, which does not directly assess ventilation. However, when capnography monitoring is not available, using continuous oximetry to calculate ODI4% is superior to intermittent oximetry monitoring. In most institutions, oximetry is monitored on the general care floor at intervals of 4 to 6 hours.12,13 An adverse respiratory event can occur during the time between monitoring cycles, as other studies have shown.13,14 Our results are consistent with previous evidence and show nocturnal ODI4% episodes are common, observed in roughly three quarters of our cohort.5,13,15 This suggests that a majority of patients receiving opioids on the general care floor will develop oxyhemoglobin desaturation. The calculation of ODI could detect a current desaturation event, and it may be useful to risk stratify patient subsets at higher risk of future adverse respiratory events. This subset of patients may require a longer period of continuous monitoring to detect adverse respiratory events that require early treatment. In turn, this could prevent more severe complications like respiratory arrest and arrhythmias, which increases patient morbidity and mortality.5 Although the median opioid dosage was statistically higher among patients with ≥1 ODI4% episode, this did not reach clinical significance, and as has been concluded by other studies, opioid dosage alone is likely not sufficient for predicting whether a patient will experience oxygenation or ventilation challenges on the general care floor.9,16
In our study, ODI4% was highly correlated with RD at an optimal cutoff of ≥15 events/hour of ODI4%. There are some other studies that looked at varying cutoffs of ODI, including ODI3%.17 However, the threshold of ODI4% is well supported by several other large studies that use it to predict obstructive sleep apnea. Waseem et al studied 1218 patients using ODI4% to predict moderate to severe and severe OSA and found the optimal cutoff of ≥15 events/hour of ODI4% had high sensitivity and specificity.8 Similarly, Chung et al showed that an ODI4% ≥15 events/hour correlated well with moderate OSA (Apnea-Hypopnea-Index of 15 episodes per hour) with an accuracy of 86%.7
Patients receiving opioid therapy should be monitored with continuous oximetry equipped to calculate ODI4%. With continuous oximetry and capnography, any current respiratory events can be detected. Using the real-time ODI4% measurements, the likelihood of future respiratory events may be evaluated. Patients with an ODI4% frequency of ≥15 events/hour should be considered high risk for subsequent RD events.2 This subset of patients should have a longer period of monitoring and opioids should be prescribed on discharge with great caution. In the future, a wearable device can be considered if these patients were to be discharged home with opioids to detect any adverse respiratory event that can potentially occur post discharge.
Our study did not find associations between ODI4% and adverse events. However, this is likely due to the nature of the post-hoc analysis and the low number of patients who experienced respiratory adverse events, causing the analysis to be underpowered. Hwang et al found that among 172 general surgical patients, patients with ODI ≥5 events/hour had higher postoperative complication rates than those with ODI <5 events/hour (15.3% vs 2.7%; adjusted OR, 7.2).11 Chung et al examined postoperative ODI among 573 general surgical patients and found that patients with ODI >28.5 events/hour have double the risk for postoperative complications.18,19
In our study, the majority of the respiratory depression episodes were due to apnea (97%) while hypoxemia (defined as oxyhemoglobin saturation ≤85% for ≥ 3 minutes) was less common (8%).4 Because ODI4% does not require oxyhemoglobin saturation to decrease to a preset level, it can be more sensitive in identifying patients at risk for serious RD episodes such as apneic pauses. Since many postoperative patients are administered supplemental oxygen, the severity of RD episodes could be masked.4,10 Unfortunately, our data did not allow us to calculate the temporality of the ODI episodes relative to the RD episode, because in the original PRODIGY study not all potential RD episodes were adjudicated. However, Driver et al analyzed a subset of PRODIGY patients whose potential RD episodes were fully adjudicated, and found that patients who developed RD typically had multiple episodes (usually repetitive apneic episodes), with the episodes typically developing in the late afternoon/early evening and peaked in frequency between 02:00 to 06:00.2 This early morning peak correlates with the nocturnal ODI episodes we evaluated between 00:00 and 06:00, suggesting a relationship between these ODI and RD events. Future studies are necessary to prove this relationship. However, studies of postoperative naloxone administration on wards have found that the peak frequency of naloxone administration is within the first few hours following post anesthesia care unit discharge, typically in the late afternoon to early evening the day of surgery,20,21 thus limiting the utility of nocturnal ODI4% to identify patients at risk for RD as many severe events occur before the first night.
There are several limitations to this study. Firstly, in the initial PRODIGY study, the timing of the application of the Capnostream™ monitor was not fixed relative to the end of surgery. Hence, the first RD/ODI episode may have occurred before the monitor application and gone unrecorded, leading to an overestimation of the time to the initial RD/ODI episode.4,12 Secondly, data did not allow temporal comparison of ODI and RD episodes. Thirdly, we did not account for supplemental oxygen administration, which could have mitigated the utility of ODI to detect RD.
Conclusion
Our study suggests that ODI4%, calculated with continuous pulse oximetry is strongly correlated with the risk for RD. Patients with ≥15 episodes of ODI4% are at high risk of RD. The use of continuous pulse oximetry, which can calculate real time ODI4%, could identify high risk patients and allow clinicians to evaluate the need for more intense monitoring, such as continuous capnography.
Abbreviations
OSA, obstructive sleep apnea; OR, odds ratio; CI, confidence interval; AUC, area under the curve; SpO2, oxygen saturation; EtCO2, end-tidal carbon dioxide; ODI, oxygen desaturation index; BMI, body mass index; RD, respiratory depression; ASA, American Society of Anesthesiologists; IV, intravenous; CNS, central nervous system; IQR, interquartile range; MME, morphine milligram equivalents; CPAP, continuous positive airway pressure; PRODIGY, Prediction of Opioid-induced respiratory Depression in patients monitored by capnoGraphY; STROBE, Strengthening the reporting of observational studies in epidemiology.
Data Sharing Statement
The data supporting the conclusions of this article are included within the article and Supplementary Information.
Ethics Approval and Informed Consent
This trial was approved by the institutional review board or research ethics committee of each participating site, including: Western Institutional Review Board (Beaumont Hospital, Emory University, Ohio State University Wexner Medical Center, and Providence Regional Medical Center); University at Buffalo Institutional Review Board (University at Buffalo); Cleveland Clinic Institutional Review Board (Cleveland Clinic); The MetroHealth System Institutional Review Board (MetroHealth Medical Center); Partners Human Research Committee (Brigham and Women’s Hospital); Colorado Multiple Institutional Review Board (University at Colorado); National Healthcare Group (NHG) Domain Specific Review Board (DSRB) (National University of Singapore); CPP Ile de France 2 (Hopital Foch); Ethik Kommission Medizinische Fakultät (University Hospital Bonn); Rinshoushiken Shinsa Senmon Inkai (Okayama University Hospital); The Jikei Ethics Committee (Jikei University); METC MUMC+ (University Medical Center, Maastricht); and Comité de Ética del Hospital Clinico Universitario de Valencia (Hospital Clinico Universitario de Valencia). All patients provided written informed consent before enrollment.
Acknowledgments
PRODIGY Group Investigators: In addition to the listed authors, the PRODIGY Group includes:
Sergio D. Bergese, MD (Department of Anesthesiology, Stony Brook University School of Medicine, Stony Brook, New York, US); Carla R. Jungquist, NP, PhD (University at Buffalo School of Nursing, Buffalo, New York, US); Hiroshi Morimatsu, MD, PhD (Department of Anesthesiology and Resuscitology, Okayama University Hospital, Okayama, Japan); Shoichi Uezono, MD (Jikei University School of Medicine, Tokyo, Japan); Simon Lee, MD (Department of Anesthesiology, Emory University, Atlanta, Georgia, US); Richard D. Urman, MD (Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women’s Hospital, Boston, Massachusetts, US); Robert McIntyre Jr, MD (Department of Surgery, University of Colorado School of Medicine, Aurora, Colorado, US); Carlos Tornero, MD, PhD (Department of Anesthesiology, Resuscitation and Pain Therapeutics, Hospital Clinico Universitario de Valencia, Valencia, Spain); Albert Dahan, MD, PhD (Department of Anesthesiology, Leiden University Medical Center, Leiden, the Netherlands); Leif Saager, MD, MMM (Klinik für Anästhesiologie, Universitätsmedizin Göttingen, Göttingen, Germany); Maria Wittmann, MD (Department of Anaesthesiology, University Hospital Bonn, Bonn, Germany); Dennis Auckley, MD (Division of Pulmonary, Critical Care, and Sleep Medicine, MetroHealth Medical Center, Case Western Reserve University, Cleveland, Ohio, US); Luca Brazzi, MD, PhD (Department of Anesthesia, Intensive Care and Emergency, University of Turin, Turin, Italy); Morgan Le Guen, MD, PhD (Department of Anaesthesiology, Hôpital Foch, Suresnes, France); Roy Soto, MD (Department of Anesthesiology, Beaumont Hospital, Royal Oak, Michigan, US); Frank Schramm, MD (Department of Anesthesiology, Providence Regional Medical Center, Everett, Washington, US); Wolfgang Buhre, MD (Department of Anesthesiology, University Medical Center, Maastricht, the Netherlands); Frank J. Overdyk, MD (Trident Anesthesia Group, LLC, Charleston, South Carolina, US). A portion of this work was presented at the Society of Anesthesia and Sleep Medicine 11th Annual Meeting in Oct 2021 and was recognized as a top abstract (third prize).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The PRODIGY study was funded by Medtronic. All authors (or their institutions) received research support from Medtronic to conduct the study. The authors had access to study data and final responsibility for the decision to submit for publication.
Disclosure
KEL and FDP report Medtronic employment. TNW received consulting fees from Medtronic and Merck. AKK reports consulting fees from Medtronic, Edwards Lifesciences, Philips North America, GE Healthcare, Retia Medical, Potrero Medical, Caretaker Medical, and Trevena Pharmaceuticals, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Lee LA, Caplan RA, Stephens LS, et al. Postoperative opioid-induced respiratory depression: a closed claims analysis. Anesthesiology. 2015;122(3):659–665. doi:10.1097/ALN.0000000000000564
2. Driver CN, Laporta ML, Bergese SD, et al. Frequency and temporal distribution of postoperative respiratory depressive events. Anesth Analg. 2021;132(5):1206–1214. doi:10.1213/ANE.0000000000005478
3. Dahan A, Aarts L, Smith TW. Incidence, reversal, and prevention of opioid-induced respiratory depression. Anesthesiology. 2010;112(1):226–238. doi:10.1097/ALN.0b013e3181c38c25
4. Khanna AK, Bergese SD, Jungquist CR, et al. PRediction of opioid-induced respiratory depression on inpatient wards using continuous capnography and oximetry: an international prospective, observational trial. Anesth Analg. 2020;131(4):1012–1024. doi:10.1213/ANE.0000000000004788
5. Overdyk FJ, Carter R, Maddox RR, Callura J, Herrin AE, Henriquez C. Continuous oximetry/capnometry monitoring reveals frequent desaturation and bradypnea during patient-controlled analgesia. Anesth Analg. 2007;105(2):412–418. doi:10.1213/01.ane.0000269489.26048.63
6. Stites M, Surprise J, McNiel J, Northrop D, De Ruyter M. Continuous capnography reduces the incidence of opioid-induced respiratory rescue by hospital rapid resuscitation team. J Patient Saf. 2021;17(6):e557–e561. doi:10.1097/pts.0000000000000408
7. Chung F, Liao P, Elsaid H, Islam S, Shapiro CM, Sun Y. Oxygen desaturation index from nocturnal oximetry: a sensitive and specific tool to detect sleep-disordered breathing in surgical patients. Anesth Analg. 2012;114(5):993–1000. doi:10.1213/ANE.0b013e318248f4f5
8. Waseem R, Chan MTV, Wang CY, Seet E, Chung F. Predictive performance of oximetry in detecting sleep apnea in surgical patients with cardiovascular risk factors. PLoS One. 2021;16(5):e0250777. doi:10.1371/journal.pone.0250777
9. Urman RD, Khanna AK, Bergese SD, et al. Postoperative opioid administration characteristics associated with opioid-induced respiratory depression: results from the PRODIGY trial. J Clin Anesth. 2021;70:110167. doi:10.1016/j.jclinane.2021.110167
10. Khanna AK, Overdyk FJ, Greening C, Buhre WF, Buhre WF. Respiratory depression in low acuity hospital settings-seeking answers from the PRODIGY trial. J Crit Care. 2018;47:80–87. doi:10.1016/j.jcrc.2018.06.014
11. Hwang D, Shakir N, Limann B, et al. Association of sleep-disordered breathing with postoperative complications. Chest. 2008;133(5):1128–1134. doi:10.1378/chest.07-1488
12. Filson K, Atherholt C, Simoes M, et al. Post-operative vital signs: how often is too often? J Clin Oncol. 2018;36(30_suppl):210. doi:10.1200/JCO.2018.36.30_suppl.210
13. Sun Z, Sessler DI, Dalton JE, et al. Postoperative hypoxemia is common and persistent: a prospective blinded observational study. Anesth Analg. 2015;121(3):709–715. doi:10.1213/ANE.0000000000000836
14. Anderloni A, Fugazza A, Troncone E, et al. Single-stage EUS-guided choledochoduodenostomy using a lumen-apposing metal stent for malignant distal biliary obstruction. Gastrointest Endosc. 2018;87:AB347. doi:10.1016/j.gie.2018.08.047
15. Urman RD, Seger DL, Fiskio JM, et al. The burden of opioid-related adverse drug events on hospitalized previously opioid-free surgical patients. J Patient Saf. 2021;17(2):e76–e83. doi:10.1097/PTS.0000000000000566
16. Belcher AW, Khanna AK, Leung S, et al. Long-acting patient-controlled opioids are not associated with more postoperative hypoxemia than short-acting patient-controlled opioids after noncardiac surgery: a cohort analysis. Anesth Analg. 2016;123(6):1471–1479. doi:10.1213/ane.0000000000001534
17. Ng Y, Joosten SA, Edwards BA, et al. Oxygen desaturation index differs significantly between types of sleep software. J Clin Sleep Med. 2017;13(4):599–605. doi:10.5664/jcsm.6552
18. Chung F, Zhou L, Liao P. Parameters from preoperative overnight oximetry predict postoperative adverse events. Minerva Anestesiol. 2014;80(10):1084–1095.
19. Suen C, Ryan CM, Mubashir T, et al. Sleep study and oximetry parameters for predicting postoperative complications in patients with OSA. Chest. 2019;155(4):855–867. doi:10.1016/j.chest.2018.09.030
20. Weingarten TN, Herasevich V, McGlinch MC, et al. Predictors of delayed postoperative respiratory depression assessed from naloxone administration. Anesth Analg. 2015;121(2):422–429. doi:10.1213/ANE.0000000000000792
21. Deljou A, Hedrick SJ, Portner ER, et al. Pattern of perioperative gabapentinoid use and risk for postoperative naloxone administration. Br J Anaesth. 2018;120(4):798–806. doi:10.1016/j.bja.2017.11.113
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.